Embed Size (px)
Citation preview

Comparison of Morphologic Findings in Spontaneously Occurring Hypertrophic
Cardiomyopathy in Humans, Cats and Dogs Si-Kwang Liu, DVM, PhD, William C. Roberts, MD, and Barry J. Maron, MD
Morphologic features of spontaneously occurring hypertrophic cardiomyopathy (HC) were compared in 38 humans, 51 cats and 10 dogs. Asymmetric hypertrophy of the ventricular septum, marked disorganization of cardiac muscle cells, abnormal intramural coronary arteries and myocardial fib* sis were each present in the ventricular septum of human, feline, and canine forms of HC; these ab normalities were generally more severe and most frequently identified in humans. Asymmetric left ventricular hypertrophy (based on the calculated septal-t&e wall thickness ratio) was most corn mon in humans (31 of 38 [Sl%]) and dogs (8 of 10 [80%]), as compared with cats (16 of 51[31%]; p ~0.001) with HC; In all 3 species, hypertrophy was often diffuse, involving substantial portions of the anterolateral and posterior free walls, and the ventricular septum. Marked septal disorganization (25% of the tissue section) was present in 35 pa- tients (92%), bwt in only 14 cats (27%) and 2 dogs (20%) (p *O.OOl). Abnormal intramural coronary aIc teties occurred with similar frequency in the veb tricular septum of patients (n q 25; 66%), cats (n q 38; 74%) and dogs (n q 6; 60%) (p cNS). Mob erateto-severe septal fibrosis was identiied more commonly in humans (15 of 38 [39%]) than in ani- mals (13 of 61 [21%]; p ~0.001). In all 3 species, abnormal intramural coronary arteries were most commonly observed within or at the marguts of areas of fibrous tissue. 7hese morphologic fin& ings describe spontaneously occurring models of HC in cats and dogs with substantial stnrctural similarities to the well-recognized disease entity in humans.
(AmJCardiol1993372:944-951)
From the Department of Pathology, The Animal Medical Center, New York, New York, and the Pathology Branch, National Heart, Lung, and Blood Institute, National Institutes of Health, Bethesda, Maryland. Manuscript received February 22, 1993; revised manuscript received and accepted June 7,1993.
Address for reprints: Si-Kwang Liu, DVM, PhD, Department of Pathology, The Animal Medical Center, 510 East 62nd Street, New York, New York 10021.
H ypertrophic cardiomyopathy (HC) is a primary (and often familial) cardiac disease in which the most characteristic morphologic feature is a hy-
pertrophied, nondilated left ventricle,1 and the myo- cardium typically shows bizarre and disorganized cellu- lar architecture, abnormal small intramural coronary ar- teries and increased amounts of matrix or replacement fibrosis.2-23 Although HC has been a well-recognized and extensively studied clinical and pathologic entity in patients since 1958,2J4J5 a morphologically similar con- dition occurring spontaneously in cats24,25 and dogs2(j,” has only more recently been identified. The present study extends our morphologic observations to the ca- nine and feline forms of HC, and compares certain struc- tural hallmarks of this disease observed at necropsy.
METHODS Selection of case material: The cardiovascular regis-
try of the Pathology Department of The, Animal Medi- cal Center was reviewed for a 2-year period. During that time, 189 cats and 177 dogs with cardiac disease were examined at necropsy; the hearts of 51 cats and 10 dogs were identitied as having HC. Of 61 animals, 50 (82%) were male. Cats with HC were most commonly of the domestic shorthair breed (n = 39 [77%]); in addition, 7 (14%) were Persian, 4 (8%) were Siamese, and 1 (1%) was Maine Coon. Four dogs were German shepherds, and 1 each was a Doberman pinscher, Airedale, French poodle, Great Dane, bulldog and Boston terrier. In the 61 animals, death was sudden in 23 (38%), due to heart failure with or without thromboembolism in 33 (54%), and due to noncardiac causes in 5 (8%).
Case records of the Pathology Branch of the Nation- al Heart, Lung, and Blood Institute were reviewed also, and 38 hearts with HC that previously underwent de- tailed histologic characterization were selected for com- parative study. - 5 11~15,23,28 Patients were aged 11 to 53 years (mean 26); 17 (45%) were male. Five patients had symptoms of cardiac dysfunction; 15 had been asympto- matic, and sudden death was the first deftnitive mani- festation of their cardiac disease. Death was sudden in 22 patients, due to congestive heart failure in 5, during or shortly after operation in 8, and a result of cerebro- vascular accident, suicide or cardiac catheterization in 1 each. Of 25 patients with cardiac catheterization, 16 had obstruction to left ventricular outflow (gradient 230 mm Hg under basal or provocable conditions), and the other 9 were nonobstructive.
The diagnosis of HC in all 99 hearts studied was based on the presence of a hypertropbied nondilated left ventricle in the absence of another cardiac or systemic disease (such as systemic hypertension, aortic valvular
944 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 72 OCTOBER 15, 1993
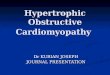
stenosis or coronary artery disease) capable of produc- ing the magnitude of hypertrophy present in that pa- tient.’ The hearts of 60 cats, 25 dogs and 83 human pa- tients that died of cardiac diseases other than HC, or of noncardiac causes and had normal hearts, both struc- turally and functionally, were studied for the purposes of selected morphologic comparisons (Table I).
Preparation of tissue: In each of the 273 humans, cats and dogs studied (99 with HC, and 174 controls), full-thickness tissue blocks were obtained from the left ventricular wall in the transverse plane perpendicular to the long axis of the left ventricle, approximately one half the distance between the apex and base of the aortic valve, in the: (1) ventricular septum, (2) anterolateral free wall approximately 2 cm lateral to the left anterior descending coronary artery, and (3) posterior free wall between the papillary muscles. Tissue was imbedded in paraflin, sectioned at 6 p thickness, and stained with hematoxylin and eosin or Movat’s pentachrome.
Left ventricular wall thicknesses were measured in formalin-iixed gross specimens perpendicular to the en- docardial surfaces. Trabeculae, papillary muscles, crista supraventricular muscle and the endocardial contact plaques were excluded from these measurements.
Definition and classification of abnormal cardiac muscle cell mngement: Cardiac muscle cell disorga- nization was classified into 2 major types. Type I disor- ganization, the most common, consisted of areas of my- ocardium in which adjacent cells were aligned per- pendicularly or obliquely to each other, forming tangled masses or ‘ ‘pinwheel’ ’ configurations. Alternatively, type I disorganization appeared as relatively broad bun- dles of muscle cells oriented at oblique or perpendicu- lar angles to each other; cells within these bundles were normally arranged.
Type I[ disorganization consisted of relatively nar- row, longitudinally cut bundles of cells that were inter- laced in various directions among larger groups of trans- versely cut cells (which appeared circular). This type of disorganization gave the myocardium a distinctive “swirled’ ’ appearance.
Abnormally arranged cardiac muscle cells were not considered representative of true disorganization if pres- ent in areas where cells normally converge at acute an- gles: (1) junction of ventricular septum with ventricular free walls; (2) trabeculations; (3) edges of areas of fi- brosis; (4) points of convergence of major muscle bun- dles; or (5) adjacent to interstitial spaces.
~~mtitation ofcmtll musde cell wemenk A previously described technique was used to quanti- tatively assess the extent to which cardiac muscle cell disorganization was present in each tissue section?-9 Histologic sections were photographed, and the images were enlarged to occupy 30 X 40 inch positive prints. A transparent cellulose overlay was placed over the print. Areas of myocardium occupied by disorganized cardiac muscle cells were outlined. The transparent overlay was then reproduced as a 5 X 7 inch photo- graph. Areas into which the tissue section had been di- vided were outlined separately with a line-point mark- ing pen on tablet paper and quantitated using a video planimetry system; the percent area of tissue section oc-
TABLE I Cardiac Diseases in 168 Control Patients or Animals
Disease -
Cats Dogs Humans
Aortic valve disease 0 0 17 - Coronary heart disease 0 0 15 Mitral valve disease 0 0 10 Systemrc hypertension 0 0 8 Dilated (congestive) cardiomyopathy 16 3 6 Primary pulmonary hypertension 0 0 6 Pulmonary valve stenosis 0 0 3 Aortic & mitral valve disease 0 0 2 Supravalvular aortic stenosis 2 0 2 Ventricular septal defect 0 1 2 Discrete subaortic stenosis 0 2 1 Malformation mitral valve complex 3 2 0 Dysplasia of tricuspid valve 3 2 0 Normal heart 36 15 11
Total 60 25 83
cupied by disorganized cardiac muscle cells calculated with respect to the area of myocardium “at risk” for disorganization.
Analysis of intramural coronary arteries: Assess- ment of intramural coronary artery anatomy was con- tinned to those small vessels (~1,500 l.r diameter in hu- mans, and ~1,200 k in animals) that were viewed in cross section (transverse cut) without obvious obliquity and did not appear to be branches of intramural vessels, or portions of a “tunneled” epicardial vessel. Small cor- onary arteries present in trabeculae or papillary muscles were excluded from this analysis. Sections were consid- ered abnormal with >l abnormal intramural coronary artery in humans and 1 or more arteries in animals.
Analysis of myacardial fibrosis: The extent of fi- brous tissue formation was assessed qualitatively in each tissue section. Mild fibrosis was judged to be present when an isolated small scar or prominent interstitial fi- brous tissue, or both, was identified; severe fibrosis con- sisted of replacement scarring occupying substantial por- tions of the tissue section. Moderate fibrosis was in- termediate in extent between the mild and severe grades.
Statistical methods: Data were expressed as mean Z!Z SEM. Differences between means were assessed by Student’s unpaired t test and l-way analysis of variance.
RESULTS Heart weigh& Heart weights were 19 to 33 g (28.0
+ 0.5 SEM) in the 51 cats, and 98 to 385 g (231 Z!Y 23) in the 10 dogs. Heart weight in relation to body weight was significantly greater in cats (6.4 + 0.1 g/kg) and dogs (9.6 + 0.3 g/kg) with HC than in normal control cats (4.8 f 0.1 g/kg; p <O.OOl) and dogs (6.6 If: 0.3 g/kg; p <O.OOl). Heart weights were 300 to 1,002 g (548 f 35) in the 28 adult patients with HC, and 270 to 650 g (457 f 36) in the 10 children aged ~18 years.
Ventricular septal tlridmess (Figure 1 and TaMe II): Maximal ventricular septal thickness was 9.0 f 0.2 mm in the 51 cats, and 19 + 2 in the 10 dogs with HC, and was significantly greater in these cats and dogs than in their respective controls with normal hearts (5.0 f 0.2 and 12.0 + 0.5 mm; p <O.OOl). Ventricular septal thick- ness in each patient with HC exceeded the generally ac- cepted upper limits for necropsy measurements (i.e., 15
HC IN HUMANS, CATS AND DOGS 945
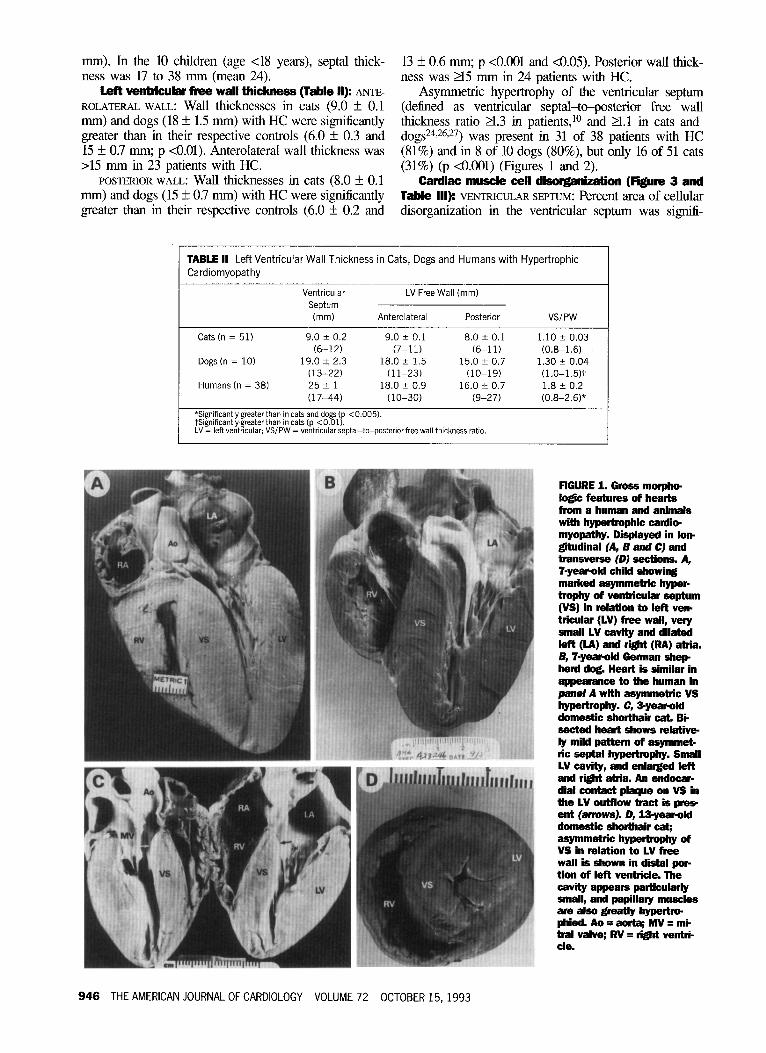
mm). In the 10 children (age ~18 years), septal thick- 13 f 0.6 mm; p <O.OOl and ~0.05). Posterior wall thick- ness was 17 to 38 mm (mean 24). ness was 215 mm in 24 patients with HC.
Left venWcular free wall thickness (TaMe II): ANTE-
ROLATERAL WALL: wall thiCktleSSeS in Cats (9.0 + 0.1 mm) and dogs (18 + 1.5 mm) with HC were significantly greater than in their respective controls (6.0 f 0.3 and 15 * 0.7 mm; p cO.01). Anterolateral wall thickness was >15 mm in 23 patients with HC.
Asymmetric hypertrophy of the ventricular septum (defined as ventricular septal-t-posterior free wall thickness ratio a.3 in patients,‘O and 21.1 in cats and dogs24>26,“) was present in 31 of 38 patients with HC (81%) and in 8 of 10 dogs (SO%), but only 16 of 51 cats (31%) (p <O.OOl) 0;igures 1 and 2).
POSTERIOR WALL: Wall thicknesses in cats (8.0 + 0.1 mm) and dogs (15 I!I 0.7 mm) with HC were significantly greater than in their respective controls (6.0 f 0.2 and
Cardiac muscle cell disorganizath (Figure 3 and Table Ill): VENTRICULAR SEPTUM: Percent area of cellular disorganization in the ventricular septum was signiti-
TABLE II Left Ventricular Wall Thickness in Cats, Dogs and Humans with Hypertrophic Cardiomyopathy
Ventricular Septum
(mm)
LV Free Wall (mm)
Anterolateral Posterior VSIPW
Cats h = 51) 9.0 + 0.2 9.0 + 0.1 8.0 zk 0.1 1.10 k 0.03 (6-12) (7-l 1) (6-11) (0.8-1.6)
Dogs (n = 10) 19.0 2 2.3 18.0 f 1.5 15.0 2 0.7 1.30 k 0.04 (13-22) (1 l-23) (10-19) (l.O-1.5jt
Humans (n = 38) 25 f 1 18.0 e 0.9 16.0 iz 0.7 1.8 k 0.2 (17-44) (10-30) (9-27) (0.8-2.6)*
*Significantly greater than in cats and dogs (p <0.005). tsignificantlygreaterthan in cats(p <O.Ol). LV = left ventricular; VSIPW = ventricularseptal-to-posterior free wall thickness ratio.
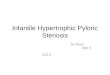
RGUREl.Gross me lo& features of hearts from a human and animals with hypertrophic cardb myopathy. Displayed in lou grtudinal (A, B and C) and transverse (0) sections. A, 7.year-old child showing marked asymmetric hyper- trophy of ventricular septum (VS) in relation to left verb tricular (LV) free wall, very small LV cavity and dilated left (LA) and right (RA) atria. B, ‘I-year-aid Berman shep herd dog. Heart is similar in appearance to the human in panel A with asymmetric VS hypertrophy. C, syeawld domestic shorthair cat. Bi- sected heart shows relativ* ly mild pattern of asymmet- lit septal hypertrophy. Small LV cavity, and enlalged left and ri&t atria. An endocap dial contact plaque on VS in the LV outflow tract is pre, ent (amws). D, U-year-old domestic shorthair eat; asymmetric hypertrophy of VS in relation to LV free wall is shown in distal por- tion of left ventricle. The cavity appears partiilarly small, and papillary muscles are also greatly hypertr@ phied. Ao q aorta; MV q mC tral valve; RV q li@t ventri- cle.
946 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 72 OCTOBER 15,1993
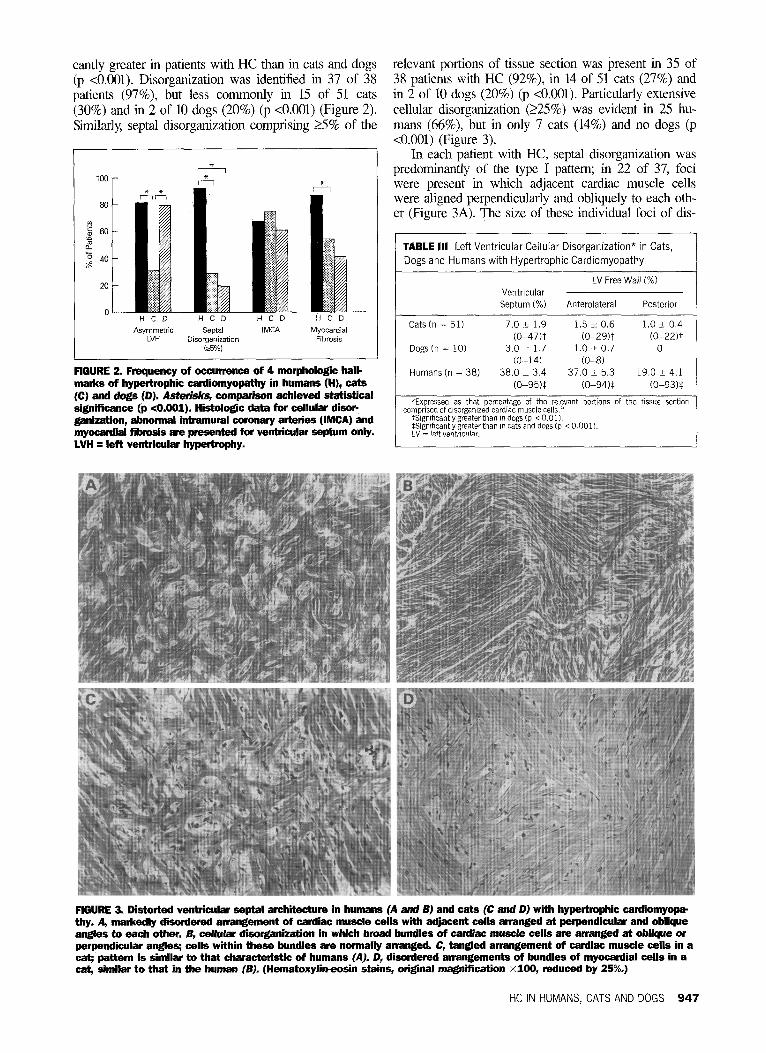
cantly greater in patients with HC than in cats and dogs relevant portions of tissue section was present in 35 of (p <O.OOl). Disorganization was identified in 37 of 38 38 patients with HC (92%), in 14 of 51 cats (27%) and patients (97%), but less commonly in 15 of 51 cats in 2 of 10 dogs (20%) (p <O.OOl). Particularly extensive (30%) and in 2 of 10 dogs (20%) (p <O.OOl) (Figure 2). cellular disorganization (225%) was evident in 25 hu- Similarly, septal disorganization comprising 25% of the mans (66%), but in only 7 cats (14%) and no dogs (p
<O.OOl) (Figure 3).
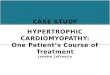
flGURE 2. Frequency of occurrence of 4 morphologic hall- marks of hypertrophic cardiomyopathy in humans (H), cats
80
20
0 HCD HCD HCD HCD
Asymmetric Sepvll IMCA Myocardial LVH Disorganization Fibrosis
k5%)
In each patient with HC, septal disorganization was predominantly of the type I pattern; in 22 of 37, foci were present in which adjacent cardiac muscle cells were aligned perpendicularly and obliquely to each oth- er (Figure 3A). The size of these individual foci of dis-
TABLE Ill Left Ventricular Cellular Disorganization* in Cats, Dogs and Humans with Hypertrophic Cardiomyopathy
LV Free Wall (%) Ventricular
septum (%) Anterolateral Posterior
Cats (n = 51) 7.0 t 1.9 1.5 j: 0.6 1.0 & 0.4 co-47H co-29Yl (O-22Yt
Dogs (n = 10) 3.0 + 1.7 1.0 -t 0.7 0 (O-14) (O-8)
Humans (n = 38) 38.0 ? 3.4 37.0 2 5.3 19.0 + 4.1 co-95H (O-94)$ (O-93)$
(C) and dogs (D). Asterisks, comparison achiived statistical significance (p <O.OOl). Histologic data for cellular disolc
*Expressed as that percentage of the relevant portions of the tissue section comprised of disorganized cardiac muscle cell~.~
ganization, abnormal intramural coronary arteries (IMCA) and myocardii fibrosis are presented for ventricular septum only. LVH q left ventricular hypertrophy.
tSlgnlficantlygreaterthan indogs (p <O.Ol). lsigniflcantlygreater than m cats and dogs (p <O.OOl). LV = left ventricular.
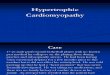
RGURE 3. Distorted ventricular septal archiiecture in humans (A and B) and cats (C and D) with hypertrophic cardiomyop thy. A, markedly disordered an-angement of cardiac muscle cells with adjacent cells arranged at perpendicular and oblique angles to each other. 6, cellular disorganization in whii broad bundles of cardiac muscle cells are arranged at oblique or perpendicular angles; cells within these bundles are normally arranged. C, tangled arrangement of cardiac muscle cells in a eat; pattern is similar to that characteristic of humans (A]- D, disordered anangements of bundles of myocardial cells in a cat, similar to that in the human (BJ (Hematoxylirreosin stains, origmal magnification X100, reduced by 25%.)
HC IN HUMANS, CATS AND DOGS 947
organization showed great variability, but most were rel- In animals with HC, type I disorganization involving atively small. The other 15 patients had type I disor- foci of adjacent cardiac muscle cells also predominated ganization in which broad bundles of cells were orient- (Figure 3C). These areas of disorganization varied con- ed at oblique and perpendicular angles (Figure 3B). siderably in size, but were usually smaller than in pa- Type II disorganization also was present in 5 patients. tients with HC. Cats often showed a distinctive “swiss
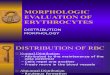
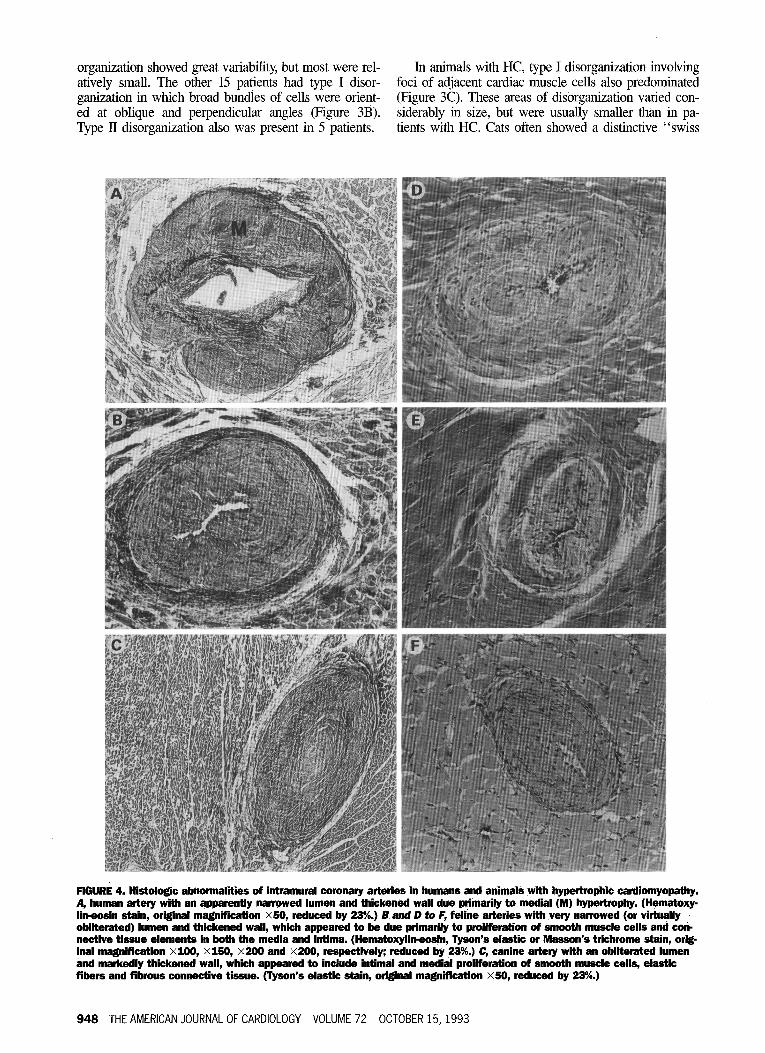
flGURE 4. Histologic abnormalities of intramural coronary arteries in humans and animals with hypertrophic cardiomyopathy. A, human artery with an apparently narrowed lumen and thickened wall due primarily to medial (M) hyperbophy. (Hematoxy- lhr-eosin stain, original magnification X50, reduced by 23%.) B and D to F, feline arteries with very narrowed (or virtually ’ obliterated) lumen and thickened wall, which appeared to be due primarily to prolffmtion of smooth muscle cells and COW nective tissue elements in both the media and brtima. (Hematoxylirreosin, Tyson’s elastic or Masson’s trichrome stain, ori& inal magnification X100, X150, X200 and X200, respectively; reduced by 23%.) C, canine artery with an obliterated lumen and markedly thickened wall, which appeared to include httimal and medial proliferation of smooth muscle cells, elastic fibers and fibrous connective tissue. (Tyson’s elastic stain, origbial magnification X50, reduced by 23%.)
948 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 72 OCTOBER 15,1993
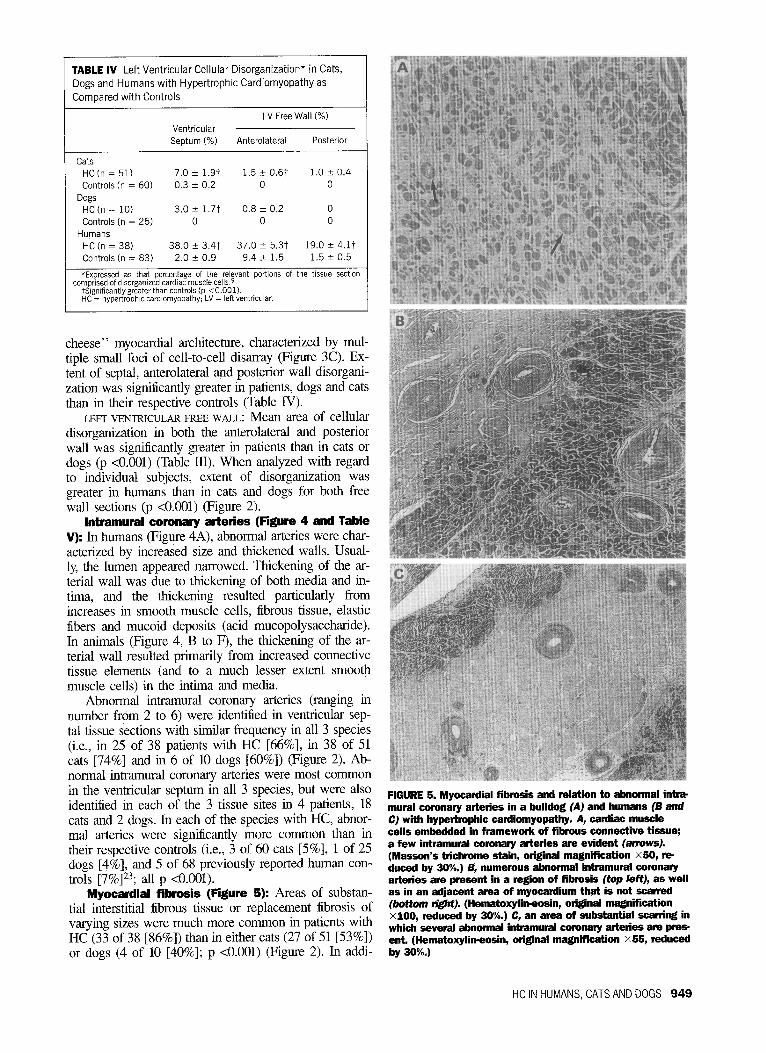
TABLE IV Left Ventricular Cellular Disorganization* in Cats, Dogs and Humans with Hypertrophic Cardiomyopathy as Compared with Controls
Ventricular Septum (%)
LV Free Wall (%)
Anterolaterai Posterior
Cats HC (n = 51) 7.0 F 1.91 1.5 t 0.6t 1.0 k 0.4 Controls (n = 60) 0.3 k 0.2 0 0
Dogs HC (n = 10) 3.0 f 1.7t 0.8 i 0.2 0 Controls (n = 25) 0 0 0
Humans HC (n = 38) 38.0 2 3.4t 37.0 f 5.3t 19.0 + 4.17 Controls (n = 83) 2.0 f 0.9 9.4 2 1.5 1.5 + 0.5
*Expressed as that percentage of the relevant portions of the tissue section comprised of disorganized cardiac muscle cell~.~
tslgnificantlygreater than controls (p <O.OOl). HC = hypettrophic cardlomyapathy; LV = left ventricular.
,
cheese” myocardial architecture, characterized by mul- tiple small foci of cell-to-cell disarray (Figure 3C). Ex- tent of septal, anterolateral and posterior wall disorgani- zation was significantly greater in patients, dogs and cats than in their respective controls (Table IV).
cm ~~~N~KuLAR FREE WALL: Mean area of cellular disorganization in both the anterolateral and posterior wall was significantly greater in patients than in cats or dogs (p <O.OOl) (Table Ill). When analyzed with regard to individual subjects, extent of disorganization was greater in humans than in cats and dogs for both free wall sections (p <O.OOl) (Figure 2).
Intramural coronary arteries (Figure 4 and Table V): In humans (Figure 4A), abnormal arteries were char- acterized by increased size and thickened walls. Usual- ly, the lumen appeared narrowed. Thickening of the a.r- terial wall was due to thickening of both media and in- tima, and the thickening resulted particularly from increases in smooth muscle cells, fibrous tissue, elastic fibers and mucoid deposits (acid mucopolysaccharide). In animals (Figure 4, B to F), the thickening of the ar- terial wall resulted primarily from increased connective tissue elements (and to a much lesser extent smooth muscle cells) in the intima and media.
Abnormal intramural coronary arteries (ranging in number from 2 to 6) were identified in ventricular sep- tal tissue sections with similar frequency in all 3 species (i.e., in 25 of 38 patients with HC [66%], in 38 of 51 cats [74%] and in 6 of 10 dogs [60%]) (Figure 2). Ab- normal intramural coronary arteries were most common in the ventricular septum in all 3 species, but were also identified in each of the 3 tissue sites in 4 patients, 18 cats and 2 dogs. In each of the species with HC, abnor- mal arteries were signiiicantly more common than in their respective controls (i.e., 3 of 60 cats [5%], 1 of 25 dogs [4%], and 5 of 68 previously reported human con- trols [7%]23; all p <O.OOl).
Myocardial fibrosis (Figure 5): Areas of substan- tial interstitial fibrous tissue or replacement fibrosis of varying sizes were much more common in patients with HC (33 of 38 [86%]) than in either cats (27 of 51 [53%]) or dogs (4 of 10 [40%]; p <O.OOl) (Figure 2). In addi-
FIGURE 5. Myocardial fibrosis and relation to abnormal itirr mural coronary arteries in a bulldog (A] and humans (6 and C) with hypertrophic cardiomyopathy. A, cardiac muscle cells embedded in framewoh of fibrous connective tissue; a few intramural coronary arteries are evident (arrowsJ. (Masson’s trichrome stain, original magnification X50, r* duced by 30%.) B, numerous abnormal intramural coronary arteries are present in a redon of fibrosis (top left), as well as in an adjacent area of myocardium that is not scarred (bottom riglft], (Hematoxyiirreosin, original magnification X100, reduced by 30%.) C, an area of substantial scant@ in which several abnormal intramural coronary artelies a~ pres- ent. (Hematoxylirreosin, original magnifcation X55, reduced by 30%.)
HC IN HUMANS, CATS AND DOGS 949
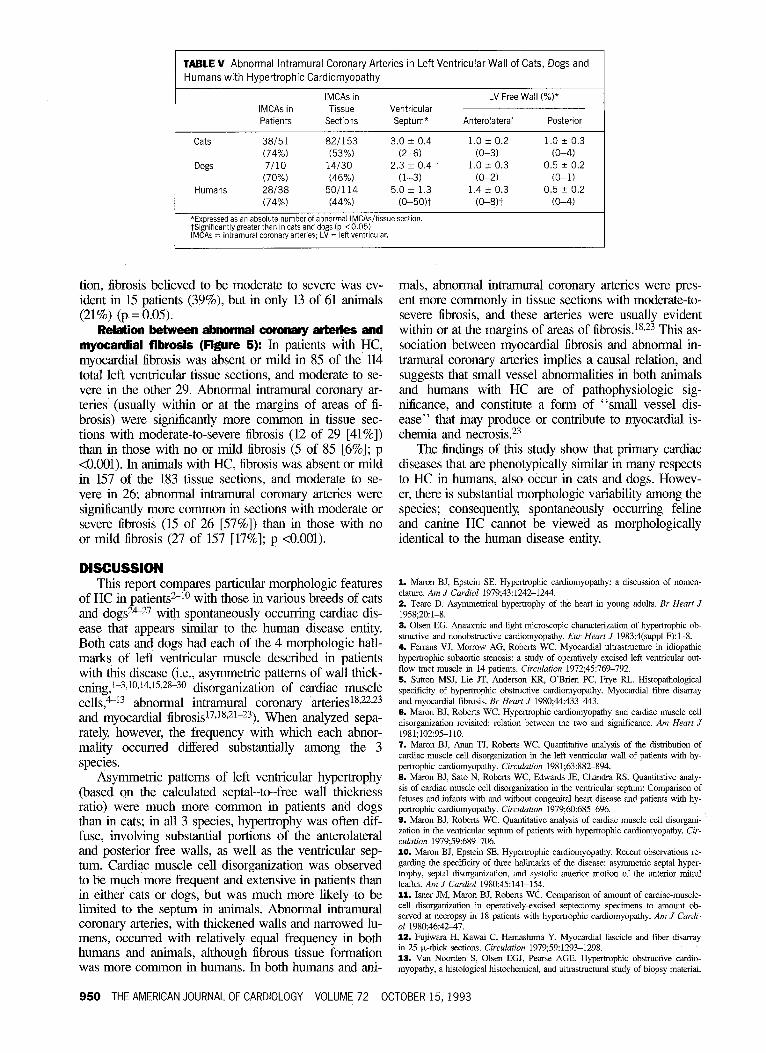
TABLE V Abnormal Intramural Coronary Arteries in Left Ventricular Wall of Cats, Dogs and Humans with Hypertrophic Cardiomyopathy
IMCAs in Patients
IMCAs in Tissue
Sections Ventricular
Septum*
LV Free Wall (%I*
Anterolateral Posterior
Cats 38151 821153 3.0 k 0.4 1.0 k 0.2 1 .o z!z 0.3 (74%) (53%) (Z-6) (O-3) (O-4)
Dogs 7110 14/30 2.3 2 0.4 1.0 + 0.3 0.5 + 0.2 (70%) (46%) (l-3) (O-2) (0-l)
Humans 28138 501114 5.0 2 1.3 1.4 2 0.3 0.5 ” 0.2 (74%) (44%) co-50H (O-8)? (O-4)
*Expressed as an absolute number of abnormal IMCAsitissue section. tsignificantlygreater than in cats and dogs (p <0.05). IMCAs = intramural coronary arteries; LV = left ventricular.
tion, fibrosis believed to be moderate to severe was ev- ident in 15 patients (39%), but in only 13 of 61 animals (21%) (p = 0.05).
Relation betwean abnormal coronary arteries and myocardial fibrosis (Figure 5): In patients with HC, rnyocardial fibrosis was absent or mild in 85 of the 114 total left ventricular tissue sections, and moderate to se- vere in the other 29. Abnormal intramural coronary ar- teries (usually within or at the margins of areas of fi- brosis) were significantly more common in tissue sec- tions with moderate-to-severe fibrosis (12 of 29 [41%]) than in those with no or mild fibrosis (5 of 85 [6%]; p <O.OOl). In animals with HC, fibrosis was absent or mild in 157 of the 183 tissue sections, and moderate to se- vere in 26; abnormal intramural coronary arteries were significantly more common in sections with moderate or severe fibrosis (15 of 26 [57%]) than in those with no or mild fibrosis (27 of 157 [17%]; p <O.OOl).
DISCUSSION This report compares particular morphologic features
of HC in patients2-lo with those in various breeds of cats and dogs24-27 with spontaneously occurring cardiac dis- ease that appears similar to the human disease entity. Both cats and dogs had each of the 4 morphologic hall- marks of left ventricular muscle described in patients with this disease (i.e., asymmetric patterns of wall thick- en~g,l-3,10,14,15,28-30 di sorganization of cardiac muscle cells4-13 abnormal intramural coronary arteries1s~22~23 and myocardial fibrosis 17J8,21-23). When analyzed sepa- rately, however, the frequency with which each abnor- mality occurred differed substantially among the 3 species.
Asymmetric patterns of left ventricular hypertrophy (based on the calculated septal-to-free wall thickness ratio) were much more common in patients and dogs than in cats; in all 3 species, hypertrophy was often dif- fuse, involving substantial portions of the anterolateral and posterior free walls, as well as the ventricular sep- tum. Cardiac muscle cell disorganization was observed to be much more frequent and extensive in patients than in either cats or dogs, but was much more likely to be liited to the septum in animals. Abnormal intramural coronary arteries, with thickened walls and narrowed lu- mens, occurred with relatively equal frequency in both humans and animals, although fibrous tissue formation was more common in humans. In both humans and ani-
mals, abnormal intramural coronary arteries were pres- ent more commonly in tissue sections with moderate-to- severe fibrosis, and these arteries were usually evident within or at the margins of areas of fibrosis.1s,23 This as- sociation between myocardial fibrosis and abnormal in- tramural coronary arteries implies a causal relation, and suggests that small vessel abnormalities in both animals and humans with HC are of pathophysiologic sig- nificance, and constitute a form of “small vessel dis- ease” that may produce or contribute to myocardial is- chemia and necrosis.23
The findings of this study show that primary cardiac diseases that are phenotypically similar in many respects to HC in humans, also occur in cats and dogs. Howev- er, there is substantial morphologic variability among the species; consequently, spontaneously occurring feline and canine HC cannot be viewed as morphologically identical to the human disease entity.
1. Maron BJ, Epstein SE. Hypertrophic cardiomyopathy: a discussion of nomen- clature. Am J Cardiol 1979;43:1242-1244. 2. Teare D. Asymmetrical hypemophy of the heart in young adults. Br He& J 1958;20:1-8. 3. Olsen EG. Anatomic and light microscopic characterization of hypertrophic ob- stmctive and nonobstructive cardiomyopathy. Eur Heart J 1983;4(suppl F):l-8. 4. Femans VJ, Morrow AG, Roberts WC. Myocaniial ultrastructure in idiopathic hypetiophic subaortic stenosis: a study of operatively excised left ventricular out- flow tract muscle in 14 patients. Circuhtion 1972;45:76%792. 5. Sutton MSJ, Lie JT, Anderson KR, O’Brien PC, Frye RL. Histopathological specificity of hypertrophic obstmctive cardiomyopathy. Myocardial fibre disarray and myocardial fibrosis. Br Heart .I 1980;44:433443. 6. Maron BJ, Roberts WC. Hypemophic cardiomyopathy and cardiac muscle cell disorganization revisited: relation between the hvo and significance. Am Heart J 1981;102:95-110. 7. Maron BJ, Anan TJ, Roberts WC. Quantitative analysis of the distribution of cardiac muscle cell disorganization in the left ventricular wall of patients with hy- pertrophic cardiomyopathy. Circulation 198 1;63:882-894. 6. Maron BJ, Sato N, Roberts WC, Edwards JE, Char&a RS. Quantitative a&y- sis of cardiac muscle cell disorganization in the ventricular septum: Comparison of fetuses and infants with and without congenital heart disease and patients with hy- pertrophic cardiomyopathy. Circuhtion 1979;60:685696. 6. Maron BJ, Roberts WC. Quantitative analysis of cardiac muscle cell disorgani- zation in the ventricular septum of patients with hypertrophic cardiomyopathy. Cir- culation 1979;59:689-706. 10. Maron BJ, Epstein SE. Hypemophic cardiomyopathy. Recent observations re- garding the specificity of three hallmarks of the disease: asymmetric septal hyper- trophy, septal disorganization, and systolic anterior motion of the anterior mitral leaflet. Am J Cardiol 1980;45:141-154. 11. Isner JM, Maron BJ, Roberts WC. Comparison of amount of cardiac-muscle- cell disorganization in operatively-excised septectomy specimens to amount ob- served at necropsy in 18 patients with hypertrophic cardiomyopathy. Am J Cardi- 01 1980:46:42-47. 12. Fujiwara H, Kawai C, Hamashima Y. Myocardial fascicle and fiber disarray in 25 k-thick sections. Circulation 1979;59:1293-1298. 13. Van Noorden S, Olsen EGJ, Peane AGE. Hypertrophic obstructive cardio- myopathy, a histological histochemical, and ultrastructural study of biopsy material.
950 THE AMERICAN JOURNAL OF CARDIOLOGY VOLUME 72 OCTOBER 15,1993

Cardiovasc Res 1971;5:118-13 1. 14. Wigle ED, Sasson 2, Henderson MA, Ruddy TD, Fulop J, Rakowski H, Williams WG. Hypettrophic cardiomyopathy. The importance of the site and the extent of hypemophy. A review. Prog Cardiovasc Dis 1985;28:1-83. 15. Maron BJ, Bonow RO, Cannon RO, Leon MB, Epstein SE. Hypertrophic car- diomyopathy: interrelation of clinical manifestations, pathophysiology and therapy. N Engl J Med 1987;316:780-789, 841c852. 16. McKenna WJ, Camm AJ. Sudden death in hypertrophic cardiomyopathy: as- sessment of patients at high risk. Circulation 1989;SO: 1489-1492. 17. Roberts CS, Roberts WC. Morphologic features. In: Zipes DP, Rowlands DJ, eds. Progress in Cardiology 212. Philadelphia: Lea & Febiger, 19893-22. 18. Maron BJ, Epstein SE, Roberts WC. Hypertmphic cardiomyopathy and trans. mural myocadial infarction without significant atherosclerosis of the extramural coronary armies. Am J Cardiol 1979;43: 108&1102. 19. Goodwin JF. Congestive and hypertrophic cardiomyopathies: a decade of study. Lmtcet 1970;1:731-739. 20. Spirit0 P, Maron BJ. Relation between extent of left ventricular hypemophy and diastolic ffiling abnormalities in hypertrophic cardiomyopathy. J Am Ml Car- dial 1990;15:808-813. 21. Factor SM, Butany J, Sole MJ, Wigle ED, Williams WC, Rojkind M. Patho- logic fibrosis and matrix connective tissue in the subaortic myocaxlium of patients with hypertrophic cardiomyopathy. J Am CoN Cardiol 1991;17:1343-1351.
22. Tanaka M, Fujiwara H, Onodera T, Wu D-J, Hamashima Y, Kawai C. Quan- titative analysis of myocardial fibrosis in normals, hypertensive hearts, and hyper- trophic cardiomyopathy. Br Heart J 1986;55:575-581. 23. Maron BJ, Wolfson JK, Epstein SE, Roberts WC. Intramural (“small vessel”) coronary artery disease in hypertrophic cardiomyopathy. J Am Coil Cardiol 1986;s: 545-557. 24. Liu SK, ‘Maron BJ, Tilley LP. Feline hypertrophic cardiomyopathy: gross anatomic and quantitative histologic features. Am J Pathol 1981;102:388-395. 25. Tilley LP, Liu S K, Gilbertson SR, Wagner BM, Lord PF. primary myocar- dial disease in the cat. Am J Pathol 1977;87:493-522. 28. Liu S K, Muon BJ, Tilley LP. Hypertrophic cardiomyopathy in the dog. Am J Pachol 1979;94:497-508. 27. Liu S K, Hsu FS, Lee RCT. An Atlas of Cardiovascular Pathology. Taiwan: Pig Research Institute 1989198-227. 28. Roberts WC, Ferrans VJ. Pathologic anatomy of the caxiiomyopathies. Hum Path01 1975;6:287-342. 29. Maron BJ, Gottdiener JS, Epstein SE. Patterns and significance of the distri- bution of left ventricular hypertrophy in hypertrophic cardiomyopathy: a wide-angle, two-dimensional echocardiographic study of 125 patients. Am J Cnrdiol 1981;48: 418428. 30. Maron BJ. Asymmetry in hypertrophic cardiomyopathy: the septal to free wall thickness ratio revisited. Am J Cardiol 1985;55:835-838.
HC IN HUMANS, CATS AND DOGS 951




![GENETIC BASIS OF HYPERTROPHIC CARDIOMYOPATHYThroughout the years, names such as idiopathic hypertrophic subaortic stenosis[5], muscular subaortic stenosis[6] and hypertrophic obstructive](https://img.pdfslide.us/doc/110x75/60571329c95e4748070a14f6/genetic-basis-of-hypertrophic-cardiomyopathy-throughout-the-years-names-such-as.jpg)




![Sylvie MEAUME1 Management of scars: updated practical Anne ...€¦ · wound healing [1]. Hypertrophic scars usually remain within the border of the original wound and may spontaneously](https://img.pdfslide.us/doc/110x75/5f0bc07a7e708231d4320a82/sylvie-meaume1-management-of-scars-updated-practical-anne-wound-healing-1.jpg)