Embed Size (px)
Citation preview

Full Terms & Conditions of access and use can be found athttp://www.tandfonline.com/action/journalInformation?journalCode=ieop20
Expert Opinion on Pharmacotherapy
ISSN: 1465-6566 (Print) 1744-7666 (Online) Journal homepage: http://www.tandfonline.com/loi/ieop20
Comparison between insulin degludec/liraglutidetreatment and insulin glargine/lixisenatidetreatment in type 2 diabetes: a systematic reviewand meta-analysis
Xiaoling Cai, Xueying Gao, Wenjia Yang & Linong Ji
To cite this article: Xiaoling Cai, Xueying Gao, Wenjia Yang & Linong Ji (2017) Comparisonbetween insulin degludec/liraglutide treatment and insulin glargine/lixisenatide treatment in type2 diabetes: a systematic review and meta-analysis, Expert Opinion on Pharmacotherapy, 18:17,1789-1798, DOI: 10.1080/14656566.2017.1400011
To link to this article: https://doi.org/10.1080/14656566.2017.1400011
View supplementary material
Accepted author version posted online: 01Nov 2017.Published online: 05 Nov 2017.
Submit your article to this journal
Article views: 1094
View Crossmark data
Citing articles: 4 View citing articles
ORIGINAL RESEARCH
Comparison between insulin degludec/liraglutide treatment and insulin glargine/lixisenatide treatment in type 2 diabetes: a systematic review and meta-analysisXiaoling Cai, Xueying Gao, Wenjia Yang and Linong Ji
Endocrine & Metabolism Department, Peking University People’s Hospital, Beijing, China
ABSTRACTAim: To evaluate the efficacy and adverse effects of IDegLira and IGlarLixi treatment and to perform acomparison between two strategies.Methods: The registration number is CRD42017053952. Randomized controlled trials of IGlarLixi treat-ment or IDegLira treatment compared with placebo or active hypoglycemic agents in type 2 diabeteswere included.Results: Eight trials were included. The absolute HbA1c change relative to baseline after IGlarLixitreatment was −1.50% with significance (95% CI, −1.89% to −1.12%, p < 0.01); the absolute HbA1cchange after IDegLira treatment was −1.89% with significance (95% CI, −2.04% to −1.73%, p < 0.01).Comparisons between IGlarLixi treatment and IDegLira treatment indicated no significant differencesbetween groups. The absolute weight change after IGlarLixi treatment significantly decreased(weighted mean difference (WMD), −0.62 kg; 95% CI, −0.93 to −0.31 kg, p = < 0.01), but the absoluteweight change after IDegLira treatment was not significantly changed (WMD, −0.81 kg; 95% CI, −3.26 to1.65 kg, p = 0.52). There were no significant differences between groups.Conclusion: Glucose control of IGlarLixi treatment or IDegLira treatment was significantly lower thanthat at baseline. Comparisons between the two treatment groups indicated no significant differencesbetween groups in absolute HbA1c changes or body weight changes relative to baseline.
ARTICLE HISTORYReceived 12 September 2017Accepted 30 October 2017
KEYWORDSIDegLira; IGlarLixi; HbA1c;body weight
1. Introduction
According to the American Diabetes Association andEuropean Association for the Study of Diabetes guideline,the combined use of basal insulin and glucagon-like peptide1 receptor agonist (GLP-1 RA) is a recommended strategy tomanage hyperglycemia when glucose cannot be controlled bybasal insulin or GLP-1 RA [1].
The combination of basal insulin with a GLP-1 RA has pro-vided higher efficacy than that of the individual therapies. Basalinsulin therapy improves fasting plasma glucose (FPG) andHbA1c levels, but it is associated with weight gain and increasedrisk of hypoglycemia [2], whereas GLP-1 RAs affect glucose con-trol through augmented incretin effects and induce weight losswithout increasing the risk of hypoglycemia [3–7]. Therefore,combination therapy of these two classes of hypoglycemic med-ications has the potential of mitigating the barriers associatedwith their individual use. A recently published meta-analysis hasdemonstrated the efficacy of GLP-1 RA and basal insulin in theform of both free and fixed-ratio combinations in glucose andbody weight control [8].
To date, two types of fixed-ratio combinations of basal insu-lin and GLP-1 RA have been approved for use in type 2 diabetespatients. One is insulin degludec/liraglutide (IDegLira), a fixed-ratio combination of basal insulin degludec (IDeg) and the GLP-1 analog liraglutide (Lira), and the other is insulin glargine/lixisenatide (IGlarLixi), a fixed-ratio combination of basal insulin
glargine (IGlar) and the GLP-1 analog lixisenatide (Lixi); both aredelivered via a single, daily injection. IDegLira combines IDeg,which decreases FPG levels [9], and Lira, which mainly lowersFPG but also modestly decreases postprandial glucose excur-sions [10]. IGlarLixi combines IGlar, which decreases the FPGlevel, and Lixi, which has a predominant postprandial plasmaglucose (PPG)-lowering effect. The efficacy on glucose controlof glargine has been demonstrated to be comparable to that ofdegludec when used in combination with oral hypoglycemicagents [11], whereas liraglutide treatment has been found to besuperior to lixisenatide treatment in lowering HbA1c [12,13].
IGlarLixi is a combination of insulin glargine and lixisena-tide, of which the complement of a long-acting insulin anda short-acting GLP-1 RA addresses both FPG and PPG,whereas IDegLira treatment is a combination of insulindegludec and liraglutide, a combination of a long-actinginsulin and a long-acting GLP-1 RA, which may result in aredundant effect on FPG levels but little effect on PPGlevels. Therefore, we hypothesized that, when using afixed-ratio combination with basal insulin, the superiorityof long-acting GLP-1 RAs over short-acting GLP-1 RAsmight be compromised.
Therefore, we performed this meta-analysis to evaluate theefficacy and adverse effects of IDegLira and IGlarLixi treatmentand to perform a comparison between these two types oftreatment.
CONTACT Linong Ji [email protected] Endocrinology and Metabolism Department, Peking University People’s Hospital, Beijing, 100044, ChinaSupplemental data can be accessed here.
EXPERT OPINION ON PHARMACOTHERAPY, 2017VOL. 18, NO. 17, 1789–1798https://doi.org/10.1080/14656566.2017.1400011
© 2017 Informa UK Limited, trading as Taylor & Francis Group

2. Methods
2.1. Search strategy
The electronic search was performed from December 2016 toMarch 2017, and randomized clinical trials publicly availablecomparing the fixed-ratio combination of insulin and GLP-1 RAwith placebo or active hypoglycemic treatment in type 2diabetes patients were identified. There are currently twotypes of fixed-ratio combination of insulin and GLP-1 RA: oneis IGlarLixi (combination of insulin glargine and lixisenatide)and the other is IDegLira (combination of insulin degludec andliraglutide). Therefore, the following search terms were used:type 2 diabetes, lixisenatide, liraglutide, IGlarLixi, IDegLira, andrandomized controlled trials (RCTs). The databases of theMEDLINE and the Cochrane Library Central Register ofControlled Trials were searched. The registration number ofthis meta-analysis is CRD42017053952.
2.2. Inclusion criteria and data extraction
The inclusion criteria were as follows: (1) IGlarLixi treatmentcompared with placebo or active hypoglycemic agents; (2)IDegLira treatment compared with placebo or active hypogly-cemic agents; (3) in type 2 diabetes participants; (4) study lengthlonger than 12 weeks; (5) the efficacy of glucose control was theprimary outcome of the study; and (6) the studies were RCTs.
The exclusion criteria were as follows: (1) nonrandomizedtrials; (2) trials involving type 1 diabetes; (3) study length lessthan 12 weeks; and (4) inability to determine efficacy of glu-cose control from the trial.
Two investigators (XYG and WJY) screened the titles andabstracts independently to identify potentially eligible trials.Any discrepancies were discussed with a third author (XLC)until a consensus was reached. The two investigators indepen-dently reviewed the main reports and supplementary materi-als and extracted the study and patient characteristics andtreatment strategies. The quality of each study and the riskof bias were evaluated using the Cochrane instrument.
2.3. End points
The primary end point of this meta-analysis was absolute HbA1cchange relative to baseline after IGlarLixi treatment and IDegLiratreatment in type 2 diabetes patients. The secondary end pointswere the following: (1) absolute FPG changes relative to baselineafter IGlarLixi treatment and after IDegLira treatment; (2) absolutePPG changes or mean 9-point self-monitoring blood glucose(SMBG) changes relative to baseline after IGlarLixi treatment andafter IDegLira treatment; (3) absolute body weight changes rela-tive to baseline after IGlarLixi treatment and after IDegLira treat-ment; and (4) association between the efficacy of IGlarLixitreatment or IDegLira treatment and baseline characteristics,such as age, sex, bodymass index (BMI), bodyweight, and HbA1c.
2.4. Statistical analysis
Treatment effects and adverse effects were estimated with arandom-effects model or fixed-effects model meta-analysis.
The absolute changes relative to baseline after IGlarLixi treat-ment or IDegLira treatment were estimated by computing themean differences in HbA1C levels, FPG levels, PPG levels, andbody weight, together with 95% confidence intervals (95% CI).The weighted mean difference (WMD) and 95% CI were alsoestimated for placebo-corrected or active-controlled glucosechanges and weight changes after IGlarLixi treatment orIDegLira treatment. By computing the odds ratios togetherwith 95% CIs, adverse events and hypoglycemia were esti-mated. Higgins I2 statistics were used to quantify the percen-tage of the total variance in the summary estimate due tobetween-study heterogeneity. Publication bias was assessedvia a funnel plot and Egger’s test analysis. Statistical testingwas two sided, with p < 0.05 considered statistically signifi-cant. Most of the statistical analyses were performed with theReview Manager statistical software package (version 5.2,Nordic Cochrane Centre, Copenhagen, Denmark). Somemeta-regression analyses were performed with STATA soft-ware (version 11.0, Stata Corp, College Station, TX, USA). Thismeta-analysis was conducted according to the PreferredReporting Items for Systematic Reviews and Meta-Analyses(PRISMA) guidelines for conducting and reporting meta-ana-lyses of RCTs.
3. Results
3.1. Studies included in this meta-analysis andqualifications
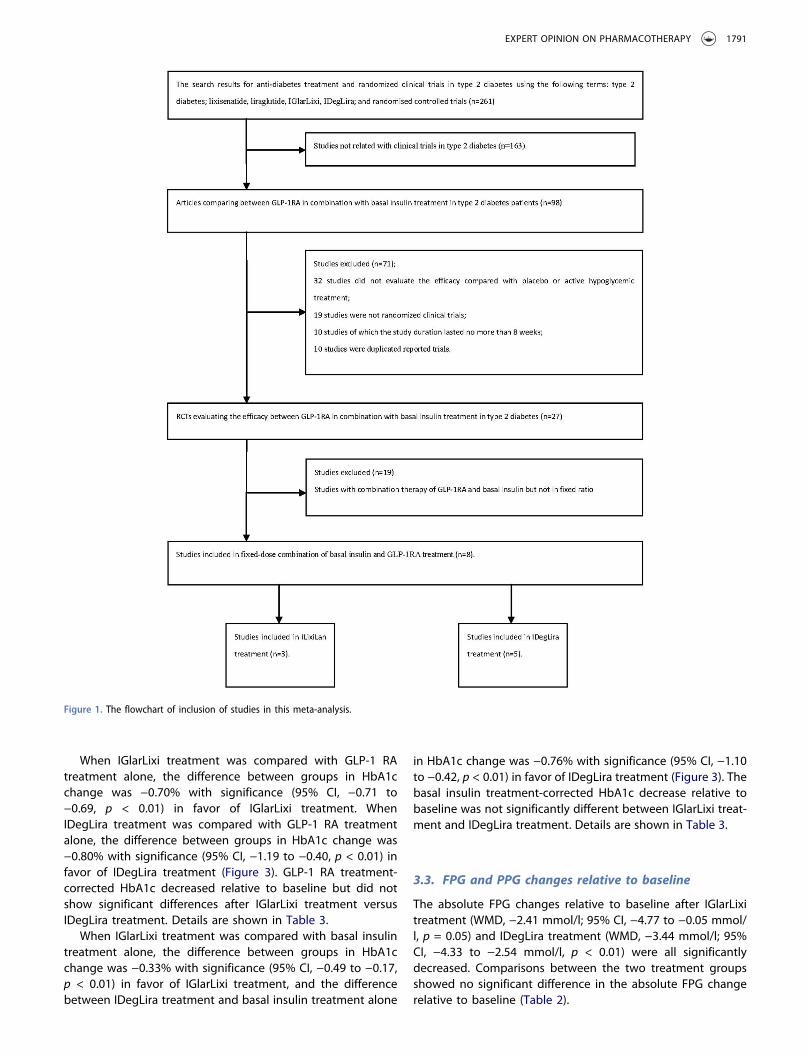
The electronic search was performed from December 2016 toMarch 2017, and 261 citations were selected according to thesearch terms. By screening the abstracts and the full text,according to the inclusion criteria, 253 articles were excluded,and the flowchart of included studies is summarized inFigure 1. Eight randomized clinical trials were included in theanalysis [14–21], among which three trials were included withIIGlarLixi treatment [14–16] and five trials with IDegLira treat-ment compared with placebo or GLP-1 RA alone or basalinsulin alone [17–21]. The baseline characteristics of studiesincluded in this meta-analysis are shown in Table 1.
By using the Cochrane instrument, the risk of bias wasevaluated. Overall, the risk of bias was low; the randomsequence generation, the allocation concealment, the blindingof participants and personnel, the blinding of outcome assess-ment, and the incomplete outcome data were all wellreported, and the selective reporting was low (SupplementalFigure S1).
3.2. HbA1c changes relative to baseline
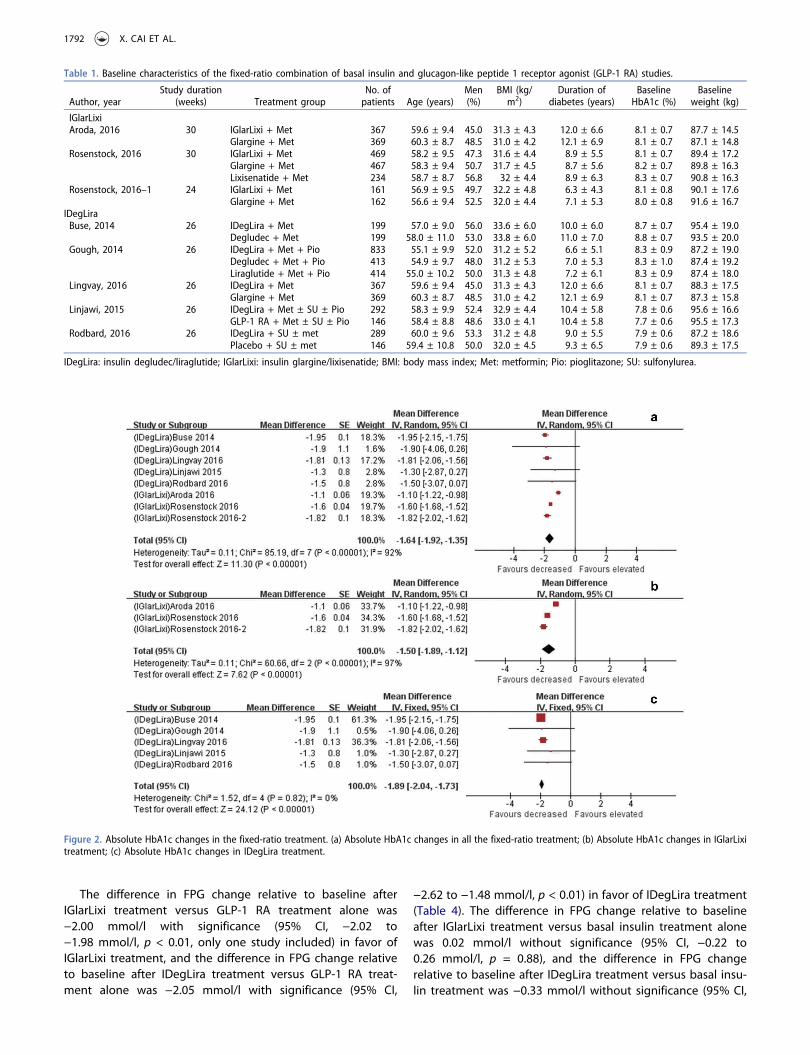
In terms of HbA1c, the absolute HbA1c change relative tobaseline after IGlarLixi treatment was −1.50% with significance(95% CI, −1.89 to −1.12, p < 0.01) and that after IDegLiratreatment was −1.89% with significance (95% CI, −2.04 to−1.73, p < 0.01) (Figure 2). Comparisons between IGlarLixitreatment and IDegLira treatment indicated no significantdifferences between groups in absolute HbA1c change relativeto baseline. Details are shown in Table 2.
1790 X. CAI ET AL.
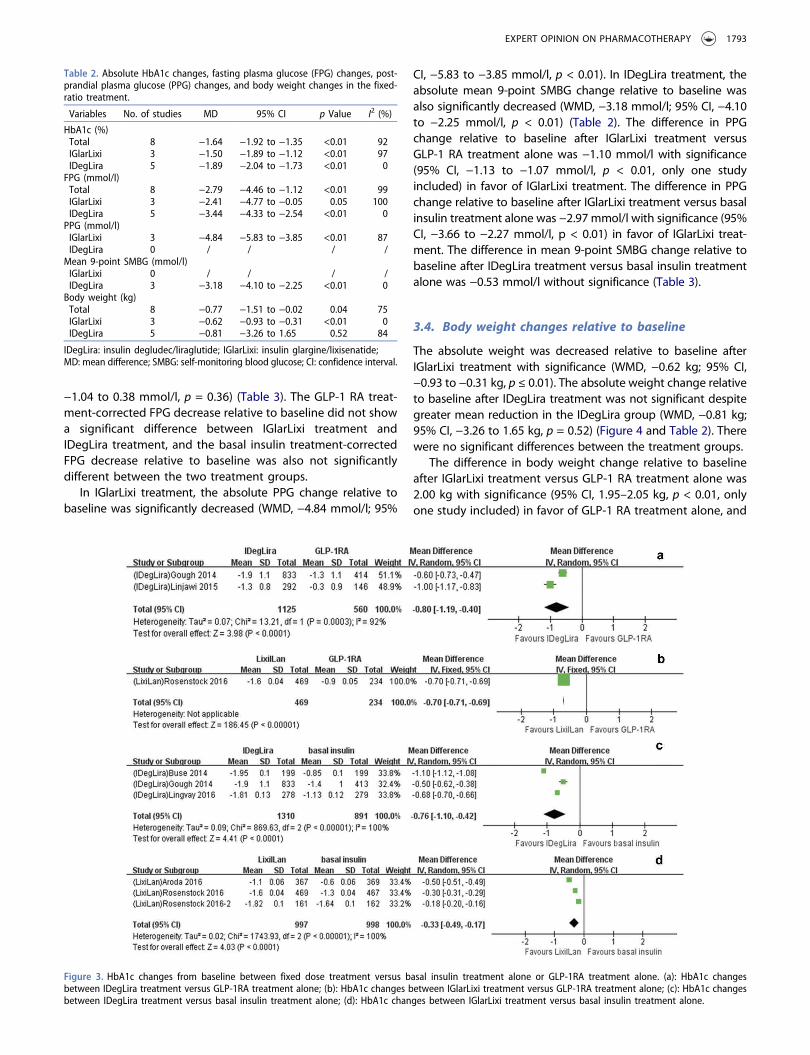
When IGlarLixi treatment was compared with GLP-1 RAtreatment alone, the difference between groups in HbA1cchange was −0.70% with significance (95% CI, −0.71 to−0.69, p < 0.01) in favor of IGlarLixi treatment. WhenIDegLira treatment was compared with GLP-1 RA treatmentalone, the difference between groups in HbA1c change was−0.80% with significance (95% CI, −1.19 to −0.40, p < 0.01) infavor of IDegLira treatment (Figure 3). GLP-1 RA treatment-corrected HbA1c decreased relative to baseline but did notshow significant differences after IGlarLixi treatment versusIDegLira treatment. Details are shown in Table 3.
When IGlarLixi treatment was compared with basal insulintreatment alone, the difference between groups in HbA1cchange was −0.33% with significance (95% CI, −0.49 to −0.17,p < 0.01) in favor of IGlarLixi treatment, and the differencebetween IDegLira treatment and basal insulin treatment alone
in HbA1c change was −0.76% with significance (95% CI, −1.10to −0.42, p < 0.01) in favor of IDegLira treatment (Figure 3). Thebasal insulin treatment-corrected HbA1c decrease relative tobaseline was not significantly different between IGlarLixi treat-ment and IDegLira treatment. Details are shown in Table 3.
3.3. FPG and PPG changes relative to baseline
The absolute FPG changes relative to baseline after IGlarLixitreatment (WMD, −2.41 mmol/l; 95% CI, −4.77 to −0.05 mmol/l, p = 0.05) and IDegLira treatment (WMD, −3.44 mmol/l; 95%CI, −4.33 to −2.54 mmol/l, p < 0.01) were all significantlydecreased. Comparisons between the two treatment groupsshowed no significant difference in the absolute FPG changerelative to baseline (Table 2).
Figure 1. The flowchart of inclusion of studies in this meta-analysis.
EXPERT OPINION ON PHARMACOTHERAPY 1791
The difference in FPG change relative to baseline afterIGlarLixi treatment versus GLP-1 RA treatment alone was−2.00 mmol/l with significance (95% CI, −2.02 to−1.98 mmol/l, p < 0.01, only one study included) in favor ofIGlarLixi treatment, and the difference in FPG change relativeto baseline after IDegLira treatment versus GLP-1 RA treat-ment alone was −2.05 mmol/l with significance (95% CI,
−2.62 to −1.48 mmol/l, p < 0.01) in favor of IDegLira treatment(Table 4). The difference in FPG change relative to baselineafter IGlarLixi treatment versus basal insulin treatment alonewas 0.02 mmol/l without significance (95% CI, −0.22 to0.26 mmol/l, p = 0.88), and the difference in FPG changerelative to baseline after IDegLira treatment versus basal insu-lin treatment was −0.33 mmol/l without significance (95% CI,
Table 1. Baseline characteristics of the fixed-ratio combination of basal insulin and glucagon-like peptide 1 receptor agonist (GLP-1 RA) studies.
Author, yearStudy duration
(weeks) Treatment groupNo. ofpatients Age (years)
Men(%)
BMI (kg/m2)
Duration ofdiabetes (years)
BaselineHbA1c (%)
Baselineweight (kg)
IGlarLixiAroda, 2016 30 IGlarLixi + Met 367 59.6 ± 9.4 45.0 31.3 ± 4.3 12.0 ± 6.6 8.1 ± 0.7 87.7 ± 14.5
Glargine + Met 369 60.3 ± 8.7 48.5 31.0 ± 4.2 12.1 ± 6.9 8.1 ± 0.7 87.1 ± 14.8Rosenstock, 2016 30 IGlarLixi + Met 469 58.2 ± 9.5 47.3 31.6 ± 4.4 8.9 ± 5.5 8.1 ± 0.7 89.4 ± 17.2
Glargine + Met 467 58.3 ± 9.4 50.7 31.7 ± 4.5 8.7 ± 5.6 8.2 ± 0.7 89.8 ± 16.3Lixisenatide + Met 234 58.7 ± 8.7 56.8 32 ± 4.4 8.9 ± 6.3 8.3 ± 0.7 90.8 ± 16.3
Rosenstock, 2016–1 24 IGlarLixi + Met 161 56.9 ± 9.5 49.7 32.2 ± 4.8 6.3 ± 4.3 8.1 ± 0.8 90.1 ± 17.6Glargine + Met 162 56.6 ± 9.4 52.5 32.0 ± 4.4 7.1 ± 5.3 8.0 ± 0.8 91.6 ± 16.7
IDegLiraBuse, 2014 26 IDegLira + Met 199 57.0 ± 9.0 56.0 33.6 ± 6.0 10.0 ± 6.0 8.7 ± 0.7 95.4 ± 19.0
Degludec + Met 199 58.0 ± 11.0 53.0 33.8 ± 6.0 11.0 ± 7.0 8.8 ± 0.7 93.5 ± 20.0Gough, 2014 26 IDegLira + Met + Pio 833 55.1 ± 9.9 52.0 31.2 ± 5.2 6.6 ± 5.1 8.3 ± 0.9 87.2 ± 19.0
Degludec + Met + Pio 413 54.9 ± 9.7 48.0 31.2 ± 5.3 7.0 ± 5.3 8.3 ± 1.0 87.4 ± 19.2Liraglutide + Met + Pio 414 55.0 ± 10.2 50.0 31.3 ± 4.8 7.2 ± 6.1 8.3 ± 0.9 87.4 ± 18.0
Lingvay, 2016 26 IDegLira + Met 367 59.6 ± 9.4 45.0 31.3 ± 4.3 12.0 ± 6.6 8.1 ± 0.7 88.3 ± 17.5Glargine + Met 369 60.3 ± 8.7 48.5 31.0 ± 4.2 12.1 ± 6.9 8.1 ± 0.7 87.3 ± 15.8
Linjawi, 2015 26 IDegLira + Met ± SU ± Pio 292 58.3 ± 9.9 52.4 32.9 ± 4.4 10.4 ± 5.8 7.8 ± 0.6 95.6 ± 16.6GLP-1 RA + Met ± SU ± Pio 146 58.4 ± 8.8 48.6 33.0 ± 4.1 10.4 ± 5.8 7.7 ± 0.6 95.5 ± 17.3
Rodbard, 2016 26 IDegLira + SU ± met 289 60.0 ± 9.6 53.3 31.2 ± 4.8 9.0 ± 5.5 7.9 ± 0.6 87.2 ± 18.6Placebo + SU ± met 146 59.4 ± 10.8 50.0 32.0 ± 4.5 9.3 ± 6.5 7.9 ± 0.6 89.3 ± 17.5
IDegLira: insulin degludec/liraglutide; IGlarLixi: insulin glargine/lixisenatide; BMI: body mass index; Met: metformin; Pio: pioglitazone; SU: sulfonylurea.
Figure 2. Absolute HbA1c changes in the fixed-ratio treatment. (a) Absolute HbA1c changes in all the fixed-ratio treatment; (b) Absolute HbA1c changes in IGlarLixitreatment; (c) Absolute HbA1c changes in IDegLira treatment.
1792 X. CAI ET AL.
−1.04 to 0.38 mmol/l, p = 0.36) (Table 3). The GLP-1 RA treat-ment-corrected FPG decrease relative to baseline did not showa significant difference between IGlarLixi treatment andIDegLira treatment, and the basal insulin treatment-correctedFPG decrease relative to baseline was also not significantlydifferent between the two treatment groups.
In IGlarLixi treatment, the absolute PPG change relative tobaseline was significantly decreased (WMD, −4.84 mmol/l; 95%
CI, −5.83 to −3.85 mmol/l, p < 0.01). In IDegLira treatment, theabsolute mean 9-point SMBG change relative to baseline wasalso significantly decreased (WMD, −3.18 mmol/l; 95% CI, −4.10to −2.25 mmol/l, p < 0.01) (Table 2). The difference in PPGchange relative to baseline after IGlarLixi treatment versusGLP-1 RA treatment alone was −1.10 mmol/l with significance(95% CI, −1.13 to −1.07 mmol/l, p < 0.01, only one studyincluded) in favor of IGlarLixi treatment. The difference in PPGchange relative to baseline after IGlarLixi treatment versus basalinsulin treatment alone was −2.97 mmol/l with significance (95%CI, −3.66 to −2.27 mmol/l, p < 0.01) in favor of IGlarLixi treat-ment. The difference in mean 9-point SMBG change relative tobaseline after IDegLira treatment versus basal insulin treatmentalone was −0.53 mmol/l without significance (Table 3).
3.4. Body weight changes relative to baseline
The absolute weight was decreased relative to baseline afterIGlarLixi treatment with significance (WMD, −0.62 kg; 95% CI,−0.93 to −0.31 kg, p ≤ 0.01). The absolute weight change relativeto baseline after IDegLira treatment was not significant despitegreater mean reduction in the IDegLira group (WMD, −0.81 kg;95% CI, −3.26 to 1.65 kg, p = 0.52) (Figure 4 and Table 2). Therewere no significant differences between the treatment groups.
The difference in body weight change relative to baselineafter IGlarLixi treatment versus GLP-1 RA treatment alone was2.00 kg with significance (95% CI, 1.95–2.05 kg, p < 0.01, onlyone study included) in favor of GLP-1 RA treatment alone, and
Table 2. Absolute HbA1c changes, fasting plasma glucose (FPG) changes, post-prandial plasma glucose (PPG) changes, and body weight changes in the fixed-ratio treatment.
Variables No. of studies MD 95% CI p Value I2 (%)
HbA1c (%)Total 8 −1.64 −1.92 to −1.35 <0.01 92IGlarLixi 3 −1.50 −1.89 to −1.12 <0.01 97IDegLira 5 −1.89 −2.04 to −1.73 <0.01 0FPG (mmol/l)Total 8 −2.79 −4.46 to −1.12 <0.01 99IGlarLixi 3 −2.41 −4.77 to −0.05 0.05 100IDegLira 5 −3.44 −4.33 to −2.54 <0.01 0PPG (mmol/l)IGlarLixi 3 −4.84 −5.83 to −3.85 <0.01 87IDegLira 0 / / / /Mean 9-point SMBG (mmol/l)IGlarLixi 0 / / / /IDegLira 3 −3.18 −4.10 to −2.25 <0.01 0Body weight (kg)Total 8 −0.77 −1.51 to −0.02 0.04 75IGlarLixi 3 −0.62 −0.93 to −0.31 <0.01 0IDegLira 5 −0.81 −3.26 to 1.65 0.52 84
IDegLira: insulin degludec/liraglutide; IGlarLixi: insulin glargine/lixisenatide;MD: mean difference; SMBG: self-monitoring blood glucose; CI: confidence interval.
Figure 3. HbA1c changes from baseline between fixed dose treatment versus basal insulin treatment alone or GLP-1RA treatment alone. (a): HbA1c changesbetween IDegLira treatment versus GLP-1RA treatment alone; (b): HbA1c changes between IGlarLixi treatment versus GLP-1RA treatment alone; (c): HbA1c changesbetween IDegLira treatment versus basal insulin treatment alone; (d): HbA1c changes between IGlarLixi treatment versus basal insulin treatment alone.
EXPERT OPINION ON PHARMACOTHERAPY 1793
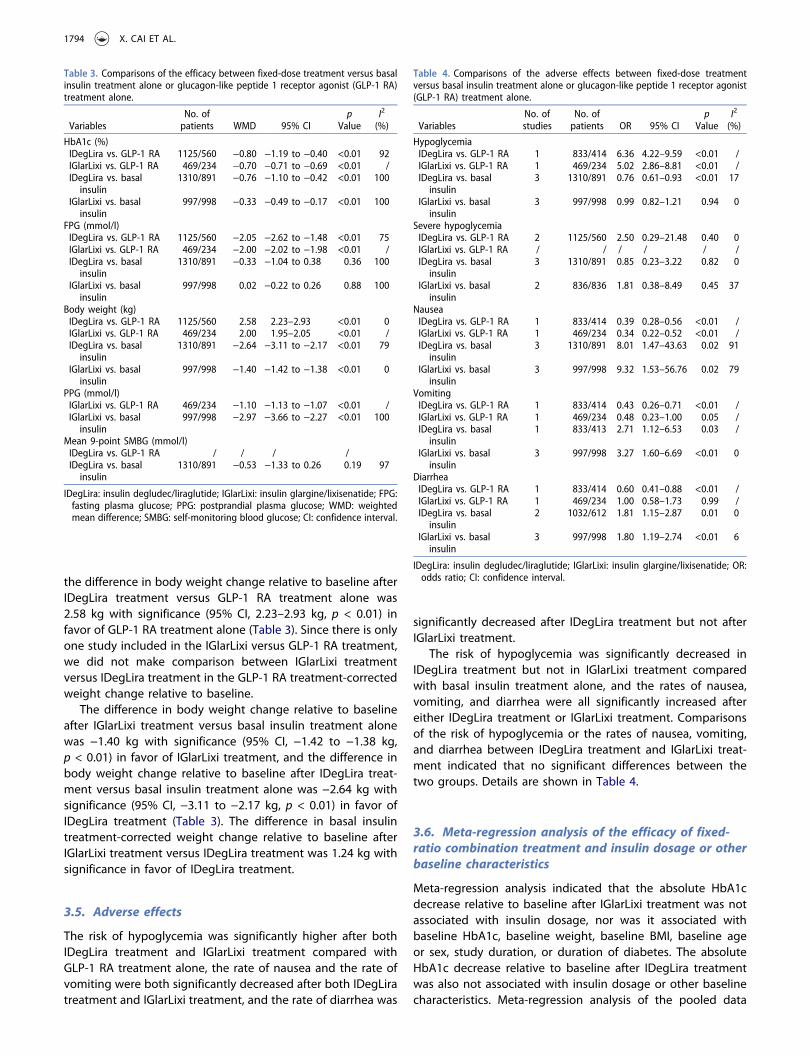
the difference in body weight change relative to baseline afterIDegLira treatment versus GLP-1 RA treatment alone was2.58 kg with significance (95% CI, 2.23–2.93 kg, p < 0.01) infavor of GLP-1 RA treatment alone (Table 3). Since there is onlyone study included in the IGlarLixi versus GLP-1 RA treatment,we did not make comparison between IGlarLixi treatmentversus IDegLira treatment in the GLP-1 RA treatment-correctedweight change relative to baseline.
The difference in body weight change relative to baselineafter IGlarLixi treatment versus basal insulin treatment alonewas −1.40 kg with significance (95% CI, −1.42 to −1.38 kg,p < 0.01) in favor of IGlarLixi treatment, and the difference inbody weight change relative to baseline after IDegLira treat-ment versus basal insulin treatment alone was −2.64 kg withsignificance (95% CI, −3.11 to −2.17 kg, p < 0.01) in favor ofIDegLira treatment (Table 3). The difference in basal insulintreatment-corrected weight change relative to baseline afterIGlarLixi treatment versus IDegLira treatment was 1.24 kg withsignificance in favor of IDegLira treatment.
3.5. Adverse effects
The risk of hypoglycemia was significantly higher after bothIDegLira treatment and IGlarLixi treatment compared withGLP-1 RA treatment alone, the rate of nausea and the rate ofvomiting were both significantly decreased after both IDegLiratreatment and IGlarLixi treatment, and the rate of diarrhea was
significantly decreased after IDegLira treatment but not afterIGlarLixi treatment.
The risk of hypoglycemia was significantly decreased inIDegLira treatment but not in IGlarLixi treatment comparedwith basal insulin treatment alone, and the rates of nausea,vomiting, and diarrhea were all significantly increased aftereither IDegLira treatment or IGlarLixi treatment. Comparisonsof the risk of hypoglycemia or the rates of nausea, vomiting,and diarrhea between IDegLira treatment and IGlarLixi treat-ment indicated that no significant differences between thetwo groups. Details are shown in Table 4.
3.6. Meta-regression analysis of the efficacy of fixed-ratio combination treatment and insulin dosage or otherbaseline characteristics
Meta-regression analysis indicated that the absolute HbA1cdecrease relative to baseline after IGlarLixi treatment was notassociated with insulin dosage, nor was it associated withbaseline HbA1c, baseline weight, baseline BMI, baseline ageor sex, study duration, or duration of diabetes. The absoluteHbA1c decrease relative to baseline after IDegLira treatmentwas also not associated with insulin dosage or other baselinecharacteristics. Meta-regression analysis of the pooled data
Table 3. Comparisons of the efficacy between fixed-dose treatment versus basalinsulin treatment alone or glucagon-like peptide 1 receptor agonist (GLP-1 RA)treatment alone.
VariablesNo. ofpatients WMD 95% CI
pValue
I2
(%)
HbA1c (%)IDegLira vs. GLP-1 RA 1125/560 −0.80 −1.19 to −0.40 <0.01 92IGlarLixi vs. GLP-1 RA 469/234 −0.70 −0.71 to −0.69 <0.01 /IDegLira vs. basalinsulin
1310/891 −0.76 −1.10 to −0.42 <0.01 100
IGlarLixi vs. basalinsulin
997/998 −0.33 −0.49 to −0.17 <0.01 100
FPG (mmol/l)IDegLira vs. GLP-1 RA 1125/560 −2.05 −2.62 to −1.48 <0.01 75IGlarLixi vs. GLP-1 RA 469/234 −2.00 −2.02 to −1.98 <0.01 /IDegLira vs. basalinsulin
1310/891 −0.33 −1.04 to 0.38 0.36 100
IGlarLixi vs. basalinsulin
997/998 0.02 −0.22 to 0.26 0.88 100
Body weight (kg)IDegLira vs. GLP-1 RA 1125/560 2.58 2.23–2.93 <0.01 0IGlarLixi vs. GLP-1 RA 469/234 2.00 1.95–2.05 <0.01 /IDegLira vs. basalinsulin
1310/891 −2.64 −3.11 to −2.17 <0.01 79
IGlarLixi vs. basalinsulin
997/998 −1.40 −1.42 to −1.38 <0.01 0
PPG (mmol/l)IGlarLixi vs. GLP-1 RA 469/234 −1.10 −1.13 to −1.07 <0.01 /IGlarLixi vs. basalinsulin
997/998 −2.97 −3.66 to −2.27 <0.01 100
Mean 9-point SMBG (mmol/l)IDegLira vs. GLP-1 RA / / / /IDegLira vs. basalinsulin
1310/891 −0.53 −1.33 to 0.26 0.19 97
IDegLira: insulin degludec/liraglutide; IGlarLixi: insulin glargine/lixisenatide; FPG:fasting plasma glucose; PPG: postprandial plasma glucose; WMD: weightedmean difference; SMBG: self-monitoring blood glucose; CI: confidence interval.
Table 4. Comparisons of the adverse effects between fixed-dose treatmentversus basal insulin treatment alone or glucagon-like peptide 1 receptor agonist(GLP-1 RA) treatment alone.
VariablesNo. ofstudies
No. ofpatients OR 95% CI
pValue
I2
(%)
HypoglycemiaIDegLira vs. GLP-1 RA 1 833/414 6.36 4.22–9.59 <0.01 /IGlarLixi vs. GLP-1 RA 1 469/234 5.02 2.86–8.81 <0.01 /IDegLira vs. basalinsulin
3 1310/891 0.76 0.61–0.93 <0.01 17
IGlarLixi vs. basalinsulin
3 997/998 0.99 0.82–1.21 0.94 0
Severe hypoglycemiaIDegLira vs. GLP-1 RA 2 1125/560 2.50 0.29–21.48 0.40 0IGlarLixi vs. GLP-1 RA / / / / / /IDegLira vs. basalinsulin
3 1310/891 0.85 0.23–3.22 0.82 0
IGlarLixi vs. basalinsulin
2 836/836 1.81 0.38–8.49 0.45 37
NauseaIDegLira vs. GLP-1 RA 1 833/414 0.39 0.28–0.56 <0.01 /IGlarLixi vs. GLP-1 RA 1 469/234 0.34 0.22–0.52 <0.01 /IDegLira vs. basalinsulin
3 1310/891 8.01 1.47–43.63 0.02 91
IGlarLixi vs. basalinsulin
3 997/998 9.32 1.53–56.76 0.02 79
VomitingIDegLira vs. GLP-1 RA 1 833/414 0.43 0.26–0.71 <0.01 /IGlarLixi vs. GLP-1 RA 1 469/234 0.48 0.23–1.00 0.05 /IDegLira vs. basalinsulin
1 833/413 2.71 1.12–6.53 0.03 /
IGlarLixi vs. basalinsulin
3 997/998 3.27 1.60–6.69 <0.01 0
DiarrheaIDegLira vs. GLP-1 RA 1 833/414 0.60 0.41–0.88 <0.01 /IGlarLixi vs. GLP-1 RA 1 469/234 1.00 0.58–1.73 0.99 /IDegLira vs. basalinsulin
2 1032/612 1.81 1.15–2.87 0.01 0
IGlarLixi vs. basalinsulin
3 997/998 1.80 1.19–2.74 <0.01 6
IDegLira: insulin degludec/liraglutide; IGlarLixi: insulin glargine/lixisenatide; OR:odds ratio; CI: confidence interval.
1794 X. CAI ET AL.

including both IGlarLixi treatment and IDegLira treatmentindicated that the absolute HbA1c decrease relative to base-line was not associated with baseline characteristics and insu-lin dosage, nor was associated with body weight changesrelative to baseline.
We also performed meta-regression analysis of the associa-tion between absolute FPG changes or PPG changes relativeto baseline and the insulin dosage or other baseline character-istics after IGlarLixi treatment or IDegLira treatment or pooleddata, indicating no significant associations. The meta-regres-sion analysis of the association between absolute body weightchanges and insulin dosage or other baseline characteristics aswell as duration of diabetes of the pooled data, indicated nosignificant associations (Table S1).
The insulin dosages of IGlarLixi treatment and IDegLiratreatment used in this meta-analysis are shown in Table S2.The average insulin dosages between the two treatmentgroups were comparable. The data represent the dosage ofGLP-1 RA used are shown in Table S2.
4. Discussion
It has been suggested that the fixed-ratio combinations ofIDegLira and of IGlarLixi might offer a simpler way to use thetherapeutic strategy of combination therapy of basal insulinand GLP-1 RA. This meta-analysis demonstrated that the abso-lute HbA1c changes and the absolute FPG levels after IGlarLixitreatment (−1.50% in HbA1c and −2.41 mmol/l in FPG) andIDegLira treatment (−1.89% in HbA1c and −3.44 mmol/l in
FPG) were significantly decreased relative to baseline, andcomparisons between IGlarLixi treatment and IDegLira treat-ment did not indicate significant differences in absoluteHbA1c changes (0.39%) or FPG changes (1.01 mmol/l) relativeto baseline. This meta-analysis also found that, the absolutePPG change relative to baseline was significantly lower afterIGlarLixi treatment, and mean 9-point SMBG change was sig-nificantly lower after IDegLira treatment.
According to this meta-analysis, we also found that com-parisons of the HbA1c level between IGlarLixi treatment andIDegLira treatment, compared with GLP-1 RA, did not showsignificant differences; the between-group difference in FPGlevel was not significant, but the between-group difference inbody weight increase was 0.58 kg with significance in favor ofIGlarLixi treatment. Compared with basal insulin, the between-group differences in HbA1c level and FPG level were notsignificant, but the between-group difference in body weightdecrease was 1.24 kg with significance in favor of IDegLiratreatment.
To our knowledge, information on direct comparisonsbetween liraglutide and lixisenatide is not available.According to previous studies, treatment with liraglutidealone has been found to lead to a decrease in HbA1c rangingfrom 0.6% to 2.8% corrected by placebo and a decrease in FPGranging from 1.2 to 2.2 mmol/l corrected by placebo [22–25],whereas treatment with lixisenatide alone results in a decreasein HbA1c ranging from 0.3% to 0.8% corrected by placebo anda decrease in FPG ranging from 0 to 1.2 mmol/l corrected byplacebo [6,7,26,27]. In this meta-analysis, the efficacy of
Figure 4. Absolute weight changes in the fixed-ratio treatment. (a) Absolute weight changes in all the fixed-ratio treatment; (b) Absolute weight changes in IGlarLixitreatment; (c) Absolute weight changes in IDegLira treatment.
EXPERT OPINION ON PHARMACOTHERAPY 1795
glucose control in terms of absolute HbA1c decrease and FPGdecrease was comparable between IGlarLixi treatment andIDegLira treatment, whereas both HbA1c decrease and FPGdecrease corrected by placebo were superior in liraglutidetreatment compared to lixisenatide treatment when thesecompounds were used alone. How can we explain thisphenomenon?
First, it might be associated with differences in composi-tions of the two fixed-ratio compounds. IGlarLixi treatment is acombination of insulin glargine and lixisenatide, which is acombination of a basal insulin and a short-acting GLP-1 RA,whereas IDegLira treatment is a combination of insulin deglu-dec and liraglutide, which is a combination of a basal insulinand a long-acting GLP-1 RA. The corresponding GLP-1 RAs arelixisenatide and liraglutide: one is short acting and the other islong acting. It has been suggested that, because short-actingGLP-1 RAs delay gastric emptying, they have greater effects onpostprandial glucose levels than long-acting agents, whereaslong-acting compounds decreased plasma glucose through-out the entire period of time [12,13]. Direct comparisonsbetween liraglutide and lixisenatide have provided evidenceof these effects [28–30]. Liraglutide leads to greater decreasesin HbA1c than lixisenatide (p < 0.01) in a phase II study [28],and the changes in FPG are also greater with liraglutide thanwith lixisenatide (−1.3 vs. −0.3 mmol/l, p < 0.0001), whereaslixisenatide resulted in a significantly greater decrease in PPG(liraglutide −7.3 mmol/l vs. lixisenatide −10.1 mmol/l). Anotheradd-on metformin study [29] also indicated that liraglutidereduced HbA1c more than lixisenatide (difference in HbA1c−0.62%, p < 0.0001) and reduce FPG more (difference in FPG−1.15mmol/L, p < 0.0001). However, in the same study, post-prandial glucose increments were smaller with lixisenatidecompared with liraglutide (p < 0.05). In another study [30],the results have shown that, in terms of decreasing area underthe PPG curve, lixisenatide has a significantly greater effectthan liraglutide. Therefore, when used alone, long-acting GLP-1 RAs such as liraglutide have greater overall efficacy than thatof short-acting GLP-1 RAs, whereas short-acting GLP-1 RAssuch as lixisenatide have an advantage in improving PPG.
However, when using a fixed-ratio combination with basalinsulin, the advantage of long-acting GLP-1 RAs, comparedwith short-acting GLP-1 RAs, in improving HbA1c and FPGlevels may disappear, as indicated in this meta-analysis.Short-acting GLP-1 RAs such as lixisenatide delay gastric emp-tying and thus decrease postprandial blood glucose exposure,and they are used in combination with basal insulin such asglargine, which improves glucose control by causing a down-ward shift in the entire 24-h glucose curve. This type of fixed-ratio combination targets both FPG and PPG levels and there-fore the components have a complementary effect on glucosecontrol. However, long-acting GLP-1 RAs such as liraglutideresult in great improvements in glucose control by allowingfor enhanced effects on 24-h glucose levels, and when used incombination with basal insulin, such as degludec, which alsoyields a 24-h glucose effect, both compounds focus mostly onFPG without having complementary effects, but there mightbe redundant effects on fasting glucose control. This possibi-lity might explain why the decreases in HbA1c and FPG weregreater with liraglutide than with lixisenatide when they were
used alone, but when these compounds were used as a fixed-ratio combination therapy with basal insulin, the efficacy ofHbA1c and FPG levels was comparable between IDegLiratreatment and IGlarLixi treatment, according to the results ofthis meta-analysis.
Second, this finding might be attributable to the insulindosage of the fixed-dose combination therapy. We concludedthat the insulin dosage used in all eight of the trials in thefixed-dose combination group in IGlarLixi treatment wasapproximately 36–46 U/day, and the degludec used inIDegLira treatment was approximately 28–53 U/day. Thedosage of basal insulin between groups was comparable. Wealso conducted meta-regression analysis to evaluate whetherthe HbA1c decrease in the fixed-dose combination therapywas associated with the insulin dosage used in the trials, butthe results indicated no significance. Therefore, the insulindosage used in the fixed-dose combination therapy couldnot explain the above phenomenon.
According to this meta-analysis, the between-group differ-ence in body weight increase was 0.58 kg with significancecompared with GLP-1 RA treatment alone, in favor of IGlarLixitreatment, and the between-group difference in body weightdecrease was 1.24 kg with significance compared with basalinsulin treatment alone, in favor of IDegLira treatment. Theefficacy of body weight decrease between liraglutide treatmentand lixisenatide treatment when used alone has previouslybeen evaluated. According to a previous meta-analysis [31],liraglutide treatment results in a significantly greater decreaseof 2.51 kg in body weight compared with placebo, whereaslixisenatide treatment is associated with a significant weightdecrease of 0.90 kg compared with placebo. When these com-pounds are used as fixed-ratio combination therapy with basalinsulin, the difference in the efficacy of body weight decreasewas minimized between IDegLira treatment and IGlarLixi treat-ment, according to the results of this meta-analysis.
Of course, because this study was a meta-analysis, it hassome limitations. First, in the fixed-ratio combination of basalinsulin and GLP-1 RA treatment, there was only one trialcompared with placebo treatment, whereas the others wereall compared with active hypoglycemic agents as insulintreatment alone or GLP-1 RA treatment alone. Therefore, weused the absolute HbA1c decrease, FPG decrease, and PPGdecrease relative to baseline as parameters for the evaluationof glucose control and compared these absolute changesbetween IGlarLixi treatment and IDegLira treatment for sur-rogates. However, in the analysis of the efficacy of lixisena-tide treatment alone or liraglutide treatment alone, all of theparameters for the evaluation of glucose control were cor-rected by placebo and thus might be considered to occurwithout considering the placebo effect. However, because ofthe limited number of trials and the lack of direct compar-ison studies, this methodology was the only way to comparethe two types of compound treatment. Second, the numberof studies included in this meta-analysis is small, especiallyfor IGlarLixi group. We have researched in the database, butno more study could be included. Therefore, to explain theresults from this meta-analysis, we should be cautious.Further studies are really needed in order to make futuremeta-analysis more robust in terms of efficacy of this drug
1796 X. CAI ET AL.

combination. Third, the baseline variables in each study andthe efficacy of glucose control and body weight change ineach study were used as parameters in this meta-analysisand meta-regression analysis – but not the pooled, patient-level data. So, the higher baseline HbA1c was found to beassociated with greater reduction in HbA1c during intensifi-cation of treatment in some studies, but results from thismeta-regression analysis did not find this correlation. Onereason for this might be associated with the limitation wehave mentioned that data were not the pooled, patient-leveldata. Another reason might be that the reported studieswere all individual studies, and if we pooled all the datatogether, there might get different results. Therefore, resultsfrom this meta-regression analysis did not find the sameresults as previous reported in some individual studies.However, these data are seldom available because most trialsare sponsored by industry. Therefore, we used the para-meters of glucose control and safety in each trial for surro-gates. Fourth, the conclusion from this meta-analysis is basedupon indirect comparisons in absence of head-to-head trialsso that caution is mandatory. In fact, a head-to-head trialwould be of most interest to confirm this hypothesis.Moreover, the high heterogeneity among the studies in thismeta-analysis should be noted. For instance, the comparatorused in the IGlarLixi is always IGlar, whereas the comparatorsused in the IDegLira are heterogeneous. An I2 value >50%represented substantial heterogeneity, and we used a ran-dom-effects model if there was a high level of heterogeneityand performed sensitivity analysis to minimize the effect ofheterogeneity on the results. What is more, the small numberof studies, where all three available studies of IGlarLixi thatwere published by the same group could introduce bias. Andthe limitation of the data we could get as PPG was assessedonly in the IGlarLixi trials, while mean 9-point SMBG wasassessed only in the IDegLira trials. Therefore, the findingsof this meta-analysis should be interpreted with caution.
5. Conclusion
This meta-analysis demonstrated that absolute HbA1c levelsand absolute FPG levels in IGlarLixi treatment and in IDegLiratreatment were significantly lower than baseline levels.Comparisons between IGlarLixi treatment and IDegLira treat-ment indicated no significant differences between groups inthe absolute HbA1c changes or FPG changes relative tobaseline.
Acknowledgments
We thank for Dr. Lingli Zhou, Dr. Yifei Chen, Dr. Ling Chen and Prof.Xueyao Han during the study at Peking University People’s HospitalEndocrinology and Metabolism Department.
Authors’ contributions
LN Ji and XL Cai conceived and designed the systematic review protocol;XY Gao and WJ Yang performed the study selection and data extraction;XL Cai and XY Gao performed the statistical analyses; and XL Cai and LN Jiprepared the manuscript outlines and drafts. All authors contributed to
the critical revision of manuscript drafts, as well as giving final approval forsubmitted manuscript content.
Funding
This paper was not funded.
Declaration of interest
LN Ji has received fees for lecture presentations and for consulting fromAstraZeneca, Merck, Novartis, Lilly, Roche, Sanofi-Aventis, NovoNordisk,Bayer and Takeda. The authors have no other relevant affiliations orfinancial involvement with any organization or entity with a financialinterest in or financial conflict with the subject matter or materials dis-cussed in the manuscript apart from those disclosed. Peer reviewers onthis manuscript have no relevant financial or other relationships todisclose.
References
Papers of special note have been highlighted as either of interest (•) or ofconsiderable interest (••) to readers.
1. Inzucchi SE, Bergenstal RM, Buse JB, et al.; American DiabetesAssociation (ADA); European Association for the Study ofDiabetes (EASD). Management of hyperglycemia in type 2 diabetes:a patient-centered approach: position statement of the AmericanDiabetes Association (ADA) and the European Association for theStudy of Diabetes (EASD). Diabetes Care. 2012;35:1364–1379.
2. Rosenstock J, Schwartz SL, Clark CM Jr, et al. Basal insulin therapy intype 2 diabetes: 28-week comparison of insulin glargine (HOE 901)and NPH insulin. Diabetes Care. 2001;24:631–636.
3. Charbonnel B, Bertolini M, Tinahones FJ, et al. Lixisenatide plusbasal insulin in patients with type 2diabetes mellitus: a meta-analysis. J Diabetes Complications. 2014;28:880–886.
4. Raccah D, Lin J, Wang E, et al. Once-daily prandial lixisenatideversus once-daily rapid-acting insulin in patients with type 2 dia-betes mellitus insufficiently controlled with basal insulin: analysis ofdata from five randomized, controlled trials. J DiabetesComplications. 2014;28:40–44.
5. Riddle MC, Aronson R, Home P, et al. Adding once-daily lixisenatidefor type 2 diabetes inadequately controlled by established basalinsulin: a 24-week, randomized, placebo-controlled comparison(GetGoal-L). Diabetes Care. 2013;36:2489–2496.
6. Seino Y, Min KW, Niemoeller E, et al.; EFC10887 GETGOAL-L AsiaStudy Investigators. Randomized, double-blind, placebo-controlledtrial of the once-daily GLP-1 receptor agonist lixisenatide in Asianpatients with type 2 diabetes insufficiently controlled on basalinsulin with or without a sulfonylurea (GetGoal-L-Asia). DiabetesObes Metab. 2012;14:910–917.
7. Riddle MC, Forst T, Aronson R, et al. Adding once-daily lixisenatidefor type 2 diabetes inadequately controlled with newly initiatedand continuously titrated basal insulin glargine: a 24-week, rando-mized, placebo-controlled study (GetGoalDuo 1). Diabetes Care.2013;36:2497–2503.
8. Maiorino MI, Chiodini P, Bellastella G, et al. Insulin and glucagon-like peptide 1 receptor agonist combination therapy in type 2diabetes: a systematic review and meta-analysis of randomizedcontrolled trials. Diabetes Care. 2017 Apr;40(4):614–624.
•• A recently published meta-analysis has demonstrated the effi-cacy of GLP-1 RA and basal insulin in the form of both free andfixed-ratio combinations.
9. Zinman B, Philis-Tsimikas A, Cariou B, et al.; NN1250-3579 (BEGINOnce Long) Trial Investigators. Insulin degludec versus insulin glar-gine in insulin-naive patients with type 2 diabetes: a 1-year, rando-mized, treat-to-target trial (BEGIN Once Long). Diabetes Care.2012;35:2464–2471.
10. Buse JB, Rosenstock J, Sesti G, et al.; LEAD-6 Study Group.Liraglutide once a day versus exenatide twice a day for type 2
EXPERT OPINION ON PHARMACOTHERAPY 1797

diabetes: a 26-week randomised, parallel-group, multinational,open-label trial (LEAD-6). Lancet. 2009;374:39–47.
11. Marso SP, McGuire DK, Zinman B, et al.; Buse, for the DEVOTE StudyGroup. Efficacy and safety of degludec versus glargine in type 2diabetes. New Eng J Med. 2017.
12. Madsbad S. Review of head-to-head comparisons of glucagon-likepeptide-1 receptor agonists. Diabetes Obes Metab. 2016;18:317–332.
13. Abd El Aziz MS, Kahle M, Meier JJ, et al. A meta-analysis comparingclinical effects of short- or longacting GLP-1 receptor agonistsversus insulin treatment from head-to-head studies in type 2 dia-betic patients. Diabetes Obes Metab. 2017;19;216–227.
14. Aroda VR, Rosenstock J, Wysham C, et al. Efficacy and safety oflixilan, a titratable fixed-ratio combination of insulin glargine pluslixisenatide in type 2 diabetes inadequately controlled on basalinsulin and metformin: the LixiLan-L randomized trial. DiabetesCare. 2016;39:1972–1980.
• This is one trial included in this meta-analysis.15. Rosenstock J, Aronson R, Grunberger G, et al. Benefits of lixilan, a
titratable fixed-ratio combination of insulin glargine plus lixisena-tide, versus insulin glargine and lixisenatide monocomponents intype 2 diabetes inadequately controlled on oral agents: the LixiLan-O randomized trial. Diabetes Care. 2016;39:2026–2035.
• This is one trial included in this meta-analysis.16. Rosenstock J, Diamant M, Aroda VR, et al. Efficacy and safety of
lixilan, a titratable fixed-ratio combination of lixisenatide and insu-lin glargine, versus insulin glargine in type 2 diabetes inadequatelycontrolled on metformin monotherapy: the lixilan proof-of-conceptrandomized trial. Diabetes Care. 2016;39:1579–1586.
• This is one trial included in this meta-analysis.17. Buse JB, Vilsboll T, Thurman J, et al. Contribution of liraglutide in
the fixed-ratio combination of insulin degludec and liraglutide(IDegLira). Diabetes Care. 2014;37:2926–2933.
• This is one trial included in this meta-analysis.18. Gough SC, Bode B, Woo V, et al. Efficacy and safety of a fixed-ratio
combination of insulin degludec and liraglutide (IDegLira) com-pared with its components given alone: results of a phase 3,open-label, randomised, 26-week, treat-to-target trial in insulin-naive patients with type 2 diabetes. Lancet Diabetes Endocrinol.2014;2:885–893.
• This is one trial included in this meta-analysis.19. Lingvay I, Pérez MF, García-Hernández P, et al. Effect of insulin
glargine up-titration vs insulin degludec/liraglutide on glycatedhemoglobin levels in patients with uncontrolled type 2 diabetes:the DUAL V randomized clinical trial. JAMA. 2016;315:898–907.
• This is one trial included in this meta-analysis.20. Linjawi S, Bode B, Chaykin L, et al. Efficacy and safety of IDegLira
(combination of insulin degludec + liraglutide), in insulin-naïvepatients with T2D uncontrolled on GLP-1 receptor agonist (GLP-1RA) therapy. Diabetes. 2015;64(Suppl.1):A255. abstract 1002-P.
• This is one trial included in this meta-analysis.21. Rodbard HW, Bode BW, Harris SB, et al. Safety and efficacy of insulin
degludec/liraglutide (IDegLira) added to sulphonylurea alone or tosulphonylurea and metformin in insulin-naive people with type 2diabetes: the DUAL IV trial. Diabet Med. 2017;34:189–196.
• This is one trial included in this meta-analysis.22. Zinman B, Gerich J, Buse JB, et al. Efficacy and safety of the human
glucagon-like peptide-1 analog liraglutide in combination withmetformin and thiazolidinedione in patients with type 2 diabetes(LEAD-4 Met+TZD). Diabetes Care. 2009;32:1224–1230.
23. Vilsboll T, Zdravkovic M, Le-Thi T, et al. Liraglutide, a long-actinghuman glucagon-like peptide-1 analog, given as monotherapy sig-nificantly improves glycemic control and lowers body weight with-out risk of hypoglycemia in patients with type 2 diabetes. DiabetesCare. 2007;30:1608–1610.
24. Vilsboll T, Brock B, Perrild H, et al. Liraglutide, a once-daily humanGLP-1 analogue, improves pancreatic B-cell function and arginine-stimulated insulin secretion during hyperglycaemia in patients withtype 2 diabetes mellitus. Diabetic Med. 2008;25:152–156.
25. Davies MJ, Bergenstal R, Bode B, et al. Efficacy of liraglutide forweight loss among patients with type 2 diabetes: the SCALE dia-betes randomized clinical trial. JAMA. 2015;314:687–699.
26. Pinget M, Goldenberg R, Niemoeller E, et al. Efficacy and safety oflixisenatide once daily versus placebo in type 2 diabetes insuffi-ciently controlled on pioglitazone (GetGoal-P). Diabetes ObesMetab. 2013;15:1000–1007.
27. Fonseca VA, Alvarado-Ruiz R, Raccah D, et al. Efficacy and safety ofthe once-daily GLP-1 receptor agonist lixisenatide in monotherapy:a randomized, double-blind, placebo-controlled trial in patientswith type 2 diabetes (GetGoal-Mono). Diabetes Care.2012;35:1225–1231.
28. Kapitza C, Forst T, Coester HV, et al. Pharmacodynamic character-istics of lixisenatide once daily versus liraglutide once daily inpatients with type 2 diabetes insufficiently controlled on metfor-min. Diabetes Obes Metab. 2013;15:642–649.
29. Nauck M, Rizzo M, Johnson A, et al. Once-daily liraglutide versuslixisenatide as add-on to metformin in type 2 diabetes: a 26-weekrandomized controlled clinical trial. Diabetes Care. 2016;39:1501–1509.
30. Meier JJ, Rosenstock J, Hincelin-Méry A, et al. Contrasting effectsof lixisenatide and liraglutide on postprandial glycemic control,gastric emptying, and safety parameters in patients with type 2diabetes on optimized insulin glargine with or without metfor-min: a randomized, open-label trial. Diabetes Care.2015;38:1263–1273.
31. Cai X, Ji L, Chen Y, et al. Comparisons of weight changes betweenSGLT2 inhibitors treatment and GLP-1 analogs treatment in type 2diabetes patients: a meta-analysis. J Diabetes Investig. 2017;8:510–517.
1798 X. CAI ET AL.















![Basal Insulin and Combinations - jjdi.com€¦ · v Actions/Uses of Basal Insulin Basal insulin (NPH, glargine [U-100 and U-300], detemir, degludec U-100, U-200) • Controls fasting](https://img.pdfslide.us/doc/110x75/5b15fceb7f8b9a472e8c4f1d/basal-insulin-and-combinations-jjdicom-v-actionsuses-of-basal-insulin-basal.jpg)













