Embed Size (px)
DESCRIPTION
Citation preview
EVIDENCE-BASED CHILD HEALTH: A COCHRANE REVIEW JOURNAL
Evid.-Based Child Health 7:2: 629–717 (2012)
Published online in Wiley InterScience (www.interscience.wiley.com). DOI: 10.1002/ebch.1833
Immunostimulants for preventing respiratory tract infection
in children (Review)
Del-Rio-Navarro BE, Espinosa-Rosales FJ, Flenady V, Sienra-Monge JJL
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2011, Issue 6
http://www.thecochranelibrary.com
Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
T A B L E O F C O N T E N T S
631HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .631ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .632PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .632SUMMARY OF FINDINGS FOR THE MAIN COMPARISON . . . . . . . . . . . . . . . . . . .635BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .637OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .637METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 639Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 640Figure 3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 641Figure 4. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 642
642RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Figure 5. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 646Figure 6. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 647Figure 7. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 648Figure 8. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 648
649DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .651AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .651ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .652REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .661CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .693DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 Any IS compared with placebo, Outcome 1 Mean number of ARTIs. . . . . . . . 695Analysis 1.2. Comparison 1 Any IS compared with placebo, Outcome 2 Percent difference in ARTIs. . . . . . . 697Analysis 2.1. Comparison 2 Bacterial IS compared with placebo, Outcome 1 Mean number of ARTIs. . . . . . 699Analysis 2.2. Comparison 2 Bacterial IS compared with placebo, Outcome 2 Percent difference in ARTIs. . . . . 700Analysis 3.1. Comparison 3 Bacterial IS trials with n equal to or greater than 40 compared with placebo, Outcome 1 Mean
number of ARTIs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 701Analysis 3.2. Comparison 3 Bacterial IS trials with n equal to or greater than 40 compared with placebo, Outcome 2
Percent difference in ARTIs. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 702Analysis 4.1. Comparison 4 Bacterial IS trials with n equal to or greater than 40 only OM-85 and BV D53 compared with
placebo, Outcome 1 Mean number of ARTIs. . . . . . . . . . . . . . . . . . . . . . . . 704Analysis 4.2. Comparison 4 Bacterial IS trials with n equal to or greater than 40 only OM-85 and BV D53 compared with
placebo, Outcome 2 Percent difference in ARTIs. . . . . . . . . . . . . . . . . . . . . . 705Analysis 5.1. Comparison 5 Adverse events, Outcome 1 Gastrointestinal adverse events. . . . . . . . . . . 706Analysis 5.2. Comparison 5 Adverse events, Outcome 2 Skin adverse events. . . . . . . . . . . . . . . 707Analysis 6.1. Comparison 6 OM-85 trials, Outcome 1 Mean number of ARTIs. . . . . . . . . . . . . . 708Analysis 6.2. Comparison 6 OM-85 trials, Outcome 2 Percent difference in ARTIs. . . . . . . . . . . . . 709Analysis 7.1. Comparison 7 D53 trials, Outcome 1 Mean number of ARTIs. . . . . . . . . . . . . . . 710Analysis 7.2. Comparison 7 D53 trials, Outcome 2 Percent difference in ARTIs. . . . . . . . . . . . . . 711
711ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .713APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .716WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .716HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .716CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .716DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .717SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .717INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
630Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
[Intervention Review]
Immunostimulants for preventing respiratory tract infectionin children
Blanca Estela Del-Rio-Navarro1, Francisco J Espinosa-Rosales2, Vicki Flenady3, Juan JL Sienra-Monge1
1Department of Allergy and Immunology, Hospital Infantil de México “Federico Gómez”, Mexico City, Mexico. 2Department ofImmunology, Instituto Nacional de Pediatría (National Institute of Pediatrics), México D.F., Mexico. 3 Translating Research Into Practice(TRIP) Centre - Mater Medical Research Institute, Mater Health Services, Woolloongabba, Australia
Contact address: Blanca Estela Del-Rio-Navarro, Department of Allergy and Immunology, Hospital Infantil de México “Fed-erico Gómez”, Dr. Marquez 162, Colonia de los Doctores, Mexico City, DF, CP 06720, Mexico. [email protected]@yahoo.com.mx.
Editorial group: Cochrane Acute Respiratory Infections Group.Publication status and date: New search for studies and content updated (no change to conclusions), published in Issue 6, 2011.Review content assessed as up-to-date: 3 March 2011.
Citation: Del-Rio-Navarro BE, Espinosa-Rosales FJ, Flenady V, Sienra-Monge JJL. Immunostimulants for preventing res-piratory tract infection in children. Cochrane Database of Systematic Reviews 2006, Issue 4. Art. No.: CD004974. DOI:10.1002/14651858.CD004974.pub2.
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Acute respiratory tract infections (ARTIs) are a major cause of childhood morbidity and mortality. Immunostimulants (IS) may reducethe incidence of ARTIs.
Objectives
To determine the efficacy and safety of IS in preventing ARTIs in children.
Search methods
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) 2011, issue 1, which contains the Acute RespiratoryInfections Group’s Specialised Register, MEDLINE (1966 to February week 4, 2011), EMBASE (1990 to February 2011), GoogleScholar (2009 to February 2011), Scopus (2009 to February 2011), PASCAL (1990 to February 2010), SciSearch (1990 to February2010) and IPA (1990 to February 2010).
Selection criteria
We included all comparative randomized controlled trials (RCTs) which enrolled participants less than 18 years of age. The interventionwas IS medication, administered by any method, compared to placebo to prevent ARTIs.
Data collection and analysis
We analyzed the outcome on ARTIs both as the mean number of ARTIs by group and as a percent change in the rate of ARTIs. Weundertook meta-analyses using a random-effects model and presented results as mean differences (MD) with 95% confidence intervals(CI). Two review authors independently assessed the search results and risk of bias, and extracted data. A funnel plot suggested theremay be publication bias in the identified trials.
631Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Evid.-Based Child Health 7:2: 629–717 (2012)
Main results
Thirty-five placebo-controlled trials (4060 participants) provided data in a form suitable for inclusion in the meta-analyses. Whencompared with placebo, the use of IS was shown to reduce ARTIs measured as the total numbers of ARTIs (MD -1.24; 95% CI -1.54to -0.94) and the difference in ARTI rates (MD -38.84%; 95% CI -46.37% to -31.31%). Trial quality was generally poor and a highlevel of statistical heterogeneity was evident. The subgroup analysis of bacterial IS, D53 and OM-85 studies produced similar results,with lower heterogeneity. No difference in adverse events was evident between the placebo and IS groups.
Authors’ conclusions
This review shows that IS reduce the incidence of ARTIs by 40% on average in susceptible children. Studies in healthy children are notavailable. Although the safety profile in the studies was good, some IS may be unsafe. ARTI-susceptible children may benefit from IStreatment. Further high-quality trials are needed and we encourage national health authorities to conduct large, multicentre, double-blind, placebo-controlled RCTs on the role of IS in preventing ARTIs in children.
P L A I N L A N G U A G E S U M M A R Y
Immunostimulants to prevent acute respiratory tract infections in children
Acute respiratory tract infections (ARTIs) are responsible for 19% of all deaths in children younger than five years of age, mainly in low-income countries in Africa, Asia and Latin America. In high-income countries ARTIs are among the most frequent illnesses, leadingto 20% of medical consultations, 30% of days lost from work and 75% of antibiotic prescriptions. In the USA the total cost of non-influenza-related viral ARTIs is around $40 billion annually, while the corresponding cost for influenza is US $87.1 billion. The mainsigns and symptoms of ARTIs include sneezing, runny nose, sore throat, cough and malaise. Children living in rural communities, notattending daycare centres, suffer about seven ARTI episodes in the first year of life; eight ARTIs per year from the ages of one to four;six per year aged five to nine; and five per year aged 10 to 19. Children exposed to risks factors, such as attendance at daycare centres,overcrowding, contact with older siblings, smoking at home and lack of breast feeding, may suffer more ARTIs.
Several treatments have been used to reduce the incidence of ARTIs (vitamin A, vitamin C, zinc, antibiotics). Among them areimmunostimulants (herbal extracts, bacterial extracts, synthetic compounds), which aim to increase the immune defences of therespiratory tract. We searched for clinical trials of immunostimulants to prevent ARTIs in children compared to placebo. Our reviewincludes 35 studies with 4060 participants. However, the quality of many of the studies was poor and the results were very diverse.
By combining results, immunostimulants reduced 1.24 ARTIs in a six-month period, equivalent to a 39% reduction in ARTIs comparedto the placebo group. Only 20 studies provided adequate data on adverse events: the most frequent were rash, nausea, vomiting,abdominal pain and diarrhea. The main limitations of this review were the poor methodological quality and diverse trial results.We conclude that ARTI-susceptible children may benefit from immunostimulants, but more high-quality studies are needed. Wesuggest that national health authorities conduct high-quality randomized controlled trials to assess the true effects of immunostimulantpreparations.
632Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-BasedChild
Health
7:2
:629–717
(2012)
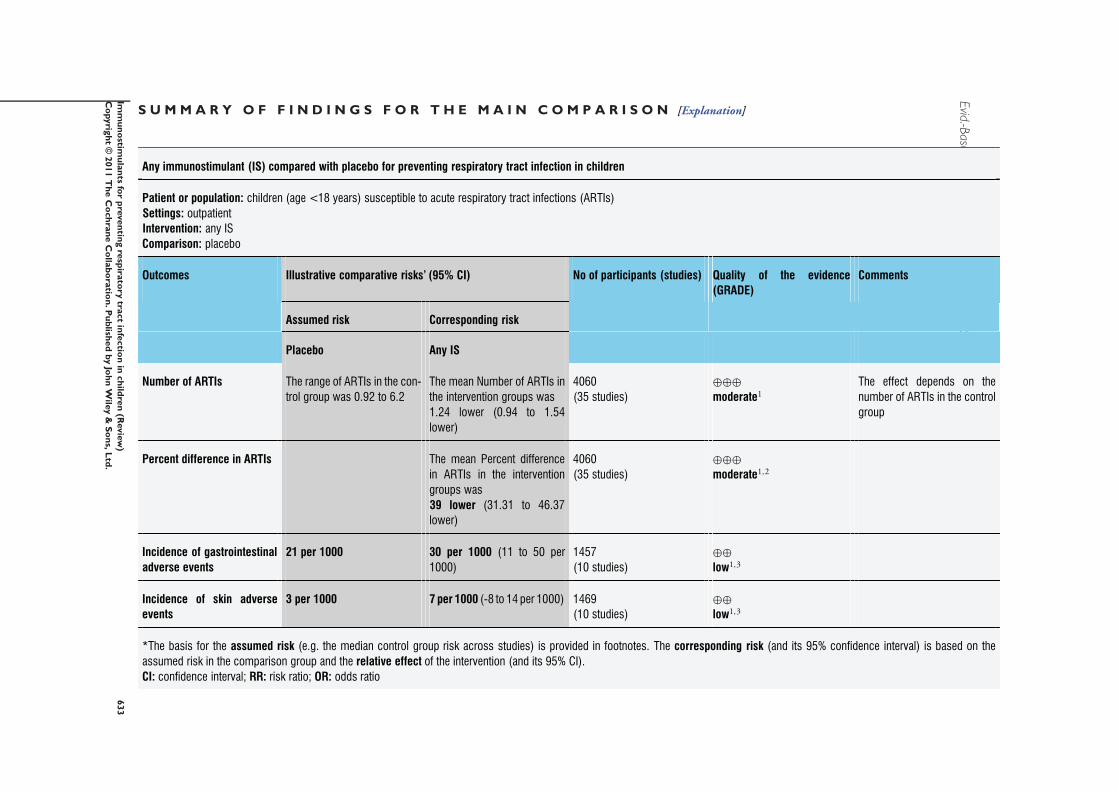
S U M M A R Y O F F I N D I N G S F O R T H E M A I N C O M P A R I S O N [Explanation]
Any immunostimulant (IS) compared with placebo for preventing respiratory tract infection in children
Patient or population: children (age <18 years) susceptible to acute respiratory tract infections (ARTIs)
Settings: outpatient
Intervention: any IS
Comparison: placebo
Outcomes Illustrative comparative risks’ (95% CI) No of participants (studies) Quality of the evidence
(GRADE)
Comments
Assumed risk Corresponding risk
Placebo Any IS
Number of ARTIs The range of ARTIs in the con-
trol group was 0.92 to 6.2
The mean Number of ARTIs in
the intervention groups was
1.24 lower (0.94 to 1.54
lower)
4060
(35 studies)
⊕⊕⊕
moderate1The effect depends on the
number of ARTIs in the control
group
Percent difference in ARTIs The mean Percent difference
in ARTIs in the intervention
groups was
39 lower (31.31 to 46.37
lower)
4060
(35 studies)
⊕⊕⊕
moderate1,2
Incidence of gastrointestinal
adverse events
21 per 1000 30 per 1000 (11 to 50 per
1000)
1457
(10 studies)
⊕⊕
low1,3
Incidence of skin adverse
events
3 per 1000 7 per 1000 (-8 to 14 per 1000) 1469
(10 studies)
⊕⊕
low1,3
*The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the
assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI).
CI: confidence interval; RR: risk ratio; OR: odds ratio
633
Imm
un
ostim
ula
nts
for
pre
ven
ting
resp
irato
rytra
ct
infe
ctio
nin
ch
ildre
n(R
evie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.

Evid.-BasedChild
Health
7:2
:629–717
(2012)
GRADE Working Group grades of evidence
High quality: further research is very unlikely to change our confidence in the estimate of effect.
Moderate quality: further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Low quality: further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
Very low quality: we are very uncertain about the estimate.
1Funnel plot shows possible publication bias, risk of bias in the studies moderate, and high heterogeneity among studies. A group of six studies with good quality point to the benefit of IS2 Heterogenity decreased with calculation of percent difference ARTIs.3 Adverse events were reported only in 10 trials; selective outcome reporting
xxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxxx
634
Imm
un
ostim
ula
nts
for
pre
ven
ting
resp
irato
rytra
ct
infe
ctio
nin
ch
ildre
n(R
evie
w)
Co
pyrig
ht
©2011
Th
eC
och
ran
eC
olla
bo
ratio
n.P
ub
lished
by
Joh
nW
iley
&S
on
s,L
td.
Evid.-Based Child Health 7:2: 629–717 (2012)B A C K G R O U N D
Description of the condition
In 1998 the World Health Organization (WHO) considered acuterespiratory tract infections (ARTIs) to be “the forgotten pandemic”as ARTIs caused 19% of all deaths in children younger than fiveyears and 8.2% of all disabilities and premature mortality (WHO1998). In 2000, 1.9 million (95% confidence interval (CI) 1.6 to2.2 million) children died from ARTIs worldwide, with 70% ofthe deaths in Africa and South-East Asia (Williams 2002). AR-TIs are the leading cause of morbidity in high-income countries(USA, Canada, Western Europe) and account for 20% of medicalconsultations, 30% of days lost from work and 75% of antibi-otic prescriptions (WHO 1998). ARTIs are responsible for mostsick days amongst school children (Haskins 1986) and parentalabsenteeism from work (Bell 1989). The cost of ARTIs in high-income countries is significant. For example, between 2000 and2002 there were approximately 500 million non-influenza-relatedviral ARTI episodes in the USA per year; the total economic im-pact of these episodes was around $40 billion annually (direct costsof $17 billion per year and indirect costs of $22.5 billion per year)(Fendrick 2003). Based on the 2003 US population, it has beencalculated that the total economic burden of annual influenza epi-demics in the USA was $87.1 billion US dollars ($47.2 to $149.5)(Molinari 2007). Risk factors for ARTIs in childhood include at-tendance at daycare centres (Schwartz 1994), overcrowding (Bell1989; Selwyn 1990), contact with elder siblings (Selwyn 1990),male gender (Monto 2002), smoking at home (Jin 1993) and lackof breast feeding (Wright 1989).Community health studies in high-income countries have pro-vided basic information on the incidence of ARTIs in children.In the Cleveland Family Study, 100 families were visited weeklyby nurses during 1948 to 1957. The annual frequency of respi-ratory illness was 6.72 in children less than one year old; 7.95 inchildren aged one to four years; 6.21 in children aged five to nineyears; 5.02 in children aged 10 to 14 years; and 4.71 in 15 to 19-year olds (Monto 2002). In the first phase of the Tecumseh study,from 1965 to 1971, 4905 residents registered their incidence ofARTIs for the six-year period. In the first report the residents hadsuffered approximately 14,600 ARTIs. The annual incidence ofARTIs per person was 6.1 in children less than one year old; 5.7 inchildren aged one to two years; 4.7 in children aged three to fouryears; 3.5 in children aged five to nine years; 2.7 in children aged10 to 14 years old; and 2.4 in 15 to 19-year olds (Monto 1974).In the second report of the Tecumseh study, which covered twophases comprising a total of 11 years (1965 to 1971 and 1976 to1981), the mean annual number of ARTIs was 4.9 in the groupaged from zero to four years; and 2.8 in the group aged five to 19years (Monto 1993). In both phases of the study viruses were themost common agents causing ARTIs.During the 1980s, the Board on Science and Technology for In-ternational Development (BOSTID) undertook a co-ordinated
effort to establish the aetiology and epidemiology of ARTIs inchildren in high-income countries. The project was carried outin populations from 0 to 59 months of age in Africa, Asia andLatin America. The incidence rate in six community-based stud-ies ranged from 12.7 to 16.8 ARTIs per 100 child-weeks and theincidence of lower ARTIs was from 0.2 to 0.4 per 100 child-weeks. The children studied spent from 21.7% to 40.1% of theobserved weeks with ARTIs and from 1% to 14.4% of the ob-served weeks with lower ARTIs. Viral agents were more frequentlyrecovered than bacterial agents; respiratory syncytial virus (RSV)was the most frequent virus (Selwyn 1990). In Mexico, a studyassessing the effect of daycare centres on ARTI incidence followed144 children (aged 43 days to 4 months at entry) at home for oneyear. The study found that these children had six ARTIs each year,with a median of 40 sick days in a year (Flores-Hernandez1999).Viruses were the main aetiological agents for ARTIs in childrenat daycare centres (Denny 1986) and in the community (Monto1993). The most common virus isolates are rhinovirus, respiratorysyncytial virus, parainfluenza virus and adenovirus. Lower ARTIsare also frequently associated with viral infections, but bacterialagents may be found in 4.5% to 40% of the cases (Selwyn 1990).Up to 50% of children admitted to hospital with proven bacte-rial ARTIs also have evidence of concurrent or recent viral ARTIs(Campbell 1995). The damage caused by viruses to epithelial cellsin the airways may increase the adherence of bacteria and lead toa bacterial superinfection (Hament 1999).History of respiratory infections in the first 12 years among chil-dren was established in a cohort of German children living in ur-ban areas. The mean cumulative number of ARTIs in the 12 yearswas 21.9 (standard deviation (SD) 9.0) episodes; the mean annualnumber was 1st year, 3.1 (2.1) episodes; 2nd year, 3.2 (2.5); 3rdyear, 2.1 (2.0); 4th year, 2.3 (2.1); 5th year, 1.8 (1.6); 7th throughto the 9th year, 1.1 (1.0) episodes; 10th year through 12th year,1.0 (0.9) episodes (Grüber 2008). The frequency of ARTIs in thisstudy was about a half of the classic Monto studies (Monto 1974;Monto 1993). The authors regarded incidence above the twofoldstandard deviation as clinically relevant; more than seven episodesin the 1st year of life, more than eight episodes in year two, morethan six episodes in year three and year four more than five episodesin year five, more than four episodes in year six, and more thanthree episodes from year seven onwards.In a healthy population without any special risk factors or immun-odeficiencies, there is a subgroup of people with a higher incidenceof ARTIs. A cohort of children from Nijmegen, Netherlands wasfollowed for 21 years to register the occurrence of ARTIs. Thenumber of respiratory infections was assessed at the ages of two,four, eight and 21. It was considered that a person had a recurrentinfection if the number of ARTIs was above 75th percentile of thedistribution of respiratory infection at each assessment. Twenty-three percent of the people had recurrent respiratory infection intwo or more assessments and 1% suffered from recurrent infectionin the four assessments (Rovers 2006).
635Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
Recent influenza epidemics have increased interest in effective un-specific measures to protect the global population, outside the pro-duction of appropriate vaccines which could take more than sixto nine months to be ready for use. These unspecific measures in-clude physical methods to reduce the spread of respiratory virusessuch as hand washing, wearing masks, gloves and gowns (Jefferson2009). In military populations, reported additional measures toprevent respiratory tract infections include reducing contact be-tween units, reducing crowding, installing cloth barriers betweenbeds, indoor air dilution and ventilation, dust suppression andair sterilisation (Lee 2005). Other measures include vitamin andmineral supplementation, such as vitamin A (Chen 2008a), vita-min C (Hemilä 2010), vitamin D (Yamshchikov 2009) and zinc(Aggarwal 2007). Interventions which stimulate the immune sys-tem (immunostimulants) have been proposed as effective measuresto reduce ARTIs.Some years ago, the idea that bacterial lysates, plant extracts orimidazole compounds, could induce unspecific immunity againstviruses and distinct bacteria was not very solid. However, the re-cent discovery of Toll-like-receptors (TLRs) supports the possiblemechanism of action of immunostimulants (Krieg 2003). TLRswere discovered in the 1990s and their importance on immunitywas found later, see How the intervention might work below. Infact, there is evidence that two bacterial lysates may act on TLR2(Alyanakian 2006; Nikolova 2009), as well as levamisole (Chen2008b).
Description of the intervention
The main way to prevent ARTI complications is to prevent theseinfections and administer early antibiotic treatment when bac-terial ARTIs are diagnosed (Heikkinen 1999; Henderson 1982;WHO 1998). Non-specific preventative measures for ARTIs stud-ied in clinical trials include general hygiene methods in childrenattending daycare centres (CDCIDSG 1984); the administrationof nutritional supplements such as vitamin A to malnourishedchildren (Barreto 1994), vitamin C to normal and malnourishedchildren (Hemila 1997; Jefferson 2001) and trace elements tomalnourished and susceptible children (Sazawal 1998); preven-tive antibiotics (Dajani 1995); administration of gamma glob-ulins (Nydahl-Persson 1995); nasal spray of immunoglobulins(Heikkinen 1998); herbal extracts (Grimm 1999); xylitol sugarsyrup or chewing gum (Uhari 1998); and the use of immunos-timulants (IS) from different sources. The sources are synthetic(Passali 1994a); thymic extracts or factors (De Mattia 1993); or ofbiological origin such as Klebsiella extracts containing lipopolysac-charide (Dahan 1986) and mixtures of bacterial extracts (Berber1996).
How the intervention might work
The actual mechanism of IS is not yet fully understood. Currentlythe mechanisms of action are known for only two synthetic IS,tucaresol and imiquimod. The mechanism of tucaresol is to form acomplex on the surface of T cells (a Schiff reaction with the amines,probably on CD2). This complex provides an additional stimu-lant which facilitates the activation of the T cells (a co-stimula-tory signal activating the MAPK ERK2 pathway) (Rhodes 1995).Imiquimod and other related molecules activate the immune cellsby binding to the receptor for the bacterial products that activatethe unspecific defence mechanism and promote the immune re-sponse; they bind to the Toll-like receptor 7 (TLR7) activating theMyD88-dependent signalling pathway (Hemmi 2002).It may be postulated that products with IS properties activate theimmune cells using the receptors that recognise common bacte-rial products or receptors that provide additional stimulation foractivation. For instance, Toll-like receptors (TLR) recognise com-ponents common to a range of bacteria, so-called pathogen-as-sociated molecular patterns (PAMPs) such as lipopolysaccharide,peptidoglycan, lipoteichoic acid, lipoarabinomannan, un-methy-lated DNA with CpG motif and bacterial lipoproteins which ac-tivate the innate immune responses. The innate immune responseis responsible for the early mechanisms of defence against infec-tion; for instance the phagocytosis and neutralisation of bacte-ria entering the body. The mechanisms that enhance the innateimmune responses (cytokines and chemokines) also stimulate theadaptive immune response (production of specific antibodies andreproduction of specific T cells) (Hoffmann 1999; Schnare 2001;Takeuchi 2001). In fact, there is evidence that two bacterial lysatesmay act on TLR2 (Alyanakian 2006; Nikolova 2009), as well aslevamisole (Chen 2008b).
Why it is important to do this review
Most ARTIs are caused by viruses, hundreds of which may causethis type of infection. It would be impractical, therefore, to havea vaccine for each possible pathogenic agent. Therefore, spe-cific immunisation may not be the ultimate solution to preventARTIs. The introduction of the pneumococcal conjugate vac-cine decreased carriage and invasive infections due to the vaccineserotypes, but it has been replaced by other non-vaccine serotypesthat are becoming antibiotic resistance (Hsu 2009; Huang 2009;Mera 2009).IS could provide an alternative to vaccines for preventing AR-TIs but the efficacy of these medications is controversial (Collet1992; Valleron 1992). Several bacterial extracts and synthetic com-pounds are used in Europe and the Americas to prevent ARTIs.However, the evidence of the safety and efficacy of this approachis unclear. A systematic review of immunostimulation for the pre-vention of ARTIs in children is required to enable a robust ap-praisal of the current evidence on the safety and efficacy of thisapproach and to provide clues for the development of new IS.
636Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Evid.-Based Child Health 7:2: 629–717 (2012)
O B J E C T I V E S
To assess the safety and efficacy of immunostimulants (IS) admin-istered to children to prevent ARTIs when compared with placebo,in terms of frequency of these infections and reported adverse ef-fects. Trials comparing two IS were also included.
M E T H O D S
Criteria for considering studies for this review
Types of studies
Randomised controlled trials (RCTs) comparing IS, administeredby any method, to placebo to prevent ARTIs. Trials referring tointerferon inducers, vitamins and nutritional supplements werenot included.
Types of participants
Participants younger than 18 years of age. We did not include trialsthat included participants who suffered from asthma, allergy andatopy, or chronic respiratory diseases.
Types of interventions
The use of an IS administered by any method to prevent ARTIs.Administration of IS could begin in the presence of active ARTI.We considered trials utilising concomitant therapies such as an-tipyretics or antibiotics for inclusion.
Types of outcome measures
A broad definition of ARTI was accepted and included using differ-ent specific diagnoses, such as cold, influenza, tonsillitis, pharyngi-tis, bronchitis and otitis media. Aetiological agents were not stud-ied and no distinction was made between bacterial and viral AR-TIs. Physician diagnosis of ARTI and adverse events was accepted.
Primary outcomes
The number of ARTIs in children suffered during the study period.
Secondary outcomes
1. The percentage of ARTIs.2. The incidence of adverse events.
Search methods for identification of studies
Electronic searches
For this update we searched the Cochrane Central Register of Con-trolled Trials (CENTRAL) 2011, issue 1, which contains the AcuteRespiratory Infections Group’s Specialised Register, MEDLINE(1966 to February week 4, 2011), EMBASE (1990 to February2011), Google Scholar (2009 to February 2011), Scopus (2009to February 2011), PASCAL (1990 to February 2010), SciSearch(1990 to February 2010) and IPA (1990 to February 2010). De-tails of the previous searches are in Appendix 1.We used the following search strategy to search MEDLINE andCENTRAL. To search MEDLINE, we combined the search strat-egy with the Cochrane Highly Sensitive Search Strategy for identi-fying randomized trials in MEDLINE: sensitivity- and precision-maximising version (2008 revision); Ovid format (Lefebvre 2009).The search strategy was adapted for EMBASE (see Appendix 2).Details of the PASCAL, SciSearch, IPA and previous Embasesearch are in Appendix 3.MEDLINE (Ovid)
1 exp Respiratory Tract Infections/2 (respiratory adj5 infection*).tw.3 1 or 24 exp Adjuvants, Immunologic/5 immunostimulant*.tw,nm.6 immunomodulat*.tw,nm.7 immunoadjuvant*.tw,nm.8 immunologic adjuvant*.tw,nm.9 (immunobalt or lw50020 or luivac or paspat or munos-tin).tw,nm.10 (om-85 bv or om85bv or om 85 bv).tw,nm.11 (bronchovaxom or broncho-vaxom or broncho vaxom).tw,nm.12 (pulmonar-om or pulmonar om).tw,nm.13 d53.tw,nm.14 (ribomunyl or ribovac or immucytal).tw,nm.15 Lipopolysaccharides/16 lipopolysaccharide*.tw,nm.17 (ru41740 or ru-41740 or ru 41740 or biostim).tw,nm.18 Thymus Extracts/19 thymus extract*.tw,nm.20 (thymic extract* or thymomodulin*).tw,nm.21 Pelargonium/22 (pelargonium* or umckaloabo).tw,nm.23 (am3 or imunoferon or immunoferon or inmunoferon).tw,nm.24 glycophosphopep*.tw,nm.25 (pidotimod or adimod).tw,nm.26 Levamisole/27 levamisole.tw,nm.28 or/4-2729 3 and 28
637Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
Searching other resources
We used identified articles as references for a Science CitationIndex search. We searched bibliographies of all included trials aswell as those of relevant reviews to identify additional studies.Finally, we sent a letter to all first authors, as well as pharma-ceutical companies that manufacture immunostimulant drugs, re-questing data and references for any relevant published and un-published trials. There were no language or publication restric-tions. We also searched for studies in the trial registration website: metaRegister of Controlled Trials (http://www.controlled-trials.com/mrct/). We searched for IS trial registries in the U.S.National Institutes of Health in http://www.ClinicalTrials.gov.
Data collection and analysis
Selection of studies
Two review authors (BN, JSM) independently searched for trialsfor inclusion and risk of bias assessment. We resolved differencesby discussion.
Data extraction and management
We analyzed and managed data using Review Manager (RevMan2008). Two authors (BN, JSM) independently extracted data. Wesought missing data from investigators of individual trials, as nec-essary, in order to perform analyses on an intention-to-treat (ITT)basis.Dr Arturo Berber contacted trial authors to request unpublisheddata. Responses were received from 10 trial authors (Arroyave1999; Collet 1993; Gómez-Barreto 1998; Gutiérrez-Tarango2001; Jara-Pérez 2000; Karam-Bechara 1995; Paupe 1991;
Saracho-Weber 2001 (co-worker Vázquez-Ramos); Schaad 1986;Schaad 2002). However, no additional data were provided. A fur-ther 11 trial authors were contacted by Dr Berber without response(Aymard 1994; Careddu 1994a; Careddu 1994b; Fiocchi 1986;Fiocchi 1988; Fiocchi 1989; Fiocchi 1990; Motta 1994; Paupe1986; Rutishauser 1998 (co-worker Grevers); Valleron 1992). Dr.Arturo Berber provided the database for OM-85 trials from Mex-ico. In 2010, we made attempts to contact the following au-thors: Joseph Bellanti, Jean Bousquet, Herman A. Cohen, CraigI Coleman, Jean Paul Collet, Alessandro Fiocchi, Sergio Mar-cassa, Renzo Mora, RJ Riedl-Seifert, Urs B. Schaad, DragankaStankulova, Claudia Steurer-Stey and James A. Taylor, and manu-facturers Luipold (luivac), OM Pharma (broncho-vaxom), PierreFabre (ribomunyl) and Polichem (adimod). Only Sergio Marcassa,Renzo Mora, RJ Riedl-Seifert, Urs B. Schaad (by himself and inname of OM Pharma) replied; no information regarding new stud-ies was obtained.
Assessment of risk of bias in included studies
We measured trial quality using seven domains.1. Random sequence generation (selection bias).2. Allocation concealment (selection bias).3. Blinding (performance bias and detection bias).4. Blinding of participants and personnel (performance bias).5. Blinding of outcome assessment (detection bias).6. Incomplete outcome data (attrition bias).7. Selective reporting (reporting bias).
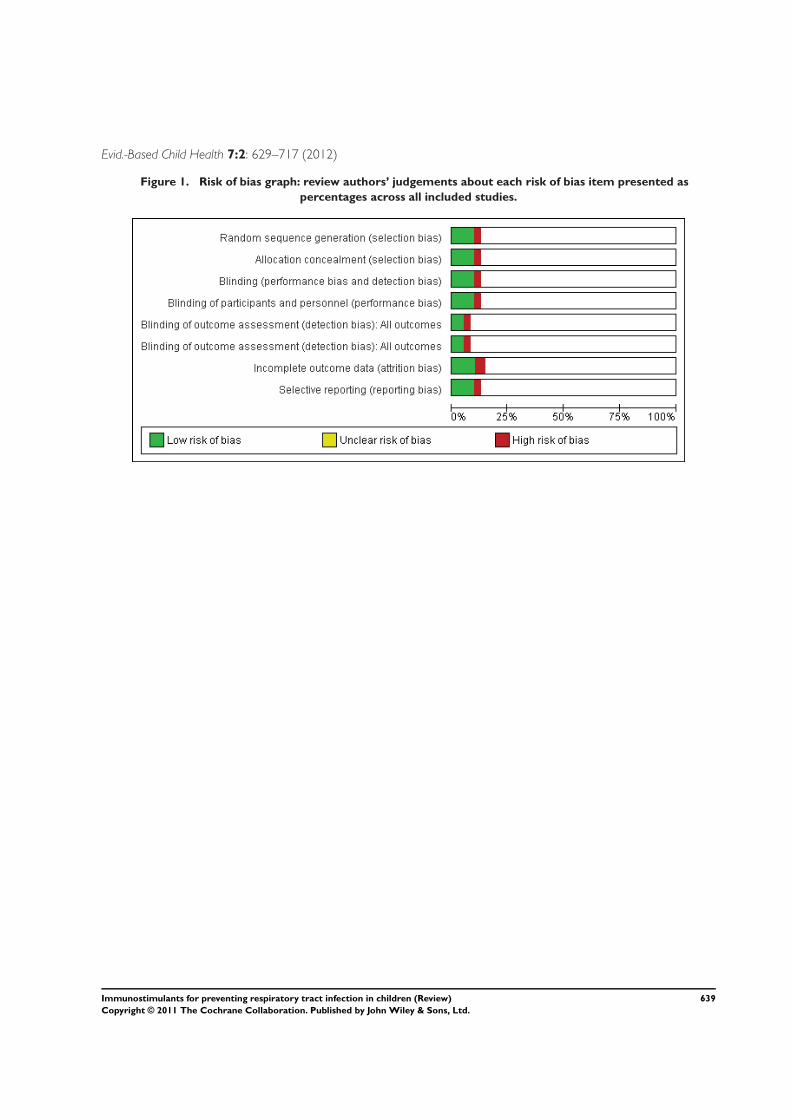
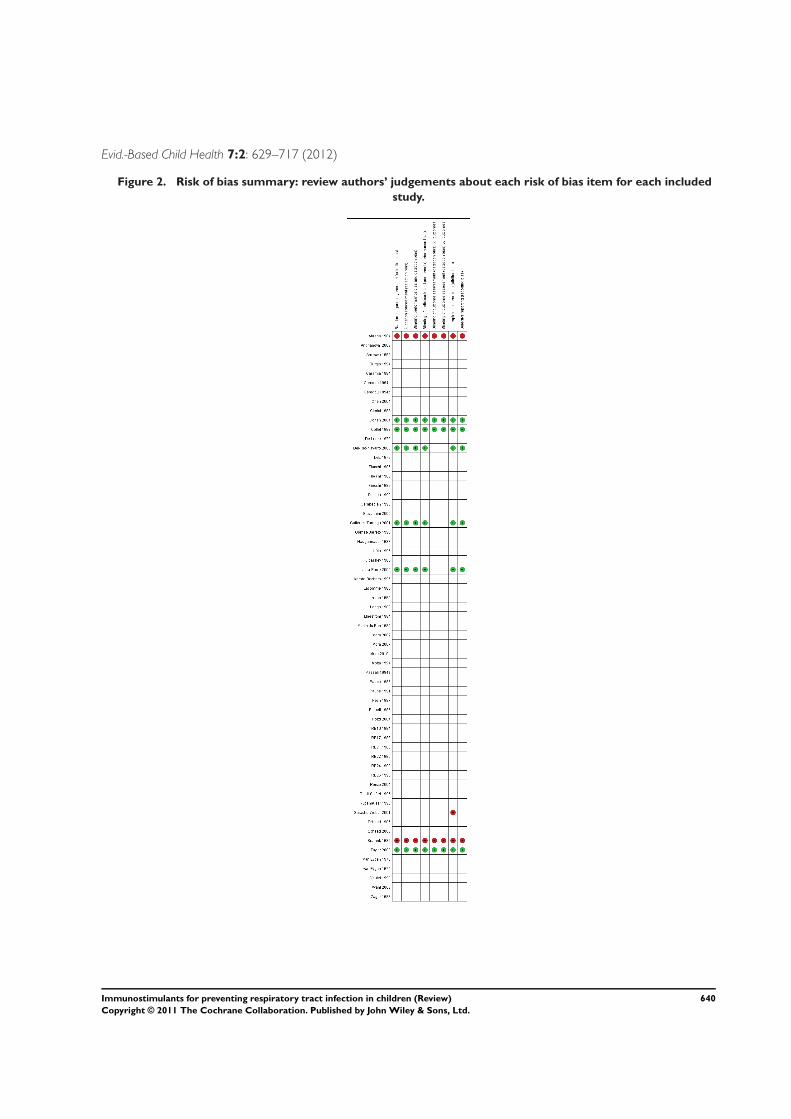
We assigned a quality rating for above domains for each includedtrial using the criteria outlined in the Cochrane Handbook for Sys-tematic Reviews of Interventions (Higgins 2011) as high risk, lowrisk or uncertain risk . Figure 1 and Figure 2 shows the results ofrisk of bias assessment for the seven domains.
638Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
Figure 1. Risk of bias graph: review authors’ judgements about each risk of bias item presented as
percentages across all included studies.
639Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
Figure 2. Risk of bias summary: review authors’ judgements about each risk of bias item for each included
study.
640Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
Measures of treatment effect
We reported the mean differences (MD) (and 95% confidenceintervals (CI)) for the meta-analysis of data measured on a contin-uous scale. We assessed heterogeneity by visual inspection of theoutcomes tables and by using two statistics of heterogeneity (Hand I2 statistic) (Higgins 2003). Due to the observed statisticalheterogeneity, we used the random-effects model.
Unit of analysis issues
Regarding the trials with a description of randomisation and al-location, the unit of randomisation was the individual subject(Cohen 2004; Collet 1993; Del-Rio-Navarro 2003; Gutiérrez-Tarango 2001; Jara-Perez 2000; Taylor 2003).
Dealing with missing data
The studies only analyse the available data, ignoring the missingdata.
Assessment of heterogeneity
The way in which the outcomes were reported varied widely acrossthe trials. We decided to use the mean number of ARTIs and itsstandard deviation (SD) as the outcome as it allows the use of para-metric statistical methods that provide more power to the tests. Weassumed that the number of ARTIs in the IS-treated group wouldbe comparable to the number of ARTIs in the placebo group; andboth of these would depend on the susceptibility of the children(determined by age, duration of trial and seasons of the year dur-ing the trial). Consequently we expected to have heterogeneity inthe mean number of ARTIs. Therefore, we decided to standardisethe results using the percentage of infections considering the meannumber of infections in the placebo group as 100%.
Assessment of reporting biases
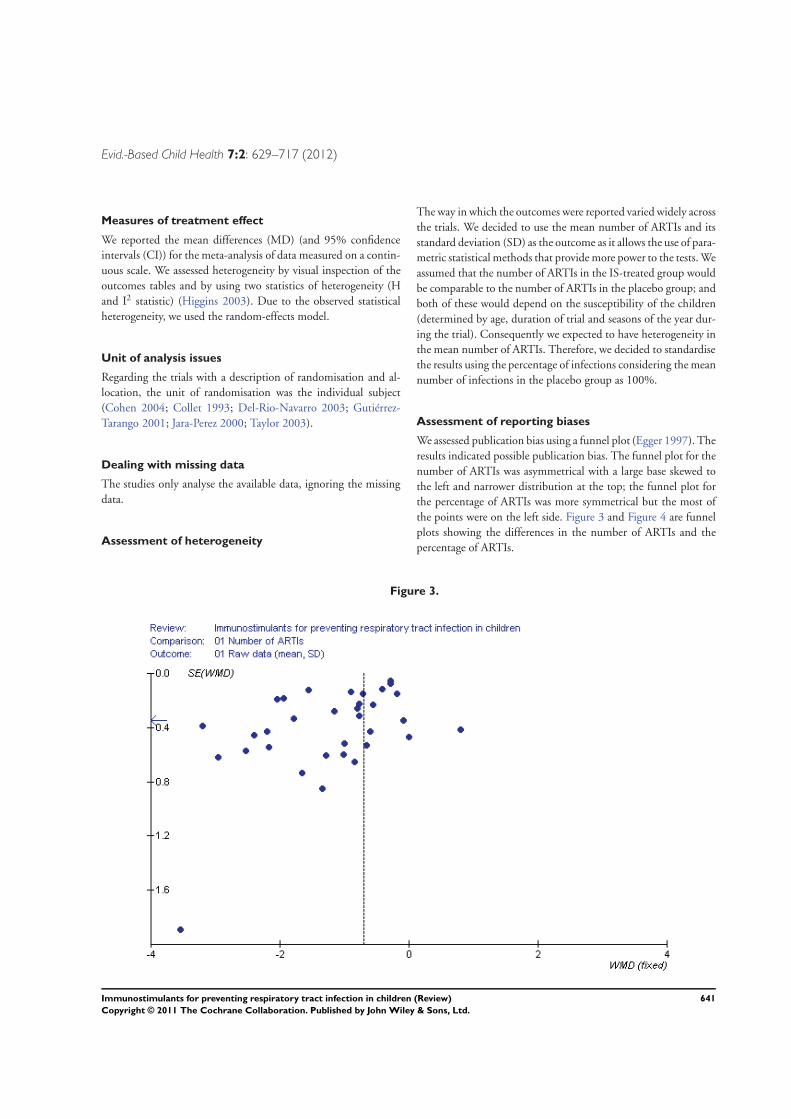
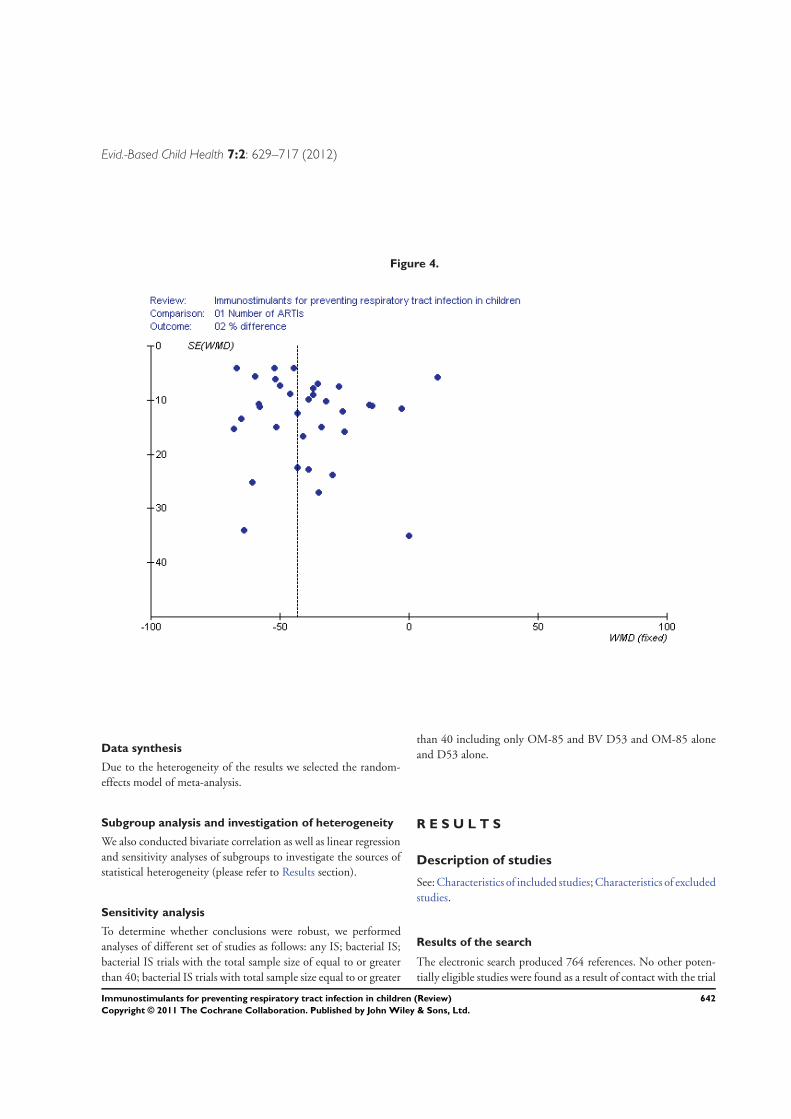
We assessed publication bias using a funnel plot (Egger 1997). Theresults indicated possible publication bias. The funnel plot for thenumber of ARTIs was asymmetrical with a large base skewed tothe left and narrower distribution at the top; the funnel plot forthe percentage of ARTIs was more symmetrical but the most ofthe points were on the left side. Figure 3 and Figure 4 are funnelplots showing the differences in the number of ARTIs and thepercentage of ARTIs.
Figure 3.
641Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
Figure 4.
Data synthesis
Due to the heterogeneity of the results we selected the random-effects model of meta-analysis.
Subgroup analysis and investigation of heterogeneity
We also conducted bivariate correlation as well as linear regressionand sensitivity analyses of subgroups to investigate the sources ofstatistical heterogeneity (please refer to Results section).
Sensitivity analysis
To determine whether conclusions were robust, we performedanalyses of different set of studies as follows: any IS; bacterial IS;bacterial IS trials with the total sample size of equal to or greaterthan 40; bacterial IS trials with total sample size equal to or greater
than 40 including only OM-85 and BV D53 and OM-85 aloneand D53 alone.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excludedstudies.
Results of the search
The electronic search produced 764 references. No other poten-tially eligible studies were found as a result of contact with the trial
642Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
authors or searching of trial registries. Of the references obtained,we identified 93 studies as potentially eligible.
Included studies
We included 61 placebo-controlled clinical trials involving 4149participants. The studies were very heterogenous in the interven-tions studied, the number of ARTIs in the placebo groups and inthe reporting of outcomes.
Population
The participants enrolled in the included trials were children rang-ing from six months to 18 years of age. The echinacea trials differedin the selection criteria of participants as they used children with-out a significant health problem and without a history of recurrentARTI. The remainder of the trials included a history of recurrentARTIs in the inclusion criteria. All the trials were conducted inthe Northern (boreal) hemisphere except Fukuda’s (Fukuda 1999).Fall and winter seasons referred to the months from Septemberto January. The year of the trial was not specified in most of thestudies.
Interventions
Forty studies used bacterial products, four studies used herbal ex-tracts (echinacea and garlic), 11 studies used synthetic compounds,five studies used thymic extracts (thymomodulin) and one studyused a synthetic interferon. All trials used a placebo control. Thecommon names of the medications are in Table 1.Twenty-two studies had a duration shorter than six months, 33studies had a duration of six months and only six studies had aduration longer than six months. The duration of seven D53 trialswas less than six months and nine D53 trials had a duration of sixmonths. In all D53 trials the description of the methodology wasnot clear and different routes of administration were used (nasalspray or by mouth). Ten OM-85 BV trials lasted six months; twotrials had a duration of longer than six months.
Outcomes
Only 35 of the 61 included studies reported the mean and SDof the incidence of respiratory infections or provided data to cal-culate these measure, allowing their inclusion in the meta-analy-sis (Ahrens 1984; Arroyave 1999; Careddu 1994a; Clerici 1988;Cohen 2004; De Loore 1979; Del-Rio-Navarro 2003; Fiocchi1986; Garabedian 1990; Gutiérrez-Tarango 2001; Gómez-Barreto1998; Hauguenauer 1987; Hüls 1995; Jara-Pérez 2000; Karam-Bechara 1995; Lacomme 1985; Litzman 1999; Maestroni 1984;Motta 1994; Paupe 1986; Pech 1987; Piquett 1986; RB10 1994;RB17 1988; RB21 1988; RB22 1990; RB24 1990; RB25 1990;Saracho-Weber 2001; Schaad 1986; Schaad 2002; Van Eygen1976; Van Eygen 1979; Vautel 1993; Zagar 1988). In these studies
the ARTIs were defined by the presence of respiratory signs andsymptoms.The remaining 24 studies reported a variety of end points: symp-toms, clinical scales or presence or absence of respiratory infec-tions. Some trials reported the frequency of ARTIs as either equalto or more than one infection (Burgio 1994; Careddu 1994b;Fukuda 1999; Mora 2010a; Paupe 1991; Rutishauser 1998; Taylor2003; Wahl 2008); equal to or more than two infections (Mora2007); equal to or more than three infections (Collet 1993); thetotal number of ARTIs; mean number of ARTIs (Caramia 1994;Chen 2004; Dils 1979; Fiocchi 1988; Longo 1988; Passali 1994;Pozzi 2004; Riedl-Seifert 1995; Sramek 1986); or reduction inthe number of ARTIs (Andrianova 2003; Iuldashev 1988). Othersmeasured the severity of symptoms using clinical scales that werenot validated (Fiocchi 1989; Giovannini 2000; Mora 2002; Renzo2004) or as days suffering symptoms (Martin du Pan 1982).
Excluded studies
We excluded 36 studies: 32 did not comply with the selectioncriteria; two compared several IS treatments without a placebogroup; and two were duplicate reports of trials already included.See Characteristics of excluded studies table.
Risk of bias in included studies
The description of the methodology was not clear in most ofthe studies. Only 17.1% (6 out of 35) studies reported adequaterandomisation and blinding (participants and treating physicianswere blinded) (Cohen 2004; Collet 1993; Del-Rio-Navarro 2003;Gutiérrez-Tarango 2001; Jara-Perez 2000; Taylor 2003) (Figure1). Using the quality rating criteria (Higgins 2011), the quality ofthe rest of the trials (28 out of 34 (82.4%)) was B; randomisationand follow through of participants was unclear. See Table 2 for adescription of the quality of the trials.Only 17.1% (6 out of 35) studies reported on the number ofparticipants lost to follow up (Cohen 2004; Collet 1993; Del-Rio-Navarro 2003; Gutiérrez-Tarango 2001; Jara-Perez 2000; Taylor2003). Of these, five studies reported losses. While losses wereminimal, 0.5% to 7% in three studies, two studies reported aloss of 18% and 24%. As additional data were not obtained fromthe investigators on the outcomes of participants who were lostto follow up an intention-to-treat (ITT) analysis could not beundertaken. The numbers lost to follow up are explained in furtherdetail.In the Cohen 2004 trial, 160 out of 215 in the IS group com-pleted the trial (27 dropped out because the medication had anunpleasant taste, 24 due to non-compliance which was not fullyexplained, four dropped out due to a lack of confidence in thetreatment); and 168 out of 215 of the placebo group completedthe trial (22 dropped out because the placebo had an unpleasanttaste, 21 due to non-compliance which was not fully explained,
643Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
and one dropped out due to a lack of confidence in the treatment).A total of 24% were lost to follow up.In the Del-Rio-Navarro 2003 trial, 20 out of 25 in the IS groupcompleted the trial. Five children were lost to follow up. Twentyout of 24 in the placebo group completed the trial. Two childrenwere lost to follow up (the parents of one participant withdrewconsent for their child to continue in the trial and one left becausethe trial medication caused the child to have diarrhea). A total of18% were lost to follow up.In the Collet 1993 trial, 199 out of 210 in the IS group and 196out of 213 placebo group completed the trial. For both groups,the 28 lost to follow up were related either to the parents movingto a different location or the mothers stopped working and nolonger took their children to the daycare centres where the trialswere being held. A total of 7% were lost to follow up.In the Taylor 2003 trial, 242 out of 263 in the IS group completedthe trial (six withdrew before the first ARTI, five changed theirminds about participating, one never received the study medica-tion, five withdrew during the first ARTI, three refused the studymedication, one was concerned about the effect on their immunesystem, for one the protocol was too complicated, six log bookswere never received, four were lost to follow up); 244 out of 261in the placebo group completed the trial (three withdrew beforethe first ARTI, two changed their minds about participating, onewas excluded for taking another medication, one withdrew duringthe first ARTI, nine log books were never received and four werelost to follow up). A total of 7% were lost to follow up.In the Jara-Pérez 2000 trial, 99 out of 100 in the IS group com-pleted the trial. The case report from one child was lost. One hun-dred out of 100 in the placebo group completed the trial. A totalof 0.5% were lost to follow up.In the Gutiérrez-Tarango 2001 trial, outcomes were reported forall enrolled children. All the participants completed the trial.The outcome assessor was blinded to the treatment allocation in8.8% (three out of 34) of the studies (Cohen 2004; Collet 1993;Taylor 2003). Only 14.7% (five out of 34) of studies (Cohen 2004;Collet 1993; Del-Rio-Navarro 2003; Gutiérrez-Tarango 2001;Taylor 2003) were considered of quality A (Higgins 2011). Therest of the studies were of poor quality.
Allocation
In the studies with a proper description of randomisation andallocation (Cohen 2004; Collet 1993; Del-Rio-Navarro 2003;Gutiérrez-Tarango 2001; Jara-Perez 2000; Taylor 2003), the im-plementation of the random sequence of the treatments was re-ported. In Cohen 2004 active medication and the placebo weresupplied directly by the manufacturer and all randomisation lotswere stored in a sealed envelope at the pharmacy of the company,to be opened only in the event of an emergency. In Collet 1993participants were allocated to IS or placebo according to a pro-gram for remote data entry (Minitel a national telecommunica-
tion system network in France). Additionally, randomisation wasalso stratified by study centre and blocked for every four children.In the studies by Del-Rio-Navarro 2003 and Gutiérrez-Tarango2001 consecutive numbered study medication boxes, as well as aclosed opaque envelope describing the treatment, were supplieddirectly by the manufacturer; participants received a patient num-ber coincident with treatment number when the selection criteriawere completed. In the Jara-Perez 2000 study consecutive num-bered study medication boxes, as well as a closed opaque enve-lope describing the treatment, were supplied directly by the man-ufacturer; participants received a patient number corresponding atreatment according to an alphabetical name list. In Taylor 2003,each study centre had a supply of study medication (active medi-cation and placebo) in consecutively numbered bottles that wereidentical in appearance, contents of each bottle were randomlydetermined using a computer-generated randomisation list, andrandomisation was stratified by site and in blocks of 10. Enrolledchildren were assigned a unique study number corresponding tothe numbers on the bottles of study medication. Figure 1 showsthe review authors’ judgement of the risk of bias related to allo-cation concealment presented as percentages across all includedstudies and Figure 2shows the risk for each included study.
Blinding
Six studies (Cohen 2004; Collet 1993; Del-Rio-Navarro 2003;Gutiérrez-Tarango 2001; Jara-Perez 2000; Taylor 2003) claimedthat IS and placebo treatment had identical appearance and thatthe taste of both were similar. Investigators and participants werenot aware of the received treatment.
Incomplete outcome data
Only six studies (Cohen 2004; Collet 1993; Del-Rio-Navarro2003; Gutiérrez-Tarango 2001; Jara-Perez 2000; Taylor 2003) re-ported the number of patients lost to follow up. All used only theavailable data for the analyses. No imputation for the incompletedata were intended.Cohen 2004 had a total of 24% lost to follow up; the frequenciesand causes of it were similar in active and placebo groups. Inthe Del-Rio-Navarro 2003 trial 18% of participants were lost tofollow up; more children in the active group were lost (5/25 inactive group versus 2/25 in the placebo group). In the Collet 1993trial, 7% of participants were lost to follow up; in both groups therates and the reasons were similar. In the Taylor 2003 trial, 7% ofparticipants were lost to follow up; in both groups the rates andthe reasons were similar. In the Jara-Pérez 2000 trial only the dataof one participant on IS was lost. In the Gutiérrez-Tarango 2001trial, all the participants completed the trial.
Selective reporting
644Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
The study protocols were not available. Sixty-one randomized,placebo-controlled clinical trials were identified. Only 35 stud-ies reported the mean and SD of the incidence of respiratoryinfections or provided data to calculate these measure (Ahrens1984; Arroyave 1999; Careddu 1994a; Clerici 1988; Cohen2004; De Loore 1979; Del-Rio-Navarro 2003; Fiocchi 1986;Garabedian 1990; Gutiérrez-Tarango 2001; Gómez-Barreto 1998;Hauguenauer 1987; Hüls 1995; Jara-Pérez 2000; Karam-Bechara1995; Lacomme 1985; Litzman 1999; Maestroni 1984; Motta1994; Paupe 1986; Pech 1987; Piquett 1986; RB10 1994;RB17 1988; RB21 1988; RB22 1990; RB24 1990; RB25 1990;Saracho-Weber 2001; Schaad 1986; Schaad 2002; Van Eygen1976; Van Eygen 1979; Vautel 1993; Zagar 1988). Seven trialsreported the frequency of ARTIs (Burgio 1994; Careddu 1994b;Collet 1993; Fukuda 1999; Paupe 1991; Rutishauser 1998; Taylor2003). The rest of the studies did not use outcome measures rele-vant to the prevention of respiratory infections.
Other potential sources of bias
In 29 out of the 35 included studies, the process of randomisationand allocation was not described. Additionally, the disposition ofparticipants and reasons for withdrawals were not reported.Funnel plots of IS effects have a considerable asymmetry, indicat-ing possible publication bias, i.e. publishing only positive results(see Assessment of reporting biases). Language bias is also possible(publication in languages other than English and publication in
non-indexed, small, local journals).
Effects of interventions
See: Summary of findings for the main comparison Summaryof findings table
Effect of immunostimulants (IS) on acute respiratory
tract infections (ARTIs)
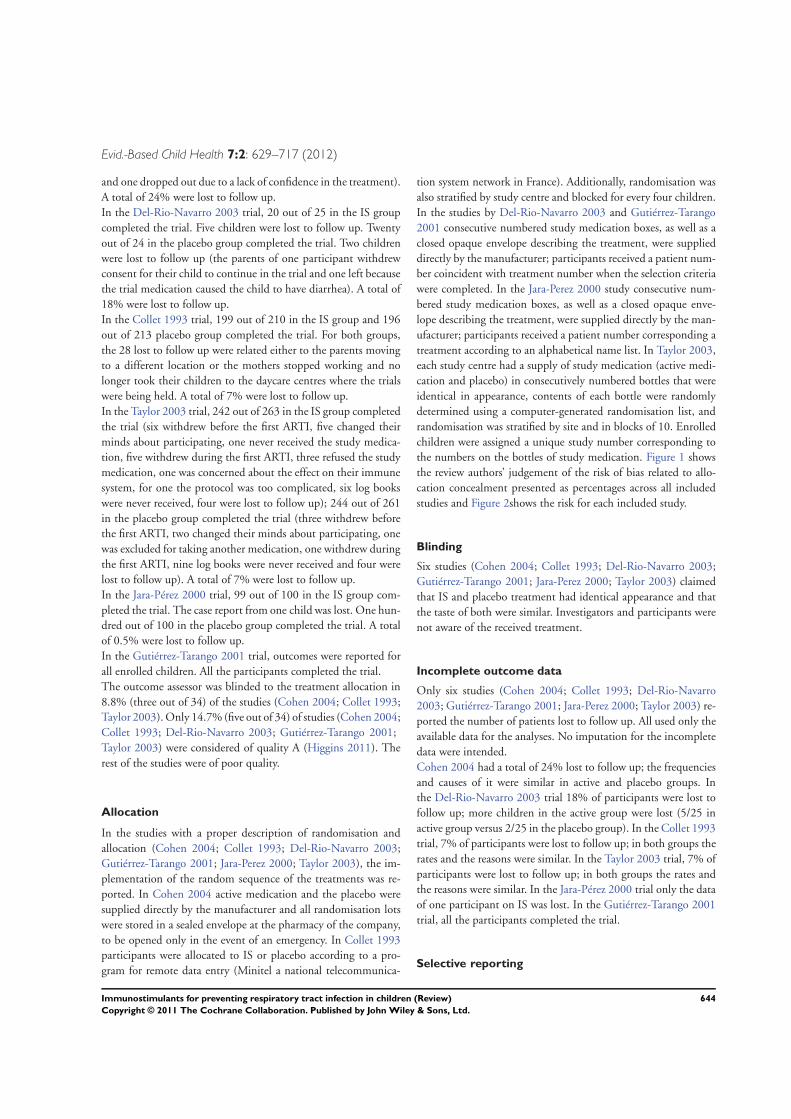
Of the 61 included studies only 35 provided data in a form suitablefor inclusion in the meta-analysis for this outcome. All 35 trialscompared IS with a placebo.Twenty-four out of 35 studies showed a reduction of ARTIs, bothas total numbers and as a percentage reduction of ARTIs (consid-ering the mean number of ARTIs in the placebo group as 100%).In the meta-analysis the use of IS was shown to reduce the totalnumber of ARTIs (mean difference (MD) -1.24 95% CI -1.54to -0.94) as well as producing a percentage change in the rate ofARTIs (MD -38.84%; 95% CI -46.37% to -31.31%). The totalnumber of ARTIs outcome showed high heterogeneity (I2 statistic= 94.0%, Chi2 test = 582.02, P < 0.00001); the use of percent-age change in the rate of ARTIs reduced the heterogeneity butit remained very high (I2 statistic = 83.0%, Chi2 test = 195.07,P < 0.00001). Therefore, we decided to use the random-effectsmodel with MD to calculate the global effect of immunostimu-lants (Figure 5; Figure 6).
645Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
Figure 5. Forest plot of comparison: Any IS compared with placebo, outcome: 1.1 Mean number of ARTIs.
646Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Evid.-Based Child Health 7:2: 629–717 (2012)
Figure 6. Forest plot of comparison: Any IS compared with placebo, outcome: 1.2 Per cent difference in
ARTIs.
We investigated heterogeneity by bivariate correlation as well asby linear regression. The variables considered were total numberof children in the study, duration of the trial, mean number ofARTIs in the control group versus the mean difference in numberof ARTIs and mean difference in the percentage of ARTIs. Themain source of heterogeneity was the mean number of ARTIs inthe control group, using the mean difference in number of ARTIs(linear regression model correlation - 0.672, P < 0.001). Usingthe mean difference in the percentage of ARTIs, the source ofheterogeneity was related to the mean difference in the number ofARTIs and mean number of ARTIs in the control group (linearregression model correlation 0.834, P < 0.001). The age of theparticipants in each trial could be another important source ofvariation in the number of ARTIs, as younger children wouldsuffer more ARTIs. Yet the age in each trial was diverse, includingenrolled preschool children, school-aged children and adolescents.This made the exploration of this potential source of variationproblematic. In general, the net reduction in the number of ARTIswas dependent on the background rate of ARTIs.
Another potential source of heterogeneity was the type of IS. Wedecided to investigate this source of heterogeneity by performingsub-analyses as follows.
1. Including the bacterial IS studies data (and excluding theSaracho-Weber 2001 trial because it was the only trial with moreARTIs in the IS group than in the placebo group, probably dueto a clerical mistake inverting ARTI incidences). The number oftrials was 24; total number of participants was 2154, the numberof IS participants was 1091 and the number of placeboparticipants was 1063. The reduction in the total number ofARTIs was MD -1.41 (95% CI -1.85 to -0.98); the reduction inthe number of ARTIs as a percentage was MD -41.21 (95% CI -49.10 to -33.31).
2. Only bacterial IS studies data (excluding Saracho-Weber2001) with a total number of participants of at least 40. Thenumber of trials was 19; the total number of participants was2009, the number of IS participants was 1019 and the numberof placebo participants was 990. The reduction in the total
647Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
number of ARTIs was MD -1.42 (95% CI -1.92 to -0.93); andthe reduction in the number of ARTIs as a percentage was MD -38.44 (95% CI -47.25 to -29.63).
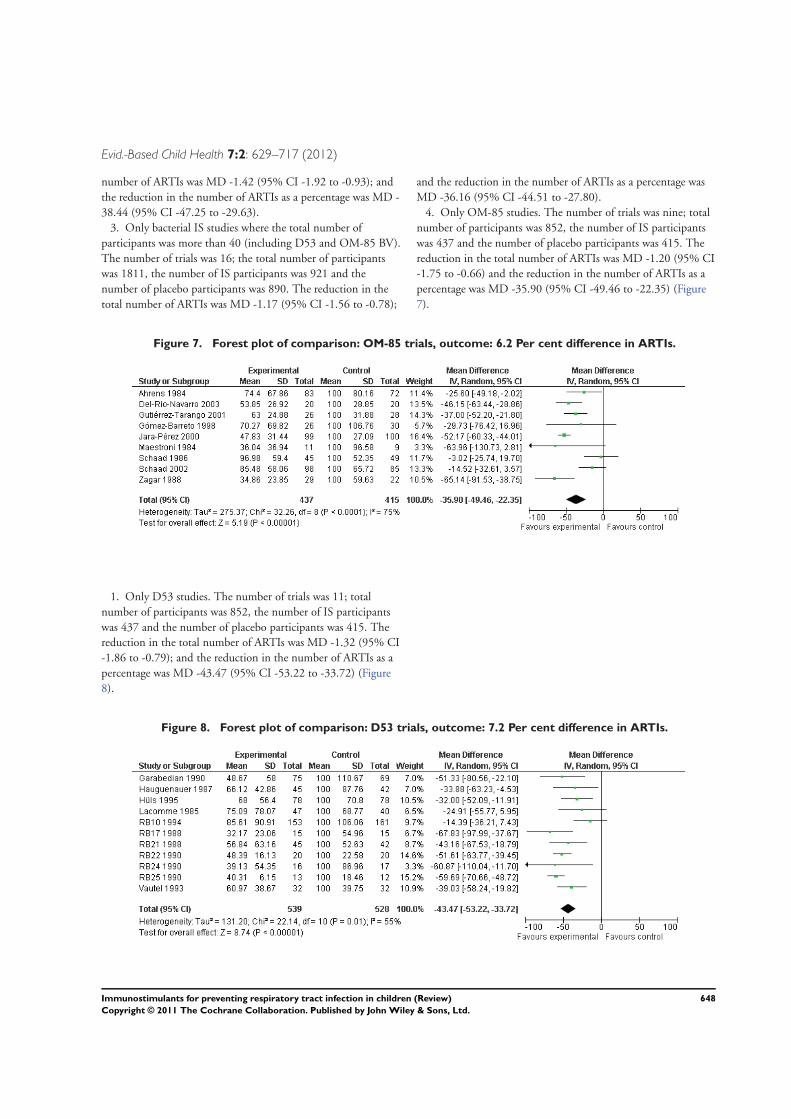
3. Only bacterial IS studies where the total number ofparticipants was more than 40 (including D53 and OM-85 BV).The number of trials was 16; the total number of participantswas 1811, the number of IS participants was 921 and thenumber of placebo participants was 890. The reduction in thetotal number of ARTIs was MD -1.17 (95% CI -1.56 to -0.78);
and the reduction in the number of ARTIs as a percentage wasMD -36.16 (95% CI -44.51 to -27.80).
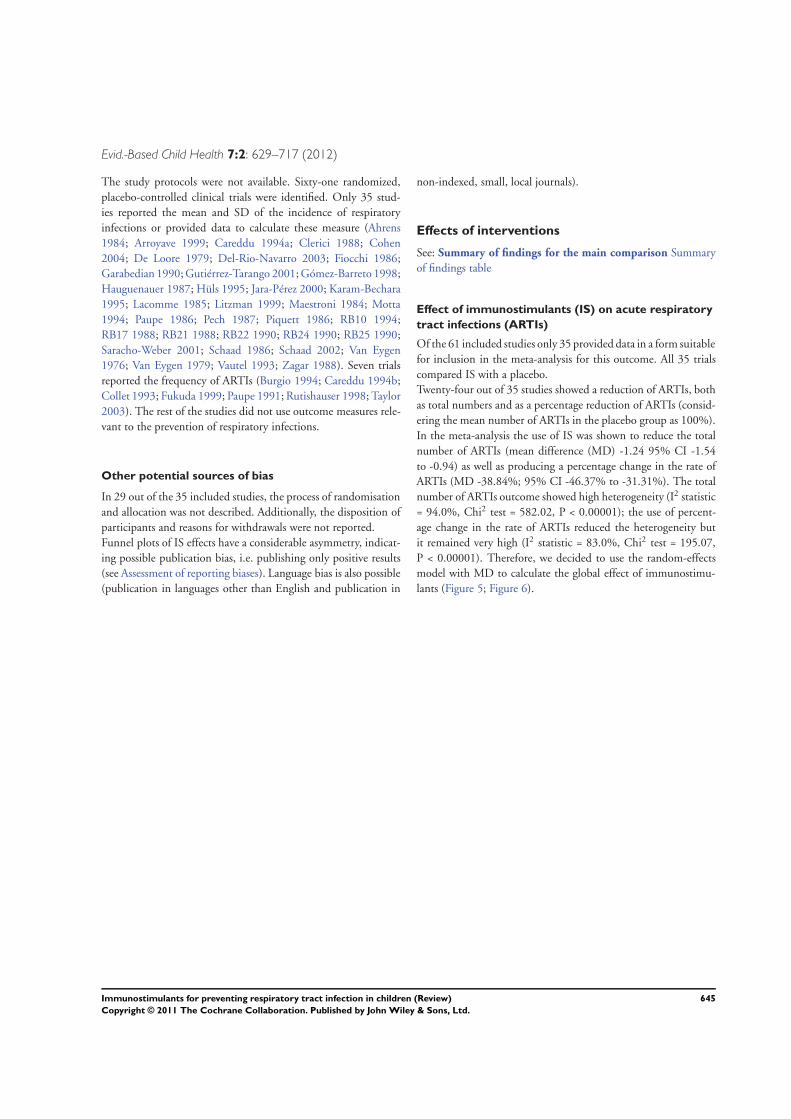
4. Only OM-85 studies. The number of trials was nine; totalnumber of participants was 852, the number of IS participantswas 437 and the number of placebo participants was 415. Thereduction in the total number of ARTIs was MD -1.20 (95% CI-1.75 to -0.66) and the reduction in the number of ARTIs as apercentage was MD -35.90 (95% CI -49.46 to -22.35) (Figure7).
Figure 7. Forest plot of comparison: OM-85 trials, outcome: 6.2 Per cent difference in ARTIs.
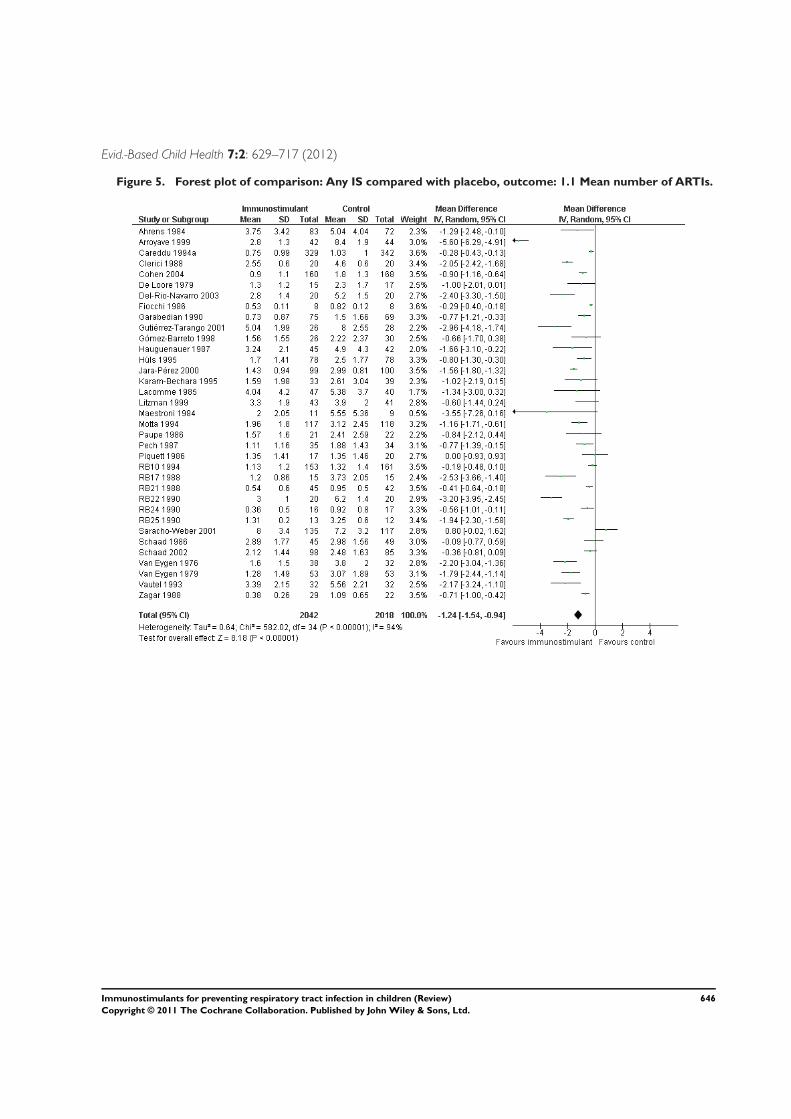
1. Only D53 studies. The number of trials was 11; totalnumber of participants was 852, the number of IS participantswas 437 and the number of placebo participants was 415. Thereduction in the total number of ARTIs was MD -1.32 (95% CI-1.86 to -0.79); and the reduction in the number of ARTIs as apercentage was MD -43.47 (95% CI -53.22 to -33.72) (Figure8).
Figure 8. Forest plot of comparison: D53 trials, outcome: 7.2 Per cent difference in ARTIs.
648Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)We did not perform the sub-analyses for good quality trials as onlytwo out of five trials provided data as mean and SD (Del-Rio-Navarro 2003; Gutiérrez-Tarango 2001). The selection of bacterialIS studies reduced the heterogeneity of the percentage differenceoutcome from very high (I2 statistic > 75) to moderate (I2 statistic <75) (Higgins 2003). However, the percentage differences and 95%CI in the total number of ARTIs were similar to the overall analysisfor all sub-analyses. The reduction of the I2 statistic when onlythe bacterial IS were analyzed confirmed that the different kindsof IS were another major source of heterogeneity. The combinedanalysis of percentage difference outcome of D53 and OM-85 hadan I2 statistic of 65%; D53 alone 55%; OM-85 alone 75%.
Adverse effects
Twenty studies provided data on adverse events in a form suit-able for inclusion in the meta-analysis. The most frequent eventswere skin and gastrointestinal effects (nausea, vomiting, abdomi-nal pain and diarrhea). No statistically significant difference wasshown in these adverse events when comparing IS with a placebo.A summary of the reported safety data for each trial is noted in theoutcome section of the Characteristics of included studies table.In 22 studies, authors did not report the presence or absence ofadverse events (Andrianova 2003; Bánovein 1992; Clerici 1988;Fiocchi 1986; Fiocchi 1988; Garabedian 1990; Giovannini 2000;Hauguenauer 1987; Iuldashev 1988; Longo 1988; Maestroni1984; Martin du Pan 1982; Piquett 1986; Prusek 1987; RB101994; RB17 1988; RB21 1988; RB22 1990; RB24 1990; RB251990; Saracho-Weber 2001; Sramek 1986). In eight studies, trialauthors claimed that no adverse event were observed (Chen 2004;De Loore 1979; Dils 1979; Karam-Bechara 1995; Mora 2007Renzo 2004; Van Eygen 1976; Zagar 1988). In four studies no ad-verse events were observed in the immunostimulant group (Burgio1994; Fiocchi 1989; Lacomme 1985; Schaad 1986). Five studiesreported a single case of adverse events in the IS group (Fukuda1999; Gómez-Barreto 1998; Paupe 1986; Paupe 1991; Van Eygen1979). One study reported only two adverse events (Wahl 2008).In three studies no adverse events related to administration of thetrial medications were reported (Arroyave 1999; Jara-Pérez 2000;Mora 2010a).
D I S C U S S I O N
Summary of main results
This review shows that IS reduce the incidence of ARTIs by about40% on average (from 35 trials with a total of 4060 participants).However, due to the poor quality of the included trials this may bean overestimate of the true effect of IS. Most of the trials reporteda low incidence of adverse events or no adverse events. The mostfrequent adverse events were gastrointestinal complaints such as
nausea, vomiting, abdominal pain and diarrhea; and skin disorderssuch as rash, urticaria and pruritus.The possible beneficial effects of immunostimulants in the pre-vention of ARTIs, cancers, AIDS/HIV infections, tuberculosis etc.have been awaited expectantly by many clinicians and medicalresearchers. One of the main indications of registered IS is theprevention of ARTIs in children, as they are more susceptible toARTIs. IS use is common in some countries in Europe and in theAmericas as result of the demand to reduce the incidence of ARTIsin children.While the use of IS is currently controversial and is viewed withskepticism by many physicians, there have been several clinical tri-als supporting their use as ancillary treatment and in the preven-tion of ARTIs. Yet their mechanism of action and possible bene-fits and risks are not well known. The aim of this review was tosynthesise all the evidence currently available from trials on thistopic to enable a more robust, unbiased assessment of the role ofefficacy and safety of IS to prevent ARTIs in children.After reviewing all available IS studies on the prevention of ARTIsin children, we empathise with the skepticism of many physicians.This review has a number of limitations due to the quality andreporting of the trials on this topic, the heterogeneity of the in-cluded trials and the possibility of publication bias. Few paperscomplied with standards for methodological quality and reportingof clinical trials, with the majority having significant deviationsfrom these standards. In addition, the lack of detail in many of thetrial publications limited the quality of this review.The most common problems with the included trials were thatthey:
• did not report data on ARTIs sufficient to reproduceparametric and non-parametric statistical tests or carry out meta-analysis;
• did not establish the normal incidence of ARTIs in the localpopulation and the number of infections in susceptible children,therefore, endpoint changes were not properly established;
• did not identify the possible causes of recurrent ARTIs;• did not try to isolate or identify the causative pathogen;• did not calculate the sample size required;• used small sample sizes;• did not include a clinical definition of ARTI and other end
points or used non validated scales;• misused statistical tests, especially the use of Student’s t test
for data under suspicion of non-normal distribution (SD >mean/2 or mean - SD < 0);
• under reported adverse events or did not report them at all;• did not report the power of the statistical tests in trials
without significant difference;• did not report or explain the flow chart and attrition of the
participants and the statistical methods did not consider the datafrom missing participants (censored data);
• published articles in low impact journals;• included heterogeneous groups of children comprising
649Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Evid.-Based Child Health 7:2: 629–717 (2012)
infants, toddlers, schoolboys and girls and adolescents withoutconsidering the incidence of ARTIs in each group;
• did not control for or report on confounding factors (that isto say, age groups, concomitant asthma or allergy, number ofsiblings, smokers at home, birth weight, seasons during the study,time and timing of attendance at daycare centre or school).
• did not report the quality and standardisation of the herbalsupplements (Wolsko 2005) and bacterial extracts.
All the trials were conducted in populations of highly susceptiblechildren (secondary prevention) except Collet 1993 and Jara-Pérez2000, which studied children over-exposed to ARTIs due to thefact that they attended daycare centres and an orphanage, respec-tively, and Martin du Pan 1982 which included a subgroup fromdaycare centres. In contrast, the echinacea trials were carried out inpopulations without a history of recurrent ARTIs (Cohen 2004;Taylor 2003).The lack of significance of the findings of some trials could beascribed to small sample size, duration of the intervention, seasonof intervention, broad participant selection criteria (mainly diverseage groups) and low incidence of ARTIs in the studied population(caused by an over-reporting of previous ARTIs or reduction ofincidence as children grew older).Thymic extracts have been withdrawn from sale in several coun-tries, due to the possible prion contamination and consequentrisk of bovine spongiform encephalopathy (WHO 2005). The useof levamisole is restricted because of the risk of agranulocytosis,neurologic disease (Symoens 1978) and leukoencephalopathy (Xu2009).The overall effect of IS was a reduction in the total number ofARTIs (MD -1.24; 95% CI -1.54 to -0.94) but the individualsize of the effect in each trial depended on the number of ARTIsin the control group. The size of the effect could seem small butexpressing the reduction of ARTIs as a percentage indicates a goodeffect, about 40% (MD -38.84%; 95% CI -46.37 to -31.31). Theresults indicate that the reduction in the incidence of ARTIs is areal possibility but as the net effect depends on the background rateof ARTIs the effect would only be noticeable when the number ofinfections to be reduced is higher than the normal incidence fora given age group. Therefore, the use of IS for the prevention ofARTIs must be limited to children with proven high susceptibilityto ARTIs or over-exposed children who are over-exposed to ARTIsbecause they are in daycare centres, orphanages, kindergarten orelementary school.Sub-analysis of studies with available databases (Del-Rio-Navarro2003; Gutiérrez-Tarango 2001; Jara-Pérez 2000) have shown thatIS are not very effective in the prevention of one ARTI but are inthe prevention of recurrent infections (that is, two or three). Thismay be the reason why echinacea trials fail to show protection tothe first infection but had some effect on the second infection. Inaddition, the participants had no history of increased incidenceof ARTI. In a re-analysis of one study (Taylor 2003) it was foundthat 69.2% of the children treated with placebo had a second
ARTI while only 55.8% of children on echinacea had a secondinfection (P = 0.01). However, this effect could not be exploredin this review.In all meta-analyses it is important to consider the presence andpossible effect of publication bias; that is, the selective publicationof trials with positive results. The funnel plot demonstrated con-siderable asymmetry, indicating possible publication bias. Othertypes of bias that could affect the funnel plot are the language bias(publication in languages other than English and publication innon-indexed, small, local journals), poor methodological design,inadequate analysis and inadequate presentation of the results. Inonly one study (Saracho-Weber 2001) the treated group had anincrease in ARTIs and, therefore, a positive difference.The high heterogeneity limits the external validity of the analyseswith all the studies. However, when we selected only the studieson bacterial IS (particularly those of D53 and OM-85 BV), andused percentage of ARTIs, the heterogeneity could be regardedas acceptable. It is important to note that the size of the effectsis similar in the different sub-analyses, supporting the externalvalidity of the conclusions.On the basis of the asymmetry shown in the funnel plot, the het-erogeneity of the trials and the low quality of many included trials,the possibility of bias (resulting in an overestimation of the trueeffects of IS on ARTIs) should be considered as high. Therefore,caution needs to be applied when interpreting the possible advan-tages of IS shown in this review. However, the results of this reviewprovide a reference to the probable effect of IS in the prevention ofARTIs in children and point to the need for further clinical trials.Further trials on IS must follow the established guidelines (Collet1992; Moher 2001; Valleron 1992), estimate sample size accordingto realistic incidence of ARTI and control for confounding factors.Multivariable analysis should be used when confounding factorsare identified. Reports of such trials must include enough data toreplicate non-parametric statistical tests (for instance, frequencyof ARTIs at the end point) and include statistical analysis dealingwith censored data (Mahe 1999). Registration of all the protocolsand ongoing trials would be desirable to obtain all the possibleoutcomes. It would be necessary to conduct trials on otitis andlower ARTIs with large numbers of highly susceptible children.Considering the present review, the prevention of ARTIs usingIS may be possible. Larger clinical trials, adequately powered forimportant population groups, sponsored by health authorities,would be desirable to establish the true effects of IS and the effectof individual IS preparations.
Overall completeness and applicability ofevidence
According to the funnel plots, it is possible that some trials withnegative results have not been published (Figure 3 and Figure 4).
650Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Evid.-Based Child Health 7:2: 629–717 (2012)
Quality of the evidence
Although the global quality of the trials was poor, a group ofstudies comply with the quality standards (Cohen 2004; Collet1993; Del-Rio-Navarro 2003; Gutiérrez-Tarango 2001; Jara-Perez2000; Taylor 2003).Due to the above and the classification of the studies with theGRADEpro tool, the global quality of the evidence on the effect ofimmunostimulants to reduce the incidence of ARTIs is regardedas moderate. Additional research is likely to have an impact on ourconfidence in the estimate of effect and may change the estimate.Meanwhile, the evidence of the incidence of adverse events is con-sidered as low. Further research is very likely to have an importantimpact on our confidence in the estimate of effect and is likelyto change the estimate, as the incidence of adverse events was notproperly reported in most of the studies. See Summary of findingsfor the main comparison.
Potential biases in the review process
We consider the risk of biases in the review process minimal, asthe plausible sources of information have been consulted and theauthors and manufactures were contacted. Additionally, no exter-nal funding was provided for this review.
Agreements and disagreements with otherstudies or reviews
The present review is in agreement with a previous meta-analysison the effect of IS showing a percent decrease in ARTIs of -42.64%(95% CI -45.19% to -40.08%) (Berber 2001).Another review on the effect of D53 in the incidence of ARTIsshowed a reduction of child ear, nose and throat (ENT) infec-tions of 27% to 68%, and a decrease in child ENT and bron-chopulmonary infections of 32% to 61% compared with placebo(Bellanti 2003). This concurs with the effect of D53 shown in thisreview.Other meta-analyses on the effect of individual IS report an effectas a percent reduction of -31.86% (95% CI -34.32 to -29.40) forD53, and a corresponding reduction of -39.28% (95% CI -52.58to -25.98) for OM-85 (De-La-Torre-Gonzalez 2005). Both CIsare in agreement with those in this review.Schaad (Schaad 2010) in a meta-analysis reported that in an OM-85 BV-treated population, 32% had three or more ARTIs in sixmonths, against 58.2% in the placebo-treated population. The
reduction with OM-85 was -1.21 (95% CI -1.39 to -1.03), whichis similar to the findings in this review.The results of this review do not agree with the review by Steurer-Stey (Steurer-Stey 2007) which pooled two OM-85 studies tocalculate the risk of fewer than three infections over six months offollow up in children not in daycare (RR 0.82; 95% CI 0.65 to1.02).
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
This review indicates that IS reduce the incidence of ARTIs by 40%on average in susceptible children. The trials have shown benefitsof IS in toddlers (two to five years), school boys (six to 12 years)and children with a high incidence of ARTIs, for example childrenattending daycare and children living in orphanages. Studies inhealthy children are not available. Although the safety profile in thestudies was good, some IS may be unsafe. For instance, levamisolehas been related to agranulocytosis and neurologic disease, andthymic extracts introduce the risk of prion contamination andtherefore the risk of bovine spongiform encephalopathy.
Implications for research
Further high-quality trials are required to confirm the true effectof IS and individual IS preparations in the prevention of ARTIs.We encourage national health authorities to conduct large, mul-ticentre, double-blind, placebo-controlled studies to establish theprecise benefits and risks for using IS to prevent ARTIs. It is nec-essary to conduct more studies on the number and frequency ofARTIs and the physiological and immunological basis of recurrentARTIs.
A C K N O W L E D G E M E N T S
We especially acknowledged the great editorial work of Liz Doo-ley. We thank Arturo Berber for his contribution to the protocol.The authors also wish to thank the following people for comment-ing on the draft review of the first version: Chanpen Choprapa-won, Ville Peltola, Richard Shoemaker and Ludovic Reveiz; andto Anne Lyddiatt, Ville Peltola, Sree Nair and Ludovic Reveiz forthe comments on the updated draft review.
651Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
R E F E R E N C E S
References to studies included in this review
Ahrens 1984 {published data only}
Ahrens J. Multicentre double-blind clinical trial withbroncho-vaxom in children. Therapiewoche 1984;34:3469–75.
Andrianova 2003 {published data only}
Andrianova IV, Sobenin IA, Sereda EV, Borodina LI,Studenikin MI. Effect of long-acting garlic tablets “allicor”on the incidence of acute respiratory viral infections inchildren. Terapevticheskii Arkhiv 2003;75(3):53–6.
Arroyave 1999 {published data only}
Arroyave CM. Klebsiella pneumoniae glycoproteins ascoadjuvants in the prevention of recurrent respiratoryinfections in children 1 to 6 years of age [Glicoproteínas deKlebsiella pneumoniae como coadyuvantes en la prevenciónde infecciones recurrentes respiratorias en niños de 1 a 6años de edad]. Revista Alergia México 1999;46(3):66–71.[MEDLINE: 10425883]
Burgio 1994 {published data only}
Burgio GR, Marseglia GL, Severi F, De Benedetti F,Masarone M, Ottolenghi A, et al. Immunoactivationby pidotimod in children with recurrent respiratoryinfections. Arzneimittelforschung 1994;44(Suppl 12A):152–9. [MEDLINE: 7857357]
Caramia 1994 {published data only}
Caramia G, Clemente E, Solli R, Mei V, Cera R,Carnelli V, et al. Efficacy and safety of pidotimod in thetreatment of recurrent respiratory infections in children.Arzneimittelforschung 1994;44(Suppl 12A):1480–4.[MEDLINE: 7857347]
Careddu 1994a {published data only}∗ Careddu P. Role of immunoactivation with pidotimodin recurrent respiratory infections in childhood.Arzneimittelforschung 1994;44(Suppl 12A):1506–11.[MEDLINE: 7857353]Careddu P, Biolchini A, Alfano S, Zavattini G. Pidotimodin the prophylaxis of recurrent acute tonsillitis in childhood.Advances in Oto-Rhino-Laryngology 1992;47:328–31.[MEDLINE: 1456157]
Careddu 1994b {published data only}
Careddu P, Alfano S, Zavattini G. Pidotimod in theprophylaxis of recurrent acute tonsillitis in childhood.Advances in Therapy 1992;9(3):174–83.∗ Careddu P, Mei V, Venturoli V, Corsini A. Pidotimodin the treatment of recurrent respiratory infections inpaediatric patients. Arzneimittelforschung 1994;44(Suppl12A):1485–9. [MEDLINE: 7857348]
Chen 2004 {published data only}
Chen AH, Chen RC, Zhang CQ, Chen D, Huang S,Lin Y, et al. Efficacy of sublingual polyvalent bacterialvaccine (Lantigen B) in children with recurrent respiratoryinfection: a randomized double-blind controlled clinical
trial. Zhonghua Er Ke Za Zhi [Chinese Journal of Pediatrics]
2004;42(6):463–4.
Clerici 1988 {published data only}
Clerici-Schoeller M, Careddu P, Sandri MT, Cazzola P.Recurrent respiratory infections in children: prevention ofacute episodes by oral administration of thymomodulin.Current Therapeutic Research, Clinical and Experimental
1988;44(4):503–9.
Cohen 2004 {published data only}
Cohen HA, Varsano I, Kahan E, Sarrell EM, Uziel Y.Effectiveness of an herbal preparation containing echinacea,propolis, and vitamin C in preventing respiratory tractinfections in children: a randomized, double-blind,placebo-controlled, multicenter study. Archives of Pediatrics
& Adolescent Medicine 2004;158(3):217–21.
Collet 1993 {published data only}
Aymard M, Chomel JJ, Allard JP, Thouvenot D, HoneggerD, Floret D, et al. Epidemiology of viral infections andevaluation of the potential benefit of OM-85 BV on thevirologic status of children attending day-care centers.Respiration 1994;61(Suppl 1):24–31. [MEDLINE:7800968]∗ Collet JP, Ducruet T, Kramer MS, Haggerty J, Floret D,Chomel JJ, et al. Stimulation of nonspecific immunity toreduce the risk of recurrent infections in children attendingday-care centers. The Epicreche Research Group. Pediatric
Infectious Disease Journal 1993;12(8):648–52. [MEDLINE:8414777]
De Loore 1979 {published data only}
De Loore F, Heck E, Van Eygen M, Casneuf J. Levamisole(R 12564) in the prevention of recurrent upper respiratorytract infections in children: a double-blind, placebo-controlled study. Current Medical Research and Opinion
1979;6(2):142–7.
Del-Rio-Navarro 2003 {published and unpublished data}
Del Río Navarro BE, Luis Sienra Monge JJ, Berber A,Torres Alcantara S, Avila Castañón L, Gómez Barreto D.Use of OM-85 BV in children suffering from recurrentrespiratory tract infections and subnormal IgG subclasslevels. Allergologia et Immunopathologia 2003;31:7–13.
Dils 1979 {published data only}
Dils F. A placebo controlled, double-blind evaluation oflevamisole in the reduction of the frequency, duration andseverity of attacks in children suffering from recurrent upperrespiratory tract infections. Journal of International Medical
Research 1979;7(4):302–4.
Fiocchi 1986 {published data only}
Fiocchi A, Borella E, Riva E, Arensi D, Travaglini P, CazzolaP, et al. A double-blind clinical trial for the evaluation ofthe therapeutical effectiveness of a calf thymus derivative(thymomodulin) in children with recurrent respiratoryinfections. Thymus 1986;8(6):331–9. [MEDLINE:3544353]
652Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
Fiocchi 1988 {published data only}
Fiocchi A, Zuccotti G, Rottoli A, Grasso U, Pogliani L,Vimercati E, et al. Treatment with immucytal in recidivantrespiratory infection in the pediatric age [Trattamento conimmucytal nele infezioni respiratorie recidivanti in etapediatrica]. Rivista di Pediatria Preventiva e Sociale 1988;38
(4):213–9.
Fiocchi 1989 {published data only}
Fiocchi A, Arancio R, Cinquepalmi P, Sala M, Zuccotti GV,Riva E, et al. Recurrent respiratory infections in childhood:experience with a bacterial extract plus bacterial ribosomes(immucytal). Journal of International Medical Research
1990;18(1):50–60. [MEDLINE: 2185964]∗ Fiocchi A, Vignati B, Cinquepalmi P, Machado E, PeanoL, Pulejo R, et al. Treatment using immucytal in childrenwith recurrent respiratory infections: an Italian multicenterexperience [Terapia con immucytal di bambini affettida infezioni respiratorie recidivanti: esperienza italinapolicentrica]. La Pediatria Medica e Chirurgica 1989;11(3):285–92. [MEDLINE: 2687818]
Fukuda 1999 {published data only}
Fukuda Y, Jordão-Neves BM, da-Cunha J, MangabeiraAlbernaz PL. Assessment of efficacy and safety ofthymomodulin (Leucogen®) in the prevention ofrecurrent otitis media and recurrent tonsillitis [Estudoclínico–imunológico da eficácia de timomodulina(Leucogen®) na otite média aguda recorrente e naamigdalite de repetição]. Pediatria Moderna 1999;XXV
(10):828–34. [: www.moerirajr.com.br/pediatriamoderna/ped1099/pedleuco.htm]
Garabedian 1990 {published data only}
Bellanti J, Olivieri D, Serrano E. Ribosomalimmunostimulation: assessment of studies evaluating itsclinical relevance in the prevention of upper and lowerrespiratory tract infections in children and adults. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2003;17:355–67.Boyle P, Bellantu JA, Robertson C. Meta-analysis ofpublished clinical trials of a ribosomal vaccine (RibomunylR) in prevention of respiratory infections. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2000;14:389–408.∗ Garabedian EN, Dubreuil C, Triglia JC. Effectivenessand tolerance of Ribomunyl tablets in preventing middleear infections in children affected by S.O.M. InternationalCongress on Prevention of Infection, Nice, France. 1990.
Giovannini 2000 {published data only}
Giovannini M, Fiocchi A, Sala M, Fontana P, Fiori L, SilanoM, et al. Immucytal(R) in the prevention and treatmentof recurrent upper respiratory tract infections in children:a randomized, placebo-controlled, double-blind study.International Journal of Immunotherapy 2000;16(3-4):67–75.
Gutiérrez-Tarango 2001 {published and unpublished data}
Gutiérrez-Tarango MD, Berber A. Safety and efficacy oftwo courses of OM-85 BV in the prevention of respiratory
tract Infections in children during 12 months. Chest 2001;119(6):1742–8.
Gómez-Barreto 1998 {published and unpublished data}
Gomez Barreto D, De la Torre C, Alvarez A, Faure A, BerberA. Safety and efficacy of OM-85-BV plus amoxicillin/clavulanate in the treatment of subacute sinusitis and theprevention of recurrent infections in children [Seguridady eficacia de OM–85–BV más amoxicilina/clavulanatoen el tratamiento de la sinusitis subaguda y prevenciónde infecciones recurrentes en niños]. Allergologia et
Immunopathologia 1998;26(1):17–22. [MEDLINE:9585823]
Hauguenauer 1987 {published data only}
Bellanti J, Olivieri D, Serrano E. Ribosomalimmunostimulation: assessment of studies evaluating itsclinical relevance in the prevention of upper and lowerrespiratory tract infections in children and adults. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2003;17:355–67.Boyle P, Bellantu JA, Robertson C. Meta-analysis ofpublished clinical trials of a ribosomal vaccine (RibomunylR) in prevention of respiratory infections. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2000;14:389–408.∗ Haguernauer JP. Prevention of the ENT repeatinginfectious episodes by D53 tablets in children of less than 5years [Prévention des épisodes infectieux récidivants de lasphére ORL par D53 comimés chez lénfant de moins de 5ans]. Immunologie Medicale 1987;18:36–9.
Hüls 1995 {published data only}
Bellanti J, Olivieri D, Serrano E. Ribosomalimmunostimulation: assessment of studies evaluating itsclinical relevance in the prevention of upper and lowerrespiratory tract infections in children and adults. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2003;17:355–67.∗ Hüls P, Welbers P, Lindemann H. Immunotherapyof children with the help of a multibacterial ribosomalpreparation [Immuntherapie bei kindern mit hilfe einesmultibakteriellen ribosomenpräparates]. Der Kinderartz
1995;26(8):1018–24.
Iuldashev 1988 {published data only}
Iuldashev AK, Slepushkin AN, Khodzhaeva MA, SchastnyiEI, Kamilov FK. Prophylactic efficacy of reaferon in viralhepatitis A and acute respiratory infections in children.Zhurnal Mikrobiologii, Epidemiologii, i Immunobiologii
1988;5:65–9.
Jara-Pérez 2000 {published and unpublished data}
Jara-Perez JV, Berber A. Primary prevention of acuterespiratory tract infections in children using a bacterialimmunostimulant: a double-masked, placebo-controlledclinical trial. Clinical Therapeutics 2000;22(6):748–59.[MEDLINE: 10929921]
Karam-Bechara 1995 {published data only}
Karam-Bechara J, Rodríguez-Suárez R, Fuare-Fontela A,Posada-Maldonado EE, Rivera-Gutiérrez SM, Sánchez-Díaz
653Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Evid.-Based Child Health 7:2: 629–717 (2012)
R. Thymomodulin in the prevention of recurrent infectiousepisodes of chronic bronchitis in pediatric patients. Doubleblind trial [Timomodulina en la prevención de los episodiosinfecciosos recurrentes de la bronquitis crónica en pacientespediátricos. Estudio doble ciego]. Investigación Médica
Internacional 1995;22(43):43–51.
Lacomme 1985 {published data only}
Bellanti J, Olivieri D, Serrano E. Ribosomalimmunostimulation: assessment of studies evaluating itsclinical relevance in the prevention of upper and lowerrespiratory tract infections in children and adults. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2003;17:355–67.Boyle P, Bellantu JA, Robertson C. Meta-analysis ofpublished clinical trials of a ribosomal vaccine (RibomunylR) in prevention of respiratory infections. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2000;14:389–408.∗ Lacomme Y, Narcy P. Prevention of the repeating episodesof ENT superinfection by ribosomal immunotherapy in thechild. Clinical results of a multicenter study [Prévention parimmunothérapie ribosomale des épisodes de superinfectionrécidivantes de la sphére ORL chez l’enfant. Résultatscliniques d’une étude multicentrique]. Immunologie
Medicale 1985;11:73–5.
Litzman 1999 {published data only}
Litzman J, Lokaj J, Krejci M, Pesak S, Morgan G.Isoprinosine does not protect against frequent respiratorytract infections in childhood. European Journal of Pediatrics
1999;158(1):32–7.
Longo 1988 {published data only}
Longo F, Lepore L, Agosti E, Panizon F. Evaluation of theeffectiveness of thymomodulin in children with recurrentrespiratory infections. La Pediatria Medica e Chirurgica
1988;10(6):603–7. [MEDLINE: 3244540]
Maestroni 1984 {published data only}
Losa GA, Maestroni GJ. Clinical and immunobiologicalaction of an orally administered bacterial extract.Schweizerische Medizinische Wochenschrift 1984;114(25):930–2. [MEDLINE: 6235582]∗ Maestroni GJ, Losa GA. Clinical and immunobiologicaleffects of an orally administered bacterial extract.International Journal of Immunopharmacology 1984;6(2):111–7.
Martin du Pan 1982 {published data only}
Martin du Pan RE, Martin du Pan RC. Clinical studyconcerning the prevention of infections of the upperrespiratory tract of preschool children. Schweizerische
Rundschau fur Medizin Praxis 1982;71(36):1385–9.
Mora 2002 {published data only}
Mora R, Barbieri M, Passali GC, Sovatzis A, Mora F,Cordone MP. A preventive measure for otitis mediain children with upper respiratory tract infections.International Journal of Pediatric Otorhinolaryngology 2002;63(2):111–8.
Mora 2007 {published data only}
Mora R, Dellepiane M, Crippa B, Salami A. Ribosomaltherapy in the prophylaxis of recurrent pharyngotonsillitisin children. International Journal of Pediatric
Otorhinolaryngology 2007;71(2):257–61. [PUBMED:17126918]
Mora 2010a {published data only}
Mora R, Dellepiane M, Crippa B, Guastini L, SantomauroV, Salami A. Ribosomal therapy in the treatment ofrecurrent acute adenoiditis. European Archives of Oto-Rhino-Laryngology 2010 (in press (pending)). [PUBMED:20052587]
Motta 1994 {published data only}
Motta G, De Campora E, De Vita C, Esposito S,Galletti C, Incutti V, et al. Immunoactivity of pidotimodagainst episodes of recurrent tonsillitis in childhood.Arzneimittelforschung 1994;44(Suppl 12A):1521–4.[MEDLINE: 7857356]
Passali 1994a {published data only}∗ Passali D, Calearo C, Conticello S. Pidotimod in themanagement of recurrent pharyngotonsillar infections inchildhood. Arzneimittelforschung 1994;44(12A):1511–6.[MEDLINE: 7857354]Passali D, Calearo C, Conticello S, Ferri P, ZavattiniG. Recurrent pharingo-tonsillar infections in infants.Treatment with pidotimod [Le infezioni ricorrentifaringo–tonsillari dell’infanzia: tattamento con pidotimod].Otorinolaringologia Pediatrica 1994;V(3):231–9.
Paupe 1986 {published data only}
Paupe J, Paupe G. Biostim prevention of recurrentrespiratory infections in children. A double-blind versusplacebo study [Prévention par le biostim des infectionsrespiratoiresá répétition chez l’enfant]. Annales de Pediatrie
1986;33(9):843–5.
Paupe 1991 {published data only}∗ Paupe J. Immunotherapy with an oral bacterial extract(OM-85 BV) for upper respiratory infections. Respiration
1991;58(3-4):150–4. [MEDLINE: 1745846]Paupe J. Value of Imocur in the prevention of recurrentinfections in children under six years of age. Results of amulticenter, placebo-controlled trial [Interet d’imocur(r)dans la prevention des infections recidivantes del’enfantde moins de six ans. Resultats d’une etude multicentriquecontre placebo]. Annales de Pediatrie 1990;37(7):475–9.[MEDLINE: 2256645]
Pech 1987 {published data only}
Pech A, Zanaret M. Double blind trial of biostim versusplacebo in children repeating rhinopharyngities [Etudedu biostim double aveugle contre placebo dans lesrhinopharyngities récidivantes del’enfant]. Les Cahiers
d’ORL 1987;22:217–20.Reinert P, Morales M, Brin S, Fagnani. Evaluation of RU41740 for the prevention of recurrent nasopharyngealinfections in pediatric patients [Evaluation d’un traitementpreventif par RU 41740 (biostim) des infections
654Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
rhinopharyngees recidivantes de l’enfant]. Annales de
Pediatrie 1995;42:454–60.
Piquett 1986 {published data only}
Piquet JJ, Piedro P. Bisotim investigation in the treatmentof recurrent ENT infections in children [Intéret du biostimdans le traitement des infections ORL récidivantes del’enfant]. Les Cahiers d’ORL 1986;21:725–30.Reinert P, Morales M, Brin S, Fagnani. Evaluation of RU41740 for the prevention of recurrent nasopharyngealinfections in pediatric patients [Evaluation d’un traitementpreventif par RU 41740 (biostim) des infectionsrhinopharyngees recidivantes de l’enfant]. Annales de
Pediatrie 1995;42:454–60.
Pozzi 2004 {published data only}
Pozzi E, Serra C. Efficacy of Lantigen B in the prevention ofbacterial respiratory infections. Monaldi Archives for Chest
Disease 2004;61(1):19–27.
RB10 1994 {published data only}∗ Bellanti J, Olivieri D, Serrano E. Ribosomalimmunostimulation: assessment of studies evaluating itsclinical relevance in the prevention of upper and lowerrespiratory tract infections in children and adults. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2003;17:355–67.
RB17 1988 {published data only}∗ Bellanti J, Olivieri D, Serrano E. Ribosomalimmunostimulation: assessment of studies evaluating itsclinical relevance in the prevention of upper and lowerrespiratory tract infections in children and adults. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2003;17:355–67.
RB21 1988 {published data only}∗ Bellanti J, Olivieri D, Serrano E. Ribosomalimmunostimulation: assessment of studies evaluating itsclinical relevance in the prevention of upper and lowerrespiratory tract infections in children and adults. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2003;17:355–67.
RB22 1990 {published data only}∗ Bellanti J, Olivieri D, Serrano E. Ribosomalimmunostimulation: assessment of studies evaluating itsclinical relevance in the prevention of upper and lowerrespiratory tract infections in children and adults. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2003;17:355–67.
RB24 1990 {published data only}∗ Bellanti J, Olivieri D, Serrano E. Ribosomalimmunostimulation: assessment of studies evaluating itsclinical relevance in the prevention of upper and lowerrespiratory tract infections in children and adults. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2003;17:355–67.
RB25 1990 {published data only}∗ Bellanti J, Olivieri D, Serrano E. Ribosomalimmunostimulation: assessment of studies evaluating itsclinical relevance in the prevention of upper and lower
respiratory tract infections in children and adults. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2003;17:355–67.
Renzo 2004 {published data only}
Renzo M, Giovanni R, Maria PF, Barbara C, StefanoO, Francesco M, et al. Short ribosomal prophylaxis inthe prevention of clinical recurrences of chronic otitismedia in children. International Journal of Pediatric
Otorhinolaryngology 2004;68(1):83–9.
Riedl-Seifert 1995 {published data only}
Riedl-Seifert RJ, van Aubel A, Kammereit A, Elsasser U.Reduction of the number and severity of respiratory tractinfections in children by oral immunostimulation. Advances
in Experimental Medicine and Biology 1995;371B:799–802.[MEDLINE: 7502900]
Rutishauser 1998 {published data only}
Rutishauser M, Pitzke P, Grevers G, van Aubel A, ElsasserU, Kammereit A. Use of a polyvalent bacterial lysate inpatients with recurrent respiratory tract infections: resultsof a prospective, placebo-controlled, randomized, double-blind study. Advances in Therapy 1998;15(6):330–41.
Saracho-Weber 2001 {published data only}
Saracho-Weber F, Vázquez-Ramos V, Ayala-Barajas C.Evaluation of glycoprotein of Klebsiella pneumoniaeefficacy in recurrent infections [Evaluación de la eficacia deglucoproteínas de Klebsiella pneumoniae en infeccionesrecurrentes]. Alergia Asma e Inmunología Pediátrica 2001;10
(2):33–9.
Schaad 1986 {published data only}
Schaad UB, Farine JC, Fux T. Prospective placebo-controlleddouble-blind study using a bacterial lysate in infectionsof the respiratory tract and ENT region in children[Prospective placebo–kontrollierte Doppelblindstudie miteinem Bakterienlysat bei Infektionen der Atemwege und desORL–Bereiches im Kindesalter]. Helvetica Paediatrica Acta
1986;41(1-2):7–17.
Schaad 2002 {published and unpublished data}
Schaad UB, Mutterlein R, Goffin H, BV-Child StudyGroup. Immunostimulation with OM-85 in children withrecurrent infections of the upper respiratory tract: a double-blind, placebo-controlled multicenter study. Chest 2002;122:2042–9.
Sramek 1986 {published data only}
Sramek J, Josifko M, Helcl J, Holoubkova E, Janout V,Kozesnik B, et al. Bacterial lysate (I.R.S. 19) appliedintranasally in the prevention of acute respiratory diseasesin children: A randomized double-blind study. Journal of
Hygiene, Epidemiology, Microbiology, and Immunology 1986;30(4):377–85. [MEDLINE: PMID: 3805711]
Taylor 2003 {published data only}
Barret B. Efficacy and safety of echinacea in treating upperrespiratory tract infections in children: a randomizedcontrolled trial. Journal of Pediatrics 2004;145(1):135–6.∗ Taylor JA, Weber W, Standish L, Quinn H, GoeslingJ, McGann M, et al. Efficacy and safety of echinaceain treating upper respiratory tract infections in children:
655Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
a randomized controlled trial. JAMA 2003;290(21):2824–30.Weber W, Taylor JA, Stoep AV, Weiss NS, Standish LJ,Calabrese C. Echinacea purpurea for prevention of upperrespiratory tract infections in children. Journal of Alternative
and Complementary Medicine 2005;11:1021–6.Weber WJ, Taylor JA, Vander Stoep A, Weiss N, StandishLJ, Calabrese C. The effect of echinacea purpurea treatmenton prevention of upper respiratory tract infections inchildren. Journal of Investigative Medicine 2004;52(Suppl2):392.
Van Eygen 1976 {published data only}
Van Eygen M, Znamensky PY, Heck E, Raymaekers I.Levamisole in prevention of recurrent upper-respiratory-tract infections in children. Lancet 1976;1(7956):382–5.
Van Eygen 1979 {published data only}
Van Eygen M, Dils F, Gillerot J, Verschueren E. A double-blind pediatric evaluation of levamisole in the preventionof recurrent upper respiratory tract infections. European
Journal of Pediatrics 1979;131(3):147–53.
Vautel 1993 {published data only}
Bellanti J, Olivieri D, Serrano E. Ribosomalimmunostimulation: assessment of studies evaluating itsclinical relevance in the prevention of upper and lowerrespiratory tract infections in children and adults. BioDrugs:
Clinical Immunotherapeutics, Biopharmaceuticals and Gene
Therapy 2003;17:355–67.∗ Vautel JM, Cauquil J, Perruchet AM, Thomas AM.Prevention of recurrent ear, nose, and throat infections inyoung children with Ribomunyl, double-blind, placebo-controlled study. Current Therapeutic Research, Clinical and
Experimental 1993;53(6):722–9.
Wahl 2008 {published data only}∗ Wahl RA, Aldous MB, Worden KA, Grant KL. Echinaceapurpurea and osteopathic manipulative treatment inchildren with recurrent otitis media: a randomizedcontrolled trial. BMC Complementary and Alternative
Medicine 2008;8(56):1–9. [PUBMED: 18831749]
Zagar 1988 {published data only}
Zagar S, Lofler-Badzek D. Broncho-vaxom in children withrhinosinusitis: a double-blind clinical trial. Journal for Oto-
Rhino-Laryngology and its Related Specialties 1988;50(6):397–404. [MEDLINE: 3068610]
References to studies excluded from this review
Almeida 1999 {published data only}
Almeida VM, Matta JJ, Hernández DD, Campos MG.Immunomodulatory effect of a glycoprotein from klebsiellaversus levamisole in asthmatic patients with phagocyticdeficiency. Alergia, Asma e Inmunología Pediátricas 1999;8(3):85–9.
Aymard 1994 {published data only}
Aymard M, Chomel JJ, Allard JP, Thouvenot D, HoneggerD, Floret D, et al. Epidemiology of viral infections andevaluation of the potential benefit of OM-85 BV on the
virologic status of children attending day-care centers.Respiration 1994;61(Suppl 1):24–31.
Barr 1965 {published data only}
Barr SE, Brown H, Fuchs M, Orvis H, Connor A, MurrayFJ, et al. A double-blind study of the effects of bacterialvaccine on infective asthma. Journal of Allergy and Clinical
Immunology 1965;36:47–61.
Bánovein 1992 {published data only}
Banovcin P, Minarik M, Rosslerova V, Miklerova M, Cap J,Pullmann R. Broncho-vaxom and IRS 19 in the treatmentof recurrent respiratory tract inflammation in children[Broncho–vaxom a IRS 19 vliebe recidivujucich zapalovdychacich ciest u deti]. Ceskoslovenska Pediatrie 1992;47
(11):666–9. [MEDLINE: 1483278]
Das 2000 {published data only}
Das GC. Evaluation of immunomodulatory effects ofbacterial vaccine in patients with recurrent respiratory tractinfections. XVII International Congress of Allergology andClinical Immunology (ICACI). 2000.
Fiocchi 1990 {published data only}
Fiocchi A, Arancio R, Cinquepalmi P, Sala M, Zuccotti GV,Riva E, et al. Recurrent respiratory infections in childhood:experience with a bacterial extract plus bacterial ribosomes(immucytal). Journal of International Medical Research
1990;18(1):50–60.
Fontana 1965 {published data only}
Fontana VJ, Salanitro AS, Wolfe HI, Moreno F.Hyposensitization with bacterial vaccine in infectiousasthma. A double-blind study and a longitudinal study.JAMA 1965;193:895–900.
Grimfeld 2004 {published data only}
Grimfeld A, Holgate ST, Canonica GW, Bonini S, BorresMP, Adam D, et al. Prophylactic management of children atrisk for recurrent upper respiratory infections: the preventiaI study. Clinical & Experimental Allergy 2004;34(11):1665–72. [PUBMED: 15544588]
Grimm 1999 {published data only}
Grimm W, Muller HH. A randomized controlled trial ofthe effect of fluid extract of Echinacea purpurea on theincidence and severity of colds and respiratory infections.American Journal of Medicine 1999;106(2):138–43.
Heinz 2010 {published data only}
Heinz SA, Henson DA, Austin MD, Jin F, NiemanDC. Quercetin supplementation and upper respiratorytract infection: a randomized community clinical trial.Pharmacological Research 2010;62(3):237–42.
Herrera-Basto 1998 {published data only}
Herrera-Basto E, Hernández-Guerra R, Escamilla G,Robledo JL. Pidotimod in the treatment of recurrentrespiratory infection [Pidotimod en el tratamiento de lainfección respiratoria recurrente]. Investigación Médica
Internacional 1998;25(8):8–13.
Kozhukharova 1987 {published data only}
Kozhukharova MS, Slepushkin AN, Radeva KhT,Lavrukhina LA, Demidova SA. Evaluation of dipyridamole
656Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
efficacy as an agent for preventing acute respiratory viraldiseases. Voprosy Virusologii 1987;32(3):294–7.
Lauriello 1990 {published data only}
Lauriello G, Giella D, Berra A, Matonti V. Combinationof oral bacterial vaccines and antibiotics in acute recurrentrespiratory infections [Sull’associazione vaccino battericoorale e antibiotici in corso di infezioni respiratorie acutericorrenti]. Clinica Terapeutica 1990;133:87–90.
Luchikhin 2000 {published data only}
Luchikhin LA, Beliakova LV, Gurov AV. Prevention andtreatment of upper respiratory tract infections with IRS-19and polydex with phenylephrine. Vestnik Otorinolaringologii
2000;4:54–7.
Ma 1994 {published data only}
Ma R, Zhang XL, Tian J. Clinical study on repeatedinfantile respiratory tract infection treated by kangganzhibao oral liquor. Zhongguo Zhong Xi Yi Jie He Za Zhi
1994;14(10):586–8.
Macchi 2005 {published data only}
Macchi A, Vecchia LD. Open comparative, randomizedcontrolled clinical study of a new immunostimulatingbacterial lysate in the prophylaxis of upper respiratory tractinfections. Arzneimittelforschung 2005;55(5):276–81.
Makovetskaya 2001 {published data only}
Makovetskaya GA, Zhestkova VV, Kuznetsova TL.Efficiency of the IRS-19 aerosol vaccine in children withrelapsing diseases of upper respiratory tract. Kazanskii
Meditsinskii Zhurnal 2001;82(1):15–6.
Mora 2010b {published data only}
Mora R, Dellepiane M, Crippa B, Guastini L, SantomauroV, Salami A. Ribosomal therapy in the treatment ofrecurrent acute adenoiditis. European Archives of Oto-Rhino-
Laryngology 2010;267(8):1313–8.
Mueller 1969 {published data only}
Mueller HL, Lanz M. Hyposensitization with bacterialvaccine in infectious asthma. A double-blind study and alongitudinal study. JAMA 1969;208:1379–83.
Nespoli 1992 {published data only}
Nespoli L. Action of thymomodulin in the prevention ofrespiratory infection in the child entering to elementaryschool [Attivita della timomodulina nella prevenzione delleinfezioni respiratorie del bambino ala prima scolarizzazione].Rivista di Pediatria Preventiva e Sociale 1992;42(2):133.
Obrosova-Serova 1972 {published data only}
Obrosova-Serova NP, Fedorova GI, Glukhov PI, Shal’novMI, Litvinov VG. Effectiveness of midantan and interferoninducers as means of non-specific prevention of influenza.Antibiotiki 1972;17(8):734–8.
Oggiano 1985 {published data only}
Oggiano N, Di Girolamo F, Salvucci C, Marinelli M,Gentili A, Pecora R, et al. Oral polyvalent bacterial vaccinein children with recurrent respiratory infections [Vaccinobatterico orale polivalente in bambini con infezionirespiratoire ricorrenti (I.R.R.)]. Minerva Pediatrica 1985;37:741–5.
Oldini 1990 {published data only}
Oldini C, De Berti G, Vecchi E. The employment of theImmucytal spray in nasopharyngeal pathology [L’Impiegodell’Immucytal spray nella patologia nasofaringea].Otorinolarongologia 1990;40:67–72.
Ortega del 2005 {published data only}
Ortega del Alamo P, Rivera Rodriguez T, Sanz FernandezR. The effect of AM3 in the resolution of otitis media witheffusion (OME) in paediatric patients [Efecto de AM3 sobrela resolución de la otitis media serosa (OMS) en pacientespediátricos]. Acta Otorrinolaringologica Espanola 2005;56
(1):1–5.
Predy 2005 {published data only}
Predy GN, Goel V, Lovlin R, Donner A, Stitt L, Basu TK.Efficacy of an extract of North American ginseng containingpoly-furanosyl-pyranosyl-saccharides for preventing upperrespiratory tract infections: a randomized controlled trial.Canadian Medical Association Journal 2005;173:1043–8.
Prusek 1987 {published data only}
Prusek W, Jankowski A, Radomska G, WieczorekE, Podwysocka M. Immunostimulation in recurrentrespiratory tract infections therapy in children. Archivum
Immunologiae et Therapiae Experimentalis 1987;35(3):289–302. [MEDLINE: 3502238]
Razi 2010 {published data only}
Razi CH, Harmanci K, Abaci A, Özdemir O, Hizli S,Renda R, et al. The immunostimulant OM-85 BV preventswheezing attacks in preschool children. Journal of Allergy
and Clinical Immunology 2010;126(4):763–9.
Riedl-Seifert 1993 {published data only}
Riedl-Seifert RD, van Aubel A, Kämmereit A, Elsasser U.Infection recurrence in children - still a crux medicorum?Results of a double-blind placebo-controlled with an oralbacterial lysate to infections in children [Infektrezidiveim Kindesalter – noch immer iene Crux medicorum?Ergebnisse einer plazebokontrollierten Doppelblindstudiemit einem oralen Bakterienlysat bei infektanfälligenKindern]. Journal of Pharmacoloy and Therapy 1993;3:108–17.
Rosaschino 2004 {published data only}
Rosaschino F, Cattaneo L. Strategies for optimizingcompliance of paediatric patients for seasonal antibacterialvaccination with sublingually administered polyvalentmechanical bacterial Lysates (PMBL). Acta Bio Medica
Ateneo Parmense 2004;75(3):171–8.
Rossi 2004 {published data only}
Rossi S, Tazza R. Efficacy and safety of a newimmunostimulating bacterial lysate in the prophylaxis ofacute lower respiratory tract infections. A randomised,open, controlled clinical trial. Arzneimittelforschung 2004;54(1):50–6.
Ruah 2001 {published data only}
Ruah SB, Ruah C, van Aubel A, Abel S, Elsasser U. Efficacyof a polyvalent bacterial lysate in children with recurrentrespiratory tract infections. Advances in Therapy 2001;18
(4):151–62.
657Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
Rytel 1974 {published data only}
Rytel MW, Ferstenfeld JE, Rose HD, Balay J, Pierce WE,Lynch KL. Efficacy of a “mixed bacterial vaccine” inprophylaxis of acute respiratory infections: possible roleof interferon. American Journal of Epidemiology 1974;99:347–59.
Scotti 1987 {published data only}
Scotti L, Biondelli G, Borzani M. Use of a polyvalentoral bacterial vaccine in recurrent respiratory infections inchildren [Impiego di un vaccino batterico orale polivalentenelle infezioni respiratorie recidivanti del bambino].Minerva Pediatrica 1987;39:251–6.
Steinsbekk 2005 {published data only}
Steinsbekk A, Bentzen N, Fønnebø V, Lewith G. Selftreatment with one of three self selected, ultramolecularhomeopathic medicines for the prevention of upperrespiratory tract infections in children. A double-blindrandomized placebo controlled trial. British Journal of
Clinical Pharmacology 2005;59(4):447–55. [PUBMED:15801940]
Vascotto 1985 {published data only}
Vascotto M, Fossi E, Mancini E, Guerrini L. Efficacy of apolyvalent bacterial vaccine administered by aerosol in thetreatment of children with respiratory infections [Efficaciadi un vaccino batterico polivalente somministrato per viaaerosolica nel trattamento del bambino catarrale]. Minerva
Pediatrica 1985;37:409–14.
Yale 2004 {published data only}
Yale SH, Liu K. Echinacea purpurea therapy for thetreatment of the common cold: a randomized, double-blind, placebo-controlled clinical trial. Archives of Internal
Medicine 2004;164(11):1237–41.
Additional references
Aggarwal 2007
Aggarwal R, Sentz J, Miller MA. Role of zinc administrationin prevention of childhood diarrhea and respiratoryillnesses: a meta-analysis. Pediatrics 2007;119(6):1120–30.[PUBMED: 17545379]
Alyanakian 2006
Alyanakian MA, Grela F, Aumeunier A, Chiavaroli C,Gouarin C, Bardel E, et al. Transforming growth factor-{beta} and natural killer T-cells are involved in the protectiveeffect of a bacterial extract on type 1 diabetes. Diabetes
2006;55(1):179–85.
Barreto 1994
Barreto ML, Santos LM, Assis AM, Araújo MPN, FarenzenaGG, Santos PAB, et al. Effect of vitamin A supplementationon diarrhoea and acute lower-respiratory-tract infections inyoung children in Brazil. Lancet 1994;344(8917):228–31.[MEDLINE: 7913157; : 94301083 94301083]
Bell 1989
Bell DM, Gleiber DW, Mercer AA, Phifer R, Guinter RH,Cohen AJ, et al. Illness associated with child day care:a study of incidence and cost. American Journal of Public
Health 1989;79(4):479–84. [MEDLINE: 2929808; :89191073]
Bellanti 2003
Bellanti JA, Olivieri D, Serrano E. Ribosomalimmunostimulation: assessment of studies evaluating itsclinical relevance in the prevention of upper and lowerrespiratory tract infections in children and adults. BioDrugs
2003;17(5):355–67.
Berber 1996
Berber AC, Del-Rio-Navarro BE. Use of broncho-vaxomin private practice: phase IV trial in 587 children. Clinical
Therapeutics 1996;18(6):1068–79. [MEDLINE: 9001824]
Berber 2001
Berber A, Del-Rio-Navarro B. Compilation and meta-analysis of randomized placebo-controlled clinical trials onthe prevention of respiratory tract infections in childrenusing immunostimulants. Journal of Investigational
Allergology and Clinical Immunology 2001;11(4):235–46.[PUBMED: 11908811]
Campbell 1995
Campbell H. Acute respiratory infection: a globalchallenges. Archives of Diseases in Childhood 1995;73(4):281–6. [MEDLINE: 7492188]
CDCIDSG 1984
The Child Day Care Infectious Disease Study Group.Public health considerations of infectious diseases in childday care centres. Journal of Pediatrics 1984;105:683–701.
Chen 2008a
Chen H, Zhuo Q, Yuan W, Wang J, Wu T. Vitamin Afor preventing acute lower respiratory tract infections inchildren up to seven years of age. Cochrane Database
of Systematic Reviews 2008, Issue 1. [DOI: 10.1002/14651858.CD006090.pub2]
Chen 2008b
Chen LY, Lin YL, Chiang BL. Levamisole enhances immuneresponse by affecting the activation and maturation ofhuman monocyte-derived dendritic cells. Clinical &
Experimental Allergy 2008;151(1):174–81. [PUBMED:18005262]
Collet 1992
Collet JP. Immunomodulators and primary preventionof respiratory infections: methodological considerations.Developments in Biological Standardization 1992;77:159–65.[MEDLINE: 1426657]
Dahan 1986
Dahan R, Constantini D, Caulin C, Yagello M. Clinicaltrials with C 1740, an immunomodulator compoundproposed for prevention of acute infectious exacerbations inchronic bronchitis. Methods and Findings in Experimental
and Clinical Pharmacology 1986;8(1):41–3. [MEDLINE:3517520]
Dajani 1995
Dajani A, Taubert K, Frrieri P, Peter G, Shulman S.Treatment of acute streptococcal pharyngitis and preventionof rheumatic fever. Pediatrics 1995;96(4 Pt 1):758–64.[MEDLINE: 7567345]
658Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
De Mattia 1993
De Mattia D, Decandia P, Ferrante P, Pace D, Martire B,Ciccarelli M, et al. Effectiveness of thymostimulin and studyof lymphocyte-dependent antibacterial activity in childrenwith recurrent respiratory infections. Immunopharmacology
and Immunotoxicology 1993;15(4):447–59. [MEDLINE:8227971]
De-La-Torre-Gonzalez 2005
De-la-Torre-Gonzalez C, Pacheco-Rios A, Escalante-Dominguez AJ, del-Rio-Navarro BE. Comparative meta-analysis of immunostimulant agents used in pediatricpatients in Mexico [Metaanalisis comparativo de losinmunoestimulantes utilizados enpediatría en México].Revista Alergia Mexico 2005;52(1):25–38. [PUBMED:15957470]
Denny 1986
Denny FW, Collier AM, Henderson FW. Acute respiratoryinfections in day care. Reviews of Infectious Diseases 1986;8(4):527–32. [MEDLINE: 3529308]
Egger 1997
Egger M, Davey Smith G, Schneider M, Minder C. Biasin meta-analysis detected by a simple, graphical test. BMJ
1997;315(7109):629–34.
Fendrick 2003
Fendrick AM, Monto AS, Nightengale B, Sarnes M. Theeconomic burden of non-influenza-related viral respiratorytract infection in the United States. Archives of Internal
Medicine 2003;163:487–94.
Flores-Hernandez1999
Flores-Hernandez S, Reyes-Morales H, Perez-Cuevas R,Guiscafre-Gallardo H. The day care center as a risk factorfor acute respiratory infections. Archives of Medical Research
1999;30(3):216–23.
Grüber 2008
Grüber C, Keil T, Kulig M, Roll S, Wahn U, Wahn V,MAS-90 Study Group. History of respiratory infections inthe first 12 yr among children from a birth cohort. Pediatric
Allergy and Immunology 2008;19(6):505–12. [PUBMED:18167154]
Hament 1999
Hament JM, Kimpen JL, Fleer A, Wolfs TF. Respiratoryviral infection predisposing for bacterial disease: a concisereview. FEMS Immunology and Medical Microbiology 1999;26(3-4):189–95. [MEDLINE: 10575129]
Haskins 1986
Haskins R, Kotch J. Day care and illness: evidence, costs,and public policy. Pediatrics 1986;77(6 Pt 2):951–82.[MEDLINE: 3012455]
Heikkinen 1998
Heikkinen T, Ruohola A, Ruuskanen O, Waris M,Uhari M, Hammarström L. Intranasally administeredimmunoglobulin for the prevention of rhinitis in children.Pediatric Infectious Diseases Journal 1998;17(5):367–72.[MEDLINE: 9613647]
Heikkinen 1999
Heikkinen T, Thint M, Chonmaitree T. Prevalence ofvarious respiratory viruses in the middle ear during acuteotitis media. New England Journal of Medicine 1999;340
(4):260–4. [MEDLINE: 9920949]
Hemila 1997
Hemila H. Vitamin C intake and susceptibility to thecommon cold. British Journal of Nutrition 1997;77(1):59–72. [MEDLINE: 9059230]
Hemilä 2010
Hemilä H, Chalker E, Douglas B. Vitamin C for preventingand treating the common cold. Cochrane Database
of Systematic Reviews 2010, Issue 3. [DOI: 10.1002/14651858.CD000980.pub3]
Hemmi 2002
Hemmi H, Kaisho T, Takeuchi O, Sato S, Sanjo H,Hoshino K, et al. Small anti-viral compounds activateimmune cells via the TLR7 MyD88-dependent signallingpathway. Nature Immunology 2002;3:196–200.
Henderson 1982
Henderson FW, Collier AM, Sanyal MA, Watkins JM,Fairclough DL, Clyde WA Jr, et al. A longitudinal studyof respiratory viruses and bacteria in the etiology of acuteotitis media with effusion. New England Journal of Medicine
1982;306(23):1377–83. [MEDLINE: 6281639]
Higgins 2003
Higgins JP, Thompson SG, Deeks JJ, Altman DG.Measuring inconsistency in meta-analyses. BMJ 2003;327:557–60.
Higgins 2011
Higgins JPT, Green S (editors). Cochrane Handbook for
Systematic Reviews of Interventions Version 5.1.0 [updatedMarch 2011]. The Cochrane Collaboration, 2011. .Available from www.cochrane-handbook.org 2011.
Hoffmann 1999
Hoffmann JA, Kafatos FC, Janeway CA, Ezekowitz RA.Phylogenetic perspectives in innate immunity. Science 1999;284:1313–8.
Hsu 2009
Hsu HE, Shutt KA, Moore MR, Beall BW, Bennett NM,Craig AS, et al. Effect of pneumococcal conjugate vaccineon pneumococcal meningitis. New England Journal of
Medicine 2009;360(3):244–56. [PUBMED: 19144940]
Huang 2009
Huang SS, Hinrichsen VL, Stevenson AE, Rifas-ShimanSL, Kleinman K, Pelton SI, et al. Continued impact ofpneumococcal conjugate vaccine on carriage in youngchildren. Pediatrics 2009;124(1):e1–11. [PUBMED:19564254]
Jara-Perez 2000
Jara-Perez JV, Berber A. Primary prevention of acuterespiratory tract infections in children using a bacterialimmunostimulant: a double-masked, placebo-controlledclinical trial. Clinical Therapeutics 2000;22:748–59.
659Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
Jefferson 2001
Jefferson TO, Tyrrell D. Antivirals for the common cold.Cochrane Database of Systematic Reviews 2001, Issue 3.[DOI: 10.1002/14651858.CD002743.pub2]
Jefferson 2009
Jefferson T, Del Mar C, Dooley L, Ferroni E, Al-AnsaryLA, Bawazeer GA, et al. Physical interventions to interruptor reduce the spread of respiratory viruses: systematicreview. BMJ 2009;339(b3675. doi):10.1136/bmj.b3675.[PUBMED: 19773323]
Jin 1993
Jin C, MacKay-Rossignol A. Effects of passive smoking onrespiratory illness from birth to age eighteen months, inShanghai, People’s Republic of China. Journal of Pediatrics
1993;123(4):553–8. [MEDLINE: 8410506]
Krieg 2003
Krieg 2003. CpG motifs: the active ingredient in bacterialextracts?. Nature Medicine 2003;9(7):831–5. [PUBMED:12835699]
Lee 2005
Lee T, Jordan NN, Sanchez JL, Gaydos JC. Selectednonvaccine interventions to prevent infectious acuterespiratory disease. American Journal of Preventive Medicine
2005;28(3):305–16. [PUBMED: 15766621]
Lefebvre 2009
Lefebvre C, Manheimer E, Glanville J. Chapter 6:Searching for studies. In: Higgins JPT, Green S editor(s).Cochrane Handbook for Systematic Reviews of Interventions.
Version 5.0.2 (updated September 2009). The Cochrane
Collaboration. Available from www.cochrane-handbook.org.Wiley, 2009.
Mahe 1999
Mahe C, Chevret S. Estimation of the treatment effect ina clinical trial when recurrent events define the endpoint.Statistics in Medicine 1999;18(14):1821–9.
Mera 2009
Mera RM, Miller LA, Amrine-Madsen H, Sahm DF.The impact of the pneumococcal conjugate vaccine onantimicrobial resistance in the United States since 1996:evidence for a significant rebound by 2007 in many classesof antibiotics. Microbial Drug Resistance 2009;15(4):261–8.[PUBMED: 19857132]
Moher 2001
Moher D, Schulz KF, Altman D. The CONSORTstatement: revised recommendations for improving thequality of reports of parallel-group randomized trials. JAMA
2001;285(15):1987–91.
Molinari 2007
Molinari NA, Ortega-Sanchez IR, Messonnier ML,Thompson WW, Wortley PM, Weintraub E, et al. Theannual impact of seasonal influenza in the US: measuringdisease burden and costs. Vaccine 2007;25(7):5086–96.[PUBMED: 17544181]
Monto 1974
Monto AS, Ulman BM. Acute respiratory illness in anAmerican community. The Tecumseh study. JAMA 1974;227:164–9.
Monto 1993
Monto AS, Sullivan KM. Acute respiratory illness inthe community. Frequency of illness and the agentsinvolved. Epidemiology and Infection 1993;110(1):145–60.[MEDLINE: 8432318]
Monto 2002
Monto AS. Epidemiology of viral respiratory infections.American Journal of Medicine 2002;112(Suppl 6A):4–12.
Nikolova 2009
Nikolova M, Stankulova D, Taskov H, Nenkov P, MaximovV, Petrunov B. Polybacterial immunomodulator respivaxrestores the inductive function of innate immunity inpatients with recurrent respiratory infections. International
Immunopharmacology 2009;9(4):425–32. [PUBMED:19186221]
Nydahl-Persson 1995
Nydahl-Persson K, Petterson A, Fasth A. A prospective,double-blind, placebo-controlled trial of i.v.immunoglobulin and trimethoprim-sulfamethoxazole inchildren with recurrent respiratory tract infections. Acta
Paediatrica 1995;84(9):1007–9. [MEDLINE: 8652950]
Passali 1994
Passali D, Calearo C, Conticello S, a multicentertrial group. Pidotimod in the management ofrecurrent pharyngotonsillar infections in childhood.Arzneimittelforschung 1994;44(12A):1511–6. [MEDLINE:7857354]
RevMan 2008
The Nordic Cochrane Centre. The Cochrane Collaboration.Review Manager (RevMan). Copenhagen: The NordicCochrane Centre. The Cochrane Collaboration, 2008.
Rhodes 1995
Rhodes J, Chen H, Hall SR, Beesley JE, Jenkins DC,Collins P, et al. Therapeutic potentiation of the immunesystem by costimulatory Schiff-base-forming drugs. Nature
1995;377:71–5.
Rovers 2006
Rovers MM, Balemans WA, Sanders EA, van der EntCK, Zielhuis GA, Schilder AG. Persistence of upperrespiratory tract infections in a cohort followed fromchildhood to adulthood. Family Practice 2006;23(3):286–90. [PUBMED: 16517546]
Sazawal 1998
Sazawal S, Black RE, Jalla S, Mazumdar S, Sinha A, BhanMK. Zinc supplementation reduces the incidence ofacute lower respiratory infections in infants and preschoolchildren: a double-blind, controlled trial. Pediatrics 1998;102(1 Pt 1):1–5. [MEDLINE: 9651405]
Schaad 2010
Schaad UB. OM-85 BV, an immunostimulant in pediatricrecurrent respiratory tract infections: a systematic review.
660Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Evid.-Based Child Health 7:2: 629–717 (2012)
World Journal Of Pediatrics 2010;6(1):5–12. [PUBMED:20143206]
Schnare 2001
Schnare M, Barton GM, Holt AC, Takeda K, Akira S,Medzhitov R. Toll-like receptors control activation ofadaptive immune responses. Nature Immunology 2001;2:947–50.
Schwartz 1994
Schwartz B, Giebink GS, Henderson FW, ReichlerMR, Jereb J, Collet JP. Respiratory infections in daycare. Pediatrics 1994;94(6 Pt 2):1018–20. [MEDLINE:7971043]
Selwyn 1990
Selwyn BJ. The epidemiology of acute respiratory tractinfection in young children: comparison of findings fromseveral developing countries. Reviews of Infectious Disease
1990;12(Suppl 8):870–88. [MEDLINE: 2270410]
Steurer-Stey 2007
Steurer-Stey C, Lagler L, Straub DA, Steurer J, BachmannLM. Oral purified bacterial extracts in acute respiratorytract infections in childhood: a systematic quantitativereview. European Journal of Pediatrics 2007;166(4):365–76.[PUBMED: 17115184]
Symoens 1978
Symoens J, Veys E, Mielants M, Pinals R. Adverse reactionsto levamisole. Cancer Treatment Reports 1978;62(11):1721–30.
Takeuchi 2001
Takeuchi O, Akira S. Toll-like receptors; their physiologicalrole and signal transduction system. International
Immunopharmacology 2001;1:625–35.
Uhari 1998
Uhari M, Kontiokari T, Niemelä M. A novel use of xylitolsugar in preventing acute otitis media. Pediatrics 1998;102
(4 Pt 1):879–84. [MEDLINE: 9755259]
Valleron 1992
Valleron AJ, Grimfield A. Evaluation of clinical trialsof immunomodulators for prevention of recurrentrespiratory infections in children. Developments in Biological
Standardization 1992;77:149–58. [MEDLINE: 1426656]
WHO 1998
WHO. Acute respiratory infections: the forgottenpandemic. Bulletin of the World Health Organization 1998;76(1):101–3. [MEDLINE: 9615503]
WHO 2005
World Health Organization. Fact Sheet 113. Bovinespongiform encephalopathy. http://www.who.int/mediacentre/factsheets/fs113/en/print.html (accessed 20July 2005) 2005.
Williams 2002
Williams BG, Gouws E, Boschi-Pinto C, Bryce J, Dye C.Estimates of world-wide distribution of child deaths fromacute respiratory infections. Lancet Infectious Diseases 2002;2:25–32.
Wolsko 2005
Wolsko PM, Solondz DK, Phillips RS, Schachter SC,Eisenberg DM. Lack of herbal supplement characterizationin published randomized controlled trials. American
Journal of Medicine 2005;118(10):1087–93. [PUBMED:16194636]
Wright 1989
Wright AL, Holberg CJ, Martinez FD, Morgan WJ, TaussigLM. Breast feeding and lower respiratory tract illnessin the first year of life. BMJ 1989;299(6705):946–9.[MEDLINE: 2508946]
Xu 2009
Xu N, Zhou W, Li S, Zhou G, Zhang N, LiangJ. Clinical and MRI characteristics of levamisole-induced leukoencephalopathy in 16 patients. Journal of
Neuroimaging 2009;19(4):326–31. [PUBMED: 19187474]
Yamshchikov 2009
Yamshchikov AV, Desai NS, Blumberg HM, Ziegler TR,Tangpricha V. Vitamin D for treatment and preventionof infectious diseases: a systematic review of randomizedcontrolled trials. Endocrine Practice 2009;15(5):438–49.[PUBMED: 19491064]
References to other published versions of this review
Del-Rio-Navarro 2006
Del-Rio-Navarro BE, Espinosa Rosales F, Flenady V,Sienra-Monge JJL. Immunostimulants for preventingrespiratory tract infection in children. Cochrane Database
of Systematic Reviews 2006, Issue 2. [DOI: 10.1002/14651858.CD004974.pub2]
∗ Indicates the major publication for the study
661Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
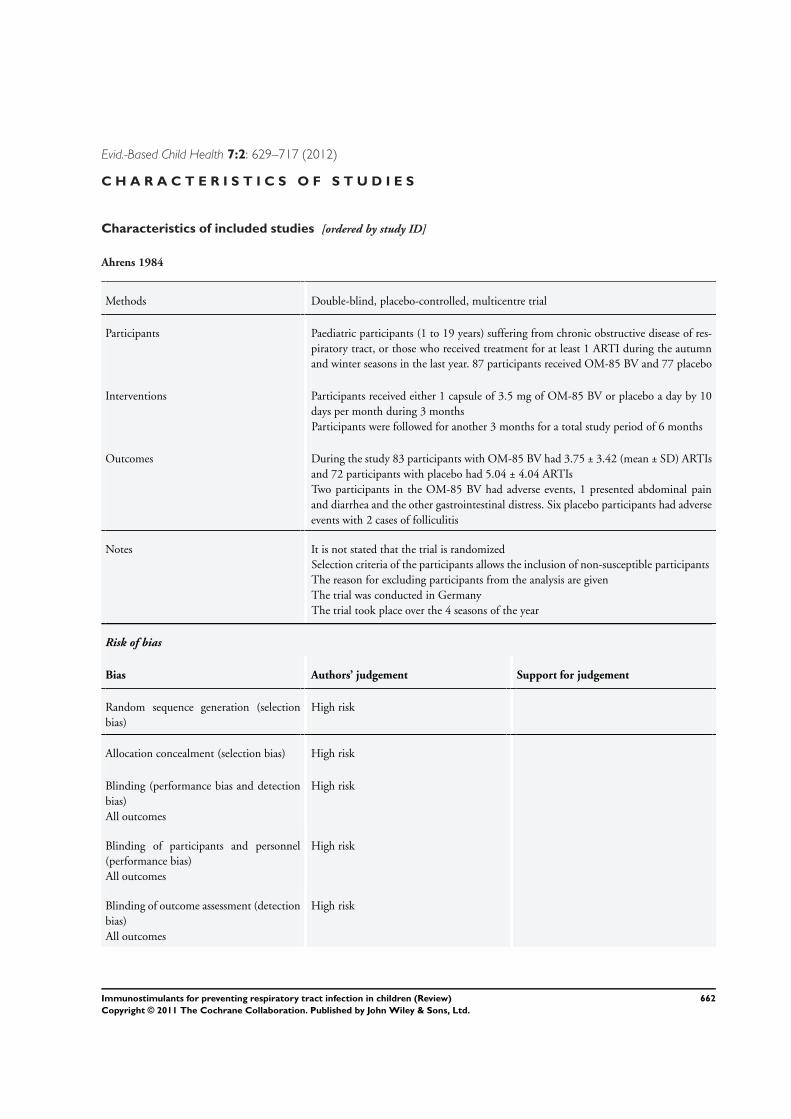
Evid.-Based Child Health 7:2: 629–717 (2012)
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Ahrens 1984
Methods Double-blind, placebo-controlled, multicentre trial
Participants Paediatric participants (1 to 19 years) suffering from chronic obstructive disease of res-piratory tract, or those who received treatment for at least 1 ARTI during the autumnand winter seasons in the last year. 87 participants received OM-85 BV and 77 placebo
Interventions Participants received either 1 capsule of 3.5 mg of OM-85 BV or placebo a day by 10days per month during 3 monthsParticipants were followed for another 3 months for a total study period of 6 months
Outcomes During the study 83 participants with OM-85 BV had 3.75 ± 3.42 (mean ± SD) ARTIsand 72 participants with placebo had 5.04 ± 4.04 ARTIsTwo participants in the OM-85 BV had adverse events, 1 presented abdominal painand diarrhea and the other gastrointestinal distress. Six placebo participants had adverseevents with 2 cases of folliculitis
Notes It is not stated that the trial is randomizedSelection criteria of the participants allows the inclusion of non-susceptible participantsThe reason for excluding participants from the analysis are givenThe trial was conducted in GermanyThe trial took place over the 4 seasons of the year
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
High risk
Allocation concealment (selection bias) High risk
Blinding (performance bias and detectionbias)All outcomes
High risk
Blinding of participants and personnel(performance bias)All outcomes
High risk
Blinding of outcome assessment (detectionbias)All outcomes
High risk
662Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
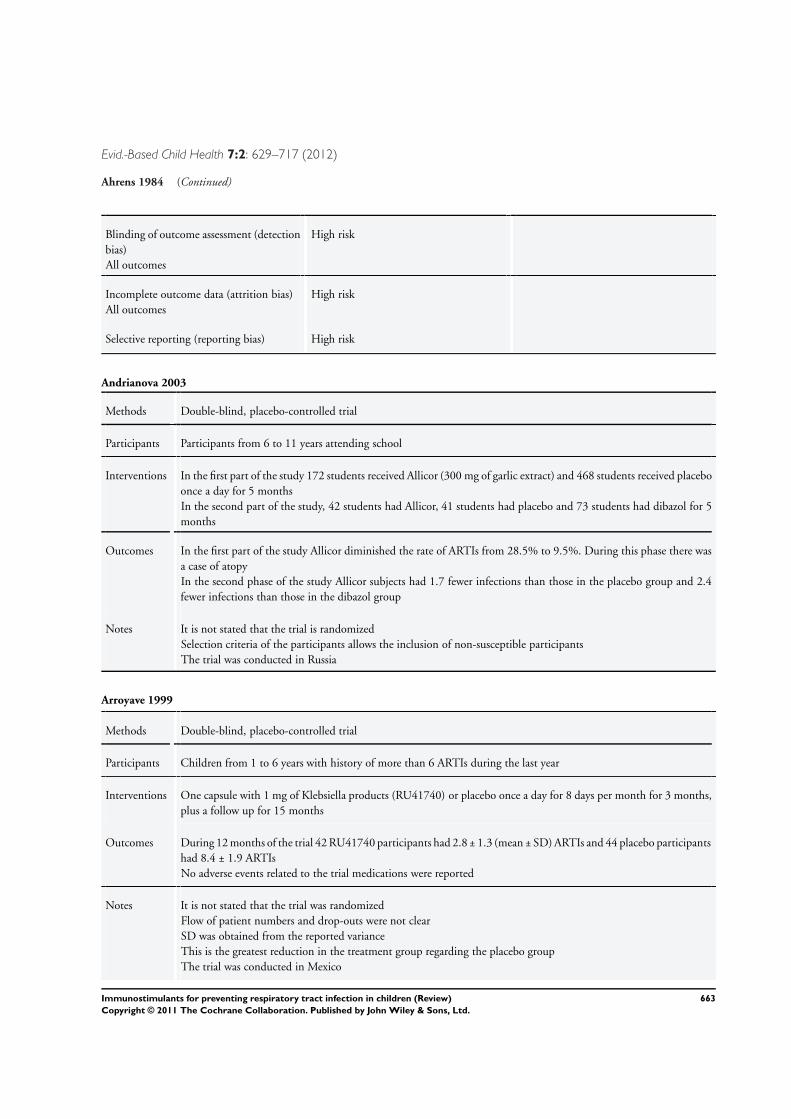
Evid.-Based Child Health 7:2: 629–717 (2012)
Ahrens 1984 (Continued)
Blinding of outcome assessment (detectionbias)All outcomes
High risk
Incomplete outcome data (attrition bias)All outcomes
High risk
Selective reporting (reporting bias) High risk
Andrianova 2003
Methods Double-blind, placebo-controlled trial
Participants Participants from 6 to 11 years attending school
Interventions In the first part of the study 172 students received Allicor (300 mg of garlic extract) and 468 students received placeboonce a day for 5 monthsIn the second part of the study, 42 students had Allicor, 41 students had placebo and 73 students had dibazol for 5months
Outcomes In the first part of the study Allicor diminished the rate of ARTIs from 28.5% to 9.5%. During this phase there wasa case of atopyIn the second phase of the study Allicor subjects had 1.7 fewer infections than those in the placebo group and 2.4fewer infections than those in the dibazol group
Notes It is not stated that the trial is randomizedSelection criteria of the participants allows the inclusion of non-susceptible participantsThe trial was conducted in Russia
Arroyave 1999
Methods Double-blind, placebo-controlled trial
Participants Children from 1 to 6 years with history of more than 6 ARTIs during the last year
Interventions One capsule with 1 mg of Klebsiella products (RU41740) or placebo once a day for 8 days per month for 3 months,plus a follow up for 15 months
Outcomes During 12 months of the trial 42 RU41740 participants had 2.8 ± 1.3 (mean ± SD) ARTIs and 44 placebo participantshad 8.4 ± 1.9 ARTIsNo adverse events related to the trial medications were reported
Notes It is not stated that the trial was randomizedFlow of patient numbers and drop-outs were not clearSD was obtained from the reported varianceThis is the greatest reduction in the treatment group regarding the placebo groupThe trial was conducted in Mexico
663Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
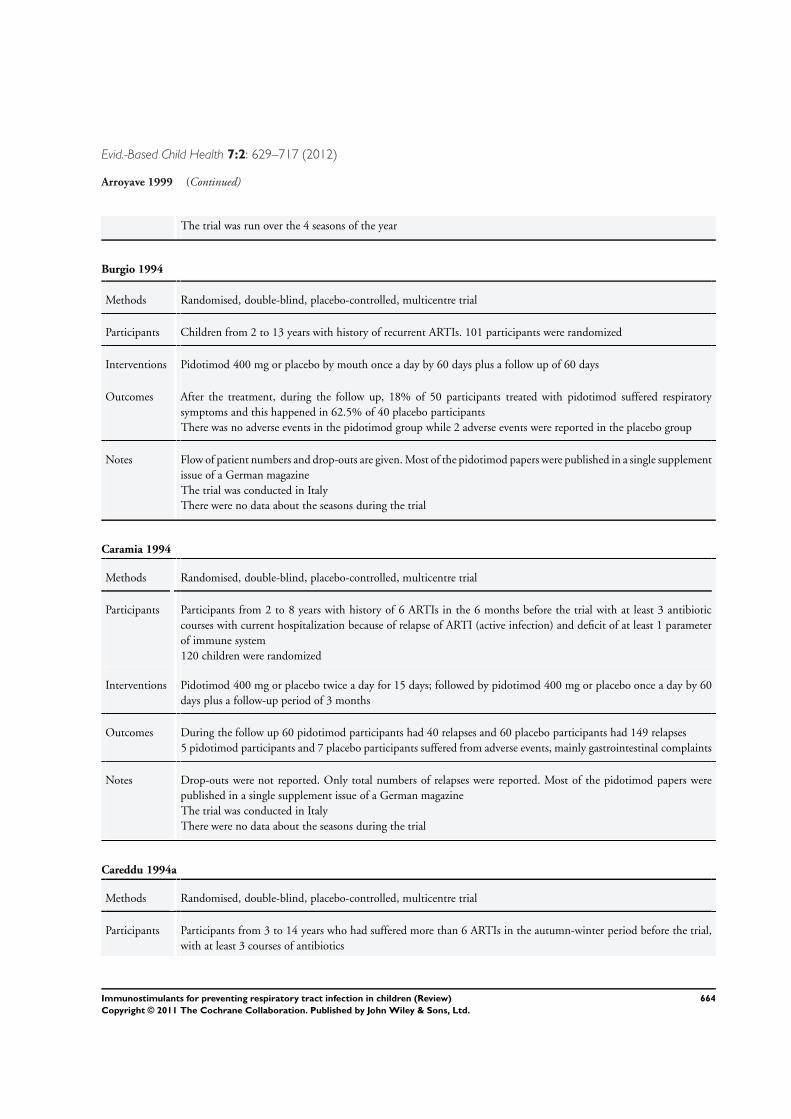
Evid.-Based Child Health 7:2: 629–717 (2012)
Arroyave 1999 (Continued)
The trial was run over the 4 seasons of the year
Burgio 1994
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Children from 2 to 13 years with history of recurrent ARTIs. 101 participants were randomized
Interventions Pidotimod 400 mg or placebo by mouth once a day by 60 days plus a follow up of 60 days
Outcomes After the treatment, during the follow up, 18% of 50 participants treated with pidotimod suffered respiratorysymptoms and this happened in 62.5% of 40 placebo participantsThere was no adverse events in the pidotimod group while 2 adverse events were reported in the placebo group
Notes Flow of patient numbers and drop-outs are given. Most of the pidotimod papers were published in a single supplementissue of a German magazineThe trial was conducted in ItalyThere were no data about the seasons during the trial
Caramia 1994
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Participants from 2 to 8 years with history of 6 ARTIs in the 6 months before the trial with at least 3 antibioticcourses with current hospitalization because of relapse of ARTI (active infection) and deficit of at least 1 parameterof immune system120 children were randomized
Interventions Pidotimod 400 mg or placebo twice a day for 15 days; followed by pidotimod 400 mg or placebo once a day by 60days plus a follow-up period of 3 months
Outcomes During the follow up 60 pidotimod participants had 40 relapses and 60 placebo participants had 149 relapses5 pidotimod participants and 7 placebo participants suffered from adverse events, mainly gastrointestinal complaints
Notes Drop-outs were not reported. Only total numbers of relapses were reported. Most of the pidotimod papers werepublished in a single supplement issue of a German magazineThe trial was conducted in ItalyThere were no data about the seasons during the trial
Careddu 1994a
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Participants from 3 to 14 years who had suffered more than 6 ARTIs in the autumn-winter period before the trial,with at least 3 courses of antibiotics
664Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
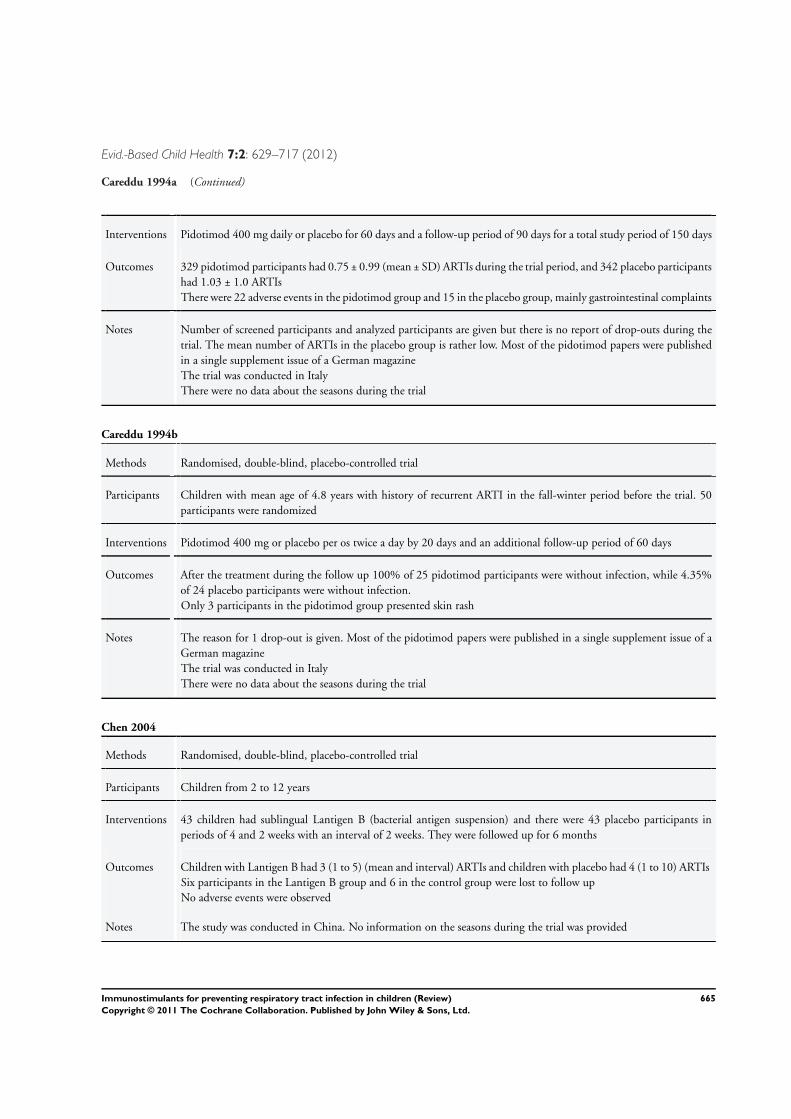
Evid.-Based Child Health 7:2: 629–717 (2012)
Careddu 1994a (Continued)
Interventions Pidotimod 400 mg daily or placebo for 60 days and a follow-up period of 90 days for a total study period of 150 days
Outcomes 329 pidotimod participants had 0.75 ± 0.99 (mean ± SD) ARTIs during the trial period, and 342 placebo participantshad 1.03 ± 1.0 ARTIsThere were 22 adverse events in the pidotimod group and 15 in the placebo group, mainly gastrointestinal complaints
Notes Number of screened participants and analyzed participants are given but there is no report of drop-outs during thetrial. The mean number of ARTIs in the placebo group is rather low. Most of the pidotimod papers were publishedin a single supplement issue of a German magazineThe trial was conducted in ItalyThere were no data about the seasons during the trial
Careddu 1994b
Methods Randomised, double-blind, placebo-controlled trial
Participants Children with mean age of 4.8 years with history of recurrent ARTI in the fall-winter period before the trial. 50participants were randomized
Interventions Pidotimod 400 mg or placebo per os twice a day by 20 days and an additional follow-up period of 60 days
Outcomes After the treatment during the follow up 100% of 25 pidotimod participants were without infection, while 4.35%of 24 placebo participants were without infection.Only 3 participants in the pidotimod group presented skin rash
Notes The reason for 1 drop-out is given. Most of the pidotimod papers were published in a single supplement issue of aGerman magazineThe trial was conducted in ItalyThere were no data about the seasons during the trial
Chen 2004
Methods Randomised, double-blind, placebo-controlled trial
Participants Children from 2 to 12 years
Interventions 43 children had sublingual Lantigen B (bacterial antigen suspension) and there were 43 placebo participants inperiods of 4 and 2 weeks with an interval of 2 weeks. They were followed up for 6 months
Outcomes Children with Lantigen B had 3 (1 to 5) (mean and interval) ARTIs and children with placebo had 4 (1 to 10) ARTIsSix participants in the Lantigen B group and 6 in the control group were lost to follow upNo adverse events were observed
Notes The study was conducted in China. No information on the seasons during the trial was provided
665Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
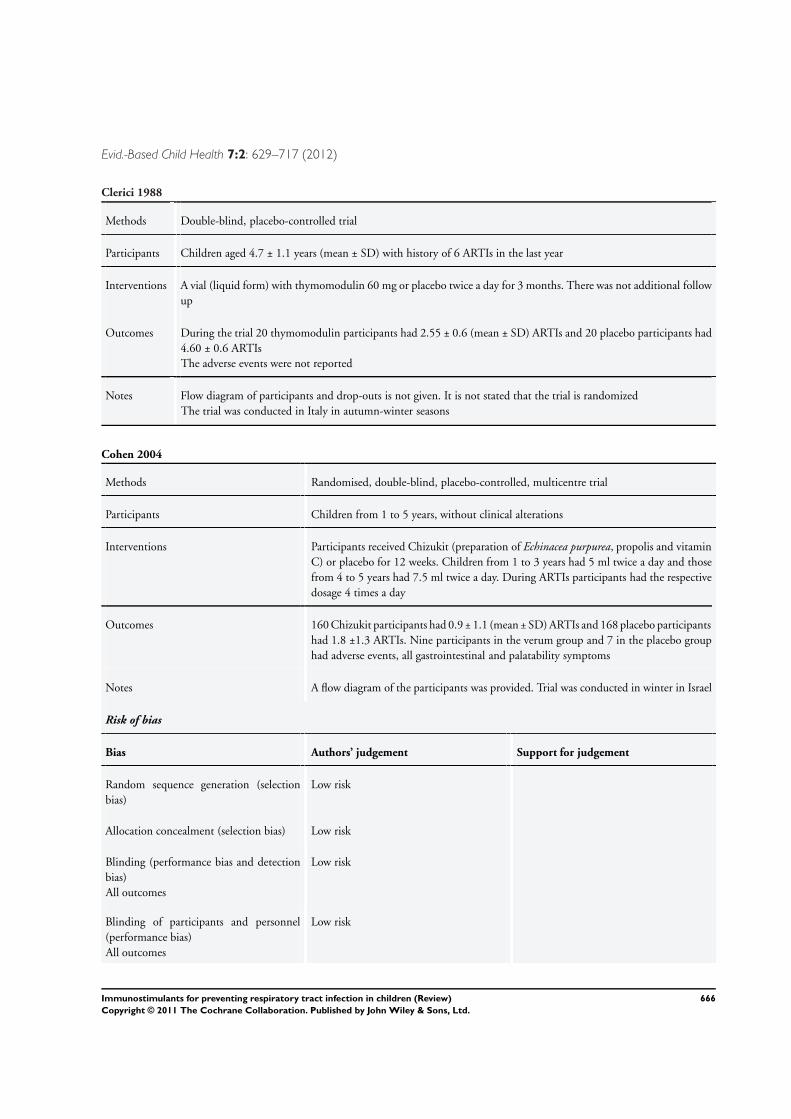
Evid.-Based Child Health 7:2: 629–717 (2012)
Clerici 1988
Methods Double-blind, placebo-controlled trial
Participants Children aged 4.7 ± 1.1 years (mean ± SD) with history of 6 ARTIs in the last year
Interventions A vial (liquid form) with thymomodulin 60 mg or placebo twice a day for 3 months. There was not additional followup
Outcomes During the trial 20 thymomodulin participants had 2.55 ± 0.6 (mean ± SD) ARTIs and 20 placebo participants had4.60 ± 0.6 ARTIsThe adverse events were not reported
Notes Flow diagram of participants and drop-outs is not given. It is not stated that the trial is randomizedThe trial was conducted in Italy in autumn-winter seasons
Cohen 2004
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Children from 1 to 5 years, without clinical alterations
Interventions Participants received Chizukit (preparation of Echinacea purpurea, propolis and vitaminC) or placebo for 12 weeks. Children from 1 to 3 years had 5 ml twice a day and thosefrom 4 to 5 years had 7.5 ml twice a day. During ARTIs participants had the respectivedosage 4 times a day
Outcomes 160 Chizukit participants had 0.9 ± 1.1 (mean ± SD) ARTIs and 168 placebo participantshad 1.8 ±1.3 ARTIs. Nine participants in the verum group and 7 in the placebo grouphad adverse events, all gastrointestinal and palatability symptoms
Notes A flow diagram of the participants was provided. Trial was conducted in winter in Israel
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk
Allocation concealment (selection bias) Low risk
Blinding (performance bias and detectionbias)All outcomes
Low risk
Blinding of participants and personnel(performance bias)All outcomes
Low risk
666Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
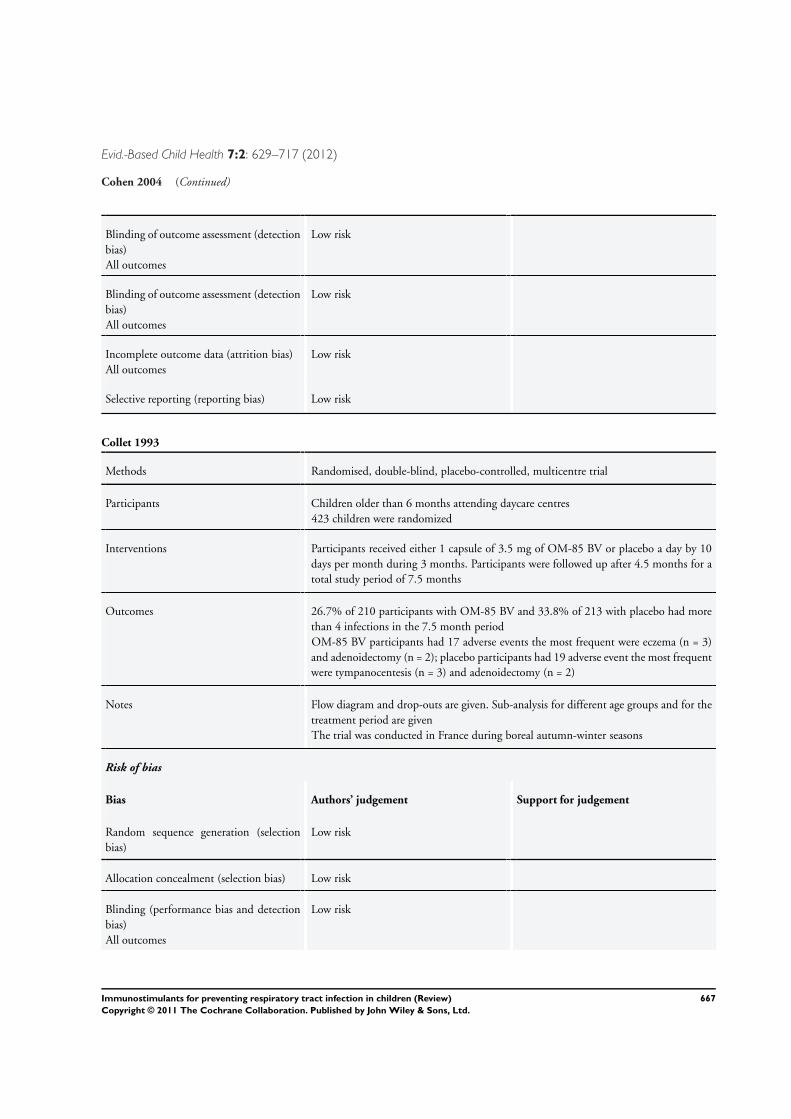
Evid.-Based Child Health 7:2: 629–717 (2012)
Cohen 2004 (Continued)
Blinding of outcome assessment (detectionbias)All outcomes
Low risk
Blinding of outcome assessment (detectionbias)All outcomes
Low risk
Incomplete outcome data (attrition bias)All outcomes
Low risk
Selective reporting (reporting bias) Low risk
Collet 1993
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Children older than 6 months attending daycare centres423 children were randomized
Interventions Participants received either 1 capsule of 3.5 mg of OM-85 BV or placebo a day by 10days per month during 3 months. Participants were followed up after 4.5 months for atotal study period of 7.5 months
Outcomes 26.7% of 210 participants with OM-85 BV and 33.8% of 213 with placebo had morethan 4 infections in the 7.5 month periodOM-85 BV participants had 17 adverse events the most frequent were eczema (n = 3)and adenoidectomy (n = 2); placebo participants had 19 adverse event the most frequentwere tympanocentesis (n = 3) and adenoidectomy (n = 2)
Notes Flow diagram and drop-outs are given. Sub-analysis for different age groups and for thetreatment period are givenThe trial was conducted in France during boreal autumn-winter seasons
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk
Allocation concealment (selection bias) Low risk
Blinding (performance bias and detectionbias)All outcomes
Low risk
667Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
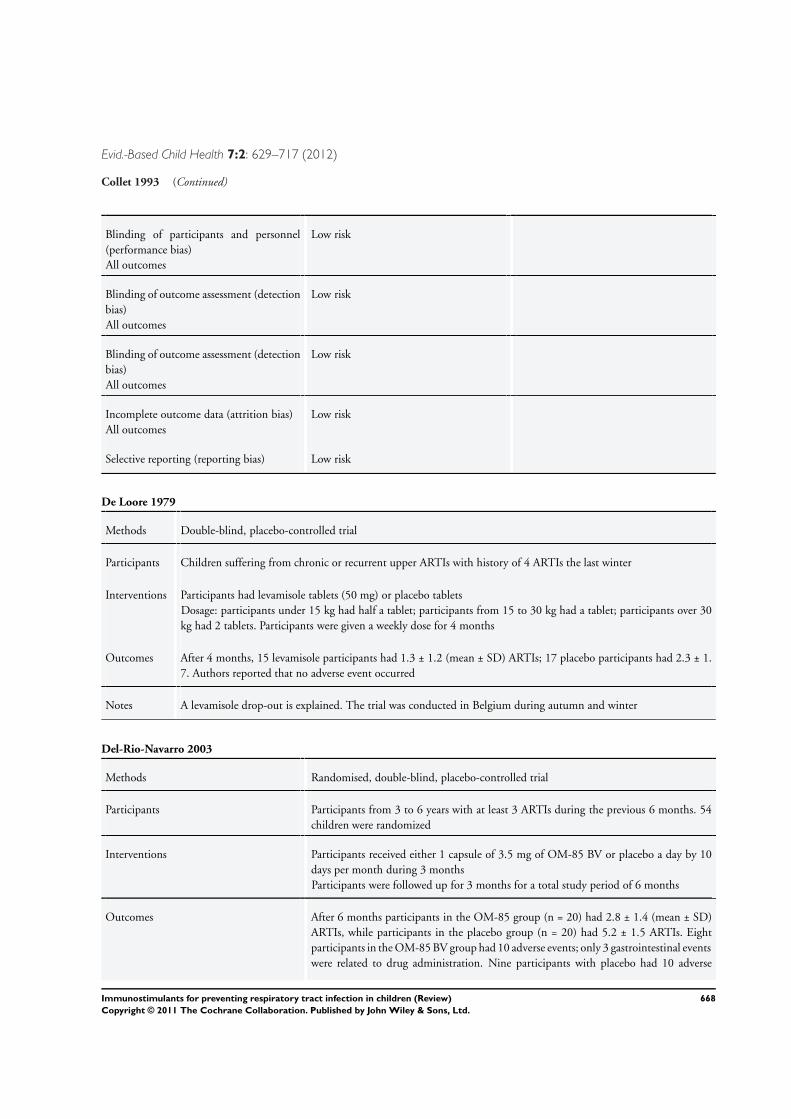
Evid.-Based Child Health 7:2: 629–717 (2012)
Collet 1993 (Continued)
Blinding of participants and personnel(performance bias)All outcomes
Low risk
Blinding of outcome assessment (detectionbias)All outcomes
Low risk
Blinding of outcome assessment (detectionbias)All outcomes
Low risk
Incomplete outcome data (attrition bias)All outcomes
Low risk
Selective reporting (reporting bias) Low risk
De Loore 1979
Methods Double-blind, placebo-controlled trial
Participants Children suffering from chronic or recurrent upper ARTIs with history of 4 ARTIs the last winter
Interventions Participants had levamisole tablets (50 mg) or placebo tabletsDosage: participants under 15 kg had half a tablet; participants from 15 to 30 kg had a tablet; participants over 30kg had 2 tablets. Participants were given a weekly dose for 4 months
Outcomes After 4 months, 15 levamisole participants had 1.3 ± 1.2 (mean ± SD) ARTIs; 17 placebo participants had 2.3 ± 1.7. Authors reported that no adverse event occurred
Notes A levamisole drop-out is explained. The trial was conducted in Belgium during autumn and winter
Del-Rio-Navarro 2003
Methods Randomised, double-blind, placebo-controlled trial
Participants Participants from 3 to 6 years with at least 3 ARTIs during the previous 6 months. 54children were randomized
Interventions Participants received either 1 capsule of 3.5 mg of OM-85 BV or placebo a day by 10days per month during 3 monthsParticipants were followed up for 3 months for a total study period of 6 months
Outcomes After 6 months participants in the OM-85 group (n = 20) had 2.8 ± 1.4 (mean ± SD)ARTIs, while participants in the placebo group (n = 20) had 5.2 ± 1.5 ARTIs. Eightparticipants in the OM-85 BV group had 10 adverse events; only 3 gastrointestinal eventswere related to drug administration. Nine participants with placebo had 10 adverse
668Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
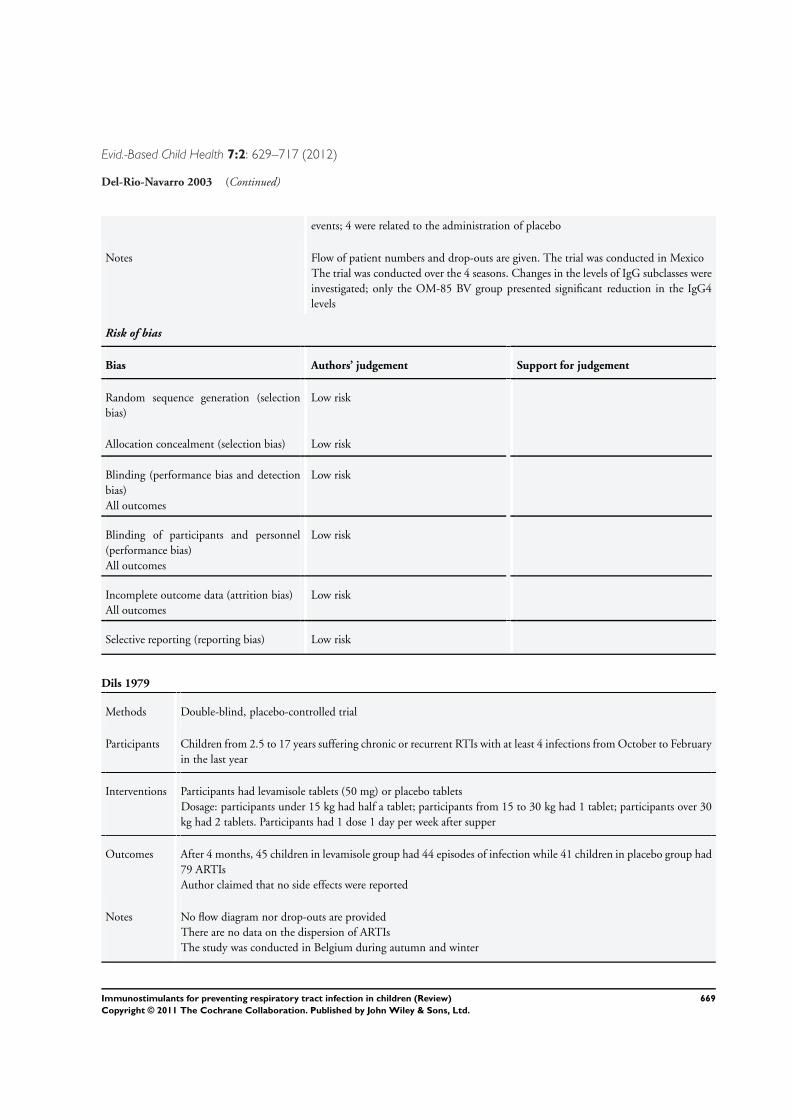
Evid.-Based Child Health 7:2: 629–717 (2012)
Del-Rio-Navarro 2003 (Continued)
events; 4 were related to the administration of placebo
Notes Flow of patient numbers and drop-outs are given. The trial was conducted in MexicoThe trial was conducted over the 4 seasons. Changes in the levels of IgG subclasses wereinvestigated; only the OM-85 BV group presented significant reduction in the IgG4levels
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk
Allocation concealment (selection bias) Low risk
Blinding (performance bias and detectionbias)All outcomes
Low risk
Blinding of participants and personnel(performance bias)All outcomes
Low risk
Incomplete outcome data (attrition bias)All outcomes
Low risk
Selective reporting (reporting bias) Low risk
Dils 1979
Methods Double-blind, placebo-controlled trial
Participants Children from 2.5 to 17 years suffering chronic or recurrent RTIs with at least 4 infections from October to Februaryin the last year
Interventions Participants had levamisole tablets (50 mg) or placebo tabletsDosage: participants under 15 kg had half a tablet; participants from 15 to 30 kg had 1 tablet; participants over 30kg had 2 tablets. Participants had 1 dose 1 day per week after supper
Outcomes After 4 months, 45 children in levamisole group had 44 episodes of infection while 41 children in placebo group had79 ARTIsAuthor claimed that no side effects were reported
Notes No flow diagram nor drop-outs are providedThere are no data on the dispersion of ARTIsThe study was conducted in Belgium during autumn and winter
669Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Evid.-Based Child Health 7:2: 629–717 (2012)
Fiocchi 1986
Methods Double-blind, placebo-controlled clinical trial
Participants Participants from 4 to 14 years with more than 6 ARTIs in the last fall-winter period with at least 3 antibiotic courses.16 participants were included
Interventions Thymomodulin 3 mg/kg/day or placebo by 3 months. There was no additional follow up
Outcomes During the 3-month period, 8 thymomodulin participants had 0.53 ± 0.11 (mean ± SD) ARTIs, and 8 placeboparticipants had 0.82 ± 0.12 ARTIsThe adverse events were not reported
Notes The sample size is clearly insufficientThe number of ARTIs in the placebo group was rather lowIt is not stated that the trial is randomizedThe trial was conducted in Italy during boreal autumn-winter seasons
Fiocchi 1988
Methods Randomised double-blind, placebo-controlled clinical trial
Participants Participants from 3 to 12 years with a clinical score more than 30 in a clinical scale for ARTIs
Interventions Participants received ribosomal extract spray (D53) or placebo, 1 puff in the nose and 1 in pharynx 3 times a dayby 2 weeks; this schedule was repeated another 2 times with intervals of 1 week between the puff administrations.Additionally participants had 1 subcutaneous injection in the weeks 2, 5 and 8Participants were followed up for 6 months
Outcomes After 6 months 30 participants in the D53 group had 36 upper ARTIs and 45 lower ARTIs, while 30 participantsin the placebo group had 43 upper ARTIs and 51 lower ARTIsAdverse events were not reported
Notes Flow of participants is not reported. The number of lower ARTIs is extremely high. Trial was conducted in Italyduring autumn-winter seasonsIt was not possible to identify this study in the Bellanti review
Fiocchi 1989
Methods Randomised, double-blind, placebo-controlled clinical trial
Participants Children from 2 to 15 years suffering recurrent ARTIs defined as 30 points in a clinical scale and more than 5 ARTIsin the last 6 months120 participants were included
Interventions Placebo or ribosomal extract spray (D53); 1 puff in each nostril plus 1 puff in the oropharyngeal cavity 3 times a dayaccording to the following schedule; 2 weeks treatment, 1 week washout and 1 week treatment in the first month;2 week treatment and 2 week washout in the second, third and fourth months. Total duration of the study was 4months
670Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
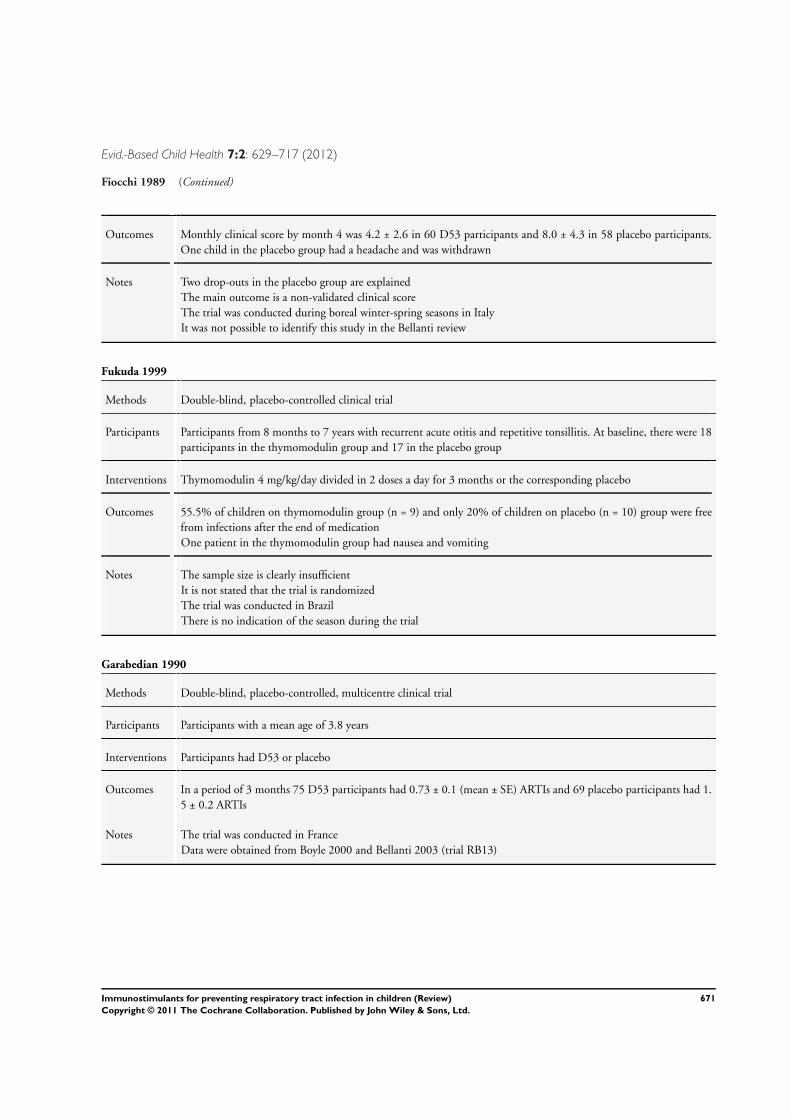
Evid.-Based Child Health 7:2: 629–717 (2012)
Fiocchi 1989 (Continued)
Outcomes Monthly clinical score by month 4 was 4.2 ± 2.6 in 60 D53 participants and 8.0 ± 4.3 in 58 placebo participants.One child in the placebo group had a headache and was withdrawn
Notes Two drop-outs in the placebo group are explainedThe main outcome is a non-validated clinical scoreThe trial was conducted during boreal winter-spring seasons in ItalyIt was not possible to identify this study in the Bellanti review
Fukuda 1999
Methods Double-blind, placebo-controlled clinical trial
Participants Participants from 8 months to 7 years with recurrent acute otitis and repetitive tonsillitis. At baseline, there were 18participants in the thymomodulin group and 17 in the placebo group
Interventions Thymomodulin 4 mg/kg/day divided in 2 doses a day for 3 months or the corresponding placebo
Outcomes 55.5% of children on thymomodulin group (n = 9) and only 20% of children on placebo (n = 10) group were freefrom infections after the end of medicationOne patient in the thymomodulin group had nausea and vomiting
Notes The sample size is clearly insufficientIt is not stated that the trial is randomizedThe trial was conducted in BrazilThere is no indication of the season during the trial
Garabedian 1990
Methods Double-blind, placebo-controlled, multicentre clinical trial
Participants Participants with a mean age of 3.8 years
Interventions Participants had D53 or placebo
Outcomes In a period of 3 months 75 D53 participants had 0.73 ± 0.1 (mean ± SE) ARTIs and 69 placebo participants had 1.5 ± 0.2 ARTIs
Notes The trial was conducted in FranceData were obtained from Boyle 2000 and Bellanti 2003 (trial RB13)
671Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
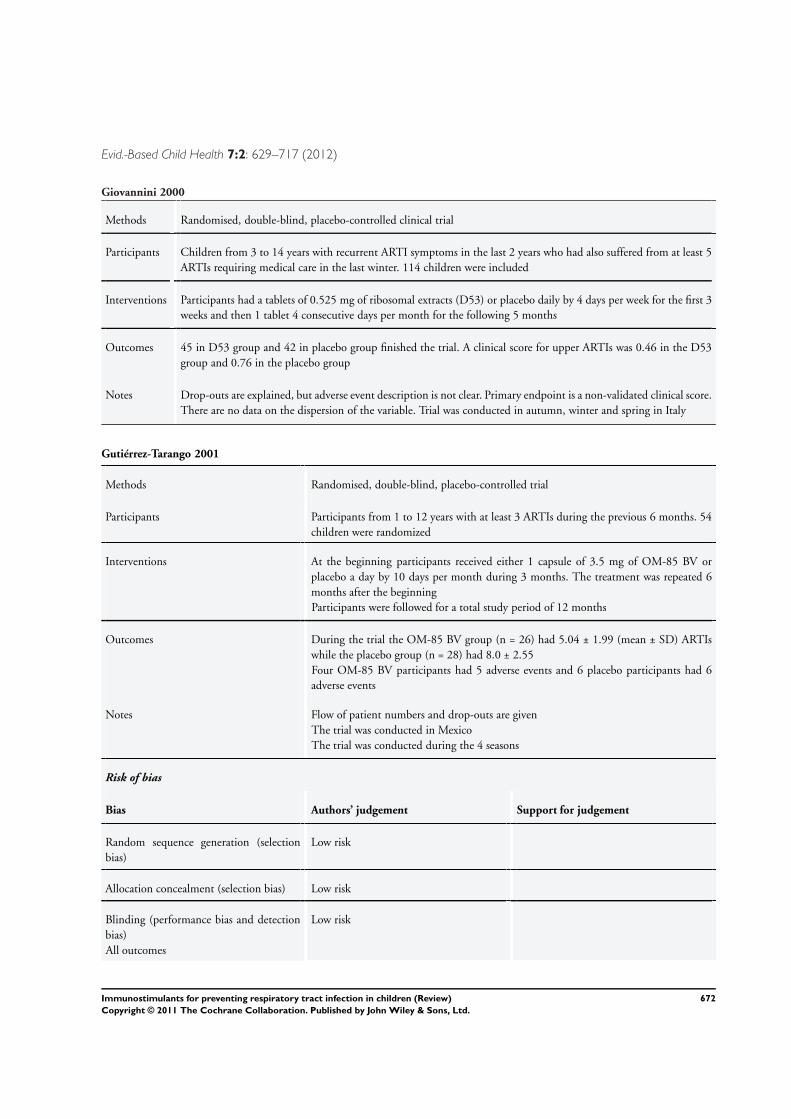
Evid.-Based Child Health 7:2: 629–717 (2012)
Giovannini 2000
Methods Randomised, double-blind, placebo-controlled clinical trial
Participants Children from 3 to 14 years with recurrent ARTI symptoms in the last 2 years who had also suffered from at least 5ARTIs requiring medical care in the last winter. 114 children were included
Interventions Participants had a tablets of 0.525 mg of ribosomal extracts (D53) or placebo daily by 4 days per week for the first 3weeks and then 1 tablet 4 consecutive days per month for the following 5 months
Outcomes 45 in D53 group and 42 in placebo group finished the trial. A clinical score for upper ARTIs was 0.46 in the D53group and 0.76 in the placebo group
Notes Drop-outs are explained, but adverse event description is not clear. Primary endpoint is a non-validated clinical score.There are no data on the dispersion of the variable. Trial was conducted in autumn, winter and spring in Italy
Gutiérrez-Tarango 2001
Methods Randomised, double-blind, placebo-controlled trial
Participants Participants from 1 to 12 years with at least 3 ARTIs during the previous 6 months. 54children were randomized
Interventions At the beginning participants received either 1 capsule of 3.5 mg of OM-85 BV orplacebo a day by 10 days per month during 3 months. The treatment was repeated 6months after the beginningParticipants were followed for a total study period of 12 months
Outcomes During the trial the OM-85 BV group (n = 26) had 5.04 ± 1.99 (mean ± SD) ARTIswhile the placebo group (n = 28) had 8.0 ± 2.55Four OM-85 BV participants had 5 adverse events and 6 placebo participants had 6adverse events
Notes Flow of patient numbers and drop-outs are givenThe trial was conducted in MexicoThe trial was conducted during the 4 seasons
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk
Allocation concealment (selection bias) Low risk
Blinding (performance bias and detectionbias)All outcomes
Low risk
672Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
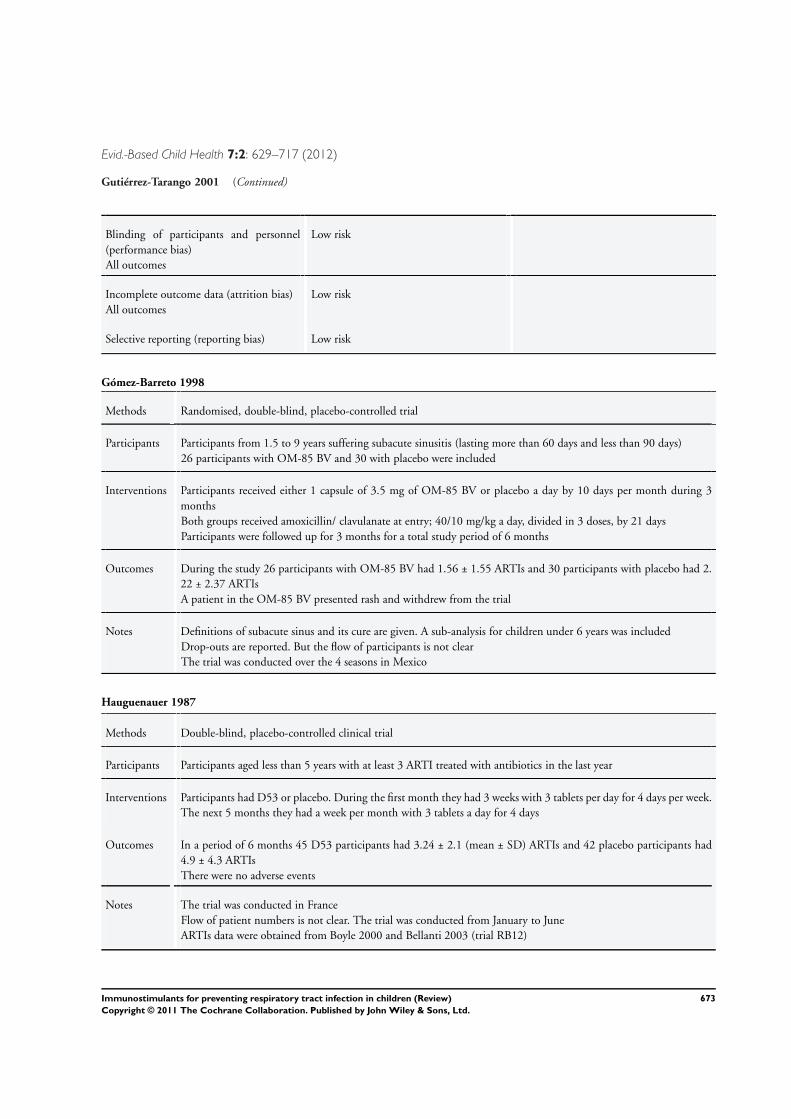
Evid.-Based Child Health 7:2: 629–717 (2012)
Gutiérrez-Tarango 2001 (Continued)
Blinding of participants and personnel(performance bias)All outcomes
Low risk
Incomplete outcome data (attrition bias)All outcomes
Low risk
Selective reporting (reporting bias) Low risk
Gómez-Barreto 1998
Methods Randomised, double-blind, placebo-controlled trial
Participants Participants from 1.5 to 9 years suffering subacute sinusitis (lasting more than 60 days and less than 90 days)26 participants with OM-85 BV and 30 with placebo were included
Interventions Participants received either 1 capsule of 3.5 mg of OM-85 BV or placebo a day by 10 days per month during 3monthsBoth groups received amoxicillin/ clavulanate at entry; 40/10 mg/kg a day, divided in 3 doses, by 21 daysParticipants were followed up for 3 months for a total study period of 6 months
Outcomes During the study 26 participants with OM-85 BV had 1.56 ± 1.55 ARTIs and 30 participants with placebo had 2.22 ± 2.37 ARTIsA patient in the OM-85 BV presented rash and withdrew from the trial
Notes Definitions of subacute sinus and its cure are given. A sub-analysis for children under 6 years was includedDrop-outs are reported. But the flow of participants is not clearThe trial was conducted over the 4 seasons in Mexico
Hauguenauer 1987
Methods Double-blind, placebo-controlled clinical trial
Participants Participants aged less than 5 years with at least 3 ARTI treated with antibiotics in the last year
Interventions Participants had D53 or placebo. During the first month they had 3 weeks with 3 tablets per day for 4 days per week.The next 5 months they had a week per month with 3 tablets a day for 4 days
Outcomes In a period of 6 months 45 D53 participants had 3.24 ± 2.1 (mean ± SD) ARTIs and 42 placebo participants had4.9 ± 4.3 ARTIsThere were no adverse events
Notes The trial was conducted in FranceFlow of patient numbers is not clear. The trial was conducted from January to JuneARTIs data were obtained from Boyle 2000 and Bellanti 2003 (trial RB12)
673Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
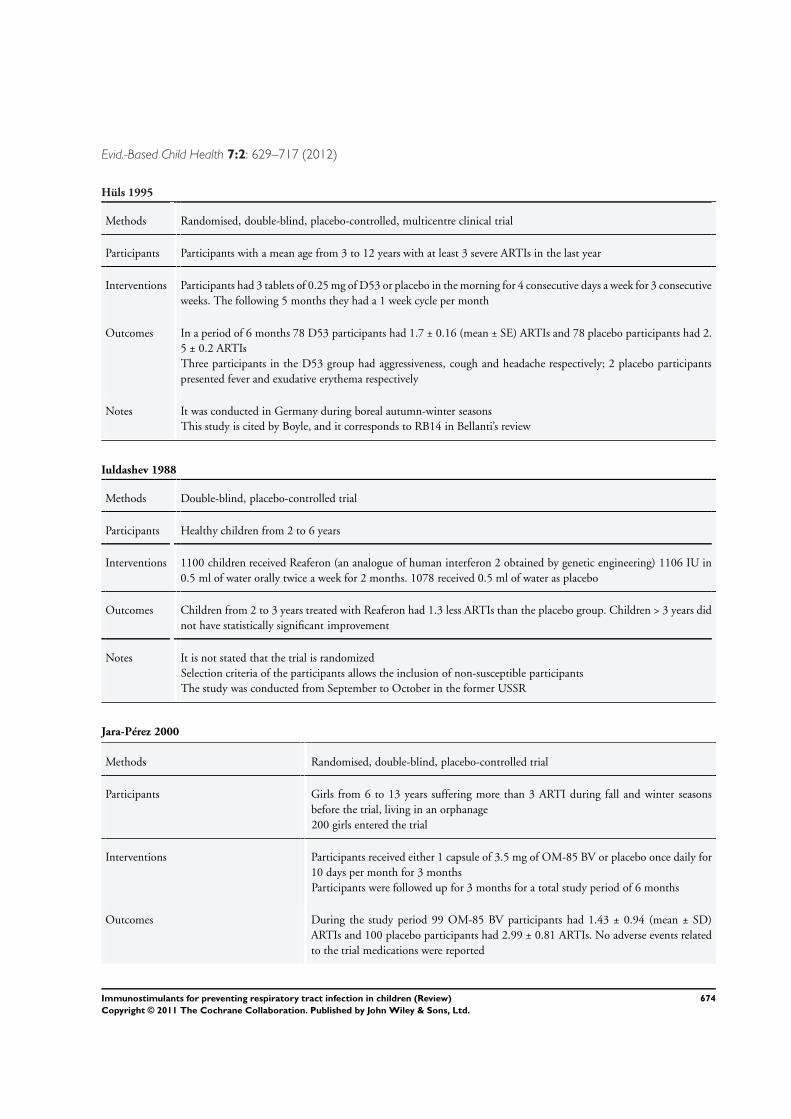
Evid.-Based Child Health 7:2: 629–717 (2012)
Hüls 1995
Methods Randomised, double-blind, placebo-controlled, multicentre clinical trial
Participants Participants with a mean age from 3 to 12 years with at least 3 severe ARTIs in the last year
Interventions Participants had 3 tablets of 0.25 mg of D53 or placebo in the morning for 4 consecutive days a week for 3 consecutiveweeks. The following 5 months they had a 1 week cycle per month
Outcomes In a period of 6 months 78 D53 participants had 1.7 ± 0.16 (mean ± SE) ARTIs and 78 placebo participants had 2.5 ± 0.2 ARTIsThree participants in the D53 group had aggressiveness, cough and headache respectively; 2 placebo participantspresented fever and exudative erythema respectively
Notes It was conducted in Germany during boreal autumn-winter seasonsThis study is cited by Boyle, and it corresponds to RB14 in Bellanti’s review
Iuldashev 1988
Methods Double-blind, placebo-controlled trial
Participants Healthy children from 2 to 6 years
Interventions 1100 children received Reaferon (an analogue of human interferon 2 obtained by genetic engineering) 1106 IU in0.5 ml of water orally twice a week for 2 months. 1078 received 0.5 ml of water as placebo
Outcomes Children from 2 to 3 years treated with Reaferon had 1.3 less ARTIs than the placebo group. Children > 3 years didnot have statistically significant improvement
Notes It is not stated that the trial is randomizedSelection criteria of the participants allows the inclusion of non-susceptible participantsThe study was conducted from September to October in the former USSR
Jara-Pérez 2000
Methods Randomised, double-blind, placebo-controlled trial
Participants Girls from 6 to 13 years suffering more than 3 ARTI during fall and winter seasonsbefore the trial, living in an orphanage200 girls entered the trial
Interventions Participants received either 1 capsule of 3.5 mg of OM-85 BV or placebo once daily for10 days per month for 3 monthsParticipants were followed up for 3 months for a total study period of 6 months
Outcomes During the study period 99 OM-85 BV participants had 1.43 ± 0.94 (mean ± SD)ARTIs and 100 placebo participants had 2.99 ± 0.81 ARTIs. No adverse events relatedto the trial medications were reported
674Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
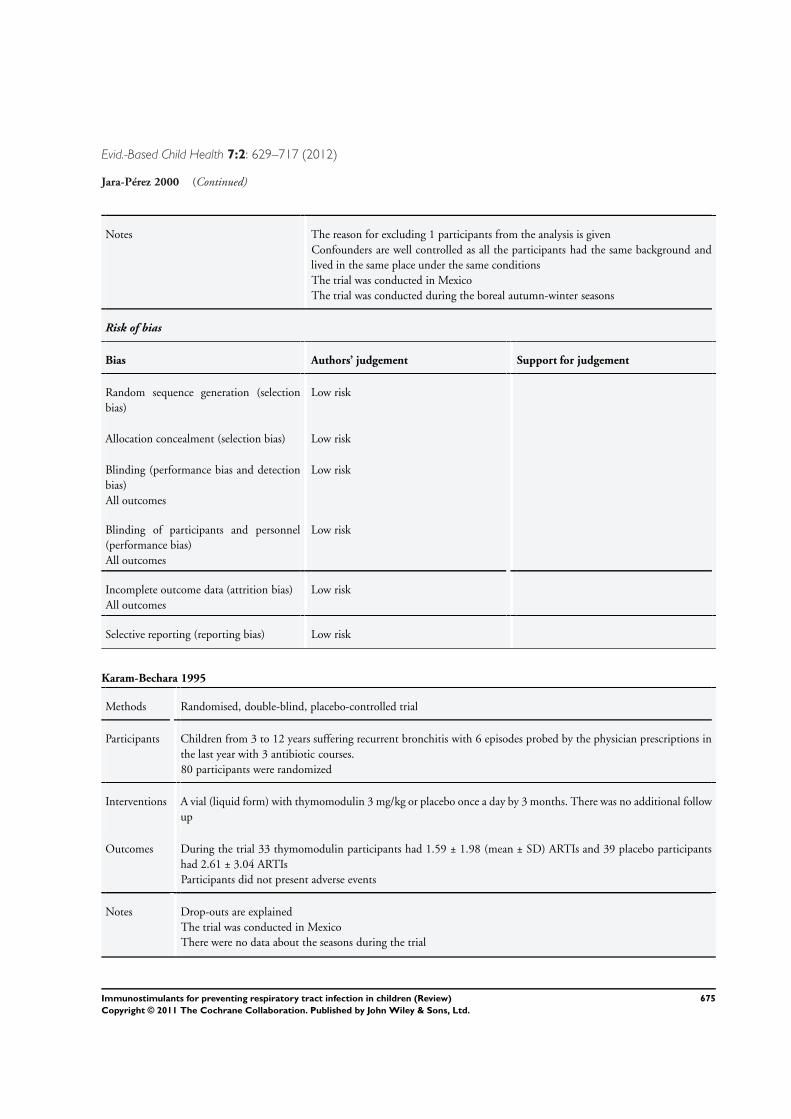
Evid.-Based Child Health 7:2: 629–717 (2012)
Jara-Pérez 2000 (Continued)
Notes The reason for excluding 1 participants from the analysis is givenConfounders are well controlled as all the participants had the same background andlived in the same place under the same conditionsThe trial was conducted in MexicoThe trial was conducted during the boreal autumn-winter seasons
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk
Allocation concealment (selection bias) Low risk
Blinding (performance bias and detectionbias)All outcomes
Low risk
Blinding of participants and personnel(performance bias)All outcomes
Low risk
Incomplete outcome data (attrition bias)All outcomes
Low risk
Selective reporting (reporting bias) Low risk
Karam-Bechara 1995
Methods Randomised, double-blind, placebo-controlled trial
Participants Children from 3 to 12 years suffering recurrent bronchitis with 6 episodes probed by the physician prescriptions inthe last year with 3 antibiotic courses.80 participants were randomized
Interventions A vial (liquid form) with thymomodulin 3 mg/kg or placebo once a day by 3 months. There was no additional followup
Outcomes During the trial 33 thymomodulin participants had 1.59 ± 1.98 (mean ± SD) ARTIs and 39 placebo participantshad 2.61 ± 3.04 ARTIsParticipants did not present adverse events
Notes Drop-outs are explainedThe trial was conducted in MexicoThere were no data about the seasons during the trial
675Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
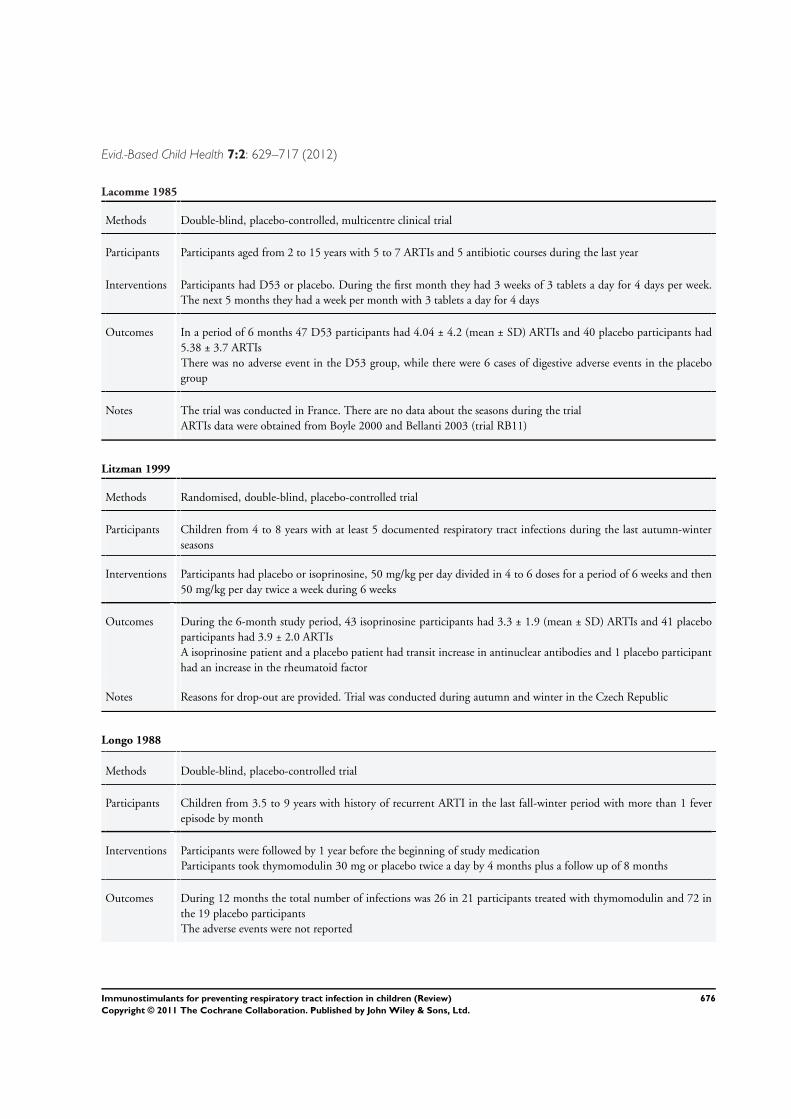
Evid.-Based Child Health 7:2: 629–717 (2012)
Lacomme 1985
Methods Double-blind, placebo-controlled, multicentre clinical trial
Participants Participants aged from 2 to 15 years with 5 to 7 ARTIs and 5 antibiotic courses during the last year
Interventions Participants had D53 or placebo. During the first month they had 3 weeks of 3 tablets a day for 4 days per week.The next 5 months they had a week per month with 3 tablets a day for 4 days
Outcomes In a period of 6 months 47 D53 participants had 4.04 ± 4.2 (mean ± SD) ARTIs and 40 placebo participants had5.38 ± 3.7 ARTIsThere was no adverse event in the D53 group, while there were 6 cases of digestive adverse events in the placebogroup
Notes The trial was conducted in France. There are no data about the seasons during the trialARTIs data were obtained from Boyle 2000 and Bellanti 2003 (trial RB11)
Litzman 1999
Methods Randomised, double-blind, placebo-controlled trial
Participants Children from 4 to 8 years with at least 5 documented respiratory tract infections during the last autumn-winterseasons
Interventions Participants had placebo or isoprinosine, 50 mg/kg per day divided in 4 to 6 doses for a period of 6 weeks and then50 mg/kg per day twice a week during 6 weeks
Outcomes During the 6-month study period, 43 isoprinosine participants had 3.3 ± 1.9 (mean ± SD) ARTIs and 41 placeboparticipants had 3.9 ± 2.0 ARTIsA isoprinosine patient and a placebo patient had transit increase in antinuclear antibodies and 1 placebo participanthad an increase in the rheumatoid factor
Notes Reasons for drop-out are provided. Trial was conducted during autumn and winter in the Czech Republic
Longo 1988
Methods Double-blind, placebo-controlled trial
Participants Children from 3.5 to 9 years with history of recurrent ARTI in the last fall-winter period with more than 1 feverepisode by month
Interventions Participants were followed by 1 year before the beginning of study medicationParticipants took thymomodulin 30 mg or placebo twice a day by 4 months plus a follow up of 8 months
Outcomes During 12 months the total number of infections was 26 in 21 participants treated with thymomodulin and 72 inthe 19 placebo participantsThe adverse events were not reported
676Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
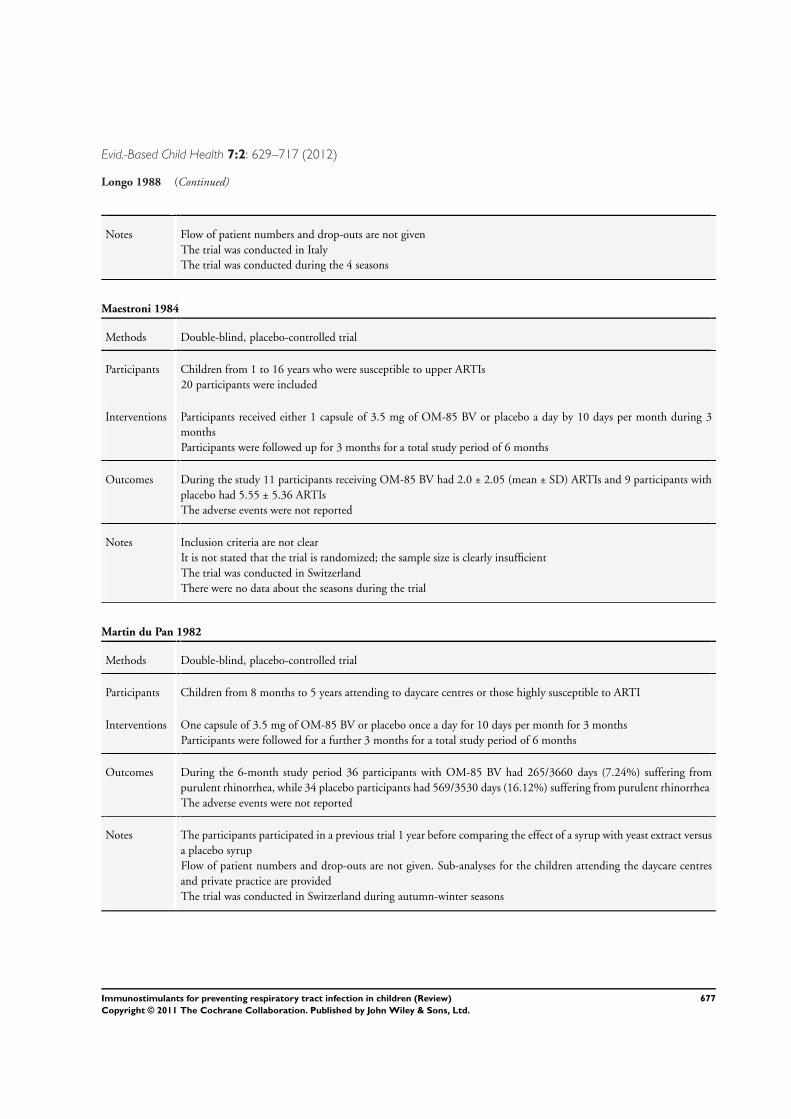
Evid.-Based Child Health 7:2: 629–717 (2012)
Longo 1988 (Continued)
Notes Flow of patient numbers and drop-outs are not givenThe trial was conducted in ItalyThe trial was conducted during the 4 seasons
Maestroni 1984
Methods Double-blind, placebo-controlled trial
Participants Children from 1 to 16 years who were susceptible to upper ARTIs20 participants were included
Interventions Participants received either 1 capsule of 3.5 mg of OM-85 BV or placebo a day by 10 days per month during 3monthsParticipants were followed up for 3 months for a total study period of 6 months
Outcomes During the study 11 participants receiving OM-85 BV had 2.0 ± 2.05 (mean ± SD) ARTIs and 9 participants withplacebo had 5.55 ± 5.36 ARTIsThe adverse events were not reported
Notes Inclusion criteria are not clearIt is not stated that the trial is randomized; the sample size is clearly insufficientThe trial was conducted in SwitzerlandThere were no data about the seasons during the trial
Martin du Pan 1982
Methods Double-blind, placebo-controlled trial
Participants Children from 8 months to 5 years attending to daycare centres or those highly susceptible to ARTI
Interventions One capsule of 3.5 mg of OM-85 BV or placebo once a day for 10 days per month for 3 monthsParticipants were followed for a further 3 months for a total study period of 6 months
Outcomes During the 6-month study period 36 participants with OM-85 BV had 265/3660 days (7.24%) suffering frompurulent rhinorrhea, while 34 placebo participants had 569/3530 days (16.12%) suffering from purulent rhinorrheaThe adverse events were not reported
Notes The participants participated in a previous trial 1 year before comparing the effect of a syrup with yeast extract versusa placebo syrupFlow of patient numbers and drop-outs are not given. Sub-analyses for the children attending the daycare centresand private practice are providedThe trial was conducted in Switzerland during autumn-winter seasons
677Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
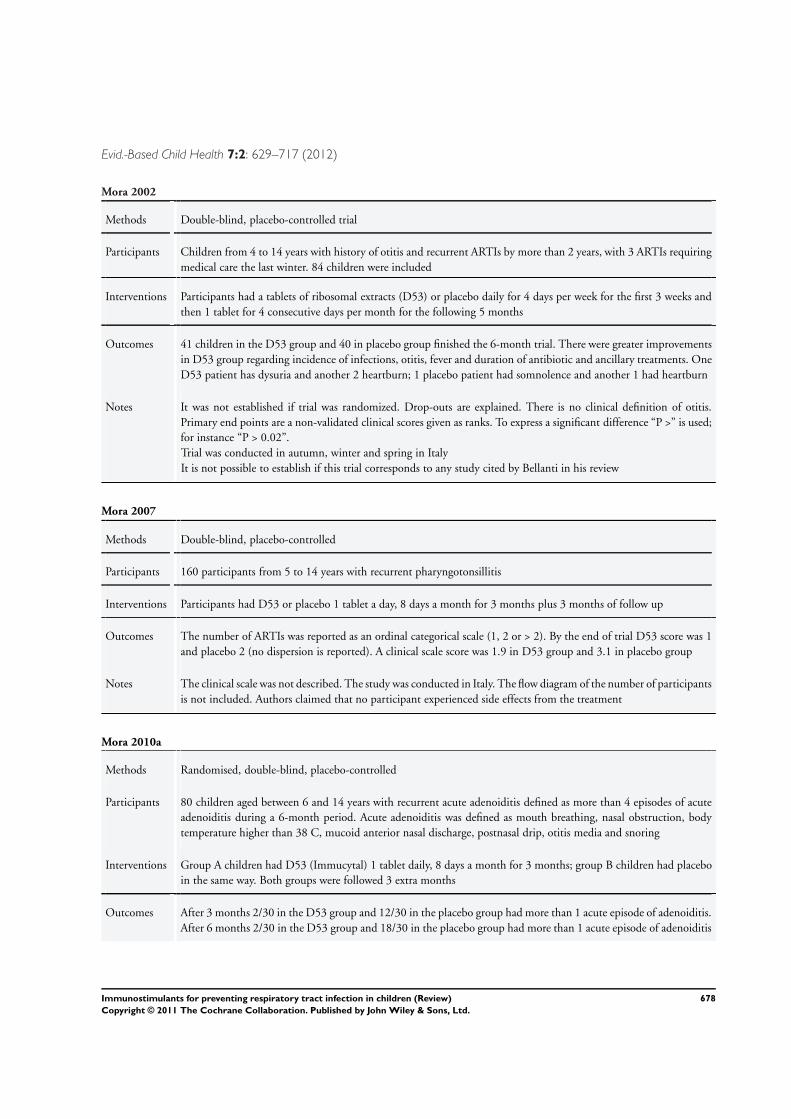
Evid.-Based Child Health 7:2: 629–717 (2012)
Mora 2002
Methods Double-blind, placebo-controlled trial
Participants Children from 4 to 14 years with history of otitis and recurrent ARTIs by more than 2 years, with 3 ARTIs requiringmedical care the last winter. 84 children were included
Interventions Participants had a tablets of ribosomal extracts (D53) or placebo daily for 4 days per week for the first 3 weeks andthen 1 tablet for 4 consecutive days per month for the following 5 months
Outcomes 41 children in the D53 group and 40 in placebo group finished the 6-month trial. There were greater improvementsin D53 group regarding incidence of infections, otitis, fever and duration of antibiotic and ancillary treatments. OneD53 patient has dysuria and another 2 heartburn; 1 placebo patient had somnolence and another 1 had heartburn
Notes It was not established if trial was randomized. Drop-outs are explained. There is no clinical definition of otitis.Primary end points are a non-validated clinical scores given as ranks. To express a significant difference “P >” is used;for instance “P > 0.02”.Trial was conducted in autumn, winter and spring in ItalyIt is not possible to establish if this trial corresponds to any study cited by Bellanti in his review
Mora 2007
Methods Double-blind, placebo-controlled
Participants 160 participants from 5 to 14 years with recurrent pharyngotonsillitis
Interventions Participants had D53 or placebo 1 tablet a day, 8 days a month for 3 months plus 3 months of follow up
Outcomes The number of ARTIs was reported as an ordinal categorical scale (1, 2 or > 2). By the end of trial D53 score was 1and placebo 2 (no dispersion is reported). A clinical scale score was 1.9 in D53 group and 3.1 in placebo group
Notes The clinical scale was not described. The study was conducted in Italy. The flow diagram of the number of participantsis not included. Authors claimed that no participant experienced side effects from the treatment
Mora 2010a
Methods Randomised, double-blind, placebo-controlled
Participants 80 children aged between 6 and 14 years with recurrent acute adenoiditis defined as more than 4 episodes of acuteadenoiditis during a 6-month period. Acute adenoiditis was defined as mouth breathing, nasal obstruction, bodytemperature higher than 38 C, mucoid anterior nasal discharge, postnasal drip, otitis media and snoring
Interventions Group A children had D53 (Immucytal) 1 tablet daily, 8 days a month for 3 months; group B children had placeboin the same way. Both groups were followed 3 extra months
Outcomes After 3 months 2/30 in the D53 group and 12/30 in the placebo group had more than 1 acute episode of adenoiditis.After 6 months 2/30 in the D53 group and 18/30 in the placebo group had more than 1 acute episode of adenoiditis
678Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Evid.-Based Child Health 7:2: 629–717 (2012)
Mora 2010a (Continued)
Notes Levels of IgE, IgA, IgG, and IgM were investigated, as well as tympanometry, rhinomanometry, and symptom visualanalogue scale by the parents. Only 60 participants completed the trial, the lost of participants are explained
Motta 1994
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Children from 3 to 14 years with history of recurrent tonsillitis with at least 8 episodes in the last 2 years, who hadsuffered tonsillitis 10 days before the enrolment to the trial
Interventions Pidotimod 400 mg (liquid form) or placebo twice a day by 15 days; then pidotimod 400 mg or placebo once a dayby 45 days. Participants were followed up for another 90 days
Outcomes During the trial 117 pidotimod participants had 1.96 ± 1.80 (mean ± SD) ARTIs and the 118 placebo participantshad 3.12 ± 2.45 ARTIs11 pidotimod participants had 15 adverse events, while 12 placebo participants had 18 adverse events, mainlygastrointestinal complaints
Notes Flow diagram of participants and drop-outs are not given. Number of infections per group was reconstructed fromthe reported frequenciesMost of the pidotimod papers were published in a single supplement issue of a German magazineThe trial was conducted in ItalyThere were no data about the seasons during the trial
Passali 1994a
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Children from 3 to 14 years with history of tonsillitis or pharyngitis in the previous autumn-winter seasons429 participants were randomized
Interventions Pidotimod 400 mg or placebo once a day for 2 months plus a follow-up period of 3 months
Outcomes Total number of infections during the treatment period of 2 months and the follow up period of 3 months were 186and 129 in the 205 pidotimod participants, while for the same periods the number of ARTIs were 278 and 276 in216 placebo participantsThere were 5 adverse events in the pidotimod group and 10 in the placebo group, mainly gastrointestinal complaints
Notes Flow of patient numbers and drop-outs are givenOnly the total number of ARTIs per group is reportedMost of the pidotimod papers were published in a single supplement issue of a German magazineThe trial was conducted in ItalyThere were no data about the seasons during the trial
679Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
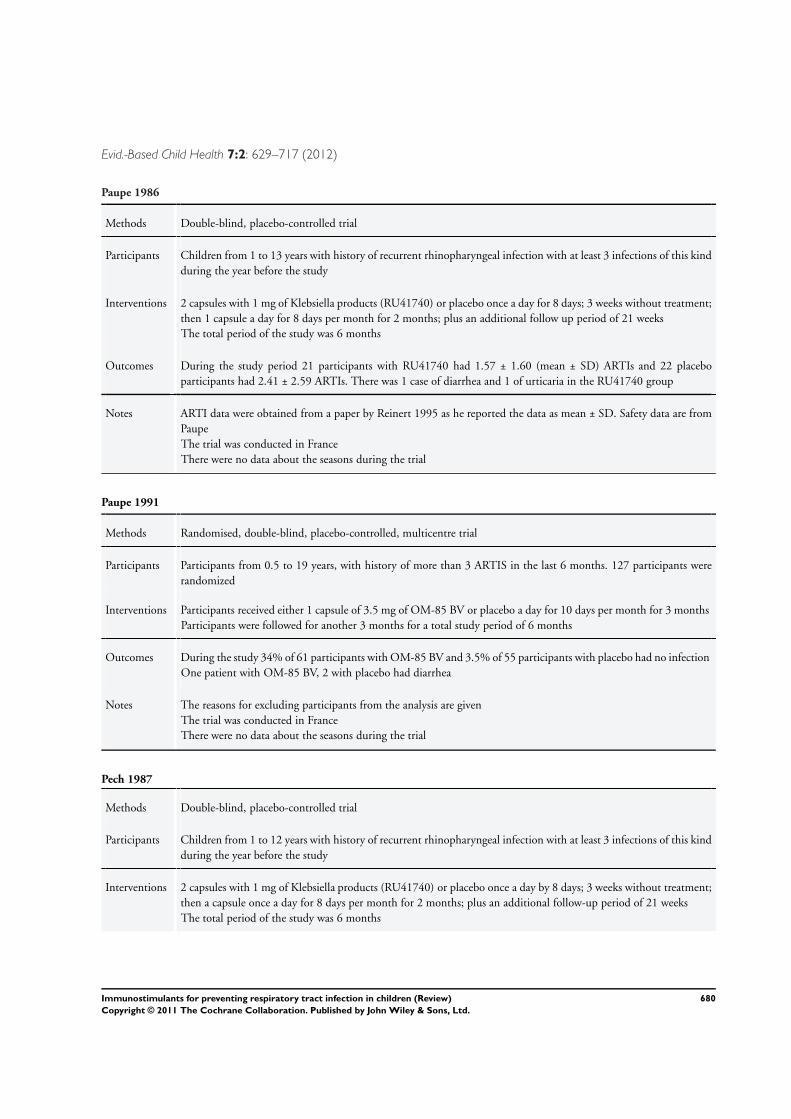
Evid.-Based Child Health 7:2: 629–717 (2012)
Paupe 1986
Methods Double-blind, placebo-controlled trial
Participants Children from 1 to 13 years with history of recurrent rhinopharyngeal infection with at least 3 infections of this kindduring the year before the study
Interventions 2 capsules with 1 mg of Klebsiella products (RU41740) or placebo once a day for 8 days; 3 weeks without treatment;then 1 capsule a day for 8 days per month for 2 months; plus an additional follow up period of 21 weeksThe total period of the study was 6 months
Outcomes During the study period 21 participants with RU41740 had 1.57 ± 1.60 (mean ± SD) ARTIs and 22 placeboparticipants had 2.41 ± 2.59 ARTIs. There was 1 case of diarrhea and 1 of urticaria in the RU41740 group
Notes ARTI data were obtained from a paper by Reinert 1995 as he reported the data as mean ± SD. Safety data are fromPaupeThe trial was conducted in FranceThere were no data about the seasons during the trial
Paupe 1991
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Participants from 0.5 to 19 years, with history of more than 3 ARTIS in the last 6 months. 127 participants wererandomized
Interventions Participants received either 1 capsule of 3.5 mg of OM-85 BV or placebo a day for 10 days per month for 3 monthsParticipants were followed for another 3 months for a total study period of 6 months
Outcomes During the study 34% of 61 participants with OM-85 BV and 3.5% of 55 participants with placebo had no infectionOne patient with OM-85 BV, 2 with placebo had diarrhea
Notes The reasons for excluding participants from the analysis are givenThe trial was conducted in FranceThere were no data about the seasons during the trial
Pech 1987
Methods Double-blind, placebo-controlled trial
Participants Children from 1 to 12 years with history of recurrent rhinopharyngeal infection with at least 3 infections of this kindduring the year before the study
Interventions 2 capsules with 1 mg of Klebsiella products (RU41740) or placebo once a day by 8 days; 3 weeks without treatment;then a capsule once a day for 8 days per month for 2 months; plus an additional follow-up period of 21 weeksThe total period of the study was 6 months
680Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
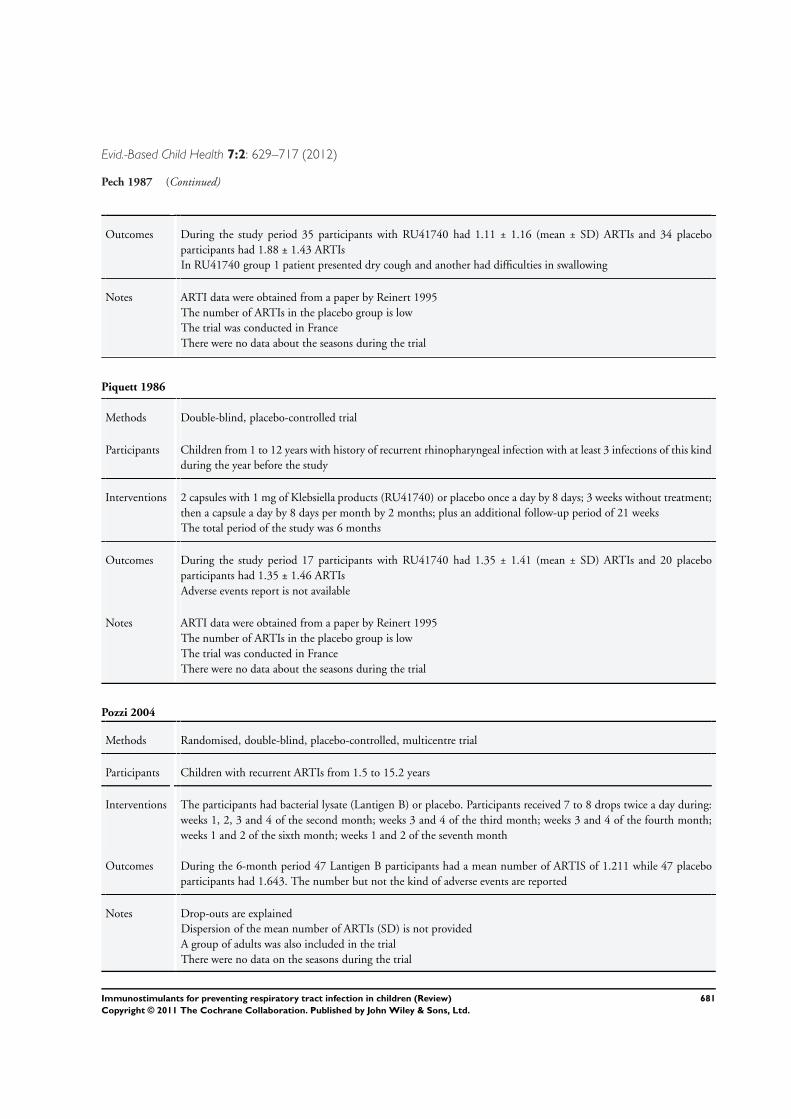
Evid.-Based Child Health 7:2: 629–717 (2012)
Pech 1987 (Continued)
Outcomes During the study period 35 participants with RU41740 had 1.11 ± 1.16 (mean ± SD) ARTIs and 34 placeboparticipants had 1.88 ± 1.43 ARTIsIn RU41740 group 1 patient presented dry cough and another had difficulties in swallowing
Notes ARTI data were obtained from a paper by Reinert 1995The number of ARTIs in the placebo group is lowThe trial was conducted in FranceThere were no data about the seasons during the trial
Piquett 1986
Methods Double-blind, placebo-controlled trial
Participants Children from 1 to 12 years with history of recurrent rhinopharyngeal infection with at least 3 infections of this kindduring the year before the study
Interventions 2 capsules with 1 mg of Klebsiella products (RU41740) or placebo once a day by 8 days; 3 weeks without treatment;then a capsule a day by 8 days per month by 2 months; plus an additional follow-up period of 21 weeksThe total period of the study was 6 months
Outcomes During the study period 17 participants with RU41740 had 1.35 ± 1.41 (mean ± SD) ARTIs and 20 placeboparticipants had 1.35 ± 1.46 ARTIsAdverse events report is not available
Notes ARTI data were obtained from a paper by Reinert 1995The number of ARTIs in the placebo group is lowThe trial was conducted in FranceThere were no data about the seasons during the trial
Pozzi 2004
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Children with recurrent ARTIs from 1.5 to 15.2 years
Interventions The participants had bacterial lysate (Lantigen B) or placebo. Participants received 7 to 8 drops twice a day during:weeks 1, 2, 3 and 4 of the second month; weeks 3 and 4 of the third month; weeks 3 and 4 of the fourth month;weeks 1 and 2 of the sixth month; weeks 1 and 2 of the seventh month
Outcomes During the 6-month period 47 Lantigen B participants had a mean number of ARTIS of 1.211 while 47 placeboparticipants had 1.643. The number but not the kind of adverse events are reported
Notes Drop-outs are explainedDispersion of the mean number of ARTIs (SD) is not providedA group of adults was also included in the trialThere were no data on the seasons during the trial
681Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
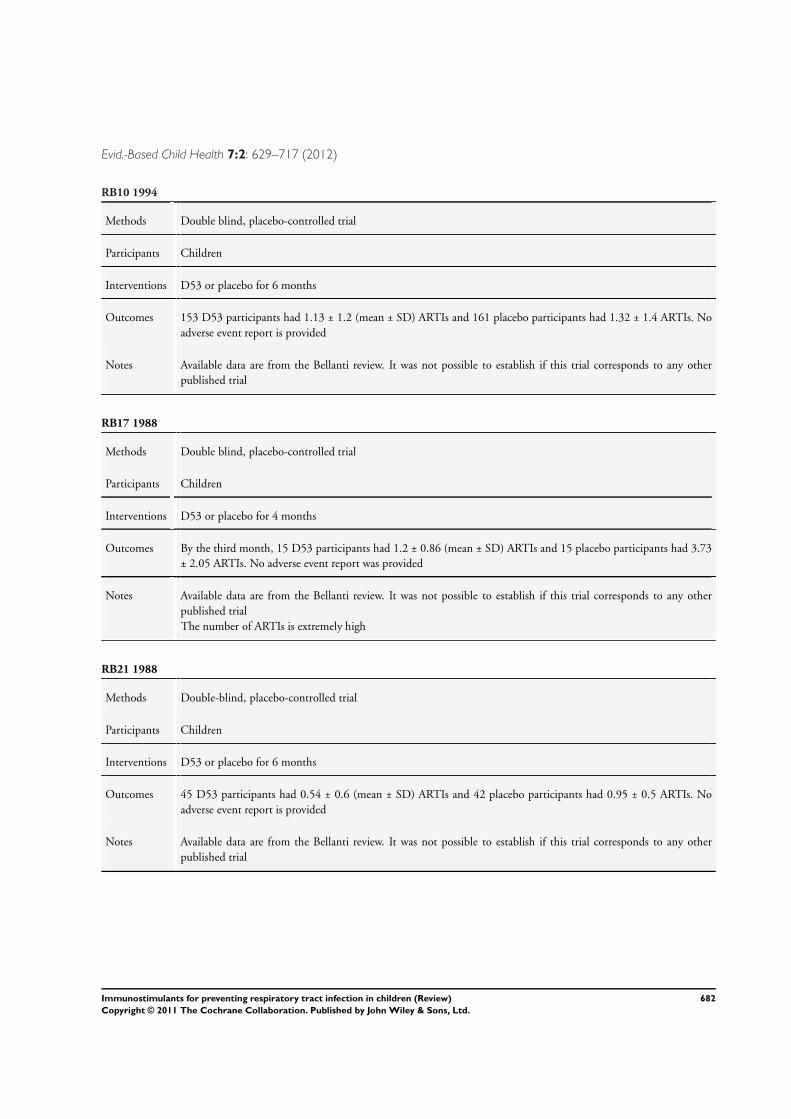
Evid.-Based Child Health 7:2: 629–717 (2012)
RB10 1994
Methods Double blind, placebo-controlled trial
Participants Children
Interventions D53 or placebo for 6 months
Outcomes 153 D53 participants had 1.13 ± 1.2 (mean ± SD) ARTIs and 161 placebo participants had 1.32 ± 1.4 ARTIs. Noadverse event report is provided
Notes Available data are from the Bellanti review. It was not possible to establish if this trial corresponds to any otherpublished trial
RB17 1988
Methods Double blind, placebo-controlled trial
Participants Children
Interventions D53 or placebo for 4 months
Outcomes By the third month, 15 D53 participants had 1.2 ± 0.86 (mean ± SD) ARTIs and 15 placebo participants had 3.73± 2.05 ARTIs. No adverse event report was provided
Notes Available data are from the Bellanti review. It was not possible to establish if this trial corresponds to any otherpublished trialThe number of ARTIs is extremely high
RB21 1988
Methods Double-blind, placebo-controlled trial
Participants Children
Interventions D53 or placebo for 6 months
Outcomes 45 D53 participants had 0.54 ± 0.6 (mean ± SD) ARTIs and 42 placebo participants had 0.95 ± 0.5 ARTIs. Noadverse event report is provided
Notes Available data are from the Bellanti review. It was not possible to establish if this trial corresponds to any otherpublished trial
682Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
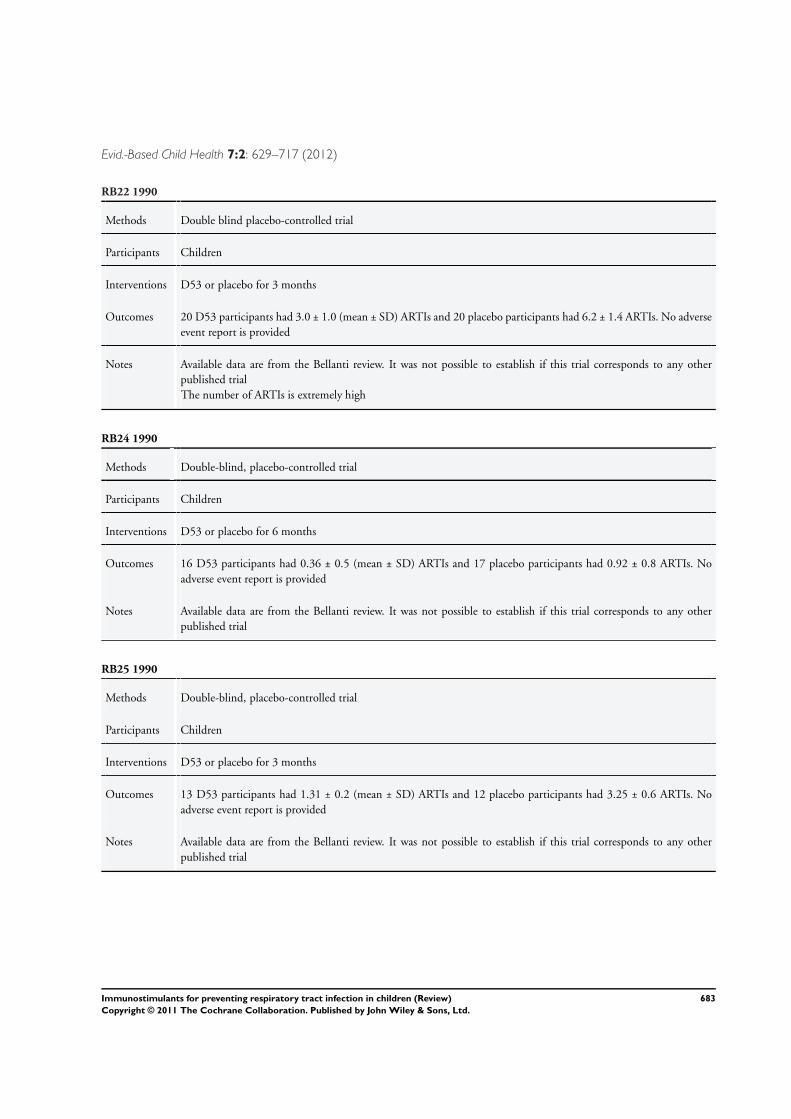
Evid.-Based Child Health 7:2: 629–717 (2012)
RB22 1990
Methods Double blind placebo-controlled trial
Participants Children
Interventions D53 or placebo for 3 months
Outcomes 20 D53 participants had 3.0 ± 1.0 (mean ± SD) ARTIs and 20 placebo participants had 6.2 ± 1.4 ARTIs. No adverseevent report is provided
Notes Available data are from the Bellanti review. It was not possible to establish if this trial corresponds to any otherpublished trialThe number of ARTIs is extremely high
RB24 1990
Methods Double-blind, placebo-controlled trial
Participants Children
Interventions D53 or placebo for 6 months
Outcomes 16 D53 participants had 0.36 ± 0.5 (mean ± SD) ARTIs and 17 placebo participants had 0.92 ± 0.8 ARTIs. Noadverse event report is provided
Notes Available data are from the Bellanti review. It was not possible to establish if this trial corresponds to any otherpublished trial
RB25 1990
Methods Double-blind, placebo-controlled trial
Participants Children
Interventions D53 or placebo for 3 months
Outcomes 13 D53 participants had 1.31 ± 0.2 (mean ± SD) ARTIs and 12 placebo participants had 3.25 ± 0.6 ARTIs. Noadverse event report is provided
Notes Available data are from the Bellanti review. It was not possible to establish if this trial corresponds to any otherpublished trial
683Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
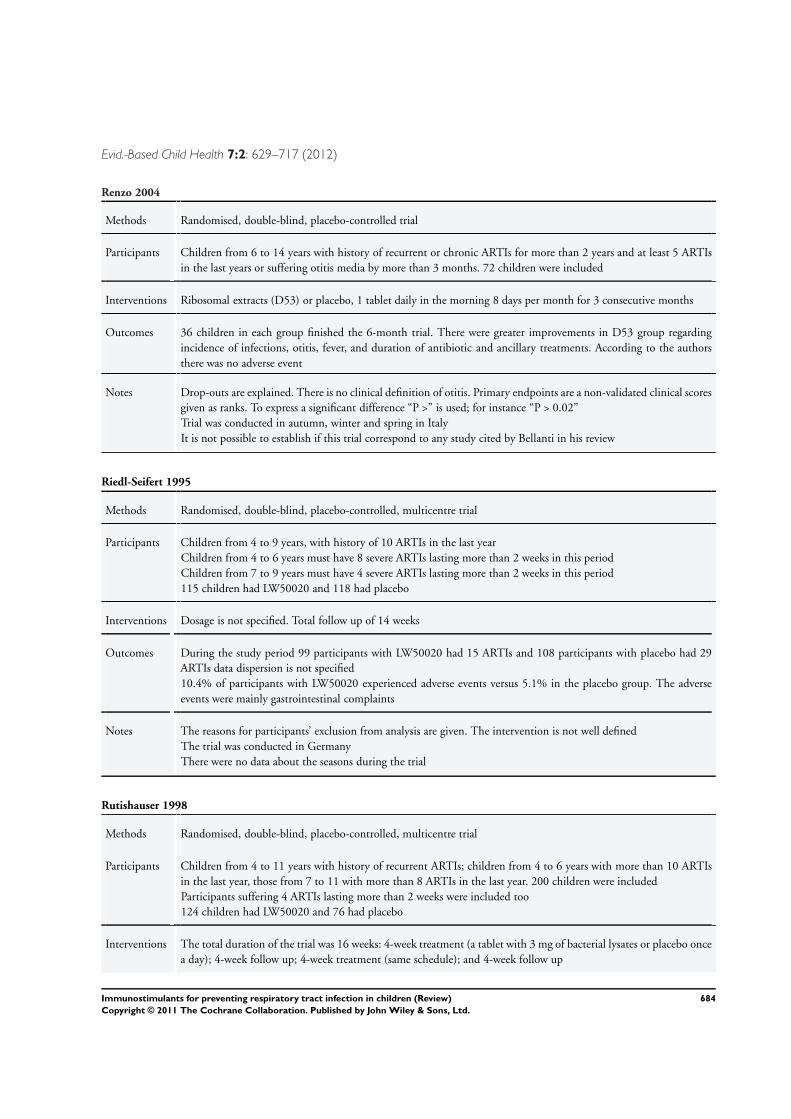
Evid.-Based Child Health 7:2: 629–717 (2012)
Renzo 2004
Methods Randomised, double-blind, placebo-controlled trial
Participants Children from 6 to 14 years with history of recurrent or chronic ARTIs for more than 2 years and at least 5 ARTIsin the last years or suffering otitis media by more than 3 months. 72 children were included
Interventions Ribosomal extracts (D53) or placebo, 1 tablet daily in the morning 8 days per month for 3 consecutive months
Outcomes 36 children in each group finished the 6-month trial. There were greater improvements in D53 group regardingincidence of infections, otitis, fever, and duration of antibiotic and ancillary treatments. According to the authorsthere was no adverse event
Notes Drop-outs are explained. There is no clinical definition of otitis. Primary endpoints are a non-validated clinical scoresgiven as ranks. To express a significant difference “P >” is used; for instance “P > 0.02”Trial was conducted in autumn, winter and spring in ItalyIt is not possible to establish if this trial correspond to any study cited by Bellanti in his review
Riedl-Seifert 1995
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Children from 4 to 9 years, with history of 10 ARTIs in the last yearChildren from 4 to 6 years must have 8 severe ARTIs lasting more than 2 weeks in this periodChildren from 7 to 9 years must have 4 severe ARTIs lasting more than 2 weeks in this period115 children had LW50020 and 118 had placebo
Interventions Dosage is not specified. Total follow up of 14 weeks
Outcomes During the study period 99 participants with LW50020 had 15 ARTIs and 108 participants with placebo had 29ARTIs data dispersion is not specified10.4% of participants with LW50020 experienced adverse events versus 5.1% in the placebo group. The adverseevents were mainly gastrointestinal complaints
Notes The reasons for participants’ exclusion from analysis are given. The intervention is not well definedThe trial was conducted in GermanyThere were no data about the seasons during the trial
Rutishauser 1998
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Children from 4 to 11 years with history of recurrent ARTIs; children from 4 to 6 years with more than 10 ARTIsin the last year, those from 7 to 11 with more than 8 ARTIs in the last year. 200 children were includedParticipants suffering 4 ARTIs lasting more than 2 weeks were included too124 children had LW50020 and 76 had placebo
Interventions The total duration of the trial was 16 weeks: 4-week treatment (a tablet with 3 mg of bacterial lysates or placebo oncea day); 4-week follow up; 4-week treatment (same schedule); and 4-week follow up
684Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
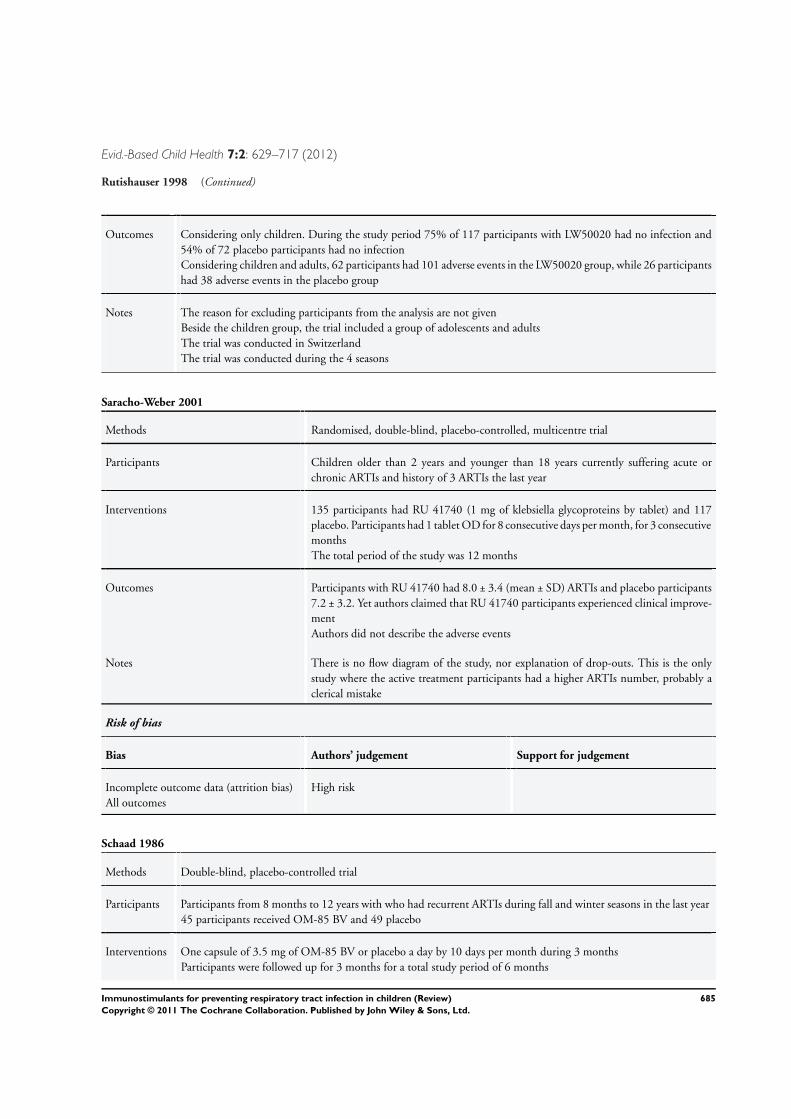
Evid.-Based Child Health 7:2: 629–717 (2012)
Rutishauser 1998 (Continued)
Outcomes Considering only children. During the study period 75% of 117 participants with LW50020 had no infection and54% of 72 placebo participants had no infectionConsidering children and adults, 62 participants had 101 adverse events in the LW50020 group, while 26 participantshad 38 adverse events in the placebo group
Notes The reason for excluding participants from the analysis are not givenBeside the children group, the trial included a group of adolescents and adultsThe trial was conducted in SwitzerlandThe trial was conducted during the 4 seasons
Saracho-Weber 2001
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Children older than 2 years and younger than 18 years currently suffering acute orchronic ARTIs and history of 3 ARTIs the last year
Interventions 135 participants had RU 41740 (1 mg of klebsiella glycoproteins by tablet) and 117placebo. Participants had 1 tablet OD for 8 consecutive days per month, for 3 consecutivemonthsThe total period of the study was 12 months
Outcomes Participants with RU 41740 had 8.0 ± 3.4 (mean ± SD) ARTIs and placebo participants7.2 ± 3.2. Yet authors claimed that RU 41740 participants experienced clinical improve-mentAuthors did not describe the adverse events
Notes There is no flow diagram of the study, nor explanation of drop-outs. This is the onlystudy where the active treatment participants had a higher ARTIs number, probably aclerical mistake
Risk of bias
Bias Authors’ judgement Support for judgement
Incomplete outcome data (attrition bias)All outcomes
High risk
Schaad 1986
Methods Double-blind, placebo-controlled trial
Participants Participants from 8 months to 12 years with who had recurrent ARTIs during fall and winter seasons in the last year45 participants received OM-85 BV and 49 placebo
Interventions One capsule of 3.5 mg of OM-85 BV or placebo a day by 10 days per month during 3 monthsParticipants were followed up for 3 months for a total study period of 6 months
685Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
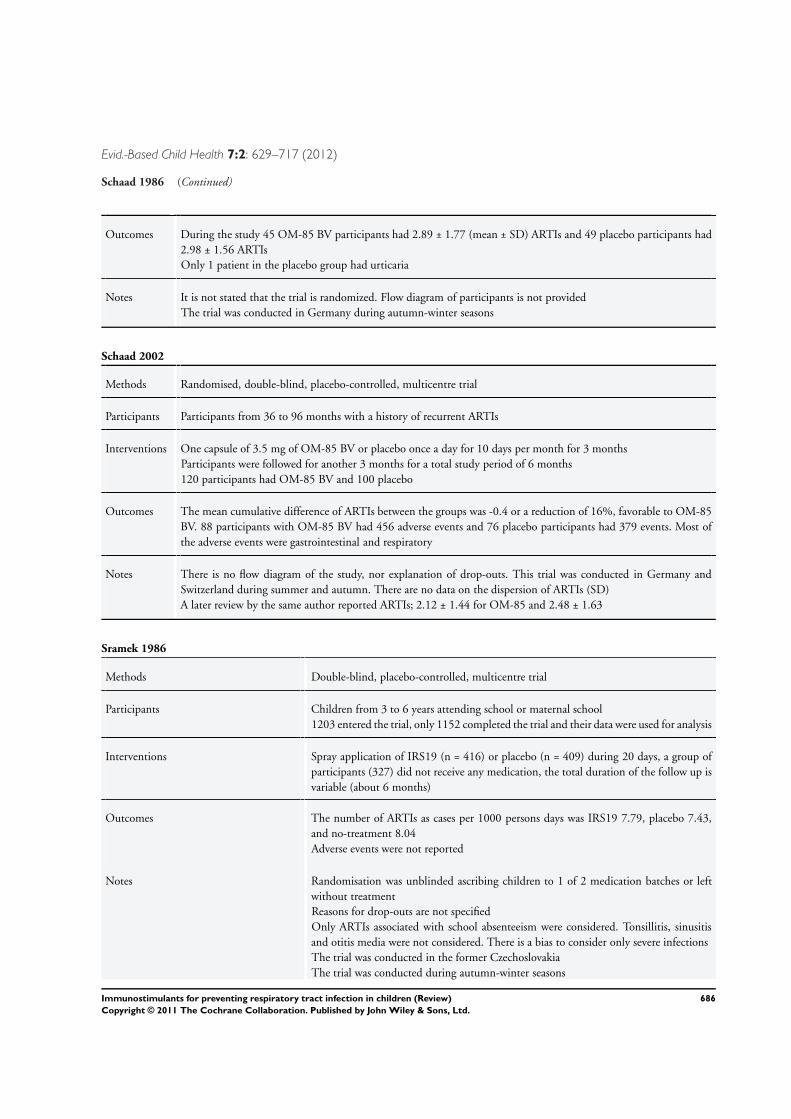
Evid.-Based Child Health 7:2: 629–717 (2012)
Schaad 1986 (Continued)
Outcomes During the study 45 OM-85 BV participants had 2.89 ± 1.77 (mean ± SD) ARTIs and 49 placebo participants had2.98 ± 1.56 ARTIsOnly 1 patient in the placebo group had urticaria
Notes It is not stated that the trial is randomized. Flow diagram of participants is not providedThe trial was conducted in Germany during autumn-winter seasons
Schaad 2002
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Participants from 36 to 96 months with a history of recurrent ARTIs
Interventions One capsule of 3.5 mg of OM-85 BV or placebo once a day for 10 days per month for 3 monthsParticipants were followed for another 3 months for a total study period of 6 months120 participants had OM-85 BV and 100 placebo
Outcomes The mean cumulative difference of ARTIs between the groups was -0.4 or a reduction of 16%, favorable to OM-85BV. 88 participants with OM-85 BV had 456 adverse events and 76 placebo participants had 379 events. Most ofthe adverse events were gastrointestinal and respiratory
Notes There is no flow diagram of the study, nor explanation of drop-outs. This trial was conducted in Germany andSwitzerland during summer and autumn. There are no data on the dispersion of ARTIs (SD)A later review by the same author reported ARTIs; 2.12 ± 1.44 for OM-85 and 2.48 ± 1.63
Sramek 1986
Methods Double-blind, placebo-controlled, multicentre trial
Participants Children from 3 to 6 years attending school or maternal school1203 entered the trial, only 1152 completed the trial and their data were used for analysis
Interventions Spray application of IRS19 (n = 416) or placebo (n = 409) during 20 days, a group ofparticipants (327) did not receive any medication, the total duration of the follow up isvariable (about 6 months)
Outcomes The number of ARTIs as cases per 1000 persons days was IRS19 7.79, placebo 7.43,and no-treatment 8.04Adverse events were not reported
Notes Randomisation was unblinded ascribing children to 1 of 2 medication batches or leftwithout treatmentReasons for drop-outs are not specifiedOnly ARTIs associated with school absenteeism were considered. Tonsillitis, sinusitisand otitis media were not considered. There is a bias to consider only severe infectionsThe trial was conducted in the former CzechoslovakiaThe trial was conducted during autumn-winter seasons
686Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
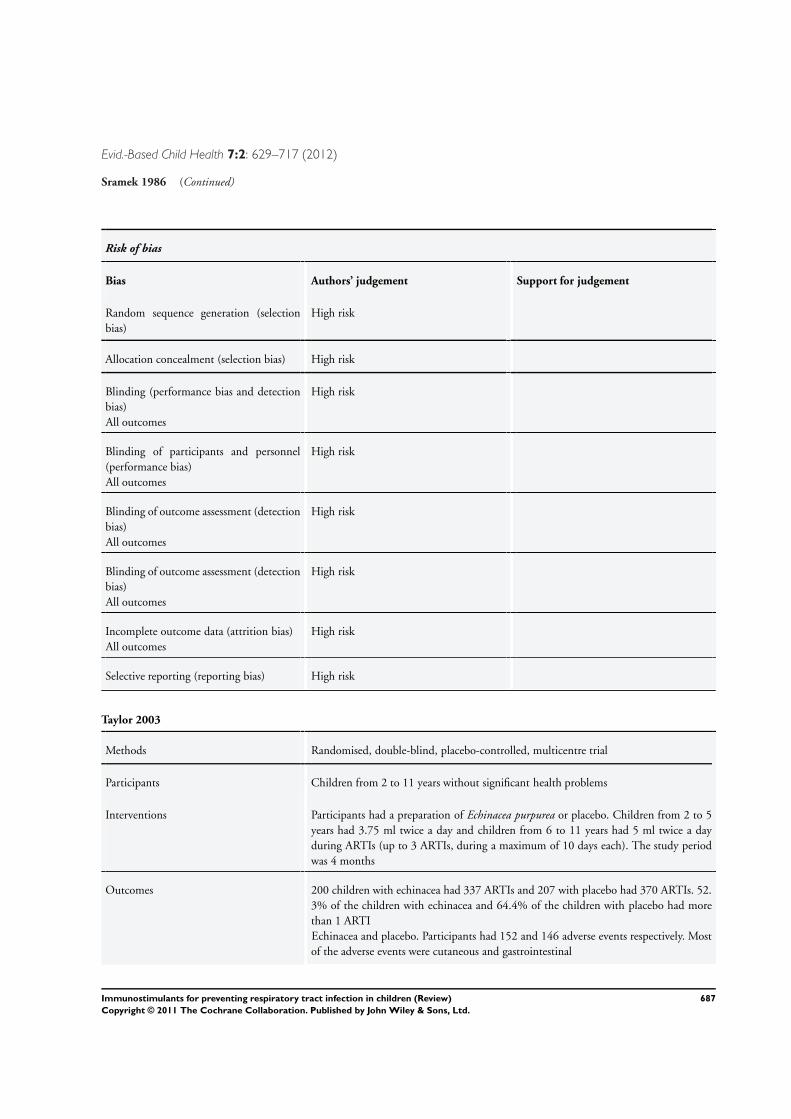
Evid.-Based Child Health 7:2: 629–717 (2012)
Sramek 1986 (Continued)
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
High risk
Allocation concealment (selection bias) High risk
Blinding (performance bias and detectionbias)All outcomes
High risk
Blinding of participants and personnel(performance bias)All outcomes
High risk
Blinding of outcome assessment (detectionbias)All outcomes
High risk
Blinding of outcome assessment (detectionbias)All outcomes
High risk
Incomplete outcome data (attrition bias)All outcomes
High risk
Selective reporting (reporting bias) High risk
Taylor 2003
Methods Randomised, double-blind, placebo-controlled, multicentre trial
Participants Children from 2 to 11 years without significant health problems
Interventions Participants had a preparation of Echinacea purpurea or placebo. Children from 2 to 5years had 3.75 ml twice a day and children from 6 to 11 years had 5 ml twice a dayduring ARTIs (up to 3 ARTIs, during a maximum of 10 days each). The study periodwas 4 months
Outcomes 200 children with echinacea had 337 ARTIs and 207 with placebo had 370 ARTIs. 52.3% of the children with echinacea and 64.4% of the children with placebo had morethan 1 ARTIEchinacea and placebo. Participants had 152 and 146 adverse events respectively. Mostof the adverse events were cutaneous and gastrointestinal
687Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
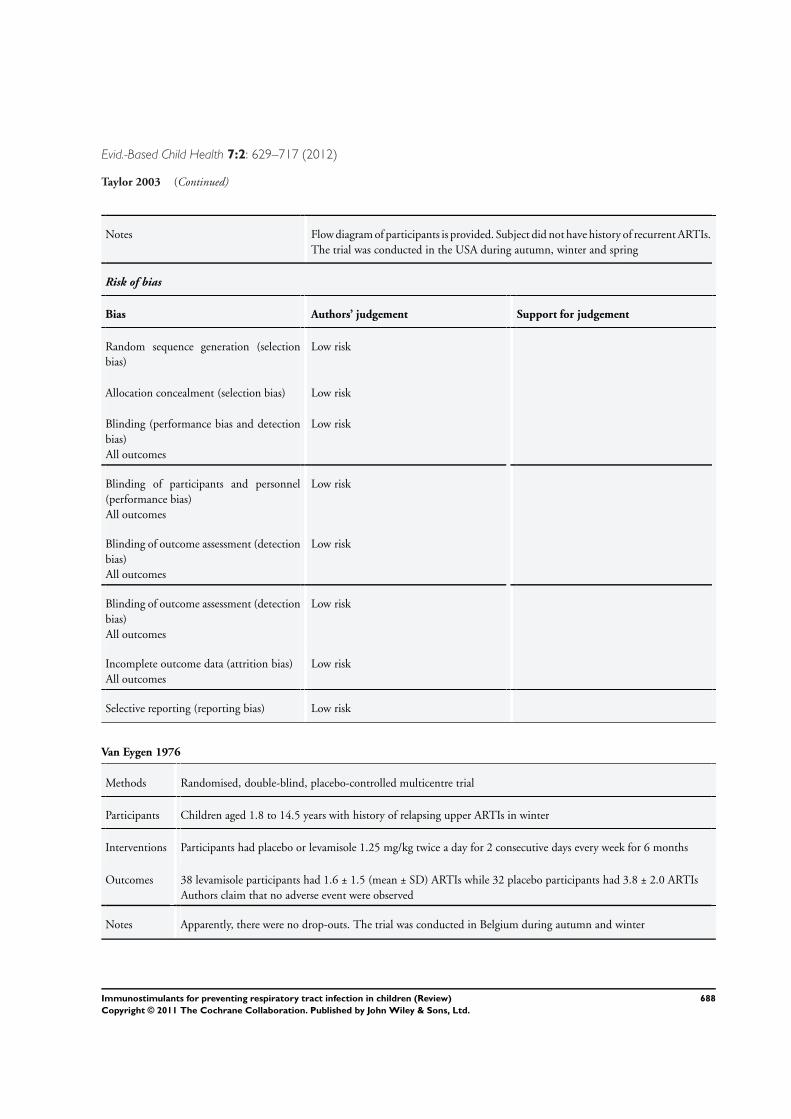
Evid.-Based Child Health 7:2: 629–717 (2012)
Taylor 2003 (Continued)
Notes Flow diagram of participants is provided. Subject did not have history of recurrent ARTIs.The trial was conducted in the USA during autumn, winter and spring
Risk of bias
Bias Authors’ judgement Support for judgement
Random sequence generation (selectionbias)
Low risk
Allocation concealment (selection bias) Low risk
Blinding (performance bias and detectionbias)All outcomes
Low risk
Blinding of participants and personnel(performance bias)All outcomes
Low risk
Blinding of outcome assessment (detectionbias)All outcomes
Low risk
Blinding of outcome assessment (detectionbias)All outcomes
Low risk
Incomplete outcome data (attrition bias)All outcomes
Low risk
Selective reporting (reporting bias) Low risk
Van Eygen 1976
Methods Randomised, double-blind, placebo-controlled multicentre trial
Participants Children aged 1.8 to 14.5 years with history of relapsing upper ARTIs in winter
Interventions Participants had placebo or levamisole 1.25 mg/kg twice a day for 2 consecutive days every week for 6 months
Outcomes 38 levamisole participants had 1.6 ± 1.5 (mean ± SD) ARTIs while 32 placebo participants had 3.8 ± 2.0 ARTIsAuthors claim that no adverse event were observed
Notes Apparently, there were no drop-outs. The trial was conducted in Belgium during autumn and winter
688Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
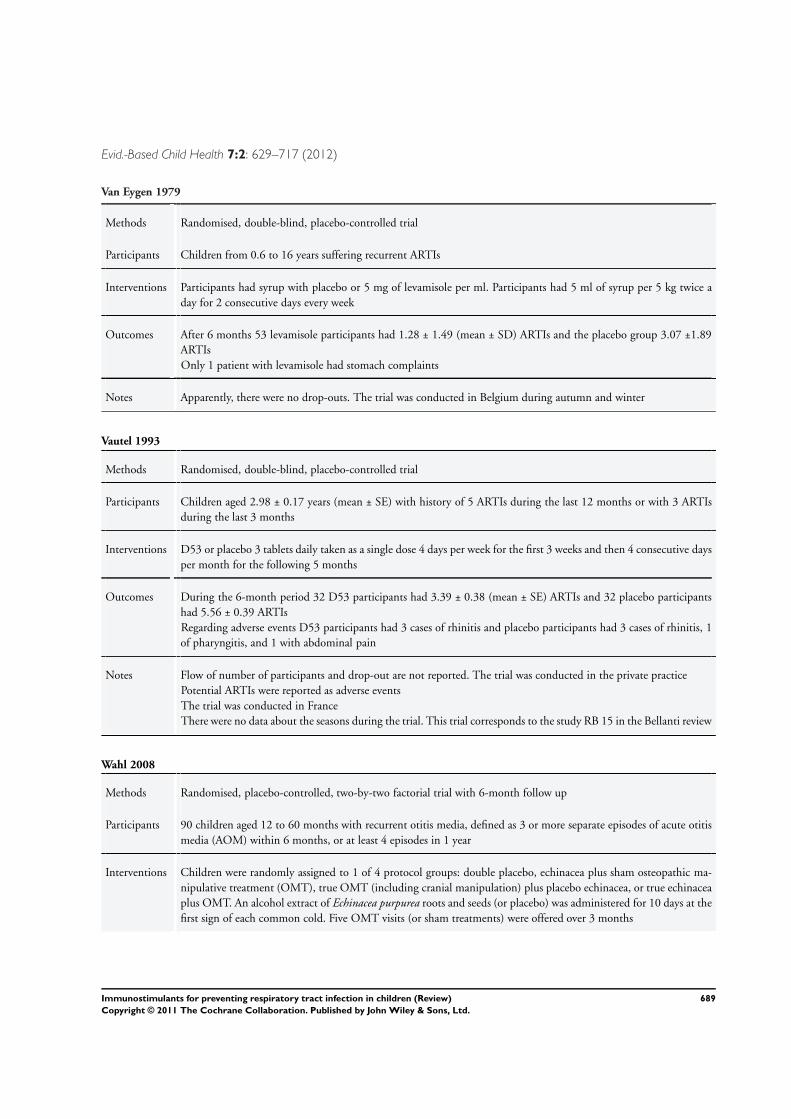
Evid.-Based Child Health 7:2: 629–717 (2012)
Van Eygen 1979
Methods Randomised, double-blind, placebo-controlled trial
Participants Children from 0.6 to 16 years suffering recurrent ARTIs
Interventions Participants had syrup with placebo or 5 mg of levamisole per ml. Participants had 5 ml of syrup per 5 kg twice aday for 2 consecutive days every week
Outcomes After 6 months 53 levamisole participants had 1.28 ± 1.49 (mean ± SD) ARTIs and the placebo group 3.07 ±1.89ARTIsOnly 1 patient with levamisole had stomach complaints
Notes Apparently, there were no drop-outs. The trial was conducted in Belgium during autumn and winter
Vautel 1993
Methods Randomised, double-blind, placebo-controlled trial
Participants Children aged 2.98 ± 0.17 years (mean ± SE) with history of 5 ARTIs during the last 12 months or with 3 ARTIsduring the last 3 months
Interventions D53 or placebo 3 tablets daily taken as a single dose 4 days per week for the first 3 weeks and then 4 consecutive daysper month for the following 5 months
Outcomes During the 6-month period 32 D53 participants had 3.39 ± 0.38 (mean ± SE) ARTIs and 32 placebo participantshad 5.56 ± 0.39 ARTIsRegarding adverse events D53 participants had 3 cases of rhinitis and placebo participants had 3 cases of rhinitis, 1of pharyngitis, and 1 with abdominal pain
Notes Flow of number of participants and drop-out are not reported. The trial was conducted in the private practicePotential ARTIs were reported as adverse eventsThe trial was conducted in FranceThere were no data about the seasons during the trial. This trial corresponds to the study RB 15 in the Bellanti review
Wahl 2008
Methods Randomised, placebo-controlled, two-by-two factorial trial with 6-month follow up
Participants 90 children aged 12 to 60 months with recurrent otitis media, defined as 3 or more separate episodes of acute otitismedia (AOM) within 6 months, or at least 4 episodes in 1 year
Interventions Children were randomly assigned to 1 of 4 protocol groups: double placebo, echinacea plus sham osteopathic ma-nipulative treatment (OMT), true OMT (including cranial manipulation) plus placebo echinacea, or true echinaceaplus OMT. An alcohol extract of Echinacea purpurea roots and seeds (or placebo) was administered for 10 days at thefirst sign of each common cold. Five OMT visits (or sham treatments) were offered over 3 months
689Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
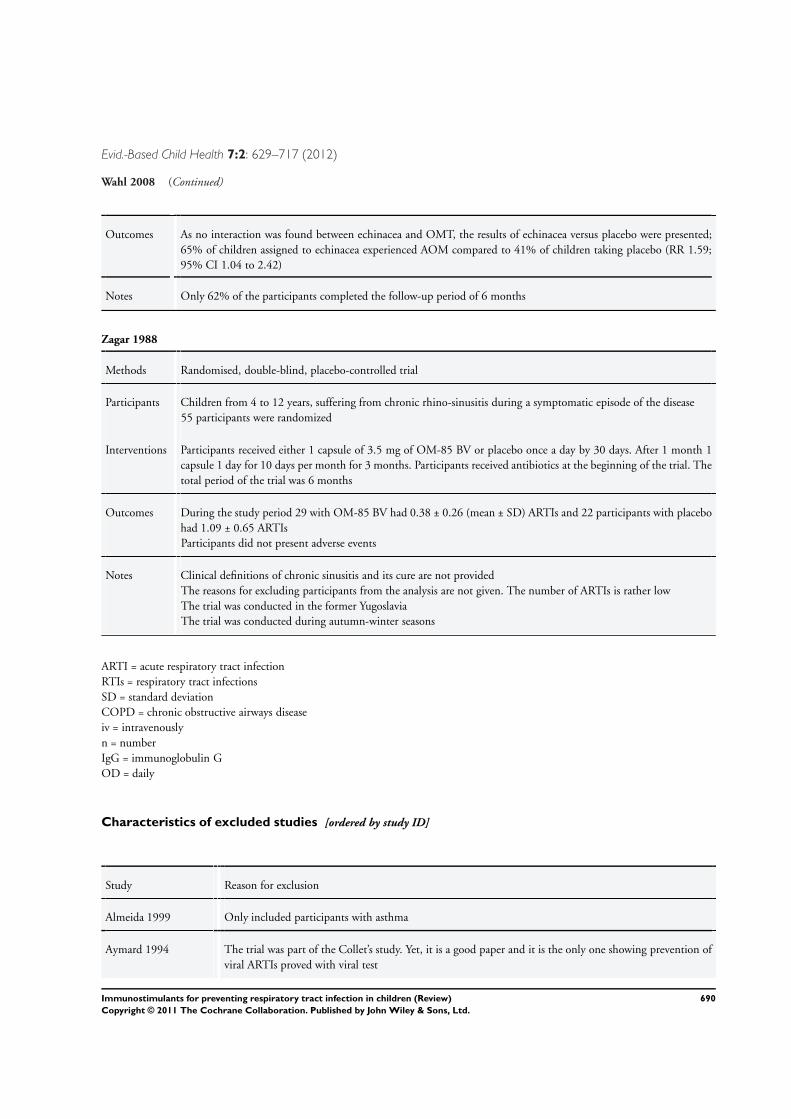
Evid.-Based Child Health 7:2: 629–717 (2012)
Wahl 2008 (Continued)
Outcomes As no interaction was found between echinacea and OMT, the results of echinacea versus placebo were presented;65% of children assigned to echinacea experienced AOM compared to 41% of children taking placebo (RR 1.59;95% CI 1.04 to 2.42)
Notes Only 62% of the participants completed the follow-up period of 6 months
Zagar 1988
Methods Randomised, double-blind, placebo-controlled trial
Participants Children from 4 to 12 years, suffering from chronic rhino-sinusitis during a symptomatic episode of the disease55 participants were randomized
Interventions Participants received either 1 capsule of 3.5 mg of OM-85 BV or placebo once a day by 30 days. After 1 month 1capsule 1 day for 10 days per month for 3 months. Participants received antibiotics at the beginning of the trial. Thetotal period of the trial was 6 months
Outcomes During the study period 29 with OM-85 BV had 0.38 ± 0.26 (mean ± SD) ARTIs and 22 participants with placebohad 1.09 ± 0.65 ARTIsParticipants did not present adverse events
Notes Clinical definitions of chronic sinusitis and its cure are not providedThe reasons for excluding participants from the analysis are not given. The number of ARTIs is rather lowThe trial was conducted in the former YugoslaviaThe trial was conducted during autumn-winter seasons
ARTI = acute respiratory tract infectionRTIs = respiratory tract infectionsSD = standard deviationCOPD = chronic obstructive airways diseaseiv = intravenouslyn = numberIgG = immunoglobulin GOD = daily
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Almeida 1999 Only included participants with asthma
Aymard 1994 The trial was part of the Collet’s study. Yet, it is a good paper and it is the only one showing prevention ofviral ARTIs proved with viral test
690Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
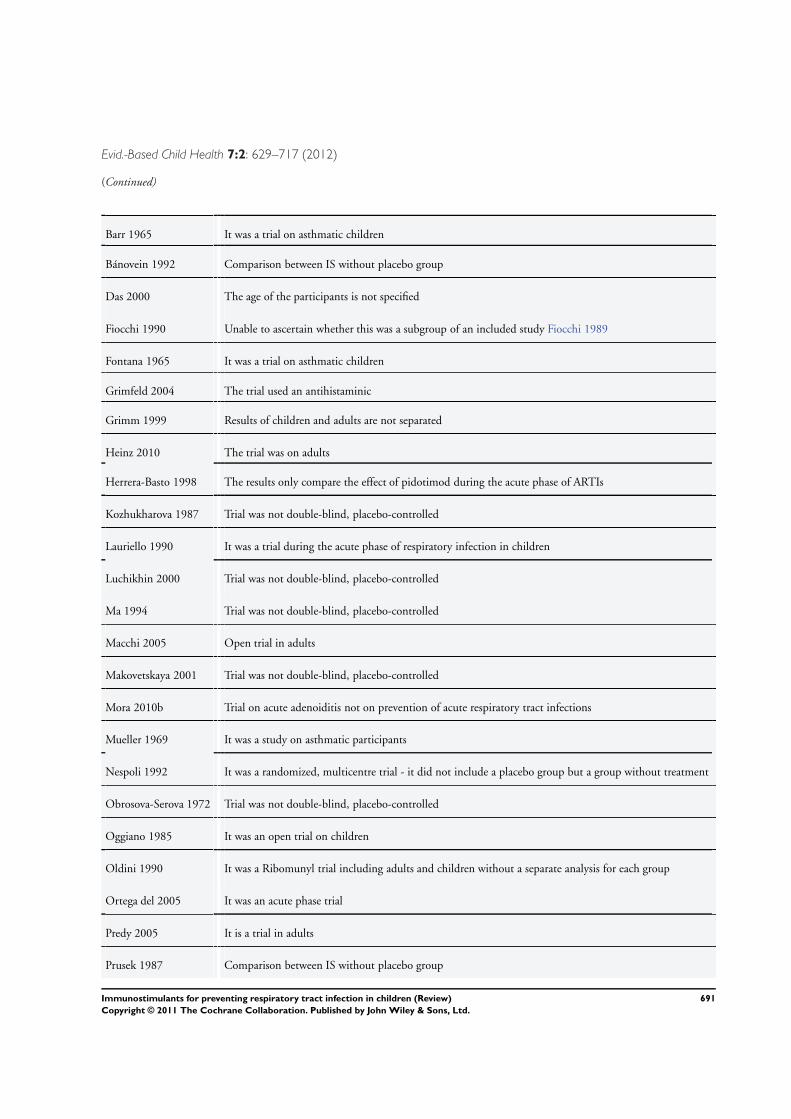
Evid.-Based Child Health 7:2: 629–717 (2012)
(Continued)
Barr 1965 It was a trial on asthmatic children
Bánovein 1992 Comparison between IS without placebo group
Das 2000 The age of the participants is not specified
Fiocchi 1990 Unable to ascertain whether this was a subgroup of an included study Fiocchi 1989
Fontana 1965 It was a trial on asthmatic children
Grimfeld 2004 The trial used an antihistaminic
Grimm 1999 Results of children and adults are not separated
Heinz 2010 The trial was on adults
Herrera-Basto 1998 The results only compare the effect of pidotimod during the acute phase of ARTIs
Kozhukharova 1987 Trial was not double-blind, placebo-controlled
Lauriello 1990 It was a trial during the acute phase of respiratory infection in children
Luchikhin 2000 Trial was not double-blind, placebo-controlled
Ma 1994 Trial was not double-blind, placebo-controlled
Macchi 2005 Open trial in adults
Makovetskaya 2001 Trial was not double-blind, placebo-controlled
Mora 2010b Trial on acute adenoiditis not on prevention of acute respiratory tract infections
Mueller 1969 It was a study on asthmatic participants
Nespoli 1992 It was a randomized, multicentre trial - it did not include a placebo group but a group without treatment
Obrosova-Serova 1972 Trial was not double-blind, placebo-controlled
Oggiano 1985 It was an open trial on children
Oldini 1990 It was a Ribomunyl trial including adults and children without a separate analysis for each group
Ortega del 2005 It was an acute phase trial
Predy 2005 It is a trial in adults
Prusek 1987 Comparison between IS without placebo group
691Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
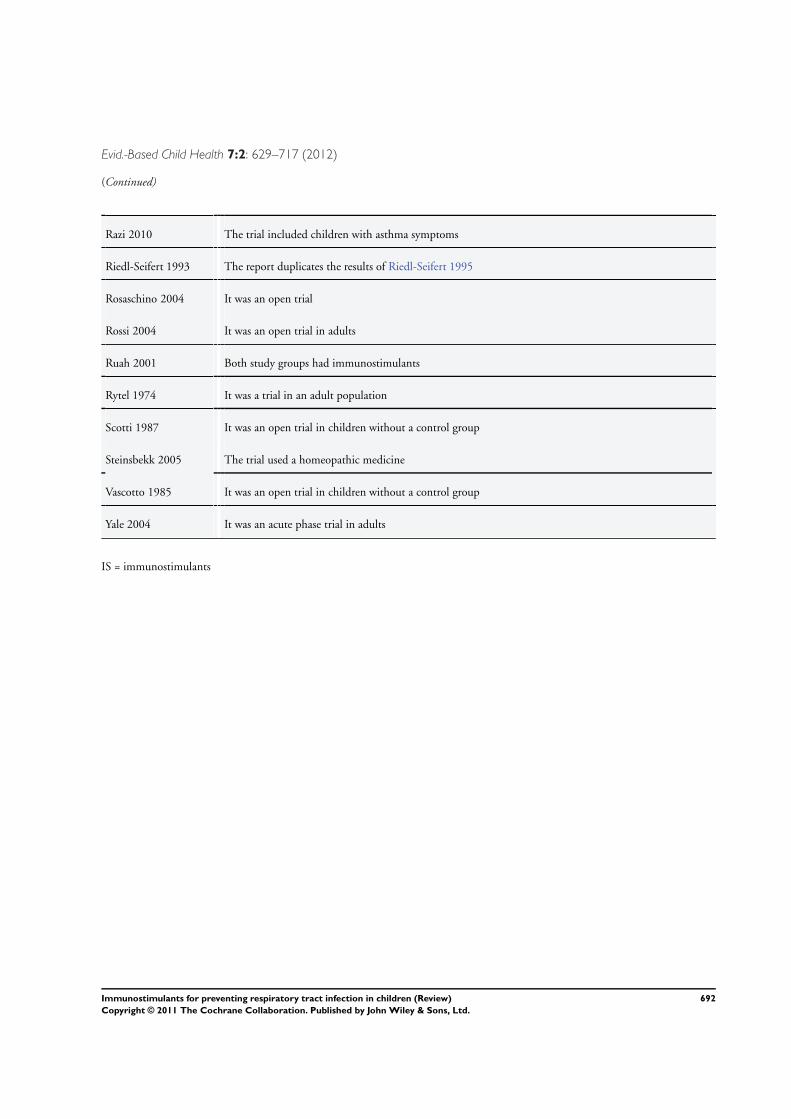
Evid.-Based Child Health 7:2: 629–717 (2012)
(Continued)
Razi 2010 The trial included children with asthma symptoms
Riedl-Seifert 1993 The report duplicates the results of Riedl-Seifert 1995
Rosaschino 2004 It was an open trial
Rossi 2004 It was an open trial in adults
Ruah 2001 Both study groups had immunostimulants
Rytel 1974 It was a trial in an adult population
Scotti 1987 It was an open trial in children without a control group
Steinsbekk 2005 The trial used a homeopathic medicine
Vascotto 1985 It was an open trial in children without a control group
Yale 2004 It was an acute phase trial in adults
IS = immunostimulants
692Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
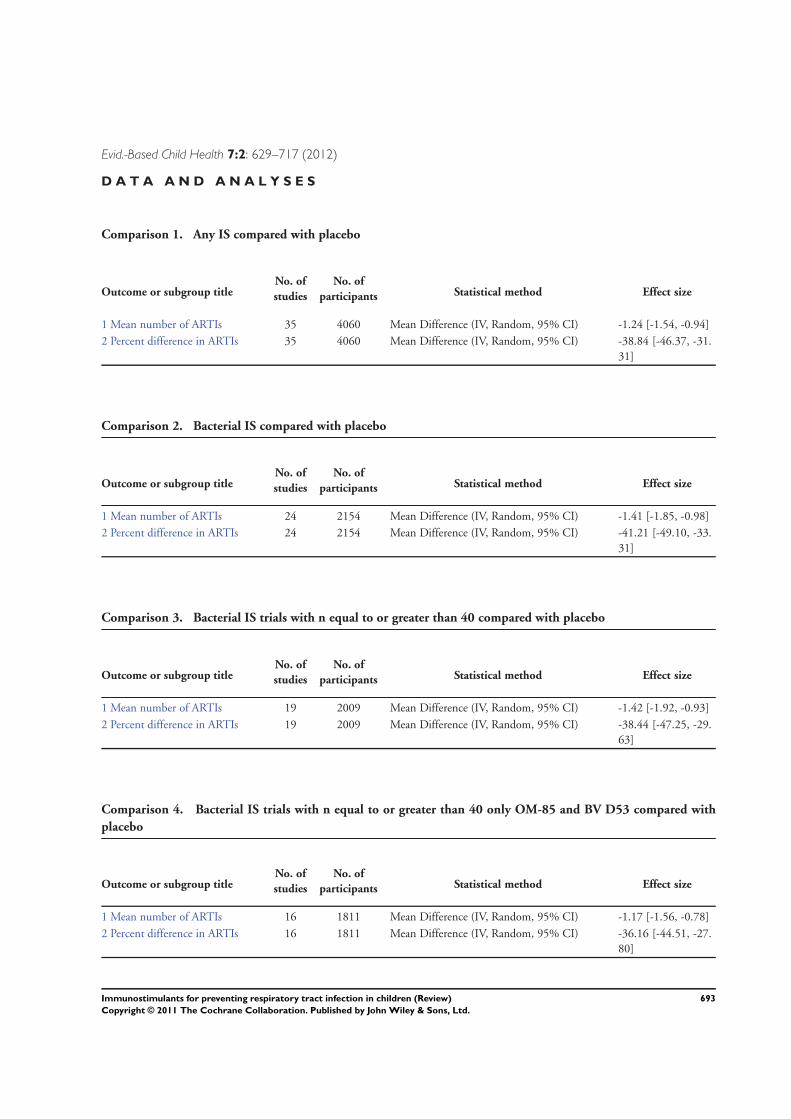
Evid.-Based Child Health 7:2: 629–717 (2012)
D A T A A N D A N A L Y S E S
Comparison 1. Any IS compared with placebo
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mean number of ARTIs 35 4060 Mean Difference (IV, Random, 95% CI) -1.24 [-1.54, -0.94]2 Percent difference in ARTIs 35 4060 Mean Difference (IV, Random, 95% CI) -38.84 [-46.37, -31.
31]
Comparison 2. Bacterial IS compared with placebo
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mean number of ARTIs 24 2154 Mean Difference (IV, Random, 95% CI) -1.41 [-1.85, -0.98]2 Percent difference in ARTIs 24 2154 Mean Difference (IV, Random, 95% CI) -41.21 [-49.10, -33.
31]
Comparison 3. Bacterial IS trials with n equal to or greater than 40 compared with placebo
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mean number of ARTIs 19 2009 Mean Difference (IV, Random, 95% CI) -1.42 [-1.92, -0.93]2 Percent difference in ARTIs 19 2009 Mean Difference (IV, Random, 95% CI) -38.44 [-47.25, -29.
63]
Comparison 4. Bacterial IS trials with n equal to or greater than 40 only OM-85 and BV D53 compared with
placebo
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mean number of ARTIs 16 1811 Mean Difference (IV, Random, 95% CI) -1.17 [-1.56, -0.78]2 Percent difference in ARTIs 16 1811 Mean Difference (IV, Random, 95% CI) -36.16 [-44.51, -27.
80]
693Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
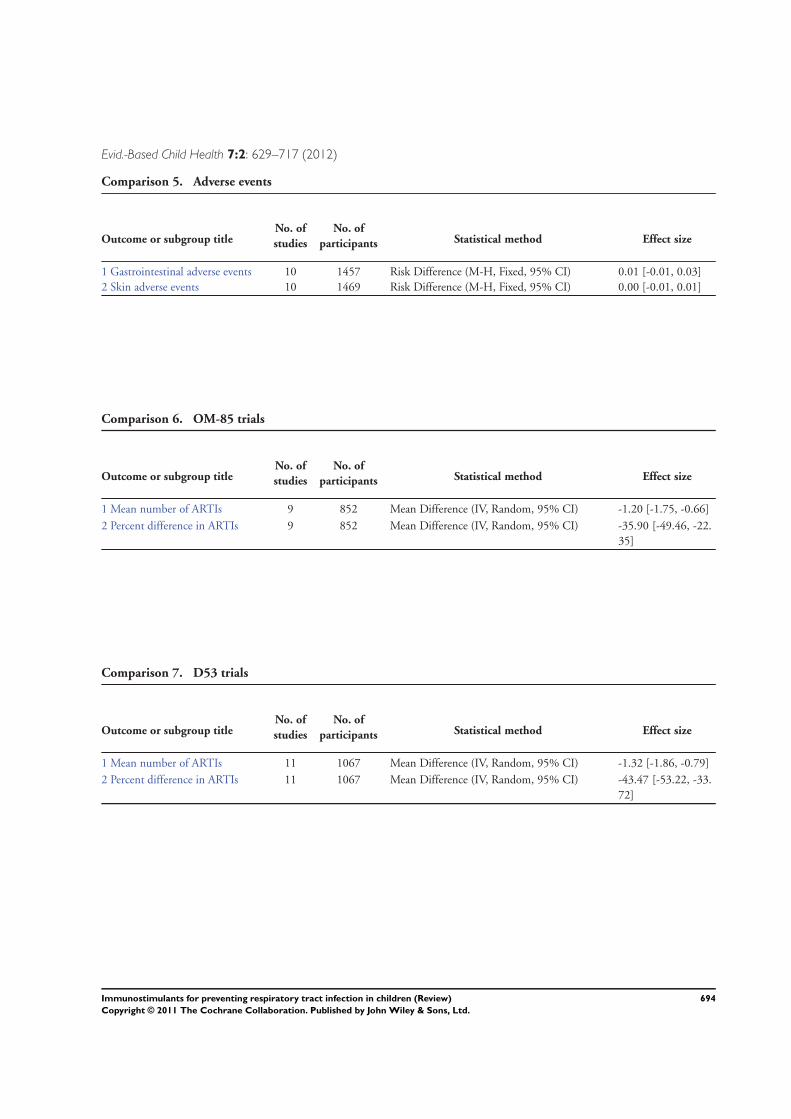
Evid.-Based Child Health 7:2: 629–717 (2012)
Comparison 5. Adverse events
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Gastrointestinal adverse events 10 1457 Risk Difference (M-H, Fixed, 95% CI) 0.01 [-0.01, 0.03]2 Skin adverse events 10 1469 Risk Difference (M-H, Fixed, 95% CI) 0.00 [-0.01, 0.01]
Comparison 6. OM-85 trials
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mean number of ARTIs 9 852 Mean Difference (IV, Random, 95% CI) -1.20 [-1.75, -0.66]2 Percent difference in ARTIs 9 852 Mean Difference (IV, Random, 95% CI) -35.90 [-49.46, -22.
35]
Comparison 7. D53 trials
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Mean number of ARTIs 11 1067 Mean Difference (IV, Random, 95% CI) -1.32 [-1.86, -0.79]2 Percent difference in ARTIs 11 1067 Mean Difference (IV, Random, 95% CI) -43.47 [-53.22, -33.
72]
694Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
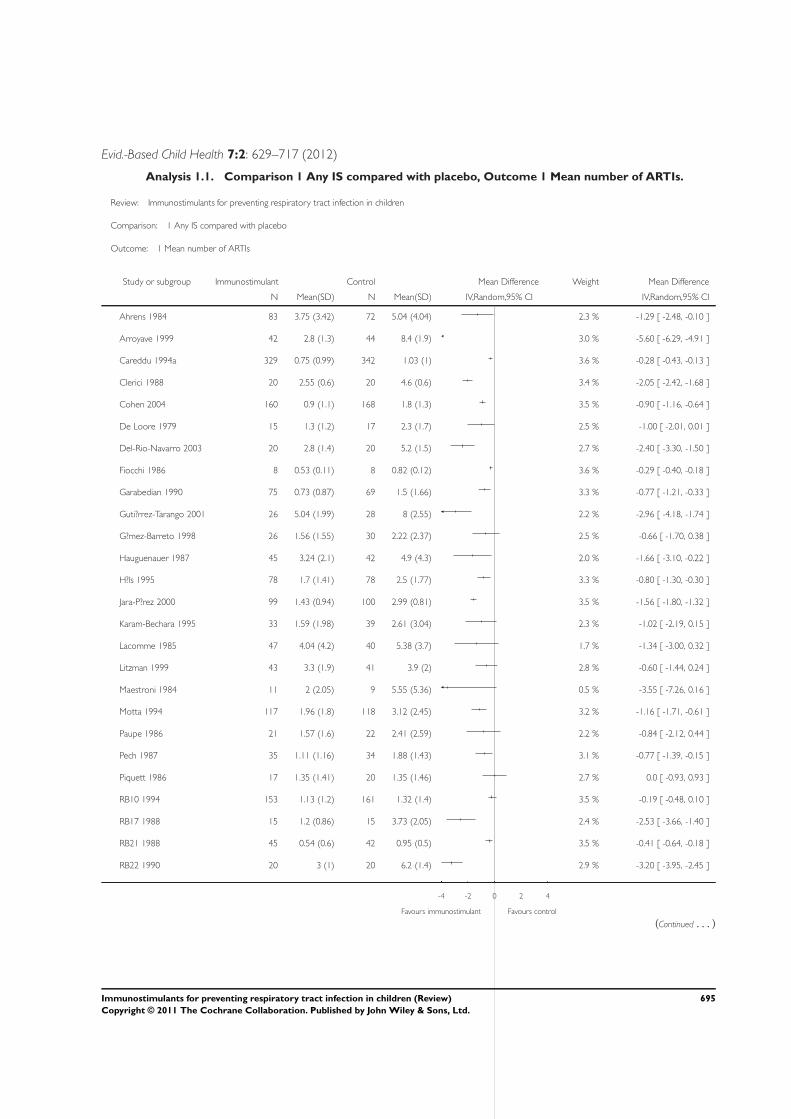
Evid.-Based Child Health 7:2: 629–717 (2012)
Analysis 1.1. Comparison 1 Any IS compared with placebo, Outcome 1 Mean number of ARTIs.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 1 Any IS compared with placebo
Outcome: 1 Mean number of ARTIs
Study or subgroup Immunostimulant Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Ahrens 1984 83 3.75 (3.42) 72 5.04 (4.04) 2.3 % -1.29 [ -2.48, -0.10 ]
Arroyave 1999 42 2.8 (1.3) 44 8.4 (1.9) 3.0 % -5.60 [ -6.29, -4.91 ]
Careddu 1994a 329 0.75 (0.99) 342 1.03 (1) 3.6 % -0.28 [ -0.43, -0.13 ]
Clerici 1988 20 2.55 (0.6) 20 4.6 (0.6) 3.4 % -2.05 [ -2.42, -1.68 ]
Cohen 2004 160 0.9 (1.1) 168 1.8 (1.3) 3.5 % -0.90 [ -1.16, -0.64 ]
De Loore 1979 15 1.3 (1.2) 17 2.3 (1.7) 2.5 % -1.00 [ -2.01, 0.01 ]
Del-Rio-Navarro 2003 20 2.8 (1.4) 20 5.2 (1.5) 2.7 % -2.40 [ -3.30, -1.50 ]
Fiocchi 1986 8 0.53 (0.11) 8 0.82 (0.12) 3.6 % -0.29 [ -0.40, -0.18 ]
Garabedian 1990 75 0.73 (0.87) 69 1.5 (1.66) 3.3 % -0.77 [ -1.21, -0.33 ]
Guti?rrez-Tarango 2001 26 5.04 (1.99) 28 8 (2.55) 2.2 % -2.96 [ -4.18, -1.74 ]
G?mez-Barreto 1998 26 1.56 (1.55) 30 2.22 (2.37) 2.5 % -0.66 [ -1.70, 0.38 ]
Hauguenauer 1987 45 3.24 (2.1) 42 4.9 (4.3) 2.0 % -1.66 [ -3.10, -0.22 ]
H?ls 1995 78 1.7 (1.41) 78 2.5 (1.77) 3.3 % -0.80 [ -1.30, -0.30 ]
Jara-P?rez 2000 99 1.43 (0.94) 100 2.99 (0.81) 3.5 % -1.56 [ -1.80, -1.32 ]
Karam-Bechara 1995 33 1.59 (1.98) 39 2.61 (3.04) 2.3 % -1.02 [ -2.19, 0.15 ]
Lacomme 1985 47 4.04 (4.2) 40 5.38 (3.7) 1.7 % -1.34 [ -3.00, 0.32 ]
Litzman 1999 43 3.3 (1.9) 41 3.9 (2) 2.8 % -0.60 [ -1.44, 0.24 ]
Maestroni 1984 11 2 (2.05) 9 5.55 (5.36) 0.5 % -3.55 [ -7.26, 0.16 ]
Motta 1994 117 1.96 (1.8) 118 3.12 (2.45) 3.2 % -1.16 [ -1.71, -0.61 ]
Paupe 1986 21 1.57 (1.6) 22 2.41 (2.59) 2.2 % -0.84 [ -2.12, 0.44 ]
Pech 1987 35 1.11 (1.16) 34 1.88 (1.43) 3.1 % -0.77 [ -1.39, -0.15 ]
Piquett 1986 17 1.35 (1.41) 20 1.35 (1.46) 2.7 % 0.0 [ -0.93, 0.93 ]
RB10 1994 153 1.13 (1.2) 161 1.32 (1.4) 3.5 % -0.19 [ -0.48, 0.10 ]
RB17 1988 15 1.2 (0.86) 15 3.73 (2.05) 2.4 % -2.53 [ -3.66, -1.40 ]
RB21 1988 45 0.54 (0.6) 42 0.95 (0.5) 3.5 % -0.41 [ -0.64, -0.18 ]
RB22 1990 20 3 (1) 20 6.2 (1.4) 2.9 % -3.20 [ -3.95, -2.45 ]
-4 -2 0 2 4
Favours immunostimulant Favours control
(Continued . . . )
695Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
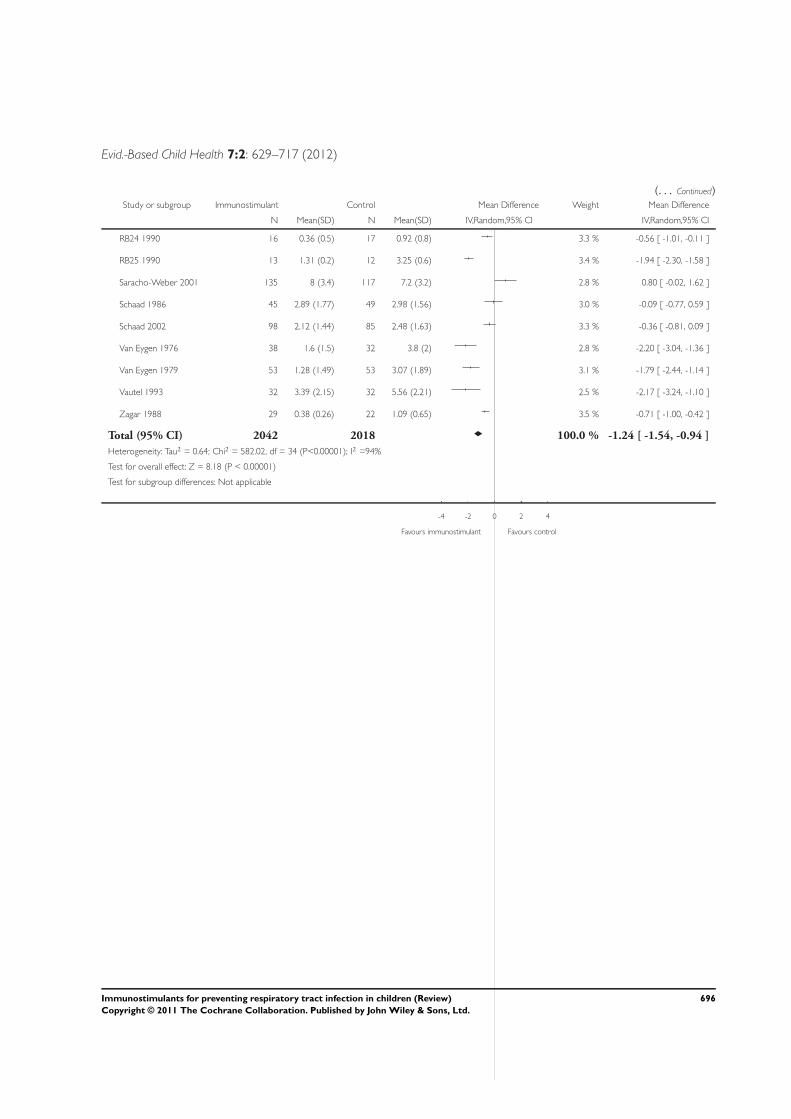
Evid.-Based Child Health 7:2: 629–717 (2012)
(. . . Continued)Study or subgroup Immunostimulant Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
RB24 1990 16 0.36 (0.5) 17 0.92 (0.8) 3.3 % -0.56 [ -1.01, -0.11 ]
RB25 1990 13 1.31 (0.2) 12 3.25 (0.6) 3.4 % -1.94 [ -2.30, -1.58 ]
Saracho-Weber 2001 135 8 (3.4) 117 7.2 (3.2) 2.8 % 0.80 [ -0.02, 1.62 ]
Schaad 1986 45 2.89 (1.77) 49 2.98 (1.56) 3.0 % -0.09 [ -0.77, 0.59 ]
Schaad 2002 98 2.12 (1.44) 85 2.48 (1.63) 3.3 % -0.36 [ -0.81, 0.09 ]
Van Eygen 1976 38 1.6 (1.5) 32 3.8 (2) 2.8 % -2.20 [ -3.04, -1.36 ]
Van Eygen 1979 53 1.28 (1.49) 53 3.07 (1.89) 3.1 % -1.79 [ -2.44, -1.14 ]
Vautel 1993 32 3.39 (2.15) 32 5.56 (2.21) 2.5 % -2.17 [ -3.24, -1.10 ]
Zagar 1988 29 0.38 (0.26) 22 1.09 (0.65) 3.5 % -0.71 [ -1.00, -0.42 ]
Total (95% CI) 2042 2018 100.0 % -1.24 [ -1.54, -0.94 ]
Heterogeneity: Tau2 = 0.64; Chi2 = 582.02, df = 34 (P<0.00001); I2 =94%
Test for overall effect: Z = 8.18 (P < 0.00001)
Test for subgroup differences: Not applicable
-4 -2 0 2 4
Favours immunostimulant Favours control
696Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
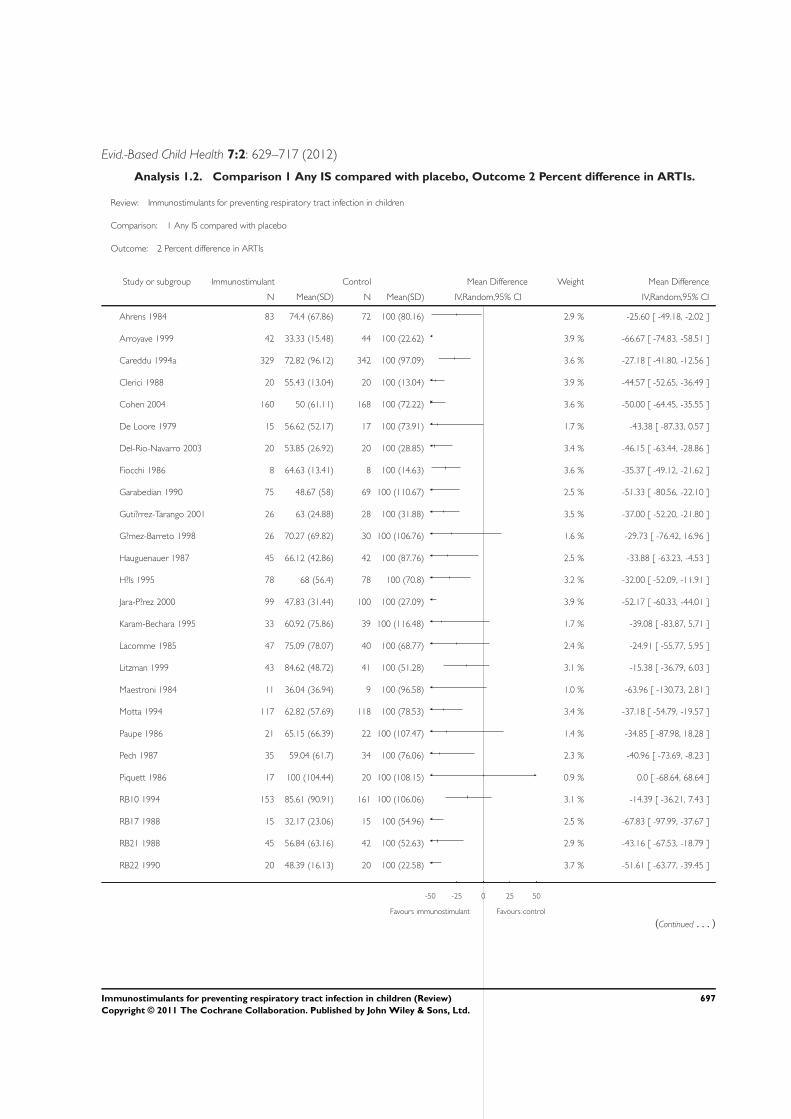
Evid.-Based Child Health 7:2: 629–717 (2012)
Analysis 1.2. Comparison 1 Any IS compared with placebo, Outcome 2 Percent difference in ARTIs.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 1 Any IS compared with placebo
Outcome: 2 Percent difference in ARTIs
Study or subgroup Immunostimulant Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Ahrens 1984 83 74.4 (67.86) 72 100 (80.16) 2.9 % -25.60 [ -49.18, -2.02 ]
Arroyave 1999 42 33.33 (15.48) 44 100 (22.62) 3.9 % -66.67 [ -74.83, -58.51 ]
Careddu 1994a 329 72.82 (96.12) 342 100 (97.09) 3.6 % -27.18 [ -41.80, -12.56 ]
Clerici 1988 20 55.43 (13.04) 20 100 (13.04) 3.9 % -44.57 [ -52.65, -36.49 ]
Cohen 2004 160 50 (61.11) 168 100 (72.22) 3.6 % -50.00 [ -64.45, -35.55 ]
De Loore 1979 15 56.62 (52.17) 17 100 (73.91) 1.7 % -43.38 [ -87.33, 0.57 ]
Del-Rio-Navarro 2003 20 53.85 (26.92) 20 100 (28.85) 3.4 % -46.15 [ -63.44, -28.86 ]
Fiocchi 1986 8 64.63 (13.41) 8 100 (14.63) 3.6 % -35.37 [ -49.12, -21.62 ]
Garabedian 1990 75 48.67 (58) 69 100 (110.67) 2.5 % -51.33 [ -80.56, -22.10 ]
Guti?rrez-Tarango 2001 26 63 (24.88) 28 100 (31.88) 3.5 % -37.00 [ -52.20, -21.80 ]
G?mez-Barreto 1998 26 70.27 (69.82) 30 100 (106.76) 1.6 % -29.73 [ -76.42, 16.96 ]
Hauguenauer 1987 45 66.12 (42.86) 42 100 (87.76) 2.5 % -33.88 [ -63.23, -4.53 ]
H?ls 1995 78 68 (56.4) 78 100 (70.8) 3.2 % -32.00 [ -52.09, -11.91 ]
Jara-P?rez 2000 99 47.83 (31.44) 100 100 (27.09) 3.9 % -52.17 [ -60.33, -44.01 ]
Karam-Bechara 1995 33 60.92 (75.86) 39 100 (116.48) 1.7 % -39.08 [ -83.87, 5.71 ]
Lacomme 1985 47 75.09 (78.07) 40 100 (68.77) 2.4 % -24.91 [ -55.77, 5.95 ]
Litzman 1999 43 84.62 (48.72) 41 100 (51.28) 3.1 % -15.38 [ -36.79, 6.03 ]
Maestroni 1984 11 36.04 (36.94) 9 100 (96.58) 1.0 % -63.96 [ -130.73, 2.81 ]
Motta 1994 117 62.82 (57.69) 118 100 (78.53) 3.4 % -37.18 [ -54.79, -19.57 ]
Paupe 1986 21 65.15 (66.39) 22 100 (107.47) 1.4 % -34.85 [ -87.98, 18.28 ]
Pech 1987 35 59.04 (61.7) 34 100 (76.06) 2.3 % -40.96 [ -73.69, -8.23 ]
Piquett 1986 17 100 (104.44) 20 100 (108.15) 0.9 % 0.0 [ -68.64, 68.64 ]
RB10 1994 153 85.61 (90.91) 161 100 (106.06) 3.1 % -14.39 [ -36.21, 7.43 ]
RB17 1988 15 32.17 (23.06) 15 100 (54.96) 2.5 % -67.83 [ -97.99, -37.67 ]
RB21 1988 45 56.84 (63.16) 42 100 (52.63) 2.9 % -43.16 [ -67.53, -18.79 ]
RB22 1990 20 48.39 (16.13) 20 100 (22.58) 3.7 % -51.61 [ -63.77, -39.45 ]
-50 -25 0 25 50
Favours immunostimulant Favours control
(Continued . . . )
697Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
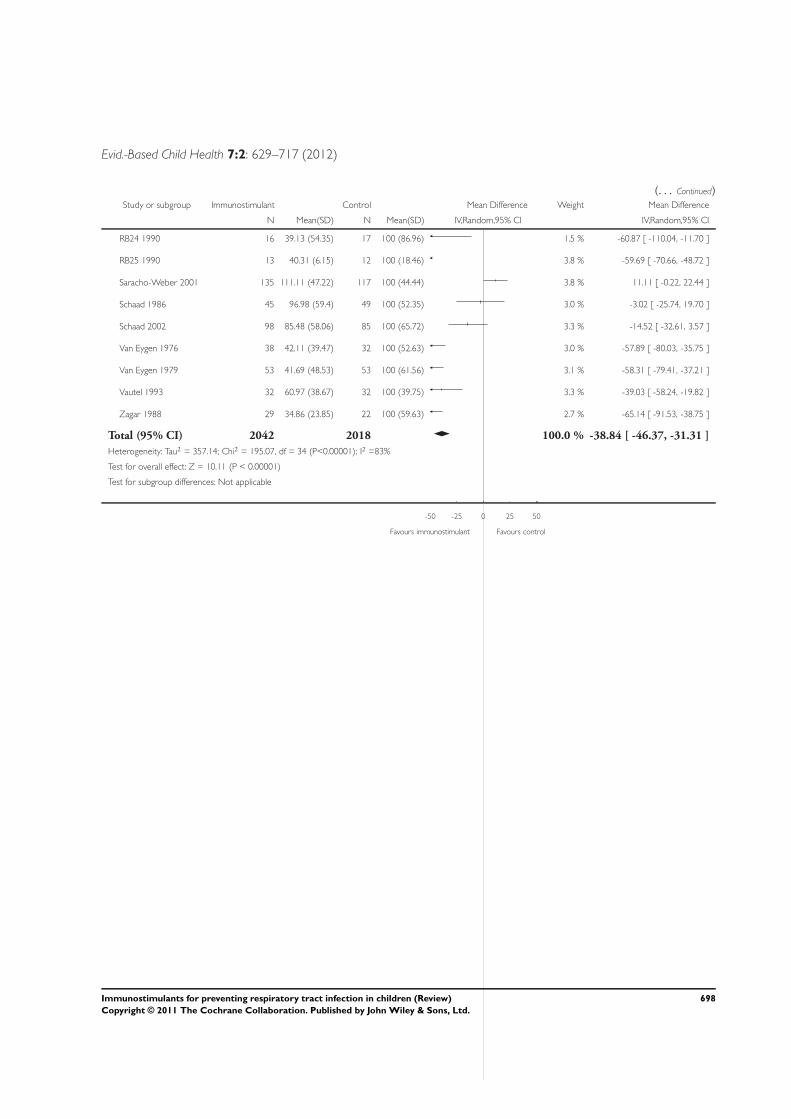
Evid.-Based Child Health 7:2: 629–717 (2012)
(. . . Continued)Study or subgroup Immunostimulant Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
RB24 1990 16 39.13 (54.35) 17 100 (86.96) 1.5 % -60.87 [ -110.04, -11.70 ]
RB25 1990 13 40.31 (6.15) 12 100 (18.46) 3.8 % -59.69 [ -70.66, -48.72 ]
Saracho-Weber 2001 135 111.11 (47.22) 117 100 (44.44) 3.8 % 11.11 [ -0.22, 22.44 ]
Schaad 1986 45 96.98 (59.4) 49 100 (52.35) 3.0 % -3.02 [ -25.74, 19.70 ]
Schaad 2002 98 85.48 (58.06) 85 100 (65.72) 3.3 % -14.52 [ -32.61, 3.57 ]
Van Eygen 1976 38 42.11 (39.47) 32 100 (52.63) 3.0 % -57.89 [ -80.03, -35.75 ]
Van Eygen 1979 53 41.69 (48.53) 53 100 (61.56) 3.1 % -58.31 [ -79.41, -37.21 ]
Vautel 1993 32 60.97 (38.67) 32 100 (39.75) 3.3 % -39.03 [ -58.24, -19.82 ]
Zagar 1988 29 34.86 (23.85) 22 100 (59.63) 2.7 % -65.14 [ -91.53, -38.75 ]
Total (95% CI) 2042 2018 100.0 % -38.84 [ -46.37, -31.31 ]
Heterogeneity: Tau2 = 357.14; Chi2 = 195.07, df = 34 (P<0.00001); I2 =83%
Test for overall effect: Z = 10.11 (P < 0.00001)
Test for subgroup differences: Not applicable
-50 -25 0 25 50
Favours immunostimulant Favours control
698Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
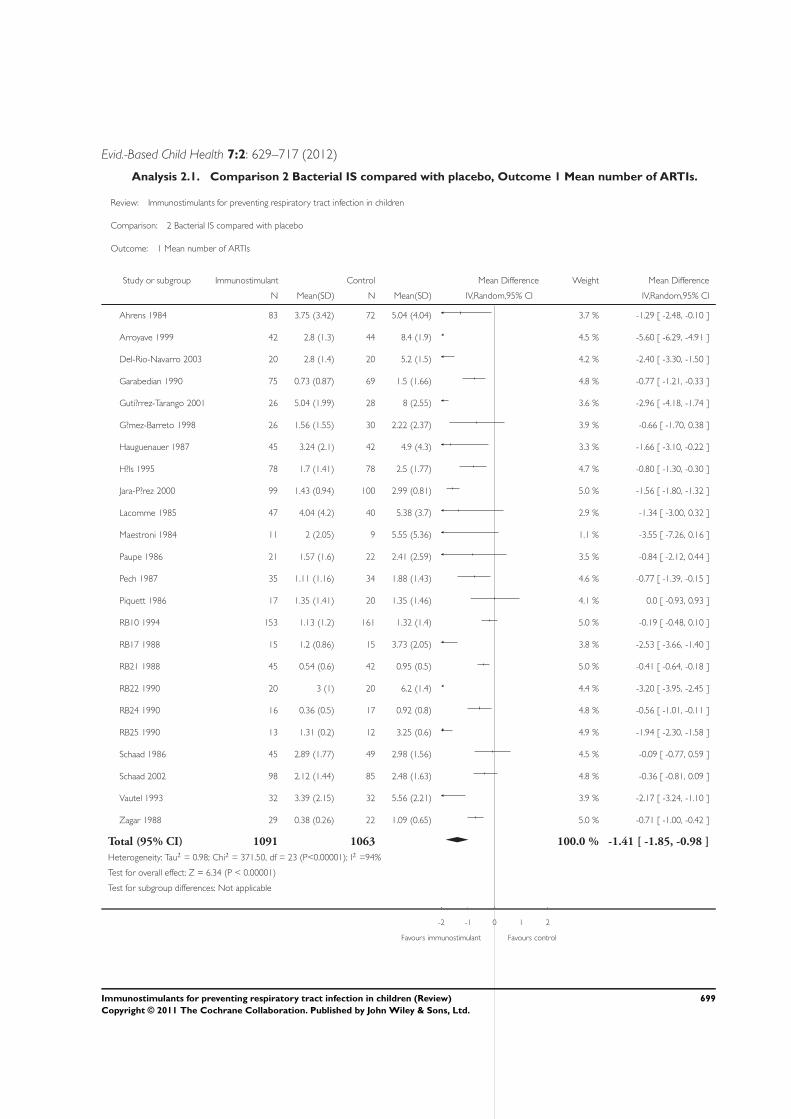
Evid.-Based Child Health 7:2: 629–717 (2012)
Analysis 2.1. Comparison 2 Bacterial IS compared with placebo, Outcome 1 Mean number of ARTIs.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 2 Bacterial IS compared with placebo
Outcome: 1 Mean number of ARTIs
Study or subgroup Immunostimulant Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Ahrens 1984 83 3.75 (3.42) 72 5.04 (4.04) 3.7 % -1.29 [ -2.48, -0.10 ]
Arroyave 1999 42 2.8 (1.3) 44 8.4 (1.9) 4.5 % -5.60 [ -6.29, -4.91 ]
Del-Rio-Navarro 2003 20 2.8 (1.4) 20 5.2 (1.5) 4.2 % -2.40 [ -3.30, -1.50 ]
Garabedian 1990 75 0.73 (0.87) 69 1.5 (1.66) 4.8 % -0.77 [ -1.21, -0.33 ]
Guti?rrez-Tarango 2001 26 5.04 (1.99) 28 8 (2.55) 3.6 % -2.96 [ -4.18, -1.74 ]
G?mez-Barreto 1998 26 1.56 (1.55) 30 2.22 (2.37) 3.9 % -0.66 [ -1.70, 0.38 ]
Hauguenauer 1987 45 3.24 (2.1) 42 4.9 (4.3) 3.3 % -1.66 [ -3.10, -0.22 ]
H?ls 1995 78 1.7 (1.41) 78 2.5 (1.77) 4.7 % -0.80 [ -1.30, -0.30 ]
Jara-P?rez 2000 99 1.43 (0.94) 100 2.99 (0.81) 5.0 % -1.56 [ -1.80, -1.32 ]
Lacomme 1985 47 4.04 (4.2) 40 5.38 (3.7) 2.9 % -1.34 [ -3.00, 0.32 ]
Maestroni 1984 11 2 (2.05) 9 5.55 (5.36) 1.1 % -3.55 [ -7.26, 0.16 ]
Paupe 1986 21 1.57 (1.6) 22 2.41 (2.59) 3.5 % -0.84 [ -2.12, 0.44 ]
Pech 1987 35 1.11 (1.16) 34 1.88 (1.43) 4.6 % -0.77 [ -1.39, -0.15 ]
Piquett 1986 17 1.35 (1.41) 20 1.35 (1.46) 4.1 % 0.0 [ -0.93, 0.93 ]
RB10 1994 153 1.13 (1.2) 161 1.32 (1.4) 5.0 % -0.19 [ -0.48, 0.10 ]
RB17 1988 15 1.2 (0.86) 15 3.73 (2.05) 3.8 % -2.53 [ -3.66, -1.40 ]
RB21 1988 45 0.54 (0.6) 42 0.95 (0.5) 5.0 % -0.41 [ -0.64, -0.18 ]
RB22 1990 20 3 (1) 20 6.2 (1.4) 4.4 % -3.20 [ -3.95, -2.45 ]
RB24 1990 16 0.36 (0.5) 17 0.92 (0.8) 4.8 % -0.56 [ -1.01, -0.11 ]
RB25 1990 13 1.31 (0.2) 12 3.25 (0.6) 4.9 % -1.94 [ -2.30, -1.58 ]
Schaad 1986 45 2.89 (1.77) 49 2.98 (1.56) 4.5 % -0.09 [ -0.77, 0.59 ]
Schaad 2002 98 2.12 (1.44) 85 2.48 (1.63) 4.8 % -0.36 [ -0.81, 0.09 ]
Vautel 1993 32 3.39 (2.15) 32 5.56 (2.21) 3.9 % -2.17 [ -3.24, -1.10 ]
Zagar 1988 29 0.38 (0.26) 22 1.09 (0.65) 5.0 % -0.71 [ -1.00, -0.42 ]
Total (95% CI) 1091 1063 100.0 % -1.41 [ -1.85, -0.98 ]
Heterogeneity: Tau2 = 0.98; Chi2 = 371.50, df = 23 (P<0.00001); I2 =94%
Test for overall effect: Z = 6.34 (P < 0.00001)
Test for subgroup differences: Not applicable
-2 -1 0 1 2
Favours immunostimulant Favours control
699Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
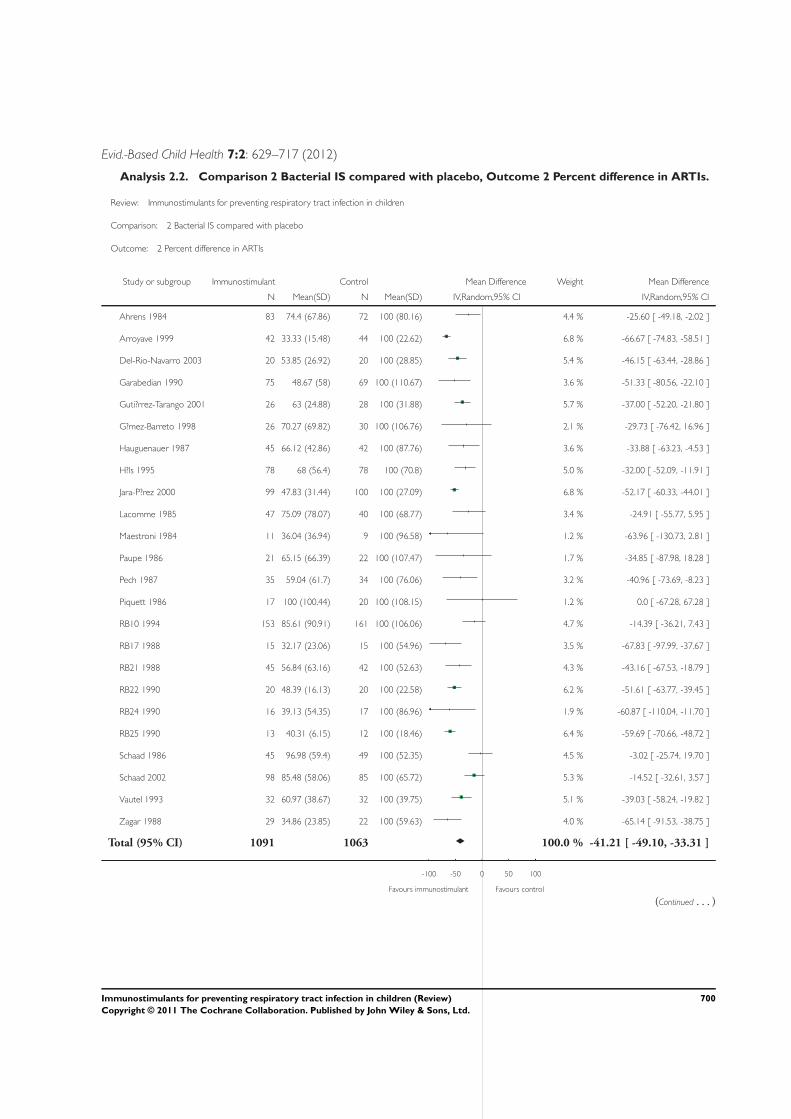
Evid.-Based Child Health 7:2: 629–717 (2012)
Analysis 2.2. Comparison 2 Bacterial IS compared with placebo, Outcome 2 Percent difference in ARTIs.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 2 Bacterial IS compared with placebo
Outcome: 2 Percent difference in ARTIs
Study or subgroup Immunostimulant Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Ahrens 1984 83 74.4 (67.86) 72 100 (80.16) 4.4 % -25.60 [ -49.18, -2.02 ]
Arroyave 1999 42 33.33 (15.48) 44 100 (22.62) 6.8 % -66.67 [ -74.83, -58.51 ]
Del-Rio-Navarro 2003 20 53.85 (26.92) 20 100 (28.85) 5.4 % -46.15 [ -63.44, -28.86 ]
Garabedian 1990 75 48.67 (58) 69 100 (110.67) 3.6 % -51.33 [ -80.56, -22.10 ]
Guti?rrez-Tarango 2001 26 63 (24.88) 28 100 (31.88) 5.7 % -37.00 [ -52.20, -21.80 ]
G?mez-Barreto 1998 26 70.27 (69.82) 30 100 (106.76) 2.1 % -29.73 [ -76.42, 16.96 ]
Hauguenauer 1987 45 66.12 (42.86) 42 100 (87.76) 3.6 % -33.88 [ -63.23, -4.53 ]
H?ls 1995 78 68 (56.4) 78 100 (70.8) 5.0 % -32.00 [ -52.09, -11.91 ]
Jara-P?rez 2000 99 47.83 (31.44) 100 100 (27.09) 6.8 % -52.17 [ -60.33, -44.01 ]
Lacomme 1985 47 75.09 (78.07) 40 100 (68.77) 3.4 % -24.91 [ -55.77, 5.95 ]
Maestroni 1984 11 36.04 (36.94) 9 100 (96.58) 1.2 % -63.96 [ -130.73, 2.81 ]
Paupe 1986 21 65.15 (66.39) 22 100 (107.47) 1.7 % -34.85 [ -87.98, 18.28 ]
Pech 1987 35 59.04 (61.7) 34 100 (76.06) 3.2 % -40.96 [ -73.69, -8.23 ]
Piquett 1986 17 100 (100.44) 20 100 (108.15) 1.2 % 0.0 [ -67.28, 67.28 ]
RB10 1994 153 85.61 (90.91) 161 100 (106.06) 4.7 % -14.39 [ -36.21, 7.43 ]
RB17 1988 15 32.17 (23.06) 15 100 (54.96) 3.5 % -67.83 [ -97.99, -37.67 ]
RB21 1988 45 56.84 (63.16) 42 100 (52.63) 4.3 % -43.16 [ -67.53, -18.79 ]
RB22 1990 20 48.39 (16.13) 20 100 (22.58) 6.2 % -51.61 [ -63.77, -39.45 ]
RB24 1990 16 39.13 (54.35) 17 100 (86.96) 1.9 % -60.87 [ -110.04, -11.70 ]
RB25 1990 13 40.31 (6.15) 12 100 (18.46) 6.4 % -59.69 [ -70.66, -48.72 ]
Schaad 1986 45 96.98 (59.4) 49 100 (52.35) 4.5 % -3.02 [ -25.74, 19.70 ]
Schaad 2002 98 85.48 (58.06) 85 100 (65.72) 5.3 % -14.52 [ -32.61, 3.57 ]
Vautel 1993 32 60.97 (38.67) 32 100 (39.75) 5.1 % -39.03 [ -58.24, -19.82 ]
Zagar 1988 29 34.86 (23.85) 22 100 (59.63) 4.0 % -65.14 [ -91.53, -38.75 ]
Total (95% CI) 1091 1063 100.0 % -41.21 [ -49.10, -33.31 ]
-100 -50 0 50 100
Favours immunostimulant Favours control
(Continued . . . )
700Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
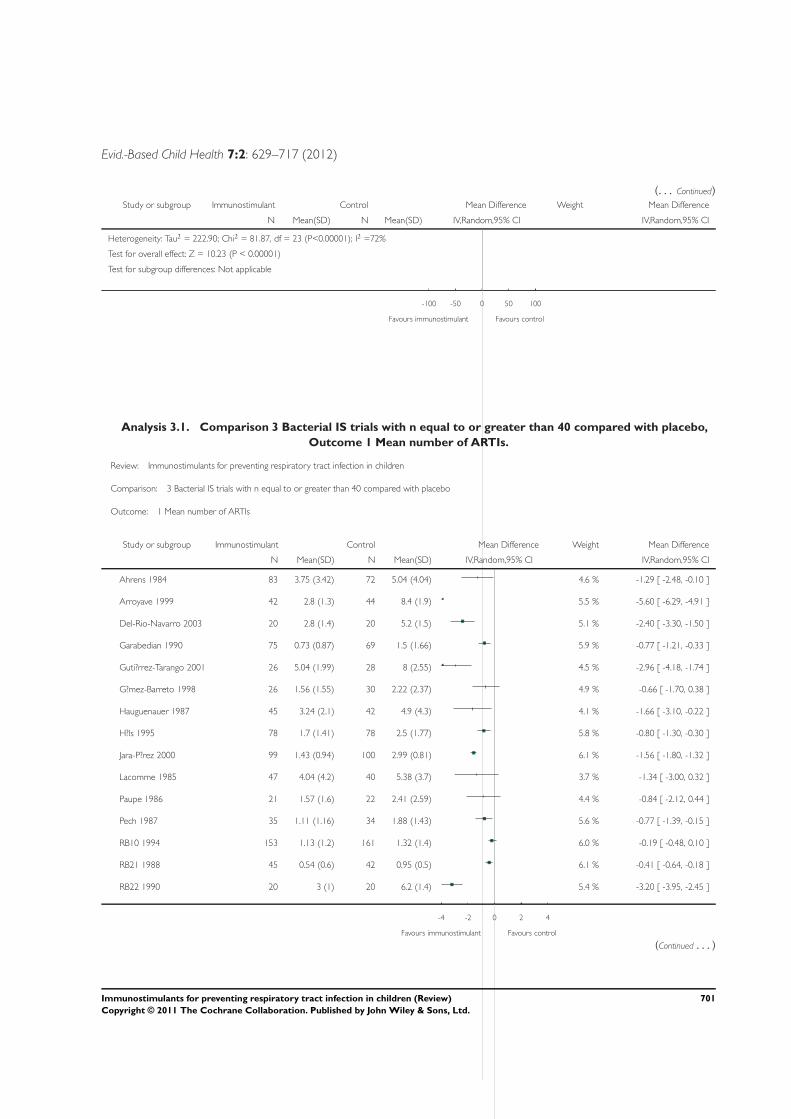
Evid.-Based Child Health 7:2: 629–717 (2012)
(. . . Continued)Study or subgroup Immunostimulant Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Heterogeneity: Tau2 = 222.90; Chi2 = 81.87, df = 23 (P<0.00001); I2 =72%
Test for overall effect: Z = 10.23 (P < 0.00001)
Test for subgroup differences: Not applicable
-100 -50 0 50 100
Favours immunostimulant Favours control
Analysis 3.1. Comparison 3 Bacterial IS trials with n equal to or greater than 40 compared with placebo,
Outcome 1 Mean number of ARTIs.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 3 Bacterial IS trials with n equal to or greater than 40 compared with placebo
Outcome: 1 Mean number of ARTIs
Study or subgroup Immunostimulant Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Ahrens 1984 83 3.75 (3.42) 72 5.04 (4.04) 4.6 % -1.29 [ -2.48, -0.10 ]
Arroyave 1999 42 2.8 (1.3) 44 8.4 (1.9) 5.5 % -5.60 [ -6.29, -4.91 ]
Del-Rio-Navarro 2003 20 2.8 (1.4) 20 5.2 (1.5) 5.1 % -2.40 [ -3.30, -1.50 ]
Garabedian 1990 75 0.73 (0.87) 69 1.5 (1.66) 5.9 % -0.77 [ -1.21, -0.33 ]
Guti?rrez-Tarango 2001 26 5.04 (1.99) 28 8 (2.55) 4.5 % -2.96 [ -4.18, -1.74 ]
G?mez-Barreto 1998 26 1.56 (1.55) 30 2.22 (2.37) 4.9 % -0.66 [ -1.70, 0.38 ]
Hauguenauer 1987 45 3.24 (2.1) 42 4.9 (4.3) 4.1 % -1.66 [ -3.10, -0.22 ]
H?ls 1995 78 1.7 (1.41) 78 2.5 (1.77) 5.8 % -0.80 [ -1.30, -0.30 ]
Jara-P?rez 2000 99 1.43 (0.94) 100 2.99 (0.81) 6.1 % -1.56 [ -1.80, -1.32 ]
Lacomme 1985 47 4.04 (4.2) 40 5.38 (3.7) 3.7 % -1.34 [ -3.00, 0.32 ]
Paupe 1986 21 1.57 (1.6) 22 2.41 (2.59) 4.4 % -0.84 [ -2.12, 0.44 ]
Pech 1987 35 1.11 (1.16) 34 1.88 (1.43) 5.6 % -0.77 [ -1.39, -0.15 ]
RB10 1994 153 1.13 (1.2) 161 1.32 (1.4) 6.0 % -0.19 [ -0.48, 0.10 ]
RB21 1988 45 0.54 (0.6) 42 0.95 (0.5) 6.1 % -0.41 [ -0.64, -0.18 ]
RB22 1990 20 3 (1) 20 6.2 (1.4) 5.4 % -3.20 [ -3.95, -2.45 ]
-4 -2 0 2 4
Favours immunostimulant Favours control
(Continued . . . )
701Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
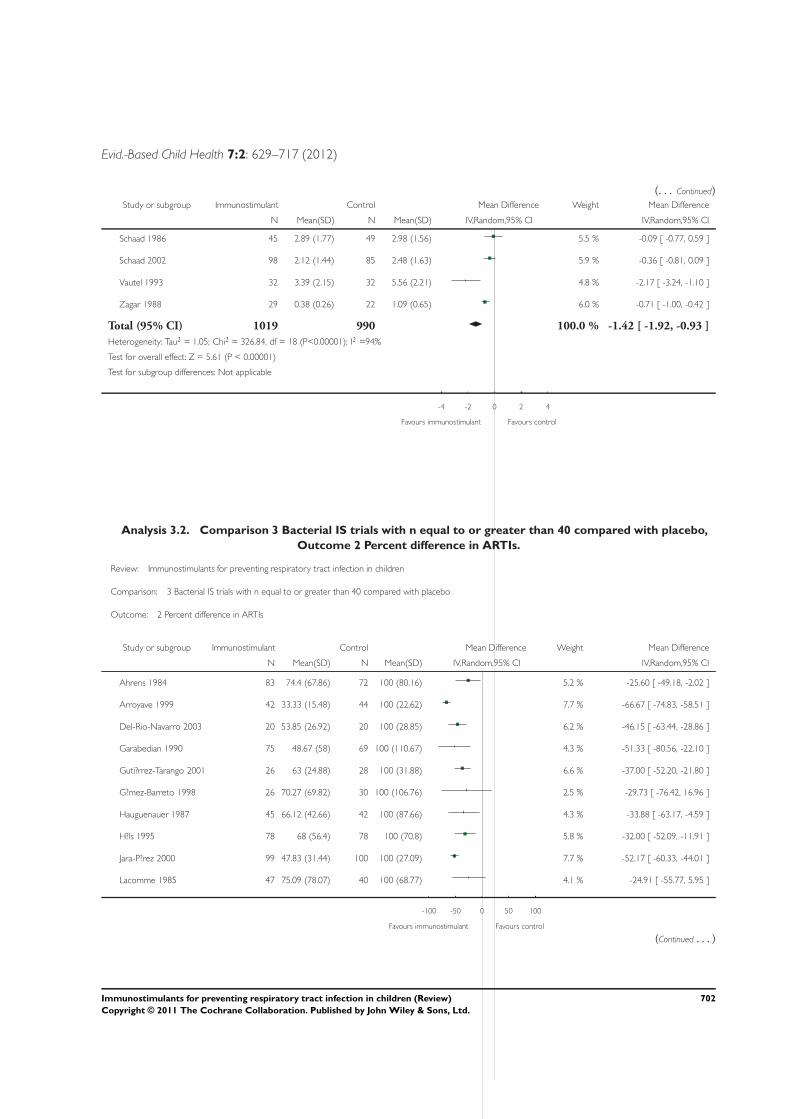
Evid.-Based Child Health 7:2: 629–717 (2012)
(. . . Continued)Study or subgroup Immunostimulant Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Schaad 1986 45 2.89 (1.77) 49 2.98 (1.56) 5.5 % -0.09 [ -0.77, 0.59 ]
Schaad 2002 98 2.12 (1.44) 85 2.48 (1.63) 5.9 % -0.36 [ -0.81, 0.09 ]
Vautel 1993 32 3.39 (2.15) 32 5.56 (2.21) 4.8 % -2.17 [ -3.24, -1.10 ]
Zagar 1988 29 0.38 (0.26) 22 1.09 (0.65) 6.0 % -0.71 [ -1.00, -0.42 ]
Total (95% CI) 1019 990 100.0 % -1.42 [ -1.92, -0.93 ]
Heterogeneity: Tau2 = 1.05; Chi2 = 326.84, df = 18 (P<0.00001); I2 =94%
Test for overall effect: Z = 5.61 (P < 0.00001)
Test for subgroup differences: Not applicable
-4 -2 0 2 4
Favours immunostimulant Favours control
Analysis 3.2. Comparison 3 Bacterial IS trials with n equal to or greater than 40 compared with placebo,
Outcome 2 Percent difference in ARTIs.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 3 Bacterial IS trials with n equal to or greater than 40 compared with placebo
Outcome: 2 Percent difference in ARTIs
Study or subgroup Immunostimulant Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Ahrens 1984 83 74.4 (67.86) 72 100 (80.16) 5.2 % -25.60 [ -49.18, -2.02 ]
Arroyave 1999 42 33.33 (15.48) 44 100 (22.62) 7.7 % -66.67 [ -74.83, -58.51 ]
Del-Rio-Navarro 2003 20 53.85 (26.92) 20 100 (28.85) 6.2 % -46.15 [ -63.44, -28.86 ]
Garabedian 1990 75 48.67 (58) 69 100 (110.67) 4.3 % -51.33 [ -80.56, -22.10 ]
Guti?rrez-Tarango 2001 26 63 (24.88) 28 100 (31.88) 6.6 % -37.00 [ -52.20, -21.80 ]
G?mez-Barreto 1998 26 70.27 (69.82) 30 100 (106.76) 2.5 % -29.73 [ -76.42, 16.96 ]
Hauguenauer 1987 45 66.12 (42.66) 42 100 (87.66) 4.3 % -33.88 [ -63.17, -4.59 ]
H?ls 1995 78 68 (56.4) 78 100 (70.8) 5.8 % -32.00 [ -52.09, -11.91 ]
Jara-P?rez 2000 99 47.83 (31.44) 100 100 (27.09) 7.7 % -52.17 [ -60.33, -44.01 ]
Lacomme 1985 47 75.09 (78.07) 40 100 (68.77) 4.1 % -24.91 [ -55.77, 5.95 ]
-100 -50 0 50 100
Favours immunostimulant Favours control
(Continued . . . )
702Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
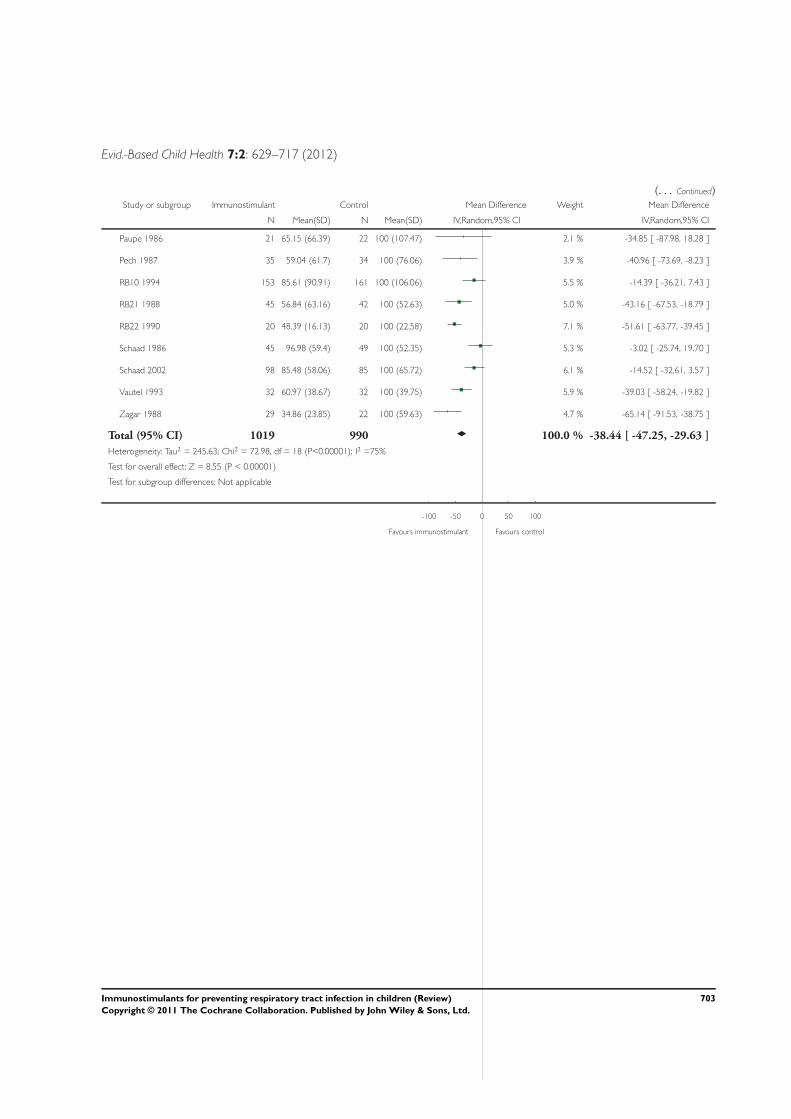
Evid.-Based Child Health 7:2: 629–717 (2012)
(. . . Continued)Study or subgroup Immunostimulant Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Paupe 1986 21 65.15 (66.39) 22 100 (107.47) 2.1 % -34.85 [ -87.98, 18.28 ]
Pech 1987 35 59.04 (61.7) 34 100 (76.06) 3.9 % -40.96 [ -73.69, -8.23 ]
RB10 1994 153 85.61 (90.91) 161 100 (106.06) 5.5 % -14.39 [ -36.21, 7.43 ]
RB21 1988 45 56.84 (63.16) 42 100 (52.63) 5.0 % -43.16 [ -67.53, -18.79 ]
RB22 1990 20 48.39 (16.13) 20 100 (22.58) 7.1 % -51.61 [ -63.77, -39.45 ]
Schaad 1986 45 96.98 (59.4) 49 100 (52.35) 5.3 % -3.02 [ -25.74, 19.70 ]
Schaad 2002 98 85.48 (58.06) 85 100 (65.72) 6.1 % -14.52 [ -32.61, 3.57 ]
Vautel 1993 32 60.97 (38.67) 32 100 (39.75) 5.9 % -39.03 [ -58.24, -19.82 ]
Zagar 1988 29 34.86 (23.85) 22 100 (59.63) 4.7 % -65.14 [ -91.53, -38.75 ]
Total (95% CI) 1019 990 100.0 % -38.44 [ -47.25, -29.63 ]
Heterogeneity: Tau2 = 245.63; Chi2 = 72.98, df = 18 (P<0.00001); I2 =75%
Test for overall effect: Z = 8.55 (P < 0.00001)
Test for subgroup differences: Not applicable
-100 -50 0 50 100
Favours immunostimulant Favours control
703Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
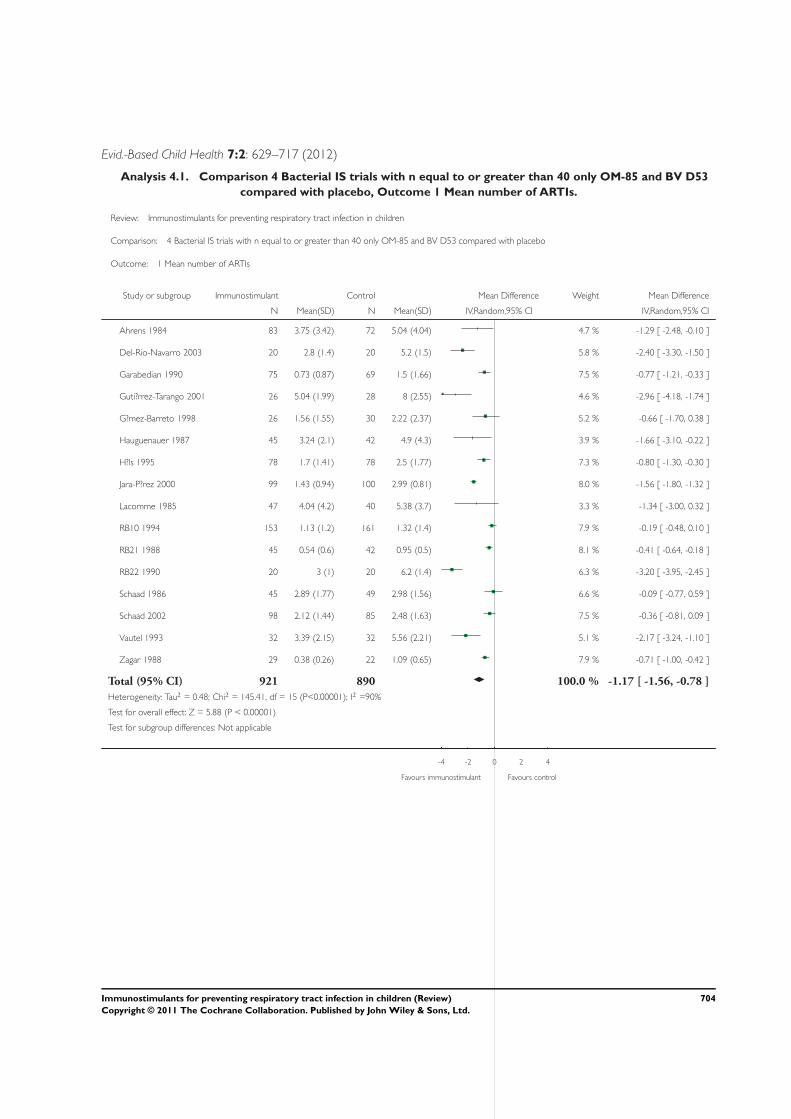
Evid.-Based Child Health 7:2: 629–717 (2012)
Analysis 4.1. Comparison 4 Bacterial IS trials with n equal to or greater than 40 only OM-85 and BV D53
compared with placebo, Outcome 1 Mean number of ARTIs.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 4 Bacterial IS trials with n equal to or greater than 40 only OM-85 and BV D53 compared with placebo
Outcome: 1 Mean number of ARTIs
Study or subgroup Immunostimulant Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Ahrens 1984 83 3.75 (3.42) 72 5.04 (4.04) 4.7 % -1.29 [ -2.48, -0.10 ]
Del-Rio-Navarro 2003 20 2.8 (1.4) 20 5.2 (1.5) 5.8 % -2.40 [ -3.30, -1.50 ]
Garabedian 1990 75 0.73 (0.87) 69 1.5 (1.66) 7.5 % -0.77 [ -1.21, -0.33 ]
Guti?rrez-Tarango 2001 26 5.04 (1.99) 28 8 (2.55) 4.6 % -2.96 [ -4.18, -1.74 ]
G?mez-Barreto 1998 26 1.56 (1.55) 30 2.22 (2.37) 5.2 % -0.66 [ -1.70, 0.38 ]
Hauguenauer 1987 45 3.24 (2.1) 42 4.9 (4.3) 3.9 % -1.66 [ -3.10, -0.22 ]
H?ls 1995 78 1.7 (1.41) 78 2.5 (1.77) 7.3 % -0.80 [ -1.30, -0.30 ]
Jara-P?rez 2000 99 1.43 (0.94) 100 2.99 (0.81) 8.0 % -1.56 [ -1.80, -1.32 ]
Lacomme 1985 47 4.04 (4.2) 40 5.38 (3.7) 3.3 % -1.34 [ -3.00, 0.32 ]
RB10 1994 153 1.13 (1.2) 161 1.32 (1.4) 7.9 % -0.19 [ -0.48, 0.10 ]
RB21 1988 45 0.54 (0.6) 42 0.95 (0.5) 8.1 % -0.41 [ -0.64, -0.18 ]
RB22 1990 20 3 (1) 20 6.2 (1.4) 6.3 % -3.20 [ -3.95, -2.45 ]
Schaad 1986 45 2.89 (1.77) 49 2.98 (1.56) 6.6 % -0.09 [ -0.77, 0.59 ]
Schaad 2002 98 2.12 (1.44) 85 2.48 (1.63) 7.5 % -0.36 [ -0.81, 0.09 ]
Vautel 1993 32 3.39 (2.15) 32 5.56 (2.21) 5.1 % -2.17 [ -3.24, -1.10 ]
Zagar 1988 29 0.38 (0.26) 22 1.09 (0.65) 7.9 % -0.71 [ -1.00, -0.42 ]
Total (95% CI) 921 890 100.0 % -1.17 [ -1.56, -0.78 ]
Heterogeneity: Tau2 = 0.48; Chi2 = 145.41, df = 15 (P<0.00001); I2 =90%
Test for overall effect: Z = 5.88 (P < 0.00001)
Test for subgroup differences: Not applicable
-4 -2 0 2 4
Favours immunostimulant Favours control
704Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
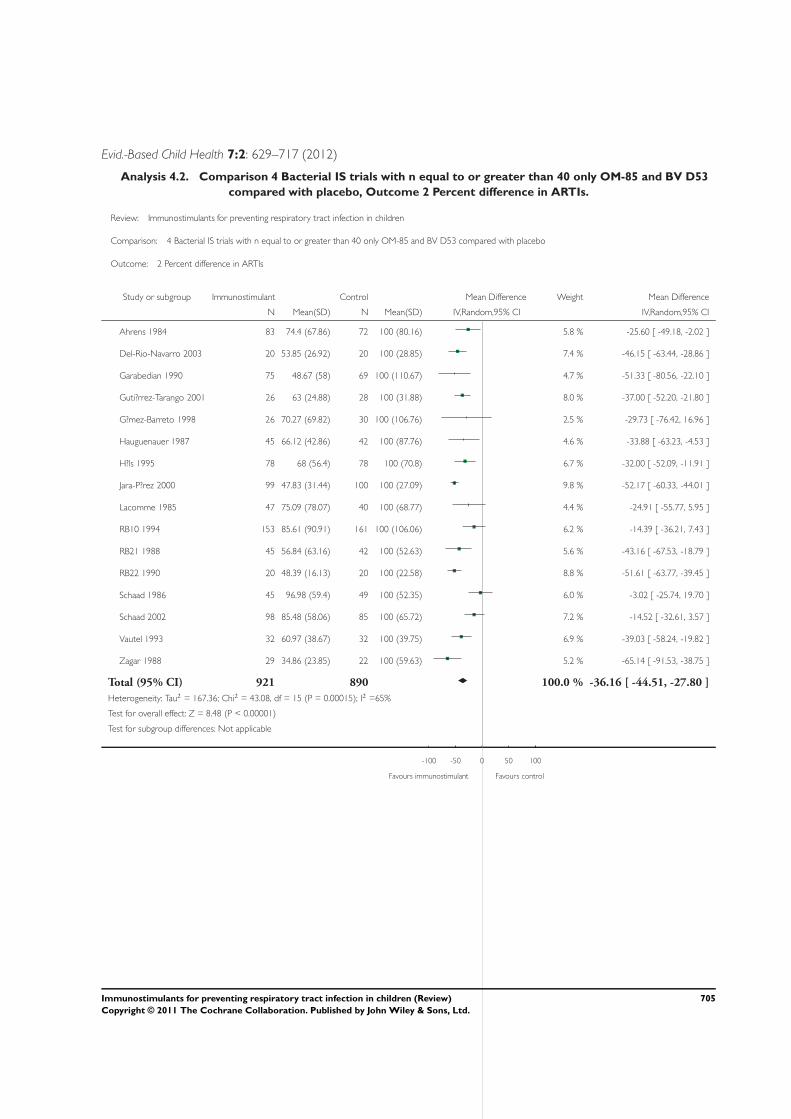
Evid.-Based Child Health 7:2: 629–717 (2012)
Analysis 4.2. Comparison 4 Bacterial IS trials with n equal to or greater than 40 only OM-85 and BV D53
compared with placebo, Outcome 2 Percent difference in ARTIs.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 4 Bacterial IS trials with n equal to or greater than 40 only OM-85 and BV D53 compared with placebo
Outcome: 2 Percent difference in ARTIs
Study or subgroup Immunostimulant Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Ahrens 1984 83 74.4 (67.86) 72 100 (80.16) 5.8 % -25.60 [ -49.18, -2.02 ]
Del-Rio-Navarro 2003 20 53.85 (26.92) 20 100 (28.85) 7.4 % -46.15 [ -63.44, -28.86 ]
Garabedian 1990 75 48.67 (58) 69 100 (110.67) 4.7 % -51.33 [ -80.56, -22.10 ]
Guti?rrez-Tarango 2001 26 63 (24.88) 28 100 (31.88) 8.0 % -37.00 [ -52.20, -21.80 ]
G?mez-Barreto 1998 26 70.27 (69.82) 30 100 (106.76) 2.5 % -29.73 [ -76.42, 16.96 ]
Hauguenauer 1987 45 66.12 (42.86) 42 100 (87.76) 4.6 % -33.88 [ -63.23, -4.53 ]
H?ls 1995 78 68 (56.4) 78 100 (70.8) 6.7 % -32.00 [ -52.09, -11.91 ]
Jara-P?rez 2000 99 47.83 (31.44) 100 100 (27.09) 9.8 % -52.17 [ -60.33, -44.01 ]
Lacomme 1985 47 75.09 (78.07) 40 100 (68.77) 4.4 % -24.91 [ -55.77, 5.95 ]
RB10 1994 153 85.61 (90.91) 161 100 (106.06) 6.2 % -14.39 [ -36.21, 7.43 ]
RB21 1988 45 56.84 (63.16) 42 100 (52.63) 5.6 % -43.16 [ -67.53, -18.79 ]
RB22 1990 20 48.39 (16.13) 20 100 (22.58) 8.8 % -51.61 [ -63.77, -39.45 ]
Schaad 1986 45 96.98 (59.4) 49 100 (52.35) 6.0 % -3.02 [ -25.74, 19.70 ]
Schaad 2002 98 85.48 (58.06) 85 100 (65.72) 7.2 % -14.52 [ -32.61, 3.57 ]
Vautel 1993 32 60.97 (38.67) 32 100 (39.75) 6.9 % -39.03 [ -58.24, -19.82 ]
Zagar 1988 29 34.86 (23.85) 22 100 (59.63) 5.2 % -65.14 [ -91.53, -38.75 ]
Total (95% CI) 921 890 100.0 % -36.16 [ -44.51, -27.80 ]
Heterogeneity: Tau2 = 167.36; Chi2 = 43.08, df = 15 (P = 0.00015); I2 =65%
Test for overall effect: Z = 8.48 (P < 0.00001)
Test for subgroup differences: Not applicable
-100 -50 0 50 100
Favours immunostimulant Favours control
705Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
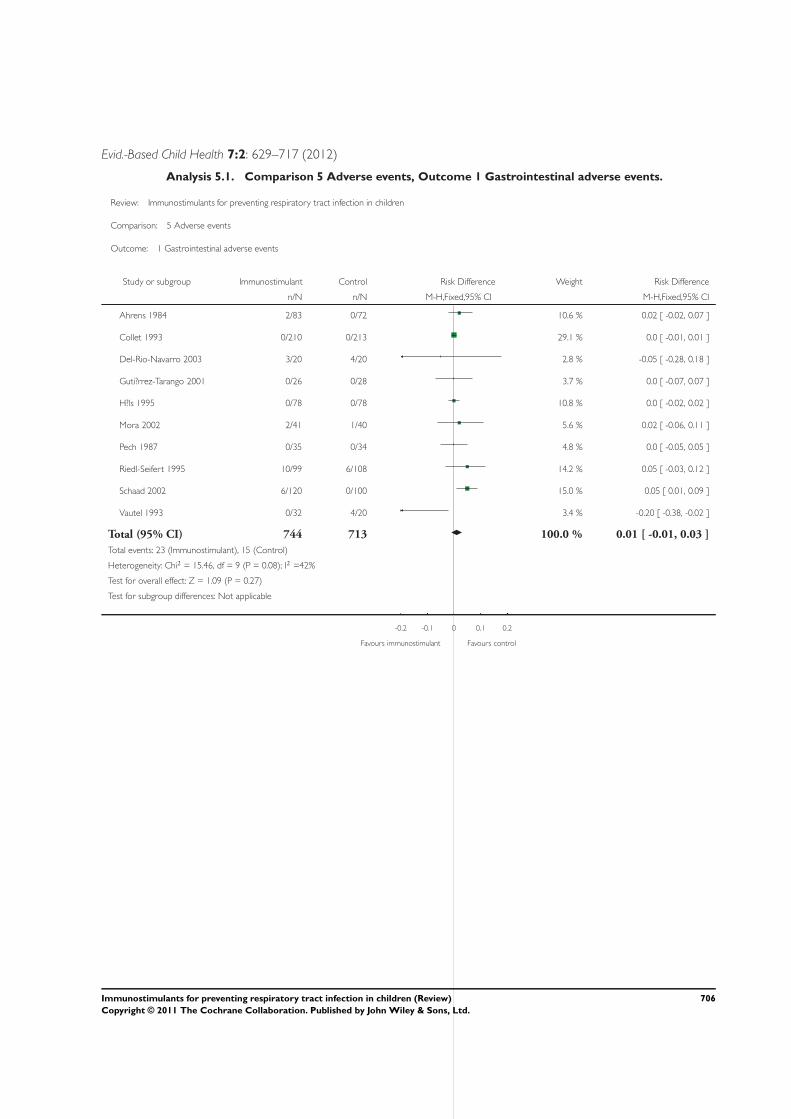
Evid.-Based Child Health 7:2: 629–717 (2012)
Analysis 5.1. Comparison 5 Adverse events, Outcome 1 Gastrointestinal adverse events.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 5 Adverse events
Outcome: 1 Gastrointestinal adverse events
Study or subgroup Immunostimulant Control Risk Difference Weight Risk Difference
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Ahrens 1984 2/83 0/72 10.6 % 0.02 [ -0.02, 0.07 ]
Collet 1993 0/210 0/213 29.1 % 0.0 [ -0.01, 0.01 ]
Del-Rio-Navarro 2003 3/20 4/20 2.8 % -0.05 [ -0.28, 0.18 ]
Guti?rrez-Tarango 2001 0/26 0/28 3.7 % 0.0 [ -0.07, 0.07 ]
H?ls 1995 0/78 0/78 10.8 % 0.0 [ -0.02, 0.02 ]
Mora 2002 2/41 1/40 5.6 % 0.02 [ -0.06, 0.11 ]
Pech 1987 0/35 0/34 4.8 % 0.0 [ -0.05, 0.05 ]
Riedl-Seifert 1995 10/99 6/108 14.2 % 0.05 [ -0.03, 0.12 ]
Schaad 2002 6/120 0/100 15.0 % 0.05 [ 0.01, 0.09 ]
Vautel 1993 0/32 4/20 3.4 % -0.20 [ -0.38, -0.02 ]
Total (95% CI) 744 713 100.0 % 0.01 [ -0.01, 0.03 ]
Total events: 23 (Immunostimulant), 15 (Control)
Heterogeneity: Chi2 = 15.46, df = 9 (P = 0.08); I2 =42%
Test for overall effect: Z = 1.09 (P = 0.27)
Test for subgroup differences: Not applicable
-0.2 -0.1 0 0.1 0.2
Favours immunostimulant Favours control
706Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
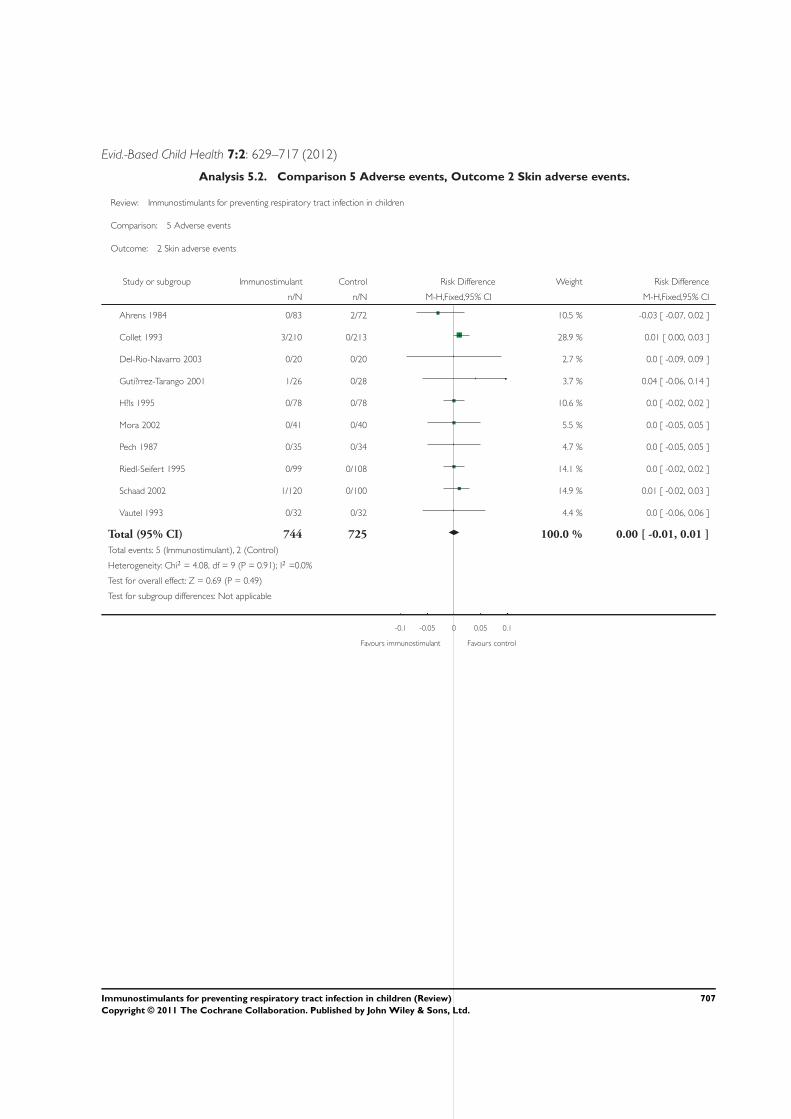
Evid.-Based Child Health 7:2: 629–717 (2012)
Analysis 5.2. Comparison 5 Adverse events, Outcome 2 Skin adverse events.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 5 Adverse events
Outcome: 2 Skin adverse events
Study or subgroup Immunostimulant Control Risk Difference Weight Risk Difference
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Ahrens 1984 0/83 2/72 10.5 % -0.03 [ -0.07, 0.02 ]
Collet 1993 3/210 0/213 28.9 % 0.01 [ 0.00, 0.03 ]
Del-Rio-Navarro 2003 0/20 0/20 2.7 % 0.0 [ -0.09, 0.09 ]
Guti?rrez-Tarango 2001 1/26 0/28 3.7 % 0.04 [ -0.06, 0.14 ]
H?ls 1995 0/78 0/78 10.6 % 0.0 [ -0.02, 0.02 ]
Mora 2002 0/41 0/40 5.5 % 0.0 [ -0.05, 0.05 ]
Pech 1987 0/35 0/34 4.7 % 0.0 [ -0.05, 0.05 ]
Riedl-Seifert 1995 0/99 0/108 14.1 % 0.0 [ -0.02, 0.02 ]
Schaad 2002 1/120 0/100 14.9 % 0.01 [ -0.02, 0.03 ]
Vautel 1993 0/32 0/32 4.4 % 0.0 [ -0.06, 0.06 ]
Total (95% CI) 744 725 100.0 % 0.00 [ -0.01, 0.01 ]
Total events: 5 (Immunostimulant), 2 (Control)
Heterogeneity: Chi2 = 4.08, df = 9 (P = 0.91); I2 =0.0%
Test for overall effect: Z = 0.69 (P = 0.49)
Test for subgroup differences: Not applicable
-0.1 -0.05 0 0.05 0.1
Favours immunostimulant Favours control
707Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
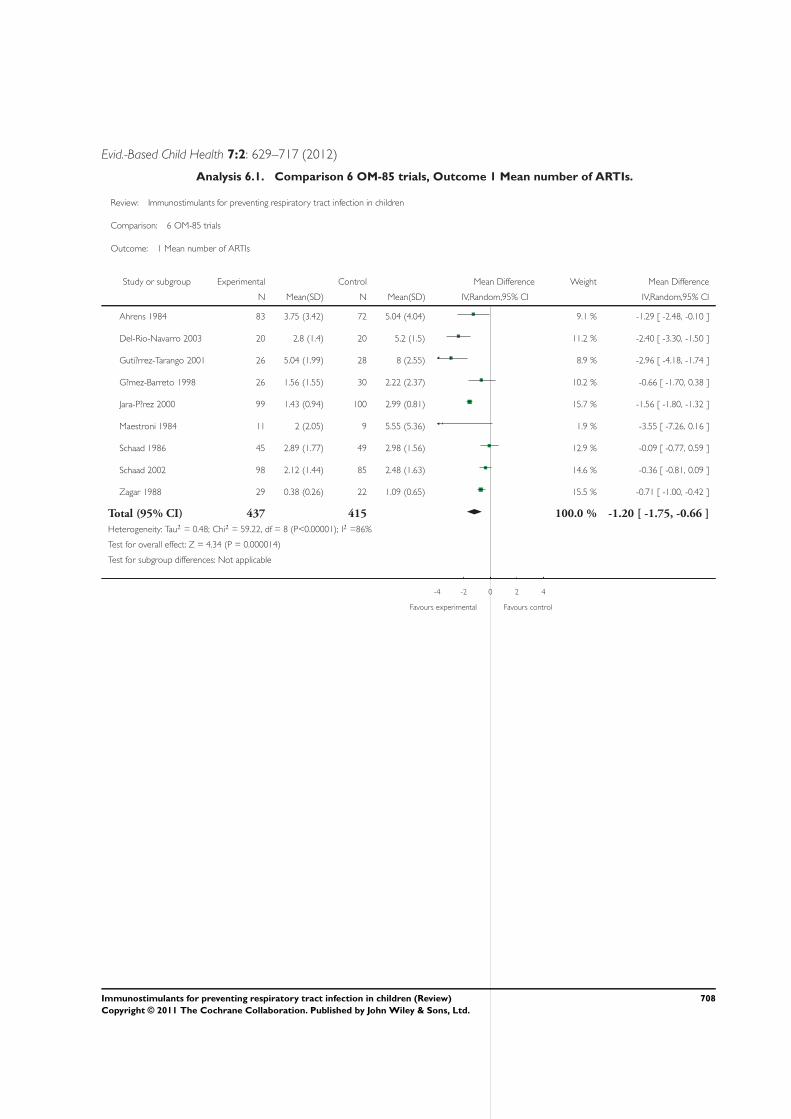
Evid.-Based Child Health 7:2: 629–717 (2012)
Analysis 6.1. Comparison 6 OM-85 trials, Outcome 1 Mean number of ARTIs.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 6 OM-85 trials
Outcome: 1 Mean number of ARTIs
Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Ahrens 1984 83 3.75 (3.42) 72 5.04 (4.04) 9.1 % -1.29 [ -2.48, -0.10 ]
Del-Rio-Navarro 2003 20 2.8 (1.4) 20 5.2 (1.5) 11.2 % -2.40 [ -3.30, -1.50 ]
Guti?rrez-Tarango 2001 26 5.04 (1.99) 28 8 (2.55) 8.9 % -2.96 [ -4.18, -1.74 ]
G?mez-Barreto 1998 26 1.56 (1.55) 30 2.22 (2.37) 10.2 % -0.66 [ -1.70, 0.38 ]
Jara-P?rez 2000 99 1.43 (0.94) 100 2.99 (0.81) 15.7 % -1.56 [ -1.80, -1.32 ]
Maestroni 1984 11 2 (2.05) 9 5.55 (5.36) 1.9 % -3.55 [ -7.26, 0.16 ]
Schaad 1986 45 2.89 (1.77) 49 2.98 (1.56) 12.9 % -0.09 [ -0.77, 0.59 ]
Schaad 2002 98 2.12 (1.44) 85 2.48 (1.63) 14.6 % -0.36 [ -0.81, 0.09 ]
Zagar 1988 29 0.38 (0.26) 22 1.09 (0.65) 15.5 % -0.71 [ -1.00, -0.42 ]
Total (95% CI) 437 415 100.0 % -1.20 [ -1.75, -0.66 ]
Heterogeneity: Tau2 = 0.48; Chi2 = 59.22, df = 8 (P<0.00001); I2 =86%
Test for overall effect: Z = 4.34 (P = 0.000014)
Test for subgroup differences: Not applicable
-4 -2 0 2 4
Favours experimental Favours control
708Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
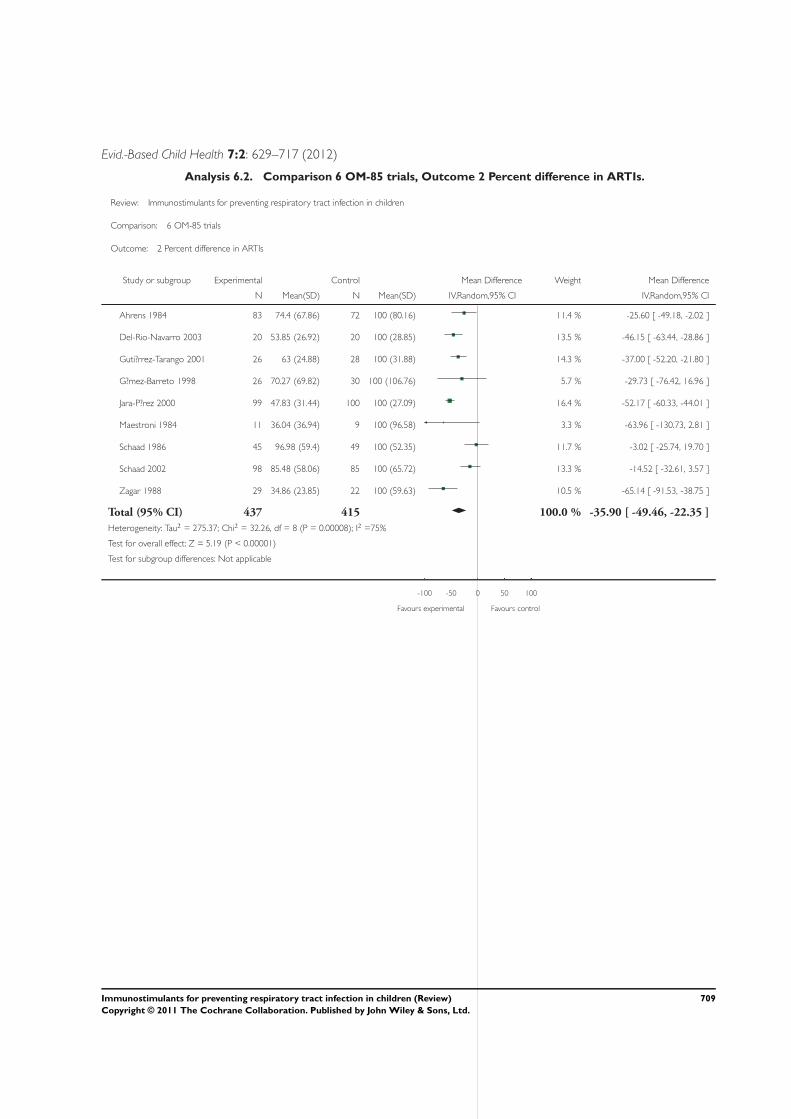
Evid.-Based Child Health 7:2: 629–717 (2012)
Analysis 6.2. Comparison 6 OM-85 trials, Outcome 2 Percent difference in ARTIs.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 6 OM-85 trials
Outcome: 2 Percent difference in ARTIs
Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Ahrens 1984 83 74.4 (67.86) 72 100 (80.16) 11.4 % -25.60 [ -49.18, -2.02 ]
Del-Rio-Navarro 2003 20 53.85 (26.92) 20 100 (28.85) 13.5 % -46.15 [ -63.44, -28.86 ]
Guti?rrez-Tarango 2001 26 63 (24.88) 28 100 (31.88) 14.3 % -37.00 [ -52.20, -21.80 ]
G?mez-Barreto 1998 26 70.27 (69.82) 30 100 (106.76) 5.7 % -29.73 [ -76.42, 16.96 ]
Jara-P?rez 2000 99 47.83 (31.44) 100 100 (27.09) 16.4 % -52.17 [ -60.33, -44.01 ]
Maestroni 1984 11 36.04 (36.94) 9 100 (96.58) 3.3 % -63.96 [ -130.73, 2.81 ]
Schaad 1986 45 96.98 (59.4) 49 100 (52.35) 11.7 % -3.02 [ -25.74, 19.70 ]
Schaad 2002 98 85.48 (58.06) 85 100 (65.72) 13.3 % -14.52 [ -32.61, 3.57 ]
Zagar 1988 29 34.86 (23.85) 22 100 (59.63) 10.5 % -65.14 [ -91.53, -38.75 ]
Total (95% CI) 437 415 100.0 % -35.90 [ -49.46, -22.35 ]
Heterogeneity: Tau2 = 275.37; Chi2 = 32.26, df = 8 (P = 0.00008); I2 =75%
Test for overall effect: Z = 5.19 (P < 0.00001)
Test for subgroup differences: Not applicable
-100 -50 0 50 100
Favours experimental Favours control
709Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
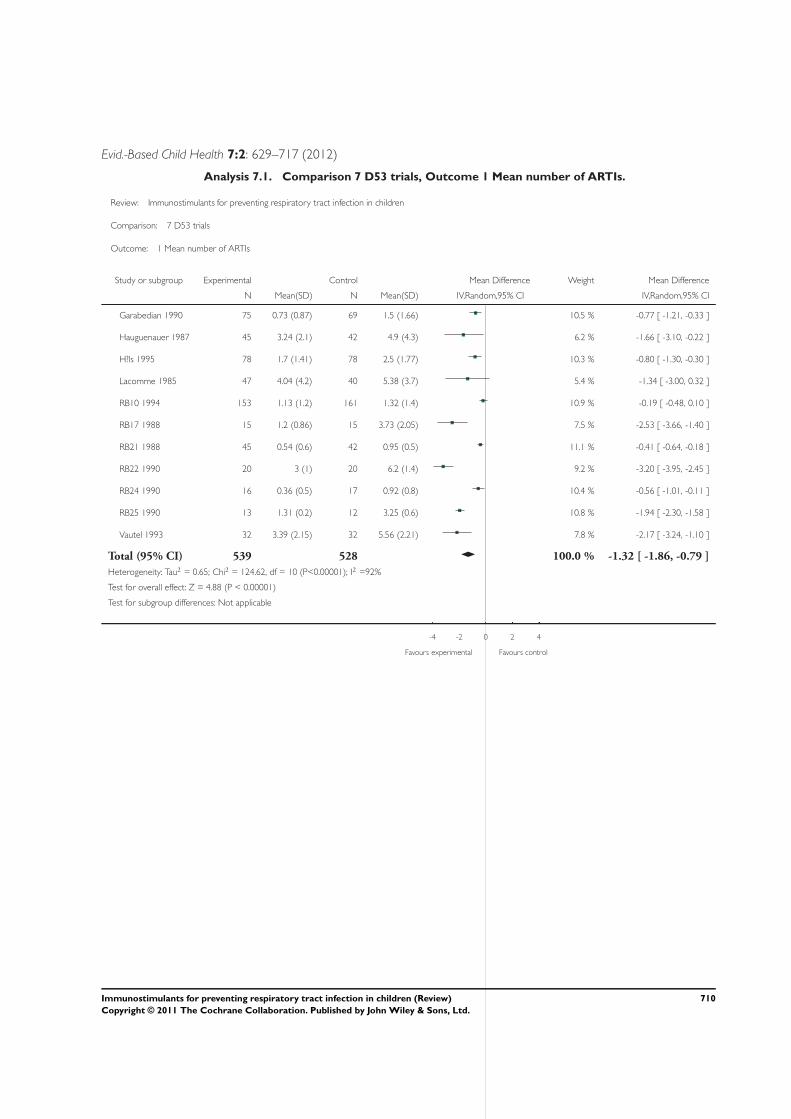
Evid.-Based Child Health 7:2: 629–717 (2012)
Analysis 7.1. Comparison 7 D53 trials, Outcome 1 Mean number of ARTIs.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 7 D53 trials
Outcome: 1 Mean number of ARTIs
Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Garabedian 1990 75 0.73 (0.87) 69 1.5 (1.66) 10.5 % -0.77 [ -1.21, -0.33 ]
Hauguenauer 1987 45 3.24 (2.1) 42 4.9 (4.3) 6.2 % -1.66 [ -3.10, -0.22 ]
H?ls 1995 78 1.7 (1.41) 78 2.5 (1.77) 10.3 % -0.80 [ -1.30, -0.30 ]
Lacomme 1985 47 4.04 (4.2) 40 5.38 (3.7) 5.4 % -1.34 [ -3.00, 0.32 ]
RB10 1994 153 1.13 (1.2) 161 1.32 (1.4) 10.9 % -0.19 [ -0.48, 0.10 ]
RB17 1988 15 1.2 (0.86) 15 3.73 (2.05) 7.5 % -2.53 [ -3.66, -1.40 ]
RB21 1988 45 0.54 (0.6) 42 0.95 (0.5) 11.1 % -0.41 [ -0.64, -0.18 ]
RB22 1990 20 3 (1) 20 6.2 (1.4) 9.2 % -3.20 [ -3.95, -2.45 ]
RB24 1990 16 0.36 (0.5) 17 0.92 (0.8) 10.4 % -0.56 [ -1.01, -0.11 ]
RB25 1990 13 1.31 (0.2) 12 3.25 (0.6) 10.8 % -1.94 [ -2.30, -1.58 ]
Vautel 1993 32 3.39 (2.15) 32 5.56 (2.21) 7.8 % -2.17 [ -3.24, -1.10 ]
Total (95% CI) 539 528 100.0 % -1.32 [ -1.86, -0.79 ]
Heterogeneity: Tau2 = 0.65; Chi2 = 124.62, df = 10 (P<0.00001); I2 =92%
Test for overall effect: Z = 4.88 (P < 0.00001)
Test for subgroup differences: Not applicable
-4 -2 0 2 4
Favours experimental Favours control
710Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
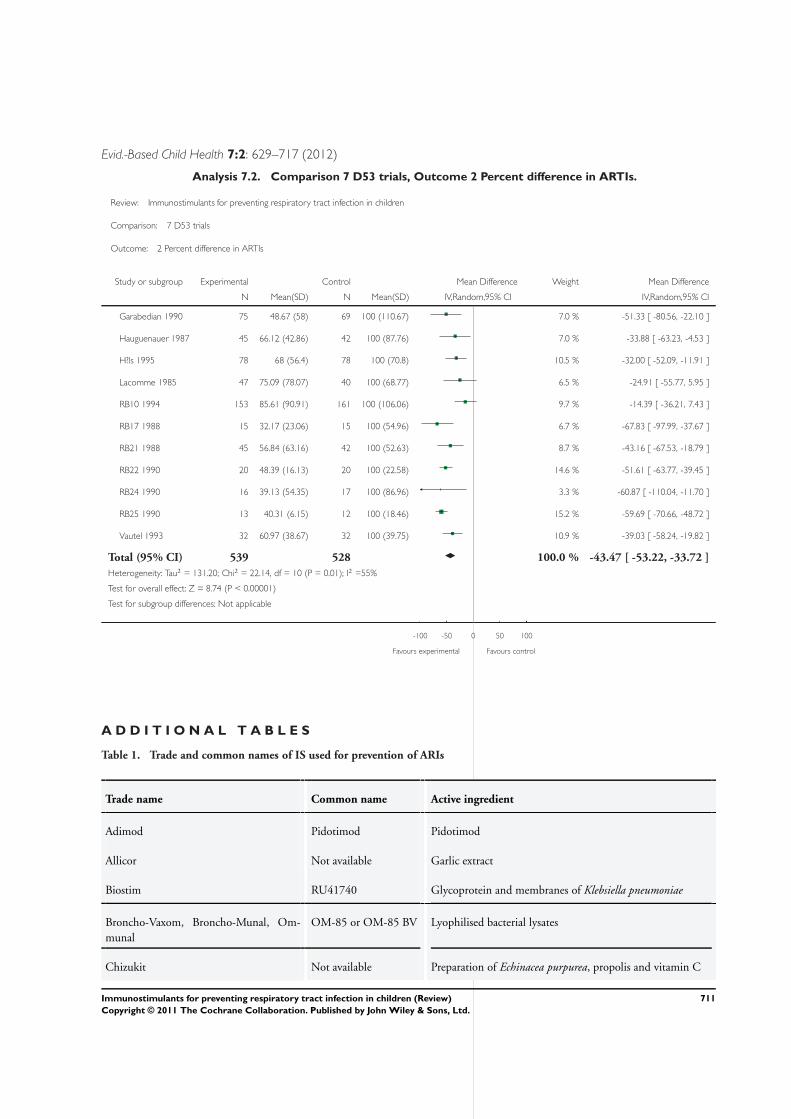
Evid.-Based Child Health 7:2: 629–717 (2012)
Analysis 7.2. Comparison 7 D53 trials, Outcome 2 Percent difference in ARTIs.
Review: Immunostimulants for preventing respiratory tract infection in children
Comparison: 7 D53 trials
Outcome: 2 Percent difference in ARTIs
Study or subgroup Experimental Control Mean Difference Weight Mean Difference
N Mean(SD) N Mean(SD) IV,Random,95% CI IV,Random,95% CI
Garabedian 1990 75 48.67 (58) 69 100 (110.67) 7.0 % -51.33 [ -80.56, -22.10 ]
Hauguenauer 1987 45 66.12 (42.86) 42 100 (87.76) 7.0 % -33.88 [ -63.23, -4.53 ]
H?ls 1995 78 68 (56.4) 78 100 (70.8) 10.5 % -32.00 [ -52.09, -11.91 ]
Lacomme 1985 47 75.09 (78.07) 40 100 (68.77) 6.5 % -24.91 [ -55.77, 5.95 ]
RB10 1994 153 85.61 (90.91) 161 100 (106.06) 9.7 % -14.39 [ -36.21, 7.43 ]
RB17 1988 15 32.17 (23.06) 15 100 (54.96) 6.7 % -67.83 [ -97.99, -37.67 ]
RB21 1988 45 56.84 (63.16) 42 100 (52.63) 8.7 % -43.16 [ -67.53, -18.79 ]
RB22 1990 20 48.39 (16.13) 20 100 (22.58) 14.6 % -51.61 [ -63.77, -39.45 ]
RB24 1990 16 39.13 (54.35) 17 100 (86.96) 3.3 % -60.87 [ -110.04, -11.70 ]
RB25 1990 13 40.31 (6.15) 12 100 (18.46) 15.2 % -59.69 [ -70.66, -48.72 ]
Vautel 1993 32 60.97 (38.67) 32 100 (39.75) 10.9 % -39.03 [ -58.24, -19.82 ]
Total (95% CI) 539 528 100.0 % -43.47 [ -53.22, -33.72 ]
Heterogeneity: Tau2 = 131.20; Chi2 = 22.14, df = 10 (P = 0.01); I2 =55%
Test for overall effect: Z = 8.74 (P < 0.00001)
Test for subgroup differences: Not applicable
-100 -50 0 50 100
Favours experimental Favours control
A D D I T I O N A L T A B L E S
Table 1. Trade and common names of IS used for prevention of ARIs
Trade name Common name Active ingredient
Adimod Pidotimod Pidotimod
Allicor Not available Garlic extract
Biostim RU41740 Glycoprotein and membranes of Klebsiella pneumoniae
Broncho-Vaxom, Broncho-Munal, Om-munal
OM-85 or OM-85 BV Lyophilised bacterial lysates
Chizukit Not available Preparation of Echinacea purpurea, propolis and vitamin C
711Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Evid.-Based Child Health 7:2: 629–717 (2012)
Table 1. Trade and common names of IS used for prevention of ARIs (Continued)
Decaris Levamisole Levamisole
Echinacea Echinacea purpurea Extract of Echinacea purpurea
Immunoferon, Inmunol AM3 Glycophosphopeptical
IRS 19 Not available Bacterial lysates
Ismigen Not available Bacterial lysates
Lantigen B Not available Bacterial antigens
Leucotrofina, Leucogen Thymomodulin Thymus extract
Luivac LW50020 Bacterial antigens
Munostin Not available Bacterial corpses and lysates
Not available SL04 Bacterial extracts
Paspat Not available Autolysate mixture of bacterial antigens for parenteral appli-cation
Prasosine Isoprinosine Isoprinosine
Pulmotabs Not available Bacterial lysates
Pulmonarom Not available Bacterial lysates
Reaferon Not available Analogue of human interferon 2 obtained by genetic engi-neering
Respivax Not available Bacterial lysates
Ribovac, Ribomunyl, Immucithal D53 Proteoglycans of K. pneumoniae plus bacterial ribosomes
TFX Thymus extract Thymus extract
Umckaloabo Pelargonium sidoides Alcohol extract from the roots of Pelargonium sidoides
712Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Evid.-Based Child Health 7:2: 629–717 (2012)
Table 2. Description of the studies
Immunos-
timulant
n n analysis
data
Duration <
6 months
Duration 6
months
Duration >
6 months
Quality A Quality B Quality C Quality D
D53 18 11 7 11 - - 18 - -
IRS19 1 0 - 1 - - - 1 -
Lantigen B 2 0 - 2 - - 2 - -
LW50020 2 0 2 - - - 2 - -
OM-85BV
12 9 - 10 2 4 8 - -
RU41740 5 5 - 3 2 - 5 - -
Total bac-terial
40 25 9 27 4 4 35 1 -
Herbal(echi-nacea/garlic)
4 1 2 1 1 2 2 - -
Isoprino-sine
1 1 - 1 - - 1 - -
Lev-amisole
4 3 2 2 - - 4 - -
Pidotimod 6 2 6 - - - 6 - -
Total syn-thetic
11 6 8 3 - - 11 - -
Thymicextract
5 3 4 - 1 - 5 - -
Syntheticinterferon
1 0 1 - - - 1 - -
Grand to-tal
61 35 24 31 6 6 53 2 -
713Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
A P P E N D I C E S
Appendix 1. Previous searches
We searched the Cochrane Central Register of Controlled Trials (CENTRAL) (The Cochrane Library Issue 4, 2005); MEDLINE(January 1966 to January 2006); EMBASE (January 1990 to January 2006); PASCAL (up to January 2006); SciSearch (up to January2006); and IPA (up to January 2006) for reports of trials.Trials were identified using the Cochrane methodology searches phase 1 and phase 2 (Dickersin 1994). The following search strategywas combined with the highly sensitive search strategy used in MEDLINE and CENTRAL and adapted for EMBASE, PASCAL,SciSearch and IPA.MEDLINE (Ovid)
1 exp Respiratory Tract Infections/2 (respiratory tract infection$ or respiratory infection$)3 or/1-24 exp Adjuvants, Immunologic/5 (immunostimulants$ or immunomodulator$)6 Immunobalt7 (LW50020 or Luivac or Paspat)8 Munostin9 (OM-85 BV or Broncho-Vaxom)10 Pulmonar-OM11 D5312 Ribomunyl13 Ribovac14 Immucytal15 exp Lipopolysaccharides/16 lipopolysaccharid$17 (RU 41740 or Biostim)18 exp Thymus Extracts/19 calf thymus extract$20 (thymic extract$ or thymomodulin)21 exp Pelargonium/22 (Pelargonium sidoides or Umckaloabo)23 AM324 Inmunoferon25 glycophosphopeptical26 or/4-2527 3 and 26Identified articles were used as references for a Science Citation Index search. Bibliographies of all included trials as well as those ofrelevant reviews were searched to identify additional studies. Finally, a letter was sent to all first authors, as well as pharmaceuticalcompanies that manufacture immunostimulant drugs, requesting data and references for any relevant published and unpublished trials.There were no language restrictions. We also searched for studies in the trial registration web site: metaRegister of Controlled Trials(http://www.controlled-trials.com/mrct/).
714Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
Appendix 2. Embase search strategy
Embase.com (Elsevier)
(Search strategy used for January 2010 to March 2011 update)#29. #25 AND #28 400 3 Mar 2011#28. #26 OR #27 841,770 3 Mar 2011#27. random*:ab,ti OR placebo*:ab,ti OR factorial*:ab,ti OR crossover*:ab,ti OR ’cross over’:ab,ti OR ’cross-over’:ab,ti OR volunteer*:ab,ti OR assign*:ab,ti OR allocat*:ab,ti OR ((singl* OR doubl*) NEAR/1 blind*):ab,ti AND [embase]/lim 802,449 3 Mar 2011#26. ’randomized controlled trial’/exp OR ’single blind procedure’/exp OR ’double blind procedure’/exp OR ’crossover procedure’/expAND [embase]/lim 237,948 3 Mar 2011#25. #3 AND #24 3,234 3 Mar 2011#24. #4 OR #5 OR #6 OR #7 OR #8 OR #9 OR #10 OR #11 OR #12 OR #13 OR #14 OR #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 OR #23 114,581 3 Mar 2011#23. ’immunostimulating agent’/de OR ’immunomodulating agent’/de AND [embase]/lim 11,919 3 Mar 2011#22. levamisole:ab,ti AND [embase]/lim 3,610 3 Mar 2011#21. pidotimod:ab,ti OR adimod:ab,ti AND [embase]/lim 68 3 Mar 2011#20. glycophosphopep:ab,ti AND [embase]/lim 3 Mar 2011#19. am3:ab,ti OR imunoferon:ab,ti OR immunoferon:ab,ti OR inmunoferon:ab,ti AND [embase]/lim 144 3 Mar 2011#18. pelargonium*:ab,ti OR umckaloabo:ab,ti AND [embase]/lim 249 3 Mar 2011#17. ’pelargonium sidoides extract’/de AND [embase]/lim 98 3 Mar 2011#16. ’thymus extract’:ab,ti OR ’thymus extracts’:ab,ti OR ’thymic extract’:ab,ti OR ’thymic extracts’:ab,ti OR thymomodulin*:ab,tiAND [embase]/lim 556 3 Mar 2011#15. ’thymus extract’/de AND [embase]/lim 514 3 Mar 2011#14. ru41740:ab,ti OR ’ru-41740’:ab,ti OR ’ru 41740’:ab,ti OR biostim:ab,ti AND [embase]/lim 122 3 Mar 2011#13. lipopolysaccharide*:ab,ti AND [embase]/lim 48,375 3 Mar 2011#12. ’lipopolysaccharide’/exp AND [embase]/lim 53,723 3 Mar 2011#11. ribomunyl:ab,ti OR ribovac:ab,ti OR immucytal:ab,ti AND [embase]/lim 68 3 Mar 2011#10. d53:ab,ti AND [embase]/lim 40 3 Mar 2011#9. ’pulmonar-om’:ab,ti OR ’pulmonar om’:ab,ti AND [embase]/lim 1 3 Mar 2011#8. bronchovaxom:ab,ti OR ’broncho-vaxom’:ab,ti OR ’broncho vaxom’:ab,ti AND [embase]/lim 113 3 Mar 2011#7. ’om 85 bv’:ab,ti OR om85bv:ab,ti OR ’om-85 bv’:ab,ti AND [embase]/lim 51 3 Mar 2011#6. immunobalt:ab,ti OR lw50020:ab,ti OR luivac:ab,ti OR paspat:ab,ti OR munostin:ab,ti AND [embase]/lim 18 3 Mar 2011#5. immunostimulant*:ab,ti OR immunomodul*:ab,ti OR immunoadjuvant*:ab,ti OR (immuno* NEAR/1 adjuvant*):ab,ti AND[embase]/lim 30,022 3 Mar 2011#4. ’immunological adjuvant’/exp AND [embase]/lim 11,700 3 Mar 2011#3. #1 OR #2 158,887 3 Mar 2011#2. (respiratory NEAR/5 infection*):ab,ti AND 30,608 3 Mar 2011[embase]/lim#1. ’respiratory tract infection’/exp AND 149,401 3 Mar 2011 [embase]/lim
Appendix 3. Search terms used for searching other databases
Our library assistant searched for clinical trials on children with the term ’respiratory’ in EMBASE, PASCAL, SciSearch and IPA from2005 to March 2010, for the following interventions:Immunostimulants OR immunomodulatorsBacterial lysates OR bacterial antigens OR bacterial extractsLW50020 OR Luivac OR PaspatOM-85 OR OM-85 BV OR Broncho-VaxomD53 OR Ribomunyl OR Ribovac OR ImmucytalRU 41740 OR BiostimAM3 OR Inmunoferon OR glycophosphopepticalPidotimod
715Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Evid.-Based Child Health 7:2: 629–717 (2012)
LevamisoleEchinacea
W H A T ’ S N E W
Last assessed as up-to-date: 3 March 2011.
Date Event Description
4 March 2011 New search has been performed Searches conducted. We included three new trials (Mora 2007; Mora 2010a;Wahl 2008) and the mean and standard deviation on the number of acute respira-tory tract infections in Schaad 2002. We excluded six new trials (Grimfeld 2004;Heinz 2010; Mora 2010b; Razi 2010; Riedl-Seifert 1993; Steinsbekk 2005). Weincluded sub-analyses on the efficacy of D53 and OM-85. The conclusions re-main unchanged
H I S T O R Y
Protocol first published: Issue 4, 2004
Review first published: Issue 4, 2006
Date Event Description
21 April 2008 Amended Converted to new review format.
24 January 2006 New search has been performed Searches conducted.
C O N T R I B U T I O N S O F A U T H O R S
Dr Blanca Estela Del-Rio-Navarro (BN) searched for papers, extracted the relevant data, analyzed data and co-wrote the review.
Dr Juan JL Sienra-Monge (JSM) searched for papers, extracted the relevant data and co-wrote the review.
Dr Francisco Espinosa-Rosales (FER) searched for papers, analyzed data and co-wrote the review.
Vicki Flenady (VF) co-wrote and made corrections to the review.
716Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Evid.-Based Child Health 7:2: 629–717 (2012)
D E C L A R A T I O N S O F I N T E R E S T
Dr Arturo Berber was the medical manager for OM-85 BV (Broncho-Vaxom) in Mexico for BASF Pharma Mexico (Química Knollde México) from 1995 to 2001. He was also the contact author of the initial protocol until he graciously stepped down because of apotential conflict of interest.
Dr Blanca Del Rio-Navarro and Dr Sienra-Monge were involved in the following IS trial: Del-Rio-Navarro BE, Luis Sienra-Monge JJ,Berber A, Torres-Alcantara S, Avila-Castanon L, Gomez-Barreto D. Use of OM-85 BV in children suffering from recurrent respiratorytract infections and subnormal IgG subclass levels. Allergologia et Immunopathologia (Madrid) 2003 Jan-Feb;31(1):7-13.
Dr Blanca Del Rio-Navarro was involved in the following IS trials: Field J, Gomez-Barreto D, Del-Rio-Navarro BE, Berber A. Useof OM-85 BV in primary prevention of acute respiratory tract infections in children in orphanages Current Therapeutics Research,Clinical and Experimental 1998 59:6 (407-18); Berber AC, Del-Rio-Navarro BE. Use of Broncho-Vaxom in private practice: phase IVtrial in 587 children. Clinical Therapeutics 1996 Nov-Dec;18(6):1068-79.
S O U R C E S O F S U P P O R T
Internal sources
• Allergy and Clinical Immunolgy Service, Children Hospital of Mexico Federico Gomez, Mexico.The review was supported by the local institution
External sources
• No sources of support supplied
I N D E X T E R M S
Medical Subject Headings (MeSH)
Adjuvants, Immunologic [∗therapeutic use]; Adolescent; Randomized Controlled Trials as Topic; Respiratory Tract Infections[∗prevention & control]
MeSH check words
Child; Humans
717Immunostimulants for preventing respiratory tract infection in children (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.





























