Embed Size (px)
Citation preview

,gen des Menschea und,[3; Abt. 2, 1909-1912;
¯ emitSt. Zeitschr. f.
19-424, 1932.the Feet of 1,054
)ints Associated with43, 1942.,’oot. Anat. Rec., 96:
586-602, _,Nov. 1921.’.ular Coalition by
ain Forms of Accidemai
(()s lunatotriquetrum)
:ies of the Hand in
helle beim F6tus.
tcture. New York,
n. J. Hered., 39: 23-27,nee. Contrib. Emb.,
.tbility. Bull. Hist.
Associated with Pain in
accessorischer
o the III Metacarpal;
gensen. Copenhagen,
~. J. Anat., 17:3: 480-530, 1929.to Iniury. J. Am. Med.
Spastic Flatfoot. J.
ereditar~
z-283, 1940.idism. Am. J. Dis.
¯ Bone and Jc
, 34~ 102-114, 1950.
¯ 01," BONE AND JOINT
COLLES’ FRACTURE
STUDY OF Two THOUSAND CASES FI?~ON[ THE ~YE~,V YORK STATE WORKMEN’S
COMPENSATION BOAR][) *’~
BY ROBERT W. BACORN, M.D., AND JOHN F. KL-R’rZKE, M.D., NEW YORK, N. Y.
Colles’ fracture, a common injury, is usually co:asidered to be rather trivial and isdelegated to the orthopaedic neophyte for treatment. It is the purpose of this paper
.~ a large number of such fractures, with the emphasis being piaced on final results
their contributory factors.Ye have defined Colles’ fracture as a complete transverse break of the distal one inchradius with dorsal displacement of the distal fragment ; non-displaced h’actures were
in~.luded. A considerable number of fractures showed commim~tion, impaction, or
tension into the radiocarpal joint.
METHODS AND MATERIAL
The Workmen’s Compensation Board files of t:he New York State Department of(New York City District) contain some 1,400,000 cases at any one time, which~nt the claims folders for the previous ten years. These are catalogued on Interna-Business Riachine cards under a number of keys, permitting rapid tabulation of
[es’ fracture cases. The medical section of each case folder contains the treating" .ian’s initial report of injury and therapy, with fuller details in a report made two
later; it also contains the progress notes, discharge note, details on %Vorkmen’s~ensation Board examinations, x-ray reports, reports of insurance-physician’s ex-
and, where pertinent, consults,nt reports and death reports. There is also theof the final Workmen’s Compensation Board examination with a detailed descrip-
functional and anatomical findings, and the decision of the Board as to thedisability in percentage of loss of function of the hand.
the years investigated, all case folders, to the number of 5,000, classified under
fracture fracture of the wrist, and [racture of the radius, were obtained; the latter,ns contained a large number of Colies’ fractures. Then the Colles’ fracture
were tabulated; completeness of data was the sole requirement for inclusio[~:of administrative details, only h~Jf of the cases from 1946, 1947, and ]948 were
All of the cases from 1945 and ]949, whether included in our main tabulationswere listed as to the type of fracture. Some further cases were drawn from the
1941 files; the war years were largely omitted to avoid prejudice in our correla-there was no significant difference between the cases o~ 1945 (injuries 0f
of 1949 (injuries of 1948). Fractures of the carpus in these two years were also
tabulation for each case of Colles’ fracture consisted of: (I) case m~mber; (2) (4) involved limb; (5) Workmen’s Compensation Board’s final estimation
of disability (percentage of loss of function of the hand) ; (6) functional supination, palmar flexion; dorsifiexion, lateral mobility, and exact defects
) as none, mild, moderate, marked, or complete; (7) diminution of gripmoderate, marked, or complete) ; (8) nature of fracture (simple or compound,
~ Bacorn and Kurtzke to the %Vorkmen’s Compensation Board. The conclusionsthose of the authors and do not necessarily represent the opinions or policy of the Workmen’s
This paper is published with the permission of Miss Mary Donlan, ChaPman of theCompensation Board
study was made possible u~der an appropriation to the Ne~vYork State Workmen’s Compensa-and was written under the supervision of Dr. Willis M. ~Veeden, Medical~Director of the Work-
Board.
NO. 3. ~LY 1953 643

644 R. ~V. BACORN AND J, F. KURTZ]~:E
impacted, comminuted, or into the radiocarpal joint); (9) degree of residual deformity(none, enlargement, or mild, moderate, or marked deformity); (10) involvement of ulnar styloid (with or without union); (11) mechanism of injury; (12) treatment reduction, anaesthesia, duration of immobilization, type of physical therapy if given,and duration); (13) sequelae and complications; and (14) time between injury and final disability award.
The total number of eases thus studied was over 2,100, but obviously not everyfactor could be evaluated in each ease. There were in addition some 1,100 radioearpalfractures other than Colles’ which were listed as to anatomical type.
DISCUSSION OF DATA
In the two years studied most thoroughly (1945 and 1949), Colles’ fracture was foundto constitute by far the most frequent individual fracture of the radius. In 1945, therewere 650 Colles’ fractures out of 1,071 radial fractures; in 1949. 662 Colles’ fractures werefound in 1.].18 radial fractures. This gives a total of 1.312 Colles’ fractures out of 2,189fractures of the radius--an incidence of 60 per cent. (Chart II). The next most frequentclass of fractures was that of the radial head (proximal) with an incidence of 14 per cent.(306 eases). Fractures of the shaft of the radius extending from the neck to within one inchof the radiocarpal articulation constituted 6.2 per cent. or 136 of these 2,189 radial frac-tures. The remaining 19.8 per cent. were fractures other tlhan Colles’, although they oc-curred within one inch of the joint: 132 eases (6 per cent.) were fractnres of the radialstyloid; 22 (1 per cent.) were Smith’s fractures, that is, "reversed Colles’ fractures";and 12.8 per cent. were of a heterogeneous group which included fissure fractures, trans-verse fractures (whether incomplete or non-displaced), and[ chip fractures.
It was impossible for us to determine an accurate incidence of Colles’ fracture amongthe general population, since no figures were available on the total number of workerscovered by the Workmen’s Compensation Law. However, we were able to determinethe incidence of Colles’ fracture among all Workmen’s Compensation Board cases for theyears of 1945~ and 1949~, in which there were 1,312 eases of Colles’ fracture out of 133,764Workmen’s Compensation Board eases in the New York C, ity District -- an incidence of0.98 per cent. The frequency in 1945 was 1.02 ~Jer cent.; in 1949 it was 0.95 per cent.
During this study it was also possible to determine the distribution of fracturesof the carpus (Chart II). In these same years (1!)45 and 1949) there were 408 fractures the carpal bones, or less than one-fifth the number of radial fractures and one-third thenumber of Colles’ fractures. Of these, thirty-one were undifferentiated, but among the
"remaining 377 carpal fractures, that of the navieular constituted 70.8 per cent. (267eases). The next most frequent fracture was that of the triangular (14.3 per cent. or riftfour eases); then came fracture of the lunate (5.6 per cent. or twenty-one.~eases). remaining five bones accounted for but 9.3 per cent. There were eight fractures (2.1per cent.) each of the pisiform, the greater multangular, and the hamate, as well as nine(2.4 per cent.) of the eapitate, with but two fractures (0.5 per cent.) of the lesser multan-gular. Some of these carpal fractures were multiple.
It was interesting to note that Colles’ fracture, the mechanism of which demandstransmission of the force through the carpus, was accompanied by but ten fractures of thenavieular (0.5 per cent.) ; no other carpal bone was so involved.
In the years 1945 and 1949, 700 fractures, comprising 58 per cent. of a total of1,206 eases, occurred in males, whereas 42 per cent. (506 eases) were found in females.:~
The ratio in either year was the same as their other, but for our total of 2,115fractures the incidence was 56.5 per cent. male to 43.5 per cent. female. The sex ratioall Workmen’s Compensation Board cases for 1945 and 1.949 was 84 per cent. male16 per cent. female. In 1945 it (vas 81.2 per cent. male to 18.8 per cent. female; in 1949,86.7 per cent. male to 13.3 per cent. female. In other ~vords, despite a five-to-one ratio for
THE JOIJI~NAL OF BONE AND JOINT SUl%GEl%YVOL. 35-

COLLES’ FRACTURE 645
;idual deformit,~lvement oftreatment (sitemrapy if given,i~jury and the
x, sly not eveD.100 radiocarpal
cture was found. In 1945, there~’ fracturc~ weret’es oul~ oft most frequent~ of 14 per cent.within one inch189 radial frac-hough theyes of the radialles’ fractures"ractures, trails-
fracture among~ber ofe to determine;rd casese out, of 133an incidence of; 0.95 peron ofJ~08 fractures ofd one-thirdbut amongper cent.~r cent.me cases).;fracturesas well as
~ lesser
vhichfractures
[.ofa~nd in~f 2,115?he sex ratior cent.emale; into-oue
iI
aS-A," NO. 3, JULY 1953JOINT

R. "W. BACOI~N AND J. F. I,~UI~TZKE
all Workmen’s Compensation Board .cases, there was almost a one-to-one ratio for Colle~’fracture. This we believe was in larg~ part due to the large number of female domestiwho had suffered falls resulting in Cotles’ fracture. Since Colles’ fracture is not primarian occupational hazard, we obtain a~ sex ratio more closely approximating that of th~general population ra~her than the heavily weighted ratio found in occupational injuries.We can in no other way explain the higher relative incidence in the female.
In 2,103 cases of Colles’ fracture, there were found to be 944 fractures of the rightradius (44.9 per cent.), and 1,159 (55.1 per cent.) of the left.. Included are twenty cases bilateral Cotles’ fracture (0.94 per cent.). The higher incidence of fracture in the left wristdoes not appear to be of any known significance. There were twenty-seven cases in whiclthe fracture was compound, an incidence of 1.3 per cent.
The mechanism of injury in a Colles’ fracture, as is well known, is most frequenth-the result of a fall on the palm of the outstretched hand. In only 8.4 per cent. (178 cases’)was there a different mode of causation--such as being struck by a heavy object, iniuriesby machines, and chauffeur’s fracture. The classical picture of Coiles’ fracture is a complete
transverse break with dorsal displacernent of the distal fragment. However, in a consider.able proportion of the cases there was comminutiou, impaetiou, or extension into the radio-carpal joint. An accurate estimation of the incidence of such forms was impossible, sincethe reports were usually not sufficiently complete. It was our impression that such formstended to result in a higher disability.
The primary ~reatment (reduction and immobilization) took place in a hospital 55 pet" cent. (1,179 cases) of the fractures, while a local physician performed this servicein the remaining 45 per cent. (953 eases).
Reduetiou of Cotles’ fracture ~vas performed in 88.3 pet" cent (1,348) of the fractures in which this factor could be assessed. Of these, 1,252 (81.9 per cent.) were sin~reductions, fifty-six (3.7 per cent.) required a second attempt, and sixteen (1 per cent.needed a third manipulation. There were only twenty-four fractures (1.6 per cent.)which an open reduction was performed. In 179 Colles’ fractures (11.7 per cent.), there wasno attempt at reduction, although, in q.ur judgment (based upon the x-ray reports, thecourse of treatment, and the final deformity), eighty of these (5.2 per cent.) were a nature that reduction should have been performed. Among these were a number ofof Colles’ fracture in which the patient refused rnanipulation.
Anaesthesia was used in the reduction of 471 Colles’ fractures; in the remain-~-erthis factor was either unknown or anaesthesia was not used, it being impossible tomine which. One hundred and sixty-eight (36 pet" cent.) were reduced under localtiou anaesthesia, including but one in which braehial block anaesthesia was used. General!anaesthesia (inhalation or intravenous) was used in the reduction bf 303 fractures (64pet" cent.).
Physical therapy was given in all but 3.4 per ceut. of a total of 1,440 eases, with 684eases in which the type of treatment was not reported. While every conceivable form oftherapy from hot soaks to histamine iontophoresis was used, the most, populardiathermy. The frequency of treatment most often noted was three times a week,is the maximum for which fees are authorized under the Workmen’s Compensation Law.~:The duration of treatment varied from 0.5 to twenty-four months, with a mean or average’f~
* The mean or average of a class is ghe sum of the components of a class divided by
class: mean = M = ~- =N
For grouped data (that is, where there are subclasses) mean = M = ~- ~(FX’)
M = X = mean of the X’sN = number in the classX = member of the classF = frequency of X’X’= a subclass (actually, the mid-point of the subclass).
THE JOURNAL OF BONE AND JOINT SURGEI:t](

’,-to-one ratio for Coll,:~er of female domestracture is notroximating that ofa occupational injuries.te female.t h’actures of the riled are twenty eases’aeture in the left wristy-seven cases in which
~vn, is most fret4 pe~" ceut. (178heavv object, injuries’ fracture is a complete[owever, in a consider_:tension into the tad;was impossible, since~ssion that such forms
place in a hospital in)erformed this service
(1,348) of the 1,527per cent.) were singlesixteen (1 per cent.)
’es (1.6 per cent.) r per cent.), there was
he x-ray reports, the,’r cent.) were ofere a number of
s; in the remainde~impossible to deter2l under local infilia was used. Generalof 303 fraetures
,440 cases, withconceivable formmost popular
:Ames a week,Jompensation Law.t a mean or averad by the number in
subclass).
COLLE~S’ FRACTURE
TABLE I
~’REQUENCY DISTRIBUTION ACCORDING TO AGE FOR ALL COLLES’ ~RACTURES AND ALL
WORKMEN’S COMPNNSATION BOARD CASES OF 1945 AND 1949, CO~IBINED
647
All Colles’ Fracturesage Group No. of Cases Per cent.
All W.C.B. Cases, 1945 and 1949.Vo. qf Cases Per cent.
II under 20 54 2.6 9,668 4.7
III 20-29 127 6.2 35,312 17.1
IV 30-39 257 12.5 46,395 22.4
V 40-49 563 27.4 50,547 24.4
50-59 683 33.5 42,496 20.5
60-69 325 15.9 19,362 9.4:
70-79 38 1.9 2,815 1.4
80-89 0 0 1 I0 0.1
2.047 100.0 206,705 100.0
4.0 months and a median* of 3.5 months. Although no statistical analysis of type orration of physical therapy in relation to final disability could be made, it is our impres-m that it did not play any appreciable role in altering the final loss of hmction. It is felt
hat the most important effective mode of physical therapy is the active and passivedone by the patient himself, under proper medical supervision, as frequently
md as early as feasible. We have seen rather severe h’aetures in elderly people treated forperiods result in a below-average disability, which was due in large measure to the
willingness to exercise his wrist l~,nd fingers. This is also the impression of I(nappCassebaum.Contrary to popular belief, Colles’ fracture most frequently results in some residual
in motion of the hand and wrist, even under the most favorable circumstances.sixty-two (2.9 per cent.) of 2,132 Colles’ fractures were judged by the physicians
Workmen’s Compensation Board to have had no permanent disability (loss of rune-The average disability in all eases of.Colles’ fracture regardless of age, adequacy of
or severity of fracture is 24 per cent. loss of function of the hand. The rangeis from 0 to 100 per cent.; both median and mode** are 20 per cent. loss of
(Chart I). In 94 per cent. of the eases, there was a resultant disability of less thanloss of hand function. This loss, as found by Workmen’s Compeusation Board
is eonsidered a permanent eondition not amenable to further treatment.2,047 eases of Colles’ fracture the ages ranged from fourteen to seventy-eight
an average age of 48.2 years (:mediau and mode each fifty years) (Chart III).out the generally accepted opinion that Colles’ fracture is a condition of the
groups. More concrete evidence of this is afforded by a comparison of the ageof Colles’ fractures xvith that of all Workme~fs Compensation Board cases
and 1949, New York City District (Table I), in which 68.6 per cent. of all Work-)ensation Board patients are under the age of rift, y, whereas 51.4 per cent. of
)atients with Colles’ fracture are aged fifty or over. A distribution index (defiimd frequency of Colles’ fraetu:ces per age group over the pereentage frequency
I Workmen’s Compensation Board es,ses for the same age-group) shows a sine-curve
from 0.35 for the 20-29 age group to 1.68 for the 60-69 age group, whereasis the value in a class so chosen that the members above and below this value are equal
the class is arranged with its mernbers in sequence.median =: Md (N -~- 1)
data, median = Md = N2
i ** The mode of a class is that member which occurs most frequently. Mo = mode.
~-~-A, NO. 3, JULY 1953

648 1%.W. BAcoR:N AND J. F,, KURTZKE
TI{E JOUI~NAL OF BONE AND

COLLES~ FRACTU]!~E 649
AND JOINT
I
II.
35-A, ~’0. 3, JULY 1953

050 R. V~’. BACORN AND J. F. KURTZKE
M
A
i 3.0’
! }o
IT
oo-!
if the age distribution ofColles’ fractures were pro-portional to that of allWorkmen’s Compensation
Board cases, the distribu-tion index would remainconstant at 1.00 (Chart IV).
It is commonly felt thatnot only are Colles’ frac .....
tares more numerous in theolder age groups but they
are, in addition, more seri-ous; patients in such groupsmay expect a higher disa-bility. By a correlation oft~ge and disability, it wasdetermined that the meanpercentage loss of functionfor each successively olderage group ranges from 9.4loss of function for the firstgroup (age less. than 20) 32.3 loss of function forthe seventh group (age 70-79), with a straight-lineslope approximating an in-crease in mean percentagedisability of 3.7 per decade
Chart V-A; Table II). Themean of each age subgroup
has been proved by statistical methods* to be.significantly different from the mean of all.cases of Colles’ fracture, except where the curve of disability-age correlation crossesvalue of the mean of all cases. In addition, each age subgroup has been shown to be signifi-cantly different** from the means of its contiguous groups -- except in the last (70-79)where there is a small number of cases.
* The standard deviation of the mean of the subgroup was compared with the mean of all Colles’ frac-tures. When the two means differ by more than twice the standard deviation of the subgroup, they are sta-~:tistically different 95 per cent. of the time.
¢~ = d ~ 1 ~n - I ’
For all Colles’ fractures14.5
For subgroup a14.5
CM = standard deviation meanas = standard deviation of a sampleZ = sum of
-- -- ± 0.314
x = mid--point of subgroupn = number of samplesa’ = number of samples in subgroup a
" ** T = the critical ratio of the difference between two means. If T is greater than :e 2.0, the two meansare significantly different 95 per cent. of the time.
Tab = Ma - Mb aD = standard error difference betweenO’Dab sample means
0"Dab = ~//0"2M~. "~ °’2~¢Ib -- r(¢M.) (¢Mb) r = coefficient of correlationThe T’s found were 4.02, 3.24~ 3.32, 2.39, 5.49, and 0.63, respectively.
THE JOURNAL OF BONE AND JOINT SURGERY

distribution ofures were pro-) that of allCompensation, the distribu-would remain.00 (Chart IV).monly felt thate Colles’ frac-umerous in theoups but theyion, more seri-;in such groupsa higher disa-correlation of
ability, it ~vasthat the mean)ss of functioneessively oldertnges from 9.4on for the first~ss than 20) to
function forgronp (age 70-
straight-lineimating an in-an percentage3.7 per decade[’able II). Thet age subgroup;he mean of all3n crosses then to be signifi-e last (70-79)
all Colles’ frac-~up, they are
;roup athe two
~etween
COLLES’ t’RACTUI~,E
T
//.I0
Thus age has been shown to be one important factor in the determination of thefinal percentage of loss of function in eases of Colles’ fracture. Another important elementin this regard is the adequacy of reduction and immobilization. These two factors are ofcourse related. In a study such as this, it is impossible to differentiate the two; but onefactor incorporates both elements: namely, the degree of residual deformity as adiudgedby the Workmen’s Compensation Board’s medical examiners. Residual deformity has been
::arbitrarily classified into five categories, tl~,e first being the return to the normal contoursize and the second, an enlarged wrisl~ in the absence of deformity. The next three
are those of true deformity (mild, ~noderate, and marked) which is most often "silver-fork" character. A deformity-disability correlation was set up and the results
conclusively that disability does increase directly with the degree of deformity inline having a slope of approximately 6 per cent. loss of function per grade" of
y (Chart VI-A). The mean percentage disabiIity ranged from 1016 (no deformity)0 42.1 (marked deformity). A statistical comparison "between two adiaeent means showed
difference in all cases but one, and that was between enlargement only anddeformity in which the difference was remarkably insignificant, tending to show that
}ithey are but two names for the same grade of deformity. In addition, by cumulative dis-!.tribution* curves, these two "grades", namely, enlargement and mild deformity, are
to be identical.i:i Thus we have only four classes of deformity: none, mild, moderate, and marked,
a slope of 10 per cent. disability per grade of de.formity. We have found that 86 perof the patients with no residual deformity have a disability of less than 20 per cent.,
only 3 per cent. of those with marked deformity have this same disability (Chart; Table III). The significance of this conclusion--that is, that there is a positive
ill * Cumulative distribution ;urves plot the cumulative" frequ,eney pc,re,enrage (,abse!s.s.a),a.gai~n..~s~t~umula-rive percentage disabilitv (ordinate) for each class involved in line eorre~ar, ion -- here ~t, ~s msam-,
VOL, 35-&, NO. 3, JULY 1953

652
TABLE III
I)EFORMITY~DISABILITY CORRELATIOX IN 2,113 C.~SES OF COLLES’ I~RACTURE
Types of ResMua] DisabilityPercentage-
Totalof 0 X X~ X" XmDisability No Deformity Enlargement Slight 5Ioderate ~Iarked
(10 No Enlargement Only Deformity Deformity Deformitypercentiles) No. Per cenl. No. Percent. No. Per cent. No. Per cent. No. Per cent. No. Percent.
0-9 64 38.6 80 7.7 17 3.7 0 0 161 7.610-19 78 47.0 369 35.7 179 38.6 43 11.9 3 3.4 672 31.820-29 19 11.4 324 31.4 135 29.2 138 38.2 14 15.7 630 29.930-39 3 1.8 146 14.1 72 15.6 96 26.6 25 28.1 342 16.240-49 2 1.2 66 6.4 42 9.1 51 14.1 17 19.1 178 8.450-59 0 24 2.3 5 1.1 17 4.7 14 15.7 60 2.860-69 0 16 1.5 10 2.2 8 2.2 9 10.1 43 2.070-79 0 8 0.8 2 0.4 6 1.7 2 2.2 18 0.980-89 0 0 1 0.2 0 2 2.2 3 0.190-99 0 1 0.1 0 1 0.3 3 3.4 5 0.2100 0 0 0 1 0.3 0 1
Total 166 100.0 1,034 100.0 463 100.1 361 100.0 89 99.9 2,113 99.9
correlation between residual deformity and disability--is proved by statistical methods.including the x-~ test*, using the null hypothesis that there is no correlation between de-’formity and disability.
One often hears that a east should be left on a fractured limb for a period just sufficientfor adequate callus to form and that immobiilization for periods beyond this greatlyenhances the probability of an increased final disability, or that immobilization per sefor some two to three months can cause a permaaent loss of function, where none wouldhave resulted had there been no east present (for example, in sprains treated as fractures).To test this hypothesis, we correlated the duratJion of immobilization with the percentageof disability in 1,654 eases of Colles’ fracture immobilized for periods ranging from zeroto sixteen weeks (one ease of eighteen weeks) (Chart V-B ; Table IV). The average periodof immobilization for all of these Colles’ fractures was 5.4 weeks, the median being fiveweeks, the mode four weeks.
By the testing of the means of successive two-week periods of immobilization(andalso of four-week periods) against the mean of all. eases of Colles’ fracture, the~e was foundto be no significant difference between the means of the individual subgroups and the meanof all Colles’ fractures. We further tested the significance of our entire distribution by
* X~ test: :
n = (R-- 1) (C - fo = observed frequencyfT theoretical frequencyE = sum of~A -- degrees of freedom
number of rowsnumber of columnsstandard deviation (unit of)
The null hypothesis sets up a theoretical frequency of an ideal ~distribution (bell) curve. If the hypothesisis correct, ~ will be less than 1 in two-thirds of the cases.
TI-IE JO12r:I:~.NAL OF BONE AND JOINT SURGERY

:Percentageof Wecks of Immol)iliz~.tion (in periods of 2 weeks) Total
Disability 0-1.9 2-3.9 4-5.9 6-7.9 8- 9.9 ! 0-11.9 12 -13.9 lq-15.9(10 percentiles) No. Per cent. No. Per cent. No. Per cenl. No. Per cent. No. Per cenl. No. Per cent. No. Per cent. No. Per cent. No. Per cent.
0-9 0 17 10.1 58 7.8 39 7.7 7 3.8 2 6.7 0 0 123 7.4
10-19 1 17 50 29.8 253 34.2 1~13 28.3 ,14 2-1.2 5 16.7 {i 33 :1 25.0 503 30.4
20-29 4 67 55 32.7 217 2!). 150 29.7 70 38.5 10 33.3 7 3!) 1 25 0 5 !:! 31.0
3~39 0 27 16.1 ll7 15.8 9~ 18.2 30 16.5 7 23.3 [} 2 50.0 275 16.64~9 1 17 11 6.5 61 8.2 40 7.9 17 9.3 2 6.7 I (i 0 133 8.0
50-59 0 .I 2..I l-I 1.9 I~ :1.{; ~ :~ :~ ~ ~ 7 :~ ;7 n 47 o o
6~9 0 3 1.8 13 1.8 14 2.8 4 2.2 2 6.7 0 0 36 2.2
7~79 0 1 0.6 4 0.5 7 1 .-~ 3 1.6 0 0 0 15 0.9
8~89 0 0 1 0.1 1 0.2 () (} 1 6 0 3 0.2
90-99 0 0 2 0.3 [ 0.2 0 0 0 0 3 0.2
100 0 0 0 0 I 0.6 0 0 0 1 0.1
Total 6 101 168 100.0 740 100.0 505 100.0 182 100.0 30 100.1 18 101 :1 ]00.0 1,653 99.8

654 1(. 3V. ]L4CORN AND J. F. KUI~TZKE
%FR
U
10’80,0
VII
r = coefficient of correlationN = number of cases = 1,653f = frequencyx abscissa (weeks of immobilization)
¯ y = ordinate (percentage of disability)
Significance of r:
determining r, .the coefficient of correlation.* This coefficient is a number which rangesfrom -- 1.000 to + 1.000. Plus or minus 1.000 signifies perfect positive or r~egativel~tion ; 0.000 signifies an absolute lack of correlation. The value ~ve found for r was +0.0974which is considered to represent no satistically valid correlation. Further, we checked theValidity of our figure for r by determining ~r which was found to be less than one-third the.
* Coefficient of correlation: ¯NZfdxdy- (Zfxdx) (Efydy) -r = ~/ENEfx (dx) ~ - (2:fx&x:) ~][NZfy(dy) ~- (Zfydy)
d = deviation from most numerous (modal) groupdx = deviation along x axis 0 = 4 weeksdy = deviation along y axis 0 = 20 to 29 per cent.fx~ total number of eases in "a" week of immobiiization:fyb = total number of cases in "b" disability percentile
7.66 X 1(}~r 7.86 X I(P = 0.0974
r, as greater than 3~,, is significant.
THE JOURNAL OF BONE AND JOINT SURGERY

.ber which rangesor negative corre-for r was -t-0.0974r, we checked theban
modal) groupeeks
~er cent.
~ability percentile
COLLES’ FRACTURE 655
of r, therefore r is significant. We haw~ sufficient data to substantiate the conclusionreached. Thus there is no correlation between the duration of immobilization and the per-
of disability in Colles’ fracture, within reasonable limits.The defects of function caused by Colles’ fracture are those of pronation and supina-
riot1 of the forearm, movements about the wrist (palr, aar flexion, dorsiflexion, and lateraland flexion and extension of the digits about the metacarpophalangeal and
)halangeal joints.In 2,122 cases of Colles’ fracture, defect in pronation was present in 28.2 per cent.,
:defect in supination in 36.9 per cent., defect in palmar flexion in 94.5 per cent., in dorsi-texion 80 per cent., and in lateral mobility 49.4 per cent. of the cases. It is obvious that
r far the most frequent permanent defect was in palmar flexion, rather closely followedb.~" limitation of dorsiflexion (Chart VII). The average limitation of motion in palmar flex-~
(of those having any defect) was approximately one-half the normal range, or "mod-crat(~" defect. Dorsiflexion and lateral mobility had an average limitation which appeared
t)e stightly less than palmar flexion, although it could not be quantitated because ofhe arbitrary classification used in describing such defects. (The Workmen’s Compensa-ion Board findings for restriction of passive motion were classed as mild, moderate,
and complete to which we have given approximate values of one-fourth, one-three-fourths, or four-fourths loss of range of n~otion.) Pronation and supinatio~
a lower average defect much closer to mild restriction (one-fourth loss). Theseare probably not due, in any large measure at least, to any disuse atrophy of the
muscles of the forearm since they are determined approximately one year after injury.:Pronation and supination defects may conceivably be explained on the basis of a
block to full movement caused by the enlargement of the bone due to callusradial tilt, and shortening, since the only muscles relating to these motions
can be involved at the distal end of t!he radius are the pronator quadratus and thes (supinator longus). There is considerable danger that the former could
ywhere beyond its origin, since it lies upon the radius. However, we have foundpronation was restricted in only one fourth of the patients, and in these, the restric-was most often mild. The brachioradiali~.may be involved since its insertion is on the
styloid, but it plays a minor role in forearm supi~aation. The flexores and extensoresare probably involved in or near the carpal tendon sheaths, and the mechanism
a traumatic synovitis with some adhesions. Flexion and extension defects inmay also be due to loss of radial tilt and shortening of the distal portion of the--
~vith callus. These latter causes will also explai~t the defects in digit motion whichto be present in almost one-half of the cases of Colles’ fracture (47.5 per cent.).
frequent of all defects of the digits was in flexion of the distal phalanx~ index finger (43.6 per cent.). Flexion of the distal phalanges of thei~ingers (35 to
was involved more often than eit:her motio~t of any other joint. For any givendefects were about twice as frequent as extension defects. The .thumb was
least involved (20 per cent. of flexion and 9.4 per Cent. of extension). Metacar-joints (20 to 25 per cent. of flexion) were involved insignificantly more often
proximal interphalangeal joints.was residual diminution of the g’zip in 34.6 per cent. of 2,130 cases of Colles’
. Only 3 per cent. of the total number of patients with Colles’ fracture had anwhich was classed as more than moderate; in 14.9 per cent. it was mild and in
. moderate, with twelve (0.6 per cent.) showing complete loss of grip.of Colles’ fracture was extremely rare, being found in only four Colles’
per cent.), but there were fourteen (0.7 per cent.) fractures which showedunion. Traumatic neuritis was extremely rare a].so, with only four cases of median-
involvement (0.2 per cent.) recorded, and or~ly one case of ulnar-nerve involvement.
were three cases of causalgia (0.1 per cent.), ~,s well as three cases of Sudeck’s
-~5-A, NO. 3, JULY 1953

656 R. W. BACORN AI~’D J. F. I~URTZKE
atrophy (0.i per cent.) and four of I)upuytren’s contracture (0.2 per cent.). Persistentpain was noted in 2 per cent., and in 1 per cent. of the cases of Colles’ fracture, limitationof shoulder motion was of significance.
Of 1,660 cases of Colles’ fracture, there were 887 fractures of the ulnar styloid (53.2per cent.), with 228 (13.7 per cent.) cases of non-union reported. Of the fractures ulnar styloid, 25.7 per cent. were, therefore, followed by non-union.
It has been stated above that the final ~Vorkmen’s Compensation Board award wasmade approximately one year after the initial iniury, by which time the residual defectswere considered permanent. The lapse of time between injury and the Workmen’s Com-pensation Board award in 1,055 cases was 12.0 months (mean, median, and mode), witha range of from four to fifty-one months.
DISCUSSION OF RESL-LTS
The first evident fact is the high incidence of Colles" fracture; it constitutes I per cent.of all Workmen’s Compensation Board cases, and 60 per cent. of fractures of the radius.It is also a fracture with a low incidence of complications, which in this study includedcompound fracture, non-union and delayed union, navicular and ulnar-styloid fractures,neuritides, causalgia, Sudeck’s atrophy, Dupuytren’s contracture, limitation of shouldermotion, and persistent pain of the wrist. However, this fracture is not the benign conditionmany consider it to be. Cassebaum found no serious functional disability in his study ofColles’ fracture, but we have seven patients i~ whom the loss of hand function was 90 percent. or more, and over 3 per cent. of all the patients have disabilities of 60 per cent. ormore. The average permanent loss of function of the hand in over 2,000 cases of Colles’fracture has been found to be 24 per cent. The percentage disabilities upon which thisfigure is based were adiudicated by the expei~ienced physicians who compose the medi(’alboard of the Workmen’s Compensation Board. In cases of doubt as to the fitting award, apanel composed of three senior Workmen’s Cc.mpensation Board physicians was employed,and, as a final arbiter, the medical director of the Workmen’s Compensation Board. Alongthe way,’the patient’s physician, insurance-.company doctors, and independent expertswere often called upon to aid in the iudgment of the final award. Therefore, weconsider each award to be an accurate estimat~ of disabiility, based solely upon the deficitsin function (range and power of motion) found at the final examination. As an estimateof the basis for such awards, here are the findings in a typical patient who was awarded25 per cent. disability: moderate limitation of palmar flexion and dorsiflexion, mild.limitation of lateral mobility, and mild flexion defects of the distal interphalangealiointsof the index, middle, and ring fingers, as well as an enlarged wrist.
However,¯ it must be admitted that such defects as are most u~sually found areminor importance for the unspecialized use of the hand; a loss of 50 per ce.nt, of the rangeof motion does not imply a hand only half u~’~able, for very seldom do we employ the
¯ range of any ioint motion. Even an ankylosed wrist is’. serviceable so long as the diespecially the first two, are reasonably agile. Nevertheless, such considerationsnot militate against the recognition of actual disability.
As to the correlations set up in the paper, little need be said. It was expectedincreasing age would mean increasing disability, and that the greater the deform~tthe greater would be the loss of function ; but iit is well to have support for suchespecially since some authors have made dii~’erent statements;. The one somewhatpected aspect was the lack of correlation between duration of immobilization¯ disability. Although the limit of immobilizat!ion was only sixteen weeks, it is theone is likely to encounter, and within this ran~;e it was found that disability did notwith the prolongation of the period of immobilization. The factors which we feel aregreatest importance in the dffort to obtain an end result with a low disability are (I)curate reduction, (2) adequate immobilization, and (3) early and persistent active motion.
THE JOURNAL OF BONE AND JOINT

cent.). Persistentacture, limitation
lnar styloid (53.2e fractures of the
Board award wase residual defectsWorkmen’s Com-and mode), with
~itutes 1 per cent.res of the radius..s study includedstyloid fractures,~tion of shoulderbenign conditiony in his study of~ction was 90 per)f 60 per cent¯ or) cases of Colles’upon which thispose the medical~ fitting award, a~s was employed,ion Board. Along’,pendent expertserefore, we mayupon the defi~¯ As an estimateho was awardedors;flexion, mild)halangeal joints¯
lly found areent. of the ran
ng as theterations
~S expectedthe deformit
such statementssomewhat
:t is thedidh we feel are)ility are (1)t active motion
COLLES’ FRACTURE 657
CONCLUSIONS
From a study of a total of 2,132 cases of Colles’ fracture from the files of the Work-men’s Compensation Board, New York State Department of Labor, New York Cityl)i~trict, the following conclusions were drawn:
1. Colles’ fracture constituted 60.0 per cent. of fractures of the radius.2. Incidence of Colles’ fracture among Workmen’s Compensation Board cases, New
York City District, in 1945 and 1949 was 1 per cent.3. Of all carpal fractures, that of the navicular constituted 70.8 per cent.4. The ratio of males to females in Colles’ fracture was 58 per cent. to 42 per cent.
for 1945 and 1949, whereas the male-to-female ratio for all Workmen’s CompensationBoard cases for the same years was 84 per .cent. to 16 per cent.
5. The left radius was involved in Colles’ fracture in 55.1 per cent. of the cases; theright in 44.9 per cent. These figures include 0.94 per cent. of bilateral Colles’ fracture.
6. The incidence of compound fractures among Colles’ fractures was 1.3 per cent.7. Iu 91.6 per cent. of the cases, the mechanism of injury was a fall on the outstretched
hand.8. A considerable proportion of Colles’ fractures showed one or more of the following:
comminution, impact;on, and extension into the radiocarpal i oint.9. Reduction of Colles’ fracture was performed in 88.3 per cent. Of the total number
of fractures, 3.7 per cent. were manipulated a second time. and 1.0 per cent. reqnired athird manipulation. In only 1.6 per cent. of the to~al was open reduction performed.Of the 11.7 per cent. in which no reduction was performed, it was our conclusion thatalmost one half required such manipulation.
10. In the 471 cases in which it was known that anaesthesia was given for reduction,anaesthesia was used in 36 per cent. and general (gaseous and intravenous) anaesthe-
in the remaining 64 per cent.11. The average duration of treatment was four months.12. Physical therapy was used in 96.6 per cent. of the cases, exclusive of active and
motion. This varied widely in type, frequency, and duration, without appearingaffect appreciably the ultimate results. -"
13. The average (mean) percentage loss of function (disability) in all patients fracture was 24 per cent. loss of the hand, based upon the findings of the Workmen’s
)ensation Board medical examiners. The range of disability was 0 through 100 per--Of all patients with Colles’ fractures 94 per cen~. had a resultant disability bf less
n 50 per cent. loss.The mean age of all patients with Colles’ fracture was 48.2 years; the median and
were fifty years; the range was fourteen to seventy-eight years inclpsive.The age distribution in Colles’ fracture has been found to be significantly higher
~ that of all Workmen’s Compensation ~Board cases for 1945 and 1949. Of all Work-
)ensation Board cases, 68.6 per cent. of the: iniuries occurred in people underof fifty, whereas 51.4 per cent. of Colles’ fractures were in people of fifty or over.The percentage of disability in Colles’ fracture increased directly with age, at a
of approximately 4 per cent. loss of function per decade.17. Residual deformity (as an inverse measure of adequacy of reduction and im-
p) has been found to have a direct correlation with disability, at a rate of 10loss of function per.grade of deformity (none, mild, moderate, marked).
duration of immobilization in Colles’ fracture had no effect upon finalsability.
The most frequent defect in passive motion about the wrist wgs in palmarpresent in 94.5 per cei~t, of the cases; defect"in dorsiflexion was found in 80 per cent.
of rotation of the forearm was present iu one third and limitation of lateralmotion in one half the cases.
VOL. 35-A, NO. 3, JULY 1953

R. ~,v. BACORN AND J, F. KURTZKE
20. Forty-eight per cent. showed restriction of motion of the digits (flexion and.extension), with flexion defects being twice as frequent as extension; the distal inter-
phalangeal joints were most often afflicted, and the index finger was the most, with
thumb the least, often involved digit.21. One third of the patients with Colles’ fracture showed residual diminution of the
grip which was mild or moderate in severity in all but 3 per cent. of the total number of
cases.22. Non-union of Colles’ fracture was found in 0.2 per cent. and delayed union in
0.7 per cent. of the cases. Other complications i~.eluded traumatic neuritis (0.2 per cent.),causalgia (0.I per cent.), Sudeck’s atrophy (0.i per cent.), ])upuytren’s contracture per cent.), persistent pain (2 per cent.), limitation of shoulder motion (I per cent.),compound fracture (1.3 per cent.), concomitant navicular fracture (0.5 per cent.).
23. Fifty-three per cent. of the eases of Colles’ fracture were accompanied by avnlshmfracture of tl~e ulnar styloid, and of these latter, one-fourth remained ununited.
24. The interval between injury and final Workmen’s Compensation Board medical
examination and award was twelve months (mean, median, and mode).
NOTE: The invaluable aid of Miss Jeanette Hanlon and her Research and Statistics Section, Workmen’sCompensation Board, and of Miss Donlan, is gratefully acknowledged.
REFERENCES
I. CASSEB.~U.~. \V. If.: Colles’ Fracture. A Studv of End. Results. J. Am. Med. Assn., 14~: 963-965, 1950.2. I(N.~PP, ~[. E.: Treatment of Some Complications of Colles’ Fracture. J. Am. Med. Assn., 148: 825-827,
1952.3.
NE’W YORK STATE "~rORKMEN’S COMPENSATION BOARD: Compensated Cases Closed in 1945. Research
and Statistics. Bulletin 1, 1946.4.
~’EW ~I’ORK STATE ~rORKMEN’S COMPENSATION LAw AIVD RULES pp~OMULGATED THEREUNDER. ~N’e w York
State Workmen’s Compensation Board, July, 1948.5.
NEW YORK STATE WORKMEN’S COMPENSATION BOAB, D: Compensated Cases Closed in 1949. Research
and Statistles. Bulletin 1, 1950.
DISCUSSION
THE USE OF IPRONIAZID IN THE TREAT~IEN’r OF BONE ANDJOINT TUBERCULOSIS :.:
(Continued from. page 6~5)
rate from injections into the sinuses, abscesses, or cavities is so uncertain that proper blood levecontrolled. Oral administration, to treat the patient’s body as a whole, is the best and the safest.
:For the same reasons the dosage should not be increased above 4 milligrams perexcept for very short times and with the realization that patients will ’become toxic. If you have ais dreadfully ill, you maY be scared into trying 6 milligrams per kilogram of body weight. Withinhours you will find that patient neurotoxic. If you continue to push ~bhis higher dosage, you are in danger ofcausing the development of a psychosis. Iniection of material into a patient on a satisfactory oralhas been found to upset the balance and cause toxicity.
Local treatment will not touch tubercle bacilli buried in the calcified lesions or in sloughed-off piecesabscess wall. The drug must be circulated in a definite concentration that will destroy the Mytuberculosis and not damage living tissue cells.
Even with a proper dosage you have to watch for toxicity. You can forget all other manifestationstoxicity, if you will examine the patient every day as to reflexes. If these become severely hypertonic,though there is no clonus, the drug dosage should be de.creased.
Do not use the drug in combination with streptomycin at present. You will confuse yourself as toand results. Other qualified investigators are working this problem out. Await their reports. Remembercannot use it at half dosage. Do not experimeHt as regards dosage: watch your patients and you will find thismaterial a great help in the treatment of bone and joint tuberculosis.
TI=LI~ JOUII.NAL OF DONE AND JOINT NUIIGERY

Do not mark this box!Document: 11000292

MARCH 1986
VOLUME 11A, NUMBER 2
THE JOURNAL OF
HANDSURGERY
Official journalAMERICAN SOCIETY FOR SURGERY OF THE HAND
AMERICAN VOLUME
ORIGINAL COMMUNICATIONS
Severely comminuted distal radialunsolved problem: Complicationsexternal fixation and pins andplaster techniques
fracture as anassociated with
Seventy-six patients with severely comminuted dis’tal radial fractures were treated at two insti-tutions, of which the overwhelming majority were Frykman class VIII. Fifteen fractures wereopen. Thirty patients were seen at the University Hospital; 17 had pins and plaster and 13 hadexternal fixation. Forty-six patients were seen at Kaiser Hospital; all had pins and plaster treat-ment. The complication rate for those with pins and plaster at lthe University Hospital was 53 %;the complication for external fixation rate was 62%. The afl~iliated-hospital complication ratewas 52%. All patients with ipsilateral forearm shaft and carpal fractures developed a nonunionof the carpal fracture. Few patients maintained anatomic red,action, and many had significantintra-articular malalignment. External fixation with threaded half pins did not obviate pinproblems ,in our series. These methods may help manage se.verely comminuted distal radialfractures, but complications should be anticipated, and alternative treatment considered, espe-cially when ipsilateral carpal or forearm shaft fractures are present. (J HAND SURG 11A:157-65,1986.)
Stephen C. Weber, M.D., and Robert M. Szabo, M.D., Sacramento, Calif.
Since Colles’~ original description, some
authors continue to claim good results with minimaltreatment of displaced distal radial fractures. _,-6 The vastmajority of authors, however, agree that results corre-late directly with restoration of normal anatomy.7"s
These fractures can also be associated with Serious com-
"From the Department of Orthopedic Surgery, University of Califor-nia, Davis, Medical Center, Sacramento. Calif.
Received for publication Jan. 29, 1985; accepted in revised form July4, 1985.
Reprint requests: Stephen C. Weber, M.D., Department of Or-thopedic Surgery, Rm. 5012A. University of California. Davis,Medical Center, 2315 Stockton Blvd., Sacramento, CA 95817.
plications.12, ~9-26 Although acceptable reduction can beobtained, it is often difficult to safely maintain reduc-tion with cast immobilization. Various techniques havebeen described to better maintain reduction, includ-ing immobilization in supination,~7"~9 early distal ulna
30resection, tension band wiring,3| percutaneous pin-ning,~-39 Rash rods,~° and open reduction with internalfixa ~ .. Since its description by Bohlel~ in 1929,traction’maintained by transfixing pins incorporatedin plastrr has been widely recommended.9’~*" xr. 4740Although [his technique restores length well, it doesnot restore normal palmar angulation ~of the distal ra-dius.W, ’* Pin complications are common and can leadto a reoperation rate as high as 16%.~ Other problems
THE JOURNAL OF HAND SURGERY 157

The Journal of158 Weber and Szabo HAND SURGERY
Table I. Distal radial fractures graded according to
the classification system of Frykman
University University Kaiser
Hospital Hospital Hospital
Frykman Pins and External Pins and
class plaster fixation plaster
I
II
III 2 1
IV 1
V 1 1
VI 1 1 1
VII 3 12
VIII 10 12 30
include difficulty managing large open wounds, com-plications associated with circumferential plaster, in-trinsic tie down by the distal pins, rotation of the frac-ture about the distal pins, and difficulty of adjustment.
These problems led to a resurgence of external fix-ation as originally described by Anderson and O’Neilv
in the management of these injuriesI°’ ~9.52-73; all authorsdescribe improved results in the management of these
fractures with this technique. Many of these reports donot differentiate minimally displaced fractures from ex-tensively comminuted high-energy fractures. Seriouscomplications including failure of fixation, iatrogenicfractures, pin infections, pin tract osteomyelitis, andloss of reduction continue to be reported with thistechnique7. 19, 54. 59-65.7o. 72.73 at a rate of 15% to 23% insome series55’ 56. 60. 67 describing "good" results. Thewrist ligaments in Colles’ fractures created in cadavermodels have been reported to remain intact34; reduc-tion of intra-articular comminution with this treatment
is said" to occur by traction on these ligaments,so called"ligamentotaxis".~ 2 Although some authorsdescribe invariate intra-articular reduction with trac-
tion techniques,~6 many have found this not to be thecase.~4’ 43 None "of the articles quoted here address thequality of reduction of intra-articular comminution pro-vided by external fixation.
It has been our experience that the severely com-minuted distal radial fracture secondary to high-velocitytrauma is often not adequately reduced with externalfixation or pins and pla.ster alone and that pin problemsoften occur to complicate both of these forms of treat-ment. We do not give a long-term functional follow-up, but instead evaluate several key points in the man-agement of patients with severely comminuted distalradial fractures: (1) the ability to restore anatomic lengthand angulation, (2) the ability to correct intra-articutar
Table II. Mechanism of injury
University
Hospital
University
Hospital
Kaiser
Hospital
Pins and External Pins and
plaster fixation plaster
Fall 10 2 27
Motor vehicle accident 2 5 6
Motorcycle accident 4 3 8
Roller skate 0 1 3
Other 1 2 2
displacement, and (3) short-term complications com-paring external fixation to pins and plaster as they occurin a younger and often multiple-injured population. Weretrospectively reviewed the experience of several or-thopedists at two institutions with 76 patients with se-verely comminuted distal radial fractures treated withei~!her pins and plaster or external fixation.
Method
All patients had severely comminuted, displaced dis-tal radial fractures, graded type III through VIII by theclassification of Frykman~2; most were Frykman classVIII (Table I). The mechanism of injury is shown Table II; more than one third were the result of high-speed motor vehicle accidents. All patients were treated
by either the attending staff or residents supervised bystaff members. Thirty patients were seen at the Uni-w;rsity of California at Davis Hospital; 17 had pins andplaster and 13 had external fixation. The mean age was
36.9 years for external fixation and 40.1 years for pinsand plaster. Eleven of the fractures were open; thr__eepatients in each group had an additional associated tong
bone fracture, and six in each group had severe, mut-tisystem injuries. Follow-up ranged from 3 to 22 months
with a mean of 6 months. Forty-.six patients were seenat Kaiser Permanente Medical Center, Sacramento,Calif.; "all had pins and plaster treatment. The mean agewas 48.9 years. Four had open fractures, five had as-sociated fractures, and five had severe, multisystemtrauma. Follow-up ranged from 3 to 36 months andaveraged 9.6 months.
Indications for operation at both institutions were (1)g~:oss comminution with little chance of restoring lengthnonoperatively, (2) failure of initial closed reduction
and splinting under hematoma block in the emergencyroom, or (3) loss of initial reduction with plaster treat-ment at follow-up of 1 to 2 weeks. Most patients wereoperated on on the day of injury, frequently in con-junction with operative procedures for their other in-

Vol. 11A, No. 2March 1986
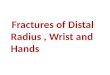
Pre op Post op FlU
o
Length
Pro op Post. op FlU
UCD P&P UCD Ext. Fix Kaiser P&P
Fig. 1. Preoperative, postoperative, and follow-up measure-ments of radial angulation and length, calculated accordingto the method of Van der Linden and Ericson for each studygroup.
juries. Mean delay to fixation was 4 days at the Uni-versity Hospital and 3.3 days at Kaiser Hospital. Eachprocedure was performed in the operating room undergeneral, axillary, or intravenous regional anesthesia; thefractures were managed with finger traps and 3 to 5 kgof traction and gentle manipulation. Pins and plasterused 3/32-inch smooth Steinmann pins in almost allcases. Distal fixation was obtained through the indexand long metacarpals and proximally through the prox-imal ulna as described by. Green14 in 42 of 44 cases atKaiser Hospital and eight of 17 at University Hospital;the remainder were fixed proximally through the radius.External fixation was done with threaded 3 mm halfpins through the index and long metacarpals and distalradius in all cases by means of the open technique atthe distal radius and proximal metacarpals. In nine pa-tients, the Hoffman small external fixator was used; theAce Colles fixator was used in three patients, and theFischer mini fixator was used in one. Two plane x-rayfilms were obtained to confirm reduction. Immediatefinger and elbow motion was encouraged; fixation wasusually maintained for 6 to 10 weeks followed by avariable amount of short-arm plaster or intermittentsplint immobilization until the fractures appeared ra-diographically healed. Pin sites were cleaned daily with
Severely comminuted distal radial fractures 159
Polmar
Anqulation
Pre op Post op FlU
+7
Fig. 2. Preoperative, postoperative, and follow-up measure-ments of palmar angulation for each study group.
Radialdisplacement
(ram)
Dorsaldisplacement
(mm)
Pre op Post op FlU
Pre op Post op .- FlU
IUCDP&P ~UCDExt. Fix ~ Kalse~ P&p
Fig. 3. Preoperative, postoperative, and follow-up measure-men,is of radial attd dorsal displacement for each study_group.
peroxide. Fracture displacement was measured accord-ing to the method of Van der Linden and Ericson74 withrespect to radial length and radial and palmar angulationof the distal fragment. X-ray films were not routinelymade of the uninjured-extremity; normal values weretaken to be 23° of radial angulation in the anteropos-teric,r plane and 11° of palmar angulation in the lateral

The Journal of161) Weber and Szabo HAND SURGERY
Table III. Amount of radiocarpal displacement preoperatively, postoperatively, and at follow-up for each studygroup, measured as the greatest distance in millimeters
University Hospital, pins and plasterUniversity Hospital, external fixationKaiser, pins and plaster
IPreoperative Postoperative ] Follow-up
(mm) (mm) ] (mm)
3.6 2.2 2.33.6 2.4 2.43.9 2.3 2.5
Table IV. Complications for each study group, shown as number and percentage of total cases
Universi~ Hospital, UniversiO, Hospital. Kaiser Hospital,Pins and plaster External fixation Pins and plaster
Pin infection 0 3 (23%) 3 (6.5%)Loose pins 3 (18%) 2 (15%) 11 (23%)Pin tract osteomyelitis 0 0 3 (6.5%)Iatrogenic fracture 1 (9%) 0 4 (8.6%)Nonunion 0 1 (7.6%) 2 (4.3%)Iatrogenic nerve palsy 1 (5.9%) 1 (7.6%) 0Loss of reduction 3 (18%) 1 (7.6%) 6 (13%)Radloulnar synostos~s 1 (5.9%) 0 0% of patients with complications 53% 61% 52%
plane. 16 Although ulnar variance can be considerable, ~4average radial length was taken to be 12 ml from thedistal ulna.~6 In addition, intra-articular displacement
along the radiocarpal joint was measured on preoper-ative, postoperative, and follow-up films. Normal val-ues for dorsal and radial displacement were not givenby Van der Linden and Ericson; the normal valuesshown here were obtained by averaging the measure-ments for those patients who had contralateral wristfilms. Significant loss of reduction was defined as thatof sufficient degree in which corrective surgery wasrecommended or performed.
Results
Twenty-eight of 30 patients reviewed from the Uni-versity Hospital and 44 of 46 patients treated at KaiserHospital .had sufficient x-ray films taken for preopera-tive, postoperative, and follow-up measurements. Ra-diographic measurements obtained are shown in Figs.1 through 3. In general, radial angulation and lengthwere reasonably well restored with both of these tech-niques. Palmar angulation was not restored to normalwith either technique. Intra-articular displacement is. shown in Table III. Intra-articular radiocarpal displace-ment Wag generally decreased, but not returned to an-atomic alignment. In most cases, a significant and un-acceptable amount of displacement existed at the ra-diocarpal joint despite many attempts a~ manipulation
and reredu.ction with both techniques (Figs. 4 through10). There: were no infections in any of the soft tissuewounds and no cases of osteomyelitis at the fracturesites in any of the open fractures.
Complications are shown in Table IV. Fifty-three per-cent of the patients treated at the University Hospitalexperienced at least one complication. With externalfixation 61% of the patients experienced complications.Most of these complications were related to pin prob-lems despite the use of threaded half pins. Fifty-twopercent of the patients treated with pins and plaster atthe affiliated hospital had complications. No pin tractosteomyelitis occurred in our small series of externalfixation. Pin infections resolved with oral antibiotics in
all but four patients who required pin removal. All loosepins were removed; five of these eleven patients hadtheir fractures rereduced in the operating room and hadthe loose pin replaced at a different site. Iatrogenicmetacarpal fractures were treated with closed reductionand casting; all iatrogenic ulnar fractures were treatedwith internal fixation. Nonunion at the dist~l radius ledto bone grafting in two patients and wrist fusion in one.Iatrogenic nerve palsies were treated with decreasingwrist flexion and resolved in all patients by follow-up.The amount of loss of reduction requiring subsequent
operative :reconstruction varied for each surgeon; how-ever, these patienys tended to have severe residual de-formities, including a mean radial length of -11 ml

Vol. 11A, No. 2March 1986 Severely commtnuted distal radial fractures 161
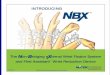
Fig. 4. Twenty-six-year-old man injured in a motorcycle ac-cident. Preoperatiye x-ray films show a comminuted Frykmanclass VIII fracture with moderate displacement of the radialstyloid fragment.
and a mean dorsal tilt of 9.6° at follow-up. Two patientswith ipsilateral scaphoid fractures and one with a radialshaft fracture were treated with pins and plaster. Alldeveloped nonunion of these associated carpal frac-tures. Five (28%) patients with pins and plaster treatedat the University Hospital were unable to complete 6weeks of immobilization with pins secondary to pin-related complications. Four (30%) of those with exter-nal fixation had similar complications. Fourteen (30%)of the patients treated at the affiliated hospital wereunable to complete the initial form of treatment. Re-operation, rate for the externally fixed group was 38%(five of 13). Three patients with pins and plaster werereoperated on at the University Hospital (I 7%) and nineat Kaiser Hospital (20%).
Discussion ~
In low-velocity injuries with minimal displacementand little soft tissue injury, the improvement in reduc-tion offered by distraction techniques can often be suf-ficient to expect a good result with acceptable compli-cation rates.~°~ ~4, t6, 43..~. 52. 55. ~0 This, however, isoften not the case in the extremely displaced high-velocity injury that frequently occurs in younger pa-tients.~4. 43, 5~ The Frykman classification system does
not differentiate these injuries, since the amount of dis-placement of the fracture fragments is not one of the
Fig. 5. Postoperative films obtained after several attemptswith external fixation to reduce the fracture. Ligamentotaxishas actually increased the intra-articular displacement by ro-tating the styloid fracture further out of anatomic position.
Fig. 6. i::::!ow-up at 10 months shows osteoporosis #ith per-sistent ~.~ca-articular malalignment and loss of palmar an-gulation.
criteria. The mean age of patients in our series withpins and plaster was younger than in most series,, and.in general the patients were more severely traumatizedwitih a concomitant increase in complications. Cer-

Weber and SzaboThe Journal of
HAND SURGERY
Fig. 7. Severely displaced, comminuted Frykman class VIIIfracture in a motorcycle rider.
Fig. 8. Initial reduction obtained with external fixation. Notedisplacement of palmar fragment with unreduced depressionof the lunate fossa of the radius.
Fig. 9. Rereduced at I0 days with open reduction of lunateassociated fragment. Better alignment but still has dis-placement of lunate fossa and dorsal angulation on the lat-eral film.
Fig. 10. Follow-up at 6 months.
tainly, the data represented here would indicate thatcareful patient selection and meticulous technique inthe use of pins and plaster is mandatory; complicationsshould be anticipated in regai’ds to pin problems andfailure to obtain or maintain reduction.
Our small series of extemal fixation of these fracturesdid not resolve this high rate of pin complications.Although some suggest a lower incidence of pin prob-lems with threaded half pins, in those series with rea-
sonable follow-up in which complications are reported,failure rates secondary to pin problems are often dis-turbingly high.55" 56 Our study does not address long-term function and thus cannot speak to several issueswhen comparing external fixation versus pins and plas-ter, such as intrinsic tie down and better hand and elbowmotion. Both of.these theoretical advantages are at-tractive, especially in the older patient in whom stiff-ness is a problem and fractures tend to be low-energy,

Vol. 11A, No. 2March 1986 Severely comminuted distal radial fractures 163
minimally displaced injuries. The low incidence ofwound complications, with either technique, minimalcomplications with circumferential plaster, and simi-larity of quality of reduction shown here do not defendthe increased cost of external fixation over pins andplaster. External fixation did not obviate pin problemsin our series.
Carpal and forearm shaft fractures are unusual withdistal radial fractures, although they have been previ-ously reported.~°’ ~4.75.76 Smith et alo 77 reported severalipsilateral injuries treated with external fixation, all ofwhich healed. None of the fractures treated this way inour series healed. The traction required to maintainreduction of the distal radius in the severely commi-nuted fracture leads us to recommend against its usewith ipsilateral carpal fractures unless additional inter-nal fixation of the long bone or carpal fracture is alsoperformed.
Perhaps most discouraging in our evaluation was thequality of reduction obtained with these techniques. Wehave shown, as have others, reasonable restoration ofradial length. Anatomic palmar tilt was not restored inmost cases, as has been previously reported.9’m’14"46"5°’7°
This is of some concern, since at least one report~7
associates failure to restore palmar tilt with symptom-atic midcarpal instability. It has also been our experi-ence that the "die punch" fragment is not often reducedwith distraction techniques alone. DePalma’s34 workwith Colles’ fractures created in cadavers is oftenquoted as definitive evidence that the wrist ligamentsin these injuries remain intact. As some individuals gainexpertise with open reduction of these fractures, softtissue injury associated with Colles’ fractures has beenfound to be not infrequent in vivo.78 It seems possiblethat the integrity of the wrist ligaments in these severeinjuries is not always adequate for reduction by "li-gamentotaxis." Most of the displaced radiocarpal com-minution was not reduced adequately with either tech-nique in our series; because these were often younglaborers, significant delayed radiocarpal arthritis con-stitutes a serious problem. Although long-term resultsin our series are unknown, the residual 2 to 3 ml stepoff shown in our patients causes us some concern, sinceradiocarpal arthritis has been shown to be present inmore than 90% of wrists with similar displacement at.10ng-term follow-up.79
In summary, although pins and plaster or externalfixation may provide an accel~table result for an isolatedlow-energy injury, the complication rate in our seriesfor younger, often multiple-injured patients was high.All carpal and forearm shaft fractures treated with dis-traction developed nonunion. Reduction of intra-artic-/
ular radiocarpal displacement was rarely anatomic, andsignificant displacement often remained despite re-peated reduction. Perhaps open reduction and internalfixation or external fixation combined with limited in-ternal fixation43 can better reduce this displacement;until future series demonstrate better results with thesec,r other techniques, the comminuted distal radial frac-ture remains very much an unsolved problem.
REFERENCES
I. Colles A: On the fracture of the carpal extremity of theradius. Edinb Med Surg J 10:181, 1814 :
2. Ahstrom JP: Results of treatment of Colles’ fractures byposterior plaster splint immobilization. Presented at theAcademy of Orthopedic Surgeons. New Orleans, Loui-siana. Feb., 1981
3. Lucas GL, Sachtjen KM: Thomas Jefferson, therapeuticnihilism, and Colles’ fracture. Orthop Rev 6:83, 1977
4. Older TM, Stabler EV, Casselbaum WH: Colles fracture:evaluation and selection of therapy. J Trauma 5:469, 1965
5. Smaill GB: Long-term follow-up of Colles’s fracture. JBone Joint Surg [Br] 47:80, 1965
6. Waugh TR: Unreduced Colles’ fractures. J Trauma 3:254,1962
7. Anderson R, O’Neil G: Comminuted fractures of thedistal end of the radius. Surg Gynecol Obstet 78:434-40,1944
8. Bacom RW, Kurtzke JF: Colles’ fracture. A study of twothousand cases from the New York State Workmen’sCompensation Board. J Bone Joint Surg [Am] 35:643,1953
.9..Cole MM, Obletz BE: Comminuted fractures of the distalend of the radius treated by skeletal transfixion in plastercast. J Bone Joint Surg [Am] 48:931, 1966
10.Cooney WP, Linscheid RL, Dobyns JH: External pinfixation for unstable Colles’ fractures. J Bone Joint~Surg[Aml 61:840, 1979
11.Fernandez DL: Correction of post-traumatic wrist defor-mity in adults by osteotomy, bone-grafting, and internalfixation. J Bone Joint Surg [Am] 64:1164, 1982
12.Frykman G: Fractures of the"distal end of the radius,including sequelae-shoulder, hand, finger syndrome, dis-turbance in the distal radioulnar joint and impairment ofnerve function. Acta Orthop Scand Suppl 108:27, 1967
13.Gartland JJ, Werley CW: Evaluation of healed Colles’fractures. J Bone Joint Surg [Am] 33:895, 1951
14.Green DP: Pins and piaster treatment of crmminutedfractures of the distal end of the radius. J Bone JointSurg [Am] 57:304, 1975 . .
15.Hobart MH, Kraft GL: Malunited Colles’ fracture. AmJ Surg 53:55, 1941
16. Scheck M: Long term follow up of treatment of com-minuted fractures of the distal end of the radius by trans-fixation with Kirschner wires and cast. J Bone Joint Surg[Am] 44:337, 1962

164 Weber and SzaboThe Journal of
HAND SURGERY
17. Taleisnik J, Watson HK: Mid carpal instability causedby fractures of the distal radius. J HAND SURG 9A:350,1984
18. Nigst H: Fractures of the distal radius in the adult: anat-omy, trauma mechanisms, fracture types, and typicalassociated injuries. Unfallheilkunde 82:1, 1979
19. Cooney WP, Dobyns ~IH, Linschied RL: Complicationof Colles’s fractures. J Bone Joint Surg [Am] 62:613,1980
20. Engkvist O, Lundborg G: Rupture oftheextensorpollicislongus tendon after fracture of the lower end of the ra-dius--a clinical and microangiographic study. Hand2:76, 1979
21. Lewis MH: Median nerve decompression after Colles’sfracture. J Bone Joint Surg [Br] 60:195, 1978
22. Morrissy RT, Nalebuff EA: Distal radial fracture withtendon entrapment. A case report. Clin Orthop 124:206,1977
23. Rycbak JS, Kalenak A: Injury to the median and ulnarnerves secondary to fracture of the radius. J Bone JointSurg [Am] 59:414, 1977
24. Younger C~, DeFiore JC: Rupture of flexor tendons tothe fingers after a Colles’ fracture. J Bone Joint Surg[Am] 59:828, 1977
25. Campbell WC: Malunited fractures. Surg Gynecol Obstet66:466, 1938
26. Speed JS, Knight RA: The treatment of malunitedColles’s fractures. J Bone Joint Surg [Am] 27:361, 1945
27. Sarmiento A, Pratt GW, Berry NC, Sinclair WF: Colles’fractures. Functional bracing in supination. J Bone JointSurg [Am] 57:311, 1975
28. Sarmiento A, Zagorski JB, Sinclair WF: Functional brac-ing of Colles’ fractures: a prospective study of immo-bilization in supination versus pronation. Clin Orthop146:175, 1980
29. Wahlstrom O: Treatment of Colles’ fracture. A prospec-tive comparison of three different positions of immobi-lization. Acta Orthop Scand 53:225, 1982
30. Spira E, Weigl K: The comminuted fracture of the distalend of the radius. Reconstr Surg Traumatol 11:128, 1969
31. Katznelson A, Volpin G, Lin E: Tension band wiring forfixation of comminuted fractures of the distal radius.Injury 12:239, 1980
32. Brennwald J, Pfeiffer K: Radiusfraktur Loco Classico.Ther Umsch 37:743, 1980
33. Clancy G J: Percutaneous Kirschner wire fixation ofColles’ fractures. J Bone J0intSurg [Am] 66:1008,1984
34. DePalma AF: Comminuted fractures of the distal end ofthe radius treated by ulnar pinning. J Bone Joint Surg[Am] 34:651, 1952 ....
35. Dowling JJ, Sawyer B: Comminuted Colles’ fractures.Evaluation of a method of treatment. J Bone Joint Surg[Am] 43:657, 1961
36. Garner RW, Grimes DW: Percutaneous pinning of dis-
placed fractures of the distal radius. Orthop Rev 6:87,1977
37. Roth B: Experience with percutaneous K-wire osteosyn-thesis in distal radius fractures. Helv Chir Acta 44:35,1978
38. Ruiz GR: Percutaneous pinning of comminuted Colles’fractures. Clin Orthop 155:290, 1981
39. SteinAH, KatzSF: Stabilizationofcomminuted fracturesof the distal inch of the radius: percutaneous pinning.Clin Orthop 108:174, 1975
40. Lucas GL, Sachtjen KM: An analysis of hand functionin patients with Colles’ fractures treated by Rush rodfixation. Clin Orthop 155:172, 1981
41. Augereau B, Kerboul M: L’Osteosynthese par plaque desfractures instables due poignet a deplacement anterieur.Int Orthop 7:55, 1983
42. Bohler J: Colles’ fractures. Clin Orthop 147:310, 198043. Melone CP: Articular fractures of the distal radius. Or-
thop Clin North Am 15:217, 198444. Weiss H, Wilde CD, Betas H: Vergleichende Behan-
dlungsergebnisse zwischen operative und konservativversorgten besonderen frakturformen am radius locotypico. Hefte Unfallmed 143:418, 1977
45. Bohler L: The treatment of fractures. New York, 1932,Grune & Stratton, pp 90-6
46. Dabezies E J, Chuinard RG, Kitziger RF: Distraction pin-ning for radial metaphysis fractures. Orthopedics 1:294,1978
47. Hammond G: Comminuted Colles’ fracture. Am J Surg54:617, 1949
48. Kain T, Mandel R J, Snedden HE, Steward WG, AdamsDJ: Comminuted distal radius fractures: two methods oftreatment. Clin Orthop 128:369, 1977
49. Ledoux RA, Theibaut A, Van der Ghinst M: Bipolarfixation of fractures of the distal end of the radius. IntOrthop 3:89, 1979
50. Suman RK: Unstable fractures of the distal-end ofthe radius (transfixion pins and a cast). Injury 15:206, 1983
51. Chapman DR, Bennett JB, Bryan WJ, Tullos HS: Com-plications of distal radial fractures: pins and plaster treat-ment. J HAND SURG 7:509, [’982
52. Andrianne Y, Donkerwolcke M, Hinsenkamp M, QuintinJ, Rasquin C, E1Banna S, Bumy F: Hoffman externalfixation of fractures of the radius and ulna. A prospectivestudy of 53 patients. Orthopedics 7:845, 1984
53. AscheG: Stabilization ofcominuted fracturesofthedistalradius uging the external midifixateur. Handchirurgie15:38-42, 1983 .
54. Cooney WP: In Edwards C, editor: External fixation.The current state of the art. New York, 1979, Williams& Wilkins, p 83
55. Cooney WP: External fixation of distal radius fractures.Clin Orthop 180:44, 1983
56. D’Anca AF, Strrnlieb SB, Byron TW, Feinstein PA: Ex:

Vol. 11A, No. 2March 1986 Severely comminuted distal radial fractures 165
ternal fixation in the management of unstable Colles’fractures. Orthopedics 7:841, 1984
57. DeLee JC: External fixation of the forearm and wrist.Orthop Rev 10:43, 1981
58. Forgon M, Mammel E: The external fixator in the man-agement of unstable Colles’ fractures. Int Orthop 5:9,t981
59. Gjengedal E: Compound fracture of the distal end of theradius treated with Hoffman’s method of external fixa-tion. Tidsskr Nor Laegenforen 99:24, 1979
60. Grana WA, Kopta JA: The Roger Anderson device in thetreatment of fractures of the distal end of the radius. JBone Joint Surg [Am] 61:t234, 1979
61. Grana WA, Randel RL: Roger Anderson Device for distalradius fractures. Association for the Organization of Reg-istered Nurses 28:1036, 1978
62. Jakob RP: Distraction of unstable distal comminuted ra-dius fractures with an external fixation device: a new wayof treatment. Z Unfallmed Beruf 73:115, 1980
63. Lanz U, Kron W: Neue technik zur korrektur in fehls-tellung Verheilter distalen radius frakturen. Handchirur-gie 8:203, 1976
64. Osborne F, Weber ER: Distal radial fractures in the adult.J Arkansas Med Soc 77:161, 1980
65. Rasquin C, Burny F, Andrianne Y, Quintin J: Traitementdes fractures du poignet par fixateur externe. Indicationset premiers resultats. Acta Orthop Belg 45:678, 1979
66. Ricciardi L, Diquigiovanni W:- The external fixationtreatment of distal articular fractures of the radius. Or-thopedics 7:637, 1984
67. Riggs SA: External mini-fixation of the hand, wrist, andforearm. Presented at the American Society for Surgeryof the Hand, New Orleans, Louisiana, Feb., 1981
68. Riggs SA, Cooney WP: External fixation of complexhand and wrist fractures. J Trauma 23:332, 1983 ̄
69’. Santavirta S, Karaharju.E, Korkala O: The use of osteo-taxis as a limb salvage procedure in severe compoundinjuries of the upper extremity. Orthopedics 7:642, 1984
70. Schuind F, Donkerwolcke M, Burny F: External fixationof wrist fractures. Orthopedics 7:841, 1984
71. Thomine JM, Demesy M: Le fixateur externe metacarpo-radial dans le traitement des fractures graves de L’Ex-tremite inferieure du radius. Ann Chir 33:731, 1979
72. Vidal J, Buscayret C, Fischbach C, Brahin B, Paran M,Escare P: Une methode originale dans le traitement desfractures comminutives de l’extremite inferieure du ra-dius: le taxis ligamentaire. Acta Orthop Belg 43:781 1977
73. Wild JJ, Hanson GW, Bennett JB, Tullos HS: Externalfixation use in the management of massive upper ex-tremity trauma. Clin Orthop 164:172, 1982
7L~.Van der Linden W, Ericson R: Colles’ fracture. Howshould its displacement be measured and how should itbe immobilized? J Bone Joint Surg [Am] 63:1285, 1981
75;.Chrisman OD, Shortell JH: Fractures of the distal endof the radius complicated by fractures of the carpal scaph-oid. N Engl J Med 241:58, 1949
76. Moller BN: Simultaneous fracture of the carpal scaphoidand adjacent bones. Hand 15:258, 1983
77. Smith JT. Keene JP, Bertin K, Mann RJ: Simultaneousfractures of the distal radius and scaphoid. Read at theWestern Orthopedic Association Annual Meeting, SanDiego, California, October, 1984
78. Mohanti RC, Kar N: Study of triangular fibrocartilageof the wrist joint in Colles’ fracture. Injury 11:32 I, 1979
79. Knirk JL, Jupiter JB: Intraarticular distal radius fracturesin young adults. Presented at the 52nd Annual Meeting,American Academy of Orthopedic Surgeons, Las Vegas,Nevada, Feb., 1985