-
7/28/2019 comparative skeletal structure.pdf
1/12
Comparative SkeletalStructureClinton Rubin, State University of
New York, Stony Brook, New York, USA
Mani Alikhani,State University of New York, Stony Brook, New
York, USA
Janet Rubin, Emory University, Atlanta, Georgia, USA
The sophisticated organization of the skeleton achieves a
structure that can withstand the
extremes of functional load-bearing. The growth, development and
repair of the
skeletal structure is realized through the tightly regulated
remodelling of bone tissue,
orchestrated by cells that specifically form or resorb the
matrix.
Bone
Bone is a highly specialized form of connective tissue that
provides an internal support system and facilitateslocomotion.
The first vertebrates appeared on Earth inthe Ordovician period,
some 500 million years ago, andsince that time bone has evolved to
become a complexliving tissue in which the extracellular matrix is
miner-alized, conferring marked rigidity and strength to
theskeletonwhilestillmaintaining some degree of elasticity.
Inaddition to understanding the palaeontological record, thestudy
of bone is important because diseases of the skeleton,such as
osteoporosis, are major health concerns that affecttens of millions
of people. Clearly, an improved under-standing of the basic science
of bone will provide atremendous opportunity to develop novel
approaches to
treat and reverse these crippling diseases.Bone regulates its
mass and architecture to meet two
critical and competing responsibilities: one structural,
theother metabolic. In the first case, the skeleton protects
vitalorgans of the cranial and abdominal cavities; it encloses
theblood-forming elements of the bone marrow, and facil-itates
locomotion. Second, the skeleton serves as a mineralreservoir that
contains 99% of the bodys total calcium,85% of its phosphorus, and
66% of its magnesium keyelements for the function of the
organism.
Bone is a composite material comprised of a mineralizedmatrix
interspersed with an organic scaffold consistingprimarily of
collagen. There are three different cell types
found in the bone tissue: osteoblasts, which form
bone,osteocytes, which maintain bone, and osteoclasts, whichare
multinucleated giant cells responsible for the resorp-tion of bone.
As a structure, bone possesses severalremarkable attributes, with
high tensile and compressivestrength similar in magnitude to that
of cast iron, while, atthe same time, being a relatively
lightweight material, andthus efficient during movement.
Bone, as an idealized structural material, can readily
beappreciated by considering the forces and impact involved
during the gallop of a thoroughbred racehorse. The canobone
(third metacarpal, towards the foot of the front limbwith a
cross-sectional area of approximately 2.5 cm omineralized tissue,
successfully holds up an animaweighing 500 kg and travelling at
about 50 km per houYet, with all its strength, hardness and
resilience, bone isdynamic living material, constantly being
renewed anreconstructed throughout the lifetime of the
individuaIndeed, bone is the only tissue in the body that has
thcapacity to heal without forming a scar. Bone even has thability
to adapt its structure relative to its functionademands,
exemplifying the paradigm of form followfunction. In the positive
direction, this plasticity
evidenced by the 40% more bone in the professional tennplayers
serving arm compared with the arm that simplthrows the ballintothe
air. Onthe negative side, there is thdrastic osteoporosis that
results from long-term spacflight, creating a significant hurdle to
extended exploratioof space.
The structural success of skeletal morphology can bexamined
effectively at various levels: by its gross anatomand functional
responsibility, by its ultrastructural morphology (cortical or
cancellous), by its microscopiorganization (lamellar or woven) and
on the basis of itdevelopment and repair, processes achieved
througendochondral ossification or intramembranous ossifica
tion.
Macroscopic Structure of Bone
On the basis of their gross appearance, bones are
typicallclassified as either long or flat. Long bones include
thbones of the axial skeleton (e.g. tibia, femur, radius, ulnand
humerus); flat bones include the skull bones pluthe sternum,
scapula and pelvis. Each long bone can b
Article Contents
Introductory article
. Bone
. Macroscopic Structure of Bone
. Microscopic Organization
. Bone Cells
. Composition of Bone Matrix
. Development of the Skeleton
. Modelling and Remodelling
. Mechanical Properties of Bone
. Cartilage
. Ligament
. Tendon
. Summary
ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Macmillan Publishers
Ltd, Nature Publishing Group / www.els.net
-
7/28/2019 comparative skeletal structure.pdf
2/12
divided into three distinct anatomical areas. The regionat the
end of a long bone is called the epiphysis. Themetaphysis is the
area just beneath the epiphysis, wherethe bone becomes more
slender. The long shaft of thebone is the diaphysis.
Characteristic of all bones are a dense outer sheet ofcortical
bone (alternatively referred to as cortical bone)
and a central medullary cavity, which is filled with eitherred
or yellow bone marrow. The marrow cavity isinterrupted throughout
its length, particularly in theepiphyseal and metaphyseal regions,
by a reticular net-work of trabecular bone (alternatively referred
to ascancellous or spongy bone). These internal trabeculae actas
well-banded reinforcement rods, or internal scaff-olding, to
buttress the outer compact bone as it becomesmore slender at the
articulating surfaces. Despite thedifferences in their appearance,
under the microscopecortical and trabecular bone can be seen to
have the samebasic histological structure (Figure 1).
Surrounding every compact bone is an osteogenic
connective tissue membrane, the periosteum, whichconsists of two
distinct layers. The inner layer, adjacentto the actual bone
surface, consists of osteoblasts andtheir precursors, as well as a
rich microvasculature.The outer layer, which is more fibrous, gives
rise tothe Sharpey fibres that penetrate the bone matrix,
bindingthe periosteum to bone and aiding in anchoringtendons,
ligaments and muscles to the bone. A singlelayer of bone cells, a
syncitium referred to as theendosteum, covers the internal surface
of bone. Theendosteum, considerably thinner than the
periosteum,physically separates the bone surface from the
bonemarrow within. The principal functions of periosteum
and endosteum are nutrition of osseous tissue andprovision of a
continuous supply of new osteoblasts forrepair or growth of
bone.
Microscopic Organization
At the microscopic level, bone can be generalized into
twspecific morphologies: the disorganized, hypercellulawoven bone,
and the highly organized, relatively hypocelular, lamellar bone.
Woven bone is the first bone tissue temerge in embryonic
development as well as the fir
mineralizing tissues to appear in repair process such afracture
healing. Woven bone has an irregular, disorganized pattern of
collagen orientation and osteocytdistribution, indicative of the
rapid manner in which it ilaid down. While woven bone is
characteristic of embryonic development and early stages of repair;
it is also founin the healthy adult skeleton at ligament and
tendoinsertions. Woven bone also is evident in specific
diseasstates which affect local bone sites such as osteogenisarcoma
or metastatic cancerous lesions. It serves a criticawound-healing
role by rapidly filling osseous defects, callus that provides the
initial continuity for fractures anosteotomy segments. Within a few
weeks of bein
deposited, woven bone is most often reabsorbed anreplaced during
remodelling by lamellar bone. It is thihighly orchestrated process
of repair and remodelling thaallows bone fractures to repair
without leaving a scar.
Lamellar, or mature, bone characteristically showcollagen fibres
arranged in lamellae (37 mm thick) thaare parallel to one another
or concentrically organizearound a vascular canal. The whole
complex of concentrilamellae, or plates, of bone that surround a
canal containing blood vessels, nerves and loose connective tissue,
icalled an osteon (Figure 2). Osteons are typically 200300mm in
diameter, consisting of up to 20 lamellar plateWithin these
mineralized plates are lacunae, small lake
that house osteocytes, the cells residing within the bontissue.
To provide added tensile strength, each lamellconsists of collagen
fibres organized such that they arparallel to one another.
Importantly, the orientation of thcollagen in adjacent lamellar
plates is distinct from that oits neighbour, adding tremendous
strength to the composite material, a strategy similar to that used
in plywood tadd rigidity. The arrangement of the collagen
matri(Figure 3) ultimately determines the orientation of the
bonmineral crystals. Mineralization proceeds and extends ovethe
collagen matrix, with the long axis of the hydroxyapatite crystal
parallel to the collagen fibre, a process that alsadds strength to
the tissue.
In addition to concentric lamellae, two other type olamellae are
recognized. Circumferential lamellae enclosthe entire bone, forming
its outer perimeter. Interstitialamellae are interspersed between
adjacent concentrilamellae and fillthe spaces between them. They
are actuallfragments of preexisting concentric lamellae, or
remnantof the early stages of woven bone.
An osteon that has formed de novo is recognized as primary
osteon. If an osteon is established within thcortex via bone
resorption, a process that succeeds i
Figure 1 Bone can be categorized into two morphological
components:cortical andcancellous bone. Thedensecortical bone
envelopesthe entire
structure,while cancellousor trabecularboneis typicallyfound
towardsthe ends of the bone. The internal spaces of bone are filled
with marrow.Reprinted, with permission, from Lynch SE, Genco RJ and
Marx RE (1999)
Tissue Engineering: Applications in Maxillofacial Surgery and
Periodontics.Quintessence.
Comparative Skeletal Structure
2 ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Macmillan
Publishers Ltd, Nature Publishing Group / www.els.net
-
7/28/2019 comparative skeletal structure.pdf
3/12
replacing preexisting bone tissue, it is referred to as
asecondary osteon, or haversian system. The bulk of bonetissue
within the adult human is haversian, as it has been
remodelled and replaced over the lifetime of the skeleton.In the
adult skeleton, when bone tissue needs to be
repaired or replaced, it undergoes a processof remodelling.Bone
remodelling is an intricate, interdependent, highlyorchestrated
process thatbegins by the removal of tissue byosteoclasts and the
tightly coupled replacement of tissue byosteoblasts. In the adult
skeleton, approximately 5% of theskeleton is constantly involved in
bone remodelling, or theturnover of bone tissue.
Bone Cells
Bone is composed, in essence, of four different cell
types:osteoblasts, osteoclasts, osteocytes and the
bone-liningcells. Osteoblasts, osteocytes and bone-lining cells
origi-nate from local osteoprogenitor cells, whereas
osteoclastsarise from the fusion of mononuclear precursors,
whichoriginate in the various haemopoietic tissues.
Osteoprogenitor cells develop from embryonic me-senchymal stem
cells and are able to proliferate anddifferentiate into
chondroblasts(cartilage-forming cells) or
osteoblasts, dependent on local factors such as cytokinesThese
osteoprogenitor cells persist throughout postnatalife and arefound
on or near all of the free surfaces of bonesuch as the inner layer
of the periosteum or the endosteumOsteoprogenitor cells are most
active during the growtand development of bones but are reactivated
in adult lifin the repair of bone fractures, and when adaptive
o
remodelling processes stimulate the need for bone formation.
Osteoblasts and osteocytes are thought to bincapable of division.
Thus, as the population of osteoblasts depletes, they are replaced
by proliferation andifferentiation of the osteoprogenitor
cells.
Osteoblasts
Osteoblasts (Figure 3) are mononucleated cells, derivefrom the
mesenchyme, that synthesize both collagenouand noncollagenous bone
proteins, which all togethemakes up the organic matrix of bone
called the osteoid
Embryonic undifferentiated mesenchymal cells can givrise to
cartilage, bone, muscle cells or adipocytedependent on the
influence of hormones and growtfactors. Osteoblasts are connected
to one another viextended cell processes that are interconnected
via gajunctions, establishing a single continuous blanket of cellon
the bone surface, all of which are in direct communication with
neighbouring cells.
The active osteoblast is a plump cuboidal cell with
aeccentrically placed or polarized nucleus, which resideaway from
that part of the cell nearest to the mineralizesurface. The
cytoplastic elements of the osteoblast includabundant endoplasmic
reticulum, a well developed Golg
body, and numerous free ribosomes that are responsiblfor the
basophilia seen in sections stained with haematoxylin and
eosin.
In bone remodelling, osteoblasts are transiently active asites
of reformation of bone. These features help tdistinguish
osteoblasts from the mesenchymal precursor(preosteoblasts), which
are also found on bone surface(Figure 4). These bone-lining cells
are flattened spindleshaped cells with oval nuclei and few
organelles. Bonelining cells cover bone surfaces, particularly in
the aduskeleton, that are quiescent in terms of bone formation
anresorption. In certain circumstances, such as when exposeto
growth factors or other anabolic stimuli, theyproliferat
and differentiate into osteoblasts.The osteoblastic lineage
comprises several cells a
different stages of differentiation, including osteoprogentor
cells, preosteoblasts and osteoblasts according to thprogressive
expression of markers of the osteoblasphenotype. Preosteoblasts
express markers such as alkaline phosphatase, osteopontin and
collagen type I, whereamature postmitotic osteoblasts express
osteocalcin.
A temporal sequence of expression of genes encodinosteoblast
phenotype markers has defined three distinc
Figure 2 Diagram depictinga section of thecorticalshaft of a
long bone,showing the arrangement of the lamellae in the osteons,
the interstitial
lamellae, and the outer and inner circumferential lamellae. The
outersurfaceis protectedby theperiosteum, whilethe innersurfaceis
covered bythe endosteum. Within the cortical shell, the branching
out of thebuttressing trabeculae can be seen. Reprinted, with
permission, from
Bloom W and Fawcett DW (1986) A Textbook of Histology, 11th
edn.Saunders.
Comparative Skeletal Structure
ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Macmillan Publishers
Ltd, Nature Publishing Group / www.els.net
-
7/28/2019 comparative skeletal structure.pdf
4/12
periods: a growth period (proliferation), a period of matrix
development and a mineralization period. A period ofactive
proliferation is reflected by mitotic activity withexpression of
cell cycle and cell growth-regulated genes(e.g. histone, c-myc,
c-fos and AP-1 (alkaline phosphatase)activity). During this
proliferation period, and fundamen-tal to development of the bone
cell phenotype, severalgenes associated with formation of the
extracellular matrix(type I collagen, fibronectin and transforming
growthfactor (TGF) b) are actively expressed, and these proteinsare
ultimately key to maintaining the intricate balancebetween bone
formation and resorption.
In bone, type I collagen, a heterotrimer of one a2 (I) andtwo a1
(I) chains,makes up about 90% of the total organic
matrix. It is the collagen, with its organization, thatprovides
a great deal of the tensile strength of bone.Therefore, even subtle
variations in the composition orcontent of the collagen can have
devastating effects. Forexample, mutations in the gene coding for
the a1 (I) chain,as well as mutations in the gene coding for the a2
(I) chain,can cause osteogenesis imperfecta, an affliction that
makesbone very susceptible to fracture.
Immediately after the downregulation of osteoblastproliferation
reflected by the decline in deoxyribonucleic
acid (DNA) synthesis and histone gene expression, th
expression of alkaline phosphatase, a protein associatewith the
bone cell phenotype, increases greater than 10fold. During this
period the extracellular matrix undergoea series of modifications
in composition and organizatiothat facilitate the mineralization of
the matrix. The onset omineralization is also signalled by the
induction of severaother genes, such as osteopontin and
osteocalcin.
It is likely that differentiation along the osteoblalineage
involves osteoblast-specific transcription factor(OSFs) that have
yet to be identified. OSF2 is a cis-actinelement in the promoter of
themouse osteocalcin gene thabinds a factor present only in nuclear
extracts oosteoblasts and confers osteoblast-specific activity.
Severa
studies have indicated that Osf2/Cbfa1 is encoded by thgene for
Cbfa1. Mutation in OSF2/CBFA1 canresultinthabnormal skeletogenesis
seen in cleidocranial dysplasiand transgenic mice who have Cbfal
knocked out arunable to ossify their cartilaginous skeletons.
In addition to secreting several matrix componentincluding type
I collagen, proteoglycans, osteocalcinosteonectin and osteopontin,
osteoblasts also producgrowth factors that have important autocrine
and paracrine effects on bone growth and remodelling (Figure 4
Figure3 Bone may be categorized into
threemicrostructuralcomponents: (1) bone cells, whichinclude
osteoblasts,osteocytesand osteoclasts(stainewith a modified Goldner
trichrome stain); (2) an organic matrix consisting of collagenous
and noncollagenous factors, such as the bone morphogenetproteins
(the mineralizedmatrixhas been removed andcells have been coloured
green to distinguish them from theorganic framework);(3) an
inorgan
component consistingprimarily of calcium andphosphate; this
componenthas beenstylizedas an arrayof hexagonalcrystals.Reprinted,
withpermissiofrom Lynch SE, Genco RJ and Marx RE (1999) Tissue
Engineering: Applications in Maxillofacial Surgery and
Periodontics. Quintessence.
Comparative Skeletal Structure
4 ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Macmillan
Publishers Ltd, Nature Publishing Group / www.els.net
-
7/28/2019 comparative skeletal structure.pdf
5/12
They also have surface receptors for a variety of
hormones,vitamins and cytokines, which influence their activity.
Asthe osteoblasts produce osteoid, they often becomeengulfed in
their own matrix and differentiate intoosteocytes.
Osteocytes
The osteocyte (Figure 3) is a mature osteoblast entrappedwithin
the bone matrix, and is now believed to be largelyresponsible for
maintaining the viability of the tissue. Notonly can osteocytes
sense alterations in physical orchemical conditions (and thus
orchestrate the recruitmentof osteoblasts and osteoclasts), it has
been recentlydemonstrated that these cells can both synthesize
andresorb matrix, thus modifying their own immediatephysical and
chemical environment.
Osteocytes reside in lacunae within the matrix and are11by far
the most abundant cells of mature bone. As
osteoblasts become entombed in their own matrix anddifferentiate
into osteocytes, the cells diminish in size andlose many parts of
their cytoplasmic organelles. Withineach osteon, osteocytes are
connected to each other vialong, slender, branched cytoplasmic
processes and gapjunctions. These cytoplasmic extensions pass
through anetwork of catacombs, called canaliculi, which
connectadjacent lacunae. These interconnecting canaliculi areideal
pathways for chemical, electrical and stress generatedfluid
communication through the dense bone matrix.
Osteocytes express cellcell channels called connexinthrough
which small molecules such as second messengercan pass, suggesting
that networks of osteocytes are iintricate communication with one
another.
Considering the skeletons ability to adapt to changes iits
functional environment, it is important to consider th
means by which the bone tissue can perceive and responto
mechanical signals. Given their preponderance in bonand their
intricate three-dimensional network, osteocyteare most probably the
key mechanosensor element in boneLoading of bone results in strain,
or deformation, in thmatrix. This deformation may evoke cellular
responseeither directly or indirectly via fluid shear stress
produceby increased fluid flow in the lacunocanalicular system
oelectrical strain potential. Osteocytes may orchestrate thoverall
remodelling response by secreting key factors, sucas
prostaglandins, nitric oxide and insulin-like growtfactors (IGFs).
These, and certainly other yet unknowfactors, activate the bone
remodelling system of osteo
blasts and osteoclasts, and thus demonstrate the balancbetween
bone forming and resorbing cells.
Recent evidence suggests that osteocytes can metabolcally
manipulate their environment more or less independent of surface
resorption and accretion. This ability iimportant to the cellular
regulation of calcium exchangMost of the bone crystals, buried away
from the endosteaand periosteal bone surfaces, appear to be
unavailable teffect the necessary mineral exchange with
extracellulafluid, making it difficult to explain the immediate
exchang
Macrophage
Monocyticprecursor CFU-M
Hematopoeticstem cell(CFU-GM)
Osteoclast
Resorption pit
Osteoclast precursors
Osteoblasts
Osteoblastprecursors
Bone and bone matrix
+ Resorption
BMPs
Growth factorsInterleukins
+ Formation
RANKL
MCSFInterleukins
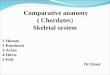
Figure 4 Osteoclasts (red) and osteoblasts (dark green) interact
through cytokines released into the bone micromilieu. Macrophages
secrete
macrophage colony-stimulating factor (MCSF), various
interleukins and tumour necrosis factor, all of which promote
osteoclast differentiation fromhaematopoietic stem cells, from the
colony forming unit for granulocyte-macrophages (CFU-GM) and the
CFU-M (CFU for macrophage) to terminal
osteoclast phenotype. Osteoblasts interact by expressing factors
which affect osteoclasts, mainly RANKL and MCSF, as well as factors
affecting bonemineralization and progression of theirown phenotype,
such as insulin-likegrowthfactors and basicfibroblast growth
factors. Importantly, disusewill als
upregulate osteoclast activity, while increases in mechanical
factors will elevate bone formation.
Comparative Skeletal Structure
ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Macmillan Publishers
Ltd, Nature Publishing Group / www.els.net
-
7/28/2019 comparative skeletal structure.pdf
6/12
of bone mineral with the extracellular fluid. There is,however,
a vast surface area on the Haversian canal andlacunar walls, and an
even larger area on the canalicularwalls,where bone mineral
exchange with extracellular fluidcan takeplace. Nevertheless,when
major reorganization ofbone tissue is called for, the bone
resorption is performedby the osteoclast.
Osteoclasts
Osteoclasts (see Figure 3) are the major resorptive cells ofbone
and are characterized by their large size and multiplenuclei. They
are specialized monocyte/macrophage familymembers that
differentiate from haematopoietic precur-sors. Whereas monocytes
are mononuclear cells, osteo-clasts form from the fusion of
monocytes. Terminaldifferentiation in this lineage is characterized
by theacquisition of mature phenotypic markers, such as
thecalcitonin receptor, tartrate-resistant acid phosphatase
(TRAP), morphological conversion into large multinu-cleated
cells, and the capacity to form resorption lacunaeon bone.
An osteoclast is a strongly polarized cell with a paucityof
rough endoplasmic reticulum, a moderate number ofribosomes,
numerous smooth vesicles, and well developedmitochondria. These
cells occupy shallow concavities,called Howship lacunae, which are
created by the erosiveaction of the osteoclast on the underlying
bone. Osteoclaststypically attach only to fully mineralized bone
matrix, andare not able to resorb bone that is not fully
mineralized.The osteoclast has three different domains: ruffled
border,sealing zone and smooth basolateral border. The ruffled
border is the central, highly infolded area of the
plasmamembrane where secretion for bone resorption takes
place.Osteoclasts appearing some distance from the surface ofbone
do not have ruffled bordersand are called inactive orresting
osteoclasts. The sealing zone is a microfilament-rich,
organelle-free area of the plasma membrane thatsurrounds the
ruffled border and serves as the point ofanchoring of the
osteoclast to the underlying bone matrixachieved by integrin
attachment. This sealing zone createsa closed subosteoclastic
compartment, or pocket, betweenthe cell and bone that permits a
confined space subject toresorption. Osteoclasts not only attach to
the bone: theycan move along the surface, thus increasing their
range of
action. During the movement of the osteoclast, the sealmust
remain intact in order for resorption to continue.
Once activated, osteoclasts resorb bone by isolating anarea of
bone under the region of cell attachment. Theosteoclasts then
actively reduce the pH of the localenvironment by production of
hydrogen ions through thecarbonic anhydrase system. The lowered pH
increases thesolubility of the apatite crystals, in essence
dissolving themineral. After the mineral is removed, the
organiccomponents of the matrix are hydrolysed through acidic
proteolytic digestion. The reconstruction of bone requireseven
to ten generations of osteoblasts to follow and fill thresorption
space. Absence of osteoclasts, or a populatioof dysfunctional
osteoclasts, leads to osteopetrosis, omarble bone disease, which
can be fatal in childhoodDevoid of osteoclasts, the development of
bone througendochondral ossification fails to create a marrow
cavity
thereby eliminating the space necessary for the productioof all
haematopoietic elements.
Many factors are involved in regulating osteoclarecruitment from
marrow precursors. Two factors predominate: MCSF and RANKL. MCSF is
necessary tsupport proliferation, early differentiation and
survival othe monocytic progenitors of osteoclasts. Loss of
MCSaction engenders deficiencies in both osteoclast anmacrophage
recruitment, as well as differentiation. MCSalone is unable to
generate osteoclasts in in vitro culturesystems; further
progression into the osteoclast lineagrequires the presence of
RANLK which binds to RANKreceptors on the monocytic precursors,
inducing lat
differentiation and fusion. Expression of RANKL on thsurfaceof
bone stromaland osteoblast cells is controlledbhormones that
regulate calcium balance, such as PTH anvitamin D. Increased PTH
causes increased expression oRANKL, leading to increased
osteoclastogenesiRANKL can also be expressed on lymphocytes and
mabe responsible for hypercalcaemia associated with
haematopathologic diseases. Bone cells also secrete a proteicalled
osteoprotegerin (OPG), which serves as a decoreceptor for RANKL,
preventing its action on monocytiprogenitors. Overexpression of OPG
is thus associatewith decreased bone turnover. Many other factors
arcapable of regulation of osteoclast formation, including c
fos, a ubiquitous nuclear transcription factor whosabsence
prevents late osteoclast differentiation, and TNFawhich can support
osteoclastogenesis even in the absencof RANKL.
Systemic factors such as vitamin D, parathyroihormone and tumour
necrosis factor can enhance thdevelopment of osteoclasts from
haematopoietic progentor cells in the presence of stromal elements
from bonelargely by up-regulating bone expression of RANKL, bualso
affecting cytokines such as the interleukins. Togethethe
osteoblasts, osteoclasts and osteocytes work togetheto lay down,
maintain and remodel the bone matrix.
Composition of Bone Matrix
The composite structure of bone allows it to withstancompressive
and tensile stresses, as well as bending antorsional moments. The
inorganic phase of bone, withydroxyapatite crystals arrayed in a
protein matrixprovides the ability to resist compression.
Individuacalcium phosphate crystals of multiple sizes are
imbedde
Comparative Skeletal Structure
6 ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Macmillan
Publishers Ltd, Nature Publishing Group / www.els.net
-
7/28/2019 comparative skeletal structure.pdf
7/12
in and around the fibrils of the collagen type I
lattice.Hydroxyapatite crystal, while effectively resisting
com-pressive loads, has a poor ability to withstand tensile
loads.As in concrete, a material that excels at resisting
compres-sion but is poor in resisting tension, tensile elements
(e.g.steel reinforcing rods) are added to create a
compositematerial that can cope with complex loading environ-
ments. As discussed, in the case of bone, this tensilestrength
arises from collagen fibrils organized intolamellae.
The collagen orientation between adjacent lamellae canrotate by
as much as 908, permitting the tissue to resistforces and moments
acting from several different direc-tions, much like the added
strength in plywood realized bythe distinct orientation of the
fibres in each specific ply.While the ultrastructural organization
is, to a certainextent, defined by the genome, the functional
environmentalso contributes to the distribution of lamellae, as
well asthe osteons that house them. This directed deposition
ofcollagen adds to the anisotropy of the bone. Given that
more than 80% of functional strains are due to bending(and thus
a high percentage of strain is tensile), thestructural quality of
the bone may ultimately be deter-mined by the quality of the
collagen and the organizationof the microarchitecture. Recent
studies have shown thatcollagen itself deteriorates with age, and
undoubtedlycontributes to the declining material properties of
theskeleton.
Before its calcification, newly synthesized bone matrix
isessentially completely organic and is called osteoid.Collagen
type I is the predominant organic component inbone, accounting for
approximately 94% of the unminer-alized matrix. Collagen fibres are
embedded in a ground
substance which is rich in proteoglycans, chondroitinsulfate,
keratan sulfate and hyaluronic acid. Other non-collagenous proteins
most often found in bone are found inosteoid, and account for
approximately 4% of its weight.These include glycoproteins and
phosphoproteins such asosteonectin; sialoproteins, which are
predominantly os-teopontin; bone Gla protein, also called BGP
(bonegamma-carboxyglutamic acid-containing protein) or
os-teocalcin; and bone morphogenetic protein. Extracts ofbone also
include enzymes, hormones, growth factors andother metabolites
essential for bone metabolism. It is eventhought that many of these
molecules serve as couplingfactors, which, when released from the
bone matrix during
osteoclastic resorption, serve to stimulate recruitment
anddifferentiation of osteoblasts.
The inorganic component of bone (see Figure 3) iscomposed
principally of a calcium phosphate mineralanalogous to crystalline
calcium hydroxyapatite, Ca10(-PO4)6(OH)2. This crystallite
structure is available for theexchange of ions. Thus magnesium and
sodium cansubstitute in the calcium position, fluoride and
chloridein the hydroxyl position, and carbonate in both thehydroxyl
and phosphate positions. These small amounts
of impurities in hydroxyapatite may alter certain
physicaproperties of the crystal, such as solubility. For
examplefluoride substitution decreases the solubility of the
crystalites, whereas carbonate increases it. Many
investigatorbelieve that the impurities of the crystalline matrix
arcritical to enabling the osteoclast to resorb the tissue.
Development of the Skeleton
Skeletal development requires the exquisite coordinatioof many
distinctive cell types and the orchestration of thecellular growth,
differentiation, apoptosis, production oextracellular matrix and
remodelling. Formation of thskeleton (ossification) occurs by
either a direct (intramembranous) or an indirect (endochondral)
process. Intramembranous ossification occurs during
embryondevelopment by the direct transformation of mesenchymacells
into osteoblasts. The first event of this process is th
migration of undifferentiated mesenchymal cells into aarea
destined to become bone. Mesenchymal cells condense, the
surrounding tissue becomes vascularized, ancells differentiate
directly into osteoblasts. Intramembranous ossification begins in
the centre of the mesenchymacell concentration. The osteoblasts
then synthesize thosteoid in which hydroxyapatite crystals are
formed bcalcium and phosphate ion enrichment. Collagen molecules
secreted by the osteoblasts during embryonic bondeposition
polymerize extracellularly to form numerourandomly oriented fibrils
throughout the trabeculae. Thearly intramembranous bone, in which
the collagen fibrerun in all directions, is described as woven
bon
Intramembranous ossification occurs primarily in thneurocranium
(which forms a protective case around thbrain) and viscerocranium
(which forms the skeleton of thface) and part of the clavicle.
In endochondral ossification, the condensed embryonimesenchyme
transforms first into a cartilage anlage (population of cells that
constitutes the beginning of tissue), which reflects both the
position and form of theventual bone at that site. During mouse
embryondevelopment the undifferentiated cells initially
expresmesenchymal matrix (e.g. collagen types I and III)
bugradually, cells in the central region dramatically changtheir
phenotype and become large and round. As thes
prechondrocytes differentiate further, their cytoplasmvolume,
endoplasmic reticulum and Golgi complex increase and they switch
from the production of mesenchymal matrix to the production of
cartilaginous matrix (e.gcollagen types II, IX, XI and matrix Gla
protein) anseveral other matrix proteins. These chondrocytes
theundergo a programme of differentiation, which
includehypertrophy, expression of type X collagen and
decreaseexpression of type II collagen. The cartilage anlage
growrapidly through appositional and interstitial growth, an
Comparative Skeletal Structure
ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Macmillan Publishers
Ltd, Nature Publishing Group / www.els.net
-
7/28/2019 comparative skeletal structure.pdf
8/12
resembles the future bone in shape, but, as it grows in size,the
cartilage anlage becomes too big to support thechondrocytes purely
through diffusion, and the hyper-trophic cells begin to die off and
ossify.
Through endochondral ossification, cells from theperichondrium
differentiate into osteoblasts and begin todeposit a thin layer of
bone, appearing as a collar, around
the cartilage (Figure 5). Concurrently, mononuclear
cells(monocytes) differentiate into chondroclasts, which beginto
break down the ossifying cartilage. From the perichon-
drium, the invasion of vascular channels begins, a keprocess
called angiogenesis. As the hypertrophic chondrocytes continue to
die through apoptosis, the osteoblasbrought in by the blood vessels
start the process odepositing bone tissue just as if bone were
forming on thsurface of adult bone. The development of bone
througendochondral ossification, therefore, allows the rapi
expansion of a bone template, through both interstitiaand
appositional growth. This swelling could not occur ithe tissue was
originally bone, as the mineralized matrirestricts growth only to
surfaces. The replacement of thdying cartilage with mineralizing
bone, however, allowskeleton to fulfil its responsibilities as a
calcium reservoand a weight-bearing structure.
Mineralization of bone tissue
The mineralization of bone begins approximately 101
days after the organic osteoid matrix has been laid downAt this
point,mineral increases almost immediately to 70%of the ultimate
content, whereas deposition of the fina30% takes several months.
While the actual process omineralization is not completely
understood, it is believethat two mechanisms are involved. The
first involves structure called the matrix vesicle, and the second
heterogeneous nucleation.
Matrix vesicles are small, round, extracellular lipidbilaminar
bound organelles, which bud from hypertrophichondrocytes or
osteoblasts undergoing the process oapoptosis as well as from cell
processes originating fromthe plasma membrane. There is a definite
polarity to th
vesicles, with mineralization occurring in a predictable
anorganized way adjacent to the requisite phosphatases othe inner
leaflet of the membrane. The matrix vesiclecontain high levels of
alkaline phosphatase, adenosintriphosphatase (ATPase), inorganic
pyrophosphatase, 5nucleotidase and ATP-pyrophosphohydrolase, in
additioto phospholipids (especially phosphatidylserine), whichave a
strong affinity for calcium ions. It is believed thathese ions
accumulate in the matrix vesicle because of theaffinity for the
phospholipids and a membrane-bouncalcium pump. At a point of
supersaturation, nucleation othe mineral begins.
Alkaline phosphatase, a biosynthetic product of osteo
blasts, is present in very high concentrations durindevelopment
and osteoid production. The regulatory rolof this disulfide-linked
dimer is not known, but its presencmay increase the local
concentration of P (phosphate) anthereby facilitate hydroxyapatite
deposition. Increasinthe concentration of P in the micromilieu
exceeds the locasolubility product and catalyses deposition along
the inneleaflet of the vesicle. Following this accretion,
thdestruction of the vesicles membrane has been attributeto an
increasing concentration of lysophospholipids withi
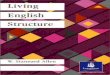
Figure 5 Development of a long bone as shown in longitudinal
sections(AJ), and in cross-sections A, B, C and D. Pale blue is
cartilage; purple,
calcified cartilage;black,bone; red,arteries.A, The original
cartilagemodel
of thebone; B, a periosteal collarof bone appears beforeany
calcification ofcartilage occurs; C, cartilage begins to calcify;
D, vascular mesenchyme
enters the calcified cartilage and divides it into two zones of
ossification (Eand F); G, blood vessels and mesenchyme penetrate
the epiphysealcartilage and the epiphyseal ossification centre
develops within it; H, a
similar ossification centredevelopsin
thelowerepiphysealcartilage; as theboneceases to growin length,
thelower epiphyseal platedisappears first(I)
and then the upper epiphyseal plate (J). The marrow cavity then
becomescontinuousthroughoutthe lengthof thebone, andthebloodvessels
of thediaphysis, metaphyses and epiphyses intercommunicate.
Reprinted, with
permission, from Bloom W andFawcettDW (1986) A Textbook of
Histology,11th edn. Saunders.
Comparative Skeletal Structure
8 ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Macmillan
Publishers Ltd, Nature Publishing Group / www.els.net
-
7/28/2019 comparative skeletal structure.pdf
9/12
the matrix vesicles, which suggests that vesicles areprogrammed
to self-destruct.
Following dissolution of the matrix vesicle membrane,the
hydroxyapatite crystals are exposed to the extravesi-cular
environment, where additional mineral accretes tothe newly formed
crystal. The crystal is then believed tomove chemotactically toward
and to bind preferentially at
the gap between collagen fibrils, precipitated by the
nestingosteonectin and fibronectin. Mineralization proceeds
andextends over the collagen matrix, with the long axis of
thehydroxyapatite crystal parallel to the collagen fibre.
In the second mechanism, apatite crystallites aredeposited in
the gap zones at the ends of collagenmolecules, where the mineral
first appears. Initially, thesegaps are filled with proteoglycans,
which bind to calcium.The proteoglycans are removed enzymatically,
leavingbehind the calcium. At next step, phosphoproteins bind tothe
collagen. Dephosphorylation of the phosphoproteins(as a result of
alkaline phosphatase activity) provides theadditional phosphate
ions for nucleation and crystal
growth.
Modelling and Remodelling
Both trabecular and cortical bone grow, change andturnover
through two fundamentally distinct mechanisms:modelling and
remodelling. Bone modelling typicallyrefers solely to the
deposition of new bone without boneresorption. Bone remodelling, in
contrast, is a specific,coupled sequence of resorption and
formation events thatreplaces previously existing bone. As this
constant turn-
over and replenishment of damaged tissue is critical toretaining
bone strength, it is clear that disruption of theseprocesses
through age and disease will ultimately compro-mise the structural
viability of the skeleton.
The mechanism for internal remodelling of denscompact bone is
via axially oriented cuttingfillincones. The cuttingfilling cone
has a front of osteoclastthat bore through the bone, followed by a
tail oosteoblasts that coordinately lay down osteoid and begithe
formation of the new secondary osteon (Figure 6A group of
osteoblasts, osteocytes and osteoclasts tha
are linked and participate in remodelling (activationresorption
and formation) of a discrete area of bonis called a bone modelling
unit (BMU). Traumatic osurgical wounds usually results in an
intense, bulocalized, modelling and remodelling response.
Thprocess, referred to as a regional acceleratory phenomeno(RAP),
is an important aspect of the postoperativhealing process. In
contrast, the slow but persistenremodelling of adult bone involves
approximately 5%of skeleton at any given time, progressing
througactivation of a resting site, resorption of the bone,
reversaof the process finishing with formation to fill in thpocket
of excavated bone (ARRF).
Both modelling and remodelling are controlled ban interaction of
metabolic and mechanical signalBone modelling is patterned by
temporal expressioof structural genes followed by the integrated
biomechanical control of functional applied loads. Howevehormones
and other metabolic agents have a stronsecondary influence,
particularly during growth anadvanced ageing. Paracrine and
autocrine mechanismsuch as local growth factors and prostaglandins,
arcapable of temporarily overriding the mechanicacontrol mechanism
during wound healing. Remodellinresponds to metabolic mediators
such as parathyroihormone and oestrogen, primarily by varying the
rat
of bone turnover. Certainly, a combination of mechanicasignals,
such as duration, magnitude and distribution oloads, also influence
remodelling and the form anfunction of bone.
Osteoblastsform new bone
Resorptioncavity
Advancedfilling cone
Completedsecondary osteon
2 1
Figure 6 The cuttingfilling cone has a head of osteoclasts that
cut through the bone, and a tail of osteoblasts that form a new
secondary osteon. Th
velocity through boneis determined by measuring between two
tetracycline labels (1 and 2) administered 1 weekapart. Reprinted,
withpermission, froGraber T and Vanarsdall RL (2000) Orthodontics:
Current Principles and Techniques, 3rd edn. Mosby.
Comparative Skeletal Structure
ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Macmillan Publishers
Ltd, Nature Publishing Group / www.els.net
-
7/28/2019 comparative skeletal structure.pdf
10/12
Mechanical Properties of Bone
Bone, as an organ, needs to be both stiff (to resistdeformation)
and tough (to prevent crack propagation).However, there is a
compromise between these twoobjectives, as they are attained
through a balance betweenthe resiliency to crack propagation
provided by collagen
and the resiliency to deformation provided by mineral. Fornormal
tensile or compressive loading, the stiffness of thematerial, or
elastic modulus, for human haversian bone isapproximately 17.0 GPa
(gigapascals, or 109 pascals) in thelongitudinal direction, 11.5
GPa in the transverse directionand 3.3 GPa in shear. The degree of
mineralization (youngbone) or porosity (old bone) compromises the
stiffness ofthe bone and thereby lowers the elastic modulus.
However,the effective modulus of the bone can compensate
fordecreased stiffness through changes in morphology, suchas the
periosteal expansion seen with ageing.
Bone tissue has the capacity to adapt to its
functionalenvironment. Theterm adaptive bone remodelling refers
to
changes in bone mass and geometry in response to analteration in
the bones mechanical environment. The mostfamiliar examples are
increased bone mass with certainkinds of exercise (such as jumping
or tournament-leveltennis playing) and bone loss following disuse
(such as bedrest or space flight-induced disuse).
Although vertebrate design and function are diverse, atthe level
of small volumes of tissue all loads and bendingmomentsresolve into
strain.Strain, a dimensionless unit ofchange in length divided by
its original length, is used inbone physiology as 102 6 strain, or
microstrain. The yieldstrain of bone, or the degree of deformation
at which thebone does not recover elastically, is approximately
7000
microstrain; that is, a 0.7% change in length causesirreversible
damage to the tissue. Ultimate strain in bone,or the degree of
deformation at which the material actuallyfractures, is 15 000
microstrain.
Strain generated in long bones by vigorous activityrarely exceed
peaks of 3000 microstrain, indicating a safetyfactor to failure of
approximately 23-fold. The similarityin peak strain magnitude of
20003500 microstrain hasbeen called dynamic strain similarity, and
suggests thatskeletalmorphology and locomotion character combine
toelicit a very specific and perhaps beneficial levelof strain.
Itis also important to emphasize that the great majority ofstrain
elicited in bone is due to bending (4 85%).
Therefore, assumption that skeletal elements are subjectsolely
to compression must be approached with caution.
Although the nature of this structurefunction relation-ship is
only poorly understood, it has been proposed thatbone remodelling
is continually influenced by the level anddistribution of the
functional strains within the bone.Alteration in bone mass,
turnover and internal replace-ment are sensitive to changes in the
magnitude, distribu-tion and rate of strain generatedwithin the
bone tissue. Forexample, static load applied continuously on
bone
produces an effect on remodelling activity that is ndifferent
from that produced by disuse. For a loadinregimen to be anabolic,
it must be dynamic in nature; statloads do not influence bone
morphology. In parallel witstudies trying to identify
pharmacological agents to inhibthe bone loss that follows the
menopauseor ageingprocesseveral investigators are attempting to
define exercis
studies or mechanical interventions that will serve as
stronanabolic agents to resist osteoporosis.
Cartilage
Cartilage is a special type of connective tissue which has stiff
and firm, but not hard, extracellular matrix. Icontrast to bone,
cartilage is neither vascular nor calcifiedCartilage provides three
basic functions. It gives flexiblsupport in appropriate anatomical
places (the nasal tip, ealobe, thoracic cage, tracheal rings); it
is a pressure-toleranextremely low friction tissue located in
specific skeleta
areas where direct pressure and articulation occur (e.gsurfaces
of bones); and it functions as a site of rapid growtin conjunction
with many bones undergoing elongation.
Cartilage consists of cells called chondrocytes, and aextensive
extracellular matrix composed of fibres anground substance.
Chondrocytessynthesize and secrete thextracellular matrix, and the
cells themselves are located imatrix cavities, called lacunae, just
as in bone. It is thextracellular matrix with its embedded fibres
that not onlgives cartilageits resiliency, but also allowsit to
bearweighand to achieve considerable tensile strength.
Collagenhyaluronic acid, proteoglycans and small amounts oseveral
glycoproteins are the principal macromolecule
present in all types of cartilage matrix. Cartilage has
nvasculature, lymphatic network or innervation of its
ownChondrocytes are nourished by diffusion of oxygen annutrition
through the matrix from blood vessels located isurrounding
connective tissues. Because diffusion is thonly source for oxygen
and nutrition, the maximum widtof the cartilage is limited.
However, vessels may pasthrough cartilage without supplying it
directly.
Cartilage, like bone, derives from the mesenchyme. Thfirst
modification observed is the rounding up of thmesenchymal cells,
which retract their extensions, multiplrapidly, and form
mesenchymal condensations. The celformed by this direct
differentiation of mesenchymal cell
are called chondroblasts. Synthesis and deposition of thmatrix
then begin to separate the chondroblasts from onanother. The
differentiation of cartilage takes place fromthe centre outward;
therefore, the more central cells havcharacteristics of
chondrocytes, while the peripheral celare typical chondroblasts.
The growth of cartilage attributable to two processes: interstitial
growth, resultinfrom the mitotic division of preexisting
chondrocytes, anappositional growth, resulting from the
differentiation operichondrial cells.
Comparative Skeletal Structure
10 ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Macmillan
Publishers Ltd, Nature Publishing Group / www.els.net
-
7/28/2019 comparative skeletal structure.pdf
11/12
Like bone, cartilage is sensitive to mechanical stimuli.The
synthesis of the extracellular matrix and maintenanceof the tissue
benefits from strain, promoting diffusion andeliciting electrical
potential. However, too much strain canbe damaging to the
cartilage, causing degeneration andleading to osteoarthritis. Based
on the amount of fibre andground substance, and the type of fibres,
three varieties of
cartilage are distinguished: hyaline cartilage, elasticcartilage
and fibrocartilage.
Hyaline cartilage
Hyaline cartilage is the most common form of cartilage.
Asdiscussed, it forms the majority of the temporary skeleton,as the
cartilage anlage, until it is gradually replaced bybone. Further,
the epiphyseal plate, located between themetaphysis and the
epiphysis of growing long bones, iscomposed of hyaline cartilage,
which is responsible for thelongitudinal growth of bone. In adults,
hyaline cartilage isfound in the nasal septum, larynx, trachea and
bronchi of
the respiratory system, on the articulating surfaces ofbones
(articular cartilage) and on the ventral ends of theribs where they
attach to the sternum. A definingcharacteristic of adult skeleton
is that the growth platehas been mineralized, preventing further
growth of longbones.
The extracellular matrix of hyaline cartilage containsprimarily
type II collagen, but several other types are alsopresent. Type XI
collagen forms a core for the type IIcollagen fibril, and
contributes to the control of fibrilgrowth. Type IX collagen, which
is really a form of aproteoglycans molecule, is found periodically
along thetype II collagen fibril and is covalently cross-linked to
it.
Collagen types VI, X, XII and XIV have also beendiscovered in
cartilage. Cartilage proteoglycans containchondroitin 4-sulfate,
chondroitin 6-sulfate and keratansulfate, covalently linked to core
proteins. These coreproteins are in turn the attachment points for
glycosami-noglycans (GAGs). Most of these proteoglycans
arenoncovalently associated with long molecules of hyaluro-nic
acid, forming proteoglycan aggregates (aggrecan) thatinteract with
collagen. The high content of water bound tothe negative charges of
GAGs serve, in essence, as a shockabsorber that is of great
functional importance, especiallyin articular cartilages. In fact,
it is believed that age-relateddegeneration of GAGs contributes to
the progressive
destruction of cartilage in the sense that it loses
itsresiliency to impact-loading. In contrast to bone, oncedamaged,
cartilage is not able to repair itself unfortu-nately this is why
so many athletes require surgery in mid-life. The amount of strain
that causes cartilage to fail is notknown, but it is believed that
this tissue is rarely strainedmore than 25%. Another important
component ofcartilage matrix is the glycoprotein chondronectin,
amacromolecule that promotes the adherence of chondro-cytes to
matrix collagen.
Except in the articular cartilage of joints, all hyalincartilage
is covered by a layer of dense connective tissuethe perichondrium,
which is essential for the growth anmaintenance of cartilage. It is
rich in collagen type I fibreand contains numerous chondroblasts
that easily differentiate into chondrocytes.
Elastic cartilage and fibrocartilage
Elastic cartilage is typically found in regions requiring
flexible form of support: the auricle of the ear, the walls othe
external auditory canals and eustachian tubes, thepiglottis, and
the cuneiform cartilage in the larynxBasically, elastic cartilage
is identical to hyaline cartilagexcept that, in addition to
collagen fibrils, it contains aabundant network of fine elastin
fibres.
Fibrocartilage has characteristics intermediate betweethose of
dense connective tissue and hyaline cartilage. It ifound in
intervertebral discs, in attachments of certailigaments to the
cartilaginous surface of bones, and in th
pubic symphysis. Chondrocytes occur singly or in rowbetween
large bundles of collagenous fibres. Fibrocartilagmatrix contains a
great number of coarse type I collagefibres, contributing to the
elasticity, toughness, resiliencand strength of the structure.
Ligament
Ligaments are tough bands of fibrous connective tissuthat tether
bones together and support organs. Ligamentoriginate and insert on
bone. From a skeletal point of view
their principal function is to maintain correct bone anjoint
geometry. The teres ligament helps to contain thfemoral head in the
pelvis, while ligaments such as thcruciates and collaterals bind
the bones around the knetogether. Ligaments, together with their
associated joincapsules (composed of similar material), are often
referreto as passive joint stabilizers, and together with
tharticular contours determine a joints range of motion. Asecond
function of ligamentous tissue is proprioceptionProprioceptive
receptors in ligament permit the sensing ojoint position, the
monitoring of ligament tension anintegrity, and the initiation of
protective reflexes.
Ligament cells are called fibroblasts, which also deriv
from mesenchymal stem cells. They are generally
orientelongitudinally along the length of the ligament
bodyFibroblasts are responsible for synthesizing and degradinthe
ligament matrix in response to various stimuli. Thmatrix comprises
virtually the entire body of the ligamenIt consists of water,
collagen, proteoglycans, fibronectinelastin, actin and a few other
glycoproteins. Water makeup approximately two-thirds of the wet
weight of ligament. Collagen (primarily type I with some type
IIIcomprises approximately 7080% of the dry weight o
Comparative Skeletal Structure
1ENCYCLOPEDIA OF LIFE SCIENCES / & 2001 Macmillan Publishers
Ltd, Nature Publishing Group / www.els.net
-
7/28/2019 comparative skeletal structure.pdf
12/12
ligament, andelastin a further1015%. In contrast to bonebeing
subject to strains of 0.3% (3000 microstrain),ligaments can stretch
up to 5% (50000 microstrain) beforethey are damaged.
Tendon
Tendons are anatomically and functionally discrete, verycomplex,
dense collagenous structures that connectmuscles to bones. Collagen
molecules combine to formordered units of microfibrils, subfibrils
and fibrils. Theseunits are arranged in closely packed, highly
ordered,parallel bundles that are oriented in a distinct
longitudinalpattern, with proteoglycans and glycoproteins in
associa-tion with water incorporated in a matrix, binding the
fibrilstogether.
Tendons contain a relatively poor blood supply and fewcells,
making the tissue relatively hypometabolic. Tendonscontain a small
number of nociceptive and proprioceptivenerves, particularly near
their attachment sites. One ofthese specialized sensory endings in
tendon is called theGolgi tendon organ, which senses tension and
providesfeedback control that alters muscle activity. Golgi
tendonorgans normally have a somewhat steady rate of
impulsetransmission to the spinal cord, one that is proportional
tothe degree of muscle tension. However, if the tension issuddenly
increased, an intense response of the tendonorgan results in a
reflex inhibitory effect on the muscle thatpresumably prevents the
development of potentiallydestructive excessive tension.
Energy storage is another important function of tendon.The
distinctly kinked morphology of the collagen withinthe tendon is
believed to facilitate the elastic storage andrecoveryof mechanical
strain energy, much like a spring. Ina runner, the tendons of the
lower limb muscles arestretched when the ball of the foot strikes
the ground, andthe kinetic energy is stored in the elastic
components of thetissue. At lift-off, the recoil of the tendon to
its originallength helps to push the foot off the ground at
thebeginning of the next stride. Unlikemusclecontraction,theelastic
energy of tendon recoil requires no energy input.
The composition of tendon is similar to that of
ligament.Collagen comprises as much as 85% of tendon dry weight;of
this 95% is type I and 5%type III and/or type V.Unlikeligament,
elastin constitutes less than 3% of tendon dryweight.
Summary
A brief overview of the biology, physiology and morphol-ogy of
bone and connective tissues, as well as the local andsystemic
factors that influence their growth, development,maintenance and
repair, has been provided. The process ofcell proliferation and
differentiation, matrix synthesis and
mineralization, growth and adaptation, all contribute tthis
elaborate balance of modelling and remodellingSystemic conditions
such as ageing or the menopausmay interfere with any number of
these processeultimately contributing to the aetiology of diseases
sucas osteoporosis. Thus, caution must be exercised wheconsidering
interventions that influence a single aspect o
this elaborate balance (e.g. calcitonin disruption oosteoclast
activity) which may, in turn, interrupt the abilitof remodelling to
function appropriately. Hopefully, it clear that the
osteoblast,osteocyte and osteoclast togetheandnot alone,are
responsiblefor the skeletons success asdynamic mineral reservoir
and structural material extraordinaire.
Further Reading
Alsina M, Guise T and Roodman GD (1996) Cytokine regulation
bone cell differentiation. Vitamins and Hormones 52: 6398.
Baron R, Ravesloot JH, Neef L et al. (1993) Cellular and
molecul
biology of the osteoclast. In: Noda M (ed.) Cellular and
MoleculaBiology of Bone, pp. 445495. San Diego: Academic Press.
Bilezikian JP, Raisz LG and Rodan GA (eds) (1996) Principles of
Bon
Biology. San Diego: Academic Press.
Buckwalter JA, Einhorn TA and Sheldon RS (eds)
(2000)Orthopaed
BasicScience. Rosemont, Illinois:AmericanAcademy of
Orthopaed
Surgeons.
Cowin SC (1989) Bone Mechanics. Boca Raton, FL: CRC Press.
Ducy P and Karsenty G (1998) Genetic control of cell
differentiation
the skeleton. Current Opinion in Cell Biology 10: 614619.
FergusonCM,MiclauT, HuD, AlpernE andHelms JA(1998) Commo
molecular pathways in skeletal morphogenesis and repair.
Annals
the New York Academy of Sciences 857: 3342.
Hall BK andMiyake T (1992)The membranous skeleton:the role of
c
condensations in vertebrate skeletogenesis.Anatomy and
Embryolog
186: 107124.Lian B and Stein GS (1992) Concepts of osteoblast
growth a
differentiation: basis for modulation of bone cell development
an
tissue formation. Critical Reviews in Oral Biology and Medicine
3(3
269305.
Martin RB,BurrDB andSharkey NA (1998)Skeletal Tissue
Mechanic
New York: Springer.
Niiweide PJ, Ajubi NE and Aarden EM (1998) Biology of
osteocyte
Advances in Organ Biology 5B: 529542.
Owen TA, Aronow M, Shalhoub V, Lian JB and Stein GS (199
Progressive development of the rat osteoblast phenotypein
vitro
reciprocal relationships in expression of genes associated
wi
osteoblast proliferation and differentiation during formation of
t
bone extracellular matrix. Journal of Cellular Physiology 143:
420
430.
Reddi AH (1994) Bone and cartilage differentiation. Current
Opinion Genetics and Development 4(5): 737744.
Rubin CT (1984) Skeletal strain and the functional strain
significance
bone architecture. Calcified Tissue International36: S11S18.
Rubin CT and Lanyon LE (1984) Dynamic strain similarity
vertebrates: an alternative to limb bone scaling.Journal of
Theoretic
Biology 107: 321327.
Rubin CT and Rubin J (2000) Biology, physiology and
morphology
bone. In: Harris E, Ruddy S and Sledge C (eds) Kellys Textbook
o
Rheumatology, 6th edn, pp. 16111634. Philadelphia, PA: W
Saunders.
Comparative Skeletal Structure
12 ENCYCLOPEDIA OF LIFE SCIENCES / 2001 M ill P bli h L d N P
bli hi G / l