Embed Size (px)
Citation preview

Sant et al. IEJDTR, 2017; 6(1): 386-389 386
ISSN: 2454-311X
COMPARATIVE EVALUATION OF ANTI-MICROBIAL EFFICACY OF CURCUMA ORAL GEL
AND CHLORHEXIDINE GEL ON THE PERIODONTAL PATHOGENS: AN IN-VITRO STUDY
ANKIT SANT1, DEEPAK DAVE2, PHORAM PATEL1, HARSHIL ZAVERI1
1 Post Graduate student, Department of Per iodontology, K. M. Shah Dental College, Vadodara, 2 Professor and HOD,
Department of Per iodontology, K. M. Shah Dental College, Vadodara, Gujarat, India. Corresponding Author: Dr Ankit Vilas
Sant, Depar tment of Per iodontology. M. Shah Dental College, Vadodara, Gujarat , India. Email: sant.ankit@gmai l.com,
Contact: +917600490588
ABSTRACT
Aim: To comparatively evaluate the antimicrobial efficacy of 1% Curcuma Oral Gel with 2% Chlorhexidine Gluconate gel
on gram negative per iodontal pathogens: Porphyromonas Gingival is (P. Gingivalis), Prevotella Intermedia (P. Intermedia),
Fusobacter ium Nucleatum (F. Nucleatum) and Aggregat ibacter Act inomycetemcomitans (A. Actinomycetemcomitans) in
in-vitro condi tions.
Materials and Method: Nutrient agar plates were inoculated by rubbing ster ile cotton swabs dipped into bacter ial
suspensions of P. gingivalis, P. intermedia, F. nucleatum and A. actinomycetemcomitans over the entire surface of the plate.
Three such sets were prepared. After inoculation, 10 mm diameter five wells were cut into the surface of each agar plate.
1% Curcuma Oral gel and 2% Chlorhexidine gel were added into wells in 4 different plates containing above mentioned 4
different bacter ia and dist i l led water was used. Plates were incubated and the diameter of zone of inhibition was
measured. The mean score of zones of inhibition were calculated and statist ical analysis was done.
Results: 2% Chlorhexidine gel had edge over 1% Curcuma gel in inhibiting the growth of micro-organisms. 1% Curcuma
gel was more effective against P.intermedia compared to P.gingivalis, F.nucleatum and A.act inomycetemcomitans. 2%
Chlorhexidine gel was more effective against A.actinomycetemcomitans and F.nucleatum compared to P.gingivalis and
P.intermedia.
Conclusion: 1% Curcuma oral gel can create a new hor izon in the field of chemical agents that can be used as an adjunct to
mechanical per iodontal therapy and can serve as a cheaper al ternative compared to 2% Chlorhexidine gel .
Keywords: Chlorhexidine gel , Per iodontal Pathogens, Turmer ic gel
INTRODUCTION
Periodontal disease eventually leads to tooth loss, if left
untreated. It is among the most widespread oral
bacter ial disease.1,2 Al though bacter ia belonging to more
than 630 different taxa exist in the oral cavity, only 10–
15 bacter ial species are recognised as potential
periodontal pathogens.3 Of them, Porphyromonas
gingivalis, Fusobacterium nucleatum, Prevotella
intermedia and Aggregatibacter actinomycetemcomitans are recognised as the major pathogens for initiation and
progression of destruction of tooth support ing
structures. The levels of P. gingivalis, P. intermedia and
other anaerobic bacter ia are seen to increase in adult
onset per iodontitis. While P. gingivalis and A.
actinomycetemcomitans are strongly associated with
localised aggressive per iodont itis, P. intermedia is
predominantly associated wi th the development of
necrotising ulcerative gingivi tis.4 Longitudinal and
retrospective studies have demonstrated an increased
r isk of per iodontal breakdown in A.
actinomycetemcomitans and P. gingivalis positive sites
and better post-treatment results in their absence.5
India has a r ich history of using plants for medicinal
purposes. Turmer ic (haldi), a rhizome of Curcuma longa,
is a common antisept ic used in traditional system of
Indian medicine. It may be a more acceptable and viable
option for the common man. It has proven proper ties
l ike anti-inflammatory, antioxidant, antimicrobial,
hepatoprotective, immunostimulant, antiseptic,
antimutagenic, and i t also accelerates wound heal ing.6
Curcumin, the main yellow bioactive component of
turmer ic, has been shown to have a wide spectrum of
biological actions.7 Li terature reports have shown that
curcumin has anti-inflammatory and ant ibacter ial
activi ties, suggesting i ts potential to be used as a
subgingival agent.7 Safety evaluation studies have
indicated that both turmer ic and curcumin are well
tolerated at a very high dose w ithout any toxic effects.7
To the best of our knowledge, there are currently no
studies assessing the efficacy of turmer ic gel with the
var ious per iodontal pathogens, using the disc diffusion
method. Hence, the present study will comprehensively
report the antimicrobial potential of turmer ic gel on
these key per iodontal pathogens. I t wil l also assess and
compare the in vitro efficacy of turmer ic gel w ith the gold
standard 2% chlorhexidine gel .
Sant et al. IEJDTR, 2017; 6(1): 386-389 387
MATERIALS AND METHODS
The study was designed as an in vitro study. Before
conduct ing the study, necessary ethical approval was
obtained from the Inst itutional Ethics Committee. Other
related approvals from the concerned author it ies were
obtained for the necessary microbial analysis. Mater ials
used in the study were 1% turmer ic gel , 2%
chlorhexidine gel and disti l led water. Microorganisms
included were P. gingivalis, P. intermedia, F. nucleatum
and A. actinomycetemcomitans strains. Test mater ials
included blood agar plates, Petr idishes and a digital
Vernier caliper . A total of 60 samples were taken.
Samples were divided into 3 reagent groups, as
ment ioned above ×4 strains of microorganisms ×3
repeti tions.
Disc diffusion method
The antibacter ial activity of 1% turmer ic gel and 2%
chlorhexidine gel was determined by disc di ffusion
method. Culture medium used was blood agar. A loop or
swab method was used to t ransfer microbial colonies to
the agar plates. Turbidity was visual ly adjusted wi th the
broth to equal that of a 0.5 McFar land turbidity standard
that had been vortexed. Alternatively, the suspension
was standardised wi th a photometr ic device. Within 15
min of adjusting the inoculums to a McFar land 0.5
turbidi ty standard, a ster i le cotton swab was dipped into
the inoculum and rotated against the tube wall above the
liquid to remove excess inoculum. Then, swabbing the
entire surface of the agar plate was done thr ice, rotat ing
plates approximately 60° to ensure even distr ibution.
Care was taken to avoid extra hi tting of the sides of the
plates to prevent creating aerosols. Inoculated plates
were allowed to stand for at least 3 min, but no longer
than 15 min before making wel ls. A hollow tube of 5 mm
diameter was heated and pressed above the inoculated
agar plates and was removed immediately, making a well
in the plate. Likewise, four wells of 5 mm diameters each
were made on each plate. 1% turmer ic gel, 2%
chlorhexidine gluconate gel and disti l led water were
added in the wells assigning each plate for each of the
solution. Within 15 min of compound application, plates
were shi fted to an anaerobic jar , which was kept in an
incubator for 48 hours. After incubation was complete,
plates were read only if the lawn of growth was
confluent or near ly confluent. The diameter of zones of
inhibition was measured for al l the wells using a digital
Vernier caliper . The mean score of zones of inhibit ion
was calculated for each solution, respectively.
Table 1: Mean zone of inhibi tion compar ing Curcuma
gel and chlorhexidine gel for
Porphyromonas gingivalis (Pg),
Prevotella intermedia (Pi),
Aggregat ibacter actinomycetemcomitans (Aa),
Fusobacter ium nucleatum (Fn)
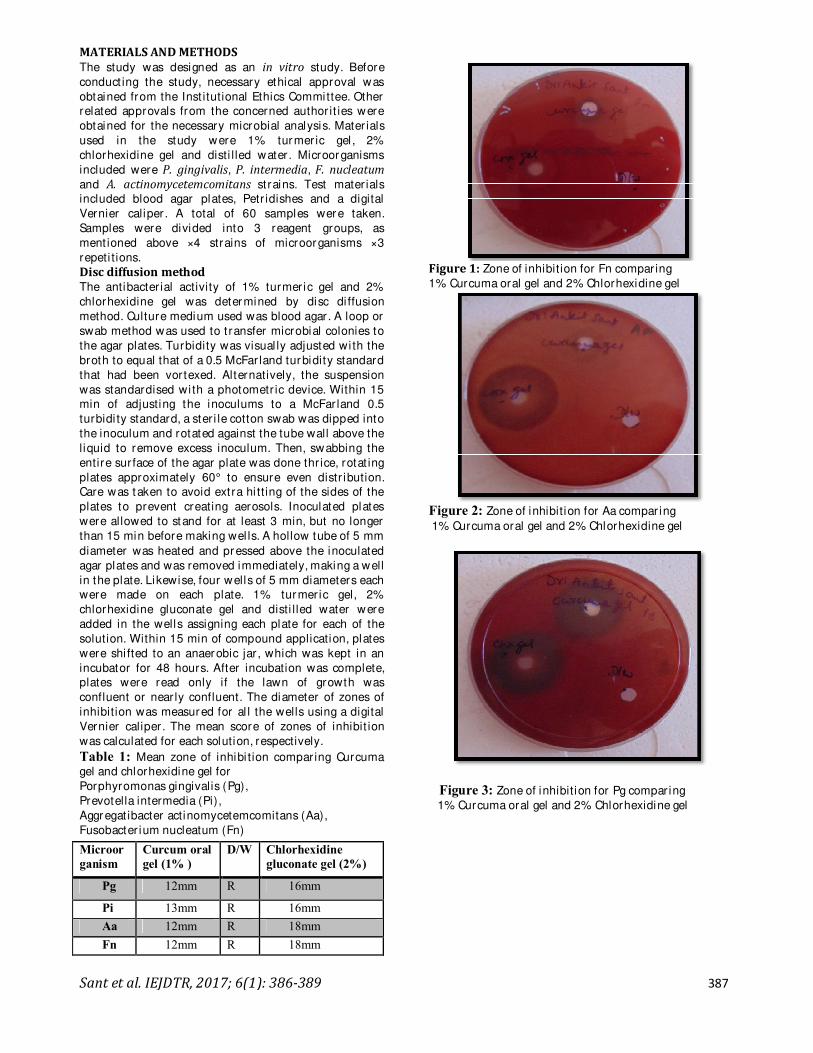
Figure 1: Zone of inhibition for Fn compar ing
1% Curcuma oral gel and 2% Chlorhexidine gel
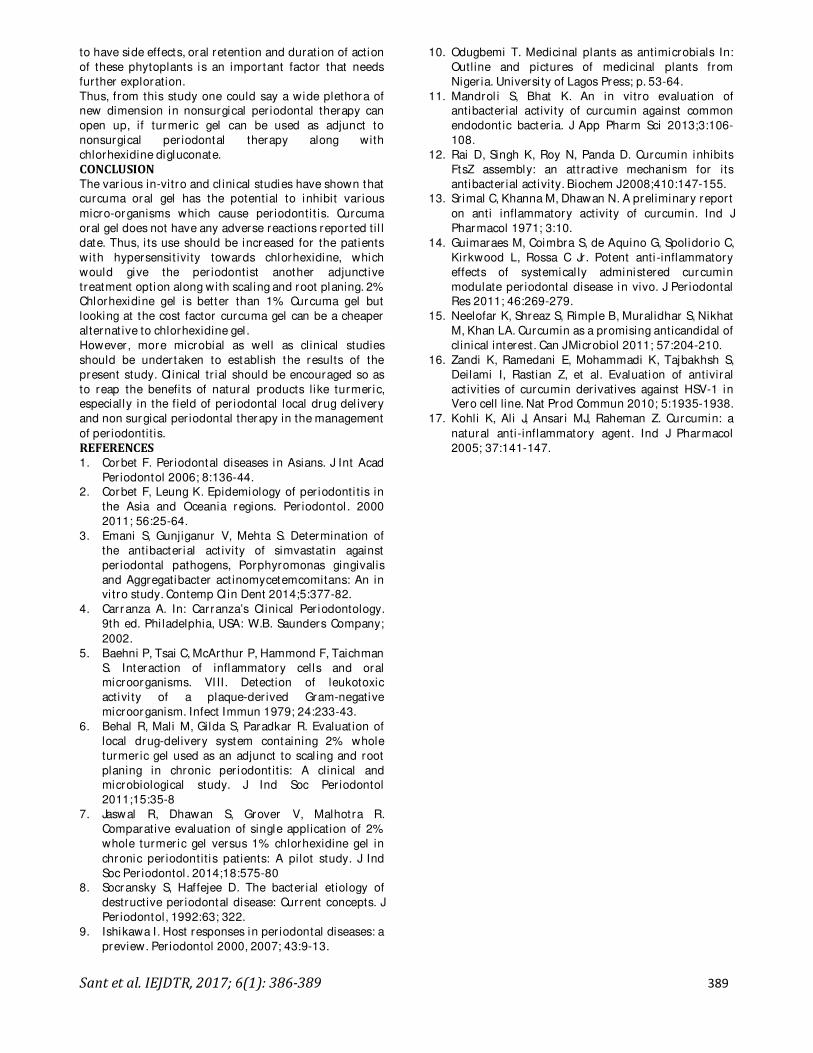
Figure 2: Zone of inhibition for Aa compar ing
1% Curcuma oral gel and 2% Chlorhexidine gel
Figure 3: Zone of inhibition for Pg compar ing
1% Curcuma oral gel and 2% Chlorhexidine gel
Microor
ganism
Curcum oral
gel (1% )
D/W Chlorhexidine
gluconate gel (2%)
Pg 12mm R 16mm
Pi 13mm R 16mm
Aa 12mm R 18mm
Fn 12mm R 18mm

Sant et al. IEJDTR, 2017; 6(1): 386-389 388
Figure 4: Zone of inhibition for Pi compar ing
1% Curcuma oral gel and 2% Chlorhexidine gel
RESULTS
2% Chlorhexidine gluconate gel showed the greatest
zone of inhibition against all per iodontal pathogens. 1%
turmer ic gel showed 13 mm zone of inhibit ion against P.
intermedia whereas 12 mm zone of inhibit ion was seen
against P. gingivalis, A. actinomycetemcomitans and F.
nucleatum. (Table-1)
DISCUSSION
The consensus report of the American Academy of
Per iodontology proved that the micro-organisms
responsible for per iodontitis are A.
actinomycetemcomitans, P. gingivalis, P. intermedia,
F.nucleatum.8 According to specific plaque hypothesis, by
eliminating above mentioned species, per iodontal
disease would regress.9 Thus per iodontal health of the
individual can be establ ished with the help of the agents
like turmer ic gel along with the use of mechanical plaque
control therapy.
The combination of microorganisms and inflammatory
response are the cause of many diseases, including
periodont itis, for which compounds having a dual anti-
inflammatory and antimicrobial activity can be desirable
therapeut ic agents.10 The results of this study
corroborate with the findings of study by Mandrol i et al,
which was done to evaluate the abili ty of curcumin to
exert antibacter ial activity against common endodontic
bacter ia l ike Streptococcus mutans, Actinomyces viscosus,
Lactobacillus casei, P. gingivalis, Prevotella intermedia
and Enterococcus faecalis.11 I t was, therefore, suggested
that curcumin has the ability to kil l several Gram-
posi tive and Gram-negative bacter ia.
A study by Rai et al (2008)12 suggested that curcumin
may inhibit bacter ial cell proli feration by inhibi ting the
assembly dynamics of FtsZ (a bacter ial protofilament),
which polymer izes to form a Z-r ing at the midcell that
orchesterates bacter ial cell division. The assembly and
stability of FtsZ protofilaments have been shown to play
cr itical roles in bacter ial cytokinesis. Thus, FtsZ may be
considered as an important antibacter ial drug target.
Another reason which might be suggested for the
antibacter ial potential of curcumin is that curcumin is a
polyphenolic compound, also having substantial
antibiofi lm act ivity.13 It inhibits the product ion of biofi lm
and disperses the biofilm made by many
microorganisms.14
Owing to the plaque biofi lm acting as the main etiological
factor in the per iodontal diseases, curcumin’s antibiofi lm
activi ty would also account for i ts antibacter ial activi ty
against per iodontal pathogens. Apart from the
antibacterial property, curcumin is a molecule known to
demonstrate antifungal act ivity15 and antivi ral activity as
wel l.16 Further, curcumin has long been touted as a
powerful anti-inflammatory and immunomodulatory
agent.17
Curcumin has been shown to regulate numerous
t ranscr iption factors, cytokines, protein kinases,
adhesion molecules, redox status and enzymes that have
been linked to inflammation.13 The ant i-inflammatory
activi ty of curcumin was first reported in 1971.17 It
reduces inflammat ion by effect ively inhibi ting
t ranscr iptional and translational expression of
proinflammatory cytokines like Inter leukin – 6 (IL – 6)
and Tumour Necrosis Factor – alpha (TNF – α). Curcumin
also demonstrated dose dependent attenuation of
nuclear factor kappa-light-chain-enhancer of activated B
cells (NF-kb) activation in the gingival tissue of rats
suffer ing from exper imental per iodontal disease. It,
fur ther, reduced the inflammatory infi lt rate, increased
collagen content, and increased fibroblastic cell numbers
in gingival tissues.17
Despite extensive research and development, poor oral
bioavai labi l ity of curcumin remains one of the major
concerns for i ts use as a therapeutic agent. This poor oral
bioavai labi l ity of curcumin can be att r ibuted to its poor
absorption, high rate of metabolism in the intestines and
rapid systemic elimination from the body. Thus,
attempts have been made to improve curcumin’s
bioavai labi l ity by use of adjuvants that can block the
metabol ic pathway of curcumin. This has been achieved
through encapsulation in l iposomes, biodegradable
microspheres, cyclodextr in, and hydrogels. Also, var ious
control led del ivery forms, such as polymer ic
micro/ nanospheres, l iposomes, micel les, parenteral
emulsion, and prodrugs have been investigated to
increase its solubili ty.
Maintenance or improvement of oral health by use of
natural products that also form a part of habi tual diet
seems to be a suitable way to preserve oral health.
Patients wi ll tend to be compl iant as they are not
burdened wi th added cost or t ime. However, this cannot
be confi rmed without appropr iate studies. Additionally,
proper util ization of available natural resources to
reduce the ever increasing prevalence of oral diseases in
rural parts of developing countr ies can help to diminish
the dangers of a poor dentist-populat ion rat io.
Active ingredients from such potent natural resources
should also be evaluated for their anti-inflammatory and
immune-modulatory properties. It is recommended that
the readily accessible natural products may be
integrated wi th presently avai lable synthetic mater ials
that are used to maintain the oral hygiene.
However, any natural product should be assessed for its
safety and cl inical applicat ion should not be done
wi thout sufficient scientific evidence. The mechanism of
action of a particular natural product needs to be studied
at a molecular level in order to assure the accuracy of
appl ication and consequently, the outcomes. Although
none of the neutraceuticals used in this study are known
Sant et al. IEJDTR, 2017; 6(1): 386-389 389
to have side effects, oral retention and duration of action
of these phytoplants is an important factor that needs
fur ther exploration.
Thus, from this study one could say a wide plethora of
new dimension in nonsurgical per iodontal therapy can
open up, if turmer ic gel can be used as adjunct to
nonsurgical per iodontal therapy along with
chlorhexidine digluconate.
CONCLUSION
The var ious in-vitro and cl inical studies have shown that
curcuma oral gel has the potential to inhibit var ious
micro-organisms which cause per iodontit is. Curcuma
oral gel does not have any adverse reactions reported ti l l
date. Thus, i ts use should be increased for the patients
with hypersensit ivity towards chlorhexidine, which
would give the per iodontist another adjunctive
treatment option along with scaling and root planing. 2%
Chlorhexidine gel is better than 1% Curcuma gel but
looking at the cost factor curcuma gel can be a cheaper
alternat ive to chlorhexidine gel .
However, more microbial as well as clinical studies
should be undertaken to establish the results of the
present study. Cl inical tr ial should be encouraged so as
to reap the benefi ts of natural products like turmer ic,
especially in the field of per iodontal local drug del ivery
and non surgical per iodontal therapy in the management
of per iodontitis.
REFERENCES
1. Corbet F. Per iodontal diseases in Asians. J Int Acad
Per iodontol 2006; 8:136-44.
2. Corbet F, Leung K. Epidemiology of per iodonti tis in
the Asia and Oceania regions. Per iodontol . 2000
2011; 56:25-64.
3. Emani S, Gunjiganur V, Mehta S. Determination of
the antibacter ial act ivity of simvastatin against
per iodontal pathogens, Porphyromonas gingivalis
and Aggregatibacter act inomycetemcomitans: An in
vi tro study. Contemp Cl in Dent 2014;5:377-82.
4. Carranza A. In: Carranza’s Clinical Per iodontology.
9th ed. Phi ladelphia, USA: W.B. Saunders Company;
2002.
5. Baehni P, Tsai C, McArthur P, Hammond F, Taichman
S. Interaction of inflammatory cells and oral
microorganisms. VI II. Detection of leukotoxic
activi ty of a plaque-der ived Gram-negative
microorganism. Infect Immun 1979; 24:233-43.
6. Behal R, Mali M, Gilda S, Paradkar R. Evaluat ion of
local drug-delivery system containing 2% whole
turmer ic gel used as an adjunct to scal ing and root
planing in chronic per iodont itis: A clinical and
microbiological study. J Ind Soc Per iodontol
2011;15:35-8
7. Jaswal R, Dhawan S, Grover V, Malhotra R.
Comparative evaluation of single application of 2%
whole turmer ic gel versus 1% chlorhexidine gel in
chronic per iodontitis patients: A pilot study. J Ind
Soc Per iodontol . 2014;18:575-80
8. Socransky S, Haffejee D. The bacter ial etiology of
destructive per iodontal disease: Current concepts. J
Per iodontol, 1992:63; 322.
9. Ishikawa I. Host responses in per iodontal diseases: a
preview. Per iodontol 2000, 2007; 43:9-13.
10. Odugbemi T. Medicinal plants as antimicrobials In:
Outline and pictures of medicinal plants from
Niger ia. Universi ty of Lagos Press; p. 53-64.
11. Mandrol i S, Bhat K. An in vitro evaluation of
antibacter ial activity of curcumin against common
endodont ic bacter ia. J App Pharm Sci 2013;3:106-
108.
12. Rai D, Singh K, Roy N, Panda D. Curcumin inhibits
FtsZ assembly: an att ract ive mechanism for its
antibacter ial activity. Biochem J 2008;410:147-155.
13. Srimal C, Khanna M, Dhawan N. A preliminary report
on anti inflammatory activity of curcumin. Ind J
Pharmacol 1971; 3:10.
14. Guimaraes M, Coimbra S, de Aquino G, Spolidor io C,
Kirkwood L, Rossa C Jr . Potent anti -inflammatory
effects of systemical ly administered curcumin
modulate per iodontal disease in vivo. J Per iodontal
Res 2011; 46:269-279.
15. Neelofar K, Shreaz S, Rimple B, Muralidhar S, Nikhat
M, Khan LA. Curcumin as a promising anticandidal of
clinical interest. Can J Microbiol 2011; 57:204-210.
16. Zandi K, Ramedani E, Mohammadi K, Tajbakhsh S,
Deilami I, Rastian Z, et al. Evaluation of antiviral
act ivities of curcumin der ivatives against HSV-1 in
Vero cell line. Nat Prod Commun 2010; 5:1935-1938.
17. Kohli K, Ali J, Ansar i MJ, Raheman Z. Curcumin: a
natural anti-inflammatory agent. Ind J Pharmacol
2005; 37:141-147.





























