Embed Size (px)
Citation preview

Commissioning Update – Specifications, Performance and
Funding
Ben Seale
January 2012

Current Position
• Draft specification for lead provider component has been completed – structure to be tested today by JCG and reported to SSP at end of month
• Ancillary specifications (e.g. Psychosocial Interventions, Medical Interventions) to be completed
• Proposed PBR structure – also to be considered by JCG and SSP
• Overall model simplified slightly• Finalised model to be tested via consultation with
stakeholders including service users, carer and providers during February for advertisement in late February / Early March

Original Proposed Model
Assessment, Care Planning, Case Management,Assertive outreach, Peer Support
Successful Treatment Completion
ReducedOffending
Employment
ImprovedHealth and Wellbeing
Residential Rehabilitation
PsychosocialInterventions
CommunityIntegration /ETE
Detoxification –Community or
Inpatient
SubstitutePrescribing
Detoxification –Community or
Inpatient
SelfReferral
HarmReduction
DIP
Hospital
Professionalreferrals
Family Interventions

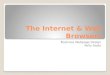
Revised Model
Lead ProviderSelfReferral
DIP
Hospital
Professionalreferrals
RECOVERYOUTCOMES
Interim -
Reduced substance misuse /
Abstinence
Improved H&WB-Injecting-- Housing
-BBV
Successful Treatment Completion
Sustained -
Reducedre-presentation
ReducedOffending
PsychosocialInterventions
ClinicalInterventions
Specialist Harm Reduction
e.g. Housing
e.g. Employment

Information Model – Single Reporting System to be managed
by lead
Referral Discharge
Early diagnostic indicatorse.g. Care plans etc.
Clinical modalities
Psychosocial Modalities
Outcome measures (1)
Outcome measures (2…)Multiple Episodes (re-presentation)

Lead Provider - Responsibilities• All interventions to be delivered in line with NICE Guidelines• Initial and comprehensive assessment – including setting Intervention
Package / Tariff and Clustering• Recovery focused care planning (encompassing both stabilisation and
abstinence pathways)• Pro-active case management / case conferencing• Access to residential placements• Hidden Harm / Safeguarding• Hospital In-Reach• Dual Diagnosis• Harm Reduction (A+I / Referral)• Peer Support and Mentoring• Assertive outreach and re-engagement• Access to mutual aid organisations• Specialist housing support for substance misusers• Community Integration and ETE• Specialist Family Support for Whole Family Approach• Ownership and Management of information system including outcome
measures

Clinical Provision - Responsibilities• All interventions to be delivered in line with NICE
Guidelines• Substitute prescribing• Detoxification – community and inpatient• General Healthcare Assessment and
Interventions• Communicable disease interventions – BBV
screening / immunisation• Expectations – rapid access (1 week) / HCA
(100%) / Reduction (90%) / Abstinence (90%) / Planned Exit (80%)

Psychosocial Provision - Responsibilities
• All interventions to be delivered in line with NICE Guidelines
• A range of evidence based interventions that can be utilised on a needs-led basis– Cognitive Behavioural Therapy– Motivational Enhancement Therapy– Social Network and Environment Based Therapies– Behavioural Couples Therapy– Structured Day Programmes
• Expectations – rapid access (1 week) / H&WB improvement (?%) / Planned Exit (80%)

Specialist Harm Reduction - Responsibilities
• All interventions to be delivered in line with NICE Guidelines
• Open Access – drugs / alcohol / PIEDs• Referral to treatment where appropriate• Advice and information• BBV screening and immunisation• Coordination of pharmacy needle exchanges• Collection of relevant data – e.g. for HPA• Expectations – rapid access (open access /
extended hours) / BBV uptake (?%) / Equipment Return Rate (80%)

Proposed Payment Structure
Operating Year
Main Payment
Interim Outcomes Payment
Sustained Outcomes Payment
2013/14 80% 20% 0%
2014/15 70% 20% 10%
2015/16 60% 20% 20%
Block Payment Planned DischargesH&WB
Reduced substance misuseAbstinence
Reduced re-presentationReduced Re-Offending

Financial considerations
• DIP budget has been reduced by 4% overall. However, the reduction is contained within the Home Office component of the budget – actual reduction equates to £20,183, leaving a total of £232,100
• The Department of Health will continue to pay their element of DIP funding as part of the Pooled Treatment Budget in 2012-13 – there is no anticipated change in this component
• Notification letter states “there will be a need to have regard for the incoming PCC when commissioning services and/or when entering into contractual agreements for 2012-13 and beyond”
• As such, commissioning plans may need to anticipate that the Home Office component will not be available

Financial considerations (2)
• Currently PTB allocations have not been published for 2012/13
• However, it is not currently anticipated that it will change
• Also, indicative public health budget for 2013 and beyond is not yet available

Discussion
- Validity of revised model- Chosen High Level Payment
Structure