Embed Size (px)
Citation preview

Current Medical Research & Opinion 2014, 1–8
0300-7995 Article RT-0124.R1/928274
doi:10.1185/03007995.2014.928274 All rights reserved: reproduction in whole or part not permitted
Original articleComparative effectiveness of vildagliptin incombination with other oral anti-diabetes agentsin usual-care conditions: the EDGE–LatinAmerica study
Carlos O. Mendivil*Universidad de los Andes, School of Medicine, Bogota,
Colombia
Fundacion Santa Fe de Bogota, Section of
Endocrinology, Bogota, Colombia
Eduardo Marquez-Rodrıguez*Instituto Jalisciense de Metabolismo, Guadalajara,
Mexico
Hospital Angeles del Carmen, Guadalajara, Mexico
Ivan D. AngelEscuela de Nutricion y Dietetica, Universidad de
Antioquia, Medellın, Colombia
Gustavo PazHospital Carlos Andrade Marın, Quito, Ecuador
Cruz RodrıguezInCardio, Maturın (Monagas), Venezuela
Jorge AlmadaNovartis Latin America, Mexico City, Mexico
Ofelia SzyskowskyClınica Santa Isabel, Buenos Aires, Argentina
Address for correspondence:Carlos O. Mendivil, Universidad de los Andes, School
of Medicine, Cra 7a # 116-05, Of. 413, Bogota,
Colombia.
Tel.: +57 321.373.5051;
Keywords:Anti-diabetics – Diabetes – Dipeptidyl peptidase-IV
inhibitors – Vildagliptin
Accepted: 21 May 2014; published online: 11 June 2014
Citation: Curr Med Res Opin 2014; 1–8
Abstract
Objective:
To assess the proportion of patients on vildagliptin add-on dual therapy who respond to treatment over a
12 month follow-up, relative to comparator oral anti-diabetes dual therapy, in a usual care setting.
Research design and methods:
Participants were patients with type 2 diabetes (T2DM) aged 18 years and older from 311 centers in
Argentina, Colombia, Ecuador, Mexico and Venezuela. Patients were taking monotherapy with an oral anti-
diabetes drug (OAD), and were prescribed a new add-on OAD based on the judgment of their personal
physician. According to this choice, patients were assigned to one of the two cohorts: vildagliptin or
comparator OADs.
Main outcome measures:
The primary endpoint was the proportion of patients achieving an A1c drop 40.3% without edema,
hypoglycemia, weight gain or discontinuation due to gastrointestinal (GI) events. The secondary endpoint
was the proportion of patients with baseline A1c �7% who reached the goal of an A1c 57% without
hypoglycemia or weight gain.
Results:
The per-protocol population (a subset of the intention-to-treat population that excluded patients with pre-
specified protocol deviations) comprised 3773 patients, 3002 in the vildagliptin cohort and 771 in the
comparator cohort. The proportion of patients reaching the primary endpoint was higher in the vildagliptin
cohort (60.3%) than the comparator cohort (50.7%), OR 1.48 (95% CI: 1.25–1.73). The same was observed
for the secondary endpoint (44.8 versus 33.1%) OR 1.64 (95% CI: 1.37–1.98). The incidence of adverse
events was low and similar between treatment cohorts.
Conclusion:
In a usual care setting, patients treated with a vildagliptin combination succeeded in lowering A1c to57%,
without weight gain, hypoglycemia or peripheral edema more often than patients treated with comparator
combinations, without increased risk of adverse events. Key limitations are the observational nature of the
study and its relatively limited 12 month timeframe.
Introduction
During the past three decades, the developing world has experienced a dramaticrise in the prevalence of type 2 diabetes mellitus (T2DM), and Latin Americahas not been the exception. The International Diabetes Federation (IDF)
*These authors contributed equally to thedevelopment of this study.
! 2014 Informa UK Ltd www.cmrojournal.com Vildagliptin combination effectiveness in Latin America Mendivil et al. 1
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
08/
25/1
4Fo
r pe
rson
al u
se o
nly.

estimated for Latin America in the year 2011 a regionalage-adjusted prevalence of diabetes of 9.2% in adults1, ahuge figure for a region of 577 million people trying toescape from poverty and underdevelopment. Diabetesimposes a high economic burden in this subcontinent: atleast 3.1 billion dollars a year in 2003 for Mexico, CentralAmerica, the Caribbean and South America, in directmedical costs alone, according to the Pan-AmericanHealth Organization (PAHO)2. Most of these costs arederived from the chronic complications of the disease, asthey result in hospitalizations with expensive diagnosticand therapeutic procedures. Even though a tight controlof glycemia and other risk factors has proven to prevent theappearance of the chronic complications of T2DM3, therates of goal achievement are remarkably low in bothindustrialized4 and developing countries5. Achievementof treatment goals is the mainstay of T2DM care, butgiven the progressive nature of the condition this oftenrequires the simultaneous use of lifestyle changes and acombination of drugs6–8.
In addition to efficacy, recent guidelines suggest thateffectiveness, tolerability, cost and patient preferencesmay influence the outcomes of therapy and should be con-sidered when choosing anti-diabetes drugs9. Usual prac-tice, usual care studies provide essential informationabout the results of an intervention when all factors poten-tially impacting treatment outcomes are taken intoaccount. Despite the pivotal role of randomized controlledtrials on the initial determination of efficacy, the general-izability of their results can be quite limited, and there is anincreasing recognition of the importance of pragmatictrials10–12.
EDGE (Effectiveness of Diabetes control withvildaGliptin and vildagliptin/mEtformin) is a prospective,1 year, usual care observational study conducted world-wide, that assesses the effectiveness and tolerability of vil-dagliptin, a dipeptidyl peptidase-IV (DPP-4) inhibitor,added to monotherapy with an oral anti-diabetes drug(OAD), compared to any two-OAD combination withoutvildagliptin (pooled). Physicians enrolled patients withT2DM inadequately controlled using one OAD, when asecond glucose-lowering agent was considered. This studysought to assess the effectiveness and tolerability of vilda-gliptin combinations versus other OAD two-agent com-binations, but also to illustrate the advantages andlimitations of large usual care studies. Most multinationalclinical trials or post-marketing studies include very few orno patients from Latin America, so there is a great paucityof reliable information on the pharmacological manage-ment of T2DM that is unmistakably applicable to ourpopulation. EDGE–Latin America aims to contribute infilling this gap.
In this manuscript, we report on the effectiveness andtolerability of vildagliptin combinations versus other OADtwo-agent combinations for patients enrolled in Latin
American countries (Argentina, Colombia, Ecuador,Mexico and Venezuela).
Methods
Study design
EDGE was a 12 month, observational, multicenter, post-authorization, prospective cohort study in which 45,868patients from 2957 centers in 27 countries from Europe,Central and Latin America, Asia and Middle East wereevaluated. Of these, 4145 patients were enrolled from311 sites in Argentina, Colombia, Ecuador, Mexico andVenezuela. Adult patients (aged 418 years) with T2DMand inadequate glycemic control while receiving OADmonotherapy with a sulfonylurea (SU), metformin, thia-zolidinedione (TZD), metiglinide, or alpha-glucosidaseinhibitor (AGI), and for whom a second oral anti-diabeticagent (OAD) was considered, were eligible. Patients whowere planned to initiate a DPP-4 inhibitor other thanvildagliptin, or a glucagon-like peptide-1 (GLP-1)mimetic/analogue, or who required three or more OADsat study entry were excluded, as were patients changedfrom one OAD or OAD class to another at the time ofstudy entry, prior to adding a new OAD. Patients who wereusing insulin at the time of study entry and patients with ahistory of hypersensitivity to any of the study drugs or drugsof similar chemical classes were excluded.
Participants were required to provide written or oralinformed consent (per country regulations) to have datacollected and agree to follow all local medication labelingor prescribing requirements of their new OAD. Physicianschose glucose-lowering treatment for their patients at theirdiscretion. To ensure non-interventional status, patientenrollment was agreed after the treatment decision wasmade. Suitable patients fell into one of two cohorts (vil-dagliptin or comparator). The term index therapy is usedto represent the combination treatment initiated at enroll-ment. For any index therapy, a fixed dose combination,when available, was allowed13. The choice of the initialmonotherapy and the decision to intensify was entirelydetermined by each treating physician individually.
Data collection
Demography (age, gender, race, height, ethnicity), bodyweight, medical history, date of diagnosis of T2DM, anti-diabetes medications taken prior to study entry, newlyinitiated add-on OAD (second component of index medi-cation), other medications (by class), most recent A1c testdate and result, and any other laboratory test dates andresults were collected at baseline during a routine officevisit. After 12 months, the final data collected includedbody weight, changes to newly initiated index OAD, most
Current Medical Research & Opinion 2014
2 Vildagliptin combination effectiveness in Latin America Mendivil et al. www.cmrojournal.com ! 2014 Informa UK Ltd
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
08/
25/1
4Fo
r pe
rson
al u
se o
nly.

recent A1c test data and result, other laboratory test datesand results, adverse events and study completion status.Interim assessments could occur at any time between base-line and final study data collection, or early termination.Laboratory testing was performed on patients in linewith normal medical practice and/or as defined by localprescribing information and/or at a time period judgedappropriate by the physician. Because of the ‘real-world’nature of the study, central laboratories were not used.However, A1c measurements were performed in the parti-cipating centers using National GlycohemoglobinStandardization Program (NGSP)-approved methodolo-gies from commercial manufacturers. In keeping with thenon-interventional observational design employed, moni-toring was conducted only at centers with high enrolment(about 5% of centers). However, physicians were requestedto maintain source documents for each patient, includingsigned informed consent forms.
Effectiveness and tolerability endpoints
Primary endpointThe primary endpoint was defined as the proportion ofpatients having a treatment response (A1c reduction40.3% from baseline to month 12) while presenting notolerability findings (peripheral edema, proven hypogly-cemic event, discontinuation due to a gastrointestinal(GI) event, or weight gain �5%). Patients who couldnot be categorized as a success or failure (e.g. due to missingA1c or body weight data at 12 month endpoint) were con-sidered non-evaluable. Non-evaluable patient data wereconsidered failures in calculation of the odds ratio (OR)for success. The main analysis of the primary endpointutilized the per-protocol (PP) population; data were cen-sored if patient changed index therapy. Patients weredefined as having proven hypoglycemia if they experi-enced any hypoglycemic event as defined below, con-firmed by the opinion of the physician, at any timeduring the 12 month observation period: i. symptoms sug-gestive of hypoglycemia that resolved promptly on theadministration of oral carbohydrate, ii. symptoms suggest-ive of hypoglycemia accompanied by a plasma glucosebelow 3.1 mmol/L (56 mg/dL), or iii. symptoms suggestiveof hypoglycemia and patient unable to initiate self-treatment therefore requiring assistance of a third partyor hospitalization.
Secondary endpointThe secondary endpoint was defined as the proportion ofpatients with a baseline A1c �7% who achieved an A1c57% without experiencing proven hypoglycemia orweight gain �3%.
Analysis of primary and secondary effectivenessand tolerability endpoints
Data were collected at baseline and at any time pointin the next 12 months, with a required reporting at 12months. This manuscript constitutes a post-hoc analysisof the global EDGE study and, as such, it providesmainly descriptive statistics. For the primary and second-ary endpoints, the probability of success was analyzed usinga binary logistic regression model to calculate odds ratios(ORs) and their 95% confidence intervals (CIs). The ORexpresses the odds in favor of success in the vildagliptingroup relative to odds in favor of success in the comparatorOADs group. Given the post-hoc nature of this analysis,only the unadjusted OR and a single multivariate model(as an exploratory analysis) are provided. The between-groups difference in A1c drop was analyzed usingANCOVA, with treatment group as a fixed factor andbaseline A1c as the model covariate.
Ethics
The protocol for EDGE was approved by the followingIndependent Review Boards (IRBs) in each country:Argentina: Comite Independiente de Etica para Ensayosen Farmacologıa Clınica de la Fundacion de EstudiosFarmacologicos y de Medicamentos ‘Profesor Luis M.Zieher’, Colombia: Comite Independiente de Etica eInvestigacion Biomedica AVANZAR, Ecuador: Comitede Bioetica de la Universidad San Francisco de Quito,Mexico: Instituto Mexicano de Educacion Medica eInvestigacion Clınica S.C., Venezuela: Comite de Eticadel CENREV – Centro Nacional De Retina Y Vıtreo.We obtained written informed consent from participantsin all countries except Mexico, where local regulationsallow IRBs to authorize a verbal informed consent in stu-dies with minimal risk like this one. The consent was rec-orded at the medical record and at the case report form. AllEthics Committees/IRBs involved in the study approvedthe consent procedure.
Results
Patient populations and baseline characteristics
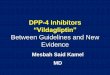
The enrolled population comprised 4145 patients withdocumented informed consent, but 296 patients (229 inthe vildagliptin and 67 in the comparator cohort) wereexcluded due to inadequate source documentation or prob-lems with the quality or accuracy of data entry (Figure 1).The intention-to-treat (ITT) population, used for baselinedemographics and safety analyses, comprised 3065 and 781patients receiving dual therapy with newly prescribed vil-dagliptin or a non-vildagliptin OAD added to prior
Current Medical Research & Opinion 2014
! 2014 Informa UK Ltd www.cmrojournal.com Vildagliptin combination effectiveness in Latin America Mendivil et al. 3
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
08/
25/1
4Fo
r pe
rson
al u
se o
nly.

monotherapy, respectively. The per-protocol populationwas a subset of the ITT population that excluded partici-pants with pre-defined protocol deviations (Figure 1).The per-protocol population was used for the analyses ofeffectiveness endpoints and comprised 3002 patients inthe vildagliptin, and 771 in the comparator cohort. Thenumber of patients with a baseline A1c57% whose treat-ment was intensified during the study were 288 (9.4%)in the vildagliptin cohort, and 66 (8.4%) in the compara-tor cohort.
The baseline characteristics of the ITT population aresummarized in Table 1. Study participants were on average55.9 years old, had been diagnosed with diabetes 5.6 yearsago, had a BMI of 29.5 kg/m2, and an A1c level of 8.5%.The sex distribution was almost even. Hypertension waspresent in 46.1% of participants, lipid disorders in 32.9%,established macrovascular complications in 5.3% and
established microvascular complications in 4.8%. The vil-dagliptin and comparator groups were similar in importantclinical variables like sex distribution, body-mass indexand baseline A1c, and had small but statistically signifi-cant differences in other variables: participants in the com-parator group were on average 2 years older (p50.001),their T2DM had lasted 0.9 years longer (p50.001), hada higher prevalence of hypertension (49.4 vs 45.2%,p¼ 0.034), lipid disorders (36.2 vs 32.0%, p¼ 0.025) anda slightly higher prevalence of microvascular complica-tions (6.7 vs 4.4%, p¼ 0.008).
The different OAD combination schemes receivedby the ITT population in each group are displayed inTable 2. In the vildagliptin cohort, the most frequentcombination was with metformin (80%). After metfor-min, the most frequent coexisting therapy was SUs, fol-lowed by TZDs, AGIs and in the last place metiglinides.Conversely, in the comparator group the most frequentcombination therapy was metforminþ SUs (62%), fol-lowed by metforminþTZDs, SUþTZDs, metiglinidesþmetformin, AGIsþmetformin, AGIsþ sulfonylureas,metiglinidesþTZDs, AGIsþTZDs and in the lastplace metiglinidesþSUs.
Primary and secondary endpoints
Table 3 shows the success rates and ORs for the primaryand secondary endpoints. The percentage of patientsin the vildagliptin group who successfully reached the pri-mary endpoint of a decrease in A1c40.3%, without per-ipheral edema, hypoglycemia, discontinuation due to GIside-effects or hypoglycemia was 60.3%. In the comparatorgroup this percentage was 50.7%. This difference resultedin an OR of 1.48 (95% CI: 1.26–1.73). As indicated inTable 3, a similar advantage for vildagliptin-based thera-pies was seen for the secondary endpoint, with 44.8% ofvildagliptin-treated patients compared to 33.1% of com-parator-treated patients reaching the secondary endpoint,resulting in an OR of 1.64 (95% CI: 1.37–1.98).
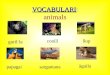
The mean change in A1c at 12 months by treatmentgroup is illustrated in Figure 2: �1.70% (95% CI: �1.74–�1.67) in vildagliptin-treated patients and �1.50% (95%CI: �1.58–�1.43) in comparator-treated patients (ana-lysis not pre-specified in protocol).
Safety analyses
The number of patients with any reported adverse event inany primary system organ class was 202 in the vildagliptincohort (6.6%) and 124 in the comparator cohort (25.9%).Table 4 summarizes adverse events that occurred duringthe study, listed by system organ class. There were fourdeaths reported among the 3065 patients in the vildaglip-tin cohort ITT population, and one death among the 781
4,145enrolled*
3,294Vildagliptin cohort
229Insufficient data
quality
67Insufficient data
quality
3,065ITT**
63Protocol
deviations
3,002Per protocol***
540Discontinued
848Comparator cohort
781ITT**
771Per protocol***
10Protocol
deviations
118Discontinued
663Patients
completed
2,525Patients
completed
Figure 1. Patient population and flow. *The enrolled population includes allpatients who gave documented informed consent. **The intention-to-treat(ITT) population is a subset of the enrolled population and includes allpatients who were assigned to new treatment at study start. Sites and/orpatients identified with quality and compliance findings, irregular data wereexcluded from the ITT analysis population. ***The per-protocol (PP)population is a subset of the ITT population. The PP population was used forthe analyses of effectiveness endpoints. Patients with the followingdeviations at baseline assessment were excluded from the per protocolpopulation: patients receiving DPP-4 inhibitors at baseline or within 1 monthprior to baseline; patients receiving GLP-1 mimetics/analogues at baselineor within 1 month prior to baseline; patients receiving insulin at baseline;patients receiving only newly initiated monotherapy or more than two oralanti-diabetes medications at baseline; drug-naive patients at baseline(patients not taking any diabetic medication prior to baseline); patients whoswapped from one oral anti-diabetes medication or class to another atbaseline; patients receiving vildagliptin at baseline or 30 days prior tobaseline or five half-lives prior to baseline; patients receiving more than oneoral anti-diabetes medication prior to baseline.
Current Medical Research & Opinion 2014
4 Vildagliptin combination effectiveness in Latin America Mendivil et al. www.cmrojournal.com ! 2014 Informa UK Ltd
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
08/
25/1
4Fo
r pe
rson
al u
se o
nly.

patients in the comparator cohort ITT population.Hypoglycemia was reported by 7 patients (0.23%) in thevildagliptin cohort, and by 10 patients (1.28%) in thecomparator cohort. After adjusting for baseline weight byANCOVA, the change in body weight for patients in thevildagliptin-therapies cohort was �3.05 kg (95% CI:�3.27–�2.85), while in the comparator cohort thisweight change was �2.50 kg (95% CI: �2.94–�2.08).
Given the presence of small but significant differencesbetween groups in some baseline variables, we ran a multi-variable logistic regression model that included as pre-dictors (besides treatment group), the followingcovariates: age, diabetes duration, hypertension (yes/no),lipid disorders (yes/no), and microvascular complications(yes/no). After multivariable adjustment, the odds ofachieving the primary endpoint were still significantly
Table 3. Primary and secondary efficacy and tolerability endpoints.
Vildagliptin ComparatorSample size for primary endpoint n¼ 3002 n¼ 771
Sample size for secondary endpoint n¼ 2422 n¼ 626 OR (95% CI) p Value
Primary EndpointDecrease in A1c40.3%, no hypoglycemia, no weightgain, no discontinuation for gastrointestinal events, noperipheral edema
1810 (60.3) 391 (50.7) 1.48 (1.25–1.73) 50.001
Secondary EndpointAmong participants with baseline A1c �7%: achieve-ment of A1c57% at end of study without provenhypoglycemic events or weight gain �3%
1085 (44.8) 207 (33.1) 1.64 (1.37–1.98) 50.001
Analyses were performed on the per-protocol population. The per-protocol (PP) population is a subset of the ITT population from which patients with any of thefollowing deviations from the protocol were excluded: use of DPP-4 inhibitors at baseline or within 1 month prior to baseline, use of GLP-1 mimetics/analogues atbaseline or within 1 month prior to baseline, use of insulin at baseline, use of more than two oral anti-diabetes medications at baseline, use of no anti-diabetes drug(drug-naive patients) at baseline, change from one oral anti-diabetes medication or class to another at baseline, use of vildagliptin at baseline or 30 days prior tobaseline and use of more than one oral anti-diabetes medication prior to baseline. Only unadjusted ORs are shown.
Table 2. Index medications by study group (ITT population).
Vildagliptin cohort* (n¼ 3065) Comparator cohort* (n¼ 781)
Vildagliptin þ n (%) Combination n (%)
Metformin 2451 (80.0) Metforminþ Sulfonylureas 483 (62.0)Sulfonylureas 439 (14.3) Metforminþ Thiazolidinediones 148 (19.0)Thiazolidinediones 132 (4.31) Sulfonylureasþ Thiazolidinediones 89 (11.4)Alpha glucosidase inhibitors 25 (0.82) MetiglinidesþMetformin 29 (3.72)Metiglinides 15 (0.49) Alpha glucosidase inhibitorsþMetformin 13 (1.67)
Alpha glucosidase inhibitorsþ Sulfonylureas 8 (1.03)Metiglinidesþ Thiazolidinediones 4 (0.51)Alpha glucosidase inhibitorsþ Thiazolidinediones 3 (0.39)Metiglinidesþ Sulfonylureas 2 (0.26)
*For three patients in the vildagliptin cohort and two in the comparator cohort, it was not possible to identify the index medication.
Table 1. Demographic and patient baseline characteristics (ITT population).
Characteristic Vildagliptin Comparator Total p Valuen¼ 3065 n¼ 781 n¼ 3846
Age (years) 55.5� 12.5 57.5� 11.7 55.9� 12.4 50.001Female sex (%) 1597 (52.1) 426 (54.6) 2023 (52.6) 0.22BMI (kg/m2) 29.5� 5.33 29.3� 5.2 29.5� 5.3 0.24Baseline A1c (%) 8.5� 1.7 8.5� 1.66 8.5� 1.69 0.42Duration of T2DM (years) 5.5� 6.1 6.4� 6.2 5.66� 6.1 50.001Hypertension (%) 1385 (45.2) 386 (49.4) 1771 (46.1) 0.034Lipid disorders (%) 981 (32.0) 283 (36.2) 1264 (32.9) 0.025Macrovascular disease (%) 154 (5.0) 51 (6.5) 205 (5.3) 0.094Microvascular disease (%) 134 (4.4) 52 (6.7) 186 (4.8) 0.008
Data are means� SD or n (%).
Current Medical Research & Opinion 2014
! 2014 Informa UK Ltd www.cmrojournal.com Vildagliptin combination effectiveness in Latin America Mendivil et al. 5
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
08/
25/1
4Fo
r pe
rson
al u
se o
nly.

higher in the vildagliptin group (OR 1.54, 95% CI 1.32–1.81), with a point estimate very similar to that found inthe univariate model.
Sensitivity analysis
In a sensitivity analysis, we evaluated the frequency of theprimary endpoint only in patients whose treatmentincluded metformin (metforminþ vildagliptin in the vil-dagliptin cohort, and metforminþ other OAD in the com-parator cohort). The results did not differ from those in thecomplete study sample: the percentage achievementof the primary study endpoint was 58.1% (1424/2451)in the vildagliptin group and 45.9% (309/673) in the com-parator group (p50.001).
Discussion
There is a very limited body of evidence from large studiesregarding the effectiveness of anti-diabetes medications asused in everyday practice14,15. This unmet need is feltaround the world, but particularly so in Latin America,a continent where the prevalence of T2DM has exhibiteda sharp increase in recent times, in parallel with the costs,morbidity and mortality associated with inadequate man-agement of the disease, and where economic resourcesavailable to treat chronic complications are sparse.The results from EDGE–Latin America contribute to fillthis gap.
First and foremost, the results from EDGE confirm thelow achievement of glycemic goals among patients withT2DM, highlighting a seemingly intractable problem ofclinical inertia despite calls from virtually every T2DMguideline in the world to be proactive and aggressive inthe pursuit of treatment goals9. A previous study inMexican patients with T2DM in Mexico found a rateof a goal A1c57% in only 37% of 2439 patients, whilethe percentage of patients reaching the composite end-point that included simultaneously A1c, blood pressureand low-density lipoprotein cholesterol goals was a mere3%5. A cross-sectional analysis of the quality of care pro-vided by specialists in Argentina to 1888 patients withT2DM from 43 centers across the country found that39.7% of patients were treated with a single anti-diabetesdrug, 35.3% with two drugs and 9.4% with three drugs.The average time from diagnosis to initiation of insulintherapy was 12 years16. Likewise, in a review of medicalrecords of patients with T2DM attending the diabetesclinics at the Salvadorean Social Security Institute, thegoal of a fasting plasma glucose level between 70 and120 mg/dL was achieved by only 26.9% of patients17.
While it is true that T2DM management in LatinAmerica appears to be less than perfect, studies in differentcountries show a comparable reality. A nationwide,
Table 4. Adverse events by primary system class and cohort (ITTpopulation).
Primary System Organ Class (SOC) Vildagliptin(n¼ 3065)
Comparator(n¼ 781)
Infections and infestations 52 (1.7%) 30 (3.9%)Gastrointestinal disorders 29 (1.0%) 17 (2.2%)Metabolism and nutrition disorders 17 (0.6%) 15 (1.9%)Nervous system disorders 22 (0.7%) 10 (1.3%)Musculoskeletal and connective tissue
disorders14 (0.5%) 15 (1.9%)
General disorders and administrationsite conditions
11 (0.4%) 7 (0.9%)
Vascular disorders 11 (0.4%) 4 (0.5%)Renal and urinary disorders 9 (0.3%) 3 (0.4%)Respiratory, thoracic and mediastinal
disorders4 (0.1%) 8 (1%)
Injury, poisoning and proceduralcomplications
6 (0.2%) 1 (0.1%)
Psychiatric disorders 4 (0.1%) 3 (0.4%)Cardiac disorders 3 (0.1%) 2 (0.3%)Neoplasms benign, malignant and
unspecified2 (0.1%) 3 (0.4%)
Skin and subcutaneous tissue disorders 4 (0.1%) 1 (0.1%)Blood and lymphatic system disorders 3 (0.1%) 1 (0.1%)Eye disorders 2 (0.1%) 1 (0.1%)Hepatobiliary disorders 3 (0.1%) 0 (0%)Investigations 2 (0.1%) 1 (0.1%)Immune system disorders 1 (0%) 1 (0.1%)Reproductive system and breast
disorders1 (0%) 1 (0.1%)
Ear and labyrinth disorders 1 (0%) 0 (0%)Pregnancy, puerperium and perinatal
conditions1 (0%) 0 (0%)
Endocrine disorders 0 (0%) 0 (0%)Surgical and medical procedures 0 (0%) 0 (0%)TOTAL 202 (6.7%) 124 (16.1%)
Adverse events were coded according to the Medical Dictionary forRegulatory Activities (MedDRA), version 14.0. Primary system organ classesare presented in descending order of total frequency of adverse events. Apatient with multiple occurrences of an adverse event under one cohort iscounted only once in the adverse event category. A patient with multipleadverse events within a primary system organ class is counted only once inthe total row for that cohort. Switches from vildagliptinþmetformin fixeddose to vildagliptin as add-on dual therapy to metformin and vice versa werenot counted as treatment change. Total also contains patients without initialdual therapy.
−1.50 *−1.70*
p<0.001p<0.001
4.0
5.0
6.0
7.0
8.0
9.0
Vildagliptin Comparator
A1c
(%
)
p<0.001
Figure 2. Glycated hemoglobin levels at study end (dark bars) versusbaseline (clear bars) in the ITT population, by group. *ANCOVA-adjustedchange in A1c.
Current Medical Research & Opinion 2014
6 Vildagliptin combination effectiveness in Latin America Mendivil et al. www.cmrojournal.com ! 2014 Informa UK Ltd
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
08/
25/1
4Fo
r pe
rson
al u
se o
nly.

population-based survey of goal achievement (includinglaboratory values plus lifestyle and weight/waist circumfer-ence goals) among T2DM patients in Spain, found thatdespite a majority of patients reaching an A1c57% (71%),none of the study participants attained all of the eight pre-established treatment goals, and only three patients previ-ously diagnosed with diabetes achieved seven of them18.This finding is especially worrisome coming from a countrywith universal health coverage and a health systemstrongly focused on primary care and preventive medicine.In the United States, a recent analysis of diabetes carebetween the years 1999 and 2010 including more than100,000 patients found 51.3% of them (in 2010) to havean A1c57%. The common objective of A1c, LDL chol-esterol and blood pressure goal attainment plus no tobaccouse was met by only 14.3% of patients19. In the Asiancontinent, a study of glycemic control in more than238,000 Chinese patients with T2DM found between17.8% and 36.1% of them to have an A1c57%, dependingon their pharmacologic regime20. Even in Canada, a coun-try with an internationally acclaimed health system, theDiabetes Registry to Improve Vascular Events [DRIVE]revealed that scarcely 53% of T2DM patients were satis-factorily reaching the A1c goal. The percentage keepingA1c under the 7% limit for the entire 12 month follow-upwas 39%21. Finally, in a 5 year survey that focused ondeveloping countries from Asia, Eastern Europe andLatin America (International Diabetes ManagementPractice Study – IDMPS), and enrolled 9901 patientswith T2DM, the overall rate of achievement of A1c57% was 36.4%22.
In EDGE–Latin America, when vildagliptin was addedas a second anti-diabetes agent, 60.3% of patients success-fully reached the primary endpoint of a decrease in A1c40.3% without peripheral edema, hypoglycemia, discon-tinuation due to GI side-effects or an increase in bodyweight �5%. The proportion of patients who started thestudy with an A1c47% and went on to reach an A1c57%after 12 months without weight gain�3% or proven hypo-glycemia was 44.8% in the vildagliptin cohort. The ORsshowed significantly greater odds of achieving the compos-ite goals with vildagliptin therapies compared to all othercombination therapies. A sensitivity analysis limited topatients in whom the combination drug was metformin(metformin plus vildagliptin in the vildagliptin groupversus metformin plus any other oral anti-diabetic in thecomparator group), did not modify at all the central find-ing of the study. The percentage of participants whoachieved the primary endpoint was higher in the vildaglip-tin than in the comparator group in all participating coun-tries (data not shown). A growing body of evidencesuggests that when it comes to glycemic targets, ‘how’ toreach them may be just as important as ‘whether or not’ toreach them23–26. Within that context, EDGE–LatinAmerica found a considerably high rate of good glycemic
control without major adverse effects, with the use of vil-dagliptin-based therapies in patients of our biological andcultural type. This finding confirms and complementswhat has been observed in prior studies about the efficacyand effectiveness of vildagliptin27–32.
One of the main limitations of the study is the some-what heterogeneous group of patients, as the study sampleincluded participants from both specialized centers andprivate office doctors. This may have impacted the overallresults because of insufficient quality and missing datawhich needed to be excluded from the effectiveness ana-lyses. Another important consideration is that, being apost-hoc analysis, this report shares all the limitations ofsecondary analyses. Nevertheless, most of those methodo-logical concerns are relevant for studies of a small samplesize, in which subgroup imbalances and confounding canhave a greater impact in the observed results. To thateffect, it is important to point out that EDGE–LatinAmerica has a sample size larger than most clinical trialsor post-marketing analyses undertaken entirely in LatinAmerica up until now. It is likely that safety events wereunderreported, as their detection and reporting was basedon a voluntary scheme. It is important to note, however,that this is the most widely used method to identify adverseevents of new drugs in clinical practice28. Overall, therates of adverse events were low and similar between treat-ment cohorts. The open design of the study allowed doc-tors to select any drug based on their clinical judgment, butthis (plus the exclusion of patients on other DPP-4 inhibi-tor therapy) resulted in an imbalance in treatment armsfavoring the novel drug of the sponsoring company.Nevertheless, the comparator group was still fairly numer-ous, and the differences between groups did not alter theodds of the primary endpoint in a multivariable analysis.
Conclusion
EDGE–Latin America found that over a 1 year follow-uptimeframe and under usual care conditions, patients withT2DM who received vildagliptin as a second-line therapywere more likely to successfully lower A1c to57% withoutweight gain, hypoglycemia or peripheral edema thanpatients who received comparator oral anti-diabetesdrugs. Because of its effectiveness, cost and cumulativeexperience with its use, metformin will continue to bethe mainstay of pharmacological T2DM treatment. Theresults of EDGE–Latin America show that, under usualpractice conditions in our countries, vildagliptin is aneffective and safe add-on therapy to metformin.
TransparencyDeclaration of fundingThis study was funded by Novartis Pharma AG. The sponsor andsteering committee had equal roles in determining study design,
Current Medical Research & Opinion 2014
! 2014 Informa UK Ltd www.cmrojournal.com Vildagliptin combination effectiveness in Latin America Mendivil et al. 7
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
08/
25/1
4Fo
r pe
rson
al u
se o
nly.

protocol finalization and data interpretation. The funderwas involved in study design and data collection but didnot have involvement in data analysis, decision to publishor preparation of the manuscript. All authors had final responsi-bility for the data, content, and decision to submitfor publication.
Declaration of financial/other relationshipsJ.A. has disclosed that he was an employee of Novartis AG at thetime of execution of this study. O.S. has disclosed that she is aconsultant to Novartis AG. C.O.M., E.M.-R., I.D.A., G.P. andC.R. have disclosed that they have no significant relationshipswith or financial interests in any commercial companies relatedto this study or article.
CMRO peer reviewers on this manuscript have no relevantfinancial or other relationships to disclose.
AcknowledgementsThe authors thank Carlos Garcıa and Marcia Kayath fromNovartis Latin America, as well as Roberto Altamira fromNovartis Mexico for their support and commitment to the exe-cution of this study.
References1. IDF. Diabetes Atlas 2012. Available at: www.idf.org/diabetesatlas. Last
accessed 05 June 2014
2. Barcelo A, Aedo C, Rajpathak S, Robles S. The cost of diabetes in Latin
America and the Caribbean. Bull World Health Organ 2003;81:19-27
3. Pedersen O, Gaede P. Intensified multifactorial intervention and cardio-
vascular outcome in type 2 diabetes: the Steno-2 study. Metabolism
2003;52:19-23
4. Ali MK, McKeever-Bullard K, Saaddine JB, et al. Achievement of goals in U.S.
diabetes care, 1999–2010. N Eng J Med 2013;368:1613-24
5. Lavalle-Gonzalez FJ, Chiquete E, de la Luz J, et al.; IDMPS-3W collaborative
group (Mexico). Achievement of therapeutic targets in Mexican patients with
diabetes mellitus. Endocrinol Nutr 2012;59:591-8
6. UK Prospective Diabetes Study Group. Effect of intensive blood-glucose
control with metformin on complications in overweight patients with type 2
diabetes (UKPDS 34). Lancet 1998;352:854-65
7. UK Prospective Diabetes Study Group. Intensive blood-glucose control
with sulphonylureas or insulin compared with conventional treatment
and risk of complications in patients with type 2 diabetes (UKPDS 33).
Lancet 1998;352:837-53
8. Holman RR, Paul SK, Bethel MA, et al. 10-year follow-up of intensive glucose
control in type 2 diabetes. N Engl J Med 2008;359:1577-89
9. Inzucchi SE, Bergenstal RM, Buse JB, et al. Management of hyperglycemia in
type 2 diabetes: a patient-centered approach: position statement of the
American Diabetes Association (ADA) and the European Association for the
Study of Diabetes (EASD). Diabetes Care 2012;35:1364-79
10. Schwartz D, Lellouch J. Explanatory and pragmatic attitudes in therapeutical
trials. J Clin Epidemiol 2009;62:499-505
11. Treweek S, Zwarenstein M. Making trials matter: pragmatic and explanatory
trials and the problem of applicability. Trials 2009;10:37
12. Ware JH, Hamel MB. Pragmatic trials – guides to better patient care? N Engl J
Med 2011;364:1685-7
13. Mathieu C, Barnett AH, Brath H, et al. Effectiveness and tolerability of second-
line therapy with vildagliptin vs. other oral agents in type 2 diabetes: a real-life
worldwide observational study (EDGE). Int J Clin Pract 2013;67:947-56
14. Bennett WL, Maruthur NM, Singh S, et al. Comparative effectiveness
and safety of medications for type 2 diabetes: an update including
new drugs and 2-drug combinations. Ann Intern Med 2011;154:602-
13
15. Roumie CL, Hung AM, Greevy RA, et al. Comparative effectiveness of sulfo-
nylurea and metformin monotherapy on cardiovascular events in type 2 dia-
betes mellitus: a cohort study. Ann Intern Med 2012;157:601-10
16. Luongo AM, Lopez-Gonzalez E, Garcia AB, et al.; en nombre del Grupo
FRADYC. Evaluacion del tratamiento de la Diabetes Tipo 2 realizado por
especialistas en Argentina. Rev ALAD 2011;1:78-87
17. Alvarenga RL, Molina JM, Gochez N, Rodrıguez PA. Caracterizacion de
pacientes que asisten al programa de clınicas metabolicas del Instituto
Salvadoreno del Seguro Social. Rev ALAD 2012;3:310-19
18. Navarro-Vidal B, Banegas JR, Leon-Munoz LM, et al. Achievement of cardi-
ometabolic goals among diabetic patients in Spain. A nationwide population-
based study. PLoS One 2013;8:e61549
19. Ali MK, Bullard KM, Saaddine JB, et al. Achievement of goals in U.S. diabetes
care, 1999–2010. N Engl J Med 2013;368:1613-24
20. Ji LN, Lu JM, Guo XH, et al. Glycemic control among patients in China with
type 2 diabetes mellitus receiving oral drugs or injectables. BMC Public Health
2013;13:602
21. Braga MF, Casanova A, Teoh H, et al.; Diabetes Registry to Improve Vascular
Events [DRIVE] Investigators. Poor achievement of guidelines-recommended
targets in type 2 diabetes: findings from a contemporary prospective cohort
study. Int J Clin Pract 2012;66:457-64
22. Chan JC, Gagliardino JJ, Baik SH, et al.; IDMPS Investigators. Multifaceted
determinants for achieving glycemic control: the International Diabetes
Management Practice Study (IDMPS). Diabetes Care 2009;32:227-33
23. Duckworth W, Abraira C, Moritz T, et al.; VADT Investigators. Glucose control
and vascular complications in veterans with type 2 diabetes. N Engl J Med
2009;360:129-39
24. ADVANCE Collaborative Group, Patel A, MacMahon S, Chalmers J, et al.
Intensive blood glucose control and vascular outcomes in patients with
type 2 diabetes: the ADVANCE collaborative group. N Engl J Med
2008;358:2560-72
25. Duckworth WC, Evans GW, Gerstein HC, et al. Intensive glucose control and
macrovascular outcomes in type 2 diabetes. Diabetologia 2009;52:2288-98
26. Abraira C, Duckworth WC, Moritz T; VADT Group. Glycaemic separation and
risk factor control in the Veterans Affairs Diabetes Trial: an interim report.
Diabetes Obes Metab 2009;11:150-6
27. Bader G, Geransar P, Schweizer A. Vildagliptin more effectively achieves a
composite endpoint of HbA1c57% without hypoglycaemia and weight gain
compared with glimepiride after 2 years of treatment. Diabetes Res Clin Pract
2013;100:e78-81
28. Bolli G, Dotta F, Colin L, et al. Comparison of vildagliptin and pioglitazone in
patients with type 2 diabetes inadequately controlled with metformin.
Diabetes Obes Metab 2009;11:589-95
29. Bolli G, Dotta F, Rochotte E, Cohen SE. Efficacy and tolerability of vildagliptin
vs. pioglitazone when added to metformin: a 24-week, randomized, double-
blind study. Diabetes Obes Metab 2008;10:82-90
30. Ferrannini E, Fonseca V, Zinman B, et al. Fifty-two-week efficacy and safety of
vildagliptin vs. glimepiride in patients with type 2 diabetes mellitus inad-
equately controlled on metformin monotherapy. Diabetes Obes Metab
2009;11:157-66
31. Filozof C, Gautier JF. A comparison of efficacy and safety of vildagliptin and
gliclazide in combination with metformin in patients with type 2 diabetes
inadequately controlled with metformin alone: a 52-week, randomized
study. Diabet Med 2010;27:318-26
32. Garber AJ, Schweizer A, Baron MA, et al. Vildagliptin in combination with
pioglitazone improves glycaemic control in patients with type 2 diabetes fail-
ing thiazolidinedione monotherapy: a randomized, placebo-controlled study.
Diabetes Obes Metab 2007;9:166-74
Current Medical Research & Opinion 2014
8 Vildagliptin combination effectiveness in Latin America Mendivil et al. www.cmrojournal.com ! 2014 Informa UK Ltd
Cur
r M
ed R
es O
pin
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f W
ashi
ngto
n on
08/
25/1
4Fo
r pe
rson
al u
se o
nly.