Embed Size (px)
Citation preview

Research in Developmpnml Disabilrries. Vol. 10. pp. 251-260. 1989 08914222/89 13.00 + .OO Printed in the USA. All rights reserved. Copyright 0 1989 Maxwell Pergamon Macmillan plc
Cognitive Battery for Differential Diagnosis of Mental Retardation vs. Psychosis
Stanley R. Kay
Department of Psychiatry, Albert Einstein College of MedicinelMontefiore Medical Center and
Bronx Psychiatric Center
Because of their severe cognitive and social deficiis, seriously impaired and re- gressed psychotics are often misdiagnosed as mentally retarded. This diagnostic
confusion, which carries dire consequences for treatment, has prevailed due to the lack of objective tests directed at this problem. Procedures are needed to specifically measure and differentiate the hallmarks of the intellectual dysfunc- tion in both conditions (i.e., cognitive abnormality /psychosis] and subnormality
[mental retardation]). Such methods also must be adapted to the particular prob- lems and limitations of these populations. We propose here the use of three long
established tests and a new developmentally rooted Cognitive Diagnostic Battery, one that assesses conceptual, perceptual-motor, and social maturity. Empirical study supported the validity of this Battery for differential diagnosis between mentally and functionally retarded psychotics matched for IQ, with 91% of the
developmentally disabled group exhibiting deficits on all three tests of conceptual
development vs. 27% in the functionally mentally retarded group.
MENTAL RETARDATION VS. PSYCHOSIS: A DIAGNOSTIC DILEMMA
Diagnosis is of fundamental consequence for the treatment and prognosis of psychiatric patients. However, even with advances such as the DSM-III, the process remains largely an art form, dominated by subjective clinical judgments. This situation is especially true for the difficult distinction be- tween mental retardation and psychiatric disorder. Central to the diagnostic
Summary of paper presented at the International Research Conference on the Mental Health Aspects of Mental Retardation, University of Illinois at Chicago, Evanston, Illinois, June 9,
1987, as part of the Symposium on “Schizophrenia and Mental Retardation,” chaired by Dr.
Andrew H. Reid.
Requests for reprints should be addressed to Dr. Kay, Schizophrenia Research Program, 1500 Waters Place, Bronx, NY 10461.
251

252 S. R. Kay
differentiation is the vague boundary line between mental subnormality- the intellectual deficit characteristic of mental retardation-and cognitive abnormality-the disrupted or regressed intellectual functioning that is common in psychosis. The reason for the frequent confounding of these two kinds of cognitive impairment is two-fold. First, there are many shared characteristics that blur the fundamental differences, and second is the lack of reliable, standardized methods to objectively delineate between the two conditions.
By textbook definition, the distinction between mental and functional retardation is clear-cut. Mental retardation is considered a developmental disability characterized by mental subnormality (IQ of 70 or below) which originates during the developmental course (prior to age 18) and is asso- ciated with failures in adaptive functioning (American Psychiatric Associa- tion, 1980). By contrast, functional retardation refers to defective intelli- gence (also an IQ of 70 or below), but of nondevelopmental origin, typically the consequence of regression or a disorganized state seen most notably in schizophrenia.
In reality, however, this differentiation is not self-evident. Like mentally
retarded persons, psychotics often exhibit failures in adaptive functioning, though due to psychiatric rather than developmental reasons. Most vexingly, the cognitive impairment of schizophrenia can be highly similar to that of mental retardation both in its quality and severity. Schizophrenic patients are often concrete, egocentric, and childlike in their thinking, which may
suggest faulty cognitive development (Blatt & Wild, 1976). They are not always thought disordered (Harrow, Tucker, Himmelhoch, & Putnam, 1972), and yet their IQs tend to be far below normal. Payne (1973) reported that the average IQ for certain nonremitted schizophrenics, such as the catatonic and hebephrenic subtypes, falls only in the 60s (i.e., in the range of
mild mental deficiency). Adding to the difficulty, mentally retarded persons often resemble psy-
chotics both in their intellectual level and behavioral profile. Like chronic regressed schizophrenics, a majority of the mentally retarded population falls in the mildly defective region, with IQs between 50 and 70 (Birch, Richardson, Baird, Horobin, & Illsley, 1970). In addition, a startling pro- portion-perhaps up to 40% (e.g., Conley, 1973) -is found to have diagnos- able psychiatric disorders, quite possibly devolving from impaired ego devel- opment. This data raises the question of whether the intellectual problem may not in fact be at least partly functional.
Indeed, a third branch to the diagnostic dilemma of subnormality VS.
abnormality presents itself: the dual condition of mental retardation and psychosis, which Reiss and associates (Reiss, Levitan & McNally, 1982) have aptly described as one of the most misdiagnosed and underserved condi- tions. Even among patients without a formal dual diagnosis, we often see

Mental Retardation vs. Psychosis 253
combined developmental and functional sources of cognitive disorder. Ex- amples include adults with a childhood history of autism, schizophrenia, or attention deficit disorder who now present residual deficits. Another case in point are chronic schizophrenics with a prominent negative syndrome, which seems traceable to poor premorbid adjustment, disrupted education, and early cognitive developmental failures (Kay, Opler, & Fiszbein, 1986). To sum up the diagnostic problem: early intellectual disorder may carry dire psychiatric consequences, and similarly early psychiatric disorder may carry dire intellectual consequences.
COGNITIVE ASSESSMENT: THE KEY TO DIFFERENTIAL DIAGNOSIS
Despite the similarities and overlap among cases with subnormality and abnormality, there remain several crucial distinctions. These are to be found in the longitudinal and qualitative aspects of the mental deficiency, namely its source and nature, rather than in the surface IQ measure. Thus, for an adult with defective intelligence, the question of “true” mental retardation hinges on whether the cognitive processes have fully matured. If intellectual growth is impaired, the next consideration is whether the developmental lag is selective (i.e., evidenced in certain cognitive realms [such as the visual- motor]) but not others (such as the conceptual). For instance, a chronic schizophrenic patient with substandard intelligence, neurological soft signs, and a poor scholastic record would not be considered mentally retarded if there is evidence of normal conceptual growth.
Unfortunately, the developmental data needed to resolve this important diagnostic issue are often unavailable, unreliable, or ambiguous. Retrospec- tive reports by parents and teachers are subject to distortions of memory and personalized interpretations, and psychosocial records are not always thor- ough nor consistent. Even a well documented history of failing grades and other adaptive difficulties might reflect on either intellectual deficit or psy- chiatric disturbance. The more decisive formal IQ testing usually is not performed until after a psychiatric problem has surfaced and the opportuni- ty to assess the premorbid cognitive growth has already passed.
It should be stressed that IQs obtained in adulthood carry no direct developmental implications. Though the original IQ concept was indeed a developmental one, this has long since been replaced by a cross-sectional normative one. Thus, the “ratio IQ,” referenced to an individual’s mental age, has given way to the present “deviation IQ,” which is instead referenced to population norms. A defective adult IQ, for this reason, cannot be inter- preted in terms of a particular mental age nor as a reflection of cognitive immaturity. The test score therefore raises the possibility of a diagnosis of mental retardation without a basis for confirmation. The likelihood of the

254 S. R. Kay
mental deficiency representing something other than retardation is, of course, especially pronounced in a psychiatric population.
More generally, since IQ scales have been devised for and standardized on the normal population, their application to clinical groups is questionable. For instance, the tests are geared to the normal range of performance and are academically oriented in content. In these respects, they are not sensitive to variations at the low extreme, and they focus on cognitive product (ability scores) rather than the cognitive processes and disorders that prevail in psychiatric conditions. The conventional IQ scales also tend to be too long, too difficult, and too esoteric to sustain the cooperation of functionally or intellectually impaired patients. As a result, these patients are considered “untestable,” a misleading label which, oddly, shifts the onus of test compat- ibility from the test itself onto the patient.
But above all, the meaning of a defective IQ score is ambiguous: it tells little about the reason for the intellectual disorder (i.e., the source and processes involved). In a psychiatric population there are many possible bases for impaired test performance. Schizophrenics may score poorly, for example, due to fundamental disorders of information processing, such as failures of attention and verbal encoding, which impede higher-order mental operations (Kay, 1982b). In addition, even the noncognitive disorders of schizophrenia, such as apathy, amotivation, and hyperarousal, can seriously confound test interpretation. Chapman and Chapman (1978) have pointed out that, as a group, schizophrenics show deficits on virtually any structured task that calls for voluntary response, even a simple tapping speed test.
Using psychometric jargon, it may be said that IQ scales lack construct validity with psychiatric patients, because defective scores cannot be related to the presumed construct. A low IQ may signify mental subnormality, cognitive abnormality, or any number of noncognitive symptoms. Not sur- prisingly, then, intelligence tests are highly sensitive to schizophrenic impair- ment and to mental decline as the illness advances (Batman, Albee, & Lane, 1966) but they have been of little use in differentiating psychotic from retarded persons.
In view of these limitations, Reiss et al. (1982) have presented a starkly critical overview of the role of psychometrics for separating apart functional and developmental retardation. They concluded, “There are no psychologi- cal tests to enable us to make this diagnosis objectively; instead the diagnosis is based [only] on subjective evaluations and discrepancies in clinical infor- mation” (p. 362).
PROPOSED BATTERY FOR DIFFERENTIAL DIAGNOSIS
A possible resolution comes from the recent movement in intellectual assessment calling for departure from the conventional, norm-guided psy-

Mental Retardation vs. Psychosis 23-S
chometric approach in favor of new theory-guided tests (Sternberg, 1981). Measures of this kind focus on specific mental operations and processes and judge performance relative to one’s own cognitive profile (idiographically) rather than relative to the general population (nomothetically). In addition, to assess subnormality in psychiatric groups, methods are needed which are developmentally rooted, examine specific spheres of functioning, and are suited for patients who may be nonverbal, severely limited intellectually, and defective in their attention, motivation, and cooperation. Let us now con- sider four test procedures- three well-established and one newly devel- oped- which, especially in combination, offer an objective basis for an informed diagnostic decision.
1. Since mental retardation is partly defined by low IQ score, we require an IQ scale that is applicable for psychotic or low-functioning patients. Such a purpose is served by picture vocabulary testing. This technique, exemplified by the Quick Test (Ammons & Ammons, 1962), involves select- ing one of several cartoon pictures that corresponds to a vocabulary word that is presented orally. Because the assessment depends on recognition vocabulary instead of more loosely structured or open-ended tasks, it is relatively resistant to interference from psychotic processes. Importantly, it applies a brief, vivid format suited for patients with limited attention, moti- vation, and communicational skills.
2. As a counterpart to verbal IQ, human figure drawing tests provide for perceptual-motor assessment. The task is brief, elementary, and nonverbal. Using the Goodenough-Harris norms (Harris, 1963) one can reliably esti- mate mental age by presence of such features as use of perspective, two- dimensional portrayal, *and realistic proportions. Scoring is based on devel- opmental norms and thereby addresses the maturity, rather than the general competence, of the drawings.
3. Another major indication of retarded development derives from the social realm, which also reflects on adaptive functioning. The Vineland Social Maturity Scale (Doll, 1965) assesses social development using a struc- tured observational scale that is rated by family members or hospital staff. The procedure thus is usable even with patients who are uncooperative, nonverbal, or otherwise “untestable.” Questions about the patient’s func- tional competence form the basis for a social age, which is referenced to developmental norms. In this way, the scale distinguishes adaptive failure relating to developmental vs. psychiatric factors. A comparison of develop- mental levels in the subareas assessed further reflects on the generality of the social deficit. A nonretarded schizophrenic, even if socially withdrawn, can be expected to show mature social development on the scale, or at least in certain subareas, such as communication, self-help, or socialization.
4. Finally, of prime importance is the question of whether conceptual and visual-motor growth have been completed. This factor is addressed by

256 S. R. Kay
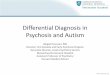
our own test series (Kay, 1982a), the Cognitive Diagnostic Battery (CDB; see Table 1). The CDB utilizes a Piagetian framework to assess developmental impairments and to distinguish these from other intellectual deficits and abnormalities that prevail in psychosis.
The first test in the CDB series, the Color-Form Preference Test, is a 20- item similarity judgment task which examines primitive bases for perceiving relationships and prerepresentational modes of thinking. The patient is asked to match a standard card with one of three cards similar in color, form, or neither cue. The response strategy is analyzed and translated ac- cording to the earlier stages of conceptual development. This is character- ized sequentially by purposeless perseveration (the stage of primary and secondary circular reactions), random response (coordination of secondary reactions), concepts dependent on perceptually salient cues (preconceptual operations), mixed color and form preference (stage of intuitive thought), and invariant application of form (concrete operations).
Using a similar paradigm, the Color Form Representation Test extends this developmental hierarchy to focus on the later verbal-symbolic stages of conceptual growth. It introduces the option of matching cards by figural representation, which is a maturer basis than either color or form. This reflects reliance on cues that are perceptually less salient while semantically and conceptually more relevant (i.e., the cognitive style dominant in the stage of formal operations, from 11 years to adult).
The Egocentricity of Thought Test is a measure of socialized thinking that derives from Piaget’s studies of how subject-object relations evolve in children. The test assesses mastery of four phases in the acquisition of positional concepts: preconceptual (up to age 5 years), egocentric (ages 5 to 8), socialized (ages 8 to 1 l), and objective (ages 11 to adult).
The Progressive Figure Drawing Test involves drawing from copy seven simple designs that children normally master at successive age periods be- tween 2 and 6 years. Serving as an index of visual-motor development, the test yields a mental age estimate that corresponds to the most advanced figure successfully reproduced.
Devised for a psychotic population, the CDB tasks are brief, elementary, sensitive to low-level functioning, and require little attention and no verbal output. The half hour battery was standardized with psychiatric inpatients as well as with normal children and adults, and on a total sample of approxi- mately 400 subjects it has shown various facets of reliability and validity (Kay, 1982a). Of particular importance has been its ability to distinguish schizophrenic from mentally retarded psychotics, who showed far greater deficits on the developmental measures. By virtue of the standardization samples, CDB norms and cut-off scores provide a probabilistic basis for ruling out mental retardation in a psychiatric population.

TA
BL
E
1
Ove
rvie
w
of
the
Co
gn
itiv
e D
iag
no
stic
B
atte
ry
Tes
t A
rea
of C
ogni
tive
Ass
essm
ent
Tes
t Mat
eria
ls
Tas
k In
volv
ed
Bas
is f
or S
cori
ng
Con
trib
utio
n to
the
C
ogni
tive
Tes
t Bat
tery
CFP
CFR
EO
T
PF
DT
Ear
ly c
once
ptua
l de
- ve
lopm
ent
Util
izat
ion
of h
ighe
r-
orde
r co
ncep
ts
Dev
elop
men
t of
so-
ci
aliz
ed t
hink
ing
Perc
eptu
al-m
otor
de
-
20 s
ets
of c
ards
tha
t di
spla
y co
mbi
natio
ns
of c
olor
and
fo
rm
20 s
ets
of c
ards
tha
t di
spla
y Se
lect
ing
optim
al
mat
ch t
o co
mbi
natio
ns
of c
olor
, st
anda
rd
card
on
the
basi
s fo
rm,
and
figu
ral
repr
esen
- of
col
or,
form
, or
fig
ural
ta
tion
repr
esen
tatio
n
Seri
es o
f qu
estio
ns
to d
eter
- m
ine
whe
ther
th
inki
ng
is
prec
once
ptua
l, eg
ocen
tric
, so
cial
ized
, or
obj
ectiv
e
7 ca
rds
that
dis
play
mod
el
draw
ings
Sele
ctin
g op
timal
m
atch
lo
stan
dard
ca
rd o
n th
e ba
sis
of c
olor
, fo
rm,
neith
er,
or
both
cue
s
To
dist
ingu
ish
righ
t an
d I&
!a
:era
litie
s fr
om o
ne’s
ow
n pe
rspe
ctiv
e,
that
of
anot
her,
an
d re
lativ
e to
ind
epen
dent
ob
ject
s
Dra
win
g de
sign
s by
cop
y
Res
pons
e pa
ttern
an
alyz
ed
for
form
dom
inan
ce,
colo
r do
min
ance
, ra
ndom
re
- sp
onse
, an
d pe
rsev
erat
ion
Num
ber
of o
ptim
al
sim
ilari
- ty
jud
gmen
ts
out
of 2
0 se
ts
Scor
ing
deno
tes
the
high
est
subt
est
leve
l pas
sed
Men
tal
age
asso
ciat
ed
with
ite
ms
succ
essf
ully
re
pro-
du
ced
Ass
essm
ent
of c
once
ptua
l st
yle
char
acte
rist
ic
of p
reve
r-
bal
and
earl
y ve
rbal
dev
el-
opm
ent
Ass
essm
ent
of v
erba
l-sy
m-
bolic
sta
ges
of c
once
ptua
l de
velo
pmen
t, an
d or
ient
a-
tion
to s
eman
tic
rele
vanc
e vs
. pe
rcep
tual
sa
lienc
e
Ass
essm
ent
of t
he l
ater
st
ages
of
subj
ect-
obje
ct
rela
- tio
ns t
hat
brid
ge c
ogni
tive
and
soci
al d
evel
opm
ent,
in-
clud
ing
egoc
entr
icity
, su
b-
ject
ivity
, re
vers
ibili
ty,
rela
- tiv
ity,
soci
aliz
atio
n,
and
obje
ctiv
ity
of t
houg
ht
Ass
essm
ent
of l
evel
of
vis-
ua
l-m
otor
de
velo
pmen
t
Not
e: B
ased
on
Kay
(198
2a).
Abb
revi
atio
ns:
CFP
=Col
or-F
orm
Pr
efer
ence
T
est;
CFR
=C
olor
Fo
rm R
epre
sent
atio
n T
est;
EO
T=E
goce
ntri
city
of
Tho
ught
T
est;
PF
DT
= P
rogr
essi
ve F
igur
e D
raw
ing
Tes
t.

258 S. R. Kay
THE CDB FOR DISTINGUISHING MENTAL VS. FUNCTIONAL RETARDATION
More recent study has found the CDB capable of separating retarded schizophrenics from functionally defective schizophrenics who were matchedfor IQ (Kay, 1986). A diagnosis of mental retardation was indepen- dently established from diagnosis by consensus of a clinical team (psychia- trist, psychologist, and social worker) which provided screening for admis- sions to the Cognitive Development Service, a unit serving the dually diagnosed at Bronx Psychiatric Center. The team applied the criteria for mental retardation of the American Association on Mental Deficiency (Grossman, 1977) as based on the aggregate of four sources of information: (a) developmental history indicating cognitive and social deficits prior to age 18 (e.g., delay in achieving developmental milestones, inability to care for oneself, etc.); (b) continued dysfunction in these realms as judged by subse- quent clinical and behavioral observations; (c) deficiencies in current psy- chometric assessment on the Quick Test (Ammons & Ammons, 1962) and Vineland Scale (Doll, 1965), yielding an IQ below 70 and social development under age 14, respectively; and (d) records of childhood intelligence testing, if available, which report an IQ below 70.
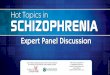
Details of the sample characteristics are summarized in Table 2. The mentally and functionally retarded groups were comparable in sex, race, and chronicity of illness (years since first hospitalization), and they both had subnormal IQs averaging 48 on the Quick Test. The nonretarded patients were significantly older (Student t-test) and, not surprisingly, were first institutionalized at a later age.
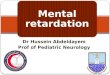
The psychometric comparisons revealed that the two groups could be significantly differentiated on the CDB. Those with an independently docu- mented developmental retardation were more likely to show developmental failure on all CDB tests than the functionally defective schizophrenics of equivalent IQ (see Table 3). As a group, the mentally retarded schizophrenics displayed significantly less test variability. More important, fully 97% of this sample exhibited disorders on all three tests of conceptual development, in contrast to only 27% of the mentally defective nonretarded group (p< .OOOl).
Aside from the statistical comparisons, the very foundation of these tests in developmental theory offers a compelling rationale for ruling out retarda- tion in those who show test competence, regardless of their IQ scores. Demonstration of an adult cognitive mode, even in a mentally defective person, implies completed cognitive development and defies a diagnosis of mental retardation. The IQ measure, by contrast, may be regarded as a surface index of general intellectual functioning which is contaminated by sundry cognitive and noncognitive impairments that are intrinsic to schizo-

Mental Retardation vs. Psychosis 259
TABLE 2
Sample Characteristics of 35 Mentally Retarded and
23 Functionally Retarded Schizophrenics
Schizophrenic Group
Sample Characteristics Mentally Retarded Functionally Retarded
Categorical variables N Males 19 Females 16 Blacks 18 Whites 17
Continuous variables Mean IQ 48 Chronicity of illness (yrs.) 11.6 Age 26.1 Age first hospitalized 14.3
% N % 54 13 56 46 10 44 52 12 51 48 11 49
SD Mean SD 12 48 17 .&l 8.4 14.4 10.4 1.00 5.7 38.7 13.5 4.24b 6.0 23.0 11.2 3.48a
Note: Based on Kay (1986). =p< .005; bp< .OOl.
phrenia and carry no specific developmental import. As such, the common practice of diagnosing retardation exclusively by IQ tests must be cautioned against, especially for an adult clinical population, where abnormality so often masquerades as subnormality.
THE CONTRIBUTION OF PSYCHOMETRICS
Therefore, in answer to the call for more specialized theory-guided tests to differentiate subnormality and abnormality, we might conclude with cau-
TABLE 3
Comparison of Mentally and Functionally Retarded Schizophrenics Achieving Optimal Scores on Developmental Tests from the Cognitive Diagnostic Battery (n=58)
Schizophrenic Group (%)
Cognitive Optimal Mentally Functionally 2 Differences Test Score Retarded Retarded (oneytailed) in Variance
CFP Form 100% 3 23 5.66’ x14= 10.48a CFR 17to20 0 9 3.30a F= 2.10a EOT 3 0 17 6.54’ F= 1.30 PFDT 6+ 23 57 3.36a F= 2.42b
Note: Based on Kay (1986). Abbreviations: CFP=Color-Form Preference Test; CFR =Color Form Representation Test; EOT=Egocentricity of Thought Test; PFDT=Progressive Figure Drawing Test. “p<.O5; bp<.O2; cp<.Ol.

260 S. R. Kay
tious optimism that some objective procedures of this kind are now availa- ble. This is to be viewed, of course, as only a first step and by no means a final step. Hopefully, the availability of new goal-directed tests will catalyze the much needed research on differential diagnosis for the multiply dis- abled. With the help of psychometrics, there is potential for converting diagnosis from mainly an art form, one based solely on open-ended inter- view and subjective ratings, into a truly scientific enterprise. On our success may very well depend the success of our patients.
REFERENCES
American Psychiatric Association. (1980). Diagnostic and statisfical manual of mental disor- ders (3rd ed.). Washington, DC: Author.
Ammons, R. B., & Ammons, C. H. (1962). The Quick Test: Provisional manual. Psychological Reports, 11, 111-161. (Monogr. Suppl. I-VII)
Batman, R. H., Albee, G. W., & Lane, E. A. (1966). Intellectual test performance of chronic
and recovered schizophrenics. Proceedings of the 74th Annual Meeting of the American Psychological Associafion. Washington, DC: American Psychological Association.
Birch, H. G., Richardson, S. A., Baird, D., Horobin, G., & Illsley, R. (1970). Mentalsubnor- mality in the community: A clinical and epidemiological study. Baltimore: Williams &
Wilkins.
Blatt, S. J., & Wild, C. M. (1976). Schizophrenia: A developmental analysis. New York:
Academic Press.
Chapman, L. J., & Chapman, J. P. (1978). The measurement of differential deficit. Journal of Psychiatric Research, 14, 303-3 11.
Conley, R. W. (1973). The economics of mental refardation. Baltimore: Johns Hopkins Univer-
sity Press.
Doll, E. A. (1965). Vineland Social Maturity Scale: Condensed manual of directions. Circle Pines, MN: American Guidance Service.
Grossman, H. (1971). Manual on terminology and classification in mental retardation. Wash-
ington, DC: American Association on Mental Deficiency. Harris, D. B. (1963). Children’s drawings as measures of intellectual mafurity: A revision and
extension of the Goodenough Draw-A-Man Test. New York: Harcourt, Brace, & World.
Harrow, M., Tucker, G. J., Himmelhoch, J., & Putnam, N. (1972). Schizophrenic “thought
disorder” after the acute phase. American Journal of Psychiatry, 128, 824-829. Kay, S. R. (1982a). The Cognitive Diagnostic Battery: Evaluation of intellectual disorders.
Odessa, FL: Psychological Assessment Resources.
Kay, S. R. (1982b). Conceptual disorder in schizophrenia as a function of encoding orientation. Journal of Nervous and Mental Disease, 170, 154-163.
Kay, S. R. (1986). Diagnosis of mental retardation in schizophrenia: Psychometric distinction between intellectual subnormality and abnormality. Journal of Psychoeducational Assess- ment, 4, 13-25.
Kay, S. R., Opler, L. A., & Fiszbein, A. (1986). Significance of positive and negative syndromes in chronic schizophrenia. Brifish Journal of Psychiafry, 149, 439-448.
Payne, R. W. (1973). Cognitive abnormalities. In H. J. Eysenck (Ed.), Handbook of abnormal psychology (pp. 420-483). London: Pitman Medical Press.
Reiss, S., Levitan, G. W., & McNally, R. J. (1982). Emotionally disturbed mentally retarded
people: An underserved population. American Psychologist, 37, 361-367. Sternberg, R. J. (1981). Testing and cognitive psychology. American Psychologist, 36, 1181-1189.