Embed Size (px)
Citation preview

Cohort Studies
November 4 2004Epidemiology 511
W. A. Kukull

Cohort Studies
D isease N o D isease
E X P O S E D
D isease N o D isease
N O TE X P O S E D
D efin ed P op u la tion
Prospective/Concurrent Retrospective
Today
The Future
The Past
Today
exclude“Diseased”

Retrospective v. Prospective• Retrospective
– Cohort is Reconstructed by the investigator– Both exposure and outcome occur before study
begins– Depends on record quality
• Prospective – Cohort is Established by investigator– Outcomes occur after study begins
• Loss to follow up is the major threat to validity for both types of cohort study

Cohort Types(not seen in Gordis)
• Closed or Fixed– a fixed set of persons followed from starting
point to endpoint– most common in short term studies
• Open or Dynamic– Additional persons can enter with time– a subject can contribute person-time to several
exposure and confounder categories

Design a cohort study: does HDL cholesterol level decrease risk of stroke?
• Population:– Reference or base population– Who will be included? How sampled?– How many to include?
• Disease incidence?
• Exposure frequency?
• Follow-up time: will we have enough cases to analyze by the end of our “grant cycle”?
Enrollment in the cohort:Non-Participation During Cohort Formation
• Those who agree to participate may differ importantly from those who do not agree
• Affects Generalizability of association– is the “risk” found by the study likely to apply to non
participants, Do exposure profiles differ?– Incidence estimates may be affected
• Does not usually affect validity of association – population disease/exposure rates may be
underestimated but the observed association will be valid

Non-Participation (2)
• If non-participants are both exposed and are independently at high (or low) disease risk, then a biased estimate of association (e.g., RR)
• If non-participation is related only to exposure or only to outcome, the association will be valid but power may be reduced.
• IN CONTRAST: non-participation is a major source of bias in Case-control studies or prevalence studies

Increase response rates
• Mail Surveys– Multiple mailing
• Telephone interviews– Interviewer experience
• In-person Interviews– Home– Clinic– Other

Starting with Non-Diseased:How do we exclude persons with stroke hx?
• Medical Records
• Employment records
• Personal Interview
• Screening test; biomarkers
• Full Clinical exam– lab and radiology(CT/MRI), – Hx, PE

Natural Hx of Diseasegenerally speaking…
PreClinical Phase
Biologic onset of disease
Clinical Phase
Sx Dx
Rx
Outcome
Which exposures are relevant to disease onset?
• Too close to onset, disease already active
• Exposure level may fluctuate
• Too distant exposures may not be possible to cause onset
• Changes in exposure during f/u
• Know as much as you can about the disease and potential mechanism of exposure action
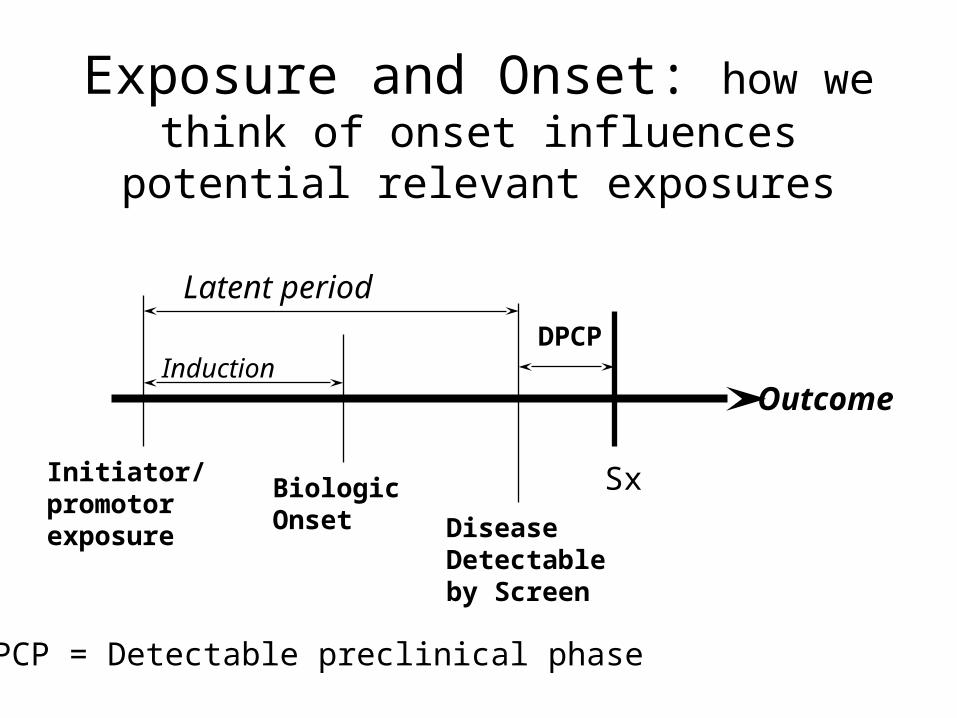
Exposure and Onset: how we think of onset influences potential relevant exposures
Latent period
Induction
Initiator/promotorexposure
Biologic Onset Disease
Detectable by Screen
Sx
Outcome
DPCP
DPCP = Detectable preclinical phase
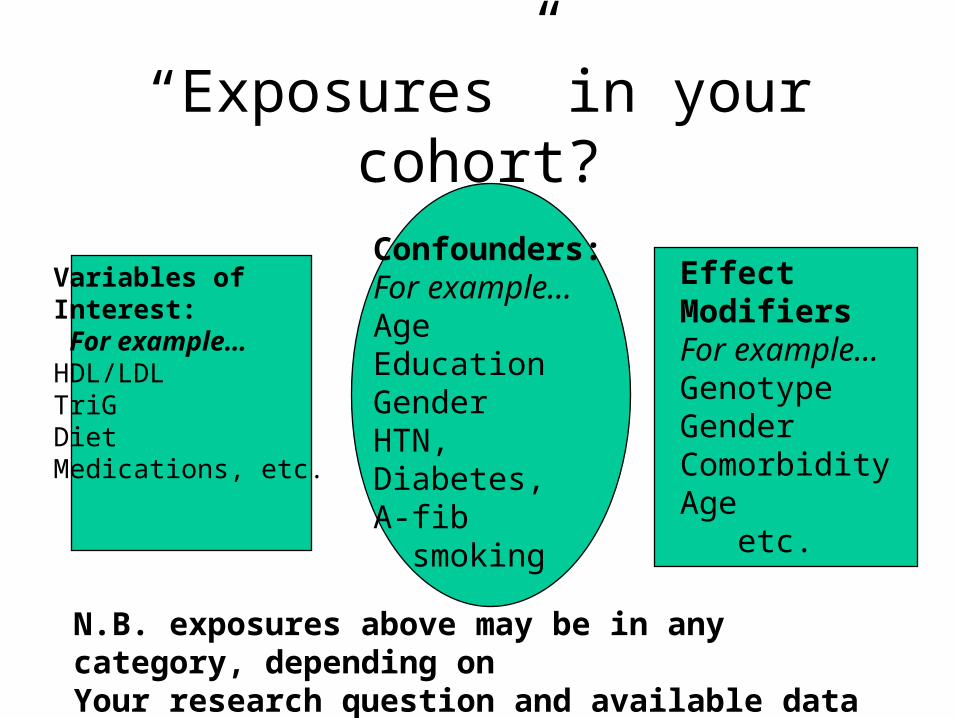
“Exposures” in your cohort?
Variables ofInterest: For example…HDL/LDLTriGDietMedications, etc.
Confounders:For example…AgeEducationGenderHTN,Diabetes,A-fib smoking
Effect ModifiersFor example…GenotypeGenderComorbidityAge etc.
N.B. exposures above may be in any category, depending on Your research question and available data
How will exposure information be obtained at baseline and F/U?
• Biological measurement (e.g., HDL)
• Questionnaire
• Self/proxy-report interview
• Clinic/hospital records
• Will data collected at f/u be different from baseline?– Blood samples; exams; interviews

Defining Follow-up
• How often will the cohort be “followed”– Continuous surveillance possible?– Monthly, yearly, every 3 years– What is feasible re: staff
• How will “disease” occurrence be counted?– Onset at f/u visit? Onset between visits?– Impact on person-time to disease onset
Stroke happens!Finding the incident cases from the cohort
• Establish firm definition of “case” – Ischemic or hemorrhagic stroke
• First occurrence?
– Clinical criteria; confirmed by imaging?– Pathology; death certificate
• Records, interview, examination• Regular intervals or continuous surveillance• Age at onset (or accumulated person-time)

Measurement Error: information bias (White et al,1998)
• Errors in Selection or design of instrument
• Errors in instrument use
• Poor execution of protocol
• Inherent subject characteristics
• Drift in accuracy over time
• Errors in data processing

Reducing Measurement Error
• Select a Cohort expected to provide accurate exposure data
• Select a cohort with greater range of exposure.
• Use repeated measurements of exposure• Quality control/reliability & validity • Drop cases that occur close to exposure
measurement time
Retention and Tracking of the Cohort (Hunt & White,1998)
• Enrollment: willingness, commitment, study requirements
• Bonding: newsletters, cards, study theme
• Regular contact (6 – 24 mo)– Tracking system; primary outcomes
• Dedicated staff
• Incentives: like cash or coffee mugs
Loss to follow-up
• Major source of bias in cohort studiesMajor source of bias in cohort studies– What if diseased subjects are lost?– What if exposed persons are lost?– What if 40% of the cohort drops out?
• What to do if it happens?– estimate best and worst case scenarios ( if all
lost subjects did or did not develop outcome)
• Large losses may invalidate the study
Example(See, Hennekens & Buring)
• Consider British Physicians study– ~66% response rate in cohort formation– Heaviest smokers 20 times more likely to die
of lung cancer– Was result invalid due to high non-response?– To obtain a “null” smoking effect: smoking
would have to have been a 30-fold protective factor in the non-respondents
Analysis
• Relative Risk– Cases/person-years (incidence density RR)– Cases per enrolled subjects (cumulative
incidence by end of study period: RR)
• Crude analysis• Stratified analysis • Multivariate analysis
– Logistic, Poisson and Proportional Hazards

Analysis: HDL and Stroke
• Is baseline HDL level associated with stroke occurrence during the study period?– Continuous measure of HDL– Categorical: high/med/low
• Which other factors are also associated with stroke? Do they mix with the HDL effect?– Stratified analysis; multivariate analysis
• Does HDL effect vary by levels of another factor?– Interaction, effect modification– Stratified analysis; multivariate analysis
Cohort Study: strengths
• Useful when Exposure is rare
• Can examine multiple outcomes of a single exposure
• Describes Temporal relationship between exposure and disease
• If prospective, minimizes exposure determination bias
• Allows direct measurement of incidence
Cohort Study: limitations
• Usually Inefficient for rare diseases
• Prospective: usually expensive and long
• Retrospective: requires good records
• Validity of the results can be seriously
affected by losses to follow-up

Cohort v. Case-Control
• Suppose 8 well-designed case-control studies consistently found an elevated odds ratio--- Would a Cohort study be warranted?
• What qualities would we want to have in cohort study enrollees?
• What sources of bias are more likely in each study design?





























