Embed Size (px)
Citation preview
ORIGINAL ARTICLE
Comparative test of radiologicalexposure between femoral andradial techniques, development ofa protective device and clinical trialdesign
Igor R C Bienert,1,2 Pedro B Andrade,1,2 Fabio S Rinaldi,2
Fernanda D T Vilela,1 Paulo A Silva,1 Joao C S Braga,1 Paulo H Waib,3
Alexandre Rodrigues,1 Fábio V G Filho,1 Katashi Okoshi4
1Interventional CardiologyDepartment, FAMEMA—MariliaState School of Medicine, SãoPaulo, Brazil2Interventional CardiologyDepartment, Santa Casa deMisericórdia de Marília, SãoPaulo, Brazil3Clinical Physiology Department,FAMEMA—Marilia State Schoolof Medicine, São Paulo, Brazil4Clinical Cardiology Department,UNESP—São Paulo StateUniversity, Botucatu MedicalSchool, São Paulo, Brazil
Correspondence toDr Igor R C Bienert, Dept.Hemodinamica, Hospital dasClinicas de Marilia, 1° andar R.Aziz Atallah / SN, Fragata,Marilia / SP, 17519–101, Brazil;[email protected]
Received 9 February 2015Accepted 16 May 2015Published Online First9 June 2015
To cite: Bienert IRC,Andrade PB, Rinaldi FS, et al.BMJ Innov 2015;1:103–110.
ABSTRACTBackground Interventional procedures via radialtechnique have progressively increased due toimproved patient comfort, lower complicationrates and reduced mortality in some scenarios.One area of interest is radiation exposure andways of minimising it. Most studies focus onpatient radiation risk with conflicting results, butthere is reasonable consensus for increasedoperator exposure from the radial technique. Theaim of this study was to evaluate radiologicalexposure under controlled radial and femoralaccess simulation tests, mapping radiation pathsand developing a radiological protection devicefor the transradial technique.Methods and results Radiation exposure wassimulated under controlled conditions forfemoral and radial techniques using a pressurisedionisation chamber and water phantom.Different measurement points were definedaccording to standard positions to simulateradiation received by the operator in the gonads,thyroid and eyes at different angles during realprocedures. The radial technique increased totalexposure by 33% over the femoral technique. Aprotective device was developed and tested afterradiation mapping. The protective device reducedcumulative radiation by 52% against the radialand 36% against the femoral technique.Conclusions In our study, operator exposure tocumulative ionising radiation was higher fromthe radial technique and the protective devicereduced radiation exposure levels in the radialand femoral techniques. These results providedthe basis for a clinical trial design to betterdefine the impact of the protection device and
radiation exposure during real world practiceusing different interventional techniques.Trial registration number http://www.clinicaltrials.gov. Unique identifier:NCT02200783.
INTRODUCTIONInterventional cardiology has, at its core,procedures using invasive vascular access.Of the strategies used, brachial dissectionis of historical significance being the firsttechnique used, and the current most fre-quent access route is the modifiedSeldinger Technique1 via femoral arterypuncture. Materials and strategies thatreduce vascular complications in invasivecoronary procedures have recently beenadded to the toolbox, especially theradial technique, which is a potentialalternative to the femoral technique.2
Some of the advantages of radial accessare lower bleeding and vascular complica-tion rates,3–5 with further reductions inhospitalisation6 and mortality in somehigher risk patient subgroups,5 7 8 and ithas increasingly been adopted all over theworld,9 with possible consideration as theroutine approach strategy of choice.9 10
Radiation risk and access routeThere are two well-known general pat-terns of damage related to ionising radi-ation: the deterministic and stochasticeffects. Deterministic effects cause celldeath that is not compensated for byreplacement or repair, with detectable
MEDICAL DEVICES
Bienert IRC, et al. BMJ Innov 2015;1:103–110. doi:10.1136/bmjinnov-2015-000043 103
group.bmj.com on March 13, 2018 - Published by http://innovations.bmj.com/Downloaded from

tissue or organ damage. It is an all-or-nothing effectwhere there is a dose threshold below which the lossof cells is insufficient to cause detectable harm.Examples are dry skin desquamation and erythaemafor doses between 3 and 5 Gy and necrosis over50 Gy. There is also a time lag, with effects generallyoccurring after 3–4 weeks. Stochastic effects arecaused by random cell damage where probability isproportional to received radiation dose without anythreshold. Of these effects, the oncological risk11 is ofconcern as the latency period after exposure can beover 40 years,12 and ways to minimise radiation havebeen afforded increasing attention.13 14
A concern arising from this context where radial tech-niques benefit patient clinical outcome, is the increasedpotential for ionising radiation exposure,15 as it canbecome a technique limitation. On average, a coronaryangiography and angioplasty correspond to patient radi-ation exposure levels of 300 and 1000 radiographs,respectively.16 Several randomised studies have exam-ined differences between radial and femoral techniquesrelated to this topic; most of their data infer higherfluoroscopy time, but without significance when com-pared to radiation dose absorbed by the patient derivedfrom the access route.17 18 The literature is relativelyscarce when focusing on operator exposure. However,there seems to be some consensus on higher exposurefrom radial access; though there is little standardisationof radiation impact assessment methods. Perhaps themain limitation of these studies is that most are of obser-vational design and few were planned using dosimetersspecifically dedicated to evaluating operator absorbeddose in accordance with access choice.19 20
Radioprotective devicesThe default optimal radiation protection set includesa radioprotection apron, a thyroid collar, lead goggles,
a vinyl lead curtain in the lower region of the cath-eterisation table and a suspended moveable glassshield. Such a set is widely used and effective in pro-tecting the operator from 95% of the radiation towhich he or she is exposed.21
Additional devices have been developed to reduceoperator exposure; these include radiation protectionsheets22 and extensor tables23 with lower shieldscovered with lead sheets, which are generally success-ful, with levels of reduction up to 30%. However,their adoption is not widespread; this may be due totechnical difficulties in their use. This opens up anarea of research and development for new technolo-gies to reduce interventionist ionising radiation expos-ure and even facilitate radial procedure performance.The Transradial Intervention Table Protection
(TRIPTable) device (patent required) is a polycarbon-ate support table anatomically-designed for the radialtechnique, facilitating puncturing, standardisingsequential technique steps, providing material supportand allowing radioprotection from a protective layerdesigned to block radiation without obstructingfluoroscopic images (figure 1).
OBJECTIVEThe objective of this study is to analyse the differencesin radiation from simulated femoral and radial routes,focusing on impact to the operator during interven-tional cardiology procedures, and aimed at developingradioprotective devices specifically for the radialtechnique.
MATERIALS AND METHODSThe study has been approved by Institutional EthicalCommittee and written informed consent wasobtained to take part in the study.
Radiological testA radiological field test was performed in a catheter-isation laboratory by simulating operator positionusing a fluoroscopy station (Philips Allura XperFD20) in a 2700 field with standard below-and-abovetable protection apparatus (superior protection glassand curtain, the first angled at 45° and positioned tocontact the lower skirt). Radiation levels were mea-sured by an external independent company using aVictoreen 450P ionisation chamber pressurised to6 atm, and a water phantom to simulate the humanbody. The acquisition sequence was performedaccording to five projections. A zero projection(cranial-caudal and zero lateral angulations) followedby angled projections at 30° to the four directions(cranial, caudal, left and right). The measuring pointswere grouped into three different simulations: radialposition with standard support (Philips standard catharm support NCVA097), and radial position with aTRIPTable device and femoral position. The femoralprojection was defined by the operator in a working
Figure 1 Transradial Intervention Table Protection (TRIPTable)device side-mounted on the table.
MEDICAL DEVICES
104 Bienert IRC, et al. BMJ Innov 2015;1:103–110. doi:10.1136/bmjinnov-2015-000043
group.bmj.com on March 13, 2018 - Published by http://innovations.bmj.com/Downloaded from

position 30 cm caudally distant from the radial pos-ition and 30 cm frontal distance from the table.Each position (radial, femoral and TRIPTable)
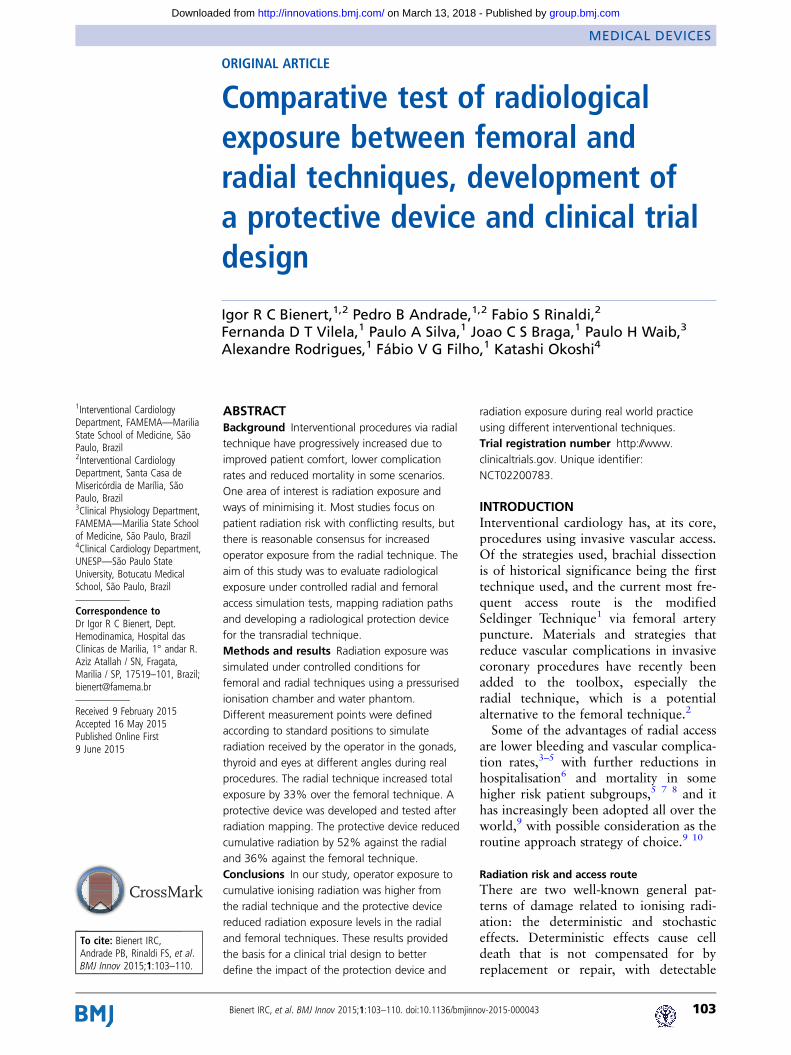
received three standardised points aiming at the eyes,thyroid and gonads (1.70, 1.30 and 0.80 m high,respectively). The X-ray tube default georeset positionwas set at 50 cm above ground and the table 40 cmfrom the tube. The flat panel was positioned 30 cmabove the table. The controlled test predefined posi-tions are shown in figure 2. Shield positioning dia-grams are shown in figures 3 and 4.
RESULTSThere were differences between groups in level ofradiation directed at the operator. Levels according tosimulated technique are shown in figure 5 and table 1(according different angulations) and by projectionand measurement sites in figure 6.Femoral radiation proportion was defined by the
formula: (specified projection−femoral projection)/femoral projection×100; this can be seen in table 2.Total radiation exposure was 33% higher by radialtechnique than femoral technique. Cumulative expos-ure incidence was 52% lower than the radial tech-nique and 36% lower than the femoral techniquewhen the TRIPTable device was used.
DISCUSSIONIn our study, the simulated radial technique exposedthe operator to the highest cumulative dose of ionis-ing radiation; the protective device reduced radiationexposure levels in the radial and femoral techniques.These results provide a basis for a clinical trialdesigned to better define the impact of operator radi-ation exposure during real world clinical practice.
TRIPTable trial designOur study hypothesis is that using the radial accessprotective device TRIPTable is not inferior to thestandard femoral technique, and is superior to thestandard radial technique as a radioprotection strategyfor the operator, in patients with acute coronary syn-dromes submitted to cardiac catheterisation. This is aprospective, 1:1:1 randomised, unicentric study com-paring the femoral and radial techniques, with andwithout a TRIPTable device (NCT02200783). Theprimary endpoint will be assessed immediately afterinterventional procedure termination. The secondaryand safety end points will be recorded after interven-tional procedure termination at time of hospital dis-charge. The possibility of bias derived from theHawthorne effect is a major concern. Thus, a rando-mised historical cohort between radial and femoraltechniques, with identical inclusion and exclusion cri-teria, will be the subject of a comparative analysis(ARISE study—NCT01653587).24
OutcomesPrimary outcome: accumulated operator radiationdose received during interventional cardiology proce-dures measured by thermoluminescent dosimeters.Secondary outcomes: accumulated radiation dose
received by each measured site (gonads, thyroid andeyes), operator radiation dose according to linear cor-relation for total dose area product, and proceduresuccess rate, defined by performing the procedurewithout needing to cross between techniques.
Patient populationPatients admitted are those with moderate to high riskacute coronary syndrome and scheduled for earlyinvasive stratification strategy by coronary angiog-raphy followed by percutaneous coronary intervention(PCI), if applicable. Patients will be evaluated in termsof the feasibility of the radial and femoral access pro-cedures. After evaluation, a patient meeting all inclu-sion criteria and no exclusion criteria may be includedin study after signing the free and informed consentform.
ProcedureProcedures will be performed according to currentguidelines, including adjunctive antithrombotic andanticoagulant pharmacotherapy. Operators participat-ing in the study should have performed at least 350diagnostic or therapeutic procedures in the last yearby transradial approach for radial experience qualifi-cation.10 Operators will be equipped with the full setof personal radiation protection in all procedures,including lead aprons, thyroid protective collar, leadgoggles, and upper and lower table shields, all with atleast 0.5 mm Pb equivalent protection.
Eligibility criteriaInclusion criteria▸ Unstable angina with an indication for invasive
stratification▸ Acute coronary syndrome without ST-segment elevation▸ Acute coronary syndrome with ST-segment elevation▸ Patient informed of the nature of the study and has
signed the informed consent▸ Patient suitable for coronary angiography and coronary
intervention either by radial or femoral access
Exclusion criteria▸ Less than 18 years old▸ Pregnant▸ Chronic use of vitamin K antagonists, direct thrombin
inhibitors, or factor Xa antagonists▸ Active bleeding or high risk of bleeding (severe hepatic
insufficiency, active peptic ulcer disease, creatinine clear-ance <30 mL/min, platelet count <100 000 mm3)
▸ Uncontrolled hypertension (persistent systolic bloodpressure >180 mm Hg)
▸ Cardiogenic shock
MEDICAL DEVICES
Bienert IRC, et al. BMJ Innov 2015;1:103–110. doi:10.1136/bmjinnov-2015-000043 105
group.bmj.com on March 13, 2018 - Published by http://innovations.bmj.com/Downloaded from
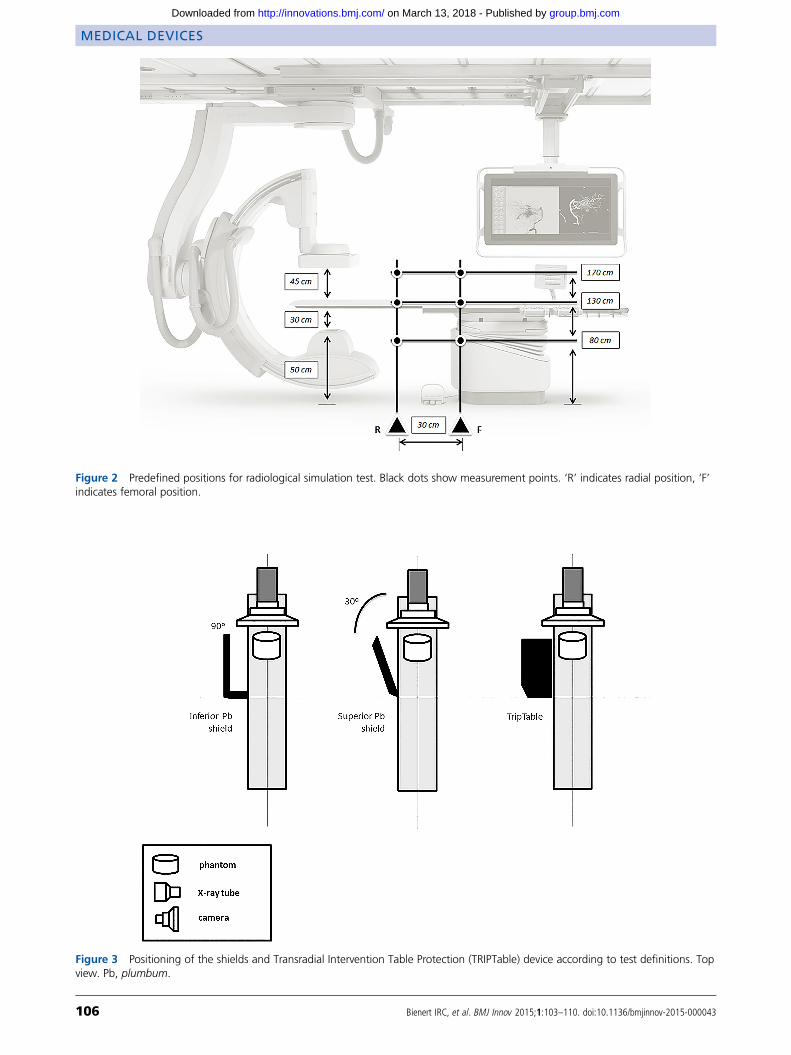
Figure 2 Predefined positions for radiological simulation test. Black dots show measurement points. ‘R’ indicates radial position, ‘F’indicates femoral position.
Figure 3 Positioning of the shields and Transradial Intervention Table Protection (TRIPTable) device according to test definitions. Topview. Pb, plumbum.
MEDICAL DEVICES
106 Bienert IRC, et al. BMJ Innov 2015;1:103–110. doi:10.1136/bmjinnov-2015-000043
group.bmj.com on March 13, 2018 - Published by http://innovations.bmj.com/Downloaded from
▸ Previous coronary artery bypass graft surgery with theuse of ≥1 graft
▸ Patients not suitable for any of the specified vascularaccess routes
▸ Concomitant severe disease with life expectancy lessthan 12 months
▸ Medical, geographical or social conditions that impedeparticipation in the study
▸ Refusal or inability to understand and sign the informedconsent form
Statistical analysisThe primary study hypothesis is that the use of thedevice is not inferior to the femoral technique in
terms of operator radiation exposure and not inferiorto the standard radial technique in terms of successrate and patient radiological exposure. The analysiswas defined as for ‘intention to treat’, which meansthere is no need for the operator to change the dosim-eter, whether the diagnostic procedure or angioplastyis completed, but only to record the type of procedureultimately performed.To balance procedure data and avoid additional
technique biases (eg, short-duration vs long-durationprocedures, projection angle, incorrect operator
Figure 4 Positioning of the shields and Transradial Intervention Table Protection (TRIPTable) device according to test definitions.Lateral view. Pb, plumbum.
Figure 5 Accumulated radiation levels achieved in differentsimulated techniques. RAO 30: right anterior oblique 30°angulation. LAO 30: left anterior oblique 30° angulation.
Table 1 Radiation exposure in different techniques andmeasurement points according to angulations
Technique 0°/0°Cranial30°
Caudal30°
LAO30°
RAO30°
Femoral*
Gonads 500 101 1020 2200 500
Thyroid 1290 91 1730 1210 1090
Eyes 230 14.2 135 280 131
Radial*
Gonads 1550 240 3300 3300 1490
Thyroid 1100 200 360 950 320
Eyes 810 13.7 148 164 96
TRIPTable*
Gonads 500 199 1380 2100 1300
Thyroid 102 22 199 420 162
Eyes 47 11.2 48 122 84
*Measurements in mSV/h.LAO, Left anterior oblique; RAO, Right anterior oblique.
MEDICAL DEVICES
Bienert IRC, et al. BMJ Innov 2015;1:103–110. doi:10.1136/bmjinnov-2015-000043 107
group.bmj.com on March 13, 2018 - Published by http://innovations.bmj.com/Downloaded from

positioning), primary study outcome will be cumula-tive dose in each set of dosimeters. In prespecified sec-ondary analysis we will also quantify the totalradiation received at each specific operator site.Sample size was estimated on the primary end point
(total radiation received by the operator as measuredcumulatively in all dosimeters: gonads, thyroid andeyes). Considering cumulative analysis of the primaryoutcome, sample size is calculated for the number ofdosimeters required, rather than the number of proce-dures. Previous randomised prospective studies19 25
that have compared the radial and femoral techniqueshave shown an average increase in radiation receivedby the operator of 61.3% in PCI when using the
transradial approach. Another study_ENREF_1818
evaluating chest radiation between radial and femoralapproaches showed an average operator absorption of20.9±13.8 mSv in the radial procedure and 15.3±10.4 mSv in the femoral procedure (p<0.001). Toanalyse a hostile scenario with a SD of 13.8 and6.45 mSv difference, we calculated a 72 dosimetersample (24 patients per group) for 80% power and96 dosimeters per group for a 90% power with an αerror of 0.05. As three dosimeters are being evaluatedper patient, we estimate 32 subjects for each arm ofthe study. In order to facilitate comparison with anexternal database, we obtained a 99 subject sample.Categorical variables will be expressed as frequency
and percentage, and compared using the χ2 or Fisherexact tests. Continuous variables will be expressed asmean and SD, or median and IQR when appropriate,and compared with the Student t test. Linear regres-sion will be used to estimate the relation betweentotal radiation dose and operator-received radiationwith the three different techniques. In all tests, theresults will be considered significant when p value<0.05.
CONCLUSIONIn our study, we found an increased radiation exposurelevel using radial technique compared to femoral tech-nique. The TRIPTable device reduced operator-directed radiation exposure under controlled simula-tion conditions compared to both techniques. There
Figure 6 Radiation levels by each projection and simulated technique. RAO 30: right anterior oblique 30° angulation. LAO 30: leftanterior oblique 30° angulation.
Table 2 Radiation exposure according to femoral proportion
Technique0°/0°(%)
Cranial30° (%)
Caudal30°(%)
OAE30° (%)
OAD30° (%)
Radial*
Gonads +210 +138 +224 +50 +198
Thyroid −15 +120 −79 −21 −71Eyes +252 −4 +10 −41 −27Mean +149 +85 +51 −4 +34
TRIPTable*
Gonads 0 +97 +35 −5 +160
Thyroid −92 −76 −88 −65 −85Eyes −80 −21 −64 −56 −36Mean −57 0 −39 −42 +13
*Measurements in mSV/h.
MEDICAL DEVICES
108 Bienert IRC, et al. BMJ Innov 2015;1:103–110. doi:10.1136/bmjinnov-2015-000043
group.bmj.com on March 13, 2018 - Published by http://innovations.bmj.com/Downloaded from

are some limitations to the analysis. This is a singlecentre simulated study and requires external validationbefore further conclusions may be drawn. Additionally,in real world situations, multiple variables can influ-ence the protection of the operator and may consider-ably interfere with radiological exposure.
Impact on daily practiceOur results suggest that there is increased operatorradiation exposure with the radial technique com-pared to the femoral technique. A protective devicecould help to decrease this. The TRIPTable trial mayhelp to better define the impact of radiation exposureduring daily clinical practice.
Study statusEnrolment was initiated in July 2014 and, up toFebruary 2015, 62 patients had been included. Theinclusion phase is expected to last through the firsthalf of 2015.
Acknowledgements The authors wish to express their gratitudeto Professor Paulo Craveiro of the physics and radiotherapydepartment (in memoriam), who was unrestrictedly helpful andoffered invaluable assistance, support and guidance. Theauthors are deeply saddened by the passing of Professor PauloCraveiro, a master of the radiation field, and as its discoverers,victim of its harmful effects. Without his knowlege this workwould not be possible. Thank you very much Professor.
Contributors Professor Paulo Craveiro (in memoriam) initiatedthe study design and provided physics research expertise.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Institutional Ethical Committee.
Provenance and peer review Not commissioned; internally peerreviewed.
REFERENCES1 Seldinger SI. Catheter replacement of the needle in
percutaneous arteriography; a new technique. Acta Radiol1953;39:368–76.
2 Campeau L. Percutaneous radial artery approach for coronaryangiography. Cathet Cardiovasc Diagn 1989;16:3–7.
3 Agostoni P, Biondi-Zoccai GG, de Benedictis ML, et al. Radialversus femoral approach for percutaneous coronary diagnosticand interventional procedures; Systematic overview andmeta-analysis of randomized trials. J Am Coll Cardiol2004;44:349–56.
4 Jolly SS, Amlani S, Hamon M, et al. Radial versus femoralaccess for coronary angiography or intervention and the impacton major bleeding and ischemic events: a systematic review andmeta-analysis of randomized trials. Am Heart J2009;157:132–40.
5 Jolly SS, Yusuf S, Cairns J, et al. Radial versus femoralaccess for coronary angiography and intervention inpatients with acute coronary syndromes (RIVAL): arandomised, parallel group, multicentre trial. Lancet2011;377:1409–20.
6 Roussanov O, Wilson SJ, Henley K, et al. Cost-effectivenessof the radial versus femoral artery approach to
diagnostic cardiac catheterization. J Invasive Cardiol2007;19:349–53.
7 Romagnoli E, Biondi-Zoccai G, Sciahbasi A, et al. Radialversus femoral randomized investigation in ST-segmentelevation acute coronary syndrome: the RIFLE-STEACS(Radial Versus Femoral Randomized Investigation inST-Elevation Acute Coronary Syndrome) study. J Am CollCardiol 2012;60:2481–9.
8 Mehta SR, Jolly SS, Cairns J, et al. Effects of radial versusfemoral artery access in patients with acute coronarysyndromes with or without ST-segment elevation. J Am CollCardiol 2012;60:2490–9.
9 Rao SV, Cohen MG, Kandzari DE, et al. The transradialapproach to percutaneous coronary intervention: historicalperspective, current concepts, and future directions. J Am CollCardiol 2010;55:2187–95.
10 Hamon M, Pristipino C, Di Mario C, et al. Consensusdocument on the radial approach in percutaneouscardiovascular interventions: position paper by the EuropeanAssociation of Percutaneous Cardiovascular Interventions andWorking Groups on Acute Cardiac Care** and Thrombosis ofthe European Society of Cardiology. EuroIntervention2013;8:1242–51.
11 Roguin A, Goldstein J, Bar O, et al. Brain and neck tumorsamong physicians performing interventional procedures. Am JCardiol 2013;111:1368–72.
12 Bashore TM. Radiation safety in the cardiac catheterizationlaboratory. Am Heart J 2004;147:375–8.
13 Christopoulos G, Papayannis AC, Alomar M, et al.Effect of a real-time radiation monitoring device onoperator radiation exposure during cardiac catheterization: theradiation reduction during cardiac catheterization usingreal-time monitoring study. Circ Cardiovasc Interv2014;7:744–50.
14 Agarwal S, Parashar A, Ellis SG, et al. Measures to reduceradiation in a modern cardiac catheterization laboratory.Circ Cardiovasc Interv 2014;7:447–55.
15 Kim KP, Miller DL. Minimising radiation exposure tophysicians performing fluoroscopically guided cardiaccatheterisation procedures: a review. Radiat Prot Dosimetry2009;133:227–33.
16 Venneri L, Rossi F, Botto N, et al. Cancer risk fromprofessional exposure in staff working in cardiaccatheterization laboratory: insights from the National ResearchCouncil’s Biological Effects of Ionizing Radiation VII Report.Am Heart J 2009;157:118–24.
17 Achenbach S, Ropers D, Kallert L, et al. Transradial versustransfemoral approach for coronary angiography andintervention in patients above 75 years of age. CatheterCardiovasc Interv 2008;72:629–35.
18 Lange HW, von Boetticher H. Reduction of operator radiationdose by a pelvic lead shield during cardiac catheterization byradial access: comparison with femoral access. JACCCardiovasc Interv 2012;5:445–9.
19 Michael TT, Alomar M, Papayannis A, et al. A randomizedcomparison of the transradial and transfemoral approaches forcoronary artery bypass graft angiography and intervention: theRADIAL-CABG Trial (RADIALVersus Femoral Access forCoronary Artery Bypass Graft Angiography and Intervention).JACC Cardiovasc Interv 2013;6:1138–44.
20 Sandborg M, Fransson SG, Pettersson H. Evaluation ofpatient-absorbed doses during coronary angiography and
MEDICAL DEVICES
Bienert IRC, et al. BMJ Innov 2015;1:103–110. doi:10.1136/bmjinnov-2015-000043 109
group.bmj.com on March 13, 2018 - Published by http://innovations.bmj.com/Downloaded from
intervention by femoral and radial artery access. Eur Radiol2004;14:653–8.
21 Chambers CE, Fetterly KA, Holzer R, et al. Radiation safetyprogram for the cardiac catheterization laboratory. CatheterCardiovasc Interv 2011;77:546–56.
22 Politi L, Biondi-Zoccai G, Nocetti L, et al. Reduction ofscatter radiation during transradial percutaneouscoronary angiography: a randomized trial using alead-free radiation shield. Catheter Cardiovasc Interv2012;79:97–102.
23 Behan M, Haworth P, Colley P, et al. Decreasing operators’radiation exposure during coronary procedures: the transradial
radiation protection board. Catheter Cardiovasc Interv2010;76:79–84.
24 de Andrade PB, LA EM, Tebet MA, et al. Design and rationaleof the AngioSeal versus the Radial approach In acute coronarySyndromE (ARISE) trial: a randomized comparison of avascular closure device versus the radial approach to preventvascular access site complications in non-ST-segment elevationacute coronary syndrome patients. Trials 2013;14:435.
25 Lange HW, von Boetticher H. Randomized comparison ofoperator radiation exposure during coronary angiography andintervention by radial or femoral approach. CatheterCardiovasc Interv 2006;67:12–16.
MEDICAL DEVICES
110 Bienert IRC, et al. BMJ Innov 2015;1:103–110. doi:10.1136/bmjinnov-2015-000043
group.bmj.com on March 13, 2018 - Published by http://innovations.bmj.com/Downloaded from
clinical trial designdevelopment of a protective device andbetween femoral and radial techniques, Comparative test of radiological exposure
Fábio V G Filho and Katashi OkoshiPaulo A Silva, Joao C S Braga, Paulo H Waib, Alexandre Rodrigues, Igor R C Bienert, Pedro B Andrade, Fabio S Rinaldi, Fernanda D T Vilela,
doi: 10.1136/bmjinnov-2015-0000432015 1: 103-110 originally published online June 9, 2015BMJ Innov
http://innovations.bmj.com/content/1/3/103Updated information and services can be found at:
These include:
References http://innovations.bmj.com/content/1/3/103#ref-list-1
This article cites 25 articles, 3 of which you can access for free at:
serviceEmail alerting
box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in the
CollectionsTopic Articles on similar topics can be found in the following collections
(29)Medical devices (5)Epidemiologic studies
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on March 13, 2018 - Published by http://innovations.bmj.com/Downloaded from