Embed Size (px)
Citation preview

Community Forum
REHOBOTH MCKINLEY CHRISTIAN HEALTH CARE SERVICES
February 12, 2014
2
RMCHCS Board of Trustees-Officers
• Priscilla Smith, Chair; Business Owner – 2006• Kathy Head, RN, MSN, Vice Chair; Nursing Program Instructor–
2007• Yogash Kumar, Secretary; Business Owner, City Council
member – 2011• David Bischoff, Treasurer; Business Owner – 2009• Michelle Stam-MacLaren, MD, RMCHCS Chief of Staff;
Pediatrician – 2010
3
RMCHCS Board of Trustees-County Appointees
• Mary Ann Armijo, Media Executive – 2014• Dave Dallago, Business Owner – 2014• Brett Newberry, Professional Services Owner – 2014• Yogash Kumar, Business Owner, City Council member – 2011
4
RMCHCS Board of Trustees-Community Members
• David Bischoff, Business Owner – 2009 • Angelo DiPaolo, Public School Administrator (retired) – 2011• Jennifer Dowling, Business Owner – 2009• Sue Eddy, Private School Department Manager – 2009• Kathy Head, RN, MSN, Nursing Program Instructor– 2007• John Luginbuhl, Pastor – 2012• Priscilla Smith, Business Owner – 2006• Shannon Tanner, Business Owner – 2009
5
RMCHCS AdministrationBarry L. Mousa, FACHEChief Executive Officer
High School: New Bremen, OhioBachelors Degree: Indiana University, IPFW, Ft Wayne, IndianaMasters Degree: Trinity University, San Antonio, TexasProfessional Certifications:
Certified Public Accountant (inactive)Board Certified Health Care Executive
Health Care Experience: Florida, Georgia, Illinois, Indiana, Louisiana, New Jersey, New Mexico, Ohio, Texas, Virginia
6
RMCHCS Administration
Robert Baker, Director of Plant Operations – 2011Ina Burmeister, Chief Development Officer – 2008Bart Hansen, Chief Financial Officer – 2011John Mezoff MD, Chief Medical Officer – 2013Mike Nye – Vice President, Professional Services and Compliance Officer – 1983
Nancy Santiesteban – Chief Nursing Officer – 1998Kimothy Sparks – Chief Quality Officer – 2013Tracy Towns – Chief Human Resources Officer - 2012
7
RMCHCS Department DirectorsJim Bancuk – Clinic Operations - 2013Larry Booker – Diagnostic Imaging -
2009Donna Corley – Emergency Services -
1989Rosemary Coyne – Home Health/Hospice - 2010
Melinda Graton – Health Information Management (interim) - 2014
Phillip Hager – Patient Financial Services (interim) - 2013
Patty Johnson – Surgical Services (staff interim) - 1994
Harry Kallipolitis – Case Management - 2013
Misty Leyba – Medical/Surgical/ Pediatrics/ICU - 1998
Cassandra Lopez – Laboratory - 1997
Art Macias – Pharmacy - 1996Tom Gonzales – Information Technology -
1996Edward Placencio – Materials
Management - 1992Doug Turner –Cardiopulmonary, Physical
and Respiratory Therapy, Sleep Lab - 2008
8
Key Issues Being Addressed
• Revenue and Services• Medicaid Program Reimbursement Shortfall• Sole Community Provider Payment Program• Emergency Services• Decisions that Positively Affect the Medicaid
“Gap”• Critical Access Hospital Designation• East Campus
9
RMCHCS Services- Cardiopulmonary / Cardiac
Rehabilitation- Clinic Services—medical and
surgical specialties- Counseling - Outpatient
Behavioral Health - Diagnostic Imaging (MRI, CT,
Mammography, Ultrasound, X-Ray)
- Emergency Services- Home Health / Hospice-
- ICU- Laboratory- Medical / Surgical- Pediatrics- Pharmacy- Physical and Speech
Therapy- Respiratory Therapy- Sleep Lab- Surgery- Women’s Health
10
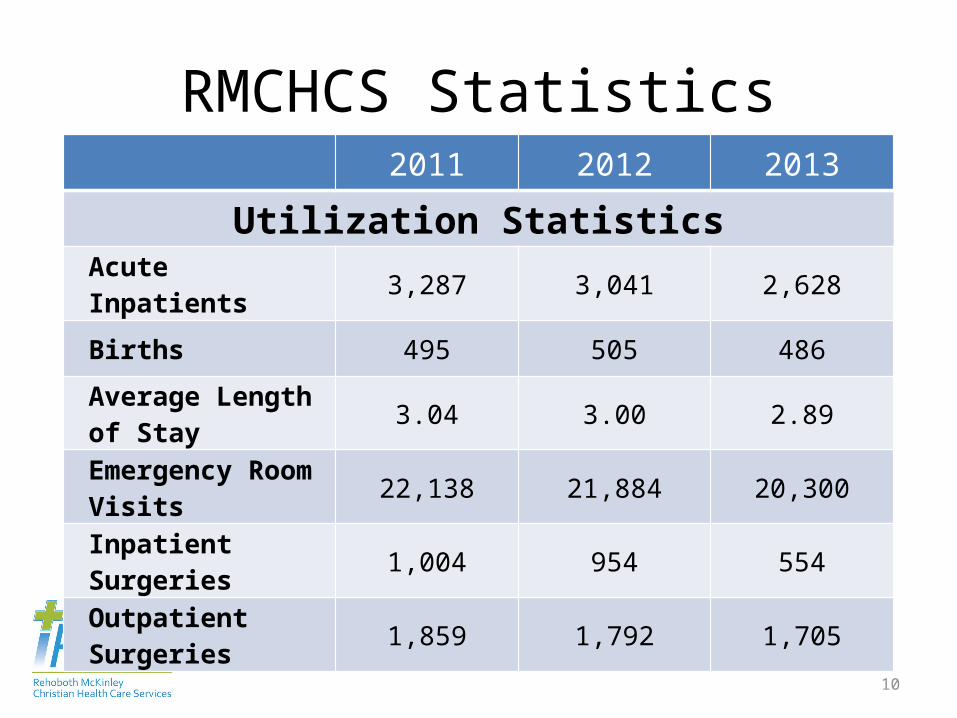
RMCHCS Statistics2011 2012 2013
Utilization StatisticsAcute Inpatients 3,287 3,041 2,628
Births 495 505 486
Average Length of Stay 3.04 3.00 2.89
Emergency Room Visits 22,138 21,884 20,300
Inpatient Surgeries 1,004 954 554
Outpatient Surgeries 1,859 1,792 1,705
11
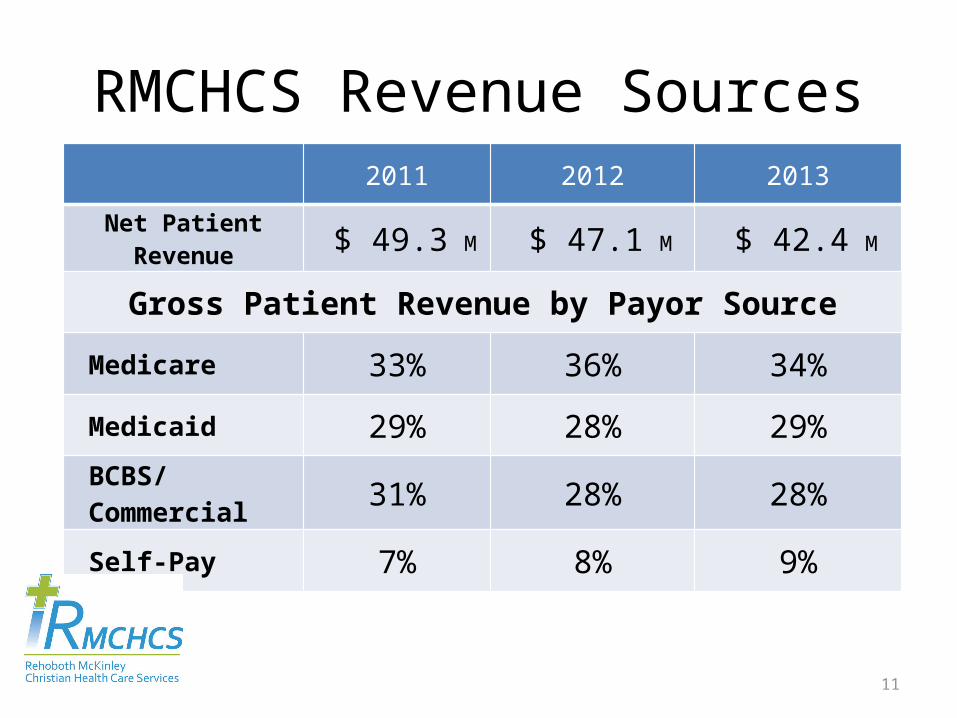
RMCHCS Revenue Sources2011 2012 2013
Net Patient Revenue $ 49.3 M $ 47.1 M $ 42.4 M
Gross Patient Revenue by Payor Source
Medicare 33% 36% 34%
Medicaid 29% 28% 29%
BCBS/Commercial 31% 28% 28%
Self-Pay 7% 8% 9%
12
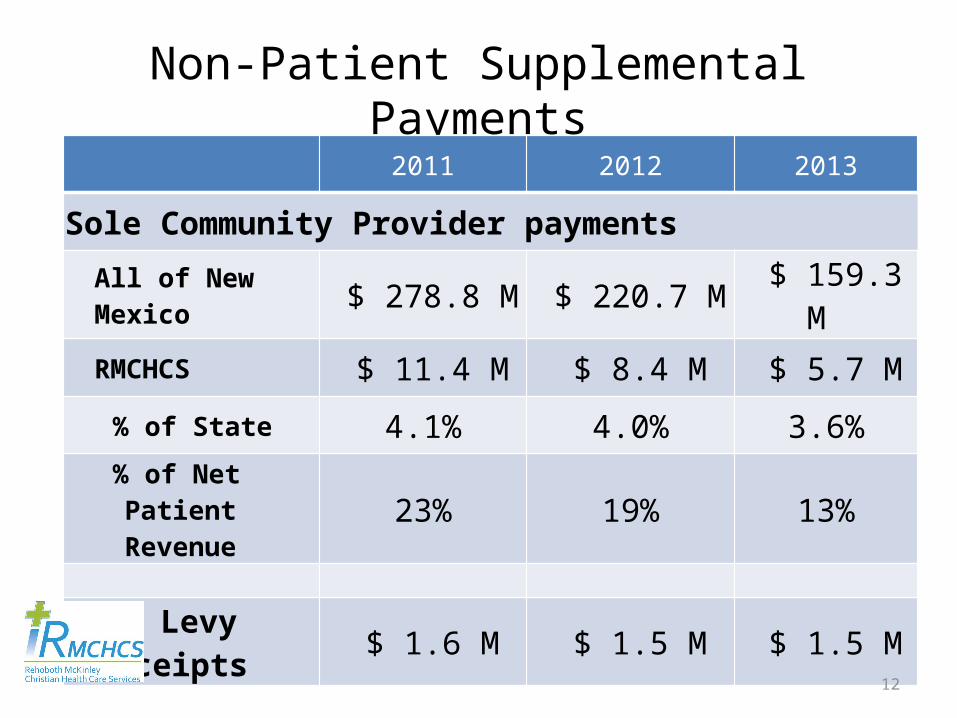
Non-Patient Supplemental Payments2011 2012 2013
Sole Community Provider payments
All of New Mexico $ 278.8 M $ 220.7 M $ 159.3 M
RMCHCS $ 11.4 M $ 8.4 M $ 5.7 M
% of State 4.1% 4.0% 3.6%% of Net Patient Revenue 23% 19% 13%
Mill Levy Receipts $ 1.6 M $ 1.5 M $ 1.5 M
13
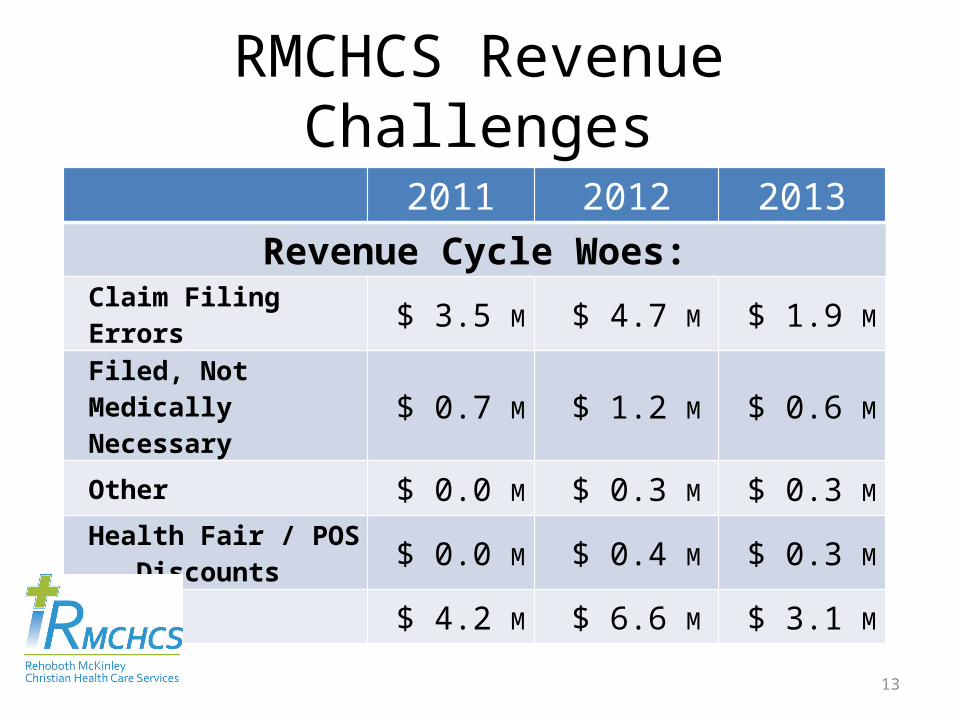
RMCHCS Revenue Challenges
2011 2012 2013Revenue Cycle Woes:
Claim Filing Errors $ 3.5 M $ 4.7 M $ 1.9 MFiled, Not Medically
Necessary $ 0.7 M $ 1.2 M $ 0.6 M
Other $ 0.0 M $ 0.3 M $ 0.3 MHealth Fair / POS
Discounts $ 0.0 M $ 0.4 M $ 0.3 M
Total $ 4.2 M $ 6.6 M $ 3.1 M
14
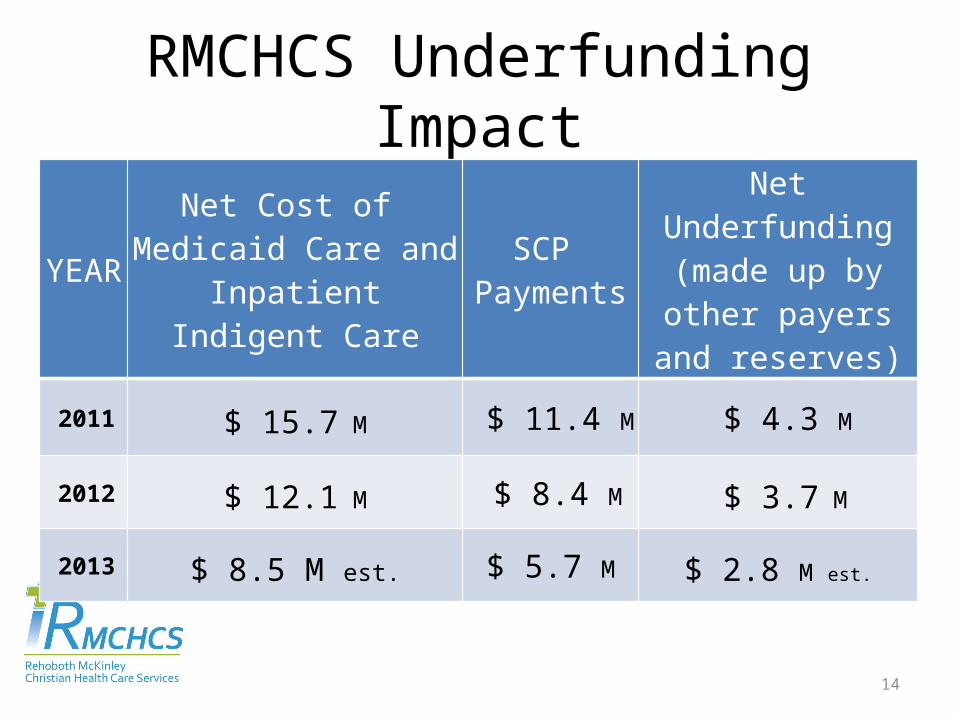
RMCHCS Underfunding Impact
YEARNet Cost of
Medicaid Care and Inpatient Indigent Care
SCP Payments
Net Underfunding (made up by other
payers and reserves)
2011 $ 15.7 M $ 11.4 M $ 4.3 M
2012 $ 12.1 M $ 8.4 M $ 3.7 M
2013 $ 8.5 M est. $ 5.7 M $ 2.8 M est.
15
Sole Community Provider Program -1
Since 1994 the Sole Community Provider program has been a core funding mechanism to supplement Medicaid payments for
many New Mexico hospitals
• June 2011—HSD suspends SCP payments o CMS alleges that sources of funds from counties were non-bona fide
donations or in-kind transfers from hospitalso SFY 2011 SCP total = $279M
• January 2012—HSD agrees to settlement with CMSo NM hospitals to repay $7.9M of CMS-calculated $53M overpayment
(for 2009). NMHA says $1B SCP overpayments for 2000-2008. o RMCHCS repays $843,000 for 2009 (SCP reduced $2.5M in SFY 2012) o SCP payments restored at a lower amount—SFY 2012 = $221M
16
Sole Community Provider Program -2
• December 2012—HSD suspends SCP paymentso 2nd time in 18 monthso CMS determines SCP payment errors in HSD’s historical calculationso CMS investigation jeopardizes entire SCP program
• May 2013—HSD agrees to settlement with CMS o SCP program transitions under Centennial Care waiver effective 1/1/14o CMS agrees to not review other years funding source and payment
calculations.
• January 2014—Centennial Care SCP program for 28 rural hospitals plus UNMH, if the underlying funds source is predictable and stableo Safety Net Care Pool (SNCP) program = $192.1M total amounto $68.9M for indigent care (maximum CMS would permit)o $132.2M for Medicaid Inpatient rate increase (HSD estimates ~75%)
17
Safety Net Care Pool Funding Plan• House Bill (HB) 350 and Senate Bill (SB) 368 establish
county gross receipts tax equivalency—generates $36.4M
• Governor Martinez proposes $9M of general state funds to augment county funding
• Total of $45.1M needed by state to maximize federal match—total funds $192.1M
18
Emergency ServicesEmergency Physician Providers contacted– Apogee– EmCare– Hospital Physician Partners (Lovelace Health System
provider)
– Pegasus Emergency Management (CHS system provider)
– Presbyterian Hospital & Healthcare Services– Schumacher Group– University of New Mexico Medical Group
19
Three Ways to Positively Affect the “GAP” in MEDICAID reimbursement
• Reduce overall costs of operations—– costs for the proportionate share of Medicaid will be
reduced
• Decrease Medicaid volume—– direct reduction on Medicaid costs, reimbursement gap,
and losses
• Increase revenue from non-Medicaid volume—– profit generated from these services will reduce the
Medicaid reimbursement gap
20
Increasing Medicare Reimbursement by Critical Access Hospital Designation -1
• Critical Access Hospitals (CAH) receive cost-based reimbursement from Medicare versus prospectively determined inpatient and outpatient fixed reimbursement rates.
• Some hospitals find that cost-based reimbursement is advantageous, and some will not. Each hospital must perform its own financial analysis.
• The Critical Access Hospital program is a Medicare reimbursement status only.
• Critical Access Hospital is a change in hospital provider designation for Medicare, and not a downgrade.
21
• Conversion to Critical Access Hospital (CAH) status does not mean losing services. Many hospitals can expand services knowing that Medicare costs will be 100% reimbursed.
• CAHs must maintain an annual average length of stay of 96 hours or less for their acute care patients.
• CAHs may have a maximum of 25 acute care inpatient beds.
• CAHs must provide 24-hour emergency services.
• As of June 30, 2013, there are 1,332 certified Critical Access Hospitals located throughout the United States and nine in New Mexico.
Increasing Medicare Reimbursement by Critical Access Hospital Designation -2
22
East Campus Changes• Behavioral Health Services (BHS) Service Lines
o inpatient addictions recovery programo outpatient individual therapy counseling
• The BHS service lines have lost significant money for many years. Medicaid volume in Addictions Program = 94% in 2013
• The buildings at East Campus are aging and very expensive to maintain
• Inpatient Addictions Recovery program closing 2/28/14
• Outpatient Therapy Counseling relocating to Main Campus on Red Rock Drive
23
Rehoboth McKinleyChristian Health Care Services










![Personnel. McK[inley] Trip July 1967 Bill Babcock, …...1 Personnel. McK[inley] Trip July 1967 Bill Babcock, leader of sorts, well meaning Leo Hammon *[left trip] July 14 Gayle Nienhauser](https://img.pdfslide.us/doc/110x75/5ea7034d7c62e3380325eb24/personnel-mckinley-trip-july-1967-bill-babcock-1-personnel-mckinley-trip.jpg)