Embed Size (px)
Citation preview

COLO-NEO-URETHROSTOMY A Diversion Operation for Urinary Incontinence
By HUGO GRANT, F.R.C.S.(Ed.) General Hospital, West Hartlepool
IN disease of the bladder, surgical use of segments of the bowel has been employed in three groups of cases.
In the first group the bladder has become contracted and is of such small capacity, as the result usually of tuberculous cystitis or Hunner’s cystitis, that enlargement has become necessary. In this group both the ureterovesical orifices and the sphincter mechanism of the bladder neck are intact and the problem is simply one of increasing the bladder volume. Isolated loops of bowel applied in various ways as tubes or with the loop opened as a flat graft are now standard procedures.
In the second group the whole bladder has been excised for carcinoma or sarcoma and a gap is left between the ureters and urethra. Both the ureterovesical junctions and the bladder-neck sphincter have been removed. Until the danger of electrolyte imbalance was appreciated the operation of transplantation of the ureters into the rectum or pelvic colon was the standard procedure.
The third group-with which we are concerned in this paper-is that in which there is incontinence of urine either as a result of damage to the sphincter mechanism or because of congenital deficiency. The ureterovesical junctions are intact and, with the exception of vesical exstrophy, the whole bladder is still present.
The operation which is at present most used in this last group is that of uretero-ileostomy. Because of the frequency of inadequate anal sphincters transplantation of the ureters into the rectum is not always satisfactory, even if one is prepared to ignore the possibility of electrolyte imbalance. Uretero-ileostomy is less likely to produce electrolyte imbalance as the bowel is used simply as a conduit, but it is not a simple operation; to divide the ureters across and reimplant them elsewhere, when the ureterovesical junctions are normal and intact, would seem to complicate the procedure unnecessarily.
Many years ago Maydl (1894) devised an operation for vesical exstrophy in which the trigone was anastomosed directly to the colon, thus preserving the ureterovesical junctions. This, however, was never practised widely, though Bax (1899) was able to collect twenty-five cases, ten of which were Maydl’s own. Follow-up of these cases was sketchy, but several of Maydl’s (1899) cases were still alive many years after the operation. Maydl (1899) was convinced of the importance of preserving the ureterovesical junctions.
Suprapubic cystostomy is unsatisfactory because of the need for a drainage tube, but operations avoiding a drainage tube have been devised with a loop of ileum as a conduit from the bladder to the abdominal wall and so allowing the use of an ileostomy bag. A loop of ileum whose mesentery arches over the uterus would appear to be liable to damage in the event of pregnancy and this would be particularly important in the first case, now to be described, as the girl was anxious to marry. These operations also have the disadvantage that leakage from the bladder neck, in spite of division and suturing, may be difficult to prevent. To avoid this leakage, Grfiths (1960), at the meeting of the British Association of Urological Surgeons in 1959, described an operation for young girls with spina bifida, in which the whole urethra was dissected out, and, after partial mobilisation and rotation of the bladder, the urethra was swung around to open on to the abdominal wall. A skin spout was then devised and an ileostomy bag fitted. The blood supply to the bladder is said to have been endangered sometimes by the mobilisation.
198

COLO-NEO-URETHROSTOMY 199
Glaser (1 960) also solved this problem of leakage by excising the wall of the bladder leaving only the trigone which was then anastomosed to an isolated loop of ileum-the other end being brought on to the abdominal wall.
Until recently the standard treatment of exstrophy of the bladder has been that of urinary diversion. Plastic operations to reconstruct the bladder and urethra are still in the experimental stage, though the results seem to be improving as better techniques are evolved. The procedure described by Lattimer and his co-workers (1960) is, however, a formidable one. In their hands
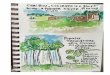
FIG. 1
This drawing illustrates the loop of pelvic colon attached at one end to the neck of the bladder and passing extraperitoneally to the stoma in the left hypogastrium. 1, Stoma. 2, Colonic loop.
3, Closed opening in lateral peritoneal leaf. 4, Bladder.
the operation takes six or eight hours and requires bilateral osteotomy of the iliac bones. He described twenty-eight cases with no mortality. One of the main problems is that of urinary incontinence, and two-thirds of the cases he had operated upon had not gained control at the time of writing. As, however, many of these children were still very young there is every hope that many of them will gain some degree of control as the years go by. About half of them still had urinary infection, two-thirds had a normal upper urinary tract, but nearly all the ureters showed reflux. Urinary fistula: and strictures had been a difficult problem.
Sturdy (1961), in an analysis of eighty-eight patients at Great Ormond Street, found very few cases which were fully continent after attempts to perform a functional reconstruction of the bladder and urethra, and he noted, as Swenson (1957) has also noted, that success is much less likely in the male child. In view, therefore, of the still experimental nature of the reconstruction operations, urinary diversion still remains the standard procedure.
The use of an isolated loop of pelvic colon has been advocated by Bourque of Montreal (1959) and Kuss of Paris (1959) as a bladder substitute, and while there would appear to be possible dangers of electrolyte imbalance in such procedures, there should be little danger if the loop were used as a colonic conduit only. These writers also prefer colocystoplasty to ileocystoplasty and a similar recommendation has been made by Goodwin and Winter (1 959).

200 B R I T I S H J O U R N A L O F U R O L O G Y
It seemed worth while, therefore, to devise an operation which would : 1. Preserve the ureterovesical junctions. 2. Avoid the complication of leakage from the bladder neck. 3. Avoid possible damage to the new arrangements in the event of pregnancy.
These criteria would be fulfilled by the use of an isolated loop of pelvic colon-one end anastomosed to the bladder neck and the other brought out on to the abdominal wall (Fig. 1).
CASE REPORTS Case 1.-The patient was a girl born on 12th July 1937. She had been attending hospital for a number of years with urinary trouble following an operation for spina
bifida in infancy. When first seen she was admitted with acute abdominal pain due to urinary infection. There was widespread inflammation and ulceration of the thighs and abdominal wall from ammoniacal dermatitis. Investigation showed bilateral hydronephrosis, a markedly trabeculated bladder and a residual urine of 10 02. Various procedures on the bladder neck reduced the residual urine to a few ounces only. Antibiotics cleared up the infection and in time her general condition vastly improved, the hydronephrosis regressed to normal-shaped excretory urograms, but the incontinence persisted.
In February 1960 she was submitted to the operation outlined above, after preparation with colonic antiseptics. Operation.-The abdomen was opened through a left paramedian incision. The bladder neck and urethra were
mobilised and the urethra was divided across close to the bladder. The resultant opening at the bladder neck was surprisingly large and required only a short upward incision to fit the calibre of the pelvic colon loop. The required length of loop was estimated by measurement in situ. An appropriate section of pelvic colon was isolated and continuity restored by anastomosing the proximal and distal ends of the remaining colon with two layers of interrupted silk sutures. A temporary czcostomy was performed. The peritoneum on the left side of the bladder was mobilised and the leaf so formed was divided down as far as the colon, thus allowing the loop of colon to be brought to the bladder neck without tension to its blood supply.
One end of the loop was sutured to the bladder neck by continuous catgut reinforced by a second row of interrupted sutures. The other end was brought out extraperitoneally, i.e., in front of the peritoneal flap, on to the abdominal wall of the left hypogastrium after excision of a disc of skin and aponeurosis. The stoma was secured by five Patey sutures. The incision in the peritoneal leaf was then sutured making the whole course of the loop extraperitoneal. This extraperitoneal route of the colon loop to the abdominal wall was the most convenient one, but is no doubt also a much safer one. The abdomen was closed with drainage to the extraperitoneal area. An adhesive plastic bag was attached to the skin over the colostomy. Convalescence was uneventful except that two weeks after the operation there was a little urinary leakage from the urethra. A week later the whole urethra was excised from below. She made an uneventful recovery thereafter and remained quite dry.
Progress.-She had never been able to go to school or have any sort of public life prior to this operation, but subsequently she took up employment and has since been married. An excretory urogram taken four months after operation showed no evidence of any back-pressure on either kidney.
Repeated estimations until the end of 1961 showed no gross biochemical abnormality. On one occasion only was the chloride elevated above normal.
Since the first operation in February 1960 two other cases have been operated upon. Case 2.-This girl, born on 22nd May 1947, has congenital absence of the lower part of the spine. The trunk
and upper limbs are fully developed, but the lower limbs are only partially developed. She was completely incontinent of urine. The degree of the deformity is shown in the X-ray, Figure 2. She is an intelligent girl with good parents who were anxious that this urinary incontinence could be controlled in such a way that she could obtain some form of employment. Although she was continent of faxes, the rectal sphincter was patulous and a rectal bladder was therefore out of the question. The absence of the lower spine meant that she took her weight on the middle of the lumbar area where her spine terminated and as a result there was vertical compression of the abdominal contents ; she had also considerable thickness of abdominal wall fat. Because of these two facts the siting of the abdominal wall stoma produced special difficulties and the need for a long conduit to traverse the great depth of the abdominal wall was clear. Her small undeveloped lower limbs were flexed and might have produced difficulties with a lateral stoma. It was therefore decided that the stoma would be better in the midline.
Excretory urogram showed no back-pressure. The bladder had a sugar-loaf appearance. On microscopic examination of the urine an occasional pus cell only was found.
On 28th September 1961 operation was undertaken. The abdomen was opened through a left lower paramedian incision. There was a considerable amount of superficial fat, the pelvis was small and narrow. A loop of pelvic colon was isolated and colonic continuity restored by end-to-end anastomosis with two layers of interrupted fine

COLO-NEO-URETHROSTOMY 201
silk sutures-a caxostoay being made to decompress the colon. The peritoneal leaf was divided vertically close to the left side of the bladder. The urethra was mobilised and divided. The distal end was ligated. A small vertical incision was made on to the anterior bladder wall to enlarge the opening which was then anastornosed to one end of the colonic loop with two layers of interrupted sutures, the inner ones being catgut and the outer ones fine silk.
FIG. 2 Excretory urogram in Case 2 six months after operation. There is no dilatation of the ureters or calyces. The absence of a sacrum, the imperfect lumbar spine and the narrow pelvis are seen.
The colonic loop was made to occupy an extraperitoneal position and the incision in the leaf of the peritoneum was closed over its mesentery. The suture was then continued upwards to close the peritoneum of the anterior abdominal wall. The muscle and skin were then closed, the free end of the colonic loop being brought out through the incision about halfway between the umbilicus and the symphysis and secured to the skin by five Patey sutures. A Foley catheter was passed down the lumen of the colonic conduit to the bladder as it was thought that the bag would not stick well over the incision, at least until it was healed.
The post-operative course was uneventful. The caecostoniy tube was removed seven days later and the Foley catheter in fourteen days. There was no leakage from the urethra. A urinal of the Rutzen type was then applied to the abdominal wall.
Excretory urograms six months after operation showed normal pyelograms and no dilatation of the ureters (see Fig. 2). Repeated blood chemistry examinations since operation have shown only one elevation of chloride above normal.
Case 3.-The third case on which colo-neo-urethrostomy was used was a qale child born on 18th March 1960 with vesical exstrophy. An excretory urogram showed a normal upper urinary tract. Blood urea was normal.
On 13th July 1961 operation was performed. The ureters were catheterised in order to make identification easy during dissection. An incision was made at the junction of the skin and the bladder epithelium round to the urethra on both sides. A vertical oblique incision was made from the right upper angle of the bladder towards the umbilicus (Fig. 3). The bladder was mobilised from the abdominal wall, this procedure being helped by opening the peritoneum. As much of the peritoneum as possible was stripped off the bladder and when the bladder was fully mobilised the
2 c

202 B R I T I S H J O U R N A L O F U R O L O G Y
r FIG. 3
The opening of the bladder appears larger in the drawing than in fact it was. The left-hand drawing illustrates the skin incision in Case 3. The right-hand drawing shows the closure.
FIG. 4
is some dilatation of the ureters. Excretory urograms in Case 3 nine months after operation. There

COLO-NEO-URETHROSTOMY 203 urethra was divided across just above the verumontanum. The bladder was now freed from a thick band of fibrous tissue running transversely behind the urethra and joining the bones of the pelvis. The bladder then dropped back into the pelvis.
A loop was now isolated from the pelvic colon, colonic continuity being restored by end-to-end anastomosis. The peritoneal leaf on the left lateral side of the bladder was divided vertically, care being taken to avoid the left ureter which ran transversely at this point. The peritoneum of the left iliac fossa was then stripped away to make an extraperitoneal route for the loop of colon. The bladder was now inverted and the distal end of the bowel was anastomosed to the opening of the bladder with one layer of interrupted catgut sutures. Tk ease with which it was possible to approximate the open end of the colon to the opening of the inverted bladder was surprising as it was thought, prior to mobilisation and inversion, that one would have to close the bladder partially before anastomosing the colon, but this was not the case. The proximal end of the loop was then passed up extraperitoneally and brought out through an opening in the left hypogastrium and sutured to the skin with Patey sutures. A crecostomy tube was then placed in the crecum.
The abdominal wall was now mobilised from the skin, and in the lower part where the rectus sheath and muscles were widely separated a vertical incision was made in the lateral part of the sheath and the aponeurotic flap thus made was turned towards the midline to assist in closing the gap. Before it was closed, however, the division in the left lateral peritoneal leaf was sutured over the mesentery of the colonic loop and this suture was carried upwards to close the anterior peritoneum. The abdominal wall was then approximated and the skin closed. The flap of skin made by the oblique vertical incision on the right side of the bladder was then brought down to fill the gap left by the displaced bladder (see Fig. 3). There was a small opening left at the bottom and just above the open urethra. It was hoped that an epithelialised cavity would form in this area and that the urethra distal to the verumontanum and ejaculatory ducts could subsequently be reconstructed. Neomycin had been given pre-operatively to depress the colonic flora and this was continued for four days. A short course of Achromycin was also given.
Convalescence was uneventful. He was discharged home on 28th August with an ileostomy bag adherent to the skin.
When last seen, in April 1962, an excretory urogram showed no back-pressure on either kidney though the lower ureters were slightly dilated (Fig. 4). Blood chemistry was within normal limits. The abdominal wall has remained firm with no evidence of herniation of the abdominal contents.
SUMMARY 1. An operation has been described in which an isolated loop of pelvic colon has been used
to provide an extraperitoneal colonic conduit between the bladder neck and the abdominal wall. 2. It is a procedure surgically less radical and technically less complicated than most of the
standard diversionary operations hitherto described. 3. It appears to be a safe operation, and in the three cases described there was in each a
simple uneventful convalescence, apart from the temporary difficulty in the first case.
REFERENCES
BAX, quoted by BURCKHARDT, E. (1899). Jber. ges. Med., 34, Bd. 11, 498-542. BOURQUE, J. P. (1959). Brit J . Urol., 31,448. GLASER, S . (1960). Proc. R. Soc. Med., 53, 354. GOODWIN, W. E., and WINTER, C. C. (1959). Surg. Gynec. Obstet., 108, 370. GRIFFITHS, I. H. (1960). Brit. J . Urol., 32, 27. Kuss, R. (1959). J. Ural., 82, 587. LATTIMER, J . K., DEAN, A. L., DOUGHERTY, L. J., Ju, D., RYDER, C., and USON, A. (1960). J.
Urol., 83, 647. MAYDL, K. (1894). Wien. med. Wschr., 44, 1113, 1169, 1209, 1256, 1297. ~ (1899). STURDY, D. E. (1961). Brit. J. Urol., 33, 266. SWENSON, 0. (1957). Surgery, 42, 61.
Wien. med. Wschr., 49, 249, 304, 360.
Addendum.-The first patient has recently been delivered of a normal healthy child v i ~ naturales. Pregnancy was uneventful apart from a brief attack of retention of urine which was relieved by a hot bath. There was a urinary infection at that time, but this has since been cleared by antibiotics. The labour itself was uneventful. She was delivered with forceps after twenty-five minutes in the second stage. Puerperium so far has been quite uneventful. Blood urea and creatinin were within normal limits. The urine is free of infection.