Embed Size (px)
Citation preview

n e u r o l o g y , p s y c h i a t r y and b r a i n r e s e a r c h 1 9 ( 2 0 1 3 ) 4 2 – 4 7
Available online at www.sciencedirect.com
journa l homepage: www.e lsev ier .com/ locate /npbr
Comparison of 3.0-T MRI findings in drug resistant andnon-resistant adult epileptic patients§
Faysal Ekici a,*, Guven Tekbas a, Hakan Onder a, Hatice Gumus a, Mehmet G. Cetincakmak a,Suzan K. Balik a, Abdullah Acar b, Cihat Hamidi a, Aslan Bilici a
aDicle University, School of Medicine, Department of Radiology, 21280 Diyarbakir, TurkeybDicle University, School of Medicine, Department of Neurology, 21280 Diyarbakir, Turkey
a r t i c l e i n f o
Article history:
Received 16 July 2012
Accepted 24 September 2012
Available online 23 October 2012
Keywords:
Adult
Epilepsy
3.0-T MRI
a b s t r a c t
Epilepsy is a common chronic disease characterized by spontaneous and recurrent seizures.
Along with the increases in life expectancy, the prevalence of epilepsy in adults increased in
parallel. 3.0-T MRI provides high signal/noise ratio and is an important tool in the determi-
nation of epileptic lesion in epilepsy patients. Our aim in this study was to research and
compare 3.0-TMRI findings of Turkish epileptic patients that are resistant and non-resistant
to medical treatment. 3.0-T MRI images from 264 consecutive patients, of which 150 were
males and 114 were females (age range 18–82 years; mean age 31.3 years) were examined,
retrospectively. Among those patients, 94 were resistant to medical treatment (DRE+) and
170 were non-resistant (DRE�). Epileptic lesion was determined in 119 of the patients.
Epileptic lesion was determined in sixty-three patients who were resistant to medical
treatment and in fifty-six patients who were non-resistant. Epileptic lesion was determined
in approximately half of the adult epilepsy patients by using 3.0-T MRI. This study demon-
strates a high prevalence of brain abnormalities in Turkish epileptic patients with DRE+. The
lesion was determined in 67% of patients with medical treatment resistance, while the
percentage for the other groupwas only 32.9%. The ratio of epileptic lesion determination by
using 3.0-T MRI was quite higher in the medical treatment resistant group than the non-
resistant group.
© 2012 Elsevier GmbH. All rights reserved.
1
Introduction
Seizures are paroxysmal changes in neurological functionsformed by abnormal and excessive neuronal electrical activi-ties. Epilepsy is a chronic disease characterized by spontane-ous and recurrent seizures. It has been reported that 5–10% ofpeople have experienced seizures at least once in their livesbut most of them do not develop epilepsy.1 Epilepsy is acommon disease affecting approximately 0.5–1% of the
§ This study was performed in Dicle University.* Corresponding author at: Dicle Üniversitesi Tıp Fak. Radyoloji A.D. 2
fax: +90 412 2488115.E-mail address: [email protected] (F. Ekici).
0941-9500/$ – see front matter © 2012 Elsevier GmbH. All rights reserhttp://dx.doi.org/10.1016/j.npbr.2012.09.002
population in industrialized countries. This percentage isreported to be higher in underdeveloped countries due toadverse environmental conditions and inadequate healthservices.2 In developed countries, parallel to progress in healthservices in the last three decades, the percentage of childrenaffectedwith epilepsyhas decreased,while this ratio for adultshas increased.2 Among epileptic patients, 20–40% are resistantto medical treatment (DRE+).3,4 Uncontrolled epilepsy nega-tively affects patients' social, business and educational livesand in addition, increases the cost of social security institu-
1280 Diyarbakir, Turkey. Tel.: +90 4122488158x4314;
ved.

n e u r o l o g y , p s y c h i a t r y and b r a i n r e s e a r c h 1 9 ( 2 0 1 3 ) 4 2 – 4 7 43
tions. Moreover, increases in the frequency and severity ofseizures bring along an increase in mortality.2
The most important step in planning the treatment forepileptic patients is detection of epileptic lesion. Neuroradio-logical studies play a key role in this regard. Electroencepha-lography (EEG) and magnetic resonance imaging (MRI) can beused to detect the causes of spontaneous seizures and seizureswithout any provocative factors during the time of develop-ment.5,6 Abnormalities were detected in 70% of the EEGs takenduring the first 24–48 h after the seizures occurred.7 Due tohigh soft tissue contrast, MRI is an indispensable instrumentfor the evaluation of epileptic patients. Moreover, detection oflesions with MRI is dependent on the experience of specialiststhat evaluate MRI values and the quality of images from theMRI devices.8 The development of strong magnets enabledhigh spatial resolution images.9 Epilepsy is one of the fieldswhere the use of 3.0-Tmagnets in structural imaging has beenresearched in more detail. The greater contrast in T2 and theincreased SNR means that small structures can be seen moreclearly.9,10 In cases with resistant epilepsy, 3.0-T MR wassuperior to 1.5-T in detecting the number of identified andcharacterized lesions.11
The goal of this study was to assess the prevalence anddifferences of brain MRI abnormalities in a Turkish cohort ofDRE+ and non-resistant DRE� adult epileptic patients.
Materials and methods
The study was approved by the ethical committee. 3.0-T MRIimages were retrospectively examined from a total of 283consecutive patients that were diagnosed with epilepsybetween December 2009 and October 2011. Four patients thatunderwent intracranial operation and fifteen patients thatwere not controlled after treatment were excluded from thestudy, resulting in a total of 264 patients that constituted thepatient group.
The diagnosis of epilepsy in this study was established onthebasis ofboth theclinical andEEG findingsbyoneneurologist(A.A, with 11 years of experience); and this diagnosis served asthe reference standard. Neurologist (A.A) informed epilepsypatients about the disease in details. Patients were informedabout administrationof themedication. Serumdrug levelsweremeasured at specific time intervals. Epileptic patients thatreceived a single antiepileptic drug to control seizures were
Table 1 – MR imaging sequence parameters.
Parameter AxialT2-weighted
CoronalT2-weighted
Sequence Sequence
Repetition time/echo time 2500/80 3000/80Inversion time (ms) – –
Field of view (mm) 230 220Matrix 400/255 336/210Section thickness (mm) 5 3Flip angle (degrees) – –
No. of signals acquired 1 1Imaging time 2 min 15 s 4 min 21 s
considered as DRE� patients. Cases were described as havingDRE+ when they had two or more seizures per month for aperiodofmore than2yearswith twoormoreantiepilepticdrugsattending the intractable epilepsy outpatient clinic.12
Examinations were performed with a 3.0-T whole-body MRimager (Achieva; Philips Medical Systems, Best, theNetherlands) by using an 8-channel head coil. All patientsunderwent brain MRI sequences appropriate to the epilepsyprotocol routinely used in our hospital. Our standard brain MRimaging protocol for epilepsy also included anaxial and coronalT2-weighted fast spin-echo sequence, and fluid-attenuatedinversion-recovery (FLAIR) sequence, and an unenhanced T1-weighted volume data set (3D Turbo Field Echo sequence). Thedetailed sequence parameters are shown in Table 1. Whenneeded, patients were administered 0.1 mmol/kg body weightparamagnetic contrast agent (gadodiamide [Omniscan; Amer-sham Health, Cork, Ireland], gadopentetate dimeglumine[Magnevist; Schering AG, Berlin, Germany] and gadobutrol[Gadovist; Schering AG, Berlin, Germany]) at 2 ml/s via theantecubital vein and spin-echo T1 images were obtained inaxial, coronal and sagittal planes. All of the images wereevaluated jointly by two radiologists (FE and GT) with 14 and 9years of experience, respectively. Evaluation was performedusing a work station (Philips Extended Brilliance Workspace,Philips Medical Systems, Best, the Netherlands).
Major pathologies that can cause epilepsy were examinedin six groups: brain damage (BD), hippocampal sclerosis (HS),vascular abnormalities, cortical development abnormalities(CDA), tumors, and cysts. Definitive diagnoses for patientswho had an undefined mass were made by histopathologicalexamination. In BD cases, trauma and cerebrovasculardiseases were investigated as causes of the damage. Segrega-tion between them was done based on the patient's history.Areas where the brain damage occurred were recorded.
Student's t test was used to compare age between thepatient groups, while chi-square test was used to compare thenumbers of cases in DRE+ and DRE� groups with detectedepileptic lesion. A P value of<0.05was accepted as statisticallysignificant.
Results
The group of patients (age range: 18–82 years; mean age, 31.3years) included 150men and 114 female patients. Themedical
AxialFLAIR
CoronalFLAIR
SagittalT1-weighted 3D fastfield echo sequence
Sequence Sequence
10,000/125 11,000/120 8.1/3.72800 2800 1006230 220 240352/198 336/210 240/2405 3 1– – 81 2 14 min 00 s 4 min 21 s 7 min 29 s

Table 2 – The distribution of the developing regions of thebrain damage.
The affected area n (%)
Frontal 25 (32.9)Temporal 22 (28.9)Parietal 12 (15.9)Occipital 10 (13.1)Basal ganglia 6 (7.9)Cerebellum 1 (1.3)Total 76 (100)
[(Fig._2)TD$FIG]
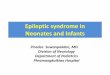
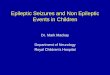
Fig. 2 – Coronal T2W image shows, atrophy and high sinyalintensity in the left hippocampus (arrow) and atrophy ofthe left fornix (double arrows).
n e u r o l o g y , p s y c h i a t r y and b r a i n r e s e a r c h 1 9 ( 2 0 1 3 ) 4 2 – 4 744
treatment non-resistant group (mean age 31.7 years) consistedof a total of 170 (64.4%) patients amongwhich 97weremen and73were women. Themedical treatment resistant group (meanage, 30.6 years) consisted of 94 (35.6%) patients, fifty-threemenand forty-one women. The age difference between DRE+ andDRE� groups was not significant ( p > 0.05).
A total of 264 patients with diagnosed epilepsy weresubjected to brain MRI examination to detect the epilepticlesion. The epileptic lesion was not detected in 145 (54.9%)patients. In the remaining 119 (45.1%) patients, at least onepathology that may have caused epilepsy was determined. In67% of DRE+ patient group epileptic lesion was detected withMRI, while this ratio for the DRE� patient group was found tobe 32.9%. A significant difference was determined betweenthese two groups (p < 0.001).
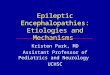
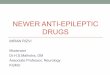
The most frequent pathology among etiological factors ofepilepsy was brain damage, with forty-nine (18.6%) of patientseffected (Fig. 1). In thirty cases the cause of brain damage wastrauma, while in nineteen cases it was cerebrovasculardiseases. When examining the damaged area of the patients'brain, we observed that six patients had damage in threeregions, fifteen patients had damage in 2 regions, and twenty-eight patients had damage in a single region, making a total ofseventy-six damaged regions. The frontal lobe is the regionwhere most of the damage was observed, followed by thetemporal lobe. The number and regions affected by theparenchymal damage are shown in Table 2. When lookingat the distribution of BD in patient groups, parenchymaldamage was the most frequent pathology in the DRE� patientgroup, while in DRE+ group it was the third most frequentpathology.
When patients from all groups were evaluated, hippocam-pal sclerosiswas the secondmost frequent pathology detectedin forty-two (15.9%) of the patients. However itwas determined
[(Fig._1)TD$FIG]
Fig. 1 – T2-weighted axial imaging shows, right fronto-parietal parenchymal damage.
that hippocampal sclerosis was the most prevalent pathologyin DRE+ group with thirty-three (35.1%) patients (Fig. 2). NineHS cases were detected in the DRE� patient group.
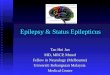
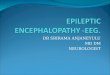
A cortical developmental abnormality was detected in tencases (3.8%) from the patient population; these includedpolymicrogyria (7), schizencephaly (2) and cortical dysplasia (1)(Fig. 3). Six of the polymicrogyria were located in perisylvianand onewas located in the bilateral parieto-occipital lobe. Bothschizencephaly cases were of the closed-type. A single corticaldysplasia case was located in the left parietal lobe. All tenpatients with cortical developmental abnormalities wereDRE+.
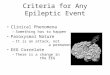
Ten (3.8%) of our patients had the following vascularpathologies: cavernous angioma (6) (Fig. 4), sinus veinthrombosis (2) and arteriovenous malformation (2). Thesepatients were equally distributed between DRE� and DRE+groups.
Among the patients with pathologies detected by MRI, four(1.5%) had tumors. Three of these cases were grade IIastrocytomas, and one was a ganglioglioma. Three of themasses were located in the temporal lobe and one in thefrontal lobe. All tumor cases were from DRE+ epilepsy group.
Arachnoid cysts were detected in four (1.5%) of our cases.All of the arachnoid cysts were located in the temporal sylvianfissure and were DRE�.
The pathologies that were detected by magnetic reso-nance imaging and their distribution into groups are shownin Table 3.

[(Fig._3)TD$FIG]
Fig. 3 – A 20-year-old man with focal cortical dysplasia. (A) FLAIR-weighted axial images shows abnormal high signal in leftparietal lobe. (B) MR spectroscopy shows a normal metabolite peaks.
n e u r o l o g y , p s y c h i a t r y and b r a i n r e s e a r c h 1 9 ( 2 0 1 3 ) 4 2 – 4 7 45
Discussion
Epilepsy is one of the most common chronic diseasesworldwide. Every year 30,000 novel cases of epilepsy arereported in the United Kingdom.13 Berg et al.14 estimated thatevery year in the USA 127/1,000,000 children will be diagnosedDRE+ and 27 of these children will undergo surgical operationdue to epilepsy. There is a medical treatment for epilepsy and2/3 of cases have successful results. A portion of the remainingpatients showa resistance tomedical treatment,while the restare forced to abandon the treatment due to toxic side effects of
[(Fig._4)TD$FIG]Fig. 4 – T2-weighted axial imaging shows low signalcorresponding to hemosiderin in right parietal lobecavernoma.
the drugs.3 Surgical procedures that were performed afterepileptogenic lesion were correctly detected by means of MRIand helped to completely stop seizures in approximately twothirds of patients and a portion of the rest showed a decreasedincidence of seizures.3,15 Urbach et al.15 in their study of 385DRE+ children and adult patients detected lesions in 83% of thepatients by means of MRI. High occurrence rates were due tothe fact that a significant proportion of patients in the studywere thosewith previously identified lesions detected via MRI.In our study with adult patients, the lesion detectionpercentage was 45.1%; in the DRE+ group this ratio was 67%and in the DRE� group it was 32.2%. The lower percentage of
Table 3 – MRI findings of patients epilepsy.
MRI findings Epileptic patientgroups
Total (n)
DRE+patients
DRE�patients
Normal 31 114 145Brain damage 9 40 49Trauma 6 26CVD 3 14 42
Hippocampal sclerosis 33 9 10Malformation of CD 10 0Polymicrogyria 7 0 10Schizencephaly 2 0Cortical dysplasias 1 0 4
Vascular causes 7 3 4Cavernoma 5 1AVM 1 1SVT 1 1
Tumor 4 0Cyst 0 4Total (n) 94 170 264
CVD: cerebrovascular disease; CD: cortical development; AVM:arterio venous malformation; SVT: sinus vein thrombosis.

n e u r o l o g y , p s y c h i a t r y and b r a i n r e s e a r c h 1 9 ( 2 0 1 3 ) 4 2 – 4 746
pathology detection may have been due to the fact that ourstudy consisted of only adults and patients who had thediagnostic procedures for the first time.
Brain damage develops following pathologies that result intissue damage such as cerebrovascular diseases, trauma,perinatal injury and infection, and is one of the causes of theepilepsy. It is alsooneof themost commoncausesof epilepsy inthe population of the patients above the age of 20.16,17 Amongthe most important causes of BD in adult patients are traumaand cerebrovascular damage. Post-traumatic epilepsy (PTE) isoneof theknownformsof traumaticbrain injuries.18Early,post-traumatic seizure stabilized penetrated injury, multiple con-tusions and subdural hematomas requiring surgical treatmentconstitute a risk for the PTE,17 and this risk is highest in thepresence of early post-traumatic seizures.18
The other pathology that results in parenchymal damageand is one of the most important causes of epilepsy in olderpatients is cerebrovascular disease.19 Epilepsy may develop asan early and late complication of cerebrovascular disease.20
The risk of developing epilepsy after cerebrovascular diseasewas reported to be between 7.7 and 11.5%.19,20 The proportionof detection of BD in epileptic patients varies between 2.2 and8.3%.21–23 In our study the most frequently detected pathologywas parenchymal damage (18.5%). In thirty-two cases with BD(12.1%) the cause of damage was determined to be trauma andin seventeen cases (6.4%) it was cerebrovascular disease. Themost important cause of the high occurrence of BD in our studymay have been because the patient group consisted of onlyadult patients. It was reported that in cases where patientsdeveloped PTE, seizures are difficult to control with medicaltreatment.24 In our study, only 18.7% of PTE cases were fromthe DRE+ group. Moreover, the vast majority of patients in ourstudy had a positive response to medical treatment. In caseswhere brain damage was detected as a cause of epilepsy, thefrontal and parietal lobes were the most frequently affectedregions.25 In our study, the most frequently affected regionwas found to be the frontal lobe, followed by the temporal lobe.The reason why there was more damage in the frontal andtemporal lobes can possibly be attributed to the fact thattrauma cases were more frequent in our patient populationand because the frontal region is more susceptible to trauma.
Hippocampal sclerosis is characterized by neuronal loss inthe hippocampus and gliosis. Hippocampal atrophy and/orhyperintense signal changes in T2 and FLAIR sequencesconstitute major MRI findings for HS.26 Thalamus, fornixand temporal lobe atrophy are other findings that are observedin 40–80% of all cases and when observed facilitate thediagnosis HS.13 Hanamiya et al.10 in their study of hippocam-pal sclerosis cases, evaluated mostly T2 images with highspatial resolution provided by 3.0-T MRI and determined thatthe most frequent abnormality was the partial loss ofhippocampal striation. When MRI is used, HS diagnosis iscorrectly made in 97% of cases. HS is the most prevalentpathology in DRE+ adults.15,24 HS detection by MRI variesbetween 10.5 and 61.8% in adult epileptic patients,15,21,22 andthis percentage climbs up to 72% in surgical series.15 In ourstudy of 264 patients, HS percentagewas 15.9% and this ratio isin agreement with the literature. In addition, HS being themost frequently observed pathology in the DRE+ group alsoparallels findings in the literature.
Any defect during the three developmental stages of thecortex may result in cortical developmental abnormalities.13
Althoughmost of these defects can easily be identified byMRI,the differentiation between cortical dysplasia and low gradeglial tumor is not always possible.27 In these cases thecombination of fluorodeoxyglucose-PET/MRI prior to surgicaltreatment can increase the ratio of correct diagnosis.27 Thepolymicrogyria is characterized by very small gyri in excessiveamounts that are caused by abnormal laminization of thecortex.28 They are mostly detected in the perisylvian region.27
In our study the polymicrogyriawere also detected at the samelocation. In a study that consisted of only adult epilepticpatients, the detection of cortical developmental abnormali-ties was 3%, while in the study with both children and adultsthis percentage varied between 2.5 and 12%.21,23 In our studywith 264 patients we detected ten (3.8%) cases of corticaldevelopmental abnormalities. This ratio overlaps with theliterature. All ten of these patients were from the DRE+ groupas expected.
According to many studies, vascular anomalies causeepilepsy in just a small group (5%).21,22 This rate has reached7% in patients undergoing surgery.15 In these studies,patients groups were constituted of cavernoma15,21 andarteriovenous malformation.22 Vascular abnormalities con-stituted 3.5% of pathologies detected in our patient groupsand this value is similar to that in the literature. In six of thecases cavernoma was detected, while two had arteriovenousmalformations. In contrast to the literature,15,21,22 weobserved sinus vein thrombus in two of our cases. Themajority (83%) of our cases with cavernomas were from theDRE+ group, while patients with arteriovenous malforma-tion and sinus vein thromboses were equally distributedbetween DRE� and DRE+ groups.
Brain tumors, especially ones of lower grades, are amongthe important causes of epilepsy.13 The importance of thesepathologies is that although they respond to surgical treat-ment they also have fatal effects. Because of this, earlydiagnosis of tumors enables removal of the epileptic lesionand also positively affects patients' mortality and morbidity.One of the first symptoms of a brain tumor is seizure, which isalso one of the primary causes of the epilepsy.15 Brain tumorsdetected in resistant epilepsy cases are mostly low grade andare frequently located in the temporal lobe.29 In epilepticpatients that underwent surgery, brain tumors were thesecond most prevalent pathology, second only to HS.15
Detection of tumors in epileptic patients during the surgicalseries varies between 22 and 23%,15,29 while this percentage isapproximately 6% for imaging.22 In our study this percentagewas lower than in the literature, constituting 1.5% of thepatients. All patients with detected tumors were resistant tomedical treatment, which also complies with the literature.
Arachnoid cysts are fluid-filled structures that have amembrane composed of real arachnoid cells and do not haveany connection with the ventricular system. They make upapproximately 1% of all intracranial masses. Their clinicalsymptoms change according to their location and can result inseizure.30 Arachnoid cysts were detected in four (1.5%) of ourcases and all of them were located in the temporal sylvianfissure. In all of these cases seizures were managed by usingsingle antiepileptic medicine.

n e u r o l o g y , p s y c h i a t r y and b r a i n r e s e a r c h 1 9 ( 2 0 1 3 ) 4 2 – 4 7 47
Conclusion
In conclusion, in our study with 3.0-T MRI, we examined adultepileptic patients and determined the epileptic focus in nearlyhalf of them. The most frequent pathology among all patientswas found to be brain damage, followed by hippocampalsclerosis. The epileptic focus was determined in approximate-ly two-thirds of DRE+ patients, while this ratio was limited toone-third of DRE� cases. The most frequent pathology in theDRE+ group was HS, while in the DRE� group it was BD. 3.0-TMRI enables correct detection of the epileptic focus in themajority of DRE+ adult patients.
r e f e r e n c e s
1. Fisher RS, Stein A, Karis J. Epilepsy for the neuroradiologist.American Journal of Neuroradiology 1997;18:851–63.
2. Duncan JS, Sander JW, Sisodiya SM, Walker MC. Adultepilepsy. Lancet 2006;367:1087–100.
3. Callaghan B, Schlesinger M, RodemerW, Pollard J, HesdorfferD, Allen Hauser W, et al. Remission and relapse in adrug-resistant epilepsy population followed prospectively.Epilepsia 2011;52:619–26.
4. Urbach H. Imaging of the epilepsies. European Radiology2005;15:494–500.
5. Hirtz D, Ashwal S, Berg A, Bettis D, Camfield C, Camfield P,et al. Practice parameter: evaluating a first nonfebrile seizurein children: report of the quality standards subcommittee ofthe American Academy of Neurology, the Child NeurologySociety and the American Epilepsy Society. Neurology2000;55:616–23.
6. American College of Emergency Physicians, AmericanAcademy of Neurology, American Association ofNeurological Surgeons, American Society of Neuroradiology.Practice parameter: neuroimaging in the emergency patientpresenting with seizure (summary statement). Annals ofEmergency Medicine 1996;28:114–8.
7. Pohlmann-Eden B, Beghi E, Camfield C, Camfield P. The firstseizure and its management in adults and children. BMJ2006;332:339–42.
8. von Oertzen J, Urbach H, Jungblut S, Kurthen M, Reuber M,Fernandez G, et al. Standard MRI is inadequate for patientswith refractory focal epilepsy. Journal of NeurologyNeurosurgery and Psychiatry 2002;73:643–7.
9. Alvarez-Linera J. 3T MRI: Advances in brain imaging.European Journal of Radiology 2008;67:415–26.
10. Hanamiya M, Korogi Y, Kakeda S, Ohnari N, Kamada K,Moriya J, et al. Partial loss of hippocampal striation in medialtemporal lobe epilepsy: pilot evaluation with high-spatial-resolution T2-weighted MR imaging at 3.0 T. Radiology2009;251:873–81.
11. Phal PM, Usmanov A, Nesbit GM, Anderson JC, Spencer D,Wang P, et al. Qualitative comparison of 3-T and 1.5-T MRI inthe evaluation of epilepsy. American Journal of Roentgenology2008;191:890–5.
12. Berg AT, Kelly MM. Defining intractability: comparisonsamong published definitions. Epilepsia 2006;47:431–6.
13. Craven I, Griffiths PD, Hoggard N. Magnetic resonanceimaging of epilepsy at 3 T. Clinical Radiology 2011;66:278–86.
14. Berg AT, Mathern GW, Bronen RA, Fulbright RK, DiMario F,Testa FM, et al. Frequency, prognosis and surgical treatmentof structural abnormalities seen with magnetic resonanceimaging in childhood epilepsy. Brain 2009;132:2785–97.
15. Urbach H, Hattingen J, von Oertzen J, Luyken C, Clusmann H,Kral T, et al. MR imaging in the presurgical workup ofpatients with drug-resistant epilepsy. American Journal ofNeuroradiology 2004;25:919–26.
16. Bronen RA. Epilepsy: the role of MR imaging. AmericanJournal of Roentgenology 1992;159:1165–74.
17. Agrawal A, Timothy J, Pandit L, Manju M. Post-traumaticepilepsy: an overview. Clinical Neurology and Neurosurgery2006;108:433–9.
18. Ferguson PL, Smith GM, Wannamaker BB, Thurman DJ,Pickelsimer EE, Selassie AW. A population-based study ofrisk of epilepsy after hospitalization for traumatic braininjury. Epilepsia 2010;51:891–8.
19. Burn J, Dennis M, Bamford J, Sandercock P, Wade D,Warlow C. Epileptic seizures after a first stroke: theOxfordshire Community Stroke Project. BMJ 1997;315:1582–7.
20. Chiang IH, Chang WN, Lin WC, Chuang YC, Chang KC, TsaiNW, et al. Risk factors for seizures after first-time ischemicstroke by magnetic resonance imaging. Acta NeurologicaTaiwanica 2010;19:26–32.
21. King MA, Newton MR, Jackson GD, Fitt GJ, Mitchell LA,Silvapulle MJ, et al. Epileptology of the first-seizurepresentation: a clinical, electroencephalographic, andmagnetic resonance imaging study of 300 consecutivepatients. Lancet 1998;352:1007–11.
22. Wieshmann UC. Clinical application of neuroimaging inepilepsy. Journal of Neurology Neurosurgery and Psychiatry2003;74:466–70.
23. Li LM, Fish DR, Sisodiya SM, Shorvon SD, Alsanjari N,Stevens JM. High resolution magnetic resonance imaging inadults with partial or secondary generalised epilepsyattending a tertiary referral unit. Journal of NeurologyNeurosurgery and Psychiatry 1995;59:384–7.
24. Semah F, Picot MC, Adam C, Broglin D, Arzimanoglou A,Bazin B, et al. Is the underlying cause of epilepsy a majorprognostic factor for recurrence. Neurology 1998;51:1256–62.
25. Kumar R, Gupta RK, Husain M, Vatsal DK, Chalwa S, RathoreRK, et al.Magnetization transfer MR imaging in patients withposttraumatic epilepsy. American Journal of Neuroradiology2003;24:218–24.
26. Jack Jr CR, Rydberg CH, Krecke KN, Trenerry MR, Parisi JE,Rdyberk JE, et al. Mesial temporal sclerosis: diagnosis withfluid-attenuated inversion-recovery versus spin-echo MRimaging. Radiology 1996;199:367–73.
27. Bronen RA, Fulbright RK, King D, Kim JH, Spencer SS,Spencer DD, et al. Qualitative MR imaging of refractorytemporal lobe epilepsy requiring surgery: Correlation withpathology and seizure outcome after surgery. AmericanJournal of Roentgenology 1997;169:875–82.
28. Brooks BS, King DW, El Gammal T, Meador K, Yaghmai F,Gay JN, et al. MR imaging in patients with intractablecomplex partial epileptic seizures. American Journal ofRoentgenology 1990;154:577–83.
29. Ostertun B, Wolf HK, Campos MG, Matus C, Solymosi L,Elger CE, et al. Dysembryoplastic neuroepithelial tumors: MRand CT evaluation. American Journal of Neuroradiology1996;17. 419-340.
30. Caruso PA, Robertson R, Setty B, Grant E. Disorders of braindevelopment. In: Atlas SW, editor. Magnetic resonance imagingof the brain and spine. 4th ed. Lippincott Williams & Wilkins;2009. p. 224–5.