Embed Size (px)
Citation preview
Cochrane Musculoskeletal Group & Patient Decision Aids
May 25, 2013
• Peter Tugwell
• Update on the Cochrane Musculoskeletal Group• Participants will learn different knowledge translation
strategies to disseminate the results of systematic reviews.
• Participants will have an overview of 10 different strategies and will be able to access them and/or get ideas to build their own
2
Learning Objectives
1.Cochrane Collaboration
2.Cochrane Musculoskeletal Group
3.Knowledge Translation
4.10 Ways of presenting Musculoskeletal Cochrane Reviews
5.More on Decision Aids
OUTLINE
3
The Cochrane Library
4
5,131 completed reviews
2235 review protocols674,519 RCTs
Come to our party!
• 2013 is the 20th anniversary of the founding of the Cochrane Collaboration
• 21st global Cochrane Colloquium will be in Quebec City September 19th – 23rd 2013
Cochrane Collaboration in 2013
• 40,000 contributors in 100+ countries• 25,000 authors• 53 Cochrane Review Groups• 13 Cochrane Centres
Please Join!Open to everyone who is committed to the
Cochrane Collaboration Principles
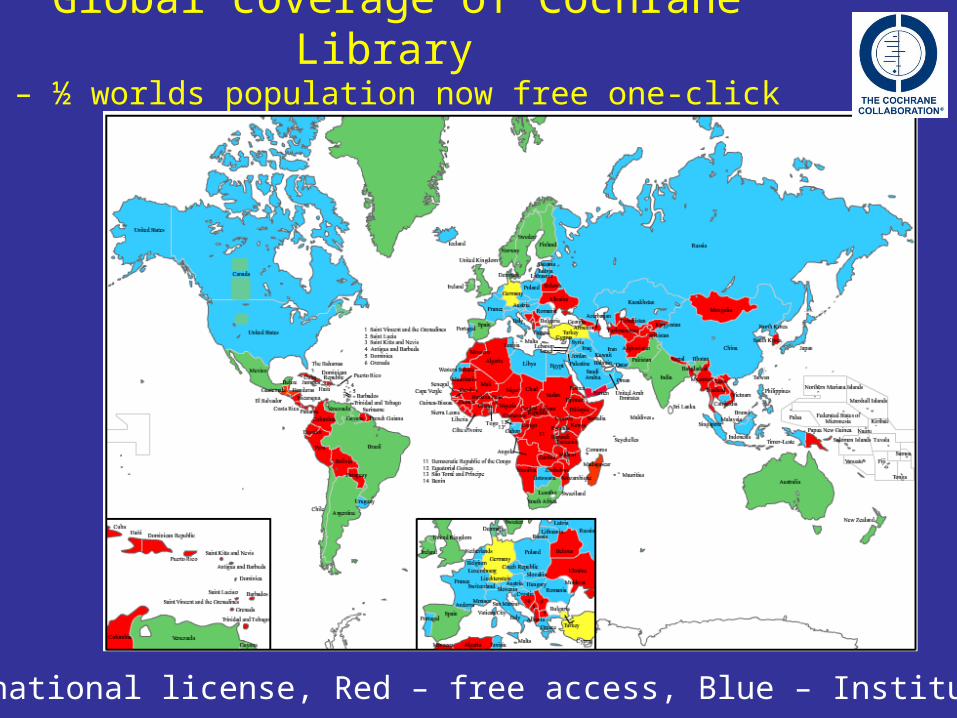
Global coverage of Cochrane Library – ½ worlds population now free one-click access
Green – national license, Red – free access, Blue – Institutions.
Impact factor of CDSR
5.963
top 10 highest General
Medical journals
Impact factor of CDSR
5.963 Up from 5.653 in 2009
top 10 highest General
Medical journals
Up from 14th in 2007
Abstract downloadevery 2 seconds
Impact factor of CDSR
5.963 Up from 5.653 in 2009
top 10 highest General
Medical journals
Up from 14th in 2007
Full text download3 seconds

Impact :‘Cochrane Inside’
The Canadian Cochrane Network and Centre • 2005-2010; Funded by:• CIHR• CIHR Institutes:
• Institute of Gender and Health • Institute of Health Services and Policy Research • Institute of Human Development, Child and Youth Health • Institute of Infection and Immunity • Institute of Musculoskeletal Health and Arthritis • Institute of Nutrition, Metabolism and Diabetes
• CADTH (2005-2008)
12
Cochrane Musculoskeletal Group
• Registered in 1993 in Ottawa, Canada, the Cochrane Musculoskeletal Group
• 161 Cochrane Reviews in Cochrane Library • 31 consumer representatives • In 2005, a second editorial base was
established at Cabrini Institute, University of Melbourne, Australia.
• Satellites in France, Scotland, Wales and USA.
May 2013:161 COCHRANE MUSCULOSKELETAL REVIEWS
Cochrane Musculoskeletal GroupIn press May 31, 2013
Folic Acid with MTX in RA
Shea et al
Hot off the Press!
15
Objectives:
To perform a systematic review of the benefits and harms of folic /folinic acid
1)in reducing the mucosal, gastrointestinal, hepatic and haematologic side effects of Methotrexate (MTX).
2.) To assess whether or not folic/folinic acid supplementation reduces MTX benefit.
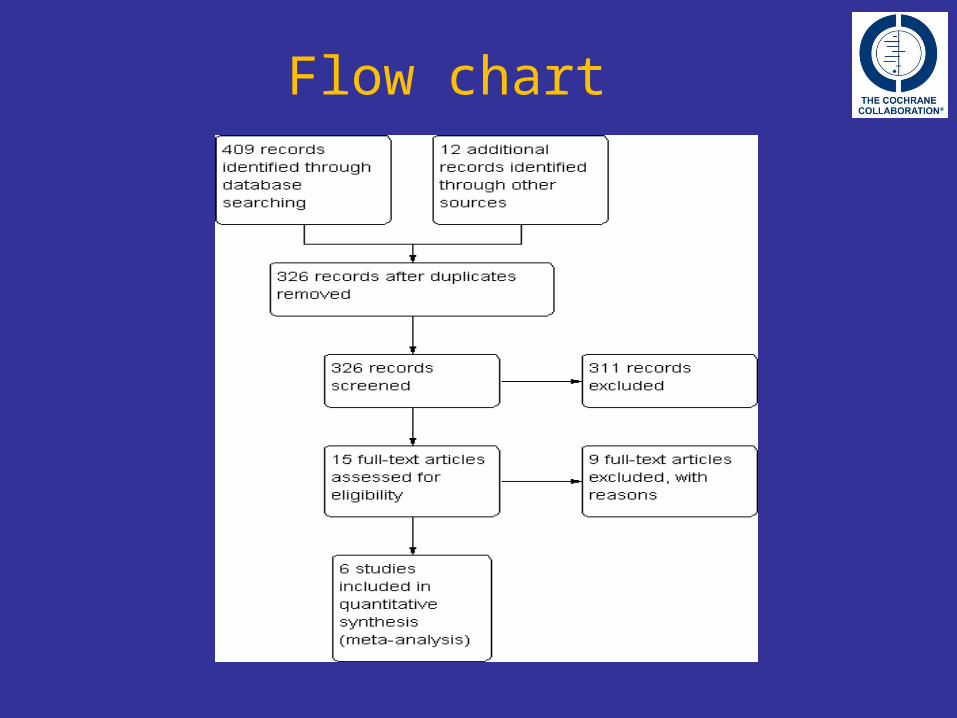
Flow chart
Results
• Best estimate of what happens to people who take folic acid or folinic acid while on MTX
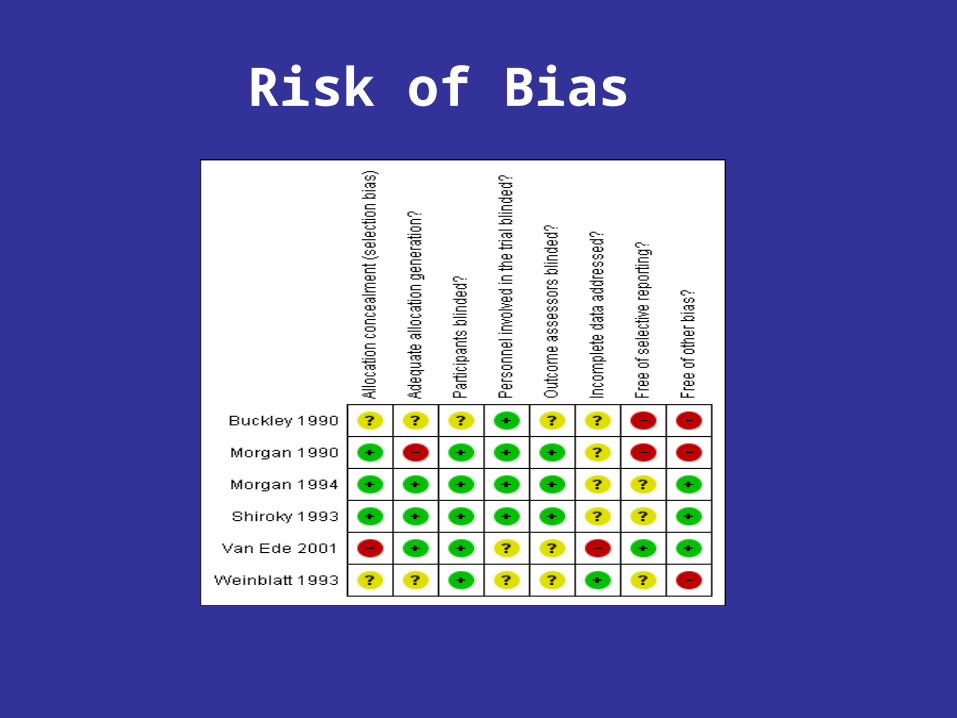
Risk of Bias
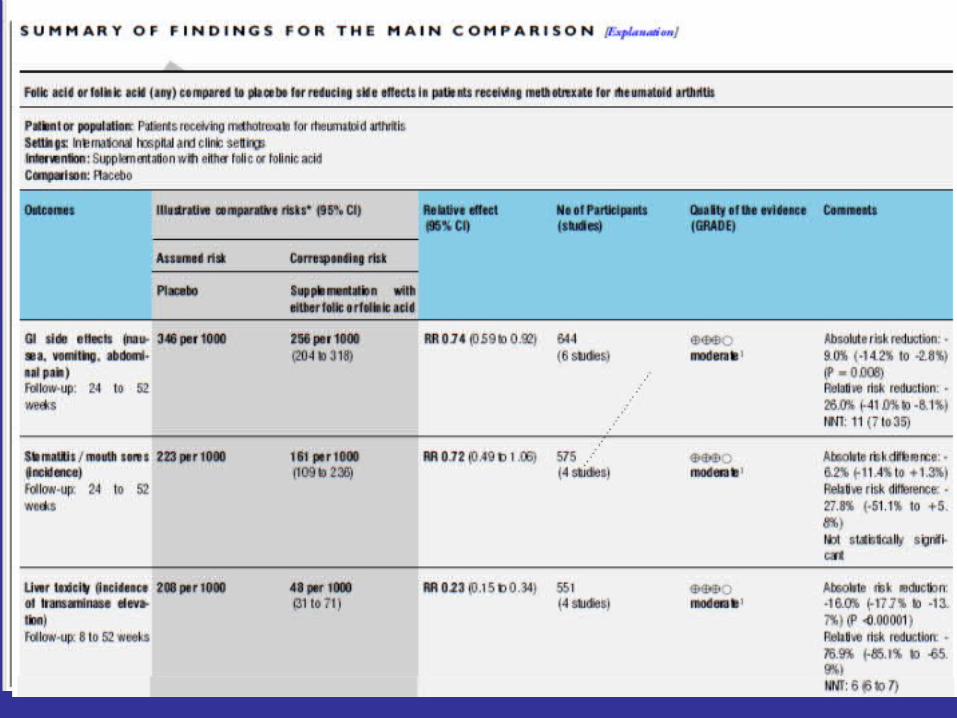
35 people out of 100 experienced stomach problems such as nausea when they took MTX alone for their rheumatoid arthritis;
26 people out of 100 experienced stomach problems such as nausea when they took folic acid or folinic acid with their MTX.
Thus: 9 fewer people out of 100 experienced stomach problems such as nausea up to 6 to 12 months after starting folic acid or folinic acid with their MTX (9.0% absolute improvement);
Stomach problems such as nausea, vomiting or abdominal pain:
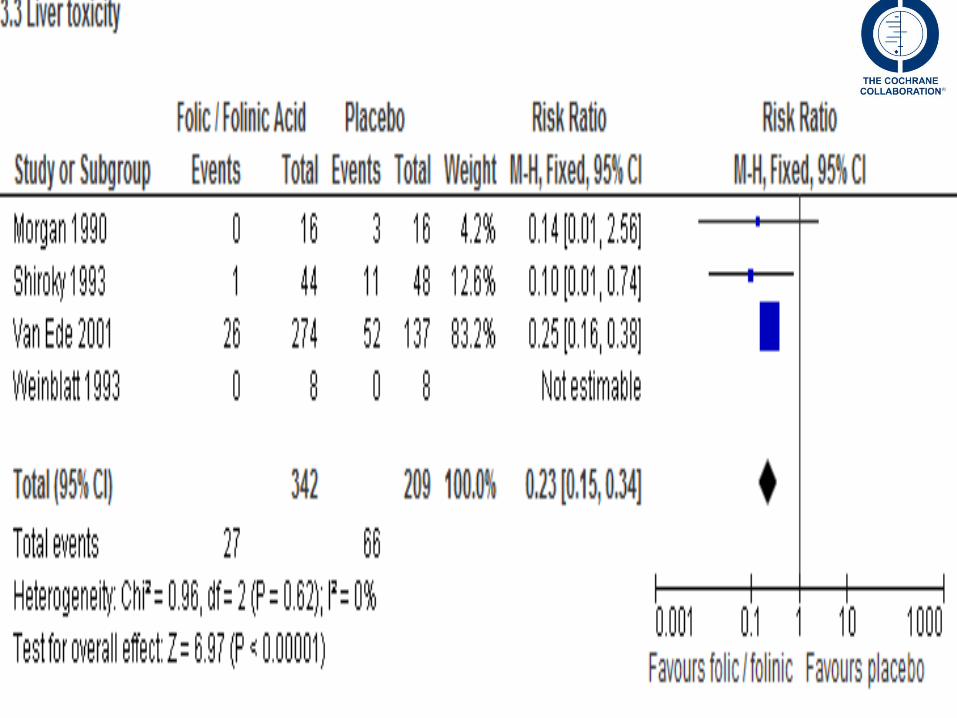
21 people out of 100 experienced abnormal liver blood tests when they took MTX alone for their rheumatoid arthritis;
5 people out of 100 experienced abnormal liver blood tests when they took folic acid or folinic acid with their MTX.
Thus: 16 fewer people out of 100 had liver problems up to 6 to 12 months after they starting folic acid or folinic acid with their MTX (16.0% absolute improvement);
Liver problems (as measured by abnormal liver blood tests):
Folic acid and folinic acid for reducing side effects in patients receiving methotrexate for rheumatoid arthritis
• Conclusions. There was a clinically important significant reduction shown in – the incidence of GI side effects, – hepatic dysfunction – discontinuation of MTX treatment for
any reason.
• The results support a protective effect of supplementation with either folic or folinic acid for patients with rheumatoid arthritis during treatment with MTX.
1. Cochrane Collaboration
2. Cochrane Musculoskeletal Group
3.Knowledge Translation4. 10 Ways of presenting Musculoskeletal Cochrane Reviews
5. Decision Aids
OUTLINE
25
26
Knowledge translation
CIHR definition
‘Knowledge translation is a dynamic and iterative process that includes the synthesis, dissemination, exchange and ethically-sound application of knowledge to improve the health of Canadians, provide more effective health services and products and strengthen the healthcare system.’
27
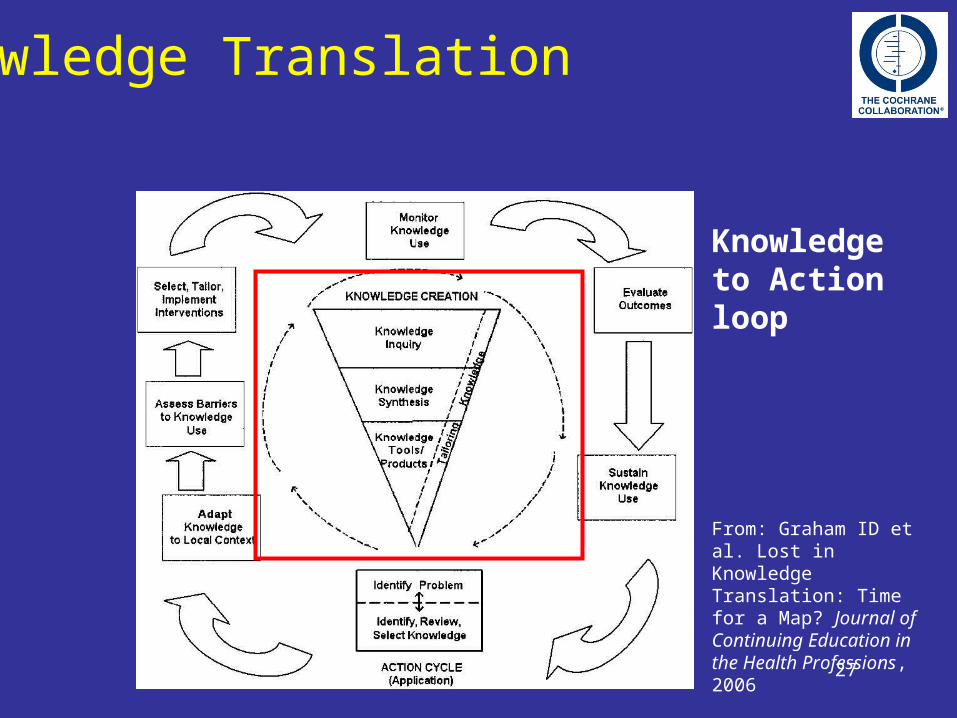
Knowledge Translation
Knowledge to Action loop
From: Graham ID et al. Lost in Knowledge Translation: Time for a Map? Journal of Continuing Education in the Health Professions, 2006
1. Cochrane Collaboration
2. Cochrane Musculoskeletal Group
3. Knowledge Translation
4. 10 Ways of presenting Musculoskeletal Cochrane Reviews
esp Decision Aids
OUTLINE
28
10 Formats for presenting Cochrane Review
Knowledge Translation to Clinicians and Patients: Update from Cochrane Musculoskeletal Group
Tamara Rader, Jordi Pardo , Anne Lydiatt, Dawn Stacey, Elizabeth Ghogomu, Lara J.Maxwell, Jasvinder A. Singh, Rachelle Buchbinder, France Légaré, Nancy Santesso, Peter Tugwell.
29
30
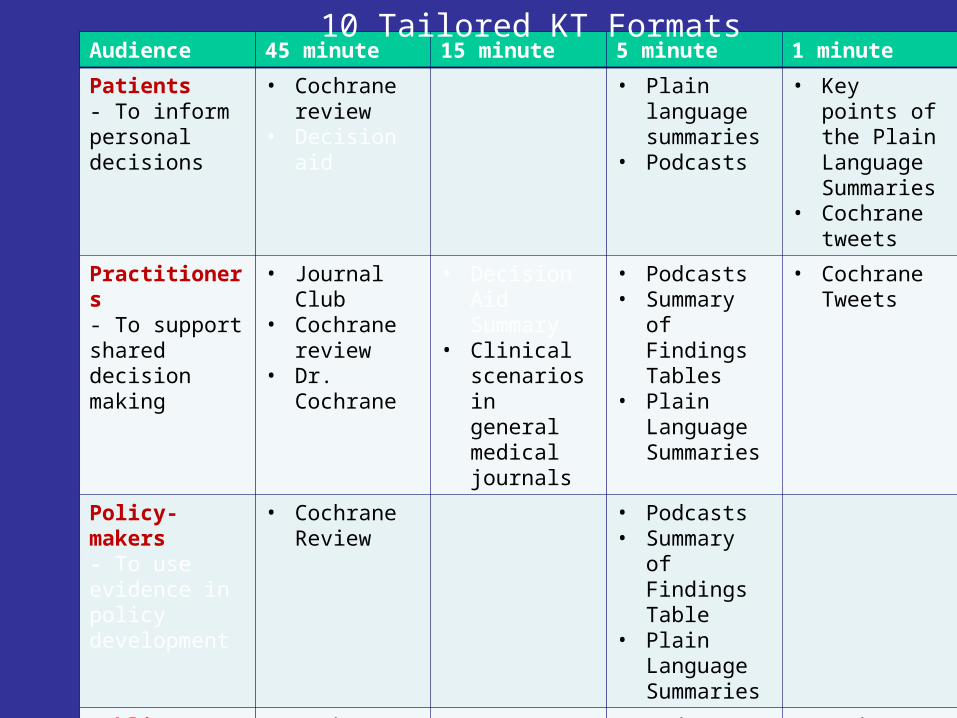
Audience 45 minute 15 minute 5 minute 1 minute
Patients - To inform personal decisions
• Cochrane review
• Decision aid
• Plain language summaries
• Podcasts
• Key points of the Plain Language Summaries
• Cochrane tweets
Practitioners - To support shared decision making
• Journal Club • Cochrane
review• Dr. Cochrane
• Decision Aid Summary
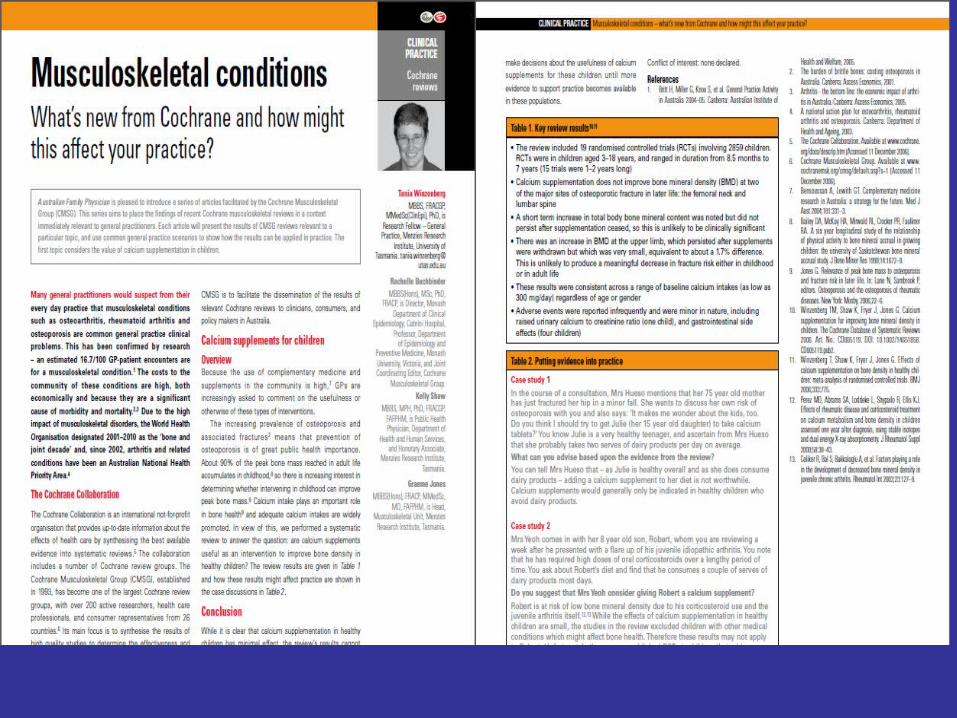
• Clinical scenarios in general medical journals
• Podcasts • Summary of
Findings Tables
• Plain Language Summaries
• Cochrane Tweets
Policy-makers- To use evidence in policy development
• Cochrane Review
• Podcasts • Summary of
Findings Table
• Plain Language Summaries
Public/Press • Cochrane Review
• Podcasts • Press
releases• Plain
Language Summaries
• Cochrane tweets
10 Tailored KT Formats
10 Cochrane KT Formats
1.Cochrane Reviews2.Cochrane Journal Club3.Cochrane Decision Aids4. Cochrane Corners in Journals5.Cochrane Summary of Findings Tables 6.Cochrane Plain Language Summaries7.Cochrane Podcasts8.Cochrane @ Twitter9.Cochrane Clinical Answers10. Dr Cochrane
#1 Cochrane reviews
#1 Cochrane reviews
• Audience: Policymakers, Practitioners, Public, Press
• Time: 45 min to browse
• Consistent format, rigorous methods
#2 Cochrane Journal Club
#2 Cochrane Journal Club
• Audience: Practitioners, Pupils
• Time: 45 min
• Provides clinical results and context, a tool for teaching and self-directed learning
#3 Cochrane Decision aids
#3 Cochrane Decision aids
• Audience: Patients, Practitioners
• Time: 45 min for patients, 15 min summary for practitioners
• Supports shared decision making
• Key features – options – asks personal values/preferences – benefits and harms– quality appraised
Cochrane Review Etanercept Decision Aid
• Take etanercept (Enbrel®): Once or twice a week, you have an injection under the skin in different parts of the thigh or abdomen. A nurse or doctor teaches you how to do this. A family member or friend can also learn. You store the drug in a refrigerator and warm it to room temperature prior to use. Most people who fear self-injection are able to give these injections with mild or no discomfort.
• Decline etanercept (Enbrel®). You may wish to discuss other treatment options with your doctor
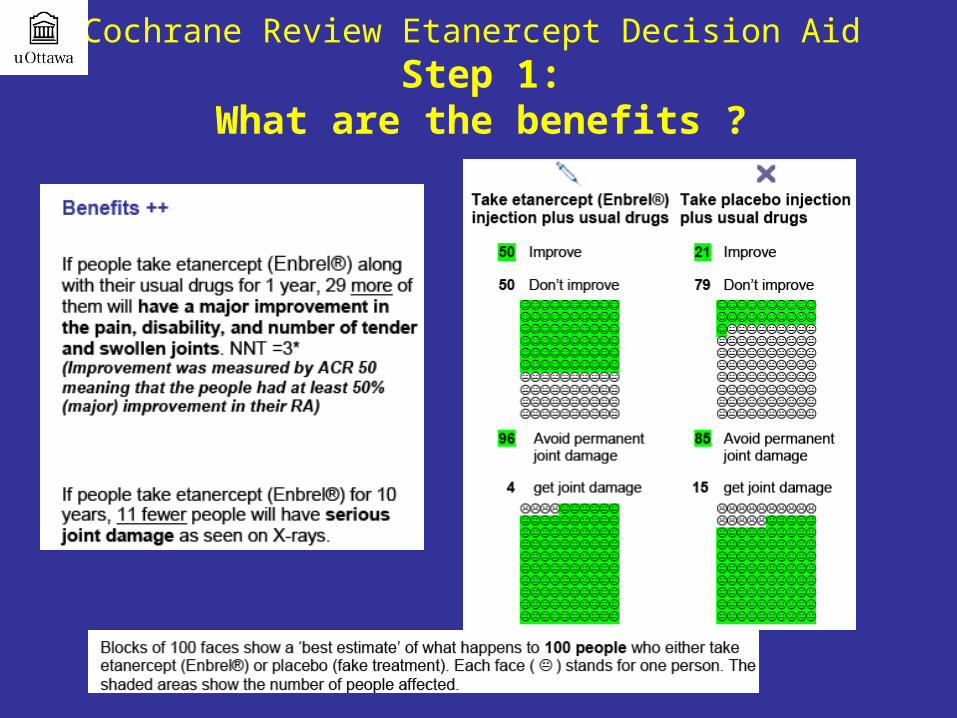
Cochrane Review Etanercept Decision Aid Step 1:
What are the benefits ?
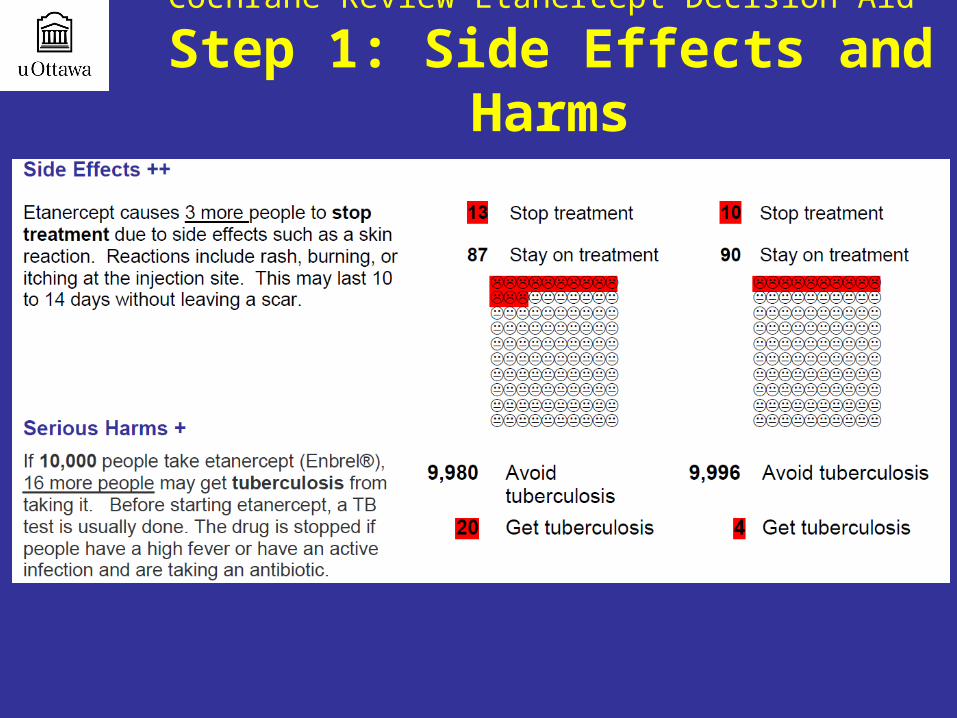
Cochrane Review Etanercept Decision Aid
Step 1: Side Effects and Harms
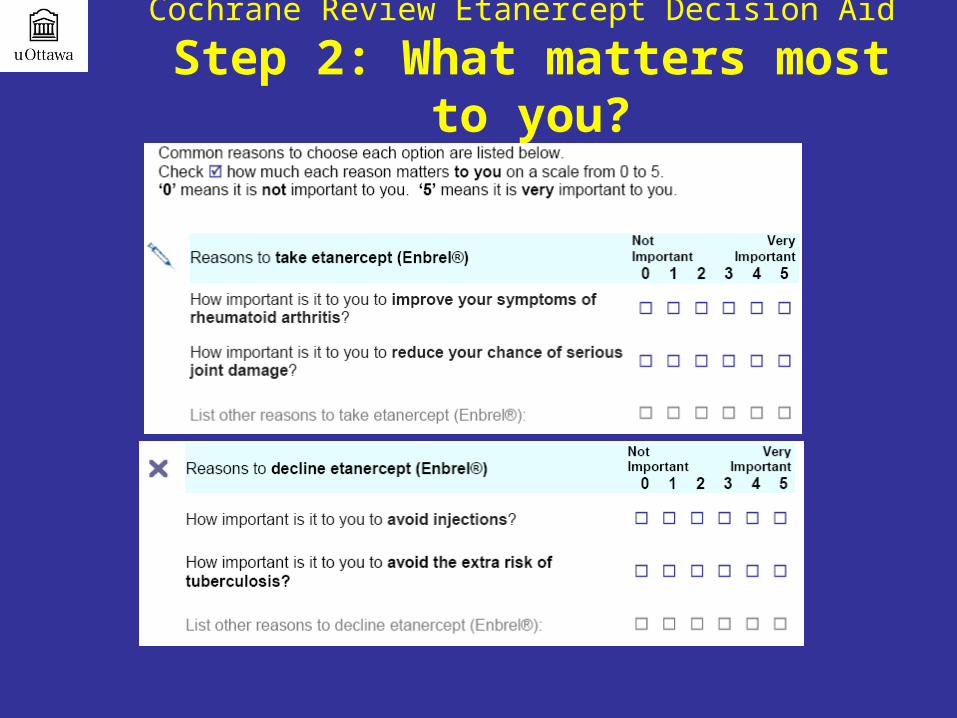
Cochrane Review Etanercept Decision Aid
Step 2: What matters most to you?
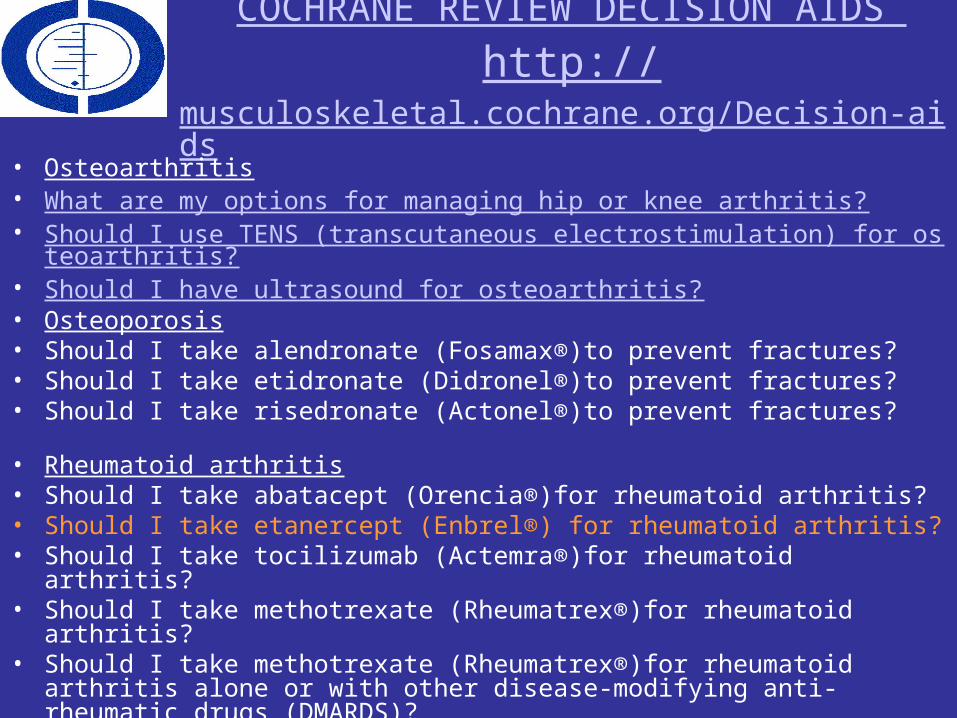
COCHRANE REVIEW DECISION AIDS http://musculoskeletal.cochrane.org/Decision-aids
• Osteoarthritis• What are my options for managing hip or knee arthritis?• Should I use TENS (transcutaneous electrostimulation) for osteoarthritis?• Should I have ultrasound for osteoarthritis?• Osteoporosis• Should I take alendronate (Fosamax®)to prevent fractures?• Should I take etidronate (Didronel®)to prevent fractures?• Should I take risedronate (Actonel®)to prevent fractures?
• Rheumatoid arthritis• Should I take abatacept (Orencia®)for rheumatoid arthritis?• Should I take etanercept (Enbrel®) for rheumatoid arthritis?• Should I take tocilizumab (Actemra®)for rheumatoid arthritis? • Should I take methotrexate (Rheumatrex®)for rheumatoid arthritis?• Should I take methotrexate (Rheumatrex®)for rheumatoid arthritis alone or
with other disease-modifying anti-rheumatic drugs (DMARDS)?
COMPARING MORE THAN ONE OPTION
THE “STEPPED CARE DECISION AID”
45
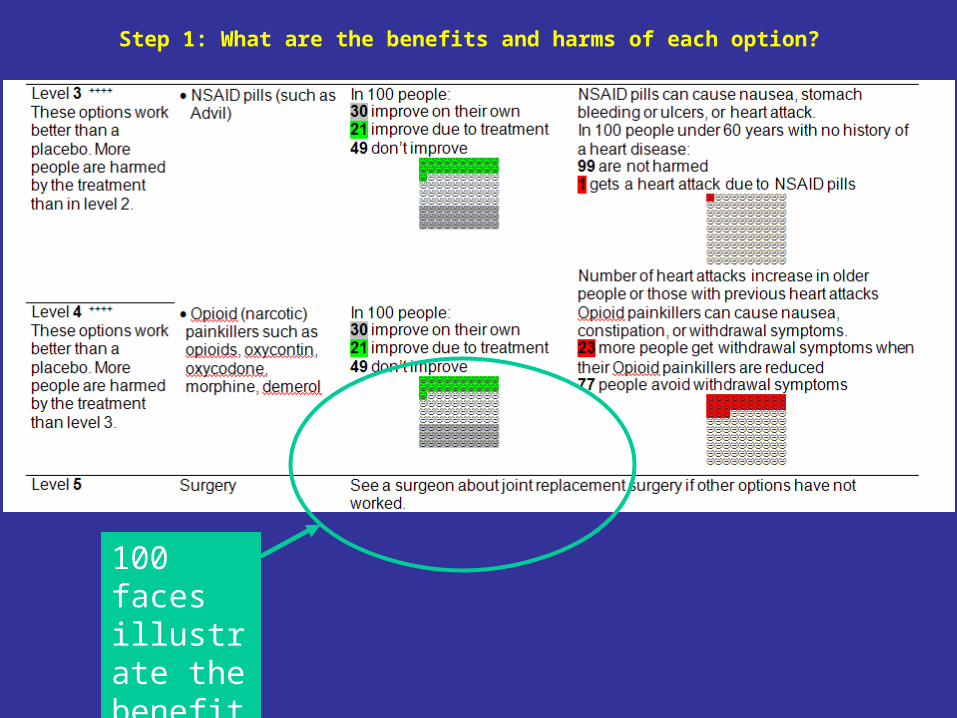
Step 1: What are the benefits and harms of each option?
100 faces illustrate the benefits of the intervention
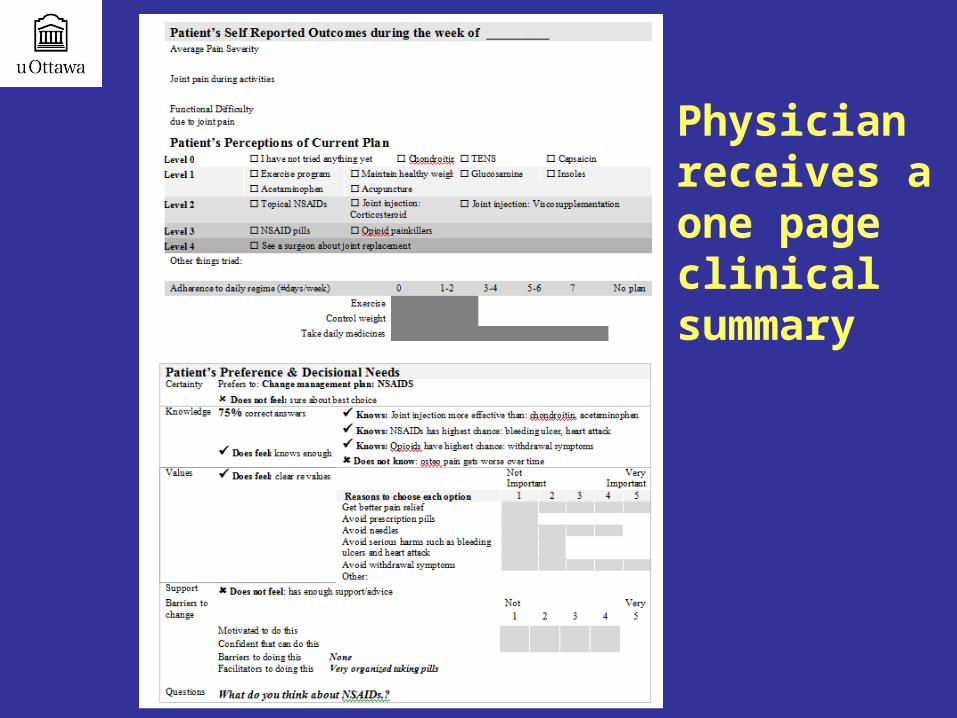
Physician receives a one page clinical summary
Web-Based Decision AidsLinda Li et al
48
The Animated Self-serve WEb-based Research (ANSWER) tool
Linda Li et alTOPICS
• About RA
• Methotrexate
• MTX Side Effects
• MTX and Pregnancy
• MTX and Alcohol
• Weighing the options 51
#4 Clinical scenarios in journals
• Audience: Practitioners
• Time: 15 min
• Adds evidence to the clinical context
#5 Cochrane Summary of Findings Table
• Audience: Practitioners, Policymakers, Press
• Time 5 min
• Provide at-a-glance results of a systematic review, including gaps in the evidence.
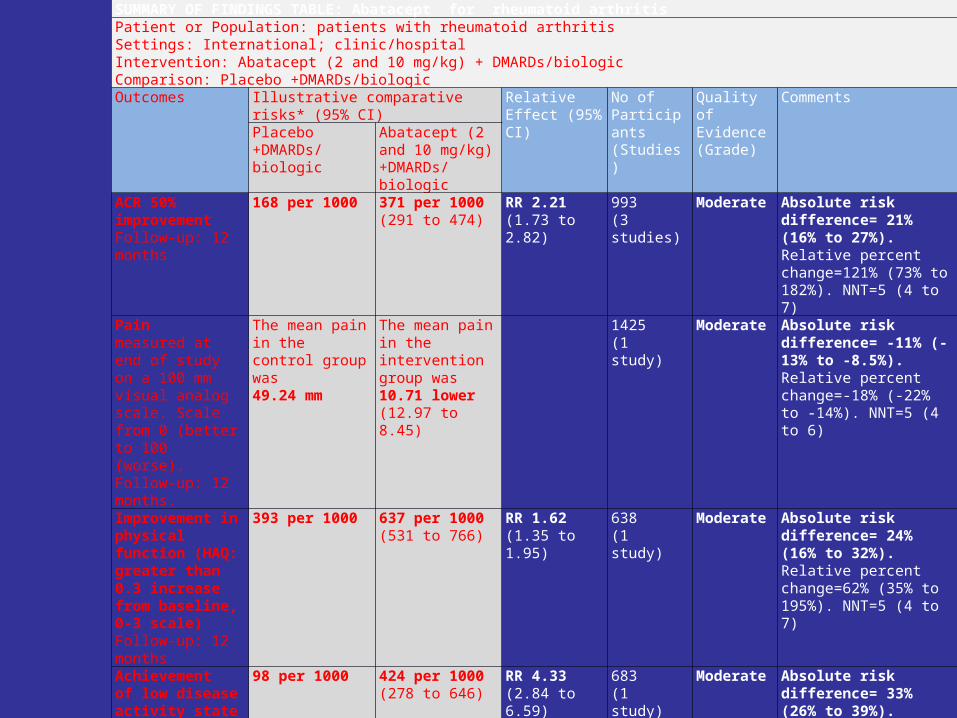
SUMMARY OF FINDINGS TABLE: Abatacept for rheumatoid arthritisPatient or Population: patients with rheumatoid arthritisSettings: International; clinic/hospitalIntervention: Abatacept (2 and 10 mg/kg) + DMARDs/biologicComparison: Placebo +DMARDs/biologicOutcomes Illustrative comparative risks* (95% CI) Relative Effect
(95% CI)No of Participants (Studies)
Quality of Evidence(Grade)
CommentsPlacebo +DMARDs/ biologic
Abatacept (2 and 10 mg/kg) +DMARDs/ biologic
ACR 50% improvementFollow-up: 12 months
168 per 1000 371 per 1000(291 to 474)
RR 2.21(1.73 to 2.82)
993 (3 studies)
Moderate Absolute risk difference= 21% (16% to 27%). Relative percent change=121% (73% to 182%). NNT=5 (4 to 7)
Painmeasured at end of study on a 100 mm visual analog scale. Scale from 0 (better to 100 (worse). Follow-up: 12 months.
The mean pain in the control group was49.24 mm
The mean pain in the intervention group was 10.71 lower(12.97 to 8.45)
1425(1 study)
Moderate Absolute risk difference= -11% (-13% to -8.5%). Relative percent change=-18% (-22% to -14%). NNT=5 (4 to 6)
Improvement in physical function (HAQ: greater than 0.3 increase from baseline, 0-3 scale) Follow-up: 12 months
393 per 1000 637 per 1000(531 to 766)
RR 1.62(1.35 to 1.95)
638(1 study)
Moderate Absolute risk difference= 24% (16% to 32%). Relative percent change=62% (35% to 195%). NNT=5 (4 to 7)
Achievement of low disease activity state (DAS 28 less than 3.2, scale 0-10)Follow-up: 12 months
98 per 1000 424 per 1000(278 to 646)
RR 4.33(2.84 to 6.59)
683(1 study)
Moderate Absolute risk difference= 33% (26% to 39%). Relative percent change=333% (184% to 559%). NNT=4 (3 to 5)
Total serious adverse eventsFollow-up: 6 to 12 months
121 per 1000 127 per 1000(105 to 155)
RR 1.05(0.87 to 1.28)
3151(6 studies)
Moderate Absolute risk difference= 1% (-2% to 3%). Relative percent change=5% (-14% to 29%). NNT=n/a
Long-term serious adverse eventsFollow-up: 2 years
See comment See comment Not estimable 950 (2 studies)
Low Number of patients with SAE: Genovese 2005: 103/357; 23.4 SAE/100 patient-years; 70% completed the LTE. Kremer 2006: 149/593; 16.3 SAE/100 patient-years; 90.5% completed the LTE
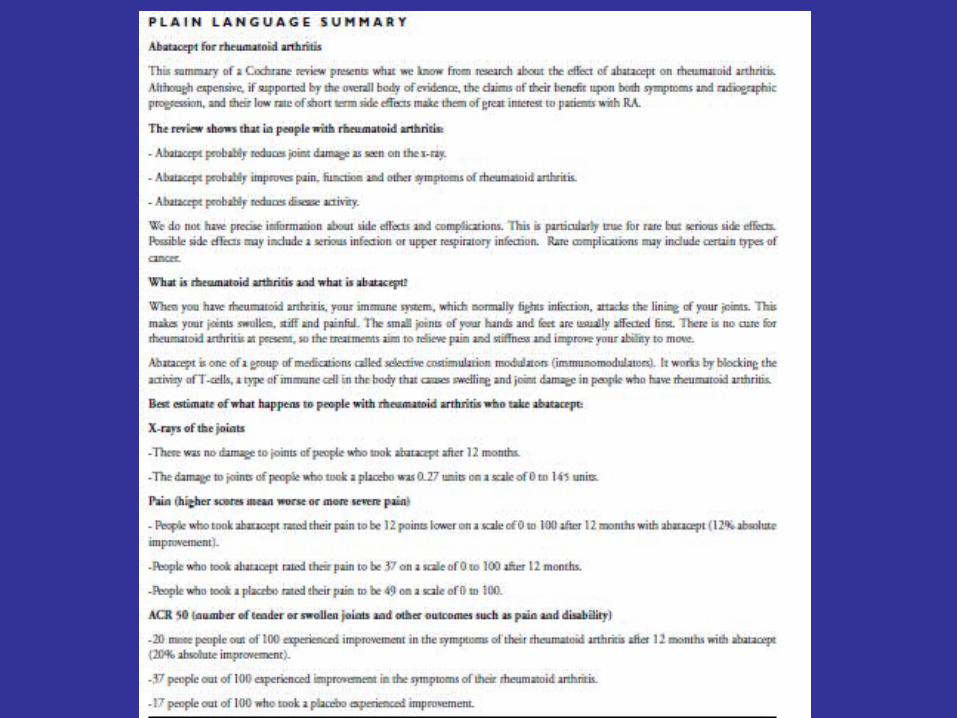
#6 Plain Language Summary
• Audience: Patients, Public, Press
• Time: 5 min
• Provides same information from the Summary of Findings Table in plain language plus background information on the condition and intervention.
#7 Cochrane Podcasts
• Audience: Patients, Public, Press
• Time: 5 min
• Author provides commentary on the results of the review and highlights of the findings.
#8 @cochranelibrary (Twitter)
• Audience: Public, Press
• Time: 1 min
• Headline style news items and announcements

#9 Cochrane Clinical Answers
• Audience: Practitioners
• Time: 15 min
• Uses Cochrane evidence to answer one clinical question at time, providing clinicians with the exact information they need.

#10 Dr. Cochrane
• Audience: Practitioners
• Time: 15 min
• Dr Cochrane is a collection of online continuing professional education and development (CEPD) modules based upon Cochrane Reviews
• Uses a storyline to convey messages
These Dr Cochrane clinical vignettes are based on Cochrane Reviews published in The Cochrane Library. Dr Cochrane is a unique self-learning experience – the integration of Cochrane evidence with a quirky fictional story and multiple-choice questions provides readers with the opportunity to explore and understand the applicability of a Cochrane Review or Overview in a new way.In this series of fictional clinical vignettes, Dr Cochrane travels across time from the past century to the present day, to solve clinical problems using evidence from Cochrane Reviews. Read the review and listen to the podcast of the review and then test your knowledge with five multiple choice questions. You can find the answers at the end.
It was a Saturday evening and Dr Cochrane was enjoying some hors d’oeuvres and a glass of Merlot at a cocktail party hosted by his local golf club. Not long after arriving, he bumped into Ellen and Terry, a couple that he had known for quite some time. Archie quickly caught up on what had been happening in their lives, and Ellen and Terry were particularly excited as their eldest son and his wife were expecting a child. After toasting to the health of their first grandchild, Archie helped himself to more food, but Terry declined.
Holes in one ,not holes in the stomach: Preventing NSAID ulcersLorenzo Moja*Italian Cochrane Centre, Mario Negri Institute for Pharmacological Research, Milan, Italy
10 Cochrane KT Formats
1.Cochrane Reviews2.Cochrane Journal Club3.Cochrane Decision Aids4. Cochrane Corners in Journals5.Cochrane Summary of Findings Tables 6.Cochrane Plain Language Summaries7.Cochrane Podcasts8.Cochrane @ Twitter9.Cochrane Clinical Answers10. Dr Cochrane
Thankyou !
• Don’t Forget!• Come to our party!• 2013 is the 20th
anniversary of the founding of the Cochrane Collaboration
• 21st global Cochrane Colloquium will be in Quebec City September 19th – 23rd 2013