Embed Size (px)
Citation preview


Colorectal Symposium
MPG Surgical Specialists
Albert Chung, MD
April 25, 2016

Agenda
• What is a colorectal surgeon?
• Overview of colorectal cancer staging
• Colorectal at MidMichigan Hospital, Midland
– Oncology initiatives
– Minimally invasive surgery
– Enhanced recovery after surgery (ERAS)

Colon and Rectal Surgeon
• ACGME1 accredited fellowship with review by the RRC2
• 1 year fellowship training – After completing general surgery (5 years)
• Training – Specialized operative procedures – Colonoscopy – Curriculum
• Board certification by American Board of Colon and Rectal Surgeons (ABCRS)
1Accreditation council for graduate medical education 2Residency review committee

Curriculum • Conditions:
– Benign • Anal/rectal abscess and anal
fistula • Rectal prolapse • Fecal incontinence • Hemorrhoids, anal fissure • Diverticulitis • Intestinal stomas • Colonic inertia
– Inflammatory bowel disease • Crohn’s disease • Ulcerative colitis
– J-pouch creation
– Malignant • Colon cancer • Rectal cancer • Anal cancer
• Procedures:
– Colonoscopy
– Anal manometry
– Rectal/anal ultrasound
– Open surgery
– Minimally invasive
• Laparoscopic
• Robotic

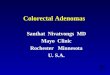
Colon and Rectal Cancer Staging
Adapted from NCCN guidelines Colon and Rectal cancer (3.2015).

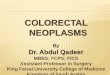
Colon and Rectal Cancer Staging

Staging the Easy Way…
• Stage 1
– T1 or T2, without N
• Stage 2
– T3 or T4, without N
• Stage 3
– Any N disease
• Stage 4
– Any M disease

Adapted from NCCN guidelines Colon and Rectal cancer (3.2015).

Clinical Staging
• Colon and rectal cancer – Complete colonoscopy with biopsy
– CT chest/abdomen/pelvis with oral and IV contrast
– Carcinoembryonic antigen (CEA), metabolic panel, CBC
• Additional: Rectal cancer – Proctoscopy
– Rectal ultrasound
– MRI of rectum
Treatment plan

Pathologic Staging
• Based on pathologic examination of surgical specimen
• Evaluation of primary tumor
• Evaluation of lymph nodes
– Minimum of 12 lymph nodes
Treatment plan

Colorectal in Midland • Hospital wide initiatives
– Clinic, OR, anesthesia, floor nursing, wound/ostomy care, physical/occupation therapy, nutrition, oncology…
• Center of Excellence of Colorectal Cancer – (Optimizing Surgical Treatment of Rectal Cancer) OSTRiCh
consortium – High volume centers
• Better survival, lower mortality, anal sphincter preserving procedure
– Oncology data reporting
• Tumor board – Every other week
– Attended by MidMichigan staff: • Medical and radiation oncologists, radiology, pathology, genetics

Colorectal in Midland
• Robotic surgery
– Better 3 dimensional visualization
– More precise instrument movement
– Elimination of human hand tremor
– Advantage: confined spaces such as pelvis
– 7 degrees of movement
– Superior ergonomics
– Shorter learning curve
– daVinci Xi arrival in 2016…


• Transanal minimally invasive surgery (TAMIS)
– Developed by: Attalah, Albert, Larach (2009)
• Florida Hospital
– Anus used as access port for laparoscopic surgery
– Surgical excision of rectal pathology without abdominal incision

Colorectal in Midland • Enhanced recovery pathway (ERAS)
– Initially developed by Kehlet, Fearon, Ljungqvist, et al. (2001)
– Standardization with evidence-based practices • Preoperative, intraop, periop, postop
– Goals of pathway: • Reduce stress, maintain physiology, enhance mobilization
Results: • Earlier return of bowel function
• Decreased LOS up to 2.5 days for open and laparoscopic cases
• Cost savings
• Considered safe: no sig. differences in readmission or mortality, lower total complications

Midland Colorectal ERAS Protocol • Clinic
– Education, nutrition, PT/OT, ostomy marking/education
• Preop – Mechanical and antibiotic bowel prep – Carbohydrate drink 2 hours before surgery – Ofirmev, gabapentin, robaxin – Transversus abdominal plane (TAP) block with exparel or bupivicaine – Intrathecal with morphine – Entereg
• Intraop – Minimal to none narcotics – Goal directed, fluid restriction
• Postop – Early mobilization – Early feeding – PCA, oral narcotics (eg percocet 7.5mg)

Current Results With ERAS • 42 total patients (25 robotic, 13 laparoscopic, 4 open)
– Admitted from outpatient, variety of pathology • Majority: IBD, colorectal carcinoma, diverticulitis
– Average age: 58.5 years (range: 26 to 81 years) – Average length of stay: 3.3 days (range: 2 to 9 days) – Number readmissions: 3
• inguinal hernia, fluid overload, ileus secondary to imodium
– Complications: • 1 urinary tract infection • 2 ileus • 1 alcohol withdrawal • 1 hyponatremia, postoperative bleeding • 1 reoperation for bowel obstruction from port site hernia
– Mortality: 0 – Conversion rate to open: 0

Length of Stay
• Right colectomy/ileocolic resection
– 8 cases, LOS: 2.5 days
• Left colectomy/Hartmann reversal/total colectomy (1)
– 12 cases, LOS: 2.9 days
• Proctectomy
– 14 cases, LOS: 4.4 days






Thank You
• Colorectal at MidMichigan Hospital, Midland
– Oncology initiatives
– Enhanced recovery after surgery (ERAS)
– Minimally invasive surgery
• Thank you to MidMichigan Midland Staff