Embed Size (px)
Citation preview
Physical training for interstitial lung disease (Review)
Holland AE, Hill C
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2010, Issue 3
http://www.thecochranelibrary.com
Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Figure 3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Figure 4. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Figure 5. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Figure 6. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
Figure 7. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
Figure 8. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Figure 9. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14
Figure 10. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Figure 11. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
16DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
17AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
17ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
17REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
19CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
25DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
26WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
26HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
27CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
27DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
27SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
28DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . . . . . . . . . . . .
28INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iPhysical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
[Intervention Review]
Physical training for interstitial lung disease
Anne E Holland1, Catherine Hill2
1Physiotherapy, Alfred Health / La Trobe University, Melbourne, Australia. 2Physiotherapy, Austin Hospital, Heidelberg, Australia
Contact address: Anne E Holland, Physiotherapy, Alfred Health / La Trobe University, Commercial Road, Melbourne, 3004, Australia.
[email protected]. [email protected].
Editorial group: Cochrane Airways Group.
Publication status and date: New search for studies and content updated (no change to conclusions), published in Issue 3, 2010.
Review content assessed as up-to-date: 1 February 2010.
Citation: Holland AE, Hill C. Physical training for interstitial lung disease. Cochrane Database of Systematic Reviews 2008, Issue 4.
Art. No.: CD006322. DOI: 10.1002/14651858.CD006322.pub2.
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Interstitial lung disease (ILD) is characterised by reduced functional capacity, dyspnoea and exercise-induced hypoxia. Physical training
is beneficial for people with other chronic lung conditions, however its effects in ILD have not been well characterised.
Objectives
To assess the effects of physical training on exercise capacity, symptoms, quality of life and survival compared to no physical training
in people with ILD.
Search methods
We searched the Cochrane Central Register of Controlled Trials (The Cochrane Library 2009, Issue 4), MEDLINE, EMBASE,
CINAHL and the Physiotherapy Evidence Database (PEDro) (all searched from inception to December 2009). The reference lists of
relevant studies were hand-searched for qualifying studies.
Selection criteria
Randomised or quasi-randomised controlled trials in which physical training was compared to no physical training or to other therapy
in people with ILD of any aetiology were included.
Data collection and analysis
Two review authors independently selected trials for inclusion, extracted data and assessed risk of bias. Authors were contacted to
obtain missing data and information regarding adverse effects. A priori subgroup analyses were specified for participants with idiopathic
pulmonary fibrosis (IPF), severe lung disease and training modality.
Main results
Five studies were included, three of which were published as abstracts. Two studies were included in the meta-analysis (43 participants
who undertook physical training and 42 control participants). One study used a blinded assessor and intention-to-treat analysis. No
adverse effects of physical training were reported. Physical training improved the 6-minute walk distance with weighted mean difference
(WMD) 38.61 metres (95% confidence interval 15.37 to 61.85 metres). Improvement in 6-minute walk distance was also seen in
the subgroup of participants with IPF (WMD 26.55 metres, 2.81 to 50.30 metres). No effect of physical training on VO2peak was
evident. There was a reduction in dyspnoea (standardised mean difference (SMD) -0.47, 95% CI: -0.91 to -0.04) however this did not
reach significance in the IPF subgroup (SMD -0.43, 95% CI: -0.94 to 0.08). Quality of life improved following physical training in all
1Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

participants (SMD 0.58, 95% CI: 0.15 to 1.02) and in IPF (SMD 0.57, 95% CI: 0.06 to 1.09). Only one study reported longer-term
outcomes, with no significant effects of physical training on clinical variables or survival at six months. Insufficient data were available
to examine the impact of disease severity or training modality.
Authors’ conclusions
Physical training is safe for people with ILD. Improvements in functional exercise capacity, dyspnoea and quality of life are seen
immediately following training, with benefits also evident in IPF. There is little evidence regarding longer-term effects of physical
training.
P L A I N L A N G U A G E S U M M A R Y
Physical training for interstitial lung disease (ILD)
People with ILD often have reduced exercise capacity and shortness of breath during exercise. Physical training can improve well being
in people with other chronic lung diseases, but little is known regarding physical training in ILD. We conducted a review to establish
whether physical training is safe for people with ILD, and to examine the effects of physical training on exercise capacity, shortness
of breath and quality of life. We also looked at whether people with idiopathic pulmonary fibrosis, a type of ILD which can progress
rapidly, could benefit from physical training. Five studies were included, however only two studies contained sufficient information
for the analysis (43 participants receiving physical exercise and 42 participants not). There were no reports of unwelcome effects of
physical training. Immediately following training, participants could walk further than those who had not undertaken the training
(on average 39 metres further in six minutes), reported less shortness of breath and improved quality of life. People with idiopathic
pulmonary fibrosis also experienced improvements following physical training although these tended to be smaller. There was not
enough information to establish whether there were any ongoing effects once the training had stopped. Bigger studies are required to
determine which method of physical training is most beneficial and whether the severity of ILD influences the benefits of physical
training.
B A C K G R O U N D
Interstitial lung disease (ILD) is a highly disabling group of con-
ditions including idiopathic pulmonary fibrosis (IPF), acute and
chronic interstitial pneumonias, connective tissue diseases and sar-
coidosis. People with ILD frequently experience breathlessness on
exertion which limits their ability to undertake daily activities. Pa-
tients report low levels of physical functioning and vitality, and
high levels of dyspnoea and fatigue. Those with the greatest exer-
cise limitation have the worst quality of life (Chang 1999). Avail-
able treatments for ILD have proved largely ineffective, offering
no improvement in survival and demonstrating only limited im-
pact on quality of life.
The mechanisms of reduced exercise capacity in ILD are multi-
factorial. Impaired gas exchange occurs as a result of destruction
of the pulmonary capillary bed, resulting in ventilation-perfusion
mismatch and oxygen diffusion limitation (Agusti 1991). Circu-
latory limitation results from pulmonary capillary destruction and
pulmonary vasoconstriction, leading to pulmonary hypertension
and cardiac dysfunction in some patients (Hansen 1996). Ven-
tilatory limitation to exercise may also occur, although it is not
thought to be a major contributor in most patients (Harris-Eze
1996). Peripheral muscle dysfunction may also play a significant
role in limiting exercise capacity (Markovitz 1998), as a result of
physical deconditioning. Patients who experience dyspnoea and
fatigue with functional activity commonly reduce their activity
levels, leading to a vicious cycle of worsening exercise capacity
and increasing symptoms. In addition, treatments for ILD such as
corticosteroids and immunosuppressive therapy may lead to drug-
induced myopathy.
Physical training, involving regular participation in an exercise
programme, improves exercise performance and reduces symp-
toms in people with other chronic lung diseases such as chronic
obstructive pulmonary disease and bronchiectasis (Nici 2006). A
number of authors have postulated that there may be similar effects
of physical training in ILD. Markovitz 1998 advocates the use of
physical training in ILD to restore muscle strength and endurance,
maximise functional level and improve quality of life. Miki 2003
found that PaO2-slope, a marker of exercise-induced hypoxaemia
obtained from cardiopulmonary exercise testing, was significantly
2Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

related to both exercise capacity and survival in IPF. They postu-
lated that this factor was amenable to improvement with physical
training. Recently published guidelines for Pulmonary Rehabili-
tation, an intervention which includes physical training, have ad-
vocated its use in ’all patients in whom respiratory symptoms are
associated with diminished functional capacity or reduced health-
related quality of life’ (Nici 2006). The safety and efficacy of this
approach in ILD is unclear. The greater prevalence of exercise-
induced hypoxia, pulmonary hypertension and arrhythmia in this
patient population compared to other chronic lung diseases raises
the possibility that response to physical training may also differ
(ATS/ERS 2000).To date there has not been a systematic review
of the literature in this area.
This review was conducted to summarize the results of literature
evaluating the safety and efficacy of physical training in adult pa-
tients with ILD, and to determine the effects of physical training
on exercise capacity, symptoms, quality of life and survival in this
patient group.
O B J E C T I V E S
(1) To determine whether physical training in patients with ILD
has beneficial effects on exercise capacity, symptoms, quality of
life and survival compared to no physical training in patients with
ILD and (2) to assess the safety of physical training in patients
with ILD.
M E T H O D S
Criteria for considering studies for this review
Types of studies
Only randomised or quasi -randomised controlled trials in which
a prescribed regimen of physical training was compared to no
physical training or to other therapy in patients with ILD were
considered for this review. Single blind and open studies were
considered for inclusion.
Types of participants
People with ILD of any aetiology, diagnosed according to the
investigators’ definition, were included. There were no exclusions
on the basis of age, gender or physiologic status.
Types of interventions
We considered any type of prescribed physical training, either
supervised or unsupervised. We recorded, wherever possible, the
precise nature of the training (intensity, frequency, duration and
whether supplemental oxygen was applied). Trials where physical
training was combined with another intervention (e.g. education
or pharmacological therapy) were eligible for inclusion.
Comparisons to be examined were:
1. Physical training versus no physical training
2. Physical training versus another intervention
3. Physical training combined with another intervention versus
no physical training
Types of outcome measures
Primary outcomes
Functional or maximal exercise capacity, measured during either
formal exercise tests (maximal oxygen uptake (VO2 max), peak
oxygen uptake (VO2 peak), maximal ventilation (Ve max), heart
rate ) or field exercise tests (increase in distance walked).
Secondary outcomes
1. Dyspnoea: all measures of dyspnoea used were considered
2. Quality of life: Quality of life as measured by generic or disease-
specific quality of life instruments. All quality of life instruments
used were considered.
3. Adverse effects: adverse cardiovascular events during training
were recorded, as well as fractures, skeletal muscle injuries and
death.
4. Survival
Search methods for identification of studies
Electronic searches
We searched the Cochrane Central Register of Controlled Trials
(CENTRAL), MEDLINE, EMBASE, CINAHL and the Physio-
therapy Evidence Database (PEDro). All databases were searched
from the period of their inception to December 2009. No lan-
guage restriction was used.
The full database search strategies are listed in the appendices
(Appendix 1, Appendix 2, Appendix 3, Appendix 4 and Appendix
5).
3Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Searching other resources
The reference lists of relevant studies and any related review pa-
pers were hand-searched for qualifying studies. We also contacted
authors of randomised controlled trials for information on other
published and unpublished studies.
Data collection and analysis
Selection of studies
Two authors (AH and CH) independently coded studies identified
in the literature searches for relevance by examining titles, abstract
and keywords fields as follows:
1. INCLUDE: Study categorically meets all review criteria;
2. UNCLEAR: Study appears to meet some review criteria but
insufficient information available to categorically determine rele-
vance;
3. EXCLUDE: Study does not categorically meet all review criteria
Two authors (AH and CH) used a full text copy of studies in
categories 1 and 2 to decide on study inclusion. Disagreements
were resolved by consensus. A full record of decisions was kept
and simple agreement and kappa statistics calculated.
Data extraction and management
Data were extracted independently by two authors using a pre-
pared checklist before being entered into Review Manager by the
primary reviewer (AH), with random checks on accuracy. Dis-
agreements were resolved by consensus. Data included characteris-
tics of included studies (methods, participants, interventions, out-
comes) and results of the included studies. Authors of included
studies were asked to verify the data extracted for their study and
to provide details of missing data where applicable.
Assessment of risk of bias in included studies
Two authors assessed the internal validity of included studies using
a component approach (including sequence generation for ran-
domisation, allocation concealment, blinding of participants and
assessors, loss to follow-up, completeness of outcome assessment
and other possible bias prevention). Disagreements were resolved
by consensus. We wrote to study authors to seek clarification where
we had inadequate information to judge the risk of bias.
Measures of treatment effect
For continuous variables, we recorded either the mean change
from baseline or the mean post-intervention values and standard
deviation (SD) for each group. The mean difference (MD) for
outcomes measured with the same metrics or standardised mean
difference (SMD) for outcomes measured with different metrics
with 95% confidence intervals (95% CI) were calculated using
RevMan 5.0. For binary outcome measures, we recorded the num-
ber of participants with each outcome event, by allocated treated
group, to allow an intention-to-treat analysis. The odds ratio (OR)
with 95%CIs were calculated for each study.
Assessment of heterogeneity
Subgroup analyses were conducted to explore possible sources of
heterogeneity. Three subgroup analyses were specified a priori:
1. Type of interstitial lung disease - idiopathic pulmonary fibrosis
(IPF) vs other: due to the progressive nature of IPF, physical train-
ing may be less effective in this form of ILD
2. Severity of lung disease: patients with more advanced disease
may be less able to participate in physical training. Participants
were considered to have severe disease if diffusing capacity for car-
bon monoxide (TLCO) was less than 45% predicted. In addi-
tion, participants who desaturated during exercise testing (SpO2
less than or equal to 88%) were compared to those who do not
desaturate.
3. Type of exercise: aerobic exercise training programs may be more
effective in improving symptoms and functional exercise tolerance
than resistance training programs
Data synthesis
We performed a pooled quantitative analysis where trials were
clinically homogeneous. A fixed or random effects model was used
depending on assessment of heterogeneity.
Sensitivity analysis
The small number of studies precluded sensitivity analyses and the
creation of funnel plots to test for publication bias. If in future
updates there are more studies included, sensitivity analysis will
be performed to analyse the effects of allocation concealment and
use of intention to treat analysis on results.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
Results of the search
There were 4783 studies identified from the initial search of the
databases. From this list, 15 full text articles were retrieved for
4Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

closer inspection. No additional studies were identified follow-
ing hand searching of reference lists or contacting study authors.
Of the 15 full text articles, agreement between the authors was
achieved on 13 articles (87%) with kappa=0.74, indicating sub-
stantial agreement. Disagreement was resolved by consensus. Five
articles were deemed to meet the inclusion criteria for this review.
Common reasons for exclusion were that studies were not ran-
domised controlled trials (n=3), studies included subjects without
lung disease (n=3), studies included mixed disease groups (n=3) or
studies did not include physical training (n=1). Full details of ex-
cluded studies can be found in Characteristics of excluded studies.
An update search conducted in December 2009 did not identify
any relevant studies for inclusion in the review.
Included studies
Five studies met the inclusion criteria for this review and all were
parallel randomised controlled trials. Full details can be found
in the ’Characteristics of Included Studies’ table. Three studies
had been published in abstract form only (Baradzina 2005; Mejia
2000; Wewel 2005). Sample sizes ranged from 22 to 99 partic-
ipants. All studies compared physical training to a no physical
training or sham training control group (Data and analyses: Com-
parison 1). Four studies examined exercise training programs con-
ducted in the outpatient setting (Baradzina 2005; Holland 2008;
Mejia 2000; Nishiyama 2008) whilst one study evaluated a home-
based exercise training program (Wewel 2005). The length of the
training programs varied from 5-12 weeks for outpatient training
and six months for home-based training.
Most studies included participants with a variety of ILDs (Holland
2008; Mejia 2000; Wewel 2005), one of which was stratified for
IPF (Holland 2008). One study included only participants with
sarcoidosis (Baradzina 2005) whilst another only included those
with IPF (Nishiyama 2008). All participants were adults with a
mean age of 52 to 70 years, with the exception of the study that
included only participants with sarcoidosis where the mean age
was 36 years (Baradzina 2005). Three studies examined the effects
of aerobic training (Baradzina 2005; Mejia 2000; Wewel 2005)
whilst the remaining studies used a combination of aerobic and
resistance training (Holland 2008; Nishiyama 2008). No study
evaluated resistance training alone and therefore no subgroup anal-
yses for type of exercise were possible. Participants in two stud-
ies underwent additional interventions that were not offered to
the control group; these included educational lectures (Baradzina
2005; Nishiyama 2008), nutritional advice, stress management
and physiotherapy (Baradzina 2005).
All studies used a measure of functional exercise tolerance, most
commonly the 6-minute walk test (Holland 2008; Nishiyama
2008; Wewel 2005). Two studies also performed a cardiopul-
monary exercise test (Holland 2008; Wewel 2005). Quality of life
was assessed in all five studies, using either the Chronic Respiratory
Disease questionnaire (Holland 2008; Mejia 2000), the St George’s
Respiratory questionnaire (Nishiyama 2008; Wewel 2005) or the
WHO questionnaire (Baradzina 2005). Dyspnoea was assessed in
three studies using the modified Medical Research Council Scale
(Holland 2008), the Baseline Dyspnoea Index (Nishiyama 2008)
and an unspecified measure (Wewel 2005).
Risk of bias in included studies
An overview of the risk of bias for domains listed below is provided
in Figure 1.
5Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
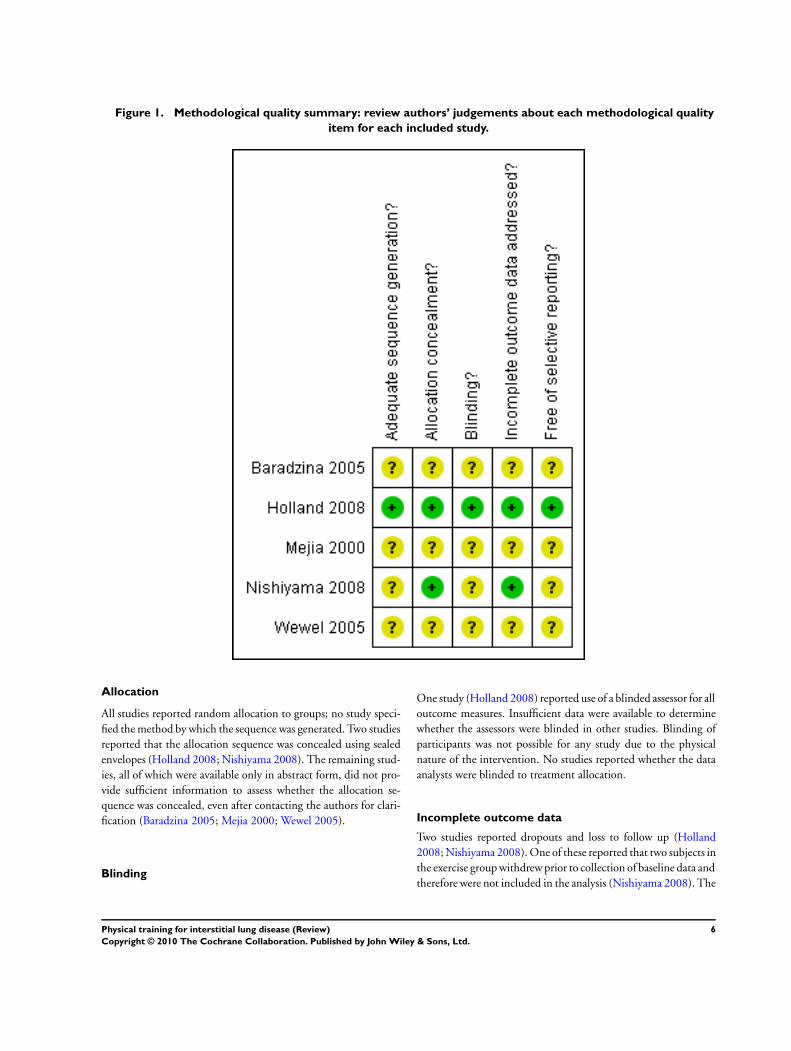
Figure 1. Methodological quality summary: review authors’ judgements about each methodological quality
item for each included study.
Allocation
All studies reported random allocation to groups; no study speci-
fied the method by which the sequence was generated. Two studies
reported that the allocation sequence was concealed using sealed
envelopes (Holland 2008; Nishiyama 2008). The remaining stud-
ies, all of which were available only in abstract form, did not pro-
vide sufficient information to assess whether the allocation se-
quence was concealed, even after contacting the authors for clari-
fication (Baradzina 2005; Mejia 2000; Wewel 2005).
Blinding
One study (Holland 2008) reported use of a blinded assessor for all
outcome measures. Insufficient data were available to determine
whether the assessors were blinded in other studies. Blinding of
participants was not possible for any study due to the physical
nature of the intervention. No studies reported whether the data
analysts were blinded to treatment allocation.
Incomplete outcome data
Two studies reported dropouts and loss to follow up (Holland
2008; Nishiyama 2008). One of these reported that two subjects in
the exercise group withdrew prior to collection of baseline data and
therefore were not included in the analysis (Nishiyama 2008). The
6Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
other study reported a significant number of dropouts, with data
analysis performed according to the intention to treat principle and
using the last observation carried forward method where data were
not available (Holland 2008). The other studies did not report
whether there were any dropouts or losses to follow up.
Selective reporting
One study was listed on a clinical trial registry (Holland 2008)
and results were reported for all outcomes at all time points. It was
not possible to determine whether all data were available for the
other studies. As three studies were available only in abstract form
(Baradzina 2005; Mejia 2000; Wewel 2005) it is likely that not all
data are currently available.
Effects of interventions
Data and analyses tables summarize the results of the meta-analysis
for the comparison of physical training versus no physical training.
Sufficient data were available from two studies for pooling in a
meta-analysis (Holland 2008, Nishiyama 2008).
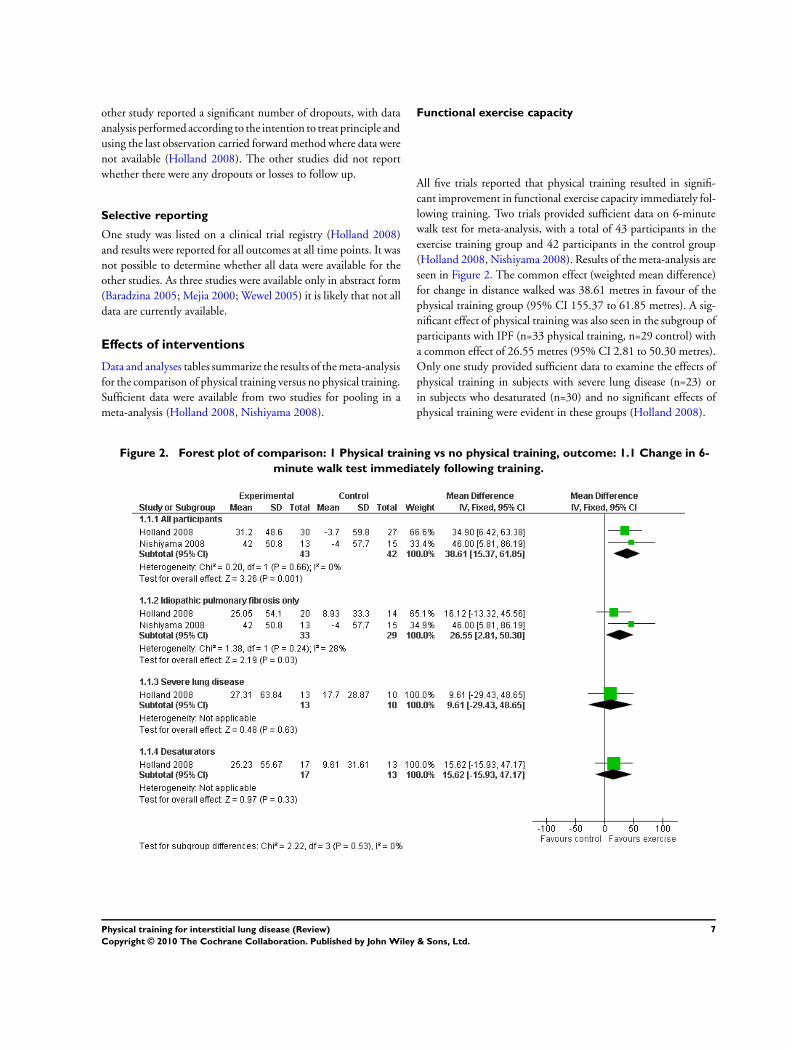
Functional exercise capacity
All five trials reported that physical training resulted in signifi-
cant improvement in functional exercise capacity immediately fol-
lowing training. Two trials provided sufficient data on 6-minute
walk test for meta-analysis, with a total of 43 participants in the
exercise training group and 42 participants in the control group
(Holland 2008, Nishiyama 2008). Results of the meta-analysis are
seen in Figure 2. The common effect (weighted mean difference)
for change in distance walked was 38.61 metres in favour of the
physical training group (95% CI 155.37 to 61.85 metres). A sig-
nificant effect of physical training was also seen in the subgroup of
participants with IPF (n=33 physical training, n=29 control) with
a common effect of 26.55 metres (95% CI 2.81 to 50.30 metres).
Only one study provided sufficient data to examine the effects of
physical training in subjects with severe lung disease (n=23) or
in subjects who desaturated (n=30) and no significant effects of
physical training were evident in these groups (Holland 2008).
Figure 2. Forest plot of comparison: 1 Physical training vs no physical training, outcome: 1.1 Change in 6-
minute walk test immediately following training.
7Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
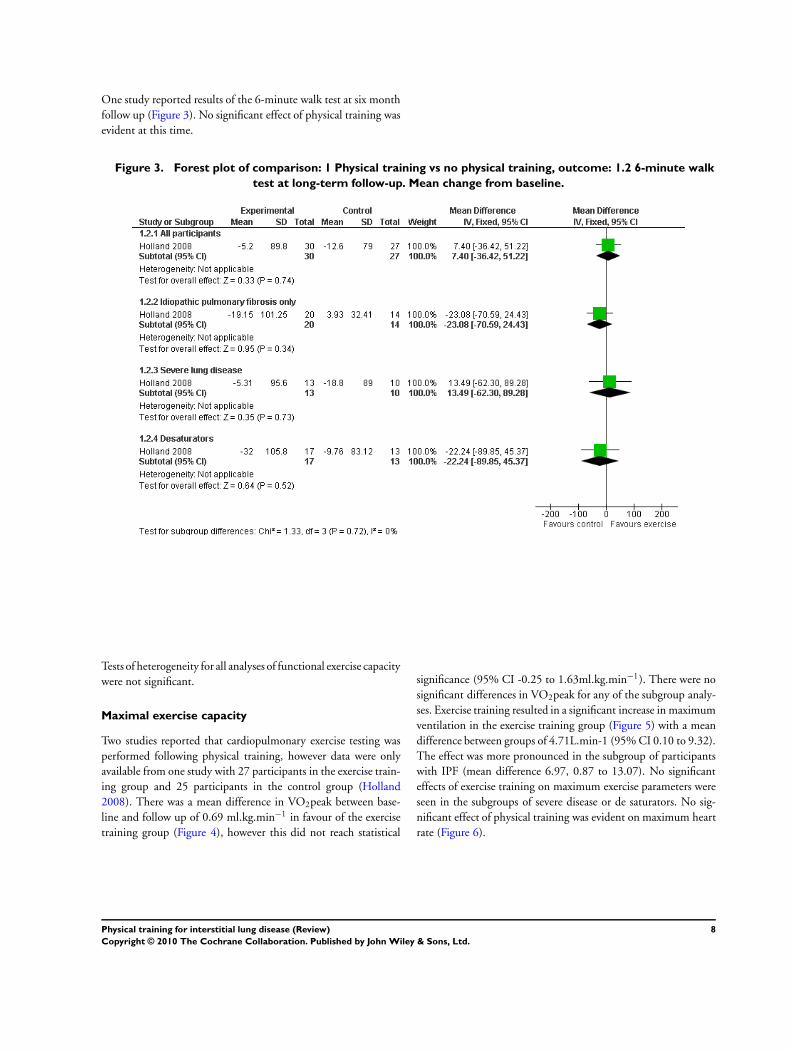
One study reported results of the 6-minute walk test at six month
follow up (Figure 3). No significant effect of physical training was
evident at this time.
Figure 3. Forest plot of comparison: 1 Physical training vs no physical training, outcome: 1.2 6-minute walk
test at long-term follow-up. Mean change from baseline.
Tests of heterogeneity for all analyses of functional exercise capacity
were not significant.
Maximal exercise capacity
Two studies reported that cardiopulmonary exercise testing was
performed following physical training, however data were only
available from one study with 27 participants in the exercise train-
ing group and 25 participants in the control group (Holland
2008). There was a mean difference in VO2peak between base-
line and follow up of 0.69 ml.kg.min−1 in favour of the exercise
training group (Figure 4), however this did not reach statistical
significance (95% CI -0.25 to 1.63ml.kg.min−1). There were no
significant differences in VO2peak for any of the subgroup analy-
ses. Exercise training resulted in a significant increase in maximum
ventilation in the exercise training group (Figure 5) with a mean
difference between groups of 4.71L.min-1 (95% CI 0.10 to 9.32).
The effect was more pronounced in the subgroup of participants
with IPF (mean difference 6.97, 0.87 to 13.07). No significant
effects of exercise training on maximum exercise parameters were
seen in the subgroups of severe disease or de saturators. No sig-
nificant effect of physical training was evident on maximum heart
rate (Figure 6).
8Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
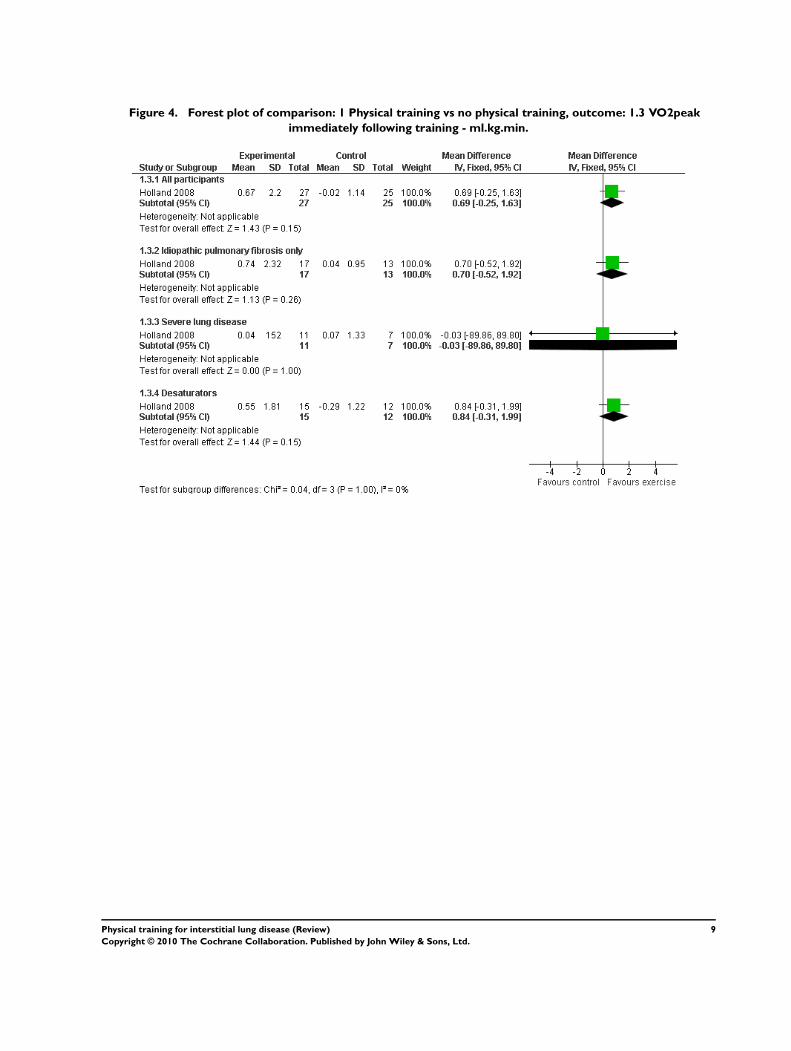
Figure 4. Forest plot of comparison: 1 Physical training vs no physical training, outcome: 1.3 VO2peak
immediately following training - ml.kg.min.
9Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
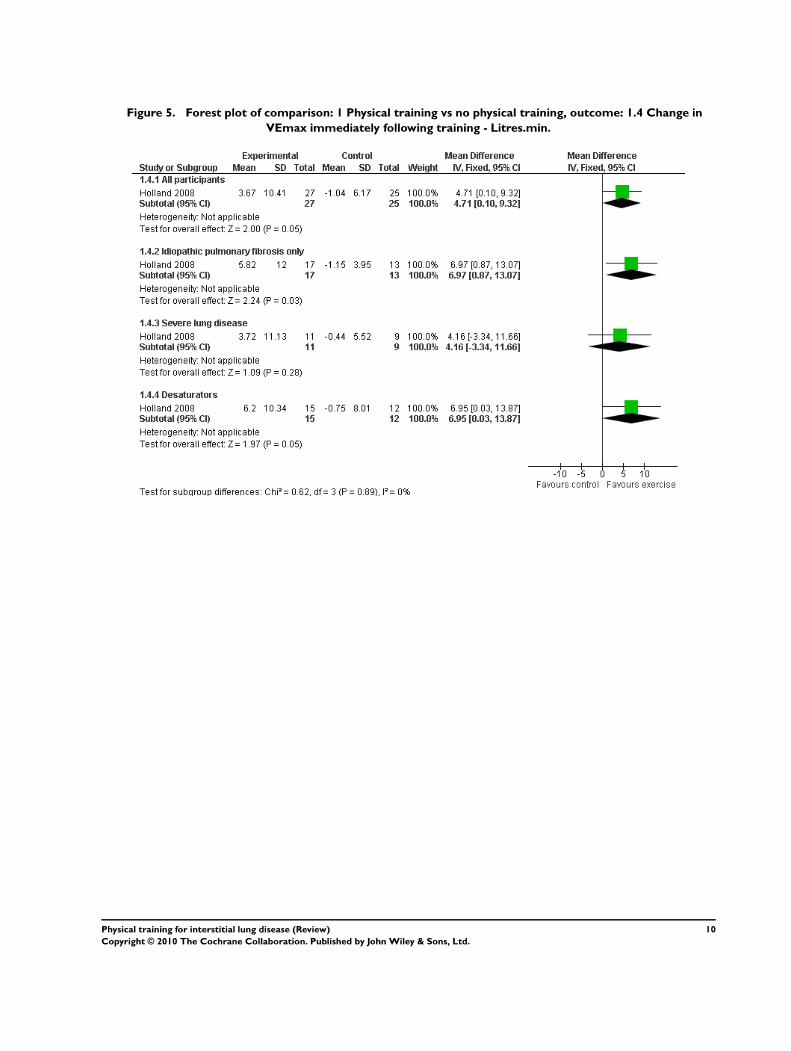
Figure 5. Forest plot of comparison: 1 Physical training vs no physical training, outcome: 1.4 Change in
VEmax immediately following training - Litres.min.
10Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
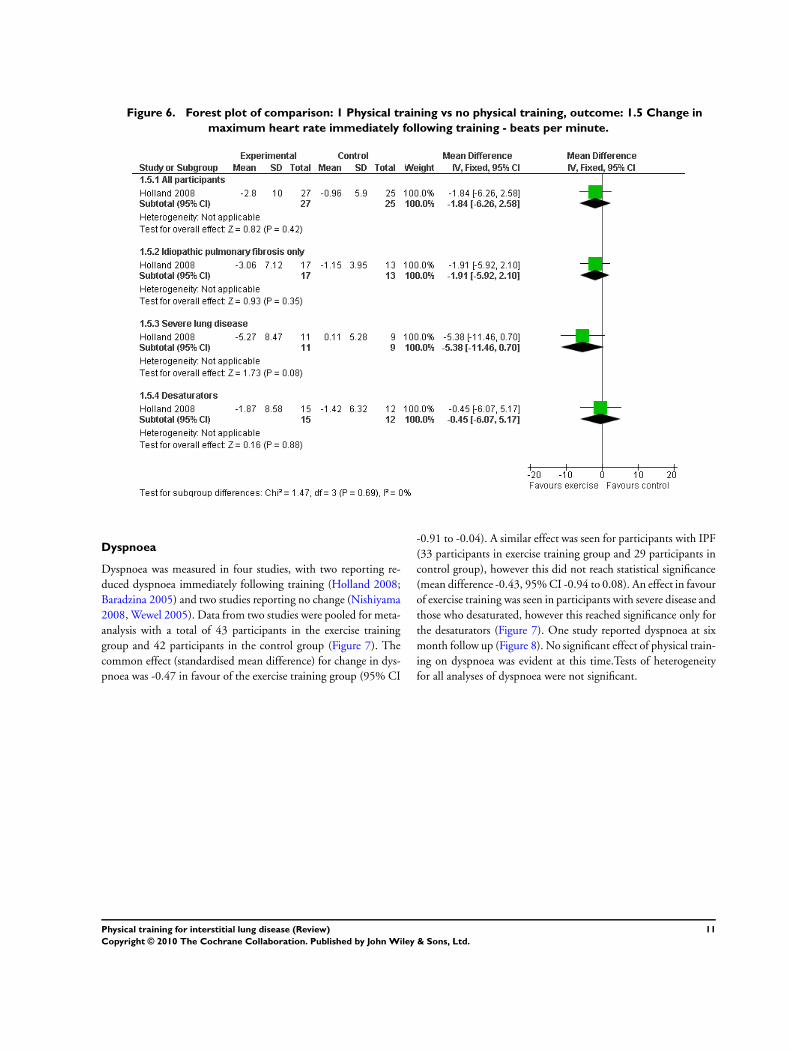
Figure 6. Forest plot of comparison: 1 Physical training vs no physical training, outcome: 1.5 Change in
maximum heart rate immediately following training - beats per minute.
Dyspnoea
Dyspnoea was measured in four studies, with two reporting re-
duced dyspnoea immediately following training (Holland 2008;
Baradzina 2005) and two studies reporting no change (Nishiyama
2008, Wewel 2005). Data from two studies were pooled for meta-
analysis with a total of 43 participants in the exercise training
group and 42 participants in the control group (Figure 7). The
common effect (standardised mean difference) for change in dys-
pnoea was -0.47 in favour of the exercise training group (95% CI
-0.91 to -0.04). A similar effect was seen for participants with IPF
(33 participants in exercise training group and 29 participants in
control group), however this did not reach statistical significance
(mean difference -0.43, 95% CI -0.94 to 0.08). An effect in favour
of exercise training was seen in participants with severe disease and
those who desaturated, however this reached significance only for
the desaturators (Figure 7). One study reported dyspnoea at six
month follow up (Figure 8). No significant effect of physical train-
ing on dyspnoea was evident at this time.Tests of heterogeneity
for all analyses of dyspnoea were not significant.
11Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
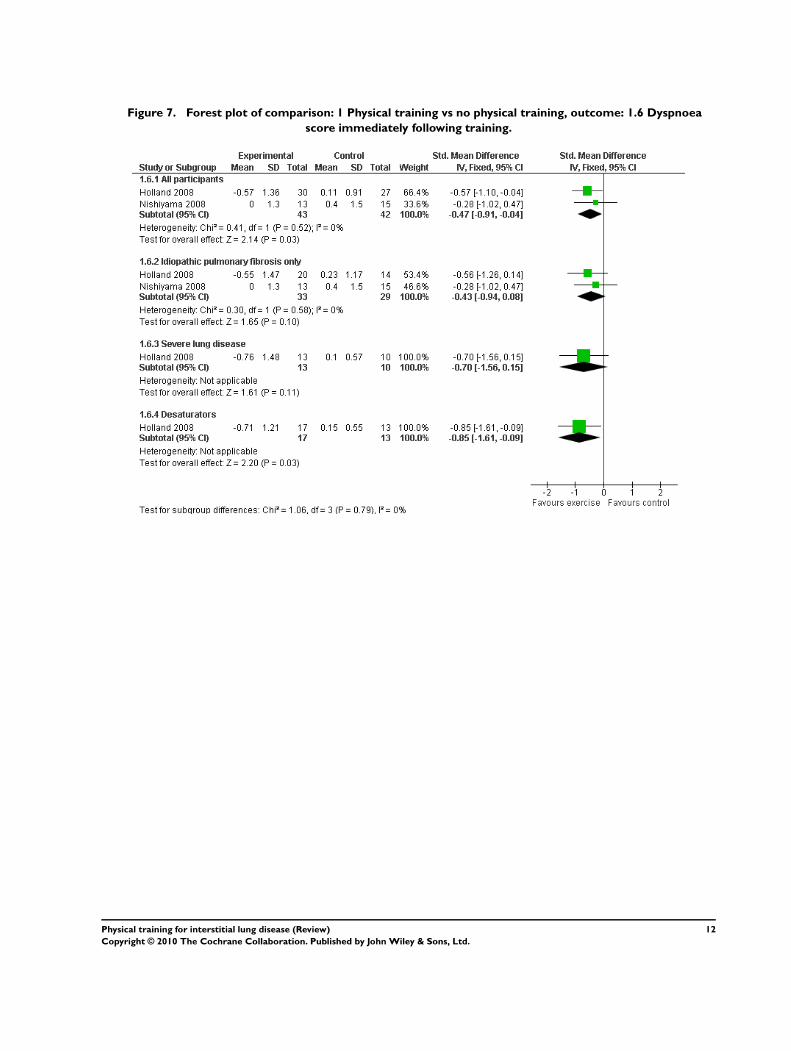
Figure 7. Forest plot of comparison: 1 Physical training vs no physical training, outcome: 1.6 Dyspnoea
score immediately following training.
12Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
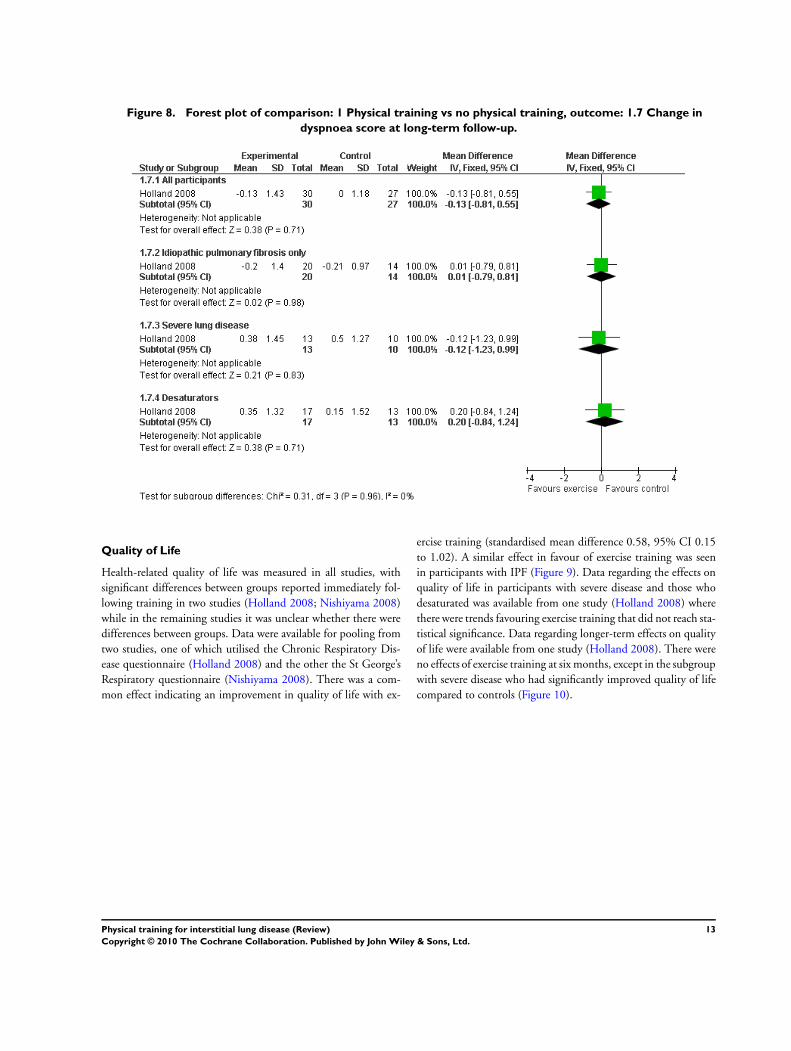
Figure 8. Forest plot of comparison: 1 Physical training vs no physical training, outcome: 1.7 Change in
dyspnoea score at long-term follow-up.
Quality of Life
Health-related quality of life was measured in all studies, with
significant differences between groups reported immediately fol-
lowing training in two studies (Holland 2008; Nishiyama 2008)
while in the remaining studies it was unclear whether there were
differences between groups. Data were available for pooling from
two studies, one of which utilised the Chronic Respiratory Dis-
ease questionnaire (Holland 2008) and the other the St George’s
Respiratory questionnaire (Nishiyama 2008). There was a com-
mon effect indicating an improvement in quality of life with ex-
ercise training (standardised mean difference 0.58, 95% CI 0.15
to 1.02). A similar effect in favour of exercise training was seen
in participants with IPF (Figure 9). Data regarding the effects on
quality of life in participants with severe disease and those who
desaturated was available from one study (Holland 2008) where
there were trends favouring exercise training that did not reach sta-
tistical significance. Data regarding longer-term effects on quality
of life were available from one study (Holland 2008). There were
no effects of exercise training at six months, except in the subgroup
with severe disease who had significantly improved quality of life
compared to controls (Figure 10).
13Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
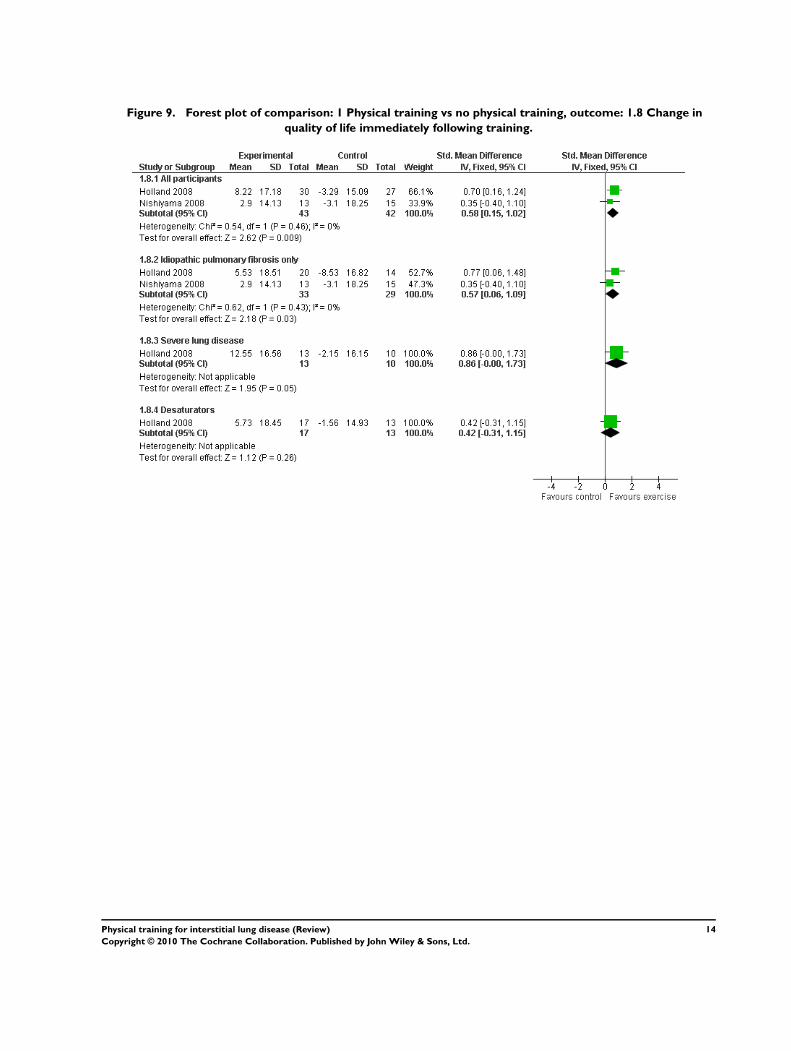
Figure 9. Forest plot of comparison: 1 Physical training vs no physical training, outcome: 1.8 Change in
quality of life immediately following training.
14Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
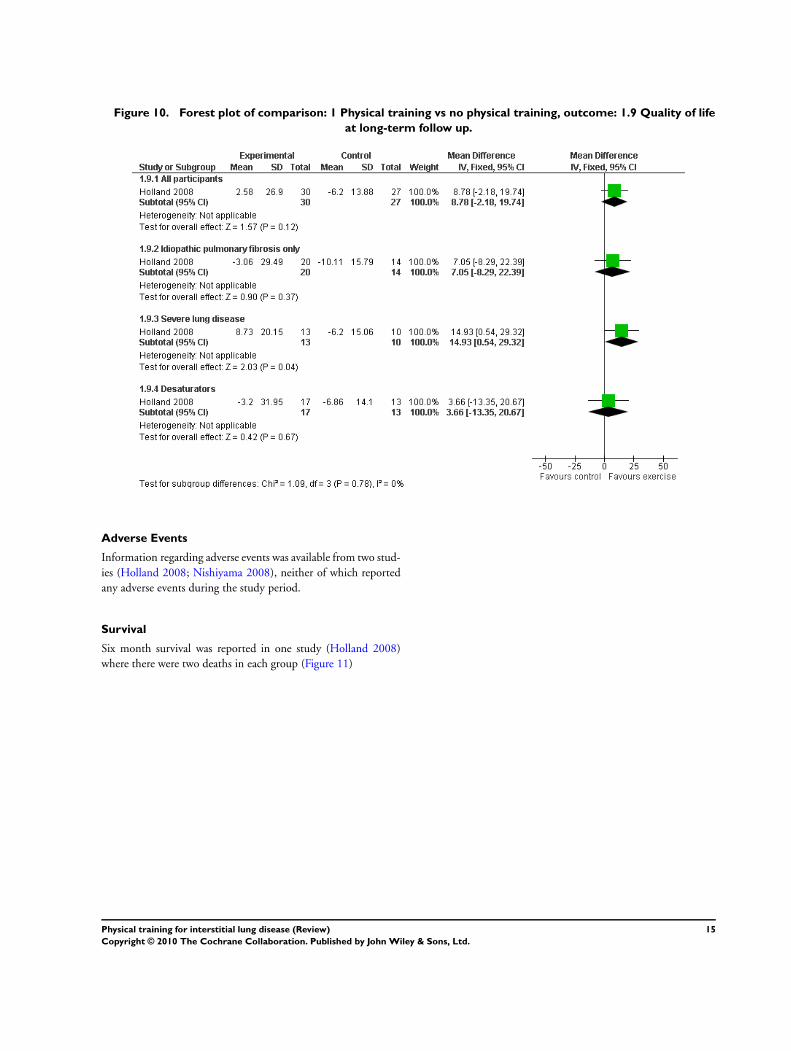
Figure 10. Forest plot of comparison: 1 Physical training vs no physical training, outcome: 1.9 Quality of life
at long-term follow up.
Adverse Events
Information regarding adverse events was available from two stud-
ies (Holland 2008; Nishiyama 2008), neither of which reported
any adverse events during the study period.
Survival
Six month survival was reported in one study (Holland 2008)
where there were two deaths in each group (Figure 11)
15Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
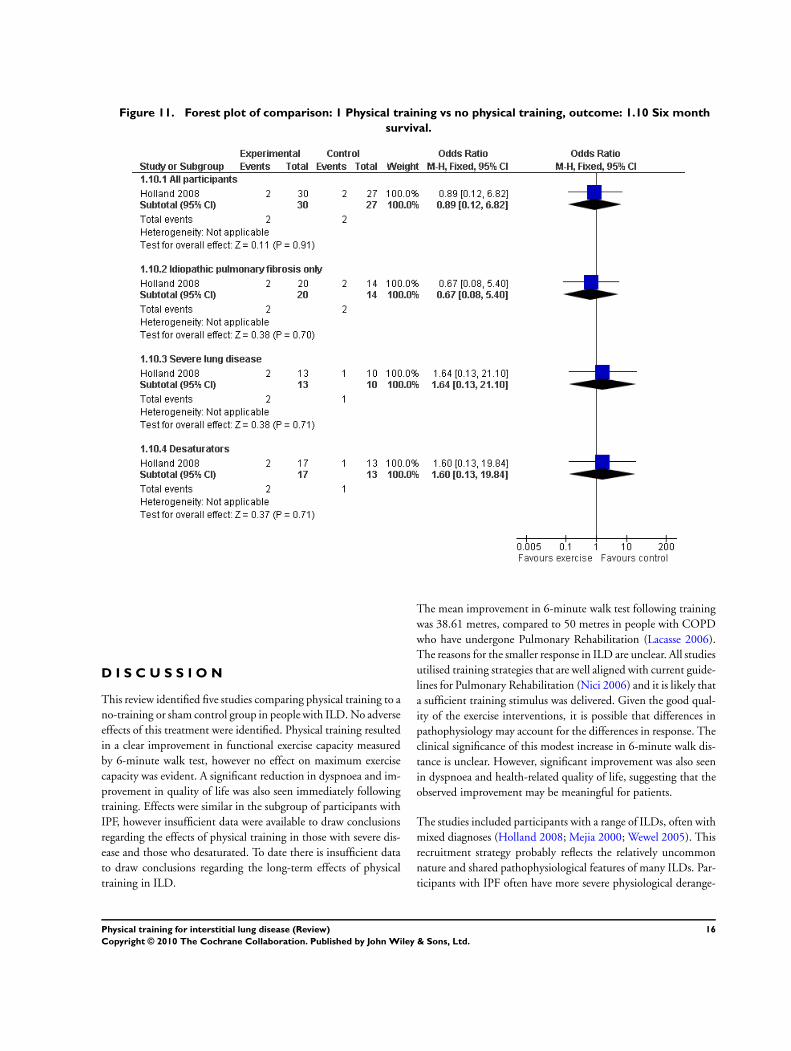
Figure 11. Forest plot of comparison: 1 Physical training vs no physical training, outcome: 1.10 Six month
survival.
D I S C U S S I O N
This review identified five studies comparing physical training to a
no-training or sham control group in people with ILD. No adverse
effects of this treatment were identified. Physical training resulted
in a clear improvement in functional exercise capacity measured
by 6-minute walk test, however no effect on maximum exercise
capacity was evident. A significant reduction in dyspnoea and im-
provement in quality of life was also seen immediately following
training. Effects were similar in the subgroup of participants with
IPF, however insufficient data were available to draw conclusions
regarding the effects of physical training in those with severe dis-
ease and those who desaturated. To date there is insufficient data
to draw conclusions regarding the long-term effects of physical
training in ILD.
The mean improvement in 6-minute walk test following training
was 38.61 metres, compared to 50 metres in people with COPD
who have undergone Pulmonary Rehabilitation (Lacasse 2006).
The reasons for the smaller response in ILD are unclear. All studies
utilised training strategies that are well aligned with current guide-
lines for Pulmonary Rehabilitation (Nici 2006) and it is likely that
a sufficient training stimulus was delivered. Given the good qual-
ity of the exercise interventions, it is possible that differences in
pathophysiology may account for the differences in response. The
clinical significance of this modest increase in 6-minute walk dis-
tance is unclear. However, significant improvement was also seen
in dyspnoea and health-related quality of life, suggesting that the
observed improvement may be meaningful for patients.
The studies included participants with a range of ILDs, often with
mixed diagnoses (Holland 2008; Mejia 2000; Wewel 2005). This
recruitment strategy probably reflects the relatively uncommon
nature and shared pathophysiological features of many ILDs. Par-
ticipants with IPF often have more severe physiological derange-
16Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

ment and a more rapid disease course compared to other ILDs
(Lama 2004) and we hypothesised that physical training might be
less effective in people with IPF. However, this review indicated
that IPF participants did achieve significant improvements in 6-
minute walk test and health-related quality of life. It should be
noted however that of the two studies contributing to the meta-
analysis, one included IPF participants only (Nishiyama 2008)
whilst the other had a majority of participants with IPF (Holland
2008) and thus the overall results of the meta-analysis are heavily
influenced by the response of IPF participants.
All studies in this review utilised either aerobic exercise training
or a combination of aerobic and resisted exercise training. These
strategies are well aligned with current guidelines for Pulmonary
Rehabilitation (Nici 2006) and the results are therefore readily
applicable to clinical practice in Pulmonary Rehabilitation pro-
grams. However, we were unable to draw any inferences regard-
ing the most effective exercise training strategy for people with
ILD. Given the relatively modest improvements in exercise capac-
ity documented here, this may be an important area for future
research. The included studies used a range of program durations
(five weeks to six months) and training frequencies (2-5 sessions
per week). Longer programs and more frequent sessions appear to
yield greater benefits in people with other chronic lung diseases
(Nici 2006). To date the most effective dose of physical training
for people with ILD has not been established.
There are a number of potential sources of bias in this review.
Of the five studies identified, three were available only in abstract
form (Baradzina 2005; Mejia 2000; Wewel 2005). These publica-
tions provided little data regarding the outcomes of interest and it
was not possible to obtain additional data from the authors. The
remaining two studies therefore provided all the data that could
be pooled for meta-analysis. Despite this limitation, there was
consistency in most reported outcomes, with all studies reporting
improved functional exercise capacity following exercise training.
Assessment of study quality was also difficult due to the limited
availability of data. As exercise training is a physical intervention
it can be assumed that no participants were blinded, however only
one study reported blinding of the assessor (Holland 2008). Only
one study reported use of an intention-to-treat analysis (Holland
2008). Given the progressive nature of many ILDs, a significant
dropout rate is likely and may impact both on the size of the re-
ported treatment effect and the feasibility of the intervention.
A U T H O R S ’ C O N C L U S I O N SImplications for practice
This review indicates that physical training is safe for people with
ILD and results in significantly improved functional exercise ca-
pacity, dyspnoea and health-related quality of life immediately fol-
lowing training. It is appropriate to include people with ILD in a
standard Pulmonary Rehabilitation program. To date there is little
evidence of a long-term benefit of physical training in ILD.
Implications for research
Further studies are required to identify whether the magnitude of
improvement following physical training is greater in participants
who do not have IPF. The optimum exercise training method for
participants with ILD has not been established and requires fur-
ther investigation in light of the modest response to training docu-
mented here. Large studies are also required to determine whether
the benefits of physical training vary according to disease severity
and whether there are any longer term effects of physical training
in ILD. Future trials should ensure that assessors are blinded to
the intervention and that appropriate methods are used to account
for dropouts.
A C K N O W L E D G E M E N T S
We thank John White who was the contact editor for this review.
We would also like to thank Toby Lasserson for support and guid-
ance.
R E F E R E N C E S
References to studies included in this review
Baradzina 2005 {published data only}
Baradzina HL, Ponachevnaya NV. Pulmonary rehabilitation
programme in sarcoidosis (abstract). European Respiratory
Journal 2005;26(Suppl. 49):333s.
Holland 2008 {published and unpublished data}
Holland AE, Hill CJ, Conron M, Munro P, McDonald CF.
Short-term improvement in exercise capacity and symptoms
following exercise training in interstitial lung disease.
Thorax 2008;63:549–5.
Mejia 2000 {published data only}
Mejia RA, Sansores RH, Perez-Padilla R, Mahler DA.
Effects of exercise training on ’quality of life’ in patients with
interstitial lung diseases (abstract). European Respiratory
Journal 2000;16(Suppl. 31):330s.
Nishiyama 2008 {published and unpublished data}∗ Nishiyama O, Kondoh Y, Kimura T, Kato K, Kataoka
A, Ogawa T, et al.Effects of pulmonary rehabilitation in
patients with idiopathic pulmonary fibrosis. Respirology
2008;13:394–9.
Nishiyama O, Taniguchi H, Kondoh Y, Kimura T, Ogawa
17Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
T, Watanabe F, et al.Pulmonary Rehabilitation in Idiopathic
Pulmonary Fibrosis. American Thoracic Society 100th
International Conference, Orlando, May 21-26. 2004:D96
Poster 110.
Wewel 2005 {published data only}
Behnke M, Schwertfeger I, Zimmerman I, Kirsten D,
Joerres RAJ, Magnussen H. Home-based exercise training
in patients with interstitial lung disease (abstract). European
Respiratory Journal 2003;22(Suppl 45):Abstract No: [1081].∗ Wewel AR, Behnke M, Schwertfeger I, Eberhardt F,
Kroidl RF, Jorres RA, et al.Home-based walking training in
patients with interstitial lung diseases (abstract). European
Respiratory Journal 2005;26(Suppl. 49):528s.
References to studies excluded from this review
Cockcroft 1981 {published data only}
Cockcroft AE, Saunders MJ, Berry G. Randomised
controlled trial of rehabilitation in chronic respiratory
disability. Thorax 198;36:200–3.
Cockcroft 1982 {published data only}
Cockcroft AE, Berry G, Brown EB, Exall C. Psychological
changes during a controlled trial of rehabilitation in chronic
respiratory disability. Thorax 1982;37:413–6.
Daltroy 1995 {published data only}
Daltroy LH, Robb-Nicholson C, Iverson MD, Wright EA,
Liang MH. Effectiveness of minimally supervised home
aerobic training in patients with systemic rheumatic disease.
British Journal of Rheumatology 1995;34:1064–9.
Jastrzebski 2006 {published data only}
Jastrzebski D, Gumola A, Gawlik R, Kozielski J. Dyspnoea
and quality of life in patients with pulmonary fibrosis after
six weeks of respiratory rehabilitation. Journal of Physiology
and Pharmacology 2006;57(Suppl. 4):139–48.
Naji 2006 {published data only}
Naji NA, Connor MC. Donnelly SC, McDonnell TJ.
Effectiveness of Pulmonary Rehabilitation in Restrictive
Lung Disease. Journal of Cardiopulmonary Rehabilitation
2006;26:237–43.
Oh 2003 {published and unpublished data}
Oh E. The effects of home-based pulmonary rehabilitation
in patients with chronic lung disease. International Journal
of Nursing Studies 2003;40:873–9.
Ong 2001 {published data only}
Ong KC, Wong WP, Jailani AR, Sew S, Ong YY. Effects of
a pulmonary rehabilitation programme on physiologic and
psychosocial outcomes in patients wtih chronic respiratory
disorders. Annals of the Academy of Medicine, Singapore
2001;30:15–21.
Senstrom 1996 {published data only}
Senstrom CH, Arge B, Sundbom A. Dynamic training
vs relaxation training as home exercise for patients wtih
inflammatory rheumatic diseases. Scandinavian Journal of
Rheumatology 1996;25:28–33.
Senstrom 1997 {published data only}
Senstrom CH, Arge B, Sundbom A. Home exercise
and compliance in inflammatory rheumatic diseases - a
prospective clinical trial. Journal of Rheumatology 1997;24:
470–6.
Tryfon 2003 {published data only}
Tryfon SM, Mavrofridis E, Ilonidis G, Patakas D.
Cardiopulmonary effects of exercise, before and after oxygen
delivery, in patients with usual interstitial pneumonia.
European Respiratory Journal 2003;22(Suppl 45):Abstract
No: [P639].
Additional references
Agusti 1991
Agusti AG, Roca J, Gea J, Wagner PD, Xaubet A, Rodriguez-
Roisin R. Mechanisms of gas-exchange impairment
in idiopathic pulmonary fibrosis. American Review of
Respiratory Disease 1991;143(2):219–25.
ATS/ERS 2000
American Thoracic Society. Idiopathic pulmonary fibrosis:
diagnosis and treatment. International consensus statement.
American Thoracic Society (ATS), and the European
Respiratory Society (ERS). American Journal of Respiratory
and Critical Care Medicine 2000;161(2):646–64.
Chang 1999
Chang JA, Curtis JR, Patrick DL, Raghu G. Assessment of
health-related quality of life in patients with interstitial lung
disease. Chest 1999;116(5):1175–82.
Hansen 1996
Hansen JE, Wasserman K. Pathophysiology of activity
limitation in patients with interstitial lung disease. Chest
1996;109(6):1566–76.
Harris-Eze 1996
Harris-Eze AO, Sridhar G, Clemens RE, Zintel TA,
Gallagher CG, Marciniuk DD. Role of hypoxemia and
pulmonary mechanics in exercise limitation in interstitial
lung disease. American Journal of Respiratory & Critical Care
Medicine 1996;154(4 Pt 1):994–1001.
Lacasse 2006
Lacasse Y, Goldstein R, Lasserson TJ, Martin S. Pulmonary
rehabilitation for chronic obstructive pulmonary
disease. Cochrane Database of Systematic Reviews 2006,
Issue 4. [Art. No.: CD003793. DOI: 10.1002/
14651858.CD003793.pub2]
Lama 2004
Lama VN, Martinez FJ. Resting and exercise physiology in
interstitial lung diseases. Clinical Chest Medicine 2004;25:
435–53.
Markovitz 1998
Markovitz GH, Cooper CB. Exercise and interstitial lung
disease. Current Opinion in Pulmonary Medicine 1998;4(5):
272–80.
Miki 2003
Miki K, Maekura R, Hiraga T, Okuda Y, Okamoto T,
Hirotani A, et al.Impairments and prognostic factors for
18Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

survival in patients with idiopathic pulmonary fibrosis.
Respiratory Medicine 2003;97(5):482–90.
Nici 2006
Nici L, Donner C, Wouters E, Zuwallack R, Ambrosino N,
Bourbeau J, et al.American Thoracic Society / European
Respiratory Society statement on pulmonary rehabilitation.
American Journal of Respiratory & Critical Care Medicine
2006;173(12):1390–413.∗ Indicates the major publication for the study
19Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
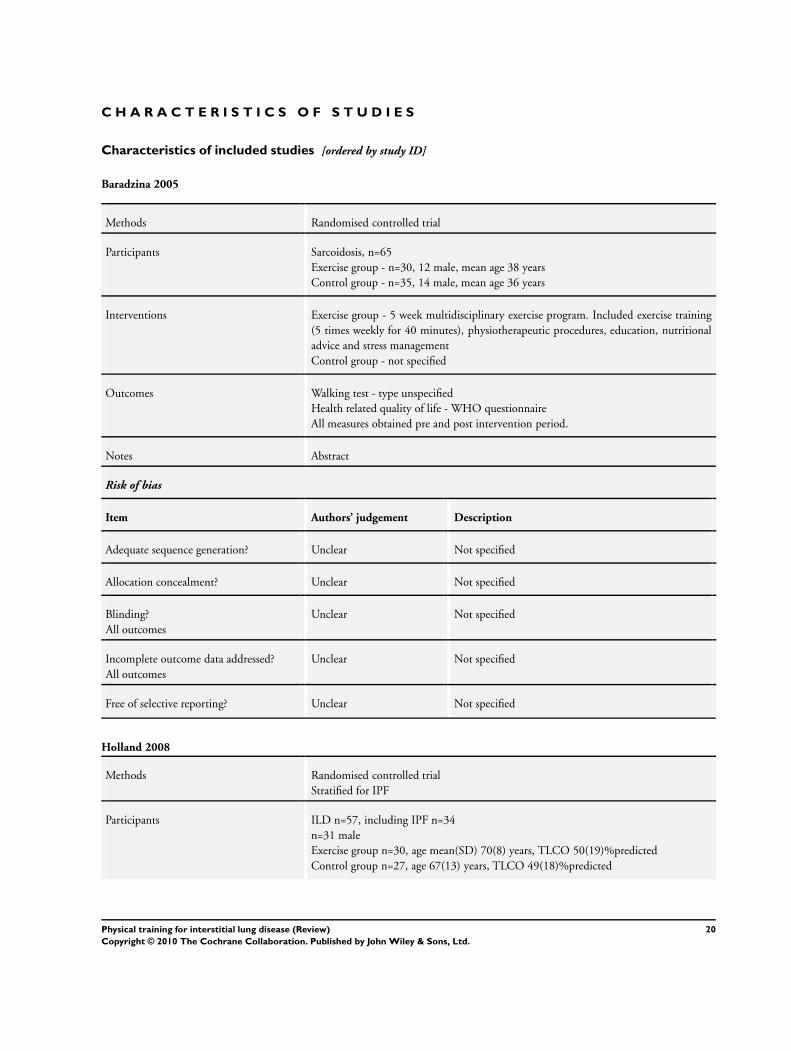
Baradzina 2005
Methods Randomised controlled trial
Participants Sarcoidosis, n=65
Exercise group - n=30, 12 male, mean age 38 years
Control group - n=35, 14 male, mean age 36 years
Interventions Exercise group - 5 week multidisciplinary exercise program. Included exercise training
(5 times weekly for 40 minutes), physiotherapeutic procedures, education, nutritional
advice and stress management
Control group - not specified
Outcomes Walking test - type unspecified
Health related quality of life - WHO questionnaire
All measures obtained pre and post intervention period.
Notes Abstract
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Not specified
Allocation concealment? Unclear Not specified
Blinding?
All outcomes
Unclear Not specified
Incomplete outcome data addressed?
All outcomes
Unclear Not specified
Free of selective reporting? Unclear Not specified
Holland 2008
Methods Randomised controlled trial
Stratified for IPF
Participants ILD n=57, including IPF n=34
n=31 male
Exercise group n=30, age mean(SD) 70(8) years, TLCO 50(19)%predicted
Control group n=27, age 67(13) years, TLCO 49(18)%predicted
20Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Holland 2008 (Continued)
Interventions Exercise group - 8 week outpatient exercise program, twice weekly supervised sessions
consisting of 30 minutes endurance exercise (cycling and walking) with initial intensity at
80% of walking speed on initial 6-minute walk test and progressed according to protocol.
Upper limb endurance and functional strength training for lower limbs also performed.
Supplemental oxygen provided for SpO2>85%. Unsupervised home exercise program
prescribed 3 times per week
Control group - weekly telephone calls for general health advice and support
Outcomes 6-minute walk test
Cardiopulmonary exercise test
Chronic Respiratory Disease questionnaire
Modified Medical Research Council scale
Measured pre and post intervention period. 6 minute walk test and questionnaires re-
peated at 6 month follow up
Notes Supported by the Victorian Tuberculosis and Lung Association
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Yes Computer generated random number se-
quence
Allocation concealment? Yes Central location, sealed opaque envelope
Blinding?
All outcomes
Yes Data collector blinded to treatment alloca-
tion.
Incomplete outcome data addressed?
All outcomes
Yes Intention to treat analysis, last observation
carried forward
Free of selective reporting? Yes All data available at all time points
Mejia 2000
Methods Randomised controlled trial
Participants ILD n=22
FVC 61(19)%predicted, age 52(14) years
Interventions 12 week exercise program, three times weekly supervised sessions of 30-35 minutes each,
interval training
Exercise training group - exercised at 60% of maximal power output on cycle ergometer
Control group - sham exercise training at minimum workload achievable on cycle er-
gometer (no resistance)
21Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
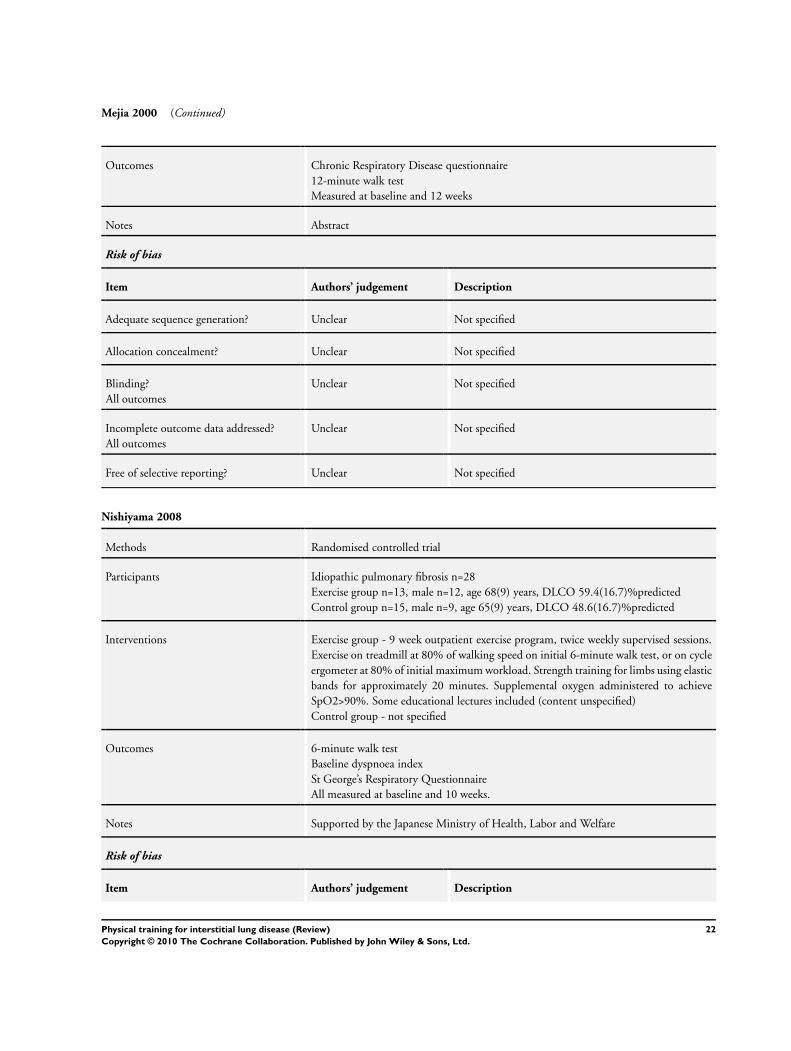
Mejia 2000 (Continued)
Outcomes Chronic Respiratory Disease questionnaire
12-minute walk test
Measured at baseline and 12 weeks
Notes Abstract
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Not specified
Allocation concealment? Unclear Not specified
Blinding?
All outcomes
Unclear Not specified
Incomplete outcome data addressed?
All outcomes
Unclear Not specified
Free of selective reporting? Unclear Not specified
Nishiyama 2008
Methods Randomised controlled trial
Participants Idiopathic pulmonary fibrosis n=28
Exercise group n=13, male n=12, age 68(9) years, DLCO 59.4(16.7)%predicted
Control group n=15, male n=9, age 65(9) years, DLCO 48.6(16.7)%predicted
Interventions Exercise group - 9 week outpatient exercise program, twice weekly supervised sessions.
Exercise on treadmill at 80% of walking speed on initial 6-minute walk test, or on cycle
ergometer at 80% of initial maximum workload. Strength training for limbs using elastic
bands for approximately 20 minutes. Supplemental oxygen administered to achieve
SpO2>90%. Some educational lectures included (content unspecified)
Control group - not specified
Outcomes 6-minute walk test
Baseline dyspnoea index
St George’s Respiratory Questionnaire
All measured at baseline and 10 weeks.
Notes Supported by the Japanese Ministry of Health, Labor and Welfare
Risk of bias
Item Authors’ judgement Description
22Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
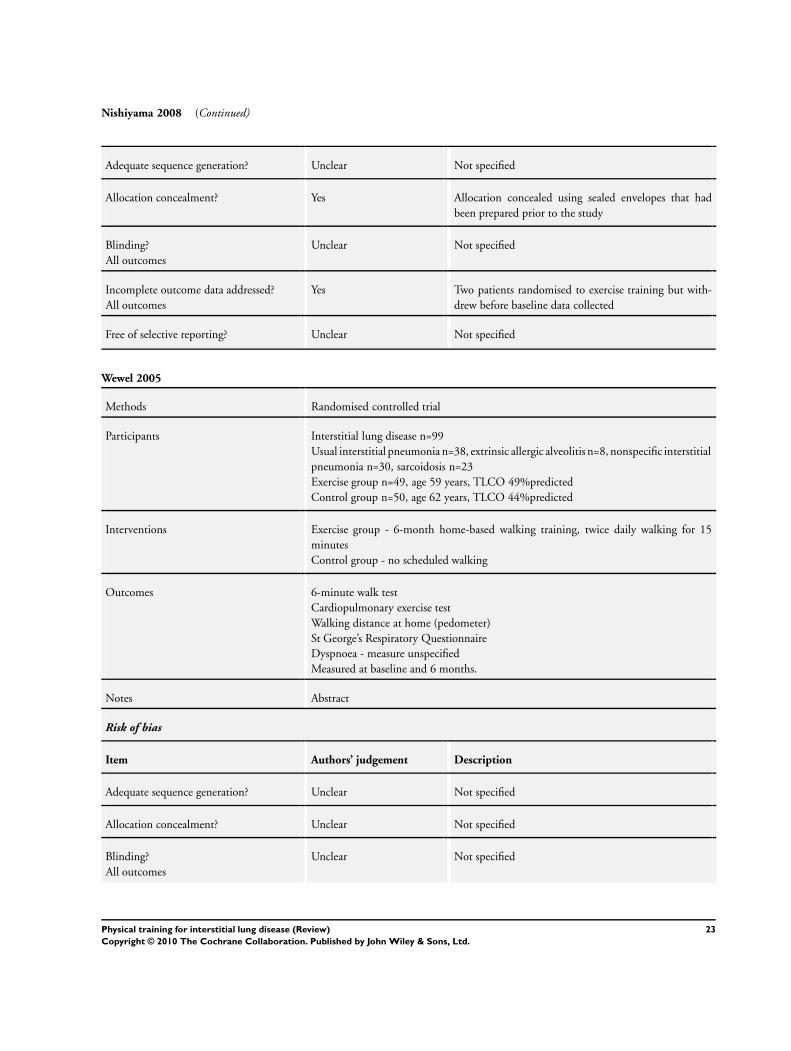
Nishiyama 2008 (Continued)
Adequate sequence generation? Unclear Not specified
Allocation concealment? Yes Allocation concealed using sealed envelopes that had
been prepared prior to the study
Blinding?
All outcomes
Unclear Not specified
Incomplete outcome data addressed?
All outcomes
Yes Two patients randomised to exercise training but with-
drew before baseline data collected
Free of selective reporting? Unclear Not specified
Wewel 2005
Methods Randomised controlled trial
Participants Interstitial lung disease n=99
Usual interstitial pneumonia n=38, extrinsic allergic alveolitis n=8, nonspecific interstitial
pneumonia n=30, sarcoidosis n=23
Exercise group n=49, age 59 years, TLCO 49%predicted
Control group n=50, age 62 years, TLCO 44%predicted
Interventions Exercise group - 6-month home-based walking training, twice daily walking for 15
minutes
Control group - no scheduled walking
Outcomes 6-minute walk test
Cardiopulmonary exercise test
Walking distance at home (pedometer)
St George’s Respiratory Questionnaire
Dyspnoea - measure unspecified
Measured at baseline and 6 months.
Notes Abstract
Risk of bias
Item Authors’ judgement Description
Adequate sequence generation? Unclear Not specified
Allocation concealment? Unclear Not specified
Blinding?
All outcomes
Unclear Not specified
23Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
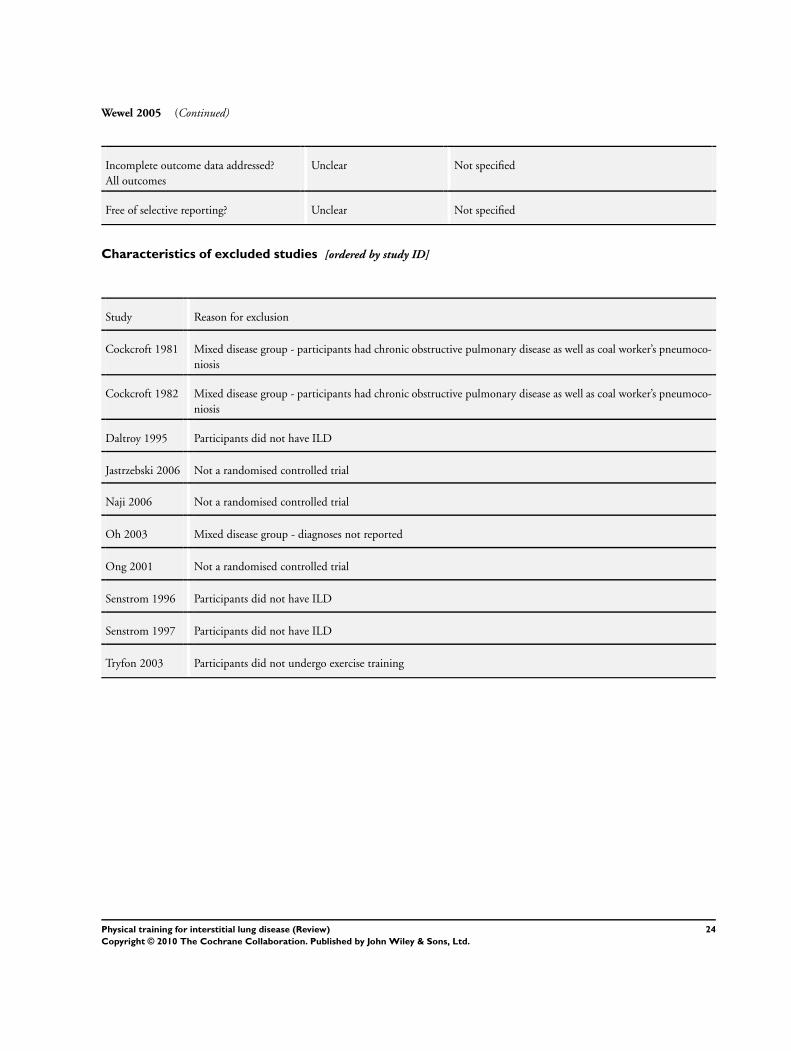
Wewel 2005 (Continued)
Incomplete outcome data addressed?
All outcomes
Unclear Not specified
Free of selective reporting? Unclear Not specified
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Cockcroft 1981 Mixed disease group - participants had chronic obstructive pulmonary disease as well as coal worker’s pneumoco-
niosis
Cockcroft 1982 Mixed disease group - participants had chronic obstructive pulmonary disease as well as coal worker’s pneumoco-
niosis
Daltroy 1995 Participants did not have ILD
Jastrzebski 2006 Not a randomised controlled trial
Naji 2006 Not a randomised controlled trial
Oh 2003 Mixed disease group - diagnoses not reported
Ong 2001 Not a randomised controlled trial
Senstrom 1996 Participants did not have ILD
Senstrom 1997 Participants did not have ILD
Tryfon 2003 Participants did not undergo exercise training
24Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
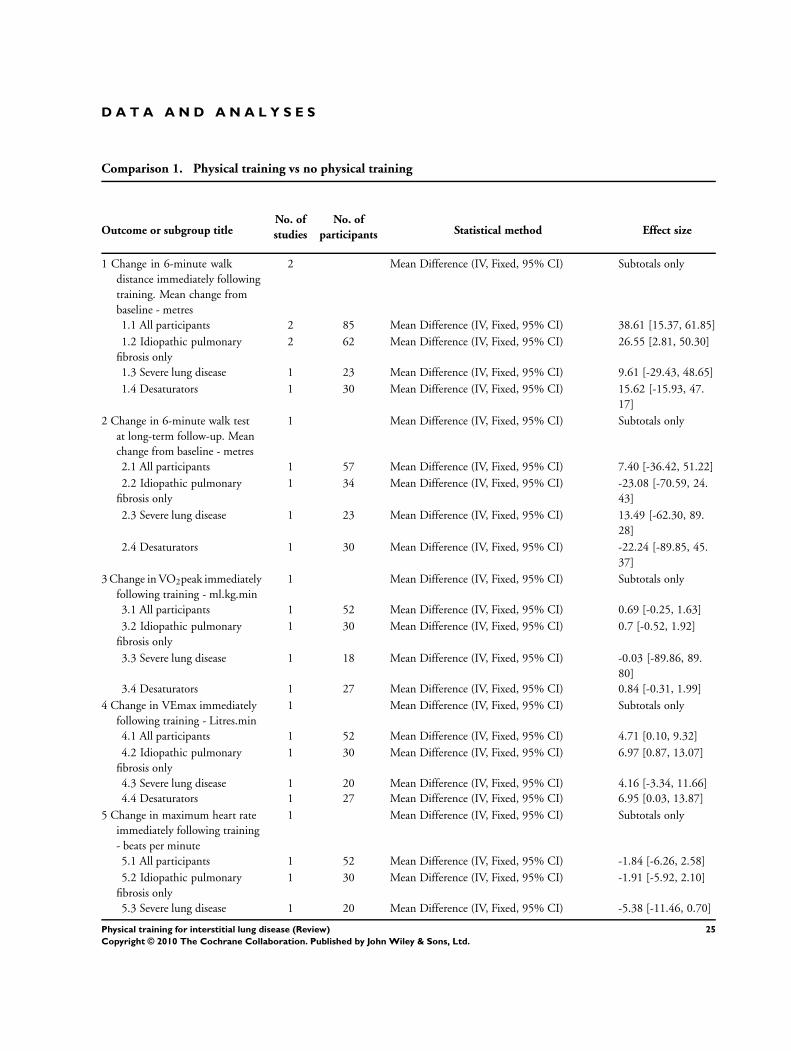
D A T A A N D A N A L Y S E S
Comparison 1. Physical training vs no physical training
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Change in 6-minute walk
distance immediately following
training. Mean change from
baseline - metres
2 Mean Difference (IV, Fixed, 95% CI) Subtotals only
1.1 All participants 2 85 Mean Difference (IV, Fixed, 95% CI) 38.61 [15.37, 61.85]
1.2 Idiopathic pulmonary
fibrosis only
2 62 Mean Difference (IV, Fixed, 95% CI) 26.55 [2.81, 50.30]
1.3 Severe lung disease 1 23 Mean Difference (IV, Fixed, 95% CI) 9.61 [-29.43, 48.65]
1.4 Desaturators 1 30 Mean Difference (IV, Fixed, 95% CI) 15.62 [-15.93, 47.
17]
2 Change in 6-minute walk test
at long-term follow-up. Mean
change from baseline - metres
1 Mean Difference (IV, Fixed, 95% CI) Subtotals only
2.1 All participants 1 57 Mean Difference (IV, Fixed, 95% CI) 7.40 [-36.42, 51.22]
2.2 Idiopathic pulmonary
fibrosis only
1 34 Mean Difference (IV, Fixed, 95% CI) -23.08 [-70.59, 24.
43]
2.3 Severe lung disease 1 23 Mean Difference (IV, Fixed, 95% CI) 13.49 [-62.30, 89.
28]
2.4 Desaturators 1 30 Mean Difference (IV, Fixed, 95% CI) -22.24 [-89.85, 45.
37]
3 Change in VO2peak immediately
following training - ml.kg.min
1 Mean Difference (IV, Fixed, 95% CI) Subtotals only
3.1 All participants 1 52 Mean Difference (IV, Fixed, 95% CI) 0.69 [-0.25, 1.63]
3.2 Idiopathic pulmonary
fibrosis only
1 30 Mean Difference (IV, Fixed, 95% CI) 0.7 [-0.52, 1.92]
3.3 Severe lung disease 1 18 Mean Difference (IV, Fixed, 95% CI) -0.03 [-89.86, 89.
80]
3.4 Desaturators 1 27 Mean Difference (IV, Fixed, 95% CI) 0.84 [-0.31, 1.99]
4 Change in VEmax immediately
following training - Litres.min
1 Mean Difference (IV, Fixed, 95% CI) Subtotals only
4.1 All participants 1 52 Mean Difference (IV, Fixed, 95% CI) 4.71 [0.10, 9.32]
4.2 Idiopathic pulmonary
fibrosis only
1 30 Mean Difference (IV, Fixed, 95% CI) 6.97 [0.87, 13.07]
4.3 Severe lung disease 1 20 Mean Difference (IV, Fixed, 95% CI) 4.16 [-3.34, 11.66]
4.4 Desaturators 1 27 Mean Difference (IV, Fixed, 95% CI) 6.95 [0.03, 13.87]
5 Change in maximum heart rate
immediately following training
- beats per minute
1 Mean Difference (IV, Fixed, 95% CI) Subtotals only
5.1 All participants 1 52 Mean Difference (IV, Fixed, 95% CI) -1.84 [-6.26, 2.58]
5.2 Idiopathic pulmonary
fibrosis only
1 30 Mean Difference (IV, Fixed, 95% CI) -1.91 [-5.92, 2.10]
5.3 Severe lung disease 1 20 Mean Difference (IV, Fixed, 95% CI) -5.38 [-11.46, 0.70]
25Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
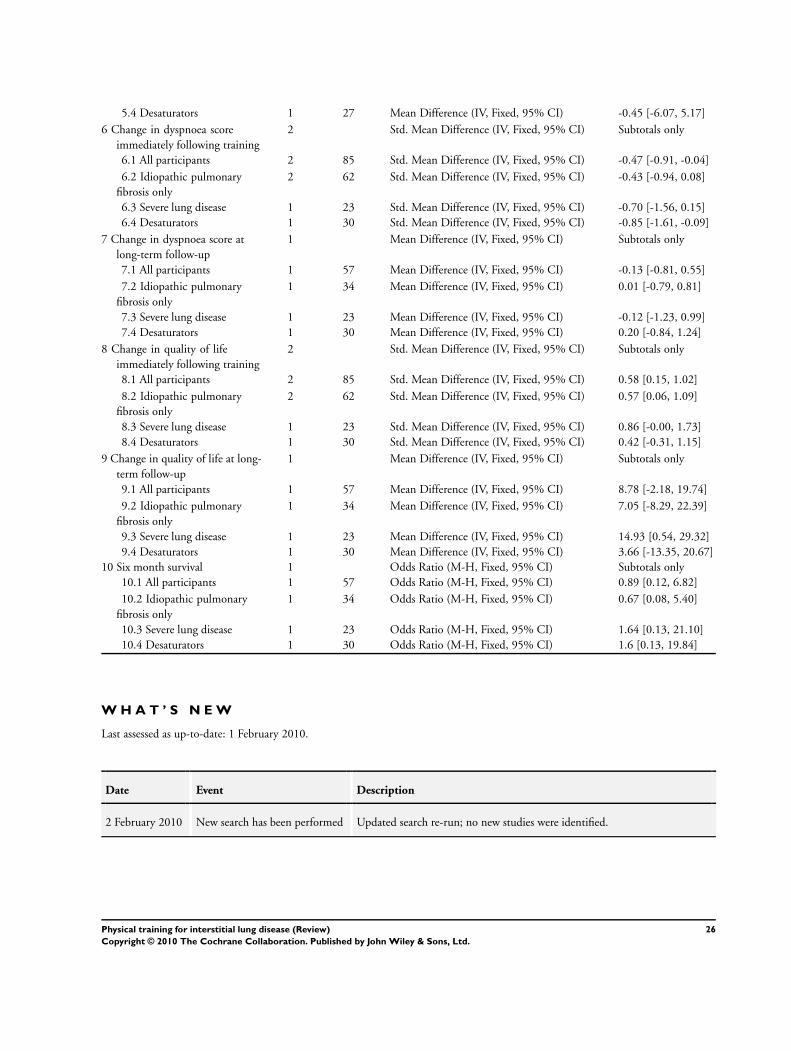
5.4 Desaturators 1 27 Mean Difference (IV, Fixed, 95% CI) -0.45 [-6.07, 5.17]
6 Change in dyspnoea score
immediately following training
2 Std. Mean Difference (IV, Fixed, 95% CI) Subtotals only
6.1 All participants 2 85 Std. Mean Difference (IV, Fixed, 95% CI) -0.47 [-0.91, -0.04]
6.2 Idiopathic pulmonary
fibrosis only
2 62 Std. Mean Difference (IV, Fixed, 95% CI) -0.43 [-0.94, 0.08]
6.3 Severe lung disease 1 23 Std. Mean Difference (IV, Fixed, 95% CI) -0.70 [-1.56, 0.15]
6.4 Desaturators 1 30 Std. Mean Difference (IV, Fixed, 95% CI) -0.85 [-1.61, -0.09]
7 Change in dyspnoea score at
long-term follow-up
1 Mean Difference (IV, Fixed, 95% CI) Subtotals only
7.1 All participants 1 57 Mean Difference (IV, Fixed, 95% CI) -0.13 [-0.81, 0.55]
7.2 Idiopathic pulmonary
fibrosis only
1 34 Mean Difference (IV, Fixed, 95% CI) 0.01 [-0.79, 0.81]
7.3 Severe lung disease 1 23 Mean Difference (IV, Fixed, 95% CI) -0.12 [-1.23, 0.99]
7.4 Desaturators 1 30 Mean Difference (IV, Fixed, 95% CI) 0.20 [-0.84, 1.24]
8 Change in quality of life
immediately following training
2 Std. Mean Difference (IV, Fixed, 95% CI) Subtotals only
8.1 All participants 2 85 Std. Mean Difference (IV, Fixed, 95% CI) 0.58 [0.15, 1.02]
8.2 Idiopathic pulmonary
fibrosis only
2 62 Std. Mean Difference (IV, Fixed, 95% CI) 0.57 [0.06, 1.09]
8.3 Severe lung disease 1 23 Std. Mean Difference (IV, Fixed, 95% CI) 0.86 [-0.00, 1.73]
8.4 Desaturators 1 30 Std. Mean Difference (IV, Fixed, 95% CI) 0.42 [-0.31, 1.15]
9 Change in quality of life at long-
term follow-up
1 Mean Difference (IV, Fixed, 95% CI) Subtotals only
9.1 All participants 1 57 Mean Difference (IV, Fixed, 95% CI) 8.78 [-2.18, 19.74]
9.2 Idiopathic pulmonary
fibrosis only
1 34 Mean Difference (IV, Fixed, 95% CI) 7.05 [-8.29, 22.39]
9.3 Severe lung disease 1 23 Mean Difference (IV, Fixed, 95% CI) 14.93 [0.54, 29.32]
9.4 Desaturators 1 30 Mean Difference (IV, Fixed, 95% CI) 3.66 [-13.35, 20.67]
10 Six month survival 1 Odds Ratio (M-H, Fixed, 95% CI) Subtotals only
10.1 All participants 1 57 Odds Ratio (M-H, Fixed, 95% CI) 0.89 [0.12, 6.82]
10.2 Idiopathic pulmonary
fibrosis only
1 34 Odds Ratio (M-H, Fixed, 95% CI) 0.67 [0.08, 5.40]
10.3 Severe lung disease 1 23 Odds Ratio (M-H, Fixed, 95% CI) 1.64 [0.13, 21.10]
10.4 Desaturators 1 30 Odds Ratio (M-H, Fixed, 95% CI) 1.6 [0.13, 19.84]
W H A T ’ S N E W
Last assessed as up-to-date: 1 February 2010.
Date Event Description
2 February 2010 New search has been performed Updated search re-run; no new studies were identified.
26Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
H I S T O R Y
Protocol first published: Issue 1, 2007
Review first published: Issue 4, 2008
Date Event Description
28 January 2009 Amended Contact details changed
10 April 2008 Amended Converted to new review format.
11 October 2006 New citation required and major changes Substantive amendment
C O N T R I B U T I O N S O F A U T H O R S
Initiation of protocol: AH
Protocol development: AH and CH
Undertook search: AH
Retrieved papers : AH
Screened retrieved papers against eligibility criteria: AH and CH
Appraised quality: AH and CH
Extracted data: AH and CH
Wrote to authors for additional information: AH
Entered data into RevMan: AH
Analysis: AH and CH
Wrote review: AH and CH
Guarantor of the review: AH
D E C L A R A T I O N S O F I N T E R E S T
AH and CH conducted one of the studies included in this review.
27Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
S O U R C E S O F S U P P O R T
Internal sources
• No sources of support supplied
External sources
• Victorian Tuberculosis and Lung Association, Australia.
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
Subgroup analysis for exercise type could not be conducted as we did not identify any trials of resistance training. Sensitivity analysis
was not performed and funnel plots were not constructed due to the small number of included studies. If in future updates there are
more studies included then these analyses will be performed.
I N D E X T E R M S
Medical Subject Headings (MeSH)
∗Exercise; Exercise Therapy; Exercise Tolerance; Lung Diseases, Interstitial [physiopathology; ∗rehabilitation]; Randomized Controlled
Trials as Topic
MeSH check words
Humans
28Physical training for interstitial lung disease (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.