Embed Size (px)
Citation preview

JOURNAL OF CLINICAL MICROBIOLOGY, JUlY 1994, p. 1816-1819 Vol. 32, No. 70095-1137/94/$04.00+0Copyright © 1994, American Society for Microbiology
Comparison of Four Different Methods for EpidemiologicTyping of Acinetobacter baumannii
H. SEIFERT,* A. SCHULZE, R. BAGINSKI, AND G. PULVERERInstitut fair Medizinische Mikrobiologie und Hygiene der Universitiat Koln, 50935 Cologne, Germany
Received 16 December 1993/Returned for modification 24 January 1994/Accepted 5 April 1994
A set of 103 epidemiologically well-defined Acinetobacter baumannii isolates obtained from nine hospitaloutbreaks and 21 unrelated strains were characterized by pulsed-field gel electrophoresis (PFGE) of totalgenomic DNA digested with ApaI. Among outbreak strains, eight different patterns and five possible variantswere identified by PFGE. Results were compared with those from traditional typing methods such as plasmidprofile analysis, antimicrobial susceptibility, and biotyping. Plasmid analysis revealed six different and tworelated patterns; one outbreak strain lacked plasmids. A total of 16 of the 21 unrelated strains harboredplasmids and exhibited unique patterns. Epidemiologically unrelated strains were placed into only two biotypesand had similar antimicrobial susceptibility patterns but were clearly distinguished by PFGE. PFGE of A.baumannii chromosomal DNA yielded reproducible and easily readable results and showed excellentdiscriminatory power. However, plasmid profile analysis may provide a cost-effective first step in epidemio-logical typing of A. baumannii isolates obtained from well-defined hospital outbreaks.
Acinetobacter baumannii is a significant pathogen, usually inthe context of serious underlying disease (3, 8, 10). Outbreaksof infections have been reported in neonatal intensive careunits (ICUs) (19), medical and surgical wards (3, 13, 20), andburn units (24) and have been associated with medical equip-ment (3, 6, 24) and hands of personnel (17).
Epidemiological issues are often difficult to resolve becauseof the ubiquitous nature of Acinetobacter species in the envi-ronment (2) and as a commensal organism on human skin andmucous membranes (18, 25). Traditional techniques used fortyping of A. baumannii are often based on phenotypic charac-ters, including antibiogram analysis (14), biotyping (4, 5, 14),phage typing (5), serotyping (27), and cell envelope proteintyping (5, 7). None of these techniques is capable of typing allstrains. More recently, genotypic methods such as analysis ofplasmid profiles (13, 17), ribotyping (7, 9), analysis of chromo-somal DNA by pulsed-field gel electrophoresis (PFGE) (1, 11),and fingerprinting by arbitrarily primed PCR (12) have beenintroduced and have improved epidemiological typing of A.baumannii.
In this study, the results of PFGE of chromosomal DNAfrom a collection of epidemiologically unrelated A. baumanniistrains as well as from isolates obtained from several well-defined hospital outbreaks were compared with those obtainedwith established and commonly used methods for strain delin-eation including comparison of antibiograms, biotyping, andanalysis of plasmid patterns.A total of 103 A. baumannii isolates recovered from different
patients from nine hospital outbreaks and 21 epidemiologicallyunrelated strains were selected from more than 400 isolatesthat were collected prospectively from 275 patients during a12-month survey (21). Representative isolates from each out-break were chosen for their similarity as shown by biotypingand susceptibility testing. Isolates were identified according tothe simplified identification scheme described by Bouvet andGrimont (4). Susceptibility to selected antimicrobial agentswas determined by a microtiter broth dilution method (Mi-croScan MIC Plus Type MK Dried Panels; Baxter Healthcare
* Corresponding author.
Corp., West Sacramento, Calif.), as described previously (22).Biotyping was performed with utilization of six carbon sources(levulinate, citraconate, L-phenylalanine, phenylacetate, 4-hy-droxybenzoate, and L-tartrate) as described by Bouvet andGrimont (4).
Plasmid DNA was prepared as described by Hartstein et al.(13), with minor modifications (23). A plasmid type wasdefined as any plasmid pattern which varied from anotherpattern with regard to the number and size of plasmid bands.Two patterns were considered similar if one of the twocompared patterns contained one or two additional bands.Identity and similarity were further confirmed by restric-tion endonuclease enzyme digestion of the preparations withHindIII and EcoRI (data not shown). Isolates were run induplicate on different gels.For PFGE, A. baumannii isolates were grown overnight on
Mueller-Hinton agar plates at 30°C. Cells were harvested,suspended in 5 ml of 75 mM NaCl-25 mM EDTA (SE buffer;pH 7.4), pelleted by centrifugation, and washed twice in thesame buffer. Bacterial cells were adjusted to 109 CFU/ml in SEbuffer. A total of 0.5 ml of the bacterial suspension was mixedwith 0.7 ml of 2% low-gelling agarose (Amresco, Solon, Ohio)and poured into a plug mold. The agarose plugs were thenincubated with a mixture of 50 mM Tris-50 mM EDTA (pH8.0), 1% N-lauryl sarcosine, and 1 mg of proteinase K per ml(Merck, Darmstadt, Germany) for 18 h at 56°C in a water bathwith gentle shaking. Genomic DNA was digested with 20 U ofApaI (New England Biolabs) for 4 h. DNA fragments wereseparated by PFGE, with use of the Pulsaphor apparatus(Pharmacia-LKB, Bromma, Sweden). Plugs were placed intothe slots of a 1.2% agarose gel and run in 0.5 x TBE buffer (45mM Tris [pH 8.0], 45 mM boric acid, 1 mM EDTA) for 24 h at150 V. Pulse times ranged from 5 to 20 s. A ladder ofbacteriophage lambda concatemers (New England Biolabs)was used as molecular weight markers. Gels were stained withethidium bromide and photographed under UV light.
Epidemiological data on the different hospital outbreaks areshown in Table 1. All outbreaks occurred in ICUs. If multipleICUs were involved, these were all located on the same floor.The duration of the outbreaks ranged from 2 months to morethan 12 months, affecting from 9 patients on a single ward to
1816
on Decem
ber 29, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from

NOTES 1817
TABLE 1. Epidemiological data and summary of typing results of 103 A. baumannii strains from nine hospital outbreaks
Location of hospital Ward No. of Duration of Body site or Antibiogram Plasmid PFGEoutbreak type patients outbreak tract Biotypec typ type typeinvolvedb (MO)
University hospital (A) NICU 10 6 Respiratory 1 A NTd aUniversity hospital (A) RU 12 2 Urinary 6 B I bChildren's hospital (B) 2 ICUs 9 6 Blood cultures 6 A II cTeaching hospital (C) BICU 12 4 Various 6 C III dTeaching hospital (C) BICU 8 3 Various 2 B IV eTeaching hospital (C) 4 ICUs 12 5 Various 9 D V fTeaching hospital (C) 4 ICUs 56 10 Various 9 D Va gTeaching hospital (C) 4 ICUs 154 >12 Various 9 E VI, VIa hCommunity hospital (D) MICU 7 8 Various 9 E VI h
a NICU, neurological ICU; RU, rehabilitation unit; 2 ICUs, neonatal ICU and preterm neonate ICU; BICU, bum unit; 4 ICUs, surgical, neurological, andneurosurgical ICUs and burn unit; MICU, medical ICU.
b Total number of patients involved in any given outbreak.Biotrype as determined by Bouvet and Grimont (4).
dNT, not typeable.
more than 150 patients in multiple ICUs. The majority ofisolates were recovered from patients who were also tempo-rally clustered. In some instances, however, identical strainswere recovered after an interval of 2 or 3 months, thusextending the duration of the outbreak.
Antibiotic susceptibility testing of A. baumannii isolatesrevealed similar patterns for any given cluster of isolates(Table 1). The following antibiotic resistance phenotypes weredetected and arbitrarily designated A through E: A, suscepti-ble to gentamicin, tobramycin, amikacin, ciprofloxacin, andimipenem; B, susceptible to imipenem only; C, susceptible totobramycin and imipenem; D, susceptible to amikacin andimipenem; and E, susceptible to amoxicillin-clavulanate, pip-eracillin, and imipenem. Resistance patterns of epidemiologi-cally unrelated strains mostly resembled pattern A.Four different biotypes were observed among the outbreak
isolates investigated. One outbreak each was due to A. bau-mannii biotypes 1 and 2, whereas A. baumannii biotypes 6 and9 were involved in three and four outbreaks, respectively.Epidemiologically unrelated strains were placed into biotypes6 (8 strains) and 9 (13 strains).
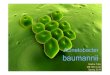
Six different plasmid types were observed among the 103 A.baumannii isolates recovered from hospital outbreaks, desig-nated arbitrarily I to VI. Representative plasmid profiles fromoutbreak strains are shown in Fig. 1. A total of 16 of the 21epidemiologically unrelated A. baumannii strains harboredplasmids, and plasmid patterns of these strains were clearlydistinct from those of the outbreak strains and from each other(data not shown). Two plasmid profiles were consideredsimilar (V/Va and VI/VIa; Fig. 1, lanes 1 to 8). Isolatesrepresenting biotype 1 were not typeable by plasmid profileanalysis. Isolates within each of the other outbreaks exhibitedidentical plasmid profiles with two exceptions. Plasmid analysisof a blood culture isolate demonstrated profile VI, whereas thecorresponding isolate recovered 2 days later from a centralvenous catheter had no detectable plasmid bands. Isolatesrepresenting plasmid profile VI were distributed among fourICUs of hospital C and were also responsible for the outbreakin a community hospital (hospital D), apparently due totransfer of a colonized patient from hospital C to hospital D.However, during the course of this outbreak two additionallow-molecular-weight plasmid bands were observed in some ofthese isolates (profile VIa). All these isolates, however, had anidentical banding pattern as shown by PFGE (data not shown).PFGE of genomic DNA after digestion with ApaI from
outbreak strains revealed eight different patterns or PFGE
types, named a through h, yielding 15 to 20 bands per strain(Fig. 2 and 3 and Table 1). There were marked restrictionlength polymorphisms among all these strains except betweenstrains representing patterns f and g, which differed by only twobands (Fig. 2, lanes 10 to 16). Those two strains had identicalsusceptibility patterns and similar plasmid profiles (V and Va)(Fig. 1, lanes 1 to 4) and were probably derived from acommon ancestral strain. Among isolates demonstrating pat-terns d and b, one and two variants, respectively, were ob-served that showed differences of one band (Fig. 3, lanes 2 to4 and 5 to 7). Among isolates representing PFGE type h, twovariants were detected that differed in one band (data not
1 9 - A E. R 7 R ln 11 12 13 14
:h r'3.1
9.4
6.5
4.3
2.32.0
FIG. 1. Plasmid DNA profiles ofA. baumannii isolates of differentbiotypes and obtained from different hospital outbreaks. Lanes: 1 to12, A. baumannii isolates as described in Table 1; 1 and 2, biotype 9isolates from hospital C (plasmid type V); 3 and 4, biotype 9 isolatesfrom hospital C (plasmid type Va); 5 and 6, biotype 9 isolates fromhospital C (plasmid type VI); 7 and 8, biotype 9 isolates from hospitalC (plasmid type VIa); 9 and 10, biotype 6 isolates from hospital A(plasmid type I); 11 and 12, biotype 6 isolates from hospital B (plasmidtype II); 13, A. baumannii ATCC 19606; 14, molecular size marker, inkilobases (Hindlll digest of lambda DNA). Chr, chromosomal DNA.
VOL. 32, 1994
on Decem
ber 29, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from

J. CLIN. MICROBIOL.
1 2 3 4 5 6 7 8 91011121314151617181920 1 2 3 4 5 6 7 8 9 101112 1314151617181920
29124 2
1194
14 5
97
482 3
FIG. 2. PFGE analysis of genomic DNA from A. baumannii iso-lates of different biotypes, obtained from different hospital outbreaks,after digestion with ApaI. Lanes: 1 and 20, lambda DNA concatemers(expressed in kilobases); 2 to 19, A. baumannii isolates as described inTable 1; 2 to 5, biotype 1 isolates from hospital A (PFGE type a); 6 to9, biotype 2 isolates from hospital C (PFGE type e); 10 to 12, biotype9 isolates from hospital C (PFGE type g); 13 to 16, biotype 9 isolatesfrom hospital C (PFGE type f); 17 to 19, biotype 9 isolates fromhospital C (PFGE type h).
shown). Isolates from the community hospital (D) and thoseresponsible for the prolonged outbreak in hospital C gavevirtually indistinguishable patterns (PFGE type h). Nonrelatedstrains gave unique PFGE patterns (Fig. 3, lanes 12 to 20) thatwere easily distinguishable from one another and from those ofoutbreak isolates. In contrast, isolates obtained from a givenoutbreak demonstrated identical or very similar banding pat-terns. Isolates demonstrating identical PFGE patterns were allplaced in the same biotype. Conversely, there was considerablerestriction length polymorphism among A. baumannii strainsthat belong to the same biotype.
For comparison and reproducibility testing, one strain wasretested on each gel. In addition, five A. baumannii strainsrepresenting different biotypes and different PFGE types weremaintained at room temperature for up to 8 months andsubcultured every 2 weeks. Longitudinal reproducibility ofplasmid profiles and PFGE patterns was studied by runningthese isolates side by side on the same gel with correspondingisolates that were kept frozen. Plasmid profiles and PFGEpatterns were identical; no loss of bands was observed.The purpose of this study was to evaluate PFGE analysis of
A. baumannii genomic DNA from a collection of epidemiolog-ically unrelated strains and from isolates obtained from mul-tiple hospital outbreaks. The results obtained were comparedwith those of biotyping, antimicrobial resistance patterns, andplasmid profile analysis to further assess the usefulness of thesetraditional methods in relation to modern molecular tech-niques for epidemiological typing of A. baumannii.The biotyping system proposed by Bouvet and Grimont (4)
allows the differentiation of 19 different biotypes. However, thediscriminatory power of biotyping is poor, especially becauseonly a few biotypes have been involved in hospital outbreaks-namely, biotypes 1, 2, 6, and 9 (7, 14). These biotypes were alsoobserved among the isolates investigated in the present study.With the exception of the large outbreak in hospital C with
FIG. 3. PFGE analysis of genomic DNA from A. baumannii bio-type 6 isolates after digestion with Apa I. Lanes: 1 and 11, lambda DNAconcatemers (as in Fig. 2); 2 to 10, A. baumannii isolates from threeoutbreaks as described in Table 1; 2 to 4, isolates from hospital C(PFGE type d); 5 to 7, isolates from hospital A (PFGE type b); 8 to 10,isolates from hospital B (PFGE type c); 12, A. baumannii referencestrain ATCC 19606; 13 to 20, unrelated A. baumannii biotype 6 strains.
multiple biotypes involved, isolates obtained from each of thehospital outbreaks were placed into a single biotype whichproved to be a stable marker during the course of the outbreak.
Antibiotic susceptibility patterns were less helpful in theepidemiological study of A. baumannii in our study. Minorvariations were frequently observed among outbreak isolatesand were difficult to interpret without the help of a comple-mentary typing system. In addition, strains exhibiting differentPFGE patterns were placed into the same susceptibility type(Table 1). Thus, both biotyping and antimicrobial susceptibilitypatterns may be suitable as screening methods in epidemiolog-ical investigations but require confirmation of results by com-plementary techniques.
Plasmid profile analysis has proved useful for the study ofoutbreaks ofA. baumannii infections (3, 13, 17). The techniqueis simple, requires a minimum of equipment and expense, andis accessible for most diagnostic laboratories. Plasmid profileanalysis in our hands demonstrated acceptable typeability.With one exception, all outbreak strains could be differentiatedby this method; among unrelated strains, 16 of 21 weretypeable. Plasmid profiles were highly reproducible for allisolates that had been stored at room temperature for pro-longed periods of time and subcultured at regular intervals.Plasmid profiles were also stable among most strains withineach outbreak. However, during the extended outbreak due toA. baumannii biotype 9 observed in hospital C, the outbreakstrain apparently acquired two additional plasmids of lowmolecular weight. Isolates representing both plasmid types-designated VI and VIa-were recovered concomitantly frompatients in the same ward and in two cases even from the samepatient. The genotypic results obtained by PFGE for all theseisolates were identical.
Analysis of genomic DNA by PFGE has proved to be highlydiscriminatory and comparable or often superior to otheravailable techniques (16, 26). This method was used by Allar-
1818 NOTES
on Decem
ber 29, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from

NOTES 1819
det-Servent et al. (1) to investigate an outbreak of A. bauman-nii in a urological ward. In a subsequent study, Gouby et al.(11) demonstrated considerable DNA polymorphism amongA. baumannii strains isolated in different parts of the world,even among strains that belong to the same biotype. In ourstudy, genetic fingerprinting of 21 unrelated A. baumanniistrains demonstrated a considerable number of restrictionfragment length polymorphisms. Each strain exhibited aunique banding pattern. The presence of such diversity is thebasis for the assumption that isolates with identical or almostidentical patterns represent a single clone. Restriction frag-ment patterns of chromosomal DNA were virtually identicalfor most temporally or epidemiologically related isolates.Comparison of profiles f and g, however, revealed minordifferences suggesting that both strains may have derived froma common ancestral strain. In addition, five possible variantswere observed among the isolates investigated. However, it hasbeen suggested that detection of a single band difference is nota reliable basis for concluding that two isolates that areepidemiologically related represent different strains (16). Thestability of the typing system was further demonstrated by theidentification of identical patterns in serially passaged strains.Numerous studies have evaluated multiple typing methods forthe epidemiological investigation of A. baumannii isolates (5,7, 14, 15). Unfortunately, controls showing dissimilarity ofunrelated isolates and similarity of serially passaged isolateshave not always been included.
Overall, there was a remarkable degree of uniformity intyping results obtained by plasmid profile analysis and PFGE.Both methods allowed differentiation among sets of outbreak-associated isolates and separation of unrelated strains. Plasmidprofiling is well suited for the analysis of outbreaks of A.baumannii infections that are restricted in terms of time andplace (those involving acute outbreaks within a single hospital).PFGE may be reserved for situations in which clinical andplasmid data conflict or are inconclusive. The usefulness ofPFGE as an epidemiological tool in comparison with othermodern molecular typing methods such as ribotyping (9) andfingerprinting by arbitrarily primed PCR (12) remains to bedetermined.
REFERENCES1. Allardet-Servent, A., N. Bouziges, M. J. Carles-Nurit, G. Bourg, A.
Gouby, and M. Ramuz. 1989. Use of low-frequency-cleavagerestriction endonucleases for DNA analysis in epidemiologicalinvestigations of nosocomial bacterial infections. J. Clin. Micro-biol. 27:2057-2061.
2. Baumann, P. 1968. Isolation of Acinetobacter from soil and water.J. Bacteriol. 96:39-42.
3. Beck-Sague, C. M., W. R. Jarvis, J. H. Brook, D. H. Culver, A.Potts, E. Gay, B. W. Shotts, B. Hill, R. L. Anderson, and M. P.Weinstein. 1990. Epidemic bacteremia due to Acinetobacter bau-mannii in five intensive care units. Am. J. Epidemiol. 132:723-733.
4. Bouvet, P. J., and P. A. Grimont. 1987. Identification and biotypingof clinical isolates of Acinetobacter. Ann. Inst. Pasteur Microbiol.138:569-578.
5. Bouvet, P. J., S. Jeanjean, J. F. Vieu, and L. Dijkshoorn. 1990.Species, biotype, and bacteriophage type determinations com-pared with cell envelope protein profiles for typing Acinetobacterstrains. J. Clin. Microbiol. 28:170-176.
6. Cefai, C., J. Richards, F. K. Gould, and P. McPeake. 1990. Anoutbreak of Acinetobacter respiratory tract infection resultingfrom incomplete disinfection of ventilatory equipment. J. Hosp.Infect. 15:177-182.
7. Dijkshoorn, L., H. M. Aucken, P. Gerner-Smidt, M. E. Kaufmann,
J. Ursing, and T. L. Pitt. 1993. Correlation of typing methods forAcinetobacter isolates from hospital outbreaks. J. Clin. Microbiol.31:702-705.
8. Fagon, J. Y., J. Chastre, A. J. Hance, P. Montravers, A. Novara,and C. Gibert. 1993. Nosocomial pneumonia in ventilated pa-tients: a cohort study evaluating attributable mortality and hospitalstay. Am. J. Med. 94:281-288.
9. Gerner-Smidt, P. 1992. Ribotyping of the Acinetobacter calcoace-ticus-Acinetobacter baumannii complex. J. Clin. Microbiol. 30:2680-2685.
10. Glew, R. H., R. C. Moellering, and L. J. Kunz. 1977. Infectionswith Acinetobacter calcoaceticus (Herellea vaginicola): clinicaland laboratory studies. Medicine 56:79-97.
11. Gouby, A., M. J. Carles-Nurit, N. Bouziges, G. Bourg, R. Mesnard,and P. J. Bouvet. 1992. Use of pulsed-field gel electrophoresis forinvestigation of hospital outbreaks of Acinetobacter baumannii. J.Clin. Microbiol. 30:1588-1591.
12. Graser, Y., I. Klare, E. Halle, R. Gantenberg, P. Buchholz, H. D.Jacobi, W. Presber, and G. Schonian. 1993. Epidemiological studyof an Acinetobacter baumannii outbreak by using polymerase chainreaction fingerprinting. J. Clin. Microbiol. 31:2417-2420.
13. Hartstein, A. I., V. H. Morthland, J. W. Rourke, J. Freeman, S.Garber, R. Sykes, and A. L. Rashad. 1990. Plasmid DNA finger-printing of Acinetobacter calcoaceticus subspecies anitratus fromintubated and mechanically ventilated patients. Infect. ControlHosp. Epidemiol. 11:531-538.
14. Joly-Guillou, M. L., E. Bergogne-Berezin, and J. F. Vieu. 1990. Astudy of the relationships between antibiotic resistance pheno-types, phage-typing and biotyping of 117 clinical isolates ofAcinetobacter spp. J. Hosp. Infect. 16:49-58.
15. Kropec, A., J. Hubner, and F. D. Daschner. 1993. Comparison ofthree typing methods in hospital outbreaks of Acinetobactercalcoaceticus infection. J. Hosp. Infect. 23:133-141.
16. Maslow, J. N., M. E. Mulligan, and R. D. Arbeit. 1993. Molecularepidemiology: application of contemporary techniques to thetyping of microorganisms. Clin. Infect. Dis. 17:153-164.
17. Patterson, J. E., J. Vecchio, E. L. Pantelick, P. Farrel, D. Mazon,M. J. Zervos, and W. J. Hierholzer. 1991. Association of contam-inated gloves with transmission of Acinetobacter calcoaceticus var.anitratus in an intensive care unit. Am. J. Med. 91:479-483.
18. Rosenthal, S., and I. B. Tager. 1975. Prevalence of gram-negativerods in the normal pharyngeal flora. Ann. Intern. Med. 83:355-357.
19. Sakata, H., K. Fujita, S. Maruyama, H. Kakehashi, Y. Mori, andH. Yoshioka. 1989. Acinetobacter calcoaceticus biovar anitratussepticaemia in a neonatal intensive care unit: epidemiology andcontrol. J. Hosp. Infect. 14:15-22.
20. Seifert, H., and R. Baginski. 1992. The clinical significance ofAcinetobacter baumannii in blood cultures. Zentralbl. Bakteriol.277:210-218.
21. Seifert, H., R. Baginski, A. Schulze, and G. Pulverer. 1993. Thedistribution of Acinetobacter species in clinical culture materials.Zentralbl. Bakteriol. 279:544-552.
22. Seifert, H., R. Baginski, A. Schulze, and G. Pulverer. 1993.Antimicrobial susceptibility of Acinetobacter species. Antimicrob.Agents Chemother. 37:750-753.
23. Seifert, H., A. Schulze, R. Baginski, and G. Pulverer. 1994. PlasmidDNA fingerprinting of Acinetobacter species other than Acineto-bacter baumannii. J. Clin. Microbiol. 32:82-86.
24. Sheretz, R. J., and M. L. Sullivan. 1985. An outbreak of infectionswith Acinetobacter calcoaceticus in burn patients: contaminationof patients' mattresses. J. Infect. Dis. 151:252-258.
25. Taplin, D., G. Rebell, and N. Zaiab. 1963. The human skin as asource of Mima-Herella infections. JAMA 186:166-168.
26. Tompkins, L. S. 1992. The use of molecular methods in infectiousdiseases. N. Engl. J. Med. 327:1290-1297.
27. Traub, W. H. 1989. Acinetobacter baumannii serotyping for delin-eation of outbreaks of nosocomial cross-infection. J. Clin. Micro-biol. 27:2713-2716.
VOL. 32, 1994
on Decem
ber 29, 2019 by guesthttp://jcm
.asm.org/
Dow
nloaded from