-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
1/49
Common Epilepsy Syndromes
Encountered in Everyday Practice
Paula Gerber, M.D.
Grand Rounds
Providence Portland Medical Center
January 21, 2009
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
2/49
Objectives
Review epidemiology of seizures andepilepsy
Review seizure and epilepsy terminology Review three common
epilepsy syndromes
and their typical presentations
Mesial temporal lobe epilepsyIdiopathic generalized epilepsy
*Psychogenic non-epileptic seizures*
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
3/49
Epidemiology
~10 % of people will have a seizure some
time in their life
~0.5-1% of the population has epilepsy
Defined as 2 or more unprovokedseizures
Partial-onset ~60%
Generalized-onset ~40%
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
4/49
Classification of Seizures
Generalized
Partial
Simple
Complex
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
5/49
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
6/49
A word about absence
seizures Absence seizures are seen in specific,
childhood and adolescent-onset epilepsy
syndromes
Petit mal seizure=absence seizure
Typically very brief staring spell,
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
7/49
Partial seizures
Simple partial seizure=aura
Depends on the cortical area from which it
arises Neocortex: somatosensory and motor symptoms
Limbic structures: rising epigastric sensation, smell,taste,
fear, dj vu, jamais vu
Can be sensory or motor Motor can be tonic or clonic
Consciousness ispreserved
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
8/49
Partial seizures
Complex partial seizure
Again, depends on the cortical area from which
it arisesConsciousness is impaired
This can sometimes only be manifest as amnesia forthe event
Can have aura (simple partial seizure) thatevolves into complex
partial seizure
Can have secondarily generalized convulsions
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
9/49
Classification of Epilepsy
Generalized vs. Localization-related
Idiopathic, Symptomatic, or Cryptogenic
Idiopathic: idio=ones ownpath=disease
Translation: genetic mutation
Symptomatic: from a known cerebral insult or
degenerative processCryptogenic: presumed symptomatic, but
no
evidence of an insult can be found
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
10/49
Case #1
23 yo LH male presents to establish care.
PMH: Epilepsy beginning in adolescence.
He reports a history of febrile seizures as an
infant, but then remained seizure free until
the age of 13, when he began having
recurrent seizures. I have big ones and little ones.
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
11/49
Case #1 cont.
Little ones: a sensation of dj vu, followed by
spacing out. Family reports lip smacking,
staring, and fumbling with hands. Afterward, he isconfused and
does not recall what happened. The
episodes last ~1 minute and occur 3-4 times per
week.
Big ones: a few times per year, he has the abovesymptoms
followed by a generalized convulsion.
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
12/49
Case #1 cont.
Medications: oxcarbazepine (Trileptal) and
lamotrigine (Lamictal)
Past medications: phenytoin (Dilantin),
carbamazepine (Tegretol), valproate
(Depakote)
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
13/49
Case #1 cont.
SHx: The patient works as a checker at WalMart,
but he is in danger of losing his job due to
frequent seizures at work. He is unable to drive.He performed
poorly in school and reports
difficulty with concentration and memory. He is
single and lives with his parents.
FHx: Uncle had seizures; pt does not know details.
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
14/49
Case #1 cont.
Exam shows slight flattening of R
nasolabial fold and subtle reduced finger
tapping on the R
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
15/49
VIDEO
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
16/49
Mesial Temporal Lobe Epilepsy
AKA: temporal lobe epilepsy, psychomotor
epilepsy
Most commonly caused by mesial temporalsclerosis or hippocampal
sclerosis
Other causes: neoplasm, vascular
malformation, cortical malformations
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
17/49
Mesial Temporal Sclerosis
Most common cause of MTLE (estimated ~70%
of cases)
Risk factors: febrile seizures, perinatal insult, CNSinfection,
head trauma
Typically early insult +/- febrile seizures, followed
by latent period, then refractory seizures develop
in late childhood or adolescence
Is it the cause or the effect of seizures?
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
18/49
Mesial Temporal Sclerosis:
Pathology MRI shows a small, bright hippocampus
with disrupted internal architecture
Pathology shows loss of cells mostprominently in the CA1 region
of thehippocampus
Cell loss also occurs outside thehippocampus, hence the broader
termmesial temporal sclerosis
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
19/49
Mesial Temporal Sclerosis
EEG shows anterior and mid-temporal
spikes and intermittent temporal slowing
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
20/49
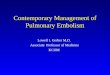
Kuzniecky R and Devinsky O(2007) Surgery Insight: surgical
management of epilepsyNat Clin Pract Neurol 3:673
681 10.1038/ncpneuro0663
Figure 1 Surgery for temporal lobe epilepsy
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
21/49
Mesial Temporal Sclerosis:
typical seizure Aura: rising epigastric sensation, also taste,
smell,
nausea, fear, dj vu, jamais vu
Staring, widened eyes, dilated pupils Lip smacking, chewing
Ipsilateral automatisms
Contralateral dystonic posturing
Postictal nose wiping
Patient may speak during the episode, but isamnestic to the
event afterward
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
22/49
Mesial Temporal Sclerosis:
typical seizureAutonomic signs and symptoms:
Abdominal sensationsApneaArrhythmias/bradyarrhythmiasChest
pain
CyanosisErythemaFlushingGenital
sensations/orgasmHyperventilationLacrimationMiosis/mydriasis/hippus
PalpitationsPerspirationPilomotor excitationTachycardiaUrinary
urgency/incontinenceVomiting
From Jerome Engel Jr., MD, PhD, Timothy A. Pedley MD,
eds.Epilepsy: A Comprehensive Textbook.
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
23/49
Mesial temporal lobe epilepsy:
the BAD news Typically refractory to medications
Seizures are frequent and debilitating,
interfering with ability to drive, work,maintain
relationships
Some patients develop significant post-ictalagitation and even
psychosis
Memory and cognitive problems developover time
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
24/49
The grim news about medications
Kwan and Brodie (2000):
525 new-onset epilepsy patients followed over 13
years 47% patients responded to 1stdrug
14% responded to a second or third drug
3% responded to combination therapy
Overall, 63% of patients were controlled with
medication
That means 37% of patients were refractory!
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
25/49
More grim news
AEDs have significant side effects:
Bone loss with phenytoin, carbamazepine, valproate
Hematologic, dermatologic and hepatic toxicity Birth defects
(especially valproate)
Renal stones: topiramate, zonisamide
Cerebellar degeneration, peripheral neuropathy, gum
hyperplasia with phenytoin Somnolence, ataxia, weight gain/loss,
tremor: many
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
26/49
Mesial temporal lobe epilepsy:
the GOOD news MTLE can be successfully treated with
surgery
The prototypical syndrome for surgicaltreatment of epilepsy
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
27/49
Mesial temporal lobe epilepsy:
the GOOD news Anterior temporal lobectomy or selective
amygdalohippocampectomy have been
shown to be effective, with seizure freedomrates of 60-80%
Bottom line: after failure of 2-3
medications, these patients should beevaluated for possible
surgery
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
28/49
Mesial Temporal Lobe Epilepsy
Dont let these patients slip through the
cracks!
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
29/49
Case #2
16 yo male presents to ED with new
generalized tonic-clonic seizure that
occurred while playing his new NintendoWii. On questioning,
admits to having had
some alcohol at the prom the night before.
Also, he has been sleep-deprived, up latestudying for
finals.
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
30/49
Case #2 cont.
Normal birth and development.
Meds: none
FH: A cousin had petite mal seizures as achild, but grew out of
them.
Exam: Normal.
ROS: Sometimes has jerks, especially inthe morning, which cause
him to dropthings. He thought he was just clumsy.
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
31/49
VIDEO--GTC
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
32/49
Video-absence
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
33/49
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
34/49
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
35/49
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
36/49
Idiopathic Generalized Epilepsy
Syndrome of generalized tonic-clonic,
myoclonic, and absence seizures=Juvenile
Myoclonic Epilepsy IGE also includes:
Childhood and Juvenile Absence Epilepsies,
Epilepsy with Generalized tonic-clonicseizures only
GEFS+
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
37/49
Idiopathic generalized epilepsy
Typically childhood or adolescent onset, butpatients can present
in young adulthood
Seizures are sensitive to alcohol use, sleepdeprivation, +/-
photic stimulation
Patients are otherwise NORMAL
Exam and MRI are NORMAL EEG shows generalized spike and wave
with a normal background
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
38/49
Idiopathic Generalized Epilepsy
Caused by genetic mutations in ion
channels
Many genes and inheritance patterns havebeen identified
Most likely IGE is a spectrum of
phenotypes caused by many differentgenotypes
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
39/49
Idiopathic generalized epilepsy
Important clinical pearl: phenytoin andcarbamazepine are
CONTRAINDICATED
and may make seizures worse Other meds that are considered to
be
contraindicated are: oxcarbazepine,gabapentin, tiagabine,
vigabatrin
Appropriate: Valproate, lamotrigine,topiramate, zonisamide,
levetiracetam
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
40/49
Case #3
26 yo woman presents with new onset
seizures x 6 months.
She describes multiple events:1) headache and tingly all
over
2) Shaking of arms and unresponsive
3) flop around like a fish
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
41/49
Case #3 cont.
Events can last from 30 minutes to several
hours, with a waxing and waning character
PMH: migraine headaches, fibromyalgia,irritable bowel syndrome,
depression
SH: Reports history of physical abuse by
stepfather as a child and more recently byex-husband.
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
42/49
Case #3 cont.
Meds: Trileptal, Depakote, Lamictal,
Zoloft, Cymbalta, Flexeril, Percocet
ROS: C/o excessive fatigue, back and headpain, memory and
concentration problems,
depressed mood, panic attacks
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
43/49
VIDEO
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
44/49
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
45/49
Psychogenic Non-epileptic Seizures
Formerly known as pseudoseizures
I prefer non-epileptic events
5-20% of seizures in outpatients 10-40% of seizures in inpatient
monitoring units
History of previous abuse is common, as is a
history of psychiatric disease and chronicpain/fatigue
syndromes
Female>male
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
46/49
Psychogenic Non-epileptic Seizures
Distinguishing features:
Non-stereotyped
Long duration
Precipitated by stress or pain
Pelvic thrusting
Eye closure Pseudo-catastrophic presentation with very
frequent events, multiple ER visits
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
47/49
Psychogenic Non-epileptic Seizures
Eye closure: Chung et al (2006):
234 consecutive EMU patients
938 ictal events Eye closure had positive predictive value of
94% for
PNES
Sensitivity of 96.2% and specificity of 98.1%
Caveats: episodes without altered consciousness orsignificant
motor activity (unpublished observation)
Also helpful for non-epileptic, physiologic events
(e.g.syncope)
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
48/49
Psychogenic Non-epileptic Events
Treatment: get off toxic AEDs! They areoften contributing to
patients neurological
complaints. Be honest, address the problem, and refer
for psychiatric help
Bottom line: dont just keep adding AEDs,send these patients for
monitoring toconfirm the dx
-
7/21/2019 Common Epilepsy Syndromes Gerber-Gore 1 21 09
49/49
QUESTIONS?