Embed Size (px)
Citation preview
Continuous subcutaneous insulin infusion (CSII) versus
multiple insulin injections for type 1 diabetes mellitus
(Review)
Misso ML, Egberts KJ, Page M, O’Connor D, Shaw J
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2010, Issue 1
http://www.thecochranelibrary.com
Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Figure 3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Figure 4. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10
Figure 5. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
Figure 6. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
Figure 7. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
18DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
20AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
20ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
21REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
32CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
88DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
90ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
93CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
94DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
94DIFFERENCES BETWEEN PROTOCOL AND REVIEW . . . . . . . . . . . . . . . . . . . . .
94INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iContinuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Continuous subcutaneous insulin infusion (CSII) versusmultiple insulin injections for type 1 diabetes mellitus
Marie L Misso1 , Kristine J Egberts2, Matthew Page3, Denise O’Connor3 , Jonathan Shaw4
1Australasian Cochrane Centre, Clayton, Australia. 2Centre for Obesity Research and Education (CORE), Monash University, Mel-
bourne, Australia. 3Australasian Cochrane Centre, Monash Institute of Health Services Research, Monash University, Clayton, Aus-
tralia. 4Baker IDI Heart and Diabetes Institute, Victoria, Australia
Contact address: Marie L Misso, Australasian Cochrane Centre, Monash Institute of Health Services Research, Monash University, 43-
51 Kanooka Grove, Clayton, Victoria, 3168, Australia. [email protected].
Editorial group: Cochrane Metabolic and Endocrine Disorders Group.
Publication status and date: New, published in Issue 1, 2010.
Review content assessed as up-to-date: 19 July 2009.
Citation: Misso ML, Egberts KJ, Page M, O’Connor D, Shaw J. Continuous subcutaneous insulin infusion (CSII) versus multiple
insulin injections for type 1 diabetes mellitus. Cochrane Database of Systematic Reviews 2010, Issue 1. Art. No.: CD005103. DOI:
10.1002/14651858.CD005103.pub2.
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
Type 1 diabetes is a metabolic disorder resulting from a defect in insulin secretion. Onset of type 1 diabetes mellitus may occur at any
age and it is one of the most common chronic diseases of childhood and adolescence. Since there are no interventions known to prevent
onset, it is vital that effective treatment regimes are available. Glycaemic control is maintained by replacement of insulin and may be
in the form of ’conventional’ insulin therapy (multiple injections per day) or continuous subcutaneous insulin infusion (CSII).
Objectives
To assess the effects of CSII compared to multiple insulin injections (MI) in people with type 1 diabetes mellitus.
Search methods
Studies were obtained from electronic searches of The Cochrane Library, MEDLINE, EMBASE and CINAHL.
Selection criteria
Studies were included if they were randomised controlled trials comparing CSII with three or more insulin injections per day (MI) in
people with type 1 diabetes mellitus.
Data collection and analysis
Two authors independently assessed risk of bias and extracted characteristics of included studies. Authors contacted study investigators
to obtain missing information. Generic inverse variance meta-analyses using a random-effects model were performed.
Main results
Twenty three studies randomised 976 participants with type 1 diabetes to either intervention. There was a statistically significant
difference in glycosylated haemoglobin A1c (HbA1c) favouring CSII (weighted mean difference -0.3% (95% confidence interval -
0.1 to -0.4). There were no obvious differences between the interventions for non-severe hypoglycaemia, but severe hypoglycaemia
appeared to be reduced in those using CSII. Quality of life measures suggest that CSII is preferred over MI. No significant difference
was found for weight. Adverse events were not well reported, no information is available on mortality, morbidity and costs.
1Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Authors’ conclusions
There is some evidence to suggest that CSII may be better than MI for glycaemic control in people with type 1 diabetes. Non-
severe hypoglycaemic events do not appear to be reduced with CSII. There is insufficient evidence regarding adverse events, mortality,
morbidity and costs.
P L A I N L A N G U A G E S U M M A R Y
Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus
Type 1 diabetes results from a defect in insulin secretion, leading to elevated levels of plasma sugar or glucose and disturbances in
carbohydrate, fat and protein metabolism. Complications may effect the eyes, kidneys, nerves and the cardiovascular system. Type 1
diabetes may occur at any age and it is one of the most common chronic diseases of childhood and adolescence. Type 1 diabetes impacts
heavily on the lifestyle of the individual as well as their families. Since there is no cure or prevention for type 1 diabetes, life-long
insulin replacement and monitoring of blood glucose levels are required. It is vital that effective insulin therapy regimes are available
for optimal management and to minimise blood glucose fluctuation (known as too low or too high blood sugar levels - hypoglycaemia
or hyperglycaemia).
Insulin therapy may be in the form of ’conventional’ therapy of multiple (typically four) injections per day or continuous subcutaneous
insulin infusion. Continuous subcutaneous insulin infusion involves attachment (via catheter on the outside of the body) to an insulin
pump that is programmed to deliver insulin to match the individual’s needs, and doses are activated by the individual to cover meals
and correct blood glucose fluctuation. Here we explore whether continuous subcutaneous insulin infusion is better than three or more
insulin injections per day for good management of type 1 diabetes.
Twenty three studies randomised 976 participants with type 1 diabetes to either continuous subcutaneous insulin infusion or multiple
injections. Seven of the 23 studies were performed in participants under 18 years of age and the remainder were performed in adults.
Study duration ranged from six days to four years. The body of evidence suggests that continuous subcutaneous insulin infusion may be
better than multiple injections for glycaemic control in people with type 1 diabetes; continuous subcutaneous insulin infusion appears
to provide no benefit for reducing non-severe hypoglycaemic events. Future studies need to consider the short and long term adverse
effects, mortality, morbidity and costs of these interventions.
B A C K G R O U N D
Description of the condition
Type 1 diabetes results from a defect in insulin secretion. A con-
sequence of this is chronic hyperglycaemia (that is elevated lev-
els of plasma glucose) with disturbances of carbohydrate, fat and
protein metabolism. Long-term complications of diabetes melli-
tus include retinopathy, nephropathy and neuropathy. The risk
of cardiovascular disease is increased. For a detailed overview of
diabetes mellitus, please see under ’Additional information’ in the
information on the Metabolic and Endocrine Disorders Group
on the Cochrane Library (see ’About the Cochrane Collabora-
tion’, ’Collaborative Review Groups-CRGs’). For an explanation
of methodological terms, see the main Glossary on The CochraneLibrary.
The onset of type 1 diabetes mellitus may occur at any age and it is
one of the most common chronic diseases of childhood and ado-
lescence. In adults with type 1 diabetes, vascular complications are
a major cause of mortality (Couper 2002). Based on young onset
patients, the incidence of this disease worldwide varies from 0.1
to 37.4 per 100,000 (Karvonen 2000). The EURODIAB Study
Group predicts that between 2005 and 2020, new cases of type 1
diabetes in European children younger than five years will double
and that the prevalence of cases in those younger than 15 years will
increase by 70% (Dabelea 2009). Type 1 diabetes impacts heavily
on the lifestyle of the individual as well as their families. Life-long
insulin replacement and monitoring of blood glucose levels are
required and patients are prone to acute and late complications of
diabetes (for example cardiovascular disease) that are influenced
by diabetes control. Moreover, the economic burden is high for
the individual, the family, the health care sector and society as a
2Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

whole, where significant health care costs arise not only at diagno-
sis but also for subsequent admissions to hospital (Sutton 1990).
Description of the intervention
Since there are no interventions shown to delay or prevent the
onset of type 1 diabetes (DPT 2002; ENDIT 2003), it is vital that
effective treatment regimes are available for optimal management
of this disease. Glycaemic control is maintained by replacement of
insulin. Insulin is administered subcutaneously from where insulin
is absorbed into the bloodstream. Here, complexes are formed en-
abling binding to the insulin receptor for activation of glucose
uptake into the muscle. There are various regimes for insulin ad-
ministration. Ideally, an individual’s insulin replacement regimen
should provide appropriate basal insulin requirements across 24
hours, provide sufficient levels to cover food intake, have ade-
quate provision for correction when needed, minimise blood glu-
cose fluctuation and therefore risk of hypoglycaemia and hyper-
glycaemia and achieve short-term and long-term targets (APEG
2004). Insulin therapy may be executed in the form of ’conven-
tional’ insulin therapy of multiple injections (like 2 to 4 injec-
tions per day) or continuous subcutaneous insulin infusion (CSII).
The multiple injection form of therapy may consist of adminis-
tering rapid-acting, short-acting, intermediate-acting or long-act-
ing types of insulin (APEG 2004), which differ in relation both
to their speed of onset and duration of glucose-lowering action.
For example, rapid-acting insulins typically begin to lower glucose
within 5 to 10 minutes of injection, and last for 4 to 6 hours,
while short-acting insulins take at least 20 minutes to begin to
act, and can last for up to eight hours. In contrast, CSII typically
administers a rapid-acting insulin (analogue) via an insulin pump
programmed to deliver basal rates to match the individual’s needs
and bolus doses are activated by the individual to cover meals and
correct hyperglycaemia. Insulin pumps are worn by the individual
externally and insulin is delivered from the pump via insertion
of a catheter into the subcutaneous tissue of the abdominal wall
(Pickup 1980a). In this review, we define multiple insulin injec-
tions as three or more per day (MI).
How the intervention might work
While CSII and MI are both successful methods of insulin therapy,
it has been suggested that CSII may be a superior alternative since
it allows to more closely mimic normal physiology and eliminate
the need for repeat injections. CSII may provide a more efficient
mode of insulin delivery to the bloodstream, minimise the risk of
hypoglycaemic events and may be more beneficial to those who
find it difficult to adhere to a regimen of multiple injections.
Adverse effects of the intervention
Potential adverse events that may arise include pump malfunction,
catheter-site infection, irritation, diabetic ketoacidosis or discom-
fort (Guinn 1988).
Why it is important to do this review
Three systematic reviews comparing MI with CSII have been pub-
lished (HTA 2004; NICE 2008; Pickup 2002). The review by
Pickup et al provides an overview of the studies located, however
there are some limitations. Firstly, on-going study and abstract
searches have not been documented, therefore it is possible that
relevant studies may have been overlooked. Secondly, important
aspects such as the search strategy and methods of study randomi-
sation have not been documented. The Health Technology As-
sessment (HTA) report and the National Institute for Clinical Ex-
cellence (NICE) guidelines are methodologically rigorous, how-
ever the most up-to-date search strategies were conducted in 2007
and therefore do not include recent randomised controlled trials.
Given the limitations of these previous systematic reviews, it is
important that we have considered these factors and used specific
methodology and criteria outlined by the Cochrane Collaboration
in our aim to present a comprehensive systematic review to assess
the effects of CSII compared to MI. Where possible and feasible,
we have performed meta-analyses.
O B J E C T I V E S
To assess the effects of continuous subcutaneous insulin infusion
(CSII) compared to multiple insulin injection for type 1 diabetes
mellitus.
M E T H O D S
Criteria for considering studies for this review
Types of studies
All published and unpublished randomised and quasi-randomised
controlled trials (blind and open, parallel and cross-over) designed
to compare people with type 1 diabetes taking insulin in the form
of either continuous subcutaneous insulin infusion (CSII) or mul-
tiple insulin injections (MI) (three or more insulin injections per
day). There were no time or language restrictions.
3Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Types of participants
Males and females with type 1 diabetes of any age taking insulin
treatment were considered in this review. The diagnostic criteria
for type 1 diabetes mellitus should have been described in the study.
To remain consistent with changes in classification and diagnostic
criteria through the years, diagnosis of type 1 diabetes status was
based upon the diagnostic criteria valid at the time of beginning
the study. Acceptable diagnostic criteria included those described
by the National Diabetes Data Group standards (NDDG 1979),
the World Health Organisation (WHO 1980), the American Di-
abetes Association (ADA 1997) or by the author of the study (in
these cases, attempts were made to contact study investigators to
determine specific criteria used to diagnose type 1 diabetes).
Types of interventions
Insulin preparation and dose of insulin varied depending on the
study, therefore all insulin preparations and doses were accepted.
Intervention
Continuous subcutaneous insulin infusion (CSII).
Control
Multiple insulin injections (MI) (three or more insulin injections
per day).
Types of outcome measures
Primary outcomes
• glycaemic control (glycosylated haemoglobin A1c (HbA1c),
daily mean blood glucose, fasting blood glucose or postprandial
blood glucose);
• number of overall, severe and non-severe hypoglycaemic
episodes;
• quality of life (ideally measured using a validated
instrument).
Secondary outcomes
• weight;
• insulin requirement to maintain glycaemic control;
• number and severity of adverse events (e.g. ketoacidosis,
local infections);
• diabetes late complications;
• mortality;
• costs.
Timing of outcome assessment
Short (less than or equal to one month), medium (more than one
month and less than six months) and longer term (equal to or
more than six months) outcome data were included in the review.
Search methods for identification of studies
Electronic searches
We searched the following sources for the identification of studies
up to 20 July 2009:
• The Cochrane Library;• MEDLINE;
• EMBASE;
• CINAHL.
For detailed search strategies please see under Appendix 1.
We also planned to search databases of ongoing studies: Cur-
rent Controlled Trials (www.controlled-trials.com - with links to
other databases of ongoing trials) and the National Research Reg-
ister (www.update-software.com/National/nrr-frame.html). This
will be performed in future updates of this review.
Searching other resources
We handsearched abstracts from international diabetes meetings
from 2002, 2003 and 2004 (including IDF, EASD, ADA).
Data collection and analysis
Selection of studies
To determine the studies to be assessed further, two independent
authors (MM, KE) scanned the titles, abstract sections and key-
words of every record retrieved, where available. Full articles were
retrieved for further assessment if the information provided was in-
sufficient to decide eligibility or if information provided suggested
that the study: 1. included people with type 1 diabetes mellitus; 2.
compared CSII and MI (three or more insulin injections per day);
3. assessed one or more relevant clinical outcome measure(s); 4.
was randomised. There were no disagreements about selection of
studies between authors.
Dealing with duplicate publications
In the case of duplicate publications and companion papers of
primary studies, we tried to maximise yield of information by
simultaneous evaluation of all available data. In cases of doubt,
the original publication (usually but not always the oldest version)
obtained priority.
4Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Data extraction and management
For studies that met the selection criteria, two out of three possible
authors (MM, KE and MP) independently extracted relevant pop-
ulation and intervention characteristics using a standard data ex-
traction template (for details see Characteristics of included studies
and Table 1, Appendix 2, Appendix 8). The authors reached agree-
ment about the data extracted through discussion.
Assessment of risk of bias in included studies
Two authors assessed risk of bias of each study independently (for
details see Characteristics of included studies). The authors ex-
plored the influence of individual risk of bias criteria in a sensitiv-
ity analysis (see ’Sensitivity analysis’). The authors reached agree-
ment about risk of bias assessments through discussion. Potential
for bias was considered using the risk of bias table which addresses
the following domains:
• sequence generation;
• allocation concealment;
• blinding of participants, personnel and outcome assessors;
• incomplete outcome data;
• selective outcome reporting;
• other sources of bias.
Each question was answered ’Yes’, ’No’ or ’Unclear’, where ’Yes’
suggests a low risk of bias, ’No’ suggests a high risk of bias and
’Unclear’ suggests doubt about the level of bias in that domain.
Summary assessments for risk of bias were made for each outcome
across studies (see ’Effects of interventions’) using the approach
suggested in the Cochrane Handbook for Systematic Reviews of In-tervention (Higgins 2008).
Measures of treatment effect
Review Manager 5.0 software was used for data analysis. Results
are expressed as mean differences, calculated from end of treat-
ment values, with 95% confidence intervals (CI) for continuous
outcomes. There are no dichotomous outcomes in this review.
Pooled results were meta-analysed using the generic inverse vari-
ance method with a random-effects model. Statistical significance
was set at a P value less than 0.05 for primary and secondary out-
come measures.
Dealing with missing data
Relevant missing information about study design or results were
sought from the study investigators, where feasible. Evaluation
of important numerical data such as screened, eligible and ran-
domised participants as well as intention-to-treat and per-proto-
col population is presented in Table 1. Attrition rates like drop-
outs, losses to follow-up and withdrawn study participants were
investigated. Issues of last-observation-carried-forward were criti-
cally appraised and compared to specification of primary outcome
parameters and power calculation.
Six cross-over studies were not adequately analysed, and did not
report correlations between baseline and end of study data, thereby
ignoring within-person variation. We reanalysed the data from
these studies assuming different correlation coefficients (0.3, 0.5,
0.7, 0.9) and have discussed the results based on the most con-
servative approach, assuming a correlation coefficient of 0.3. The
data from these studies were also reanalysed assuming the largest
standard deviation of the differences, derived from the cross-over
studies that were adequately analysed. The results from these anal-
yses can be found in Appendix 3.
Assessment of heterogeneity
Results of clinically and statistically homogenous studies were
pooled to provide estimates of the efficacy of the interventions.
Clinical homogeneity was satisfied when participants, interven-
tions, outcome measures and timing of outcome measurement
were considered to be similar. For studies that were clinically het-
erogeneous or presented insufficient information for pooling, a
descriptive analysis was performed. Statistical homogeneity was
assessed using the I2 statistic where I2 values under 50% indicated
acceptable homogeneity (low heterogeneity) (Higgins 2003).
Assessment of reporting biases
Funnel plots were planned to be used in exploratory data analyses
to assess for the potential existence of small study bias. There are
a number of explanations for the asymmetry of a funnel plot,
including true heterogeneity of effect with respect to study size,
poor methodological design of small studies and publication bias
(Sterne 2001). Thus, the findings using this exploratory data tool
were interpreted with caution.
Data synthesis
Data were summarised statistically where available, sufficiently
similar, and of sufficient quality. Generic inverse variance meta-
analyses were performed using a random-effects model for the
included continuous outcomes. Effect estimates are expressed as
mean difference and 95% confidence interval (CI). Where data
could not be combined, narrative tables of results are presented.
Subgroup analysis and investigation of heterogeneity
Subgroup analyses were conducted according to age of study par-
ticipants and study duration, since these factors may cause varia-
tions in outcomes.
We also conducted post-hoc analyses where we explored studies
that included less than 20 participants in subgroup analyses for
each outcome (Appendix 4).
5Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Sensitivity analysis
Sensitivity analyses were performed for every element on the risk
of bias table by excluding studies that had a high risk of bias. Other
elements that were employed in sensitivity analyses included:
• excluding very long or large studies to establish how much
they dominate the results;
• excluding studies using the following filters: diagnostic
criteria, date of publication, language of publication, source of
funding (industry versus other), country.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
Results of the search
The search conducted up until 20 July 2009 for all databases, iden-
tified 4343 records, from these, 201 full text papers were retrieved
for further examination. After screening the full text of the selected
papers, 23 studies finally met the inclusion criteria. An adapted
PRISMA (Preferred Reporting Items for Systematic Reviews and
Meta-Analyses) flow-chart of study selection is attached (Liberati
2009), see Figure 1.
Figure 1. Adapted PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow-
chart of study selection
6Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Assessment of inter-rater agreement
Two authors reviewed the studies, and were in agreement on those
to be fully assessed. From these, studies eligible for inclusion in
the review were identified. Both authors agreed on the final papers
chosen for assessment and on the risk of bias assessment of the
studies. There was complete agreement (100%) on the final papers
chosen for further assessment.
Included studies
Designs of included studies
Twenty-three randomised controlled trials (RCTs) meeting the
inclusion criteria of this review were identified. Details of these
studies are shown in the ’Characteristics of included studies’ ta-
ble. Eleven of the 23 included studies were of parallel design,
the other 12 had a cross-over design (Bak 1987 and Husted
1989; Bruttomesso 2008; Chiasson 1984 and 1985; Cohen 2003;
Hanaire-Broutin 2000; Hirsch 2005; Home 1982; Hoogma 2005;
Nathan 1982; Saurbrey 1988; Schmitz 1989; Weintrob 2004). Six
of the cross-over studies were analysed using adequate statistical
methodology to account for within-person variation. Six cross-
over studies were not adequately analysed, and ignored within-
person variation, so we reanalysed the data from these studies as
described above in ’Dealing with missing data’. The results from
these analyses can be found in Appendix 3.
Seventy-eight percent (18) of the studies had an initial run-in
phase lasting from two days to six months in order to achieve
stable metabolic conditions. Of the 12 studies with a cross-over
design, six reported a wash-out period before switching to the
other treatment.
The single centre design was the dominating setting (70%) but
multiple centre studies were also common (30%). Studies were
published from 1982 to 2008. Sixty-one per cent (14 studies)
could be clearly identified as partly or entirely industry sponsored
and in two studies, funding was not specified. Diagnostic criteria
for entry into the study was specified in eight of the studies.
Participants of included studies
In total, 976 people with type 1 diabetes took part in the 23
randomised controlled studies.
Seven of the 23 studies were performed in participants under 18
years of age (Cohen 2003; Doyle 2004; Meschi 1982; Nuboer
2008; Pozzilli 2003; Skogsberg 2008; Weintrob 2004).
All but one study investigated the effects in both genders. Botta
1986 only included pregnant females (n=10). It is important to
note that other studies included in this review have excluded preg-
nant females, suggesting clinical heterogeneity among the studies
in this review.
Interventions of included studies
All included studies compared continuous subcutaneous insulin
infusion (CSII) and multiple insulin injections (MI) (three or
more insulin injections per day). The duration of the intervention
ranged from six days to four years. It is important to note that
the study with an intervention period of six days (Meschi 1982)
should not be considered a real life setting and so was explored
in sensitivity analysis but the effect estimate was largely unaltered.
Most studies tried to achieve a comparable insulin dose regimen
throughout the investigation period, and treating physicians, to-
gether with the participants, tried to achieve optimisation of ther-
apy, usually by means of flexible insulin dosage in order to achieve
metabolic targets of heterogeneously defined adequate blood glu-
cose control.
Excluded studies
In total, 178 studies were excluded after careful evaluation of the
full publication. Reasons for exclusion of studies are given in the
’Characteristics of excluded studies’ table. The main reasons for
exclusion were inappropriate interventions, less than three injec-
tions per day in the MI group and non-randomised study design.
Risk of bias in included studies
For details of risk of bias in the included studies, see the
’Characteristics of included studies’ tables, Figure 2 and Figure 3.
For each outcome in ’Effects of interventions’, a summary assess-
ment for the risk of bias is provided.
7Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 2. Risk of bias summary: review authors’ judgements about risk of bias items for each included study.
8Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
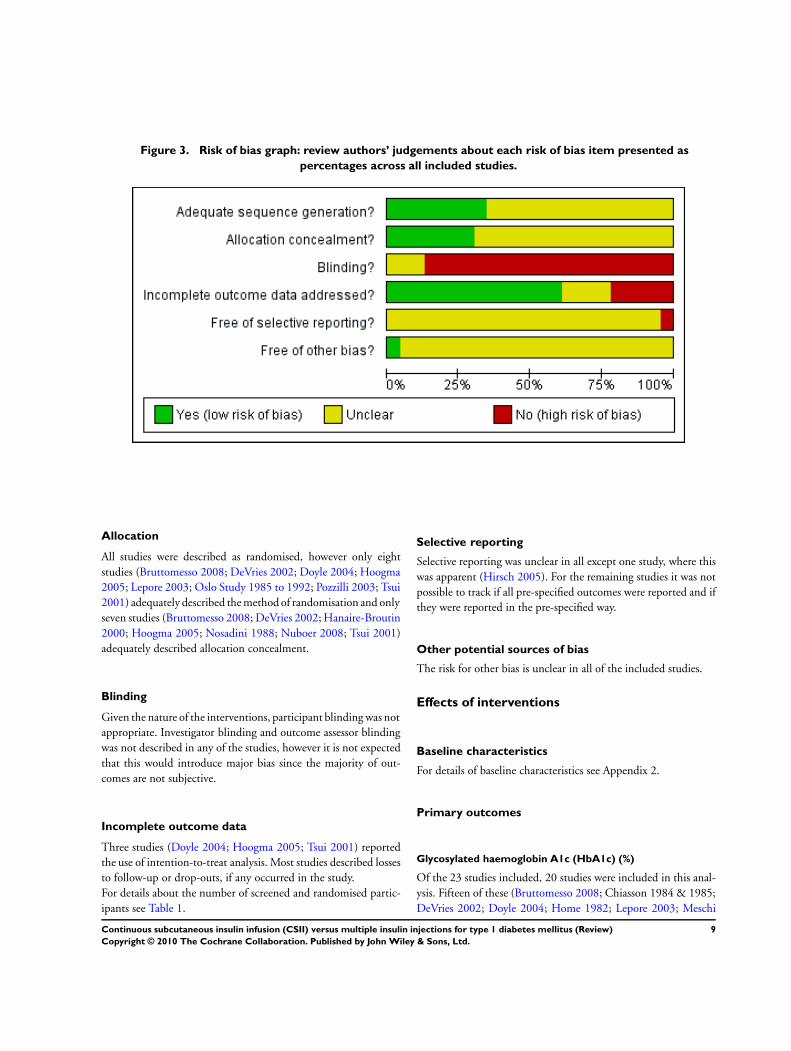
Figure 3. Risk of bias graph: review authors’ judgements about each risk of bias item presented as
percentages across all included studies.
Allocation
All studies were described as randomised, however only eight
studies (Bruttomesso 2008; DeVries 2002; Doyle 2004; Hoogma
2005; Lepore 2003; Oslo Study 1985 to 1992; Pozzilli 2003; Tsui
2001) adequately described the method of randomisation and only
seven studies (Bruttomesso 2008; DeVries 2002; Hanaire-Broutin
2000; Hoogma 2005; Nosadini 1988; Nuboer 2008; Tsui 2001)
adequately described allocation concealment.
Blinding
Given the nature of the interventions, participant blinding was not
appropriate. Investigator blinding and outcome assessor blinding
was not described in any of the studies, however it is not expected
that this would introduce major bias since the majority of out-
comes are not subjective.
Incomplete outcome data
Three studies (Doyle 2004; Hoogma 2005; Tsui 2001) reported
the use of intention-to-treat analysis. Most studies described losses
to follow-up or drop-outs, if any occurred in the study.
For details about the number of screened and randomised partic-
ipants see Table 1.
Selective reporting
Selective reporting was unclear in all except one study, where this
was apparent (Hirsch 2005). For the remaining studies it was not
possible to track if all pre-specified outcomes were reported and if
they were reported in the pre-specified way.
Other potential sources of bias
The risk for other bias is unclear in all of the included studies.
Effects of interventions
Baseline characteristics
For details of baseline characteristics see Appendix 2.
Primary outcomes
Glycosylated haemoglobin A1c (HbA1c) (%)
Of the 23 studies included, 20 studies were included in this anal-
ysis. Fifteen of these (Bruttomesso 2008; Chiasson 1984 & 1985;
DeVries 2002; Doyle 2004; Home 1982; Lepore 2003; Meschi
9Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

1982; Nathan 1982; Nosadini 1988; Nuboer 2008; Oslo Study
1985 to 1992; Pozzilli 2003; Schmitz 1989; Skogsberg 2008;
Tsui 2001) were parallel or cross-over studies using appropriate
statistical methodology; and five (Cohen 2003; Hanaire-Broutin
2000; Hoogma 2005; Saurbrey 1988; Weintrob 2004) were cross-
over studies with inadequate statistical methodology (i.e. ignor-
ing within-person variation). Therefore, we reanalysed the data
from these studies assuming different correlation coefficients (0.3,
0.5, 0.7, 0.9). The data from these studies were also reanalysed
assuming the largest standard deviation of the differences derived
from the cross-over studies with adequate statistical methodology.
Three studies were excluded because they did not report HbA1c.
Assuming a conservative correlation of 0.3, and using generic in-
verse variance with a random-effects model, the mean difference
of HbA1c was estimated to be -0.3% (95% CI -0.4 to -0.1) in
favour of CSII compared with MI. The test of heterogeneity gave
an I2 statistic of 50% and the test for overall effect gave a P value
of 0.001 (Figure 4). The effect estimates, overall treatment effects
and heterogeneity assuming other correlations and the largest stan-
dard deviation of the differences are presented in Appendix 3.
Figure 4. Forest plot of comparison: CSII versus MI, outcome: HbA1c (%).
Risk of bias summary assessment
Most information is from studies at low or unclear risk of bias.
Detailed risk of bias assessments can be found in ’Characteristics
of included studies’ tables and Figure 2 and Figure 3.
Subgroup analyses
Subgroup analyses for all outcomes were performed assuming a
conservative correlation of 0.3, using generic inverse variance with
a random-effects model. The effect estimates, overall treatment ef-
10Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

fects and heterogeneity assuming other correlations and the largest
standard deviation of the differences are presented in Appendix 3.
HbA1c - age of study participants
In studies that included participants less than 18 years of age (
Cohen 2003; Doyle 2004; Meschi 1982; Nuboer 2008; Pozzilli
2003; Skogsberg 2008; Weintrob 2004) the mean difference of
HbA1c was estimated to be -0.2% (95% CI -0.4 to -0.03) in favour
of CSII compared with MI. The test of heterogeneity gave an I2
statistic of 20%. The test for overall effect gave a P value of 0.02
(Analysis 1.2). In studies that included participants more than 18
years of age (Bruttomesso 2008; DeVries 2002; Hanaire-Broutin
2000; Home 1982; Hoogma 2005; Lepore 2003; Nathan 1982;
Nosadini 1988; Oslo Study 1985 to 1992; Saurbrey 1988; Schmitz
1989; Tsui 2001) the mean difference of HbA1c was estimated to
be -0.3% (95% CI -0.5 to -0.1) in favour of CSII compared with
MI. The test of heterogeneity gave an I2 statistic of 62%. The test
for overall effect gave a P value of 0.01 (Analysis 1.2).
HbA1c subgroup analysis - study duration
There was only one short term study (up to one month), which is
insufficient for subgroup analysis (Meschi 1982).
In medium term studies (from one to six months) (Bruttomesso
2008; Chiasson 1984 & 1985; Cohen 2003; DeVries 2002;
Doyle 2004; Hanaire-Broutin 2000; Home 1982; Hoogma 2005;
Nathan 1982; Saurbrey 1988; Schmitz 1989; Weintrob 2004),
the mean difference of HbA1c was estimated to be -0.3% (95%
CI -0.5 to -0.1) in favour of CSII compared with MI. The test
of heterogeneity gave an I2 statistic of 53%. The test for overall
effect gave a P value of 0.002 (Analysis 1.3).
In long term studies (more than six months) (Lepore 2003;
Nosadini 1988; Nuboer 2008; Oslo Study 1985 to 1992; Pozzilli
2003; Skogsberg 2008; Tsui 2001), the mean difference of HbA1c
was estimated to be -0.2% (95% CI -0.4 to 0.1) in favour of CSII
compared with MI. The test of heterogeneity gave an I2 statistic
of 57%. The test for overall effect gave a P value of 0.21 (Analysis
1.3).
Small study bias
Assuming a conservative correlation of 0.3, using generic inverse
variance with a random-effects model for studies that included
less than 20 participants (Chiasson 1984 and 1985; Cohen 2003;
Home 1982; Meschi 1982; Nathan 1982; Schmitz 1989) the mean
difference of HbA1c was estimated to be -0.7% (95% CI -1.6 to
0.1) in favour of CSII compared with MI. The test of heterogeneity
gave an I2 statistic of 63%. The test for overall effect gave a P
value of 0.09 (Analysis 1.4). The effect estimates, overall treatment
effects and heterogeneity are presented in Appendix 3.
Daily mean blood glucose (mg/dl)
Of 23 studies included, 13 were included in this analysis. Nine of
these (Bak 1987 and Husted 1989; Bruttomesso 2008; DeVries
2002; Home 1982; Meschi 1982; Nathan 1982; Nosadini 1988;
Oslo Study 1985 to 1992; Schmitz 1989) were parallel or
cross-over studies using appropriate statistical methodology; and
four (Hanaire-Broutin 2000; Hoogma 2005; Saurbrey 1988;
Weintrob 2004) were cross-over studies where appropriate statis-
tical methodology was not used (i.e. ignoring within-person varia-
tion). Therefore, we reanalysed the data as described in the results
section for HbA1c. Ten studies were excluded because they did
not report daily mean blood glucose.
Assuming a conservative correlation of 0.3, and using generic in-
verse variance with a random-effects model, a pooled mean dif-
ference of daily mean blood glucose could not be reliably esti-
mated due to substantial heterogeneity with an I2 statistic of 94%.
The effect estimates, overall treatment effects and heterogeneity
assuming other correlations and the largest standard deviation of
the differences are presented in Appendix 3.
Risk of bias summary assessment
Most information is from studies at low or unclear risk of bias.
Detailed risk of bias assessments can be found in ’Characteristics
of included studies’ tables and Figure 2 and Figure 3.
Subgroup analyses
Subgroup analyses were performed and presented as described in
the HbA1c subgroup analysis section.
Daily mean blood glucose - age of study participants
In studies that included participants less than 18 years of age
(Bak 1987 and Husted 1989; Meschi 1982; Weintrob 2004) the
mean difference of daily mean blood glucose was estimated to
be -4 mg/dl (95% CI -14 to 7) in favour of CSII compared
with MI. The test of heterogeneity gave an I2 statistic of 0%.
The test for overall effect gave a P value of 0.5 (Analysis 1.6).
In studies that included participants more than 18 years of age
(Bruttomesso 2008; DeVries 2002; Hanaire-Broutin 2000; Home
1982; Hoogma 2005; Nathan 1982; Nosadini 1988; Oslo Study
1985 to 1992; Saurbrey 1988; Schmitz 1989) the mean difference
of daily mean blood glucose was estimated to be -18 mg/dl (95%
CI -27 to -9) in favour of CSII compared with MI. The test of
heterogeneity gave an I2 statistic of 96%. Therefore, the pooled
effect estimate is not reliable (Analysis 1.6).
Daily mean blood glucose - study duration
11Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

There was only one short term study (up to one month), which is
insufficient for subgroup analysis (Meschi 1982).
In medium term studies (from one to six months) (Bak 1987 and
Husted 1989; Bruttomesso 2008; DeVries 2002; Hanaire-Broutin
2000; Home 1982; Hoogma 2005; Nathan 1982; Saurbrey 1988;
Schmitz 1989; Weintrob 2004), the mean difference of daily mean
blood glucose was estimated to be -14 mg/dl (95% CI -23 to -5)
in favour of CSII compared with MI. The test of heterogeneity
gave an I2 statistic of 95%. Therefore, the pooled effect estimate
is not reliable (Analysis 1.7).
In long term studies (more than six months) (Nosadini 1988; Oslo
Study 1985 to 1992), the mean difference of daily mean blood
glucose was estimated to be -21 mg/dl (95% CI -29 to -13) in
favour of CSII compared with MI. The test of heterogeneity gave
an I2 statistic of 0%. The test for overall effect gave a P value less
than 0.00001 (Analysis 1.7).
Small study bias
Assuming a conservative correlation of 0.3, using generic inverse
variance with a random effects model for studies that included less
than 20 participants (Home 1982; Meschi 1982; Nathan 1982;
Schmitz 1989) the mean difference of daily mean blood glucose
was estimated to be -29 mg/dl (95% CI -51 to -7) in favour of
CSII compared with MI. The test of heterogeneity gave an I2
statistic of 58%. The test for overall effect gave a P value of 0.009
(Analysis 1.8). The effect estimates, overall treatment effects and
heterogeneity are presented in Appendix 3.
Fasting blood glucose (mg/dl)
Of 23 studies included, 11 were included in this analysis. Eight of
these (Botta 1986; Bruttomesso 2008; Chiasson 1984 and 1985;
DeVries 2002; Doyle 2004; Home 1982; Lepore 2003; Oslo Study
1985 to 1992) were parallel or cross-over studies using appropriate
statistical methodology; and three (Hirsch 2005; Hoogma 2005;
Weintrob 2004) were cross-over studies where appropriate statis-
tical methodology was not used (i.e. ignoring within-person varia-
tion). Therefore, we reanalysed the data as described in the results
section for HbA1c. Twelve studies were excluded because they did
not report fasting blood glucose.
Assuming a conservative correlation of 0.3, and using generic in-
verse variance with a random-effects model, the mean difference
of fasting blood glucose was estimated to be -14 mg/dl (95% CI
-24 to -4) in favour of CSII compared with MI. The test of het-
erogeneity gave an I2 statistic of 71%. Therefore, the pooled ef-
fect estimate is not reliable (Figure 6). The effect estimates, overall
treatment effects and heterogeneity assuming other correlations
and the largest standard deviation of the differences are presented
in Appendix 3.
Risk of bias summary assessment
The proportion of information from studies at high risk of bias
is sufficient to affect the interpretation of results. Detailed risk
of bias assessments can be found in ’Characteristics of included
studies’ tables and Figure 2 and Figure 3.
Subgroup analyses
Subgroup analyses were performed and presented as described in
the HbA1c subgroup analysis section.
Fasting blood glucose - age of study participants
In studies that included participants less than 18 years of age (
Chiasson 1984 and 1985; Doyle 2004; Weintrob 2004) the mean
difference of fasting blood glucose was estimated to be -8 mg/dl
(95% CI -24 to 9) in favour of CSII compared with MI. The test of
heterogeneity gave an I2 statistic of 0%. The test for overall effect
gave a P value of 0.35 (Analysis 1.10). In studies that included
participants more than 18 years of age (Botta 1986; Bruttomesso
2008; DeVries 2002; Hirsch 2005; Home 1982; Hoogma 2005;
Lepore 2003; Oslo Study 1985 to 1992) the mean difference of
fasting blood glucose was estimated to be -16 mg/dl (95% CI -29 to
-3) in favour of CSII compared with MI. The test of heterogeneity
gave an I2 statistic of 79%. Therefore, the pooled effect estimate
is not reliable (Analysis 1.10).
Fasting blood glucose - study duration
There was only one short term study (up to one month), which is
insufficient for subgroup analysis (Hirsch 2005).
In medium term studies (from one to six months) (Botta 1986;
Bruttomesso 2008; Chiasson 1984 and 1985; DeVries 2002;
Doyle 2004; Home 1982; Hoogma 2005; Weintrob 2004), the
mean difference of fasting blood glucose was estimated to be -8
mg/dl (95% CI -19 to 2) in favour of CSII compared with MI.
The test of heterogeneity gave an I2 statistic of 63%. Therefore,
the pooled effect estimate is not reliable (Analysis 1.11).
In long term studies (more than six months) (Lepore 2003; Oslo
Study 1985 to 1992), the mean difference of fasting blood glucose
was estimated to be -37 mg/dl (95% CI -73 to -1) in favour of CSII
compared with MI. The test of heterogeneity gave an I2 statistic of
61%. Therefore, the pooled effect estimate is not reliable (Analysis
1.11).
Small study bias
Assuming a conservative correlation of 0.3, using generic inverse
variance with a random-effects model for studies that included less
than 20 participants (Botta 1986; Chiasson 1984 & 1985; Home
1982) the mean difference of fasting blood glucose was estimated
12Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

to be -14 mg/dl (95% CI -50 to 23) in favour of CSII compared
with MI. The test of heterogeneity gave an I2 statistic of 79%.
Therefore, the pooled effect estimate is not reliable (Analysis 1.12).
The effect estimates, overall treatment effects and heterogeneity
are presented in Appendix 3.
Post prandial blood glucose (mg/dl)
Of 23 studies included, five were included in this analysis. Three of
these (Botta 1986; Chiasson 1984 and 1985; DeVries 2002) were
parallel or cross-over studies using appropriate statistical method-
ology; and two (Hirsch 2005; Weintrob 2004) were cross-over
studies where appropriate statistical methodology was not used
(ie. ignoring within-person variation). Therefore, we reanalysed
the data as described in the results section for HbA1c. Eighteen
studies were excluded because they did not report post prandial
blood glucose.
Assuming a conservative correlation of 0.3, and using generic in-
verse variance with a random-effects model, the mean difference
of post prandial blood glucose was estimated to be -4 mg/dl (95%
CI -11 to 2) in favour of CSII compared with MI. The test of
heterogeneity gave an I2 statistic of 37%. The test for overall ef-
fect gave a P value of 0.18 (Figure 5). The effect estimates, overall
treatment effects and heterogeneity assuming other correlations
and the largest standard deviation of the differences are presented
in Appendix 3.
Figure 5. Forest plot of comparison: CSII versus MI, outcome: Post prandial blood glucose (mg/dl).
Risk of bias summary assessment
The proportion of information from studies at high risk of bias
is sufficient to affect the interpretation of results. Detailed risk
of bias assessments can be found in ’Characteristics of included
studies’ tables and Figure 2 and Figure 3.
Subgroup analyses
Subgroup analyses were performed and presented as described in
the HbA1c subgroup analysis section.
Post prandial blood glucose - age of study participants
In studies that included participants less than 18 years of age (
Chiasson 1984 and 1985; Weintrob 2004) the mean difference of
post prandial blood glucose was estimated to be -3 mg/dl (95%
CI -12 to 6) in favour of CSII compared with MI. The test of
heterogeneity gave an I2 statistic of 0%. The test for overall effect
gave a P value of 0.49 (Analysis 1.14). In studies that included
participants more than 18 years of age (Botta 1986, DeVries 2002,
Hirsch 2005) the mean difference of post prandial blood glucose
was estimated to be -8 mg/dl (95% CI -23 to 8) in favour of CSII
compared with MI. The test of heterogeneity gave an I2 statistic of
68%. Therefore, the pooled effect estimate is not reliable (Analysis
1.14).
Post prandial blood glucose - study duration
There was only one short term study (up to one month), which is
insufficient for subgroup analysis (Hirsch 2005).
In medium term studies (from one to six months) (Botta 1986;
Chiasson 1984 and 1985; DeVries 2002; Weintrob 2004), the
mean difference of post prandial blood glucose was estimated to
be -2 mg/dl (95% CI -4 to 0.3) in favour of CSII compared with
MI. The test of heterogeneity gave an I2 statistic of 0%. The test
for overall effect gave a P value of 0.08 (Analysis 1.15).
There were no long term studies (more than six months) for sub-
group analysis (Analysis 1.15).
13Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Small study bias
Assuming a conservative correlation of 0.3, using generic inverse
variance with a random-effects model for studies that included less
than 20 participants (Botta 1986; Chiasson 1984 & 1985) the
mean difference of post prandial blood glucose was estimated to
be 1 mg/dl (95% CI -15 to 16) in favour of CSII compared with
MI. The test of heterogeneity gave an I2 statistic of 0%. The test
for overall effect gave a P value of 0.93 (Analysis 1.16). The effect
estimates, overall treatment effects and heterogeneity are presented
in Appendix 3.
Hypoglycaemic events
Non-severe hypoglycaemic events
Non-severe hypoglycaemia was often defined as a blood glucose
level lower than 70 mg/dl. Some studies did not provide a defini-
tion. The 17 studies (Bak 1987 and Husted 1989; Bruttomesso
2008; Chiasson 1984 and 1985; Cohen 2003; DeVries 2002;
Hanaire-Broutin 2000; Hirsch 2005; Home 1982; Hoogma 2005;
Meschi 1982; Nathan 1982; Nosadini 1988; Oslo Study 1985 to
1992; Pozzilli 2003; Schmitz 1989; Saurbrey 1988; Tsui 2001;
Weintrob 2004) that reported non-severe hypoglycaemia used dif-
ferent scales and it was not appropriate to conduct a meta-analysis,
however the data indicate that there is no relevant benefit of one
intervention over the other for reducing non-severe hypoglycaemic
events. A descriptive table of results can be found in Appendix 5.
Risk of bias summary assessment
Most information is from studies at low or unclear risk of bias.
Detailed risk of bias assessments can be found in ’Characteristics
of included studies’ tables and Figure 2 and Figure 3.
Severe hypoglycaemic events
Severe hypoglycaemia was often defined as requiring assistance
from another person for recovery or resulting in coma or seizure.
Some studies did not provide a definition. The 15 studies
(Bruttomesso 2008; Cohen 2003; DeVries 2002; Doyle 2004;
Hanaire-Broutin 2000; Hirsch 2005; Hoogma 2005; Lepore
2003; Nosadini 1988; Nuboer 2008; Oslo Study 1985 to 1992;
Schmitz 1989; Skogsberg 2008; Tsui 2001; Weintrob 2004) that
reported severe hypoglycaemia used different scales and it was not
appropriate to conduct a meta-analysis, however the data indicate
that CSII may be better than MI for reducing the incidence of
severe hypoglycaemic events. A descriptive table of results can be
found in Appendix 6.
Risk of bias summary assessment
Most information is from studies at low or unclear risk of bias.
Detailed risk of bias assessments can be found in ’Characteristics
of included studies’ tables and Figure 2 and Figure 3.
Quality of life
Quality of life was measured using different instruments by 15
studies (Bak 1987 and Husted 1989; Bruttomesso 2008; Chiasson
1984 and 1985; Cohen 2003; DeVries 2002; Doyle 2004;
Hanaire-Broutin 2000; Home 1982; Hoogma 2005; Nathan
1982; Nuboer 2008; Saurbrey 1988; Schmitz 1989; Skogsberg
2008; Tsui 2001), none of which have reported minimal clinically
important differences. Four studies (Bruttomesso 2008; Cohen
2003; DeVries 2002; Skogsberg 2008) used the validated dia-
betes treatment satisfaction questionnaire (DTSQ) of which two
of these included participants less than 18 years of age. In all four
studies the CSII groups had higher scores, representing better treat-
ment satisfaction, than the MI group. Of the two studies (Cohen
2003; Doyle 2004) that used the validated diabetes quality of life
for youth scale (DQOLY), one study in adults (Cohen 2003) re-
ported a higher score, representing better quality of life, in the CSII
group than the MI group. The other study (Doyle 2004), includ-
ing participants less than 18 years of age, did not report scores but
noted that a difference between the groups was not found. Two
studies (Hoogma 2005; Tsui 2001) used the validated diabetes
quality of life scale (DQoL) and found that the MI group scored
lower, representing better quality of life, than the CSII group. Use
of the SF-12 questionnaire (Hoogma 2005), SF36 general health
perceptions scale (DeVries 2002) and the paediatric quality of life
inventory (PedsQL) (Nuboer 2008) (all validated) revealed that
CSII was favoured over MI for perception of better mental health,
perception of better general health and better quality of life, re-
spectively. It is difficult to determine which treatment is better
when independent questionnaires (Bak 1987 and Husted 1989;
Chiasson 1984 and 1985; Hanaire-Broutin 2000; Home 1982;
Hoogma 2005; Nathan 1982; Saurbrey 1988; Schmitz 1989) were
used to measure satisfaction, acceptability, preferred treatment and
reaction to treatment. It was not appropriate to conduct a meta-
analysis, however the data suggest that the majority of participants
were more satisfied with CSII than MI. A descriptive table of re-
sults can be found in Appendix 7.
Risk of bias summary assessment
Most information is from studies at low or unclear risk of bias.
Detailed risk of bias assessments can be found in ’Characteristics
of included studies’ tables and Figure 2 and Figure 3.
Secondary outcomes
14Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Weight (kg)
Of 23 studies included, eight were included in this analysis. Six of
these (Bak 1987 and Husted 1989; DeVries 2002; Home 1982;
Lepore 2003; Oslo Study 1985 to 1992; Schmitz 1989) were par-
allel or cross-over studies using appropriate statistical methodol-
ogy; and two (Hanaire-Broutin 2000; Hoogma 2005) were cross-
over studies where appropriate statistical methodology was not
used (i.e. ignoring within-person variation). Therefore, we reanal-
ysed the data as described in the results section for HbA1c. Fifteen
studies were excluded because they did not report weight.
Assuming a conservative correlation of 0.3, and using generic in-
verse variance with a random-effects model, the mean difference
of weight was estimated to be -0.4 kg (95% CI -2 to 1.3). The
test of heterogeneity gave an I2 statistic of 0%. The test for overall
effect gave a P value of 0.65 (Figure 6). The effect estimates, overall
treatment effects and heterogeneity assuming other correlations
and the largest standard deviation of the differences are presented
in Appendix 3.
Figure 6. Forest plot of comparison: CSII versus MI, outcome: Weight (kg).
Risk of bias summary assessment
Most information is from studies at low or unclear risk of bias.
Detailed risk of bias assessments can be found in ’Characteristics
of included studies’ tables and Figure 2 and Figure 3.
Subgroup analyses
Subgroup analyses were performed and presented as described in
the HbA1c subgroup analysis section.
Weight - age of study participants
There were no studies that included participants less than 18 years
of age, therefore it was not possible to conduct subgroup analyses.
Weight - study duration
There were no short term studies (up to one month) for subgroup
analysis (Analysis 1.21).
In medium term studies (from one to six months) (Bak 1987 and
Husted 1989; DeVries 2002; Hanaire-Broutin 2000; Home 1982;
Hoogma 2005; Schmitz 1989), the mean difference of weight was
estimated to be -0.2 kg (95% CI -2 to 1.5) in favour of CSII
compared with MI. The test of heterogeneity gave an I2 statistic
of 0%. The test for overall effect gave a P value of 0.78 (Analysis
1.21).
In long term studies (more than six months) (Lepore 2003; Oslo
Study 1985 to 1992), the mean difference of weight was estimated
to be -1.6 kg (95% CI -7.7 to 4.5) in favour of CSII compared
with MI. The test of heterogeneity gave an I2 statistic of 27%.
The test for overall effect gave a P value of 0.61 (Analysis 1.21).
Small study bias
Assuming a conservative correlation of 0.3, using generic inverse
variance with a random-effects model in studies that included less
than 20 participants (Botta 1986; Chiasson 1984 and 1985; Home
1982), the mean difference of weight was estimated to be -13.7
kg (95% CI -50.4 to 23) in favour of CSII compared with MI.
The test of heterogeneity gave an I2 value of 79%. Therefore, the
pooled effect estimate is not reliable (Analysis 1.22). The effect
estimates, overall treatment effects and heterogeneity are presented
in Appendix 3.
15Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Daily insulin requirement
Studies presented daily insulin requirement as either U or as U/
kg, therefore data were analysed separately according to the unit
used by the study investigators.
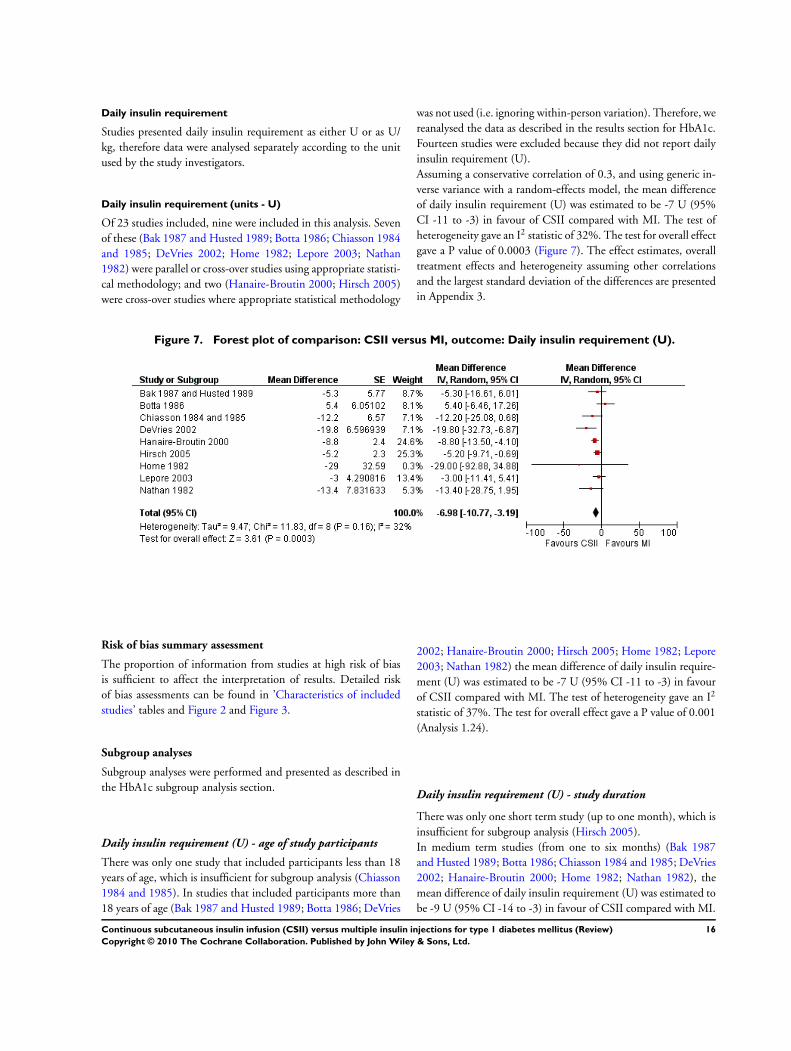
Daily insulin requirement (units - U)
Of 23 studies included, nine were included in this analysis. Seven
of these (Bak 1987 and Husted 1989; Botta 1986; Chiasson 1984
and 1985; DeVries 2002; Home 1982; Lepore 2003; Nathan
1982) were parallel or cross-over studies using appropriate statisti-
cal methodology; and two (Hanaire-Broutin 2000; Hirsch 2005)
were cross-over studies where appropriate statistical methodology
was not used (i.e. ignoring within-person variation). Therefore, we
reanalysed the data as described in the results section for HbA1c.
Fourteen studies were excluded because they did not report daily
insulin requirement (U).
Assuming a conservative correlation of 0.3, and using generic in-
verse variance with a random-effects model, the mean difference
of daily insulin requirement (U) was estimated to be -7 U (95%
CI -11 to -3) in favour of CSII compared with MI. The test of
heterogeneity gave an I2 statistic of 32%. The test for overall effect
gave a P value of 0.0003 (Figure 7). The effect estimates, overall
treatment effects and heterogeneity assuming other correlations
and the largest standard deviation of the differences are presented
in Appendix 3.
Figure 7. Forest plot of comparison: CSII versus MI, outcome: Daily insulin requirement (U).
Risk of bias summary assessment
The proportion of information from studies at high risk of bias
is sufficient to affect the interpretation of results. Detailed risk
of bias assessments can be found in ’Characteristics of included
studies’ tables and Figure 2 and Figure 3.
Subgroup analyses
Subgroup analyses were performed and presented as described in
the HbA1c subgroup analysis section.
Daily insulin requirement (U) - age of study participants
There was only one study that included participants less than 18
years of age, which is insufficient for subgroup analysis (Chiasson
1984 and 1985). In studies that included participants more than
18 years of age (Bak 1987 and Husted 1989; Botta 1986; DeVries
2002; Hanaire-Broutin 2000; Hirsch 2005; Home 1982; Lepore
2003; Nathan 1982) the mean difference of daily insulin require-
ment (U) was estimated to be -7 U (95% CI -11 to -3) in favour
of CSII compared with MI. The test of heterogeneity gave an I2
statistic of 37%. The test for overall effect gave a P value of 0.001
(Analysis 1.24).
Daily insulin requirement (U) - study duration
There was only one short term study (up to one month), which is
insufficient for subgroup analysis (Hirsch 2005).
In medium term studies (from one to six months) (Bak 1987
and Husted 1989; Botta 1986; Chiasson 1984 and 1985; DeVries
2002; Hanaire-Broutin 2000; Home 1982; Nathan 1982), the
mean difference of daily insulin requirement (U) was estimated to
be -9 U (95% CI -14 to -3) in favour of CSII compared with MI.
16Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

The test of heterogeneity gave an I2 statistic of 38%. The test for
overall effect gave a P value of 0.003 (Analysis 1.25).
There was only one long term study (more than six months), which
is insufficient for subgroup analysis (Lepore 2003).
Small study bias
Assuming a conservative correlation of 0.3, using generic inverse
variance with a random-effects model in studies that included less
than 20 participants (Bak 1987 and Husted 1989; Botta 1986;
Chiasson 1984 and 1985; Home 1982; Nathan 1982) the mean
difference of daily insulin requirement (U) was estimated to be
-6 U (95% CI -14 to 2) in favour of CSII compared with MI.
The test of heterogeneity gave an I2 statistic of 31%. The test for
overall effect gave a P value of 0.14 (Analysis 1.26). The effect
estimates, overall treatment effects and heterogeneity are presented
in Appendix 3.
Daily insulin requirement (units per kg - U/kg)
Of 23 studies included, 12 were included in this analysis. Ten of
these (Bruttomesso 2008; Cohen 2003; Doyle 2004; Meschi 1982;
Nuboer 2008; Oslo Study 1985 to 1992; Pozzilli 2003; Schmitz
1989; Skogsberg 2008; Tsui 2001) were parallel or cross-over stud-
ies using appropriate statistical methodology; and two (Hoogma
2005; Saurbrey 1988) were cross-over studies where appropriate
statistical methodology was not used (i.e. ignoring within-person
variation). Therefore, we reanalysed the data as described in the
results section for HbA1c. Ten studies were excluded because they
did not report daily insulin requirement (U/kg).
Assuming a conservative correlation of 0.3, and using generic in-
verse variance with a random-effects model, a pooled mean dif-
ference of daily mean blood glucose could not be reliably esti-
mated due to substantial heterogeneity with an I2 statistic of 94%.
The effect estimates, overall treatment effects and heterogeneity
assuming other correlations and the largest standard deviation of
the differences are presented in Appendix 3.
Risk of bias summary assessment
Most information is from studies at low or unclear risk of bias.
Detailed risk of bias assessments can be found in ’Characteristics
of included studies’ tables and Figure 2 and Figure 3.
Subgroup analyses
Subgroup analyses were performed and presented as described in
the HbA1c subgroup analysis section.
Daily insulin requirement (U/kg) - age of study participants
In studies that included participants less than 18 years of age
(Cohen 2003; Doyle 2004; Meschi 1982; Nuboer 2008; Pozzilli
2003; Skogsberg 2008) the mean difference of daily insulin re-
quirement (U/kg) was estimated to be -0.16 U/kg (95% CI -0.31
to -0.01) in favour of CSII compared with MI. The test of hetero-
geneity gave an I2 statistic of 84%. Therefore, the pooled effect es-
timate is not reliable (Analysis 1.28). In studies that included par-
ticipants more than 18 years of age (Bruttomesso 2008; Hoogma
2005; Oslo Study 1985 to 1992; Saurbrey 1988; Schmitz 1989;
Tsui 2001) the mean difference of daily insulin requirement (U/
kg) was estimated to be -0.08 U/kg (95% CI -0.15 to -0.01) in
favour of CSII compared with MI. The test of heterogeneity gave
an I2 value of 94%. Therefore, the pooled effect estimate is not
reliable (Analysis 1.28).
Daily insulin requirement (U/kg) - study duration
There was only one short term study (up to one month), which is
insufficient for subgroup analysis (Meschi 1982).
In medium term studies (from one to six months) (Bruttomesso
2008; Cohen 2003; Doyle 2004; Hoogma 2005; Saurbrey 1988;
Schmitz 1989), the mean difference of daily insulin requirement
(U/kg) was estimated to be -0.12 U/kg (95% CI -0.21 to -0.03)
in favour of CSII compared with MI. The test of heterogeneity
gave an I2 statistic of 94%. Therefore, the pooled effect estimate
is not reliable (Analysis 1.29).
In long term studies (more than six months) (Nuboer 2008; Oslo
Study 1985 to 1992; Pozzilli 2003; Skogsberg 2008; Tsui 2001),
the mean difference of daily insulin requirement (U/kg) was esti-
mated to be -0.14 U/kg (95% CI -0.32 to 0.04) in favour of CSII
compared with MI. The test of heterogeneity gave an I2 statistic of
95%. Therefore, the pooled effect estimate is not reliable (Analysis
1.29).
Small study bias
Assuming a conservative correlation of 0.3, using generic inverse
variance with a random-effects model in studies that included
less than 20 participants (Cohen 2003; Meschi 1982; Schmitz
1989) the mean difference of daily insulin requirement (U/kg)
was estimated to be -0.04 U/kg (95% CI -0.13 to 0.05) in favour
of CSII compared with MI. The test of heterogeneity gave an I2
statistic of 0%. The test for overall effect gave a P value of 0.41
(Analysis 1.30). The effect estimates, overall treatment effects and
heterogeneity are presented in Appendix 3.
Adverse events
Information about adverse events was not well reported. Twenty-
one studies reported that there were no deaths, one study did not
17Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

address this outcome and one study (Nosadini 1988) reported a
death in the CSII group, further details were not provided. Among
eight studies that did not describe the nature of adverse events,
there were more than 19 events in the CSII group and more than 10
in the MI group. Ketoacidosis was reported in two studies (Cohen
2003; DeVries 2002), where there was one event of ketoacidosis
in the CSII group of each study and one event of ketoacidosis
in the MI group of DeVries et al. Hoogma et al (Hoogma 2005)
reported 21 injection and infusion site injuries reactions in the
CSII group and Weintrob et al (Weintrob 2004) reported 12 mi-
nor infusion site infections, 16 blockages and 42 dislodgments.
All but one of the studies (Hoogma 2005) either did not report se-
rious adverse events or reported that there were no serious adverse
events. Hoogma et al reported 33 serious adverse events in the
CSII group and 58 in the MI group. Three studies reported drop-
outs as a results of adverse events. One of these (DeVries 2002)
reported one femur fracture but did not report which group the
participant was in. A second study (Doyle 2004) reported one case
of dehydration and ketosis in the MI group and the third study
(Home 1982) reported one undescribed event. In total, five CSII
participants and six MI participants were hospitalised (Bak 1987
and Husted 1989; Doyle 2004; Nuboer 2008; Saurbrey 1988)
and one CSII participant received out-patient treatment (Home
1982). For details of adverse events see Appendix 8.
Diabetes late complications
None of the studies reported on morbidity.
Mortality
None of the studies reported on mortality.
Costs
Costs were not addressed in any of the included studies.
Heterogeneity
In the HbA1c analysis comparing CSII and MI, heterogeneity was
reflected by an I2 statistic of 50%. After elimination of Nathan
1982, the study with high risk of bias, heterogeneity was signifi-
cantly reduced to 34% without altering the direction of effect.
Considerable heterogeneity was found and investigated for daily
mean blood glucose, fasting blood glucose and daily insulin re-
quired (measured in U/kg), but could not be explained by sub-
group analyses.
Statistical heterogeneity was either not present or low in the meta-
analyses of the outcomes post-prandial blood glucose, daily insulin
requirement (measured in units) and weight.
Subgroup analyses
Subgroup analyses are described in detail for each outcome in
’Effects of interventions’.
Sensitivity analyses
Sensitivity analyses were performed for every element on the risk
of bias table by excluding studies that had a high risk of bias. Other
sensitivity analyses included:
• excluding very long or large studies to establish how much
they dominate the results;
• excluding studies using the following filters: diagnostic
criteria, date of publication, language of publication, source of
funding (industry versus other), country.
Values were noted (data not shown) and found to be similar to
overall effect estimates.
Assessment of reporting biases
Funnel plot symmetry was not found in any of the meta-analysis.
D I S C U S S I O N
Summary of main results
Twenty-three studies randomised 976 participants with type 1 dia-
betes to either continuous subcutaneous insulin infusion (CSII) or
multiple insulin injections (MI) (three or more insulin injections
per day). Study duration ranged from six days to four years. Upon
meta-analysis of 20 studies that reported glycosylated haemoglo-
bin A1c (HbA1c) (overall unclear risk of bias), there was a statisti-
cally significant difference in favour of CSII, the mean difference
was -0.3% (95% confidence interval (CI) -0.4 to -0.1, P = 0.001).
Without altering the direction of effect, heterogeneity was reduced
from an I2 statistic of 50% to 34% upon removal of Nathan 1982,
a study with high risk of bias. Subgroup analyses for age did not
significantly alter the effect estimate, however subgroup analyses
for study duration showed that medium term studies (12 studies,
one to six months) had a higher effect estimate (-0.3% (95% CI
-0.5 to -0.1)) and long term studies (seven studies, more than six
months) had a lower non-significant effect estimate (-0.2% (95%
CI -0.4 to 0.1)).
Thirteen studies were meta-analysed for daily mean blood glucose
(overall unclear risk of bias). Due to considerable heterogeneity (I2 statistic of 94%) a reliable pooled effect estimate could not be
established. Subgroup analysis for age demonstrated that the effect
estimate and heterogeneity were lower and non-significant among
the two studies with participants under 18 years of age (-4 mg/dl
(95% CI -14 to 7), I2 statistic of 0%). Subgroup analysis for study
duration showed that combination of the two long term studies
18Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

resulted in a higher effect estimate (-21 mg/dl (95% CI -29 to -
13), I2 statistic of 0%).
Eleven studies reported fasting blood glucose (overall high risk of
bias). Due to considerable heterogeneity (I2 statistic of 71%) a
reliable pooled effect estimate could not be established. Subgroup
analysis for age demonstrated that the effect estimate and hetero-
geneity were lower among the three studies with participants un-
der 18 years of age (-8 mg/dl (95% CI -24 to 9), I2 statistic of
0%).
Meta-analysis of the five studies that reported post-prandial blood
glucose (overall high risk of bias) demonstrated a non-significant
difference between the interventions with an effect estimate of -
4 mg/dl (95% CI -11 to 2, I2 statistic of 37%) in favour of CSII
compared with MI. Subgroup analyses for age and study duration
did not substantially alter the effect estimates or heterogeneity.
Non-severe hypoglycaemia, often defined in the studies as a blood
glucose level lower than 70 mg/dl, was reported in 17 studies (over-
all unclear risk of bias) using different scales. It was not appropriate
to conduct a meta-analysis, however the data suggested that there
is no relevant benefit of one intervention over the other for re-
ducing non-severe hypoglycaemic events. Severe hypoglycaemia,
often defined in the studies as requiring assistance from another
person for recovery or resulting in coma or seizure, was reported
in 15 studies (overall unclear risk of bias) using different scales.
Despite it not being appropriate to conduct a meta-analysis, the
data suggest that CSII may be better than MI for reducing the
incidence of severe hypoglycaemic events.
Quality of life was reported in 15 studies (overall unclear risk of
bias) using different scales. It was not appropriate to conduct a
meta-analysis, however many of the studies used validated ques-
tionnaires and found that CSII was preferred over MI for treat-
ment satisfaction, quality of life and perception of better general
and mental health. Often, participants randomised to CSII pre-
ferred to continue with CSII at study completion rather than re-
turn to MI.
There was a statistically significant decrease in daily insulin re-
quirement measured in units (U) by nine studies (overall high risk
of bias). The mean difference was -7 U (95% CI -11 to -3, P =
0.0003, I2 statistic of 32%). There was an insufficient number of
studies for subgroup analyses for age and study duration. When
measured in units per kilogram (U/kg), the daily insulin require-
ment mean difference found among 12 studies (overall unclear
risk of bias) could not be reliably pooled due to considerable het-
erogeneity (I2 statistic of 94%).
No significant difference was found for weight (-0.4 kg (95% CI
-2 to 1.3), I2 statistic of 0%) among eight studies (overall unclear
risk of bias). Subgroup analysis for age did not significantly alter
the effect estimate, however subgroup analysis for study duration
showed that long term studies (seven studies) had a higher non-
significant effect estimate -1.6 kg (95% CI -7.7 to 4.5, I2 statistic
of 27%).
Information about adverse events other than non-severe and severe
hypoglycaemic events was not well reported. Most common other
adverse events included ketoacidosis, dehydration and injection or
infusion site complications. There were high numbers of injection
or infusion site complications, suggesting that training on the use
and care of these interventions is vital.
None of the studies reported on mortality, morbidity or costs.
Exploration of small study bias revealed that the effect estimates
for HbA1c, daily mean blood glucose, daily insulin requirement
(U/kg) and weight were higher than the effect estimates for these
outcomes when all studies were included, suggesting that small
study bias may be present for these outcomes.
Funnel plot asymmetry was found in all meta-analyses. It should
be noted that there are a number of explanations for the asymmetry
of a funnel plot, including true heterogeneity of effect with respect
to study size, poor methodological design of small studies and
publication bias (Sterne 2001).
Overall completeness and applicability ofevidence
There were many gaps in the information provided by the study
investigators about quality and data. Nineteen study investigators
were contacted for clarification of study design, data or both, and
53% (10 study investigators) replied to our questionnaire.
Six cross-over studies were not adequately analysed, and did not
report correlations between baseline and end-of-study data, there-
fore ignoring within-person variation. We reanalysed the data from
these studies assuming different correlation coefficients (0.3, 0.5,
0.7, 0.9) and have discussed the ’Effects of interventions’ based on
the most conservative approach, assuming a correlation coefficient
of 0.3. The data from these studies were also reanalysed assuming
the largest standard deviation of the differences derived from the
cross-over studies with adequate statistical methodology. The re-
sults from the analyses assuming different correlation coefficients
and the largest standard deviation of the differences (found in Ap-
pendix 3) do not vary substantially from that presented in ’Effects
of interventions’ for direction of effect and heterogeneity.
Participants in the included studies were both adults and children
with type 1 diabetes, suggesting that the results would be relevant
to a broad spectrum of age groups in similar contexts. None of the
studies were conducted in developing countries.
The mean reduction in HbA1c associated with CSII was relatively
small at 0.3 percentage points, and likely to be of only borderline
clinical relevance. However, the reduction frequency of severe hy-
poglycaemic events was of greater clinical relevance, with 8 out of
15 studies providing data on severe hypoglycaemia reporting a re-
duction of at least 50% in the frequency of severe hypoglycaemia.
Thus, CSII is likely to be a clinically useful alternative for those
individuals in whom there is concern about severe hypoglycaemia.
19Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Quality of the evidence
Using the approach described in ’Assessment of risk of bias in
included studies’, the body of evidence was classified as high, un-
clear or low risk of bias for each outcome. Risk of bias was un-
clear for most of the evidence, but for studies reporting the out-
comes daily insulin requirement (U), fasting blood glucose and
post-prandial blood glucose, the body of evidence was at high risk
of bias.
Potential biases in the review process
This review consists of published data only. In future, updates will
attempt to identify non-published studies.
The selection criteria specified that MI required three or more
injections per day, therefore many studies were excluded because
their definition of MI was two or more injections per day. We
are uncertain whether these studies would have altered the effect
estimates seen in this review.
Many different scales and units were used to report measures of
non-severe and severe hypoglycaemia and quality of life. There
were insufficient studies to conduct meta-analyses for each of the
scales and units, and as a result, our interpretation of the overall
effects of the interventions on these outcomes is subjective and
open to bias.
Agreements and disagreements with otherstudies or reviews
A systematic review by Pickup et al (Pickup 2002), a health-tech-
nology assessment (HTA) report (HTA 2004) and a NICE report
(NICE 2008) were in agreement with the findings of this review.
The systematic review by Pickup et al found that glycosylated
haemoglobin A1c and mean blood glucose concentration were
lower in people receiving CSII compared with those receiving
MI. Blood glucose concentrations were less variable during CSII
and the insulin dose required to maintain glycaemic control was
reduced with CSII.
The HTA report found that the quality of included studies was
generally poor. When compared with at least three injections per
day (MI), CSII resulted in a modest but important improvement
in glycosylated haemoglobin A1c and a short term reduction in
insulin dose in adults with type 1 diabetes. Overall hypoglycaemic
events did not differ between CSII and MI. The authors of the
HTA review were unable to identify any economic evaluations
comparing these two interventions, however it is estimated that
the additional cost associated with using CSII over MI varies from
£1091 (1208 EURO, 11/2009 exchange rate) to £1680 (1860
EURO, 11/2009 exchange rate), per annum (including the cost
of the pump and consumables).
The NICE report focused on recommendations for when to
use CSII. The report included non-randomised and randomised
studies and found improvement in HbA1c and reduction in in-
sulin dose. No difference was found for hypoglycaemic events
and weight between the two interventions but patient preference
slightly favoured CSII.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
Both continuous subcutaneous insulin infusion (CSII) and mul-
tiple insulin injections (MI)CSII are currently used in practice.
There may be benefit in using CSII over MI for improving gly-
caemic control and improving health-related quality of life in peo-
ple with type 1 diabetes. Non-severe hypoglycaemic events do not
appear to be influenced differently by either intervention.
It is important to note that there is insufficient evidence regarding
adverse events, diabetes late complications, mortality and cost - all
essential considerations in deciding which treatment to administer
in practice. Until evidence is available for these outcomes we are
unable to make a recommendation about whether either interven-
tion is superior over the other in the management of glycaemic
control in people with type 1 diabetes.
Implications for research
Long term, large scale and methodologically rigorous studies are
required to determine the effect of CSII and MI on outcomes such
as hypoglycaemia, mortality, diabetes late complications and other
adverse effects, using validated scales. Cost effectiveness data are
also required to determine superiority between the two interven-
tions.
A C K N O W L E D G E M E N T S
The authors would like to acknowledge several colleagues for their
assistance in preparation of this review: Steve McDonald from
the Australasian Cochrane Centre and Karla Bergerhoff, the Tri-
als Search Coordinator of the Cochrane Metabolic and Endocrine
Disorders Group for their assistance in developing the search strat-
egy. Joanne McKenzie from the Australasian Cochrane Centre and
Damien Jolley from Monash Institute of Health Services Research
for biostatistical advice. Miranda Cumpston and Veronica Pitt
from the Australasian Cochrane Centre for methodological advice.
The authors would like to acknowledge the following study in-
vestigators for providing additional study information or data: JF
Bak, H Hanaire Broutin, RPLM Hoogma, JH DeVries, G Lepore,
N Weintrob and B Zinman (for Tsui 2001).
20Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

R E F E R E N C E S
References to studies included in this review
Bak 1987 and Husted 1989 {published and unpublished data}
Bak JF, Nielsen OH, Pedersen O, Beck-Nielsen H. Multiple
insulin injections using a pen injector versus insulin pump
treatment in young diabetic patients. Diabetes Research
1987;6(3):155–8.
Husted SE, Nielsen HK, Bak JF, Beck-Nielsen H.
Antithrombin III activity, von Willebrand factor antigen
and platelet function in young diabetic patients treated with
multiple insulin injections versus insulin pump treatment.
European Journal of Clinical Investigation 1989;19(1):90–4.
Botta 1986 {published data only}
Botta RM, Sinagra D, Angelico MC, Bompiani GD.
[Comparison of intensified traditional insulin therapy
and micropump therapy in pregnant women with type 1
diabetes mellitus]. Minerva Medica 1986;77(17):657–61.
Bruttomesso 2008 {published data only}
Bruttomesso D, Crazzolara D, Maran A, Costa S, Dal Pos
M, Girelli A, et al.In Type 1 diabetic patients with good
glycaemic control, blood glucose variability is lower during
continuous subcutaneous insulin infusion than during
multiple daily injections with insulin glargine. Diabetic
Medicine 2008;25(3):326–32.
Chiasson 1984 and 1985 {published data only}
Chiasson JL, Ducros F, Poliquin-Hamet M, Lopez D,
Lecavalier L, Hamet P. Continuous subcutaneous insulin
infusion (Mill-Hill Infuser) versus multiple injections
(Medi-Jector) in the treatment of insulin-dependent
diabetes mellitus and the effect of metabolic control on
microangiopathy. Diabetes Care 1984;7(4):331–7.
Cohen 2003 {published data only}
Cohen D, Weintrob N, Benzaquen H, Galatzer A, Fayman
G, Phillip M. Continuous subcutaneous insulin infusion
versus multiple daily injections in adolescents with type
I diabetes mellitus: a randomized open crossover trial.
Journal of pediatric endocrinology & metabolism 2003;16(7):
1047–50.
DeVries 2002 {published and unpublished data}
DeVries JH, Snoek FJ, Kostense PJ, Masurel N, Heine RJ.
A randomized trial of continuous subcutaneous insulin
infusion and intensive injection therapy in type 1 diabetes
for patients with long-standing poor glycemic control.
Diabetes Care 2002;25(11):2074–80.
Doyle 2004 {published data only}
Doyle EA, Weinzimer SA, Steffen AT, Ahern JA, Vincent
M, Tamborlane WV. A randomized, prospective trial
comparing the efficacy of continuous subcutaneous insulin
infusion with multiple daily injections using insulin
glargine. Diabetes Care 2004;27(7):1554–8.
Hanaire-Broutin 2000 {published and unpublished data}
Hanaire-Broutin H, Melki V, Bessieres-Lacombe S, Tauber
JP. Comparison of continuous subcutaneous insulin
infusion and multiple daily injection regimens using insulin
lispro in type 1 diabetic patients on intensified treatment: a
randomized study. The Study Group for the Development
of Pump Therapy in Diabetes. Diabetes Care 2000;23(9):
1232–5.
Hirsch 2005 {published data only}
Hirsch IB, Bode BW, Garg S, Lane WS, Sussman A, Hu
P, et al.Continuous subcutaneous insulin infusion (CSII)
of insulin aspart versus multiple daily injection of insulin
aspart/insulin glargine in type 1 diabetic patients previously
treated with CSII. Diabetes Care 2005;28(3):533–8.
Home 1982 {published data only}
Home PD, Capaldo B, Burrin JM, Worth R, Alberti
KG. A crossover comparison of continuous subcutaneous
insulin infusion (CSII) against multiple insulin injections in
insulin-dependent diabetic subjects: improved control with
CSII. Diabetes Care 1982;5(5):466–71.
Hoogma 2005 {published and unpublished data}
Hoogma RPLM, Hoekstra JB, Michels BP, Levi M.
Comparison between multiple daily insulin injection
therapy (MDI) and continuous subcutaneous insulin
infusion therapy (CSII), results of the five nations study.
Diabetes Research & Clinical Practice 2006;74 Suppl 2:
S144–7.
Lepore 2003 {published and unpublished data}
Lepore G, Dodesini AR, Nosari I, Trevisan R. Both
continuous subcutaneous insulin infusion and a multiple
daily insulin injection regimen with glargine as basal insulin
are equally better than traditional multiple daily insulin
injection treatment. Diabetes Care 2003;26(4):1321–2.
Meschi 1982 {published data only}
Meschi F, Beccaria L, Vanini R, Szulc M, Chiumello G.
Short-term subcutaneous insulin infusion in diabetic
children. Comparison with three daily insulin injections.
Acta Diabetologica Latina 1982;19(4):371–5.
Nathan 1982 {published data only}
Nathan Dm LPAJ. Intensive conventional and insulin
pump therapies in adult type I diabetes. A crossover study.
Annals of Internal Medicine 1982;97:31–6.
Nosadini 1988 {published data only}
Nosadini R. Frequency of hypoglycaemic and
hyperglycaemic-ketotic episodes during conventional and
subcutaneous continuous insulin infusion therapy in
IDDM. Diabetes Nutrition and Metabolism 1988;1:289–96.
Nuboer 2008 {published data only}
Nuboer R, Borsboom GJJM, Zoethout JA, Koot HM,
Bruining J. Effects of insulin pump vs. injection treatment
on quality of life and impact of disease in children with
type 1 diabetes mellitus in a randomized, prospective
comparison. Pediatric Diabetes 2008;9(4 Pt 1):291–6.
Oslo Study 1985 to 1992 {published data only}
Brinchmann-Hansen O, Dahl-Jorgensen K, Hanssen KF.
Effects of intensified insulin treatment on various lesions of
21Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

diabetic retinopathy. American Journal of Ophthalmology
1985;100(5):644–53.
Brinchmann-Hansen O, Dahl-Jorgensen K, Hanssen KF,
Sandvik L. Oscillatory potentials, macular recovery time,
and diabetic retinopathy through 3 years of intensified
insulin treatment.[see comment]. Ophthalmology 1988;95
(10):1358–66.
Brinchmann-Hansen O, Dahl-Jorgensen K, Hanssen KF,
Sandvik L. The response of diabetic retinopathy to 41
months of multiple insulin injections, insulin pumps, and
conventional insulin therapy. Archives of Ophthalmology
1988;106(9):1242–6.
Dahl Jorgensen K. Blood glucose control and progression of
diabetic neuropathy: eight years results from the Oslo study.
Diabetologia 1992;35:A15.
Dahl-Jorgensen K. Near-normoglycemia and late diabetic
complications. The Oslo Study. Acta Endocrinologica
Supplementum 1987;284:1–38.
Dahl-Jorgensen K, Bjoro T, Kierulf P, Sandvik L, Bangstad
HJ, Hanssen KF. Long-term glycemic control and kidney
function in insulin-dependent diabetes mellitus. Kidney
International 1992;41(4):920–3.
Dahl-Jorgensen K, Brinchmann-Hansen O, Hanssen KF.
Rapid tightening of blood glucose control leads to transient
deterioration of retinopathy in insulin dependent diabetes
mellitus: The Oslo study. British Medical Journal 1985;290
(6471):811–5.
Dahl-Jorgensen K, Brinchmann-Hansen O, Hanssen
KF, Ganes T, Kierulf P, Smeland E, et al.Effect of near
normoglycaemia for two years on progression of early
diabetic retinopathy, nephropathy, and neuropathy: the
Oslo study. British Medical Journal Clinical ResearchEducation 1986;293(6556):1195–9.
Dahl-Jorgensen K, Hanssen KF, Aagenaes O, Larsen S.
[New methods for subcutaneous insulin administration. A
year’s experience with the insulin pump and multiple insulin
injection therapy]. Tidsskrift for Den Norske Laegeforening
1984;104(13):856–61.
Dahl-Jorgensen K, Hanssen KF, Kierulf P, Bjoro T, Sandvik
L, Aagenaes O. Reduction of urinary albumin excretion
after 4 years of continuous subcutaneous insulin infusion in
insulin-dependent diabetes mellitus. The Oslo Study. ActaEndocrinologica 1988;117(1):19–25.
Dahl-Jorgensen K, Torjesen P, Hanssen KF, Sandvik
L, Aagenaes O. Increase in insulin antibodies during
continuous subcutaneous insulin infusion and multiple-
injection therapy in contrast to conventional treatment.
Diabetes 1987;36(1):1–5.
Hanssen KF, Dahl-Jorgensen K, Brinchmann-Hansen O.
The influence of strict control on diabetic complications.
Acta Endocrinologica Supplementum 1985;272:57–60.
Pozzilli 2003 {published data only}
Pozzilli P, Crino A, Schiaffini R, Manfrini S, Fioriti E,
Coppolino G, et al.A 2-year pilot trial of continuous
subcutaneous insulin infusion versus intensive insulin
therapy in patients with newly diagnosed type 1 diabetes
(IMDIAB 8). Diabetes Technology & Therapeutics 2003;5
(6):965–74.
Saurbrey 1988 {published data only}
Saurbrey N, Arnold-Larsen S, Moller-Jensen B, Kuhl C.
Comparison of continuous subcutaneous insulin infusion
with multiple insulin injections using the NovoPen.
Diabetic Medicine 1988;5(2):150–3.
Schmitz 1989 {published data only}
Schmitz A, Christiansen JS, Christensen CK, Hermansen
K, Mogensen CE. Effect of pump versus pen treatment
on glycaemic control and kidney function in long-term
uncomplicated insulin-dependent diabetes mellitus
(IDDM). Danish Medical Bulletin 1989;36(2):176–8.
Skogsberg 2008 {published data only}
Skogsberg L, Fors H, Hanas R, Chaplin JE, Lindman
E, Skogsberg J. Improved treatment satisfaction but no
difference in metabolic control when using continuous
subcutaneous insulin infusion vs. multiple daily injections
in children at onset of type 1 diabetes mellitus. Pediatric
Diabetes 2008;9(5):472–9.
Tsui 2001 {published and unpublished data}
Tsui E, Barnie A, Ross S, Parkes R, Zinman B. Intensive
insulin therapy with insulin lispro: a randomized trial of
continuous subcutaneous insulin infusion versus multiple
daily insulin injection.[see comment]. Diabetes Care 2001;
24(10):1722–7.
Weintrob 2004 {published and unpublished data}
Weintrob N, Schechter A, Benzaquen H, Shalitin S, Lilos P,
Galatzer A, et al.Glycemic patterns detected by continuous
subcutaneous glucose sensing in children and adolescents
with type 1 diabetes mellitus treated by multiple daily
injections vs continuous subcutaneous insulin infusion.
Archives of Pediatrics & Adolescent Medicine 2004;158(7):
677–84.
References to studies excluded from this review
Alemzadeh 2005 {published data only}
Alemzadeh R, Palma-Sisto P, Parton EA, Holzum MK.
Continuous subcutaneous insulin infusion and multiple
dose of insulin regimen display similar patterns of blood
glucose excursions in pediatric type 1 diabetes. Diabetes
Technology & Therapeutics 2005;7(4):587–96.
Amemiya 1983 {published data only}
Amemiya S, Kato K, Asayama K. The improved response
in endogenous insulin due to continuous subcutaneous
infusion of insulin therapy in juvenile diabetes. Tohoku
Journal of Experimental Medicine 1983;141 Suppl:713–7.
Arias 1985 {published data only}
Arias P, Kerner W, Zier H, Navascues I, Pfeiffer EF.
Incidence of hypoglycemic episodes in diabetic patients
under continuous subcutaneous insulin infusion and
intensified conventional insulin treatment: assessment
by means of semiambulatory 24-hour continuous blood
glucose monitoring. Diabetes Care 1985;8(2):134–40.
Bagdade 1991 {published data only}
Bagdade JD, Helve E, Taskinen MR. Effects of continuous
insulin infusion therapy on lipoprotein surface and core
22Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

lipid composition in insulin-dependent diabetes mellitus.
Metabolism: Clinical & Experimental 1991;40(5):445–9.
Bangstad 1994 {published data only}
Bangstad HJ, Osterby R, Dahl-Jorgensen K, Berg KJ,
Hartmann A, Hanssen KF. Improvement of blood glucose
control in IDDM patients retards the progression of
morphological changes in early diabetic nephropathy.
Diabetologia 1994;37(5):483–90.
Barbosa 1981 {published data only}
Barbosa J, Menth L, Eaton J, Sutherland D, Freier EF,
Najarian J. Long-term, ambulatory, subcutaneous insulin
infusion versus multiple daily injections in brittle diabetic
patients. Diabetes Care 1981;4(2):269–74.
Barrett 1995 {published data only}
Barrett DH, Davidson PC, Steed LJ, Abel GG, Loman KE,
Saudek CD. Evaluation of the psychosocial impact of the
MiniMed variable-rate implantable insulin pump. Southern
Medical Journal 1995;88(12):1226–30.
Bech 1996 {published data only}
Bech P, Gudex C, Staehr Johansen K. The WHO (Ten)
well-being index: Validation in diabetes. Psychotherapy and
Psychosomatics 1996;65(4):183–90.
Beck-Nielsen 1984 {published data only}
Beck-Nielsen H, Richelsen B, Hasling C, Nielsen OH,
Heding L, Sorensen NS. Improved in vivo insulin effect
during continuous subcutaneous insulin infusion in patients
with IDDM. Diabetes 1984;33(9):832–7.
Beck-Nielsen 1985 {published data only}
Beck-Nielsen H, Richelsen B, Mogensen CE, Olsen T,
Ehlers N, Nielsen CB, et al.Effect of insulin pump treatment
for one year on renal function and retinal morphology in
patients with IDDM. Diabetes Care 1985;8(6):585–9.
Beck-Nielsen 1985a {published data only}
Beck-Nielsen H, Richelsen B, Sorensen NS, Nielsen OH.
Insulin pump treatment: Effect on glucose homeostasis,
metabolites, hormones, insulin antibodies and quality of
life. Diabetes Research 1985;2(1):37–43.
Beck-Nielsen 1990 {published data only}
Beck-Nielsen H, Olesen T, Mogensen CE, Richelsen B,
Olsen HW, Ehlers N, et al.Effect of near normoglycemia
for 5 years on progression of early diabetic retinopathy and
renal involvement. Diabetes Research 1990;15(4):185–90.
Behme 1984 {published data only}
Behme MT, Dupre J. Insulin-binding to erythrocytes in
type I diabetes mellitus: effects of continuous subcutaneous
infusion of insulin. Clinical & Investigative Medicine -
Medecine Clinique et Experimentale 1984;7(2):109–14.
Bell 1985 {published data only}
Bell PM, Hayes JR, Hadden DR, Archer DB. The effect of
plasma glucose control by continuous subcutaneous insulin
infusion or conventional therapy on retinal morphology and
urinary albumin excretion. Diabete et Metabolisme 1985;11
(4):254–61.
Bell 1985a {published data only}
Bell PM, Sawhney B, Hayes JR, Hadden DR. Effect of
plasma glucose control by continuous subcutaneous insulin
infusion on nerve conduction. Irish Journal of MedicalScience 1985;154(10):378–84.
Bending 1986 {published data only}
Bending JJ, Viberti GC, Watkins PJ, Keen H. Intermittent
clinical proteinuria and renal function in diabetes: evolution
and the effect of glycaemic control. British Medical JournalClinical Research Ed 1986;292(6513):83–6.
Berg 1998 {published data only}
Berg TJ, Nourooz-Zadeh J, Wolff SP, Tritschler HJ,
Bangstad HJ, Hanssen KF. Hydroperoxides in plasma are
reduced by intensified insulin treatment. A randomized
controlled study of IDDM patients with microalbuminuria.
Diabetes Care 1998;21(8):1295–300.
Bergenstal 1985 {published data only}
Bergenstal RM, Dupre J, Lawson PM, Rizza RA, Rubenstein
AH. Observations on C-peptide and free insulin in the
blood during continuous subcutaneous insulin infusion and
conventional insulin therapy. Diabetes 1985;34 Suppl 3:
31–6.
Berger 1989 {published data only}
Berger M, Chantelau EA, Spraul M. [Treatment of type
I diabetes mellitus with continuous subcutaneous insulin
infusion: indications and quality control]. Verhandlungender Deutschen Gesellschaft fur Innere Medizin 1989;95:
135–40.
Bibergeil 1987 {published data only}
Bibergeil H, Huttl I, Felsing W, Felsing U, Seidlein I,
Herfurth S, et al.36 months continuous subcutaneous
insulin infusion (CSII) in insulin dependent diabetes
(IDDM)--influence on early stages of retinopathy,
nephropathy and neuropathy--psychological analysis.
Experimental & Clinical Endocrinology 1987;90(1):51–61.
Biesenbach 1988 {published data only}
Biesenbach G, Grafinger P, Kaiser W, Stuby U, Zazgornik
J. [Metabolic control in labile type I diabetes with
conventional insulin therapy, basal bolus insulin therapy
using pens and continuous subcutaneous insulin infusion
with the pump]. Medizinische Klinik 1988;83(12):
398–401.
Bode 1996 {published data only}
Bode BW, Steed RD, Davidson PC. Reduction in severe
hypoglycemia with long-term continuous subcutaneous
insulin infusion in type I diabetes. Diabetes Care 1996;19
(4):324–7.
Bode 2004 {published data only}
Bode B, Shelmet J, Gooch B, Hassman DR, Liang J,
Smedegaard JK, et al.Patient perception and use of an
insulin injector/glucose monitor combined device. Diabetes
Educator 2004;30(2):301–9.
Bombor 1984 {published data only}
Bombor H, Bruns W, Ratzmann KP, Jutzi E, Albrecht G,
Michaelis D, et al.Long-term improvement in metabolic
control of unstable type I diabetes by s.c. insulin injection
23Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

patterns based on the dose profiles required by bed-side
artificial beta-cell. Experimental & Clinical Endocrinology1984;83(2):143–51.
Borisova 1989 {published data only}
Borisova AM, Koev D, Kirilov G. [An improvement in
insulin efficacy in patients with type-1 diabetes mellitus
following treatment using an insulin infusion pump].
Vutreshni Bolesti 1989;28(1):74–7.
Brunetti 1984 {published data only}
Brunetti P, Bueti A, Antonella MA, Calabrese G, Fabietti
PG, Santeusanio F, et al.Metabolic effects of intensified
insulin therapy. Experimental & Clinical Endocrinology1984;83(2):130–5.
Buysschaert 1981 {published data only}
Buysschaert M, Lejeune M, Lambert AE. Continuous
subcutaneous insulin infusion in the treatment of juvenile-
onset diabetes. Diabete et Metabolisme 1981;7(3):189–93.
Buysschaert 1983 {published data only}
Buysschaert M, Marchand E, Ketelslegers JM, Lambert
AE. Comparison of plasma glucose and plasma free insulin
during CSII and intensified conventional insulin therapy.
Diabetes Care 1983;6(1):1–5.
Calabrese 1982 {published data only}
Calabrese G, Bueti A, Santeusanio F, Giombolini A, Zega
G, Angeletti G, et al.Continuous subcutaneous insulin
infusion treatment in insulin-dependent diabetic patients:
a comparison with conventional optimized treatment in a
long-term study. Diabetes Care 1982;5(5):457–65.
Canny 1985 {published data only}
Canny CL, Kohner EM, Trautman J, Puklin J, Morse P.
Comparison of stereofundus photographs in patients with
insulin-dependent diabetes during conventional insulin
treatment or continuous subcutaneous insulin infusion.
Diabetes 1985;34 Suppl 3:50–5.
Carta 1986 {published data only}
Carta Q, Meriggi E, Trossarelli GF, Catella G, Dal Molin V,
Menato G, et al.Continuous subcutaneous insulin infusion
versus intensive conventional insulin therapy in type I and
type II diabetic pregnancy. Diabete et Metabolisme 1986;12
(3):121–9.
Cavallo-Perin 1983 {published data only}
Cavallo-Perin P, Pagano G, Tagliaferro V, Jarre P, Ozzello
A, Lenti G. The treatment of unstable type I diabetes:
conventional versus portable pump insulin administration.
Acta Diabetologica Latina 1983;20(4):363–70.
Chisholm 1984 {published data only}
Chisholm DJ, Kraegen EW, Hewett MJ. Hypoglycemic
episodes during continuous subcutaneous insulin infusion:
decreased frequency but increased susceptibility. Australian& New Zealand Journal of Medicine 1984;14(3):255–9.
Christensen 1986 {published data only}
Christensen CK, Christiansen JS, Christensen T,
Hermansen K, Mogensen CE. The effect of six months
continuous subcutaneous insulin infusion on kidney
function and size in insulin-dependent diabetics. Diabetic
Medicine 1986;3(1):29–32.
Christensen 1987 {published data only}
Christensen CK, Christiansen JS, Schmitz A, Christensen
T, Hermansen K, Mogensen CE. Effect of continuous
subcutaneous insulin infusion on kidney function and size
in IDDM patients: a 2 year controlled study. Journal of
Diabetic Complications 1987;1(3):91–5.
Christiansen 1987 {published data only}
Christiansen JS, Ingerslev J, Bernvil SS, Christensen CK,
Hermansen K, Schmitz A. Near normoglycemia for 1 year
has no effect on platelet reactivity, factor VIII, and von
Willebrand factor in insulin-dependent diabetes mellitus: a
controlled trial. Journal of Diabetic Complications 1987;1
(3):100–6.
Ciavarella 1985 {published data only}
Ciavarella A, Vannini P, Flammini M, Bacci L, Forlani G,
Borgnino LC. Effect of long-term near-normoglycemia
on the progression of diabetic nephropathy. Diabete et
Metabolisme 1985;11(1):3–8.
Colette 1986 {published data only}
Colette C, Monnier L, Arnal J, Selam JL, Mirouze J. Effects
of different insulin administration modalities on vitamin
D metabolism of insulin-dependent diabetic patients.
Advances in Experimental Medicine & Biology 1986;208:
501–8.
Colette 1989 {published data only}
Colette C, Pares-Herbute N, Monnier L, Selam JL, Thomas
N, Mirouze J. Effect of different insulin administration
modalities on vitamin D metabolism of insulin-dependent
diabetic patients. Hormone & Metabolic Research 1989;21
(1):37–41.
Connis 1989 {published data only}
Connis RT, Taylor TR, Gordon MJ, Mecklenburg RS,
Liljenquist JE, Stephens JW, et al.Changes in cognitive and
social functioning of diabetic patients following initiation of
insulin infusion therapy. Experimental Aging Research 1989;
15(1-2):51–60.
Coustan 1986 {published data only}
Coustan DR, Reece EA, Sherwin RS, Rudolf MC, Bates
SE, Sockin SM, et al.A randomized clinical trial of the
insulin pump vs intensive conventional therapy in diabetic
pregnancies. JAMA 1986;255(5):631–6.
Davies 1984 {published data only}
Davies AG, Price DA, Houlton CA, Burn JL, Fielding BA,
Postlethwaite RJ. Continuous subcutaneous insulin infusion
in diabetes mellitus. A year’s prospective trial. Archives of
Disease in Childhood 1984;59(11):1027–33.
de Beaufort 1985 {published data only}
de Beaufort CE, Bruining GJ, Aarsen RS, den Boer NC,
Grose WF. Does continuous subcutaneous insulin infusion
(CSII) prolong the remission phase of insulin-dependent
diabetic children? Preliminary findings of a randomized
prospective study. Netherlands Journal of Medicine 1985;28
Suppl 1:53–4.
24Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
de Beaufort 1989 {published data only}
de Beaufort CE, Houtzagers CM, Bruining GJ, Aarsen RS,
den Boer NC, Grose WF, et al.Continuous subcutaneous
insulin infusion (CSII) versus conventional injection
therapy in newly diagnosed diabetic children: two-year
follow-up of a randomized, prospective trial. DiabeticMedicine 1989;6(9):766–71.
Dicker 1987 {published data only}
Dicker D, Feldberg D, Karp M, Yeshaya A, Samuel N,
Goldman JA. Preconceptional diabetes control in insulin-
dependent diabetes mellitus patients with continuous
subcutaneous insulin infusion therapy. Journal of PerinatalMedicine 1987;15(2):161–7.
DiMeglio 2004 {published data only}
DiMeglio LA, Pottorff TM, Boyd SR, France L, Fineberg
N, Eugster EA. A randomized, controlled study of insulin
pump therapy in diabetic preschoolers. Journal of Pediatrics
2004;145(3):380–4.
Edelmann 1987 {published data only}
Edelmann E, Walter H, Biermann E, Schleicher E,
Bachmann W, Mehnert H. Sustained normoglycemia and
remission phase in newly diagnosed type I diabetic subjects.
Comparison between continuous subcutaneous insulin
infusion and conventional therapy during a one year follow-
up. Hormone & Metabolic Research 1987;19(9):419–21.
Feldt-Rasmussen 1986 {published data only}
Feldt-Rasmussen B, Mathiesen ER, Deckert T. Effect of two
years of strict metabolic control on progression of incipient
nephropathy in insulin-dependent diabetes. Lancet 1986;
328(8519):1300–4.
Feldt-Rasmussen 1986a {published data only}
Feldt-Rasmussen B, Mathiesen ER, Hegedus L, Deckert
T. Kidney function during 12 months of strict metabolic
control in insulin-dependent diabetic patients with incipient
nephropathy. New England Journal of Medicine 1986;314
(11):665–70.
Feldt-Rasmussen 1991 {published data only}
Feldt-Rasmussen B, Mathiesen ER, Jensen T, Lauritzen T,
Deckert T. Effect of improved metabolic control on loss
of kidney function in type 1 (insulin-dependent) diabetic
patients: an update of the Steno studies. Diabetologia 1991;
34(3):164–70.
Flores 1984 {published data only}
Flores d’Arcais A, Morandi F, Beccaria L, Meschi F,
Chiumello G. Metabolic control in newly diagnosed type
1 diabetic children. Effect of continuous subcutaneous
infusion. Hormone Research 1984;19(2):65–9.
Garg 2004 {published data only}
Garg SK, Walker AJ, Hoff HK, D’Souza AO, Gottlieb
PA, Chase HP. Glycemic parameters with multiple daily
injections using insulin glargine versus insulin pump.[see
comment]. Diabetes Technology & Therapeutics 2004;6(1):
9–15.
Garmo 2004 {published data only}
Garmo A, Pettersson-Frank B, Ehrenberg A. Treatment
effects and satisfaction in diabetic patients changing from
multiple daily insulin injections to CSII. Practical Diabetes
International 2004;21(1):7–12.
Giocolea 1988 {published data only}
Giocolea I, Hernandez I, Fombellida J, Vazquez JA. Renal
function of insulin-dependent diabetic patients, treated
with continuous subcutaneous insulin infusion pump. A
comparison with conventional insulin therapy during a
follow-up period of one year. Anales de Medicina Interna1988;5(4):169–72.
Goicolea 1986 {published data only}
Goicolea Opacua I, Hernandez Colau I, Vazquez Garcia JA.
[Comparative study between the subcutaneous continuous
insulin infusion pump and optimized conventional
treatment. Effects at 6 months]. Revista Clinica Espanola1986;179(1):3–7.
Goicolea 1987 {published data only}
Goicolea Opacua I, Hernandez Colau I, Cortazar Galarza
A, Vazquez Garcia JA. [Comparison of metabolic control
between the continuous subcutaneous insulin infusion
pump and augmented conventional treatment. Effects after
12 months]. Medicina Clinica 1987;88(16):617–20.
Goicolea 1988 {published data only}
Goicolea Opacua I, Martinez Castillo A, Santamaria Pelarda
E, Sola Sarabia C, Vazquez Garcia JA. [Metabolic control
using a subcutaneous insulin infusion pump: effects 2 years
after treatment]. Revista Clinica Espanola 1988;182(4):
200–2.
Goicolea 1989 {published data only}
Goicolea I, Santamaria E, Pardo C, Vazquez JA, Martin A,
Castresana I. [Course of diabetic retinopathy and metabolic
control with subcutaneous insulin infusion pump: 18-
month study]. Anales de Medicina Interna 1989;6(2):71–3.
Greene 1983 {published data only}
Greene SA, Smith MA, Baum JD. Clinical application of
insulin pumps in the management of insulin dependent
diabetes. Archives of Disease in Childhood 1983;58(8):
578–81.
Grimm 1987 {published data only}
Grimm JJ, Haardt MJ, Thibult N, Goicolea I, Tchobroutsky
G, Slama G. Lifestyle, metabolic control and social
implications of pump therapy in 54 routine type I diabetic
patients. Diabete et Metabolisme 1987;13(1):3–11.
Guerci 1998 {published data only}
Guerci B, Meyer L, Delbachian I, Kolopp M, Ziegler O,
Drouin P. Blood glucose control on Sunday in IDDM
patients: intensified conventional insulin therapy versus
continuous subcutaneous insulin infusion. Diabetes Research& Clinical Practice 1998;40(3):175–80.
Gulan 1988 {published data only}
Gulan M, Perlman K, Sole M, Albisser AM, Zinman B.
Counterregulatory hormone responses preserved after long-
term intravenous insulin infusion compared to continuous
subcutaneous insulin infusion. Diabetes 1988;37(5):
526–31.
25Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Haakens 1989 {published data only}
Haakens K, Hanssen KF, Dahl-Jorgensen K, Vaaler S,
Torjesen P, Try K. Early morning glycaemia and the
metabolic consequences of delaying breakfast/morning
insulin. A comparison of continuous subcutaneous insulin
infusion and multiple injection therapy with human
isophane or human ultralente insulin at bedtime in insulin-
dependent diabetics. Scandinavian Journal of Clinical &Laboratory Investigation 1989;49(7):653–9.
Haakens 1990 {published data only}
Haakens K, Hanssen KF, Dahl-Jorgensen K, Vaaler S,
Aagenaes O, Mosand R. Continuous subcutaneous insulin
infusion (CSII), multiple injection (MI) and conventional
insulin therapy (CT) in self-selecting insulin-dependent
diabetic patients. A comparison of metabolic control, acute
complications and patient preferences. Journal of Internal
Medicine 1990;228(5):457–64.
Hall 1989 {published data only}
Hall K, Johansson BL, Povoa G, Thalme B. Serum levels
of insulin-like growth factor (IGF) I, II and IGF binding
protein in diabetic adolescents treated with continuous
subcutaneous insulin infusion. Journal of Internal Medicine1989;225(4):273–8.
Haug 1987 {published data only}
Haug PJ, Kelly TM, Cannon RB, Edwards CQ. A self-
controlled study of the effect of continuous subcutaneous
insulin infusion on diabetic neuropathy. Journal of theNeurological Sciences 1987;82(1-3):123–32.
Heber 1977 {published data only}
Heber D, Molitch ME, Sperling MA. Low-dose continuous
insulin therapy for diabetic ketoacidosis. Prospective
comparison with “conventional” insulin therapy. Archives ofInternal Medicine 1977;137(10):1377–80.
Helve 1987 {published data only}
Helve E. High density lipoprotein subfractions during
continuous insulin infusion therapy. Atherosclerosis 1987;64
(2-3):173–80.
Helve 1987a {published data only}
Helve E, Koivisto VA, Lehtonen A. A crossover comparison
of continuous insulin infusion and conventional injection
treatment of type I diabetes. Acta Medica Scandinavica
1987;221(4):385–93.
Helve 1987b {published data only}
Helve E, Laatikainen L, Merenmies L, Koivisto VA.
Continuous insulin infusion therapy and retinopathy in
patients with type I diabetes. Acta Endocrinologica 1987;
115(3):313–9.
Hermansen 1987 {published data only}
Hermansen K, Moller A, Christensen CK, Christiansen
JS, Schmitz O, Orskov H, et al.Diurnal plasma profiles
of metabolite and hormone concentration in insulin-
dependent diabetic patients during conventional insulin
treatment and continuous subcutaneous insulin infusion. A
controlled study. Acta Endocrinologica 1987;114(3):433–9.
Hermansen 1988 {published data only}
Hermansen K, Schmitz O, Boye N, Christensen CK,
Christiansen JS, Alberti KG, et al.Glucagon responses to
intravenous arginine and oral glucose in insulin-dependent
diabetic patients during six months conventional or
continuous subcutaneous insulin infusion. Metabolism:Clinical & Experimental 1988;37(7):640–4.
Hoogma 2004 {published data only}
Hoogma RP, Spijker AJ, van Doorn-Scheele M, van Doorn
TT, Michels RP, van Doorn RG, et al.Quality of life and
metabolic control in patients with diabetes mellitus type
1 treated by continuous subcutaneous insulin infusion or
multiple daily insulin injections.[see comment]. Netherlands
Journal of Medicine 2004;62(10):383–7.
Hung 1984 {published data only}
Hung J, Menth L, Thompson MJ, Saner B, Rao KV,
Barbosa J. The Minnesota Diabetes Complications Clinical
Trial cognitive functions under long-term maximized and
standard metabolic controls. Diabete et Metabolisme 1984;
10(1):48–51.
Jakobsen 1988 {published data only}
Jakobsen J, Christiansen JS, Kristoffersen I, Christensen
CK, Hermansen K, Schmitz A, et al.Autonomic and
somatosensory nerve function after 2 years of continuous
subcutaneous insulin infusion in type I diabetes. Diabetes1988;37(4):452–5.
Jensen 1986 {published data only}
Jensen BM, Kuhl C, Molsted-Pedersen L. Preconceptional
treatment with insulin infusion pumps in insulin-dependent
diabetic women with particular reference to prevention of
congenital malformations. Acta Endocrinologica, Supplement
1986;112(277):81–5.
Kamoi 2004 {published data only}
Kamoi K, Miyakoshi M, Maruyama R. A quality-of-life
assessment of intensive insulin therapy using insulin lispro
switched from short-acting insulin and measured by an ITR-
QOL questionnaire: a prospective comparison of multiple
daily insulin injections and continuous subcutaneous
insulin infusion. Diabetes Research & Clinical Practice 2004;
64(1):19–25.
Kelly 1984 {published data only}
Kelly TM, Sanborn GE, Haug PJ, Edwards CQ. Effect of
insulin infusion pump use on diabetic retinopathy. Archivesof Ophthalmology 1984;102(8):1156–9.
Knight 1986 {published data only}
Knight G, Boulton AJM, Drury J, Ward JD. Long term
glycaemic control by alternative regimens in a feasibility
study of continuous subcutaneous insulin infusion. DiabetesResearch 1986;3(7):355–8.
Kobayashi 1987 {published data only}
Kobayashi T, Sawano S, Itoh T, Kosaka K. Plasma
immunoreactive somatostatin response to arginine after
glycemic control with continuous subcutaneous insulin
infusion in type I diabetics. Diabetes Care 1987;10(3):
286–92.
26Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Koivisto 1983 {published data only}
Koivisto VA, Tronier B. Postprandial blood glucose response
to exercise in type I diabetes: comparison between pump
and injection therapy. Diabetes Care 1983;6(5):436–40.
Kordonouri 2006 {published data only}
Kordonouri O, Hartmann R, Lauterborn R, Barnekow C,
Hoeffe J, Deiss D. Age-specific advantages of continuous
subcutaneous insulin infusion as compared with multiple
daily injections in pediatric patients: one-year follow-up
comparison by matched-pair analysis. Diabetes Care 2006;
29(1):133–4.
Kritz 1983 {published data only}
Kritz H, Hagmuller G, Lovett R, Irsigler K. Implanted
constant basal rate insulin infusion devices for Type 1
(insulin-dependent) diabetic patients. Diabetologia 1983;25
(2):78–81.
Kroc 1984 {published data only}
Kroc. Blood glucose control and the evolution of diabetic
retinopathy and albuminuria. A preliminary multicenter
trial. The Kroc Collaborative Study Group. The NewEngland journal of medicine 1984;311:365–72.
Kroc 1988 {published data only}
Kroc. Diabetic retinopathy after two years of intensified
insulin treatment. Follow-up of the Kroc Collaborative
Study. The Kroc Collaborative Study Group. JAMA :the journal of the American Medical Association 1988;260:
37–41.
Kuno 1996 {published data only}
Kuno T, Tasaki H, Miyazaki S. Continuous subcutaneous
insulin injection for self-care of young patients with insulin-
dependent diabetes mellitus. Acta Paediatrica Japonica1996;38(5):464–9.
Laatikainen 1987 {published data only}
Laatikainen L, Teramo K, Hieta-Heikurainen H, Koivisto
V, Pelkonen R. A controlled study of the influence of
continuous subcutaneous insulin infusion treatment on
diabetic retinopathy during pregnancy. Acta Medica
Scandinavica 1987;221(4):367–76.
Lager 1983 {published data only}
Lager I, Lonnroth P, von Schenck H, Smith U. Reversal of
insulin resistance in type I diabetes after treatment with
continuous subcutaneous insulin infusion. British MedicalJournal Clinical Research Ed 1983;287(6406):1661–4.
Lager 1986 {published data only}
Lager I, Attvall S, Blohme G, Smith U. Altered recognition
of hypoglycaemic symptoms in type I diabetes during
intensified control with continuous subcutaneous insulin
infusion. Diabetic Medicine 1986;3(4):322–5.
Lapolla 2003 {published data only}
Lapolla A, Dalfra MG, Masin M, Bruttomesso D, Piva I,
Crepaldi C, et al.Analysis of outcome of pregnancy in type 1
diabetics treated with insulin pump or conventional insulin
therapy. Acta Diabetologica 2003;40(3):143–9.
Lauritzen 1985 {published data only}
Lauritzen T, Frost-Larsen K, Larsen HW, Deckert T. Two-
year experience with continuous subcutaneous insulin
infusion in relation to retinopathy and neuropathy. Diabetes
1985;34 Suppl 3:74–9.
Lawson 1984 {published data only}
Lawson P, Trayner I, Rosenstock J, Kohner E. The effect of
continuous subcutaneous insulin infusion on serum lipids.
Diabete et Metabolisme 1984;10(4):239–44.
Lawson 1985 {published data only}
Lawson P, Home PD, Bergenstal R. Observations on blood
lipid and intermediary metabolite concentrations during
conventional insulin treatment or CSII. Diabetes 1985;34
Suppl 3:27–30.
Leblanc 1986 {published data only}
Leblanc H, Obadia G, Passa P. [Reduction of hypoglycemia
in 10 diabetic patients treated with continuous subcutaneous
infusion of insulin]. Presse Medicale 1986;15(10):463–6.
Lecavalier 1987 {published data only}
Lecavalier L, Havrankova J, Hamet P, Chiasson J-L. Effects
of continuous subcutaneous insulin infusion versus multiple
injections on insulin receptors in insulin-dependent
diabetics. Diabetes Care 1987;10(3):300–5.
Lepore 2004 {published data only}
Lepore G, Dodesini AR, Nosari I, Trevisan R. Effect of
continuous subcutaneous insulin infusion vs multiple daily
insulin injection with glargine as basal insulin: an open
parallel long-term study. Diabetes, Nutrition & Metabolism -Clinical & Experimental 2004;17(2):84–9.
Levy 1984 {published data only}
Levy I, Bergua M, Esmatjes E, Halperin I, Figuerola D.
[Unstable type I diabetes mellitus: comparative study
between intensive conventional treatment and continuous
subcutaneous infusion of insulin]. Medicina Clinica 1984;
83(13):525–8.
Levy-Marchal 1983 {published data only}
Levy-Marchal C, Albisser AM, Zinman B. Overnight
metabolic control with pulsed intermittent versus
continuous subcutaneous insulin infusion. Diabetes Care1983;6(4):356–60.
Levy-Marchal 1988 {published data only}
Levy-Marchal C, Czernichow P. Feasibility of continuous
subcutaneous insulin infusion in young diabetic patients.
Diabete et Metabolisme 1988;14(2):108–13.
Litton 2002 {published data only}
Litton J, Rice A, Friedman N, Oden J, Lee MM, Freemark
M. Insulin pump therapy in toddlers and preschool children
with type 1 diabetes mellitus. Journal of Pediatrics 2002;141
(4):490–5.
Ludvigsson 2003 {published data only}
Ludvigsson J, Hanas R. Continuous subcutaneous glucose
monitoring improved metabolic control in pediatric patients
with type 1 diabetes: a controlled crossover study. Pediatrics2003;111(5 Pt 1):933–8.
Lunetta 1996 {published data only}
Lunetta M, De Mauro M, Le Moli R, Nicoletti F. Effect
of octreotide on blood glucose and counterregulatory
hormones in insulin-dependent diabetic patients: the role
27Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

of dose and route of administration. European Journal of
Clinical Pharmacology 1996;51(2):139–44.
Mancuso 1986 {published data only}
Mancuso S, Caruso A, Lanzone A. Continuous
subcutaneous insulin infusion (CSII) in pregnant diabetic
women. Acta Endocrinologica, Supplement 1986;112(277):
112–6.
Marshall 1987 {published data only}
Marshall SM, Home PD, Taylor R, Alberti KG. Continuous
subcutaneous insulin infusion versus injection therapy:
a randomized cross-over trial under usual diabetic clinic
conditions. Diabetic Medicine 1987;4(6):521–5.
Marshall 1988 {published data only}
Marshall SM, Taylor R, Home PD, Alberti KG.
Intermediary metabolism, insulin sensitivity and insulin
receptor status under comparable long-term therapy with
insulin injections and continuous subcutaneous insulin
infusion. Acta Endocrinologica 1988;117(4):417–27.
McDonald 1982 {published data only}
McDonald JW, Dupre J, Rodger NW, Champion MC,
Webb CD, Ali M. Comparison of platelet thromboxane
synthesis in diabetic patients on conventional insulin
therapy and continuous insulin infusions. ThrombosisResearch 1982;28(6):705–12.
Mecklenburg 1982 {published data only}
Mecklenburg RS, Benson JW Jr, Becker NM, Brazel PL,
Fredlund PN, Metz RJ, et al.Clinical use of the insulin
infusion pump in 100 patients with type I diabetes. NewEngland Journal of Medicine 1982;307(9):513–8.
Minkina-Pedras 2005 {published data only}
Minkina-Pedras M, Jarosz-Chobot P, Malecka-Tendera
E, Deja G. [Assessment of metabolic control and
safety of continuous subcutaneous insulin infusion in
prepubertal children with type 1 diabetes mellitus].
Endokrynologia, Diabetologia i Choroby Przemiany MateriiWieku Rozwojowego 2005;11(3):171–6.
Moberg 1994 {published data only}
Moberg EA, Lins PE, Adamson UK. Variability of blood
glucose levels in patients with type 1 diabetes mellitus on
intensified insulin regimens. Diabete et Metabolisme 1994;
20(6):546–52.
Moller 1986 {published data only}
Moller A, Rasmussen L, Ledet T, Christiansen JS,
Christensen CK, Mogensen CE, et al.Lipoprotein changes
during continuous subcutaneous insulin infusion in insulin-
dependent diabetic patients. Scandinavian Journal ofClinical & Laboratory Investigation 1986;46(5):471–5.
Monnier 1987 {published data only}
Monnier LH, Rodier M, Gancel A. Plasma lipid fatty acids
and platelet function during continuous subcutaneous
insulin infusion in type I diabetes. Diabete et Metabolisme1987;13(3):210–6.
Muller 1999 {published data only}
Muller UA, Femerling M, Reinauer KM, Risse A, Voss
M, Jorgens V, et al.Intensified treatment and education of
type 1 diabetes as clinical routine. A nationwide quality-
circle experience in Germany. ASD (the Working Group
on Structured Diabetes Therapy of the German Diabetes
Association). Diabetes Care 1999;22 Suppl 2:B29–34.
Nathan 1996 {published data only}
Nathan DM, Dunn FL, Bruch J, McKitrick C, Larkin
M, Haggan C, et al.Postprandial insulin profiles with
implantable pump therapy may explain decreased
frequency of severe hypoglycemia, compared with intensive
subcutaneous regimens, in insulin-dependent diabetes
mellitus patients. American Journal of Medicine 1996;100
(4):412–7.
Ng 1986 {published data only}
Ng Tang Fui S, Pickup JC, Bending JJ, Collins AC, Keen H,
Dalton N. Hypoglycemia and counterregulation in insulin-
dependent diabetic patients: a comparison of continuous
subcutaneous insulin infusion and conventional insulin
injection therapy. Diabetes Care 1986;9(3):221–7.
Nijs 1991 {published data only}
Nijs HG, Radder JK, Poorthuis BJ, Krans HM. Glucose
disposal and intermediary metabolism during one year of
continuous subcutaneous insulin infusion (CSII). DiabetesResearch & Clinical Practice 1991;12(1):1–9.
Olsen 1985 {published data only}
Olsen T, Ehlers N, Nielsen CB, Beck-Nielsen H. Diabetic
retinopathy after one year of improved metabolic control
obtained by continuous subcutaneous insulin infusion
(CSII). Acta Ophthalmologica 1985;63(3):315–9.
Olsen 1987 {published data only}
Olsen T, Richelsen B, Ehlers N, Beck-Nielsen H. Diabetic
retinopathy after 3 years’ treatment with continuous
subcutaneous insulin infusion (CSII). Acta Ophthalmologica1987;65(2):185–9.
Pickup 1979 {published data only}
Pickup JC, Keen H, Parsons JA, Alberti KG. Continuous
subcutaneous insulin infusion:good blood glucose control
for up to 4 days. Diabetologia 1979;16(6):385–9.
Pickup 1979a {published data only}
Pickup JC, Keen H, Parsons JA, Alberti KG, Rowe AS.
Continuous subcutaneous insulin infusion: improved
blood-glucose and intermediary-metabolite control in
diabetics. Lancet 1979;1(8129):1255–7.
Pickup 1984 {published data only}
Pickup JC, Collins AC, Keen H. Urinary insulin excretion
rate: an index of free insulinaemia in insulin-dependent
diabetics. Diabetic Medicine 1984;1(4):291–4.
Pickup 1985 {published data only}
Pickup JC, Sherwin RS, Tamborlane WV, Rizza RA, Service
FJ. Conference on insulin pump therapy in diabetes.
Multicenter study of effect on microvascular disease. The
pump life. Patient responses and clinical and technological
problems. Diabetes 1985;34 Suppl 3:37–41.
Pickup 1989 {published data only}
Pickup JC, Collins AC, Walker JD, Viberti GC, Pasic J.
Patterns of hyperinsulinaemia in type 1 diabetic patients
28Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

with and without nephropathy. Diabetic Medicine 1989;6
(8):685–91.
Pietri 1980 {published data only}
Pietri A, Dunn FL, Raskin P. The effect of improved diabetic
control on plasma lipid and lipoprotein levels: a comparison
of conventional therapy and continuous subcutaneous
insulin infusion. Diabetes 1980;29(12):1001–5.
Pietri 1983 {published data only}
Pietri AO, Dunn FL, Grundy SM, Raskin P. The effect
of continuous subcutaneous insulin infusion on very-
low-density lipoprotein triglyceride metabolism in type I
diabetes mellitus. Diabetes 1983;32(1):75–81.
Reeves 1982 {published data only}
Reeves ML, Seigler DE, Ryan EA, Skyler JS. Glycemic
control in insulin-dependent diabetes mellitus. Comparison
of outpatient intensified conventional therapy with
continuous subcutaneous insulin infusion. American
Journal of Medicine 1982;72(4):673–80.
Regal 1988 {published data only}
Regal H, Koivisto VA, Maury CP, Irsigler K. No sign of
amyloidosis in pump-treated diabetics. Diabetes Research1988;8(4):195–9.
Rizza 1980 {published data only}
Rizza RA, Gerich JE, Haymond MW, Westland RE, Hall
LD, Clemens AH, et al.Control of blood sugar in insulin-
dependent diabetes: comparison of an artificial endocrine
pancreas, continuous subcutaneous insulin infusion, and
intensified conventional insulin therapy. New EnglandJournal of Medicine 1980;303(23):1313–8.
Rodger 1985 {published data only}
Rodger NW, Dupre J, Canny CLB. Continuous
subcutaneous insulin infusion in adults: Glycemic
advantage is predicted by venous plasma C-peptide
concentrations. Diabetes Care 1985;8(5):447–55.
Rodger 1988 {published data only}
Rodger NW, Behme MT, Dupre J, Chamberlain MJ.
Metabolic effects of continuous subcutaneous insulin
infusion: evidence that a rise and fall of portal vein
insulin concentration with each major meal facilitates
post-absorptive glycemic control. Clinical & InvestigativeMedicine - Medecine Clinique et Experimentale 1988;11(3):
167–86.
Saibene 1981 {published data only}
Saibene V, Melandri M, Brembilla L, Spotti D, Pozza
G. Comparison between multi-injection and continuous
subcutaneous insulin therapy in insulin-dependent diabetic
inpatients. Acta Diabetologica Latina 1981;18(1):45–50.
Schaepelynck-Belicar 2003 {published data only}
Schaepelynck-Belicar P, Vague P, Simonin G, Lassmann-
Vague V. Improved metabolic control in diabetic adolescents
using the continuous glucose monitoring system (CGMS).
Diabetes & Metabolism 2003;29(6):608–12.
Schiffrin 1982 {published data only}
Schiffrin A, Belmonte M. Multiple daily self-glucose
monitoring: its essential role in long-term glucose control
in insulin-dependent diabetic patients treated with pump
and multiple subcutaneous injections. Diabetes Care 1982;
5(5):479–84.
Schiffrin 1982a {published data only}
Schiffrin A, Belmonte MM. Comparison between
continuous subcutaneous insulin infusion and multiple
injections of insulin. A one-year prospective study. Diabetes
1982;31(3):255–64.
Schiffrin 1983 {published data only}
Schiffrin A, Desrosiers M, Moffatt M, Belmonte MM.
Feasibility of strict diabetes control in insulin-dependent
diabetic adolescents. Journal of Pediatrics 1983;103(4):
522–7.
Schiffrin 1984 {published data only}
Schiffrin A, Parikh S, Marliss EB, Desrosiers MM.
Metabolic response to fasting exercise in adolescent insulin-
dependent diabetic subjects treated with continuous
subcutaneous insulin infusion and intensive conventional
therapy. Diabetes Care 1984;7(3):255–60.
Schiffrin 1984a {published data only}
Schiffrin AD, Desrosiers M, Aleyassine H, Belmonte MM.
Intensified insulin therapy in the type I diabetic adolescent:
a controlled trial. Diabetes Care 1984;7(2):107–13.
Schiffrin 1985 {published data only}
Schiffrin A, Parikh S. Accommodating planned exercise in
type I diabetic patients on intensive treatment. Diabetes
Care 1985;8(4):337–42.
Schiffrin 1987 {published data only}
Schiffrin A, Suissa S. Predicting nocturnal hypoglycemia
in patients with type I diabetes treated with continuous
subcutaneous insulin infusion. American Journal of Medicine1987;82(6):1127–32.
Schmitz 1987 {published data only}
Schmitz O, Sorensen SS, Alberti KG, Orskov H, Hansen
HE. Metabolic control in newly kidney transplanted
insulin-dependent diabetics: improvement by insulin pump
treatment (CSII). Journal of Diabetic Complications 1987;1
(3):81–6.
Schottenfeld-Naor 1985 {published data only}
Schottenfeld-Naor Y, Galatzer A, Karp M, Josefsberg Z,
Laron Z. Comparison of metabolic and psychological
parameters during continuous subcutaneous insulin
infusion and intensified conventional insulin treatment in
type I diabetic patients. Israel Journal of Medical Sciences1985;21(10):822–8.
Scuffham 2003 {published data only}
Scuffham P, Carr L. The cost-effectiveness of continuous
subcutaneous insulin infusion compared with multiple daily
injections for the management of diabetes.[see comment].
Diabetic Medicine 2003;20(7):586–93.
Service 1985 {published data only}
Service FJ, Rizza RA, Daube JR, O’Brien PC, Dyck PJ.
Near normoglycaemia improved nerve conduction and
vibration sensation in diabetic neuropathy. Diabetologia
1985;28(10):722–7.
29Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Siebenhofer 2004 {published data only}
Siebenhofer A, Plank J, Berghold A, Horvath K, Sawicki
PT, Beck P, et al.Meta-analysis of short-acting insulin
analogues in adult patients with type 1 diabetes: continuous
subcutaneous insulin infusion versus injection therapy.
Diabetologia 2004;47(11):1895–905.
Simonson 1985 {published data only}
Simonson DC, Tamborlane WV, Sherwin RS, Smith JD,
DeFronzo RA. Improved insulin sensitivity in patients with
type I diabetes mellitus after CSII. Diabetes 1985;34 Suppl
3:80–6.
Skare 1986 {published data only}
Skare S, Dahl-Jorgensen K, Kriz V, Hanssen KF. Plasma
somatostatin and plasma glucagon in long-term IDDM
without residual B-cell function. No effect of different long-
term metabolic control. Scandinavian Journal of Clinical &
Laboratory Investigation 1986;46(7):635–8.
Skyler 1982 {published data only}
Skyler JS, Seigler DE, Reeves ML. A comparison of insulin
regimens in insulin-dependent diabetes mellitus. DiabetesCare 1982;5 Suppl 1:11–8.
Sleightholm 1986 {published data only}
Sleightholm MA, Gallimore R, Tennent GA. Continuous
subcutaneous insulin infusion does not provoke significant
acute-phase response. Diabetes Care 1986;9(1):50–2.
Slijper 1990 {published data only}
Slijper FME, De Beaufort CE, Bruining GJ, De Visser JJ,
Aarsen RSR, Kicken DAM, et al.Psychological impact of
continuous subcutaneous insulin infusion pump therapy in
non-selected newly diagnosed insulin dependent (type 1)
diabetic children: Evaluation after two years of therapy.
Diabete et Metabolisme 1990;16(4):273–7.
Steno 1982 {published data only}
Steno. Effect of 6 months of strict metabolic control on eye
and kidney function in insulin-dependent diabetics with
background retinopathy. Steno study group. Lancet 1982;1
(8264):121–4.
Sulli 2003 {published data only}
Sulli N, Shashaj B. Continuous subcutaneous insulin
infusion in children and adolescents with diabetes mellitus:
decreased HbA1c with low risk of hypoglycemia. Journal of
Pediatric Endocrinology 2003;16(3):393–9.
Tamborlane 1979 {published data only}
Tamborlane WV, Sherwin RS, Genel M, Felig P. Reduction
to normal of plasma glucose in juvenile diabetes by
subcutaneous administration of insulin with a portable
infusion pump. New England Journal of Medicine 1979;300
(11):573–8.
Tamborlane 1979a {published data only}
Tamborlane WV, Sherwin RS, Genel M, Felig P. Restoration
of normal lipid and aminoacid metabolism in diabetic
patients treated with a portable insulin-infusion pump.
Lancet 1979;1(8129):1258–61.
Tamborlane 1981 {published data only}
Tamborlane WV, Hintz RL, Bergman M, Genel M, Felig P,
Sherwin RS. Insulin-infusion-pump treatment of diabetes:
influence of improved metabolic control on plasma
somatomedin levels. New England Journal of Medicine1981;305(6):303–7.
Tamborlane 1982 {published data only}
Tamborlane WV, Puklin JE, Bergman M, Verdonk C,
Rudolf MC, Felig P, et al.Long-term improvement of
metabolic control with the insulin pump does not reverse
diabetic microangiopathy. Diabetes Care 1982;5 Suppl 1:
58–64.
Testa 1985 {published data only}
Testa MA, Puklin JE, Sherwin RS, Simonson DC. Clinical
predictors of retinopathy and its progression in patients
with type I diabetes during CSII or conventional insulin
treatment. Diabetes 1985;34 Suppl 3:61–8.
Thuesen 1986 {published data only}
Thuesen L, Christiansen JS, Sorensen KE, Falstie-Jensen N,
Christensen CK, Hermansen K, et al.Exercise capacity and
cardiac function in type 1 diabetic patients treated with
continuous subcutaneous insulin infusion. A controlled
study. Scandinavian Journal of Clinical & Laboratory
Investigation 1986;46(8):779–84.
Tilvis 1986 {published data only}
Tilvis RS, Helve E, Miettinen TA. Improvement of diabetic
control by continuous subcutaneous insulin infusion
therapy changes fatty acid composition of serum lipids
and erythrocytes in type 1 (insulin-dependent) diabetes.
Diabetologia 1986;29(10):690–4.
Toni 2004 {published data only}
Toni S, Reali MF, Fasulo A, Festini P, Medici A,
Martinucci ME. The use of insulin pumps improves the
metabolic control in children and adolescents with type 1
diabetes.[comment][erratum appears in Arch Dis Child.
2004 Oct;89(10):985 Note: Festini, F [corrected to Festini,
P]]. Archives of Disease in Childhood 2004;89(8):796–7.
Turk 1996 {published data only}
Turk Z, Flego I, Kerum G. Platelet aggregation in type 1
diabetes without microvascular disease during continuous
subcutaneous insulin infusion. Hormone & MetabolicResearch 1996;28(2):95–100.
van Ballegooie 1985 {published data only}
van Ballegooie E, de Jong PE, Donker AJ, Sluiter WJ.
The effect of continuous subcutaneous insulin infusion
on renal function in type I diabetic patients with and
without proteinuria. Proceedings of the European Dialysis &Transplant Association - European Renal Association 1985;21:
722–4.
Viberti 1981 {published data only}
Viberti G, Pickup JC, Bilous RW, Keen H, Mackintosh
D. Correction of exercise-induced microalbuminuria in
insulin-dependent diabetics after 3 weeks of subcutaneous
insulin infusion. Diabetes 1981;30(10):818–23.
Viberti 1984 {published data only}
Viberti GC, Home PD, Bilous RW, Alberti KG, Dalton
N, Keen H, et al.Metabolic effects of physical exercise
in insulin-dependent diabetics controlled by continuous
30Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

subcutaneous insulin infusion or conventional injection
therapy. Acta Endocrinologica 1984;105(4):515–20.
Warmolts 1987 {published data only}
Warmolts JR, Mendell JR, O’Dorisio TM, Cataland S.
Comparison of the effects of continuous subcutaneous
infusion and split-mixed injection of insulin on nerve
function in type I diabetes mellitus. Journal of the
Neurological Sciences 1987;82(1-3):161–9.
Weinzimer 2004 {published data only}
Weinzimer SA, Ahern JH, Doyle EA, Vincent MR, Dziura
J, Steffen AT, et al.Persistence of benefits of continuous
subcutaneous insulin infusion in very young children with
type 1 diabetes: a follow-up report. Pediatrics 2004;114(6):
1601–5.
Willi 2003 {published data only}
Willi SM, Planton J, Egede L, Schwarz S. Benefits of
continuous subcutaneous insulin infusion in children with
type 1 diabetes. Journal of Pediatrics 2003;143(6):796–801.
Wilson 2005 {published data only}
Wilson DM, Buckingham BA, Kunselman EL, Sullivan
MM, Paguntalan HU, Gitelman SE. A two-center
randomized controlled feasibility trial of insulin pump
therapy in young children with diabetes. Diabetes Care
2005;28(1):15–9.
Wredling 1997 {published data only}
Wredling R, Hannerz L, Johansson U. Variability of
blood glucose levels in patients treated with continuous
subcutaneous insulin infusion: a pilot study. Practical
Diabetes International 1997;14(1):5–8.
Yki-Jarvinen 1984 {published data only}
Yki-Jarvinen H, Koivisto VA. Continuous subcutaneous
insulin infusion therapy decreases insulin resistance in type
1 diabetes. Journal of Clinical Endocrinology & Metabolism1984;58(4):659–66.
Ziegler 1988 {published data only}
Ziegler D, Wiefels K, Dannehl K, Gries FA. Effects of one
year of near-normoglycemia on peripheral nerve function
in type 1 (insulin-dependent) diabetic patients. KlinischeWochenschrift 1988;66(9):388–96.
Additional references
ADA 1997
American Diabetes Association. Report of the Expert
Committee on the Diagnosis and Classification of Diabetes
Mellitus. Diabetes Care 1997;20(7):1183–97.
APEG 2004
Australian Paediatric Endocrine Group. Clinical Practise
Guidelines: Type 1 Diabetes in Children and Adolescents.
www.chw.edu.au/prof/services/endocrinology/apeg
www.chw.edu.au/prof/services/endocrinology/apeg http://
www.chw.edu.au/prof/services/endocrinology/apeg/ 2004.
Couper 2002
Couper JJ. Children with type 1 diabetes: where are we at?.
The Medical Journal of Australia 2002;177(5):228–9.
Dabelea 2009
Dabelea D. The accelerating epidemic of childhood
diabetes. The Lancet 2009;373(9680):1999–2000.
DPT 2002
Diabetes Prevention Trial-Type 1 Diabetes Study Group.
Effects of insulin in relatives of patients with type 1 diabetes
mellitus. New England Journal of Medicine 2002;346(22):
1685–91.
ENDIT 2003
The European Nicotinamide Diabetes Intervention Trial
(ENDIT) Group. Intervening before the onset of Type 1
diabetes: baseline data from the European Nicotinamide
Diabetes Intervention Trial (ENDIT). Diabetologia 2003;
46(3):339–46.
Guinn 1988
Guinn TS, Bailey GJ, Mecklenberg RS. Factors related
to discontinuation of continuous subcutaneous insulin-
infusion therapy. Diabetes Care 1988;11(1):46–51.
Higgins 2003
Higgins JP, Thompson SG, Deeks JJ, Altman DG.
Measuring inconsistency in meta-analyses. British Medical
Journal 2003;327(7414):557–60.
Higgins 2008
Higgins JPT, Green S (editors). Cochrane Handbook for
Systematic Reviews of Interventions Version 5.0.1 [updated
September 2008]. The Cochrane Collaboration. Available
from www.cochrane-handbook.org. WileyBlackwell, 2008.
HTA 2004
Colquitt JL, Green C, Sidhu MK, Hartwell D, Waugh N.
Clinical and cost-effectiveness of continuous subcutaneous
insulin infusion for diabetes. Health Technology Assessment
2004; Vol. 8, issue number 43.
Karvonen 2000
Karvonen M, Viik-Kajander M, Moltchanova E, Libman
I, LaPorte R, Tuomilehto J. Incidence of childhood type 1
diabetes worldwide. Diabetes Mondiale (DiaMond) Project
Group. Diabetes Care 2000;23(10):1516–26.
Liberati 2009
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC,
Ioannidis JPA, et al.The PRISMA Statement for Reporting
Systematic and Meta-Analyses of Studies That Evaluate
Interventions: Explanation and Elaboration. PLoS Med
1999;6(7):1–28. [DOI: 10.1371/journal.pmed.1000100]
NDDG 1979
National Diabetes Data Group. Classification and diagnosis
of diabetes mellitus and other categories of glucose
intolerance. Diabetes 1979;28(12):1039–57.
NICE 2008
National Institute for Health and Clinical Excellence
(NICE). Continuous subcutaneous insulin infusion for the
treatment of diabetes mellitus. London (UK): National
Institute for Health and Clinical Excellence (NICE);
Technology appraisal guidance no. 151 2008 July.
31Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Pickup 1980a
Pickup JC. A new approach to improved metabolic control
in diabetics: Continuous subcutaneous insulin infusion.
American Heart Journal 1980;100(4):417–20.
Pickup 2002
Pickup J, Mattock M, Kerry S. Glycaemic control with
continuous subcutaneous insulin infusion compared with
intensive injections in patients with type 1 diabetes: meta-
analysis of randomised controlled trials. British MedicalJournal 2002;324:1–6.
Sterne 2001
Sterne JAC, Egger M, Davey Smith G. Investigating and
dealing with publication and other biases.. British Medical
Journal 2001;323:101–105.
Sutton 1990
Sutton L, Plant AJ, Lyle DM. Services and cost of
hospitalization for children and adolescents with insulin-
dependent diabetes mellitus in New South Wales. The
Medical Journal of Australia 1990;152(3):130–6.
WHO 1980
World Health Organisation. WHO Expert Committee
on Diabetes Mellitus: second report. World Health
Organization Technical Report Series 1980;646:1–80.∗ Indicates the major publication for the study
32Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Bak 1987 and Husted 1989
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Cross-over
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 20 participants were randomised in this study. Half of the
participants were randomised to CSII and the other half were randomised to MI. After
six months they were crossed over, serving as their own control. In total, 16 participants
completed CSII and 20 completed MI
SEX (female% / male%): 1 female (6%), 15 males (94%)
AGE (mean years (SD)): 24 (2) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean (SD)): 70 (45) months
INCLUSION CRITERIA: IDDM of more than 2.5 years and diagnosed before age
30, no sign of nephropathy, hypertension or advanced retinopathy (ie. normal value of
serum creatinine), absence of albuminuria (ie. Albustic negative urine), diastolic blood
pressure below 95 mmHg, absence of cataract, retinal proliferations, haemorrhages or
exudates and less than 5 microaneurysms in the retina
EXCLUSION CRITERIA: Not reported
DIAGNOSTIC CRITERIA: WHO 1980
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: Denmark
SETTING: Out-patient, however transition phases to CSII or MI were made during
hospitalisation
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY):100 U/ml regular insulin (Ac-
trapid HM) was delivered by a Graseby MS 36 insulin infuser with a 25 G butterfly
needle placed in the anterior abdominal wall. About half of the total daily dose was
delivered as a basal infusion and the other half as bolus injections, 30 minutes before
meals
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): About 30% of the total daily dose
was delivered as intermediate acting NPH insulin (40 U/ml insulin protaphan HM)
in the thigh late at night. Short-acting insulin was delivered by a pen injector with a
disposable cartridge of 1.5 ml of short acting insulin (100 U/ml insulin actrapid HM).
Bolus injections were delivered in the abdominal wall 30 minutes before breakfast, lunch
and dinner
TREATMENT BEFORE STUDY: All of the participants were treated (as out-patients)
with intermediate-acting insulin alone or in combination with short-acting insulin once
or twice a day
TITRATION PERIOD: Not reported
33Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bak 1987 and Husted 1989 (Continued)
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES:
Bak 1987 - metabolic regulation (mean diurnal blood glucose, serum fructosamine,
fasting plasma ketone bodies, FFA, HGH and glucagon), weight, estimation of blood
glucose instability, patient’s evaluation (questionnaire)
Husted 1998 - metabolic regulation (mean diurnal blood glucose, serum fructosamine),
weight, coagulation and platelet function (platelet aggregation, serum and plasma throm-
boxane B2, plasma antithrombin III activity, plasma von Willebrand factor antigen)
Study details DURATION OF INTERVENTION: 6 months
DURATION OF FOLLOW-UP: 12 months
RUN-IN PERIOD: Duration not reported. All of the participants were treated (as out-
patients) with intermediate-acting insulin alone or in combination with short-acting
insulin once or twice a day
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: No
NON-COMMERCIAL FUNDING: Yes
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study Bak 1987 - “We therefore made a cross-over study in order to compare 6 months of
CSII therapy with 6 months of MII by evaluating metabolic control, insulin needs, and
patient acceptability.”
Husted 1998 - “The aim of the present study with cross-over design was to compare 6
months of CSII therapy with 6 months of MII by evaluating metabolic control, platelet
aggregability, thromboxane B2 levels in serum and plasma as well as ATIII activity and
von Willebrand factor antigen.”
Notes Standard deviations of the difference were extracted from paired t-test data
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Details not provided.
Allocation concealment? Unclear risk Details not provided.
Blinding?
All outcomes
High risk Not applicable for patient blinding, but
outcome assessor blinding not reported
Incomplete outcome data addressed?
All outcomes
Low risk Withdrawals, drop outs, and losses to fol-
low up were described. 4 drop-outs (20%)
Free of selective reporting? Unclear risk Details not provided.
34Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bak 1987 and Husted 1989 (Continued)
Free of other bias? Unclear risk Compliance was not reported.
Botta 1986
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Parallel
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 10 participants were included in this study, all were pregnant
females. 5 were randomised to, and completed CSII and another 5 females were ran-
domised to, and completed MI
SEX (female% / male%): 100% female
AGE (mean years (SD)): The mean age of the participants receiving CSII was 27.8 (6.
18) years and the mean age of the participants receiving MI was 25.4 (5.36) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): The mean disease duration for the
participants receiving CSII was 8.2 (8.04) years and in those receiving MI, the mean
disease duration was 9.4 (9.4) years
INCLUSION CRITERIA: Not reported
EXCLUSION CRITERIA: Not reported
DIAGNOSTIC CRITERIA: Not reported
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: Italy
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): The Micropump CPI 9100
Lilly was used to attempt to maintain the glycaemic values between 90 mg/dl and 130
mg/dl during the course of the day
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Glycaemic values were main-
tained between 90 mg/dl and 130 mg/dl during the course of the day. Rapid MC insulin
was delivered before breakfast, lunch and dinner, with the addition of intermediate in-
sulin MC with lunch and dinner. Participants were instructed to modify the dosage of
rapid insulin by two units if on the preceding day glycaemia (two hours before the meal)
was higher than 150 mg/dl or lower than 90 mg/dl
TREATMENT BEFORE STUDY: Not reported
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: fetal weight index, fasting and post-prandial glycemia,
ketonuria, hypoglycemia and pregnancy related outcomes
35Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Botta 1986 (Continued)
Study details DURATION OF INTERVENTION: 24.68 weeks for CSII and 28.80 weeks for MI
DURATION OF FOLLOW-UP: 24.68 weeks for CSII and 28.80 weeks for MI
RUN-IN PERIOD: Not reported
Publication details LANGUAGE OF PUBLICATION: Italian
COMMERCIAL FUNDING: Not reported
NON-COMMERCIAL FUNDING: Not reported
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “Considerando il particolare atteggiamento emotivo della donna diabetica nei confronti
della sua condizione patologica durante la gravidanza abbiamo tentato di valutare se
l’applicazione del microinfusore nelle donne gravide con diabete mellito di tipo I possa
determinare una maggiore compliance alla terapia ed all’autocontrollo rispetto alla ter-
apia insulinica tradizionale e ci possa consentire di ottenere dei risultati migliori nel
trattamento della gravidanza diabetica.”
Translated: Considering the detail emotional attitude of the diabetic woman regarding its
pathological condition during the pregnancy we have tried to estimate if application of
the microinfusore in the pregnant women with mellito diabetes can determine a greater
compliance to the therapy and self-control regarding the traditional insulinica therapy
and can concur to obtain to us of the better result in the treatment of the diabetic
pregnancy
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Details not provided.
Allocation concealment? Unclear risk Details not provided.
Blinding?
All outcomes
High risk Not applicable for patient blinding, but
outcome assesor blinding not reported
Incomplete outcome data addressed?
All outcomes
High risk Number and reasons of drop-outs, with-
drawals, and losses to follow up were not
reported
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was not reported.
36Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bruttomesso 2008
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Cross-over
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 42 participants were included in this study. All participants
were already on CSII treatment. 24 participants were randomised to continue with CSII
and 18 participants were randomised to start MI for four months, after which the groups
crossed over, serving as their own control
SEX (female% / male%): The final sample comprised 20 female (51%), 19 male (49%)
AGE (mean years (SD)): 38.1 (9.3) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): 16.6 (8.2) years
INCLUSION CRITERIA: Willingness to measure blood glucose frequently and profi-
ciency in adjusting insulin administration according to blood glucose values and carbo-
hydrate intake
EXCLUSION CRITERIA: Individuals with insulin allergy, untreated retinopathy, car-
diovascular disease, hepatic or renal insufficiency, drug abuse or life-threatening diseases,
women who were pregnant or lactating or intending to become pregnant were excluded
DIAGNOSTIC CRITERIA: Not reported
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 4
COUNTRY/ LOCATION: Italy
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Insulin lispro was infused and
adjusted according to the following targets: 5.0 mmol/L in the morning and before
meals, 6.0 to 8.5 mmol/L 90 minutes after meals and 6.1 to 7.5 mmol/L at bed time
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Insulin lispro was delivered at
meals and adjusted according to the following targets: 5.0 mmol/L in the morning and
before meals, 6.0 to 8.5 mmol/L 90 minutes after meals and 6.1 to 7.5 mmol/L at bed
time. Participants with less than optimal glycemic control with one glargine injection
were instructed to take twice daily glargine or extra injections of insulin lispro
TREATMENT BEFORE STUDY: All participants were treated by CSII with lispro or
aspart
TITRATION PERIOD: Four weeks - all participants using lispro continued, but two
participants changed from aspart to lispro
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): blood glucose variability
SECONDARY OUTCOMES (as stated in the publication): blood glucose concentra-
tions, number and severity of hypo/hyperglycemic episodes, number of episodes of ke-
toacidosis, insulin requirement, body weight, HbA1c, lipid profile, serum FFA and hGH,
and treatment satisfaction
ADDITIONAL OUTCOMES: NA
37Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Bruttomesso 2008 (Continued)
Study details DURATION OF INTERVENTION: 4 months
DURATION OF FOLLOW-UP: 9 months
RUN-IN PERIOD: For four weeks basal insulin infusion rate and meal-related boluses
were optimised as much as possible, while avoiding hypoglycaemia and hyperglycemia.
The target blood glucose for the trial was 5.0 mmol/L in the morning and before meals,
6.0 to 8.5 mmol/L 90 minutes after meals and 6.1 to 7.5 mmol/L at bed time
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: Yes - Disetronic Medical System AG (one of the study
investigators was a full time employee and another was funded to attend conferences)
NON-COMMERCIAL FUNDING: No
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “The superiority of continuous subcutaneous insulin infusion (CSII) over multiple daily
injections (MDI) with glargine is uncertain. In this randomized cross-over study, we
compared CSII and MDI with glargine in patients with Type 1 diabetes well controlled
with CSII. The primary endpoint was glucose variability.”
Notes Standard deviations of the difference were extracted from paired t-test data
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk Participants were randomised by Dis-
etronic Medical Systems AG (Burgdorf,
Switzerland) and treatment assignment was
determined with random lists for each cen-
tre
Allocation concealment? Low risk Participants and investigators were blinded
to the treatment sequence up to randomi-
sation
Blinding?
All outcomes
High risk Not applicable to patient blinding, but out-
come assessor blinding is not reported
Incomplete outcome data addressed?
All outcomes
Low risk Drop outs described.
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance not reported.
38Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Chiasson 1984 and 1985
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Cross-over
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTCIPATED: 12 participants were included in this study. Half of the partic-
ipants were randomised to start with CSII and the other half were randomised to start
with MI. After three months they were crossed over
SEX (female% / male%): 7 female (58%), 5 male (42%)
AGE (mean years (SD)): 26.8 (6.4) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): 15.3 (7.3) years
INCLUSION CRITERIA: Not reported
EXCLUSION CRITERIA: Not reported
DIAGNOSTIC CRITERIA: Not reported
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: Canada
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Using the Mill-HIll Infuser
(Muirhead Medical Products Ltd, London, England) and on the basis of previous study
results, initial basal rate was set at 50% of the previous insulin dose and was delivered
as a continuous infusion of regular insulin. The boluses were delivered 20 minutes
before meals as regular insulin according to the following initial schedules: 2.7 U/20g
carbohydrates before breakfast and 1.8 U/20g carbohydrates before other meals and
snacks containing more than 20g carbohydrates. The target blood glucose was 70 to 120
mg/dl before meals and <150 mg/dl 1hr after meals. All blood glucose <50 mg/dl and
>180 mg/dl were undesirable. Basal rate was increased or decreased by 1 U/24h if fasting
blood glucose was >120 mg/dl or <70 mg/dl. The boluses were increased or decreased by
0.2 U/20g carbohydrates if one hour after meal blood glucose was >150 mg/dl or below
the before meal blood glucose. Participants on CSII were also instructed to add 2 U of
regular insulin to boluses for every 100 mg/dl above blood glucose target
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Using the Medi-Jector (Derata
Corporation, Minneapolis, Minnesota) and on basis of previous study results, initial
basal rate was set at 50% of the previous insulin dose and was delivered as ultralente at 22
hours. The boluses were delivered 20 minutes before meals as regular insulin according
to the schedules described above
TREATMENT BEFORE STUDY: Not reported
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: metabolic regulation (capillary blood glucose, glyco-
suria, glycated haemoglobin), nerve conductivity, proteinuria & required insulin dose to
maintain blood glucose
39Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Chiasson 1984 and 1985 (Continued)
Study details DURATION OF INTERVENTION: 3 months
DURATION OF FOLLOW-UP: 6 months
RUN-IN PERIOD: All of the participants were admitted to the unit at the hospital to
initiate either treatment and learn how to operate the (CSII) pump or (MI) medijector,
how to calculate carbohydrates and how to modify insulin dose according to prespecified
algorithms/schedules
Publication details LANGUAGE OF PUBLICATION: English & French
COMMERCIAL FUNDING: No
NON-COMMERCIAL FUNDING: Yes - medical research councils, NIH etc
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “The present study was designed to compare continuous subcutaneous insulin infusion
(CSII) using the Mill-Hill Infuser (Muirhead Medical Products Ltd, London, England)
with multiple injections using the Medi-Jector (Derata Corporation, Minneapolis, Min-
nesota) in the treatment of insulin dependent diabetes mellitus (IDDM) and to assess
the effect of glucose control on diabetes late complications.”
Notes Standard deviations of the difference were extracted from paired t-test data
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Details not provided.
Allocation concealment? Unclear risk Details not provided.
Blinding?
All outcomes
High risk Not applicable to patient blinding, but out-
come assessor blinding is not reported
Incomplete outcome data addressed?
All outcomes
High risk Number and reasons of drop-outs, with-
drawals, and losses to follow up were not
reported
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was measured and checked by
going over the participant’s notebook at
each visit
40Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Cohen 2003
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Cross-over
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 16 participants were included in this study. The participants
were divided into two groups, one group was randomised to CSII and the other group
was randomised to MI. After six months they were crossed over, serving as their own
control. 12 participants completed the study
SEX (female% / male%): 10 female (63%), 6 male (37%)
AGE (mean years (SD)): Mean was not reported. The median age of all participants was
14.2 years (range 14.5-17.9)
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): Mean was not reported. At least two
years
INCLUSION CRITERIA: Type 1 diabetes mellitus of at least two years, low c-peptide
secretion (<0.6 ng/ml), and no other chronic disease that could interfere with treatment
EXCLUSION CRITERIA: Participants unable to detect hypoglycemia or who had
evidence of microvascular complications or other clinically significant disorders
DIAGNOSTIC CRITERIA: Not reported
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: Israel
SETTING: Out-patient (ambulatory)
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Tayco, Disetronic (Burgdorf,
Switzerland) pump with short acting analog insulin (Humalog, Eli Lily)
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Four daily injections of a com-
bination of NPH and regular insulin before breakfast, regular insulin only before lunch
and dinner, and NPH only at bed time
TREATMENT BEFORE STUDY: Not reported
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: Body mass index, body mass index standard deviation
score for age, HbA1c, frucosamine, daily insulin dose, hypo- and hyper- glycemic events,
diabetic ketoacidosis, Diabetes Treatment Satisfaction Questionnaire (DTSQ) and the
Diabetes Quality of Life Questionnaire for Youth (DQOLY)
Study details DURATION OF INTERVENTION: 6 months
DURATION OF FOLLOW-UP: 12 months
RUN-IN PERIOD: Not reported
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: Yes - Tayco Diagnostica
41Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Cohen 2003 (Continued)
NON-COMMERCIAL FUNDING: No
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “We designed an open randomized crossover trial to compare CSII with MDI for
glycemic control, dose requirements, weight change, incidence of adverse events, quality
of life and satisfaction in adolescents. ”
Notes This cross-over study was not adequately analysed, and did not report correlations be-
tween baseline and end of study data, ignoring within-person variation. Therefore, stan-
dard deviations of the difference were derived assuming different correlation coefficients
(0.3, 0.5, 0.7, 0.9) and the largest standard deviation of the differences was derived from
cross-over studies with adequate statistical methodology
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Details not provided.
Allocation concealment? Unclear risk Details not provided.
Blinding?
All outcomes
High risk Not applicable in patient blinding, but out-
come assessor blinding not reported
Incomplete outcome data addressed?
All outcomes
Low risk Withdrawals, drop outs, and losses to fol-
low up were described - three were satisfied
with pump and so didn’t want to start MI,
one who started with MI refused to connect
to pump. There was 0.25% withdrawals/
dropouts/losses to follow up
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was not reported.
42Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

DeVries 2002
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Parallel
It is important to note that at the design phase, the study investigators anticipated the possibilitythat they would have to analyse the study as a parallel RCT (rather than a cross-over) becauseof the demanding nature of the protocol and an expected high drop out rate. However, atthe point of cross-over, there had been no drop outs so the study investigators continued witha cross-over design and stopped inclusion at 79 participants (48 participants per arm werecalcluated to be required to have an 80% chance of detecting a 0.75% difference in HbA1cwith an assumed SD of 1.3%). Finally, the study investigators decided that due to the dropout rate after cross-over, they would analyse the data as a parallel study using only pre cross-over data.CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 79 participants were included in this study. 39 participants
were randomised to start with CSII and 40 participants were randomised to start with
MI. 32 participants completed CSII in the first stage and all 40 participants completed
MI (data from these participants is analysed)
SEX (female% / male%): 37 female (47%), 42 male (53%)
AGE (mean years (SD)): The mean age of participants in the group starting with CSII
was 36.2 (10.3) and the mean age of the participants starting with MI was 37.3 (10.6)
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): The mean disease duration in the group
staring with CSII was 17.6 (9.8) years and the mean disease duration in the group staring
with MI was 18.0 (9.4) years
INCLUSION CRITERIA: Type 1 diabetes, age between 18 and 70 years, persistent
poor control while on three or more insulin injections a day (defined as mean of all
HbA1c values measured ≥ 8.5% in the last six months before the study)
EXCLUSION CRITERIA: Severe active retinopathy (requiring laser therapy), impaired
hepatic function (alkaline phosphatase or alanine aminotransferase at least two times the
upper limit or normal), nephropathy (defined as serum creatinine > 150 µmol/L), insulin
resistance (defined as the use of > 1.5 units insulin/kg body weight), substance abuse,
cardiac disease (decompensated heart failure NYHA III and IV, unstable angina pectoris,
or a myocardial infarction within the last 12 months), uncontrolled hypertension (blood
pressure ≥ 180/110 mmHg), insulin allergy, and past or current psychiatric treatment
for schizophrenia, mental disorder, or bipolar disorder. Women were excluded if they
were (or intending to become) pregnant or breastfeeding
DIAGNOSTIC CRITERIA: Defined as diabetes diagnosed at or before age 30 years
with a C-peptide level ≤ 0.20 nmol/L at a concomitant glucose level ≥ 7.0 mmol/L, or
diagnosed at or before age 40 with a C-peptide level ≤ 0.05 nmol/L at a concomitant
glucose level ≥ 7.0 mmol/L
CO-MORBIDITIES: 36 participants had retinopathy, 19 had microalbuminuria, 8 had
proteinuria and 10 had neuropathy
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 11
COUNTRY/ LOCATION: Netherlands
SETTING: Out-patient
43Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

DeVries 2002 (Continued)
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): The Disetronic H-TRONplus
insulin pump was used with insulin aspart. The starting dose was 90% of the previously
used total insulin dose per day or 80% when hypoglycaemia was a problem to the
participants. It was advised to start with one basal rate, or two at the most. The nighttime
rate then being 0.2 units/hour lower than the day time rate. Initially, 50% of the total
daily insulin dose was delivered as basal insulin, the rest equally divided before meals. The
meal time bolus insulin aspart was adjusted according to the postprandial measurements
and the basal rate was adjusted according to the preprandial measurements, targeting for
the same levels as the MI group
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY):An algorithm was given to adjust
insulin doses. 80% of the previously given before meal human insulin dose was delivered
as insulin aspart before meals and participants were advised to add the preprandial dose
increment to their night time NPH insulin dose, leaving the total daily insulin dose
unchanged. When the interval between two day time injections was greater than five
hours, additional NPH doses were added: 40% of the previously given premeal human
insulin was delivered as NHP insulin and 60% as insulin aspart for each interval exceeding
five hours. Insulin aspart was adjusted according to the postprandial measurement and
NPH was adjusted according to the preprandial measurements
TREATMENT BEFORE STUDY: Not reported
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Change in HbA1c in both
randomisation groups from baseline to 12 and 16 weeks (the mean of both)
SECONDARY OUTCOMES (as stated in the publication): Number of hypoglycemias,
means of blood glucose values at the nine points in the blood glucose profiles, SD of all
measurements in these profiles, and changes in dimensions of the quality-of-life measures
ADDITIONAL OUTCOMES: Insulin requirement, body weight.
Study details DURATION OF INTERVENTION: 16 weeks
DURATION OF FOLLOW-UP: 32 weeks
RUN-IN PERIOD: Qualification phase consisted of a short re-education and intensi-
fication of the frequency of out-patient clinic visits. At week two (of 14 weeks) a 30
minute re-education session was scheduled with the diabetes nurse specialist, which in-
cluded checking for possible deficits in insulin injection technique, self monitored blood
glucose, self-regulation of insulin dose in anticipation of physical activity and meals, and
in case of holidays and illness, actions to be taken in case of hypo- or hyperglycaemia,
storage or insulin and self monitoring strips, the advice to keep bedtime insulin dosage
constant, solely to be adjusted on consistent out-of-range glucose values at awakening,
and finally the advice to take additional carbohydrate in case of a glucose value <8 mmol/
L at bed time. There were five outpatient clinic visits during this phase. A minimum of
two self monitored blood glucose measurements per day were required and a minimum
of 70% of these had to be made to qualify for randomisation
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: Yes, but the study investigators stated that they were the
sole originators of the study protocol
NON-COMMERCIAL FUNDING: No
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
44Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
DeVries 2002 (Continued)
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “The primary objective was to compare the efficacy in improving glycemic control of
continuous subcutaneous insulin infusion and insulin injection therapy in diabetic pa-
tients in persistent poor control. The secondary objective was to investigate possible
different effects of these modes of treatment on health-related quality of life.”
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk The randomisation list was computer gen-
erated and permuted blocks of six were used
for each centre
Allocation concealment? Low risk Subjects were randomised with scratch la-
bels to each intervention, sequentially as-
signed to participants by the coordinating
center
Blinding?
All outcomes
High risk Not applicable for patient blinding but out-
come assessor blinding was not reported
Incomplete outcome data addressed?
All outcomes
Low risk Due to high drop out rate after cross-over,
only the first half of the study (pre cross-
over) was analysed as a parallel study
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was measured.
Doyle 2004
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Parallel
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTCIPATED: 32 participants were included in this study. 16 were randomised
to and completed CSII. 16 were randomised to MI and 15 completed MI
SEX (female% / male%): 18 female (56%), 14 male (44%)
AGE (mean years (SD)): The mean age of participants randomised to CSII was 12.5 (3.
2) years and the mean age of participants randomised to MI was 13 (2.8) years
ETHNIC GROUPS (%): There were 11 white (69%), 3 hispanic (19%) and 2 black
45Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Doyle 2004 (Continued)
(12%) participants in the CSII group and in the MI group there were 13 white (81%),
2 (13%) hispanic and 1 (6%) black participants
DURATION OF DISEASE (mean years (SD)): The mean disease duration in partic-
ipants randomised to CSII was 6.8 (3.8) years and in those randomised to MI, mean
disease duration was 5.6 (4.0) years
INCLUSION CRITERIA: Eight to 21 years of age, otherwise healthy except for treated
thyroid or celiac disease, treated with insulin for at least six months, naïve to CSII and
glargine, willing to do at least four blood tests per day and had a screening HbA1c
between 6.5% and 11%
EXCLUSION CRITERIA: Not reported
DIAGNOSTIC CRITERIA: Not reported
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: Connecticut, USA
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): The Medtronic MiniMed 508
or Paradigm 511 was used to deliver insulin aspart. The initital base dose was 50% of the
total daily insulin dose. Initial carbohydrate-to-insulin ratios and correction doses were
based on their prerandomisation insulin doses or on age and pubertal stage. Participants
were advised to use the prescribed carbohydrate-to-insulin ratio for all meals and snacks
that were ≥15 g carbohydrates. Participants were contacted daily in the first two weeks
for dosage adjustments. Blood glucose targets were 70 to120 mg/dl before meals and
90 to 150 mg/dl at bed time. Participants were instructed to treat two consecutive high
blood glucose levels as potential catheter occulsions, and were advised to change the site
and take a correction dose of aspart by injection
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): The initial dose of glargine was
calculated as 80% of their total daily insulin dose of NPH or lentre according to usual
practice guidelines with glargine. Initial carbohydrate-to-insulin ratios and correction
doses were based on their pre-randomisation insulin doses or on age and pubertal stage.
Particpants were advised to use the prescribed carbohydrate-to-insulin ratio for all meals
and snacks that were ≥15 g carbohydrates. Participants were contacted daily in the first
two weeks for dosage adjustments. Blood glucose targets were 70 to 120 mg/dl before
meals and 90 to 150 mg/dl at bed time. Glargine was given in the morning or at bed
time
TREATMENT BEFORE STUDY: Not reported
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: HbA1c, blood glucose, insulin dose, adverse events,
quality of life
Study details DURATION OF INTERVENTION: 16 weeks
DURATION OF FOLLOW-UP: 16 weeks
RUN-IN PERIOD: For a period of 1 to 2 weeks, participants were asked to do four finger
stick blood glucose tests per day, and instructed to keep written records of the blood
glucose levels. These were evaluated by the investigator, along with the participant’s ability
46Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Doyle 2004 (Continued)
to count carbohydrates. If further teaching was necessary, the participant met with the
dietician before the next visit. Participants were instructed on how to treat hypoglycemic
episodes with glucose tablets and were sent home with instructional aids such as videos
and written literature about CSII and MI therapy to review before randomisation
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: Yes - pharmaceutical and industry.
NON-COMMERCIAL FUNDING: Yes - government and foundations.
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “The present randomized clinical trial was undertaken with a principal aim of comparing
the efficacy of CSII and MDIs with glargine lin lowering HbA1c levels in youth with
type 1 diabetes in this short-tern study”
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk Participants stratified according to sex and
age, within each stratum, a randomisa-
tion scheme was generated using a random
number table with a block size of four. Con-
ducted by the centre’s Investigational Phar-
macy
Allocation concealment? Unclear risk Details not provided.
Blinding?
All outcomes
High risk Not applicable for patient blinding, but
outcome assessor blinding was not reported
Incomplete outcome data addressed?
All outcomes
Low risk Intention-to-treat analysis described. The
study investiagtors reported 3.10% drop-
outs/withdrawals/losses to follow up, rea-
sons for these were described
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was measured only in the first
1-2 week run in phase. Selection criteria
not reported
47Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hanaire-Broutin 2000
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Cross-over
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 41 participants were included in this study. 20 participants
were randomised to and completed CSII, and 21 participants were randomised to MI
but only 20 completed MI
SEX (female% / male%): 20 female, 21 male
AGE (mean years (SD)): 43.5 (10.3) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): 20 (11.3) years
INCLUSION CRITERIA: HbA1c < 10%, negative C-peptide, and experience of inten-
sified insulin therapy. None had untreated retinopathy, impaired renal function, gastric
neuropathy, BMI > 30 kg/m2, daily insulin dose > 2 U/kg, history of hypoglycaemia
unawareness, or any sever disease that could interfere with study
EXCLUSION CRITERIA: As above
DIAGNOSTIC CRITERIA: History of type 1 diabetes and C-peptide < 0.3 ng/ml or
negative Glucagon test
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: Toulouse, France
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): The MiniMed 506 or 507 and
Htron D or V was used to deliver lispro Humalog U-100 according to glycemic targets:
70 to 120 mg/dl two hours before meal or during fasting and 120 to 180 mg/dl two
hours after meal
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Three injections of lispro before
meals and two injections of NHP before breakfast and at bedtime. Lispro Humalog U-
100 was delivered according to glycemic targets: 70 to 120 mg/dl two hours before meal
or during fasting and 120 to 180 mg/dl two hours after meal. Participants were advised
to add a third injection of NPH at noon if before dinner blood glucose was not within
the target range
TREATMENT BEFORE STUDY: At enrolment, 32 participants were treated by CSII
with regular insulin and nine participants were treated by MI with regular insulin or
insulin lispro
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: Insulin dose, weight, HbA1c, glycemia, hypoglycaemia,
satisfaction
Study details DURATION OF INTERVENTION: 4 months
DURATION OF FOLLOW-UP: 8 months
RUN-IN PERIOD: Regardless of previous treatment all participants were submitted to
48Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
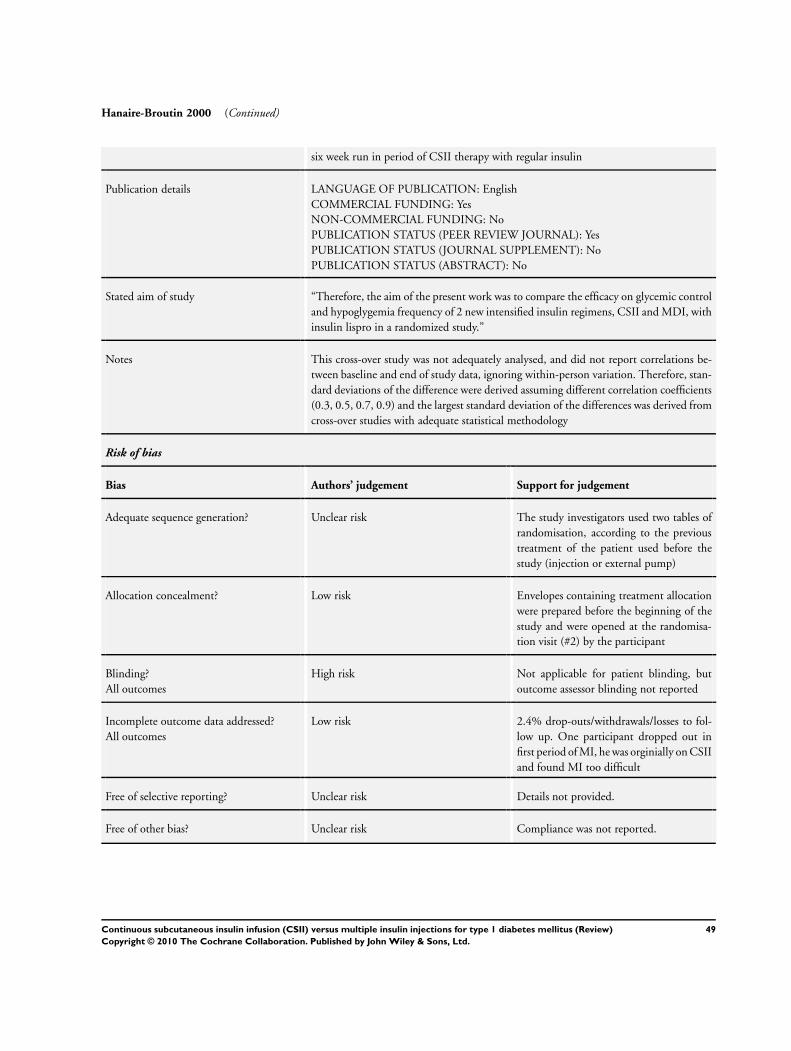
Hanaire-Broutin 2000 (Continued)
six week run in period of CSII therapy with regular insulin
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: Yes
NON-COMMERCIAL FUNDING: No
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “Therefore, the aim of the present work was to compare the efficacy on glycemic control
and hypoglygemia frequency of 2 new intensified insulin regimens, CSII and MDI, with
insulin lispro in a randomized study.”
Notes This cross-over study was not adequately analysed, and did not report correlations be-
tween baseline and end of study data, ignoring within-person variation. Therefore, stan-
dard deviations of the difference were derived assuming different correlation coefficients
(0.3, 0.5, 0.7, 0.9) and the largest standard deviation of the differences was derived from
cross-over studies with adequate statistical methodology
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk The study investigators used two tables of
randomisation, according to the previous
treatment of the patient used before the
study (injection or external pump)
Allocation concealment? Low risk Envelopes containing treatment allocation
were prepared before the beginning of the
study and were opened at the randomisa-
tion visit (#2) by the participant
Blinding?
All outcomes
High risk Not applicable for patient blinding, but
outcome assessor blinding not reported
Incomplete outcome data addressed?
All outcomes
Low risk 2.4% drop-outs/withdrawals/losses to fol-
low up. One participant dropped out in
first period of MI, he was orginially on CSII
and found MI too difficult
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was not reported.
49Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hirsch 2005
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Cross-over
CONTROLLED CLINICAL TRIAL (CCT): No
Participants WHO PARTICIPATED: 100 participants were included in this study. 50 participants
were randomised to start with CSII and 45 completed CSII and were subsequently
crossed over to MI. 50 participants were randomised to start with MI and 46 completed
MI and were subsequently crossed over to CSII
SEX (female% / male%): 63 female (63%), 37 male (37%)
AGE (mean years (SD)): The mean age of participants starting with CSII was 41.7 (11.
1) years and the mean age of participants starting with MI was 44.2 (11) years
ETHNIC GROUPS (%): In the group starting with CSII, 48 participants were caucasian
(96%) and two were hispanic (4%) and in the group starting with MI, 48 participants
were caucasian (96%), one was hispanic (2%) and one was asian (2%)
DURATION OF DISEASE (mean years (SD)): The mean disease duration of partici-
pants starting with CSII was 19.7 (11.3) years and in those starting with MI, the mean
disease duration was 23.9 (12.3) years
INCLUSION CRITERIA: People with type 1 diabetes who were ≥ 18 years, had BMI
≤ 40 kg/m2, and had HbA1c ≤ 9%.
EXCLUSION CRITERIA: Impaired hepatic or renal function, impaired cardiac func-
tion, hypoglycaemia awareness or recurrent major hypoglycemia, women of child bear-
ing age if they were pregnant, breast feeding or not practising contraception
DIAGNOSTIC CRITERIA: Not reported
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 15
COUNTRY/ LOCATION: USA
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Participants used own pumps
with insulin aspart
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Unit for unit basis single basal
bed time injection of insulin glargine and meal time boluses of insulin aspart delivered
by the Induo device (LifeScan, Milpitas, CA)
TREATMENT BEFORE STUDY: All participants were previously treated with CSII
for at least three months before the screening visit
TITRATION PERIOD: After randomisation, participants had one week to settle and
then four weeks study. At cross over, participants had one week to settle and four week
study
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: Glycemic control (fructosamine, blood glucose,
HbA1c), insulin dose, hypoglycemic events, hematology and blood chemistry
50Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hirsch 2005 (Continued)
Study details DURATION OF INTERVENTION: 4 weeks
DURATION OF FOLLOW-UP: 10 weeks
RUN-IN PERIOD: Basal insulin coverage could be modified through the scheduled
phone communications with the participants during a one week dose adjustment period
using insulin aspart with the Induo device (LifeScan, Milpitas, CA) with the goal of
fasting and before dinner glycemia in the range of 90 to 126 mg/dl (5 to 7 mmol/L)
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: Yes
NON-COMMERCIAL FUNDING: No
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “...we compared insulin aspart as the only approved rapid-acting analog for CSII with
insulin aspart/glargine in MDI therapy. Because the principles applied to mealtime
coverage were identical during both treatments, the study tests whether the theoretically
smooth profile of glargine will provide safety and efficacy comparable to the ”customized“
basal insulin delivery system that can be programmed by an infusion pump during CSII.
”
Notes This cross-over study was not adequately analysed, and did not report correlations be-
tween baseline and end of study data, ignoring within-person variation. Therefore, stan-
dard deviations of the difference were derived assuming different correlation coefficients
(0.3, 0.5, 0.7, 0.9) and the largest standard deviation of the differences was derived from
cross-over studies with adequate statistical methodology
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Details not provided.
Allocation concealment? Unclear risk Details not provided.
Blinding?
All outcomes
High risk Not applicable for patient blinding, but
outcome assessor blinding not reported
Incomplete outcome data addressed?
All outcomes
Unclear risk 9% drop-outs/withdrawals/losses to follow
up, however, reasons for these are not re-
ported
Free of selective reporting? High risk Complete data for CSII vs MI at the end
of treatment or end of study not provided
for HbA1c and mean daily blood glucose
Free of other bias? Unclear risk Compliance was measured and reported.
51Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Home 1982
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Cross-over
CONTROLLED CLINICAL TRIAL (CCT): No
Participants WHO PARTCIPATED: 10 participants were included in this study. It is not reported
how many started with each intervention
SEX (female% / male%): 4 female (40%), 6 male (60%)
AGE (mean years (SD)): 40.4 (7.3) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): 22.3 (8.3) years
INCLUSION CRITERIA: Not reported
EXCLUSION CRITERIA: Women who were pregnant, those taking drugs known to
alter carbohydrate metabolism (ie. oral contraceptives), renal disease (plasma creatinine
concentration > 2.26 mg/100ml), proliferative retinopathy, prior CVD event (ischemic
heart disease, myocardial infarct)
DIAGNOSTIC CRITERIA: Not reported
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: England
SETTING: General practice
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): 60% daily basal infusion and
40% preprandial boluses delivered by a portable infuser via injection cannula into the
abdominal wall using highly purified porcine insulin (Actrapid) and 0.15 mol/L saline
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Actrapid and Ultratardwas used.
Highly purified porcine neutral soluble insulin (Actrapid) was delivered by injection
before each main meal and highly purified bovine ultralente (Ultratard) was delivered
before main evening meal
TREATMENT BEFORE STUDY: Twice daily injection therapy.
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: Insulin dose, HbA1c, mean blood glucose, urinary glu-
cose, weight, hypoglycaemia, cholesterol, overall control, patient reaction
Study details DURATION OF INTERVENTION: 10 weeks
DURATION OF FOLLOW-UP: 10 weeks
RUN-IN PERIOD: 15 months for initial intensive education program and blood glucose
monitoring study
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: No
NON-COMMERCIAL FUNDING: Yes
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
52Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Home 1982 (Continued)
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “In an attempt to answer these questions we have compared CSII with a thrice-daily
injection regimen in a crossover study, using patients whose control has previously been
optimised on twice-daily insulin injections.”
Notes Standard deviations of the difference were extracted from paired t-test data
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Only reports that each patient was studied
on either intervention in random order
Allocation concealment? Unclear risk Details not provided.
Blinding?
All outcomes
High risk Not applicable for patient blinding, but
outcome assessor blinding not reported
Incomplete outcome data addressed?
All outcomes
Unclear risk 9.1% drop-outs/withdrawals/losses to fol-
low up - one (of eleven) patient suffered
a myocardial infarction before complet-
ing the study, however the authors have
reported throughout the paper that there
were only ten participants from the begin-
ning of the study and it is not reported at
which stage the participant was at when
they withdrew
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was not reported.
Hoogma 2005
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Cross-over
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 256 participants were included in this study. 127 participants
were randomised to start with CSII and 129 participants were randomised to start with
MI. After six months the participants were crossed over, serving as their own controls.
223 participants completed the study
53Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hoogma 2005 (Continued)
SEX (female% / male%): 135 (53%) female, 121 (47%) male
AGE (mean years (SD)): The mean age of participants starting with CSII was 35.3 (9.
8) years and the mean age of participants starting with MI was 37 (10.6) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): The mean disease duration of those
starting with CSII was 14.4 (8.9) years and in those staring with MI, the mean disease
duration was 15.4 (10.1) years
INCLUSION CRITERIA: Type 1 diabetes and absent C-peptide secretion, aged 18 to
65 years, on multiple injection therapy for at least six months
EXCLUSION CRITERIA: Hypoglycaemia awareness, progressive retinopathy, renal
insufficiency (creatinine ≥ 250 µmol/L), acute coronary syndrome or cerebrovascular
accident within the last six months, uncontrolled hypertension, autonomic neuropathy,
planned or existing pregnancy, or other clinically significant concomitant disorders
DIAGNOSTIC CRITERIA: Not reported
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 11
COUNTRY/ LOCATION: Europe
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Insulin lispro via a multi pro-
grammable insulin infusion pump (H-TRON V100 or H-TRONplus V100, Disetronic
Medical Systems AG, Burgdorf, Switzerland). Adjusted according to glycaemic targets
i.e.. blood glucose 4.0 to 7.0 mmol/L fasting and before meals, blood glucose at bed
time 6.0 to 10.0 mmol/L and blood glucose 8.0 to 10.0 mmol/L one hour after meals.
Participants were advised to decrease or increase the dose of NPH insulin if fasting glu-
cose was repeatedly < 4.0 or > 7.0 mmol/L and to decrease or increase the dose of rapid-
acting insulin at meals if the one hour post prandial blood glucose was repeatedly < 8.0
or > 10.0 mmol/L. In case of high before dinner blood glucose values it was decided to
supplement NPH insulin at lunch time and at breakfast and dinner
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): At least three injections of insulin
lispro before meals and at least one injection of insulin NPH to achieve optimal control.
Adjusted according to glycaemic targets, as above
TREATMENT BEFORE STUDY: Multiple injection therapy for at least six months
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Mean HbA1c, daily blood
glucose fluctuation (defined as the average standard deviation of the mean daily blood
glucose, using measurements taken during the 14 days prior to the final visit in each
treatment period
SECONDARY OUTCOMES (as stated in the publication): mean daily blood glucose
values (from standardised 24 hour blood glucose profiles), severity of hypoglycaemic
episodes, quality of life (using the diabetes quality of life (DQoL) questionnaire, the
SF-12 questionnaire and an additional questionnaire related to lifestyle and therapy
manageability
ADDITIONAL OUTCOMES: Insulin requirements, body weight, injection and infu-
sion site problems, adverse events
54Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hoogma 2005 (Continued)
Study details DURATION OF INTERVENTION: 6 months
DURATION OF FOLLOW-UP: 16 months
RUN-IN PERIOD: Each treatment phase started with a two month run in period,
during which patients received education to optimise intensive insulin therapy
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: Yes
NON-COMMERCIAL FUNDING: No
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “The aim of this study was to compare CSII with MDI with respect to metabolic
parameters - including HbA1c, blood glucose levels and fluctuation, and incidence of
hypoglycaemia, quality of life and adverse events, in an adequately powered RCT with
a crossover design.”
Notes This cross-over study was not adequately analysed, and did not report correlations be-
tween baseline and end of study data, ignoring within-person variation. Therefore, stan-
dard deviations of the difference were derived assuming different correlation coefficients
(0.3, 0.5, 0.7, 0.9) and the largest standard deviation of the differences was derived from
cross-over studies with adequate statistical methodology
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk Randomized 1:1 with a block size of four.
Allocation concealment? Low risk The study investigators used numbered,
sealed envelopes containing the group
number handed to the investigators. The
envelope with the lowest available number
had to be used first
Blinding?
All outcomes
High risk Not applicable for patient blinding, but
outcome assessor blinding not reported
Incomplete outcome data addressed?
All outcomes
Low risk Efficacy ITT cross-over cohort (229 partic-
ipants), safety cohort (256 participants)
272 were enrolled and randomised, 223
completed the study. Analysis was based
on the intention-to-treat cross-over cohort
(229 participants)
31 (15 in MDI-CSII, 16 in CSII-MDI)
withdrew during the first treatment phase,
12 completed phase one (two in MDI-
CSII, ten in CSII-MDI) but did not cross
55Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hoogma 2005 (Continued)
over to the second phase. Six withdrew at
phase two (three in MDI-CSII, three in
CSII-MDI)
Main reason for withdrawal was refusal to
start CSII from group MDI-CSII, or to
leave CSII for group CSII-MDI
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was measured by review of pa-
tients diary regarding number of recorded
SMBG measurements
Lepore 2003
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Parallel
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 32 participants were included in this study. 16 participants
were randomised to and completed CSII and the other 16 participants were randomised
to and completed MI
SEX (female% / male%): 17 female (53%), 15 male (47%)
AGE (mean years (SD)): In the CSII group, the mean age of the participants was 37.7
(11.2) years and in the MI group, the mean age of the participants was 42.9 (15.6) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): In the CSII group, the mean disease
duration was 19.6 (9.2) years and in the MI group, the mean disease duration was 14.7
(11.1) years
INCLUSION CRITERIA: Type 1 diabetes, age 18 - 65 years, poor metabolic control
(defined as HbA1c constantly above 8% in the previous year), treatment with multiple
daily insulin injections (regular or lispro insulin before each meal plus NPH as basal
insulin) for at least 1 year before the study, patients consenting to begin treatment with
CSII
EXCLUSION CRITERIA: Evidence of severe late complication of diabetes (i.e.. overt
nephropathy and/or proliferative retinopathy), significant cardiovascular and hepatic
disease, patients unwilling to perform at least four blood glucose measures per day
DIAGNOSTIC CRITERIA: ADA 1997
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: Italy
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Insulin lispro at multiple basal
infusion rates plus boluses at meals
56Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lepore 2003 (Continued)
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Insulin lispro at each meal com-
bined with glargine injected at dinner or at bed time
TREATMENT BEFORE STUDY: Treatment with multiple daily insulin injections
(regular or lispro insulin before each meal plus NPH as basal insulin) for at least one
year before the study
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: Insulin requirements, weight, HbA1c, blood glucose,
hypoglycaemia, total cholesterol, HDL-cholesterol, triglycerides, uric acid
Study details DURATION OF INTERVENTION: 1 year
DURATION OF FOLLOW-UP: 1 year
RUN-IN PERIOD: During the run-in period all patients received a structured education
programme (eight hours) concerning intensive insulin therapy (blood glucose self mon-
itoring, insulin therapy, carbohydrate counting, self-management strategies). Patients
treated with CSII received another two sessions (eight hours) about CSII treatment
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: No
NON-COMMERCIAL FUNDING: Yes
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes - Letter
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “For this purpose we evaluated, in an open parallel group trial of 1-year duration involving
32 type 1 diabetic patients that had been treated with MDIs (regular or lispro insulin
before each meal plus NPH as basal insulin) for at least 1 year, the efficacy of two regimens
of intensive insulin treatment: CSII versus MDIs with lispro at each meal plus glargine
as basal insulin.”
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk Computer generated sequence.
Allocation concealment? Unclear risk A progressive identification number (from
1 to 32) was given to every participant
who was randomly allocated to interven-
tion groups using a randomisation software
on an Internet service provider
Blinding?
All outcomes
High risk Not applicable for participant blinding but
outcome assessor blinding not reported
57Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lepore 2003 (Continued)
Incomplete outcome data addressed?
All outcomes
High risk
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance - the study investigators evalu-
ated the number of blood glucose self mea-
sures recorded in the memory of glucose
meter in both groups, the data of insulin in-
jections recorded in the diary of the patient
in MI group, the data of bolus and basal
insulin infusion recorded in the memory of
pump in CSII group
Meschi 1982
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Parallel
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 16 participants were included in this study. Eight participants
were randomised to and completed CSII and the other eight participants were ran-
domised to and completed MI
SEX (female% / male%): 6 female (38%), 10 male (62%)
AGE (mean years (SD)): The mean age of participants in the CSII group was 13.3 (4)
years and the mean age of participants in the MI group was 12.9 (2.4) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): Not reported
INCLUSION CRITERIA: Not reported
EXCLUSION CRITERIA: Not reported
DIAGNOSTIC CRITERIA: Not reported
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: Italy
SETTING: In-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Regular insulin was infused
through a 27 gauge short butterfly catheter implanted subcutaneously in the abdominal
wall. The portable battery driven Mill Hill Infuser pump Model 1001 was used to deliver
insulin. Preprandial insulin delivery was manually delivered 30 minutes before main
meals as single boluses. On the first day, the 24 hour infusion dose was calculated as 1.
5 U/kg of body weight divided into 0.75 U/kg as the basal rate and 0.75 U/kg in three
preprandial boluses (i.e.. 20% 30 minutes before breakfast, 40% before lunch and 40%
before dinner) adjusted to optimise metabolic control
58Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Meschi 1982 (Continued)
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): To achieve the same daily insulin
distribution, the total 24 hour insulin dose (1.5 U/kg body weight) was divided into 0.
75 U/kg as lente insulin (two injections) and 0.75 U/kg as regular insulin injections 30
minutes before main meals (three injections)
TREATMENT BEFORE STUDY: Not reported
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: Blood glucose, HbA1c, insulin dose, hypoglycaemia
Study details DURATION OF INTERVENTION: 6 days
DURATION OF FOLLOW-UP: 6 days
RUN-IN PERIOD: Four days in hospital with conventional insulin therapy of two daily
injections with a mixture of regular and lente insulin before breakfast and dinner. The
dose was increased until slight hypoglycaemic symptoms were noted
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: No
NON-COMMERCIAL FUNDING: Yes - Consiglio Nazionale delle Ricerche
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT):No
Stated aim of study “We have therefore compared CSII with an intensified conventional insulin treatment
(3 daily insulin injections) (3II).”
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Details not provided.
Allocation concealment? Unclear risk Details not provided.
Blinding?
All outcomes
High risk Not applicable for participant blinding, but
outcome assessor blinding not reported
Incomplete outcome data addressed?
All outcomes
Unclear risk Details not provided.
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was not reported.
59Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Nathan 1982
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Cross-over
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: Five participants were included in this study
SEX (female% / male%): 3 female (60%), 2 male (40%)
AGE (mean years (SD)): The mean age of participants was 31 (5.7) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): 7 (1.8) years
INCLUSION CRITERIA: Not reported
EXCLUSION CRITERIA: Not reported
DIAGNOSTIC CRITERIA: Not reported
CO-MORBIDITIES: None of the participants had significant neuropathy, nephropathy,
retinopathy, or vascular disease at the outset of the study
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: USA
SETTING: In-patient and out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): An auto syringe AS6C pump
was used with a 27-gauge pump catheter. Catheters were changed every two to seven days
depending on participant preference. About half of the total insulin dose was delivered
as basal infusion and the remainder was delivered as before meal boluses as per MI
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): The timing and amount of doses
of intermediate, long-acting and rapid acting insulins were adjusted according to gly-
caemic targets. Subcutaneous NPH insulin (intermediate-acting) was delivered 30 to 60
minutes before breakfast and either 30 minutes before dinner or at 8pm. Regular insulin
was delivered from 15 to 60 minutes before each meal depending on the response of
participant
Glycemic target - to obtain fasting plasma glucose concentrations less than 90 mg/dL
and postprandial concentrations less than 150 mg/dL without hypoglycaemic reactions
TREATMENT BEFORE STUDY: Before the study, participants were using various
insulin regimens
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: HbA1c, mean plasma glucose, hypoglycaemic reactions,
daily insulin dose, fluorophotometry
Study details DURATION OF INTERVENTION: 8 to 12 weeks
DURATION OF FOLLOW-UP: 6 months
RUN-IN PERIOD: Subjects were admitted to the General Clinical Research Center
of the Massachusetts General Hospital for an evaluation and adjustment of therapies
according to glucose profiles done at this time. Once randomised, participants were
monitored for two to three days as in-patients while the regimen was established
60Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Nathan 1982 (Continued)
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: Yes
NON-COMMERCIAL FUNDING: No
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “A crossover trial was conducted in five adult patients with type I diabetes to examine the
relative efficacy of intensive conventional and insulin pump therapies in a more realistic
outpatient setting.”
Notes One of the participants was crossed over three times, initially treated with MI for eight
weeks, them CSII for 12 weeks, MI for another four weeks and finally with CSII for 12
weeks
Another of the participants participated in a double blind cross-over fashion, so that
both the participant and the investigator were blind to the intervention. The participant
received both interventions simultaneously but when on the CSII phase, saline was
injected and when on the MI phase, saline was infused through the pump. This was
controlled by the participant’s wife, who was a registered nurse, so that the participant
was unaware of the cloudy insulin solution in either device
Standard deviations of the difference were extracted from paired t-test data
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Details not provided.
Allocation concealment? Unclear risk Details not provided.
Blinding?
All outcomes
Unclear risk One of the participants participated in a
double blind cross-over fashion, so that
both the participant and the investigator
were blind to the intervention. The partic-
ipant received both interventions simulta-
neously but when on the CSII phase, saline
was injected and when on the MI phase,
saline was infused through the pump. This
was controlled by the participant’s wife,
who was a registered nurse, so that the par-
ticipant was unaware of the cloudy insulin
solution in either device
Incomplete outcome data addressed?
All outcomes
Unclear risk Details not provided.
Free of selective reporting? Unclear risk Details not provided.
61Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Nathan 1982 (Continued)
Free of other bias? Unclear risk Compliance was measured by blood glu-
cose measurements.
Nosadini 1988
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Parallel
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 64 participants were included in this study (25 female, 39
male), however the following groups are relevant to this review: MI (ICIT), CSII
(CSII-fixed basal overnight insulin infusion rate (FBR) and CSII-higher programmable
overnight insulin infusion rate (HOR)) there were 44 participants (16 female, 28 male)
CSII-FBR - 19 participants randomised to and completed.
CSII-HOR - 10 participants randomised to and completed.
MI-ICIT - 15 participants randomised to and completed.
SEX (female% / male%):
CSII-FBR - 8 female (42%), 11 male (58%)
CSII-HOR - 4 female (40%), 6 male(60%)
MI-ICIT - 4 female (27%), 11 male (73%)
AGE (mean years (SD)):
CSII-FBR - 36 (6) years
CSII-HOR - 34 (3) years
MI-ICIT - 32 (9) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)):
CSII-FBR - 8 (3) years
CSII-HOR - 7 (3) years
MI-ICIT - 7 (4) years
INCLUSION CRITERIA: Diabetes according to NDDG, absent C-peptide response
EXCLUSION CRITERIA: Refusal of assignment to group, present C-peptide response
DIAGNOSTIC CRITERIA: NDDG
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: Italy
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): The Microjet MC20 was used
to deliver insulin on the CSII-FBR regimen and the Betatron II was used to deliver insulin
on the CSII-HOR regimen. The insulin dose was adjusted according to the glycaemic
target of a blood glucose value after and overnight fast between 90 to 110 mg/dL and
of after meal value between 130 to 160 mg/dL. The dose of the before meal insulin was
decided based on the before meal blood glucose value. The dose of intermediate insulin
in the evening was decided on the basis of the overnight fasting blood glucose value.
62Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Nosadini 1988 (Continued)
Each participant was seen every three weeks to modify the regimen to achieve better
blood glucose control
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Three daily soluble insulin injec-
tions were delivered during the day with a long-acting insulin in the evening. Participants
were allowed to modify each insulin injection (regular and long acting) within a 4 U
range. Further changes had to be by physician by phone or during examination. The
insulin dose was adjusted according to glycaemic targets of a blood glucose value after
an overnight fast between 90 to 110 mg/dL and of an after meal value between 130 to
160 mg/dL. The dose of before meal insulin was decided based on before meal blood
glucose value. The dose of intermediate insulin in the evening was decided on the basis
of the overnight fasting blood glucose value. Each participant was seen every three weeks
to modify the regimen to achieve better blood glucose control
TREATMENT BEFORE STUDY: Two to three injections per day.
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: plasma glucose, mean daily blood glucose, HbA1c, basal
and glucagon stimulated C-peptide, urinary albumin, hyper- and hypoglycaemic events
Study details DURATION OF INTERVENTION: 1 year
DURATION OF FOLLOW-UP: 1 year
RUN-IN PERIOD: Metabolic data for each participant were recorded for three months
while on existing treatment (two to three injections per day) and glucagon challenge was
performed. Each participant spent at least a week in hospital doing group teaching from
a team of a physician, diabetes nurse and dietician. Training in self monitoring and self
regulation of therapy was also conducted
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: No
NON-COMMERCIAL FUNDING: Yes - CNR Italy’s National Research Council
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “The purpose of the present investigation was to assess whether intensified conventional
insulin therapy and continuous subcutaneous insulin infusion are characterized by any
difference in the incidence of hypoglycaemic and ketoacidotic episodes in comparison
with more conventional insulin regimes.”
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Details not provided.
63Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Nosadini 1988 (Continued)
Allocation concealment? Low risk The type of treatment was enclosed in an
envelope and opened by participant
Blinding?
All outcomes
High risk Not applicable for participant blinding, but
outcome assessor blinding not reported
Incomplete outcome data addressed?
All outcomes
High risk
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was not reported.
Nuboer 2008
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Parallel
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 39 participants were included in this study. 20 participants
(13 female, 7 male) were randomised to CSII and 19 completed (12 female, 7 male),
and the other 19 participants (9 female, 10 male) were randomised to and completed
MI
SEX (female% / male%): 22 female (56%), 17 male (44%)
AGE (mean years (SD)): The mean age of participants in the CSII group was 10 (3)
years (excluding one drop out) and the mean age of participants in the MI group was 10
(3.7) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): Disease duration in the CSII group was
5.6 (3.3) years (excluding one drop out) and in the MI group was 4.7 (2.9) years
INCLUSION CRITERIA: Type 1 diabetes, diagnosed by the presence of islet antigen-
2, glutamic acid decarboxylase-65 or islet cell cytoplasmic autoantibodies, daily insulin
administration for 1 yr or longer, random C-peptide < 200 pmol, HbA1c > 8.0%, a
history of repeated symptomatic hypoglycaemia, age four to 16 years, and attendance of
a regular school
EXCLUSION CRITERIA: Clinically manifest chronic complications, pregnancy, co-
morbidity, mental retardation, psychiatric treatment or symptoms in a child or a parent,
insufficient
Dutch language capabilities and absence of a telephone at home
DIAGNOSTIC CRITERIA: Not reported
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
64Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Nuboer 2008 (Continued)
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: The Netherlands
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): For CSII, only insulin aspart was
used. H-tron Disetronic insulin pumps (Roche, Basel, Switzerland) were used, changing
the infusion catheter every two days. CSII insulin dosage was initiated as 75% of the total
daily MI dose, mostly 50% as basal insulin day and night and 50% premeal, including
snacks
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Three short-acting insulin doses
before breakfast, lunch and supper. During MI, 26 children used insulin aspart and 12
used regular insulin before meals. At bed time, longer acting insulins were given, 23
using intermediate-acting insulin neutral protamine Hagedorn (NPH) and 15 insulin
glargine
TREATMENT BEFORE STUDY: Participants had a 3.5 month run-in period
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not specified
SECONDARY OUTCOMES (as stated in the publication): Not specified
ADDITIONAL OUTCOMES: Disease impact using the Diabetes Quality of Life Ques-
tionnaire, Pediatric Quality of Life Inventory as rated by parents and children, HbA1c,
daily insulin dose (U/kg), and adverse events
Study details DURATION OF INTERVENTION: 10.5 months for CSII and 3.5 months for MDI
DURATION OF FOLLOW-UP: 10.5 months
RUN-IN PERIOD: 3.5-month run-in phase on MDII for all children, consisting of
injecting three short-acting insulin doses before breakfast, lunch and supper
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: No
NON-COMMERCIAL FUNDING: Yes - Ministry of Health and the trust Funds of
National Health Insurance CIEs and of University Hospitals (VAZ/VWS). Additional
funding was obtained from the Child Health and Wellbeing Fund, the Volkskracht Fund
and the van Leeuwen Lignac Fund, all in Rotterdam, the Netherlands
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “The aim of the present study was to investigate the changes in quality of life and of
impact of disease by either CSII or MDII prospectively in a randomized study preceded
by a 3.5-month run-in phase of MDII, following medical effects simultaneously.”
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Details not provided.
65Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
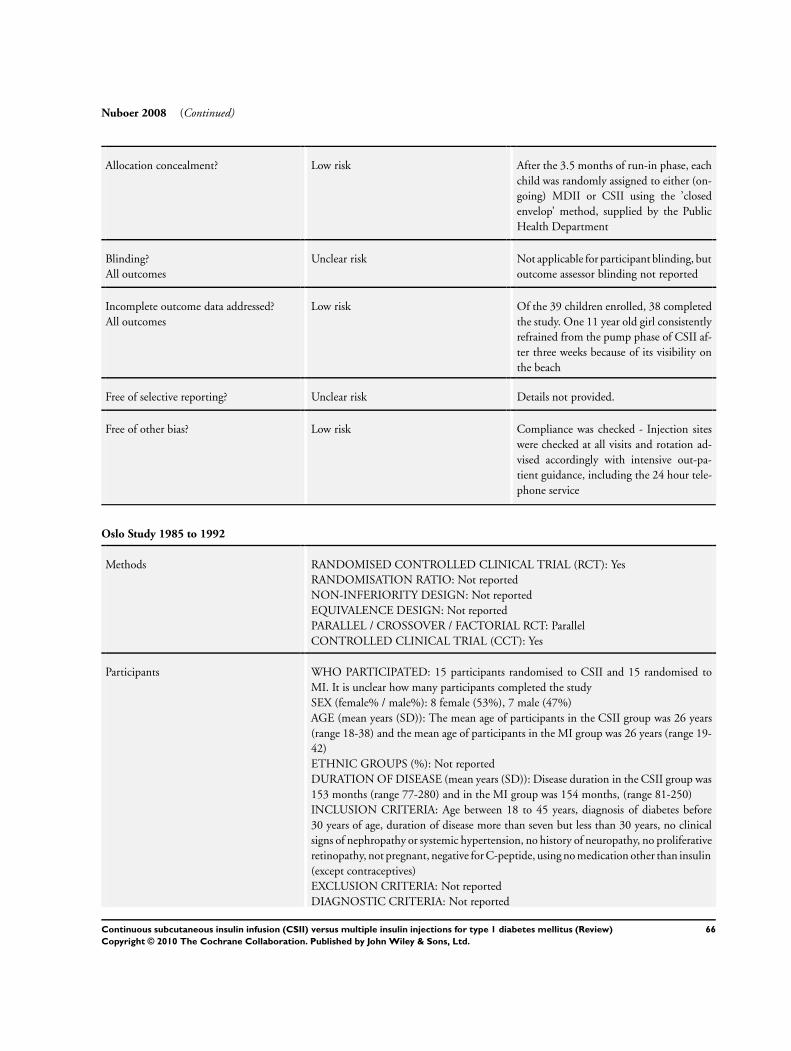
Nuboer 2008 (Continued)
Allocation concealment? Low risk After the 3.5 months of run-in phase, each
child was randomly assigned to either (on-
going) MDII or CSII using the ’closed
envelop’ method, supplied by the Public
Health Department
Blinding?
All outcomes
Unclear risk Not applicable for participant blinding, but
outcome assessor blinding not reported
Incomplete outcome data addressed?
All outcomes
Low risk Of the 39 children enrolled, 38 completed
the study. One 11 year old girl consistently
refrained from the pump phase of CSII af-
ter three weeks because of its visibility on
the beach
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Low risk Compliance was checked - Injection sites
were checked at all visits and rotation ad-
vised accordingly with intensive out-pa-
tient guidance, including the 24 hour tele-
phone service
Oslo Study 1985 to 1992
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Parallel
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 15 participants randomised to CSII and 15 randomised to
MI. It is unclear how many participants completed the study
SEX (female% / male%): 8 female (53%), 7 male (47%)
AGE (mean years (SD)): The mean age of participants in the CSII group was 26 years
(range 18-38) and the mean age of participants in the MI group was 26 years (range 19-
42)
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): Disease duration in the CSII group was
153 months (range 77-280) and in the MI group was 154 months, (range 81-250)
INCLUSION CRITERIA: Age between 18 to 45 years, diagnosis of diabetes before
30 years of age, duration of disease more than seven but less than 30 years, no clinical
signs of nephropathy or systemic hypertension, no history of neuropathy, no proliferative
retinopathy, not pregnant, negative for C-peptide, using no medication other than insulin
(except contraceptives)
EXCLUSION CRITERIA: Not reported
DIAGNOSTIC CRITERIA: Not reported
66Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Oslo Study 1985 to 1992 (Continued)
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: Multi-centre
COUNTRY/ LOCATION: Norway
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Autosyringe AS6C pump was
used in 12 participants and the Nordisk infuser was used in 3 participants during the
first two years. After the second year the following pumps were used: Nordisk Infuser,
Autosyringe AS6C, Eugly, Graseby MS26, Nipro. Subcutaneous abdominal site of in-
fusion. Approximately half of the daily insulin dose was given continuously and rest as
boluses 15 minutes pre meals. Basal and meal doses were adjusted individually in each
participant, according to glycaemic targets. Thirteen participants used four pre meal bo-
luses per day, one used three and one used six. The Nordisk infuser, Graseby and Eugly
pumps delivered regular porcine insulin at a concentration of 100 U/ml, the other pumps
delivered 40 U/ml. In the auto syringe AS6C pumps, daily insulin dose was diluted to 2.
8 ml by the corresponding insulin buffer. Fourteen participants received Velosulin and
one participant received Actrapid
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Regular porcine insulin was in-
jected 15 to 30 minutes pre meal and NPH insulin was given at bed time. Fourteen
participants were injected five times per day and one participant was injected four times
per day. Doses were adjusted according to glycaemic targets. Patients were allowed to
inject via butterfly needle for the first two years. After the second year Novopen was used
for injection of regular insulin
TREATMENT BEFORE STUDY: Not reported
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: Insulin requirements, weight, HbA1c, blood glucose
(mean and fasting), hypoglycaemia, peripheral nerve function, retinopathy
Study details DURATION OF INTERVENTION: 4 years
DURATION OF FOLLOW-UP: 4 years. Mean follow up was 40 months (range 24 to
46), all follow up was completed by the same two clinicians in the outpatient clinic after
one and three weeks, monthly during the first year, then bi-monthly
RUN-IN PERIOD: Two month pre-period with home blood glucose monitoring. All
participants injected NPH and regular porcine insulin pre breakfast and pre dinner.
Appropriate dose adjustments were made aiming to maintain blood glucose between 3
and 7 mmol/L pre meals without hypoglycaemia
Publication details LANGUAGE OF PUBLICATION: English and Norweigan
COMMERCIAL FUNDING: Yes - Nordisk Gentofte, Boehringer Mannheim
NON-COMMERCIAL FUNDING: Yes - Norwegian Council for Science and the
Humanities, Norwegian Diabetes Association, Norwegian Council on Cardiovascular
Disease, University of Oslo, Jahres Medical Foundation
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
67Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Oslo Study 1985 to 1992 (Continued)
Stated aim of study “1. To study the influence of long term near-normoglycaemia one early stages of mi-
croangiopathy and neuropathy in young insulin dependent diabetes patients
2. To compare blood glucose control in three different insulin regimens:
-Continuous subcutaneous insulin infusion with portable pumps (CSII)
-Multiple insulin injections (MI)
-Optimized conventional treatment with two daily insulin injections
all regimens combined with home blood glucose monitoring.
3. To assess the frequency of acute complications of treatment
4. To establish a routine laboratory method for the determination of stable glycosylated
haemoglobin (HbA1c) to accurately assess blood glucose control.”
Notes This study was published in multiple journals at different time points. For this review,
only data reported at the four year time point have been used, since after four years, the
participants were no longer randomised
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk Block randomisation by computer pro-
gram.
Allocation concealment? Unclear risk Statistician without prior knowledge of
participants or mode of treatment
Blinding?
All outcomes
High risk Not applicable.
Incomplete outcome data addressed?
All outcomes
High risk
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was not reported.
Pozzilli 2003
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Parallel
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 23 participants were included in this study. Eleven participants
were randomised to CSII and seven completed. Twelve participants were randomised to,
and completed MI
SEX (female% / male%): 14 female (61%), 9 male (39%)
68Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Pozzilli 2003 (Continued)
AGE (mean years (SD)): 18.4 (9) years. In the completed CSII group, the mean age of
participants was 17.9 (9) years and the mean age of participants in the MI group was
18.9 (8.5) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): ≥ 1 week
INCLUSION CRITERIA: Diagnosis according to ADA with age presentation between
12 to 35 years, including positivity for islet cell autoantibodies; duration of clinical disease
(since beginning of insulin therapy) less than four weeks; no medical contraindications
(including pregnancy) or any other major chronic disease; and willingness and capability
to participate in regular follow up
EXCLUSION CRITERIA: Not reported
DIAGNOSTIC CRITERIA: ADA
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: Multi-centre
COUNTRY/ LOCATION: Italy
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): The 507C Medtronic MiniMed
Pump was used to deliver Humalog adjusted according to glycaemic targets. Participants
calculated before meal boluses by means of carbohydrate counting and individualised
carbohydrate/insulin ratios. In participants with no history of severe hypoglycaemia, the
before meal target blood glucose range was 3.9 to 8.3 mmol/L. In participants with
reduced hypoglycaemic awareness, the before meal target blood glucose range was 4.4
to 8.9 mmol/L. If hypoglycaemia was recurrent, a higher range was used
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Three injections of short acting
insulin at meal times plus NPH at bed time. The dose was adjusted according to glycaemic
targets. If before meal blood glucose was below 6.5 mmol/L, the dose was decreased by
10%, if blood glucose levels were consistently below 4.5 mmol/L for more than three
days, the dose was decreased by 20%. Therapy was discontinued if two hours after meal
blood glucose was consistently below 7.5 mmol/L. Participants with blood glucose above
10 mmol/L received a 10% increase in their dose or had their regimen modified
TREATMENT BEFORE STUDY: Not reported
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: HbA1c, drug toxicity, basal C-peptide concentration,
insulin requirement, body mass index
Study details DURATION OF INTERVENTION: 2 years
DURATION OF FOLLOW-UP: 2 years
RUN-IN PERIOD: Not reported
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: Yes
NON-COMMERCIAL FUNDING: Yes - International Centre for Diabetes Research,
Italy
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
69Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Pozzilli 2003 (Continued)
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “The present study was designed to find out whether more intense insulin therapy such
as continuous subcutaneous insulin infusion (CSII) together with NA administration
for up to 2 years after Type 1 diabetes diagnosis would be acceptable to patients with
recent-on-set Type 1 diabetes and improve the metabolic control compared with patients
receiving the intensive subcutaneous insulin therapy (ISIT) mode of intervention.”
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk Permutated block design.
Allocation concealment? Unclear risk Details not provided.
Blinding?
All outcomes
High risk Not applicable for participant blinding, but
outcome assessor blinding not reported
Incomplete outcome data addressed?
All outcomes
Low risk Four (17%) dropped out (first four ran-
domised to CSII decided to drop out be-
fore starting treatment)
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance not reported.
Saurbrey 1988
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Cross-over
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 21 participants were included in this study. Of the 21 partici-
pants randomised, 19 completed the study (13 in CSII and 6 in MI) (8 female, 11 male)
SEX (female% / male%): 9 female (43%), 12 male (57%)
AGE (mean years (SD)): 32 (2.1) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): 14.5 (1.4) years
INCLUSION CRITERIA: Unclear (with IDDM and able to comply with intensive
insulin regimen, were assumed to be C-peptide negative)
EXCLUSION CRITERIA: Not reported
70Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Saurbrey 1988 (Continued)
DIAGNOSTIC CRITERIA: Unclear
CO-MORBIDITIES: Twelve participants had background retinopathy, four partici-
pants had symptoms of incipient sensory neuropathy and three had intermittent pro-
teinuria
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: Single centre
COUNTRY/ LOCATION: Denmark
SETTING: In-patient for the first five days. Week three to six were out-patient. Week ten
was in-patient for change of treatment. Weeks 13, 16, 20 were out-patient. Participants
had access to a physician 24/7
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): The Auto-Syringe pump (n=
6) or the Medix pump (n=13) were used to deliver insulin. Insulin dose was adjusted
according to glycaemic targets and participants were advised to inject an additional 2 to
4 U of soluble insulin if blood glucose went above 12 mmol/L
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Three or more before meal in-
jections of short acting insulin (Actrapid) with a novopen plus one injection of inter-
mediated-acting insulin delivered at bedtime with conventional syringe. Insulin dose
was adjusted according to glycaemic targets and participants were advised to inject an
additional 2 to 4 U of soluble insulin if blood glucose went above 12 mmol/L
TREATMENT BEFORE STUDY: All participants were treated with twice daily injec-
tions of short-acting plus intermediate-acting or long-acting
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: Blood glucose, HbA1c, number of hypoglycaemic
episodes, participant’s attitudes about treatments
Study details DURATION OF INTERVENTION: 10 weeks
DURATION OF FOLLOW-UP: 26 weeks
RUN-IN PERIOD: Over three weeks, participants were taught self monitoring of blood
glucose using BM-glycemie strips (Boehringer, Mannheim) and a Hypocount B meter
(Hypoguard, Melton, England)
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: Yes
NON-COMMERCIAL FUNDING: No
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “The aim of the present cross-over study was to investigate whether CSII treatment and
ICT using NovoPen for the pre-meal injections of short-acting insulin, were equally
acceptable in daily use and also equally efficient in achieving good metabolic control in
patients with IDDM.”
71Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Saurbrey 1988 (Continued)
Notes This cross-over study was not adequately analysed, and did not report correlations be-
tween baseline and end of study data, ignoring within-person variation. Therefore, stan-
dard deviations of the difference were derived assuming different correlation coefficients
(0.3, 0.5, 0.7, 0.9) and the largest standard deviation of the differences was derived from
cross-over studies with adequate statistical methodology
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Details not provided.
Allocation concealment? Unclear risk Details not provided.
Blinding?
All outcomes
High risk Not applicable for participant blinding, but
outcome assessor blinding was not reported
Incomplete outcome data addressed?
All outcomes
Low risk 9.52% drop-outs/withdrawals/losses to fol-
low up - two participants found wearing
the pump unacceptable
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Participants were asked to report blood glu-
cose etc on a daily basis (as a possible mea-
sure of compliance)
Schmitz 1989
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Cross-over
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: Ten participants were included in this study. The participants
were randomised to either CSII or MI for six months, after which they were crossed
over for another six months serving as their own control. All participants completed the
study
SEX (female% / male%): 6 female (60%), 4 male (40%)
AGE (mean years (SD)): 36.5 (7.9) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): 23.7 (2.9) years
INCLUSION CRITERIA: Diabetes duration ≥ 20 years, absence of severe diabetic late
complications i.e.. urinary albumin excretion rate (UAE) ≤ 20µg/min, normal blood
pressure and serum creatinine and no proliferative retinopathy. Furthermore, the patients
72Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Schmitz 1989 (Continued)
should have no need for medication other than insulin
EXCLUSION CRITERIA: Not reported
DIAGNOSTIC CRITERIA: Not reported
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Part of the inclusion criteria was that the participants should
have no need for medication other than insulin
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: Denmark
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Insulin was delivered by the
Nordisk Infuser using Pharmaplast 25-gauge catheters and a 5.7 ml carpule of highly
purified porcine regular insulin (Velosulin, 100 IU/ml). Participants received three to six
boluses during the day
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Participants delivered three to
four bolus injections per day using the Insuject (Nordisk) containing carpules of 2 ml
Velosulin, 100 IU/ml during day time and an injection of NPH insulin at bed time
(Insulatard, 100 IU/ml)
TREATMENT BEFORE STUDY: Not reported
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: Weight, insulin dose, HbA1c, blood glucose, kidney
function (glomerular filtration rate, renal plasma flow, urinary albumin excretion)
Study details DURATION OF INTERVENTION: 6 months
DURATION OF FOLLOW-UP: 6 months
RUN-IN PERIOD: Not reported
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: Not reported
NON-COMMERCIAL FUNDING: Not reported
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “The aims of the present investigation were in this type of patient, 1) to evaluate glycaemic
control on CSII versus MIT treatment as well as the preferential treatment modality of
the patients and 2) to study the effect of optimised glycaemic control on kidney function
in very long-term uncomplicated IDDM.”
Notes The measure of variance was not specified (i.e.. whether SD or SE), the data has been
treated as SD
There were ten participants in this study, however information about the number of
participants in each group was not provided. For data analysis, it has been assumed that
each group comprised five participants
Standard deviations of the difference were extracted from paired t-test data
73Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Schmitz 1989 (Continued)
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Details not provided.
Allocation concealment? Unclear risk Details not provided.
Blinding?
All outcomes
High risk Not applicable for participant blinding, but
outcome assessor blinding was not reported
Incomplete outcome data addressed?
All outcomes
Low risk There were no drop-outs/withdrawals/
losses to follow up.
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was not reported.
Skogsberg 2008
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Parallel
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 72 participants were randomised and 67 participants com-
pleted the study
SEX (female% / male%): 30 female (42%), 42 male (58%)
AGE (mean years (SD)): The mean age of the participants in the CSII group was 11.8
(4.9) years and the mean age of the participants in the MI group was 12.3 (4.5) years.
Standard deviations are not provided, instead 95% confidence intervals are provided
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): The mean disease duration in the CSII
group was 12.2 (2.0) years and the mean disease duration in the MI group was 10.4 (1.
7) years
INCLUSION CRITERIA: Not reported
EXCLUSION CRITERIA: Not reported
DIAGNOSTIC CRITERIA: National guidelines for children with diabetes in Sweden
- National Guidelines for Children with Diabetes in Sweden. Lund: Studentlitteratur,
1996
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
74Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Skogsberg 2008 (Continued)
Interventions NUMBER OF STUDY CENTRES: Multicentre (n=9)
COUNTRY/ LOCATION: Sweden
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): The CSII group used insulin
aspart (NovoRapid; Novo Nordisk). The insulin pumps that were used in this study were
H-Tron (Roche, Burgdorf, Switzerland)
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): The MI group received morning
and bed time intermediate-acting insulin NPH (Insulatard; Novo Nordisk, Bagsvaerd,
Denmark) and rapid-acting insulin, aspart (NovoRapid; Novo Nordisk, Bagsvaerd, Den-
mark) three to four times a day as mealtime insulin. The NPH injections were given as
separate injections, that is, not mixed with the rapid-acting insulin
TREATMENT BEFORE STUDY: Not reported
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Outcomes not specified as
primary or secondary
SECONDARY OUTCOMES (as stated in the publication): Outcomes not specified as
primary or secondary
ADDITIONAL OUTCOMES: Hemoglobin A1c (HbA1c), insulin dosage, number of
contacts with the hospital for ketoacidosis (defined as pH < 7.3), severe hypoglycemic
episodes and/or technical problems, and the Diabetes Treatment Satisfaction Question-
naire (DTSQ)
Study details DURATION OF INTERVENTION: 24 months
DURATION OF FOLLOW-UP: 24.68 weeks for CSII and 28.80 weeks for MI
RUN-IN PERIOD: Not reported
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: No
NON-COMMERCIAL FUNDING: No - This research was partly supported by Re-
search and Development Center, county of Gavleborg’, Sweden, The Swedish Children’s
Diabetes Foundation’, Novo Nordisk Scandinavia, and Roche Diagnostics, Sweden
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study ”We therefore designed this study to compare CSII with MDI in newly diagnosed diabetic
children and adolescents. Our outcome measurements were metabolic control, safety,
and treatment satisfaction
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Details not reported.
75Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Skogsberg 2008 (Continued)
Allocation concealment? Unclear risk Details not reported.
Blinding?
All outcomes
Unclear risk Not applicable for participant blinding, but
outcome assessor blinding was not reported
Incomplete outcome data addressed?
All outcomes
Low risk Of 72 participants, 67 completed the whole
study. Two in the MDI group changed to
insulin pump between 18 and 21 months
at their own/parents’ request. Two, also
in the MDI group, were switched to the
new long-acting insulin analogue, glargine,
after 18 months (initiated by the dia-
betes team). One additional participant in
the MDI group dropped out around 12
months. These participants did not differ
from the others in the MDI group regard-
ing metabolic control or treatment satisfac-
tion when they dropped out of the study
Free of selective reporting? Unclear risk Details not reported.
Free of other bias? Unclear risk Compliance was not reported.
Tsui 2001
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Parallel
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 27 participants were included in this study. 13 participants
(five female, eight male) were randomised to and 12 completed CSII. 14 participants
were randomised to and completed MI (four female, ten male)
SEX (female% / male%): 9 female (33%), 18 male (67%)
AGE (mean years (SD)): The mean age of the participants in the CSII group was 36
(12) years and the mean age of the participants in the MI group was 36 (10) years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): The mean disease duration in the CSII
group was 17 (10) years and the mean disease duration in the MI group was 15 (9) years
INCLUSION CRITERIA: Adults between 18 to 60 years with endocrine diagnosis
of type 1 diabetes for more than two years, with onset before 40 years, and able to
comply with treatment regimen. Participants were required to be treated with one to
two injections per day and be motivated to use CSII
EXCLUSION CRITERIA: History of more than two severe hypoglycemic events (coma,
seizure, loss of conciousness) in the last year, hemoglobinopathy, insulin resistance, ex-
treme obesity (BMI > 35 kg/m2), severe late complications of diabetes, evidence of sig-
76Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
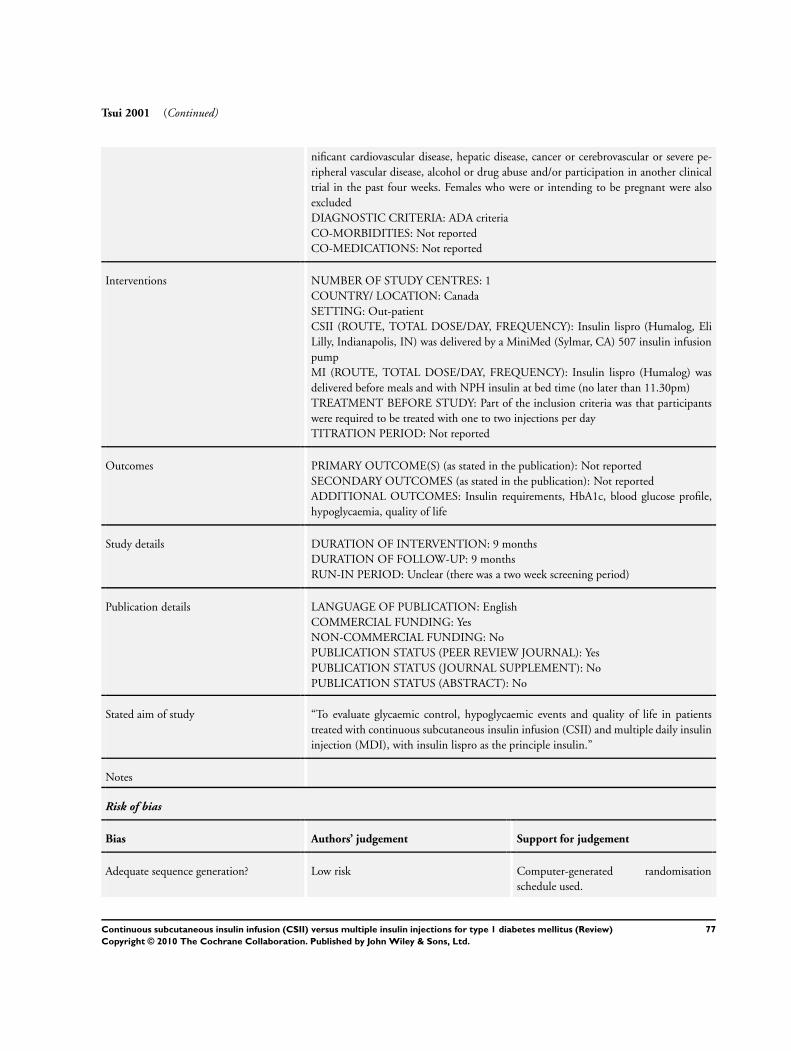
Tsui 2001 (Continued)
nificant cardiovascular disease, hepatic disease, cancer or cerebrovascular or severe pe-
ripheral vascular disease, alcohol or drug abuse and/or participation in another clinical
trial in the past four weeks. Females who were or intending to be pregnant were also
excluded
DIAGNOSTIC CRITERIA: ADA criteria
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: Canada
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Insulin lispro (Humalog, Eli
Lilly, Indianapolis, IN) was delivered by a MiniMed (Sylmar, CA) 507 insulin infusion
pump
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Insulin lispro (Humalog) was
delivered before meals and with NPH insulin at bed time (no later than 11.30pm)
TREATMENT BEFORE STUDY: Part of the inclusion criteria was that participants
were required to be treated with one to two injections per day
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: Insulin requirements, HbA1c, blood glucose profile,
hypoglycaemia, quality of life
Study details DURATION OF INTERVENTION: 9 months
DURATION OF FOLLOW-UP: 9 months
RUN-IN PERIOD: Unclear (there was a two week screening period)
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: Yes
NON-COMMERCIAL FUNDING: No
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “To evaluate glycaemic control, hypoglycaemic events and quality of life in patients
treated with continuous subcutaneous insulin infusion (CSII) and multiple daily insulin
injection (MDI), with insulin lispro as the principle insulin.”
Notes
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk Computer-generated randomisation
schedule used.
77Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Tsui 2001 (Continued)
Allocation concealment? Low risk Sealed envelopes that had been indepen-
dently prepared.
Blinding?
All outcomes
High risk Not applicable for participant blinding but
outcome assessor blinding was not reported
Incomplete outcome data addressed?
All outcomes
Low risk One drop out from CSII, 3.7% drop-outs/
withdrawals/losses to follow up. ITT con-
ducted
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was not reported.
Weintrob 2004
Methods RANDOMISED CONTROLLED CLINICAL TRIAL (RCT): Yes
RANDOMISATION RATIO: Not reported
NON-INFERIORITY DESIGN: Not reported
EQUIVALENCE DESIGN: Not reported
PARALLEL / CROSSOVER / FACTORIAL RCT: Cross-over
CONTROLLED CLINICAL TRIAL (CCT): Yes
Participants WHO PARTICIPATED: 23 participants were included in this study. Eleven participants
were randomised to start with CSII-MI and ten completed CSII-MI. Twelve participants
were randomised to start with MI-CSII and ten completed MI-CSII
SEX (female% / male%): 13 female (57%), 10 male (43%)
AGE (mean years (SD)): The age range of the participants was 9.25 to 13.75 years,
median 11.9 years
ETHNIC GROUPS (%): Not reported
DURATION OF DISEASE (mean years (SD)): The disease duration was 2.5 to 11
years, median 6 years
INCLUSION CRITERIA: Age 8 to 14 years, treated with insulin for at least two years,
deficient C-peptide secretion (fasting level, < 0.6 ng/mL), absence of other health prob-
lems except for treated hypothyroidism or antibody-negative celiac disease controlled
with gluten-free diet
EXCLUSION CRITERIA: Participants with microvascular complications, mental re-
tardation or a psychiatric disorder were excluded from this study
DIAGNOSTIC CRITERIA: ADA 1997
CO-MORBIDITIES: Not reported
CO-MEDICATIONS: Not reported
Interventions NUMBER OF STUDY CENTRES: 1
COUNTRY/ LOCATION: Israel
SETTING: Out-patient
CSII (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Participants used their pre study
insulin and doses were adjusted according to glycemic targets and amount of carbohy-
drates per meal according to 1U of insulin per 10 to 20 grams of carbohydrates. The
78Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Weintrob 2004 (Continued)
target range for glycemia was 80 to 150 mg/dL (4.4 to 8.3 mmol/L) before meals and at
midnight and 120 to 180 (6.7 to 10.2 hours) after meals. Regular insulin was delivered
20 to 30 minutes before meals and lispro was delivered immediately before meals and
snacks. Participants were asked to change the infusion site every three days and under
the following conditions: when blood glucose > 300 mg/dL (16.7 mmol/L) with positive
urine ketones or when blood glucose was > 300 mg/dL (16.7 mmol/L) and failed to
respond to a corrective insulin dose, and at any sign of insertion site infection
MI (ROUTE, TOTAL DOSE/DAY, FREQUENCY): Participants used their pre study
insulin and doses were adjusted according to glycaemic targets and amount of carbohy-
drates per meal. Participants were instructed to use a fixed caloric amount of carbohy-
drates for each meal and then adjust insulin according to postprandial glucose values.
Insulin consisted of combined neutral protamine Hagedorn (NPH) and regular insulin
before breakfast, regular insulin before lunch and supper and NHP at bed time
TREATMENT BEFORE STUDY: Three or more injections of insulin in the form
of Insulatard and Actrapid (Novo Nordisk, Bagsvaerd, Denmark) or Humalin N and
Humalin R (Eli Lilly, Inianapolis, Ind)
TITRATION PERIOD: Not reported
Outcomes PRIMARY OUTCOME(S) (as stated in the publication): Not reported
SECONDARY OUTCOMES (as stated in the publication): Not reported
ADDITIONAL OUTCOMES: Sensor performance, insulin requirements, body
weight, HbA1c, blood glucose, hypo- and hyperglycaemia, quality of life, body mass
index
Study details DURATION OF INTERVENTION: 3.5 months
DURATION OF FOLLOW-UP: 8 months
RUN-IN PERIOD: All children were treated with three or more injections of insulin
(insulatard and actrapid or humulin N and Humulin R) for two weeks
Publication details LANGUAGE OF PUBLICATION: English
COMMERCIAL FUNDING: Yes
NON-COMMERCIAL FUNDING: No
PUBLICATION STATUS (PEER REVIEW JOURNAL): Yes
PUBLICATION STATUS (JOURNAL SUPPLEMENT): No
PUBLICATION STATUS (ABSTRACT): No
Stated aim of study “In the present randomized crossover study, we compared the rate, degree, and duration of
hypoglycaemia and hyperglycaemia and the variability in glucose levels between children
and adolescents treated by CSII or MDI. We also sought to determine whether the
CGMS (Continuous Glucose Monitoring System) can improve glycaemic control and
glucose patterns.”
Notes Standard deviations of the difference were extracted from paired t-test data
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Details not provided.
79Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Weintrob 2004 (Continued)
Allocation concealment? Unclear risk Details not provided.
Blinding?
All outcomes
High risk Not applicable for participant blinding, but
outcome assessor blinding was not reported
Incomplete outcome data addressed?
All outcomes
Low risk 4.23% drop-outs/withdrawals/losses to fol-
low up. One out of 23 dropped out because
they were afraid to insert the sensor
Free of selective reporting? Unclear risk Details not provided.
Free of other bias? Unclear risk Compliance was not reported.
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Alemzadeh 2005 Not a randomised controlled trial.
Amemiya 1983 Not a randomised controlled trial.
Arias 1985 Not a randomised controlled trial and the number of multiple insulin injections per day is less than
three
Bagdade 1991 The number of multiple insulin injections per day is less than three
Bangstad 1994 The number of multiple insulin injections per day is less than three
Barbosa 1981 The number of multiple insulin injections per day is less than three
Barrett 1995 Not a randomised controlled trial.
Bech 1996 Following all reasonable attempts to contact the authors, we were unable to confirm the number of
multiple injections per day
Beck-Nielsen 1984 The number of multiple insulin injections per day is less than three
Beck-Nielsen 1985 The number of multiple insulin injections per day is less than three
Beck-Nielsen 1985a The number of multiple insulin injections per day is less than three
Beck-Nielsen 1990 The number of multiple insulin injections per day is less than three
Behme 1984 Not a randomised controlled trial and the number of multiple insulin injections per day is less than
three
80Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Bell 1985 Not a randomised controlled trial and the number of multiple insulin injections per day is less than
three
Bell 1985a Not a randomised controlled trial and the number of multiple insulin injections per day is less than
three
Bending 1986 The number of multiple insulin injections per day is less than three
Berg 1998 The number of multiple insulin injections per day is less than three
Bergenstal 1985 The number of multiple insulin injections per day is less than three
Berger 1989 Not a randomised controlled trial.
Bibergeil 1987 The number of multiple insulin injections per day is less than three
Biesenbach 1988 Not a randomised controlled trial.
Bode 1996 Not a randomised controlled trial.
Bode 2004 The number of multiple insulin injections per day is less than three
Bombor 1984 Not a randomised controlled trial.
Borisova 1989 Not a randomised controlled trial.
Brunetti 1984 Not a randomised controlled trial.
Buysschaert 1981 Not a randomised controlled trial.
Buysschaert 1983 Not a randomised controlled trial.
Calabrese 1982 Not a randomised controlled trial.
Canny 1985 The number of multiple insulin injections per day is less than three
Carta 1986 Following all reasonable attempts to contact the authors, we were unable to obtain extractable data
Cavallo-Perin 1983 Not a randomised controlled trial.
Chisholm 1984 Not a randomised controlled trial.
Christensen 1986 The number of multiple insulin injections per day is less than three
Christensen 1987 The number of multiple insulin injections per day is less than three
Christiansen 1987 The number of multiple insulin injections per day is less than three
81Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Ciavarella 1985 The number of multiple insulin injections per day is less than three
Colette 1986 Not a randomised controlled trial.
Colette 1989 Not a randomised controlled trial.
Connis 1989 Not a randomised controlled trial.
Coustan 1986 The number of multiple insulin injections per day is less than three
Davies 1984 The number of multiple insulin injections per day is less than three
de Beaufort 1985 The number of multiple insulin injections per day is less than three
de Beaufort 1989 The number of multiple insulin injections per day is less than three
Dicker 1987 Following all reasonable attempts to contact the authors, we were unable to determine whether the trial
was randomised.
DiMeglio 2004 The number of multiple insulin injections per day is less than three
Edelmann 1987 The number of multiple insulin injections per day is less than three
Feldt-Rasmussen 1986 The number of multiple insulin injections per day is less than three
Feldt-Rasmussen 1986a The number of multiple insulin injections per day is less than three
Feldt-Rasmussen 1991 The number of multiple insulin injections per day is less than three
Flores 1984 Following all reasonable attempts to contact the authors, we were unable to obtain extractable data
Garg 2004 Not a randomised controlled trial.
Garmo 2004 Not a randomised controlled trial.
Giocolea 1988 The number of multiple insulin injections per day is less than three
Goicolea 1986 The number of multiple insulin injections per day is less than three
Goicolea 1987 The number of multiple insulin injections per day is less than three
Goicolea 1988 The number of multiple insulin injections per day is less than three
Goicolea 1989 The number of multiple insulin injections per day is less than three
Greene 1983 Not a randomised controlled trial.
82Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
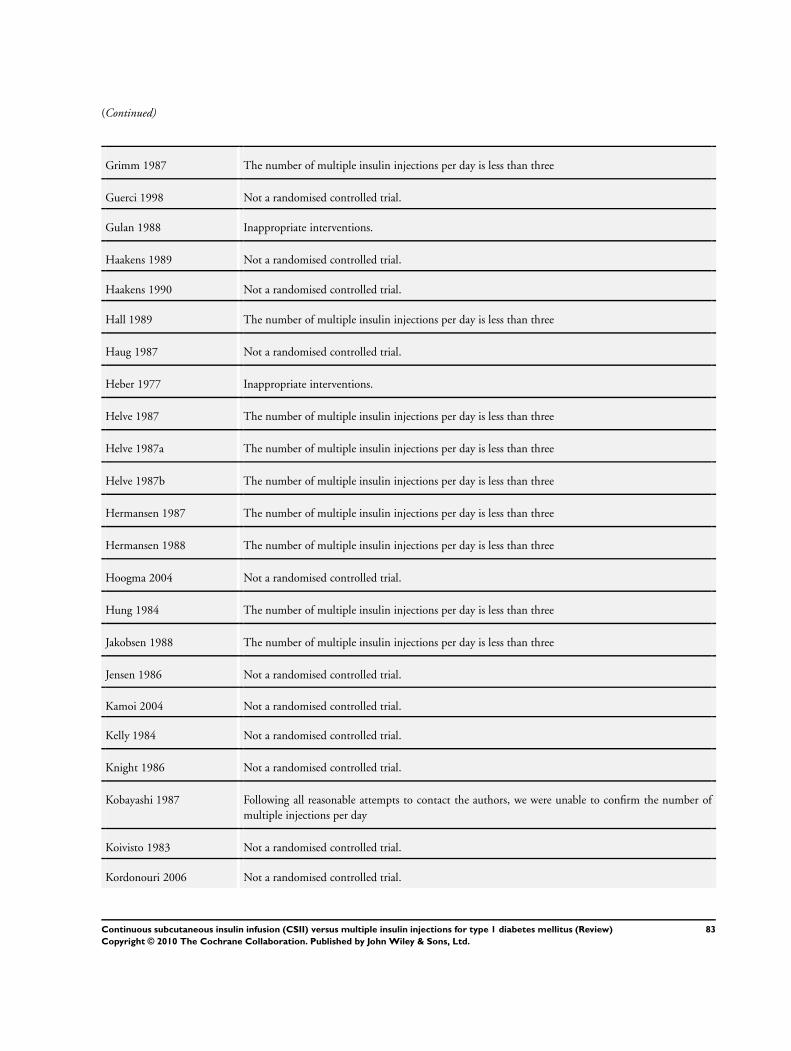
(Continued)
Grimm 1987 The number of multiple insulin injections per day is less than three
Guerci 1998 Not a randomised controlled trial.
Gulan 1988 Inappropriate interventions.
Haakens 1989 Not a randomised controlled trial.
Haakens 1990 Not a randomised controlled trial.
Hall 1989 The number of multiple insulin injections per day is less than three
Haug 1987 Not a randomised controlled trial.
Heber 1977 Inappropriate interventions.
Helve 1987 The number of multiple insulin injections per day is less than three
Helve 1987a The number of multiple insulin injections per day is less than three
Helve 1987b The number of multiple insulin injections per day is less than three
Hermansen 1987 The number of multiple insulin injections per day is less than three
Hermansen 1988 The number of multiple insulin injections per day is less than three
Hoogma 2004 Not a randomised controlled trial.
Hung 1984 The number of multiple insulin injections per day is less than three
Jakobsen 1988 The number of multiple insulin injections per day is less than three
Jensen 1986 Not a randomised controlled trial.
Kamoi 2004 Not a randomised controlled trial.
Kelly 1984 Not a randomised controlled trial.
Knight 1986 Not a randomised controlled trial.
Kobayashi 1987 Following all reasonable attempts to contact the authors, we were unable to confirm the number of
multiple injections per day
Koivisto 1983 Not a randomised controlled trial.
Kordonouri 2006 Not a randomised controlled trial.
83Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Kritz 1983 Not a randomised controlled trial.
Kroc 1984 The number of multiple insulin injections per day is less than three
Kroc 1988 Not a randomised controlled trial.
Kuno 1996 Not a randomised controlled trial.
Laatikainen 1987 The number of multiple insulin injections per day is less than three
Lager 1983 Not a randomised controlled trial.
Lager 1986 The number of multiple insulin injections per day is less than three
Lapolla 2003 Not a randomised controlled trial.
Lauritzen 1985 The number of multiple insulin injections per day is less than three
Lawson 1984 The number of multiple insulin injections per day is less than three
Lawson 1985 The number of multiple insulin injections per day is less than three
Leblanc 1986 The number of multiple insulin injections per day is less than three
Lecavalier 1987 Inappropriate interventions.
Lepore 2004 Not a randomised controlled trial.
Levy 1984 Not a randomised controlled trial.
Levy-Marchal 1983 Not a randomised controlled trial.
Levy-Marchal 1988 Not a randomised controlled trial.
Litton 2002 Not a randomised controlled trial.
Ludvigsson 2003 Not a randomised controlled trial.
Lunetta 1996 Following all reasonable attempts to contact the authors, we were unable to obtain extractable data
Mancuso 1986 Following all reasonable attempts to contact the authors, we were unable to determine whether the trial
was randomised.
Marshall 1987 The number of multiple insulin injections per day is less than three
Marshall 1988 The number of multiple insulin injections per day is less than three
84Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
(Continued)
McDonald 1982 Not a randomised controlled trial.
Mecklenburg 1982 Not a randomised controlled trial.
Minkina-Pedras 2005 Following all reasonable attempts to contact the authors, we were unable to confirm whether the trial
was randomised or the number of multiple injections per day
Moberg 1994 Not a randomised controlled trial.
Moller 1986 The number of multiple insulin injections per day is less than three
Monnier 1987 The number of multiple insulin injections per day is less than three
Muller 1999 Not a randomised controlled trial.
Nathan 1996 Inappropriate interventions.
Ng 1986 The number of multiple insulin injections per day is less than three
Nijs 1991 Not a randomised controlled trial.
Olsen 1985 The number of multiple insulin injections per day is less than three
Olsen 1987 The number of multiple insulin injections per day is less than three
Pickup 1979 Not a randomised controlled trial.
Pickup 1979a Not a randomised controlled trial.
Pickup 1984 Not a randomised controlled trial.
Pickup 1985 The number of multiple insulin injections per day is less than three
Pickup 1989 The number of multiple insulin injections per day is less than three
Pietri 1980 Not a randomised controlled trial.
Pietri 1983 Not a randomised controlled trial.
Reeves 1982 Following all reasonable attempts to contact the authors, we were unable to confirm whether the trial
was randomised
Regal 1988 Not a randomised controlled trial.
Rizza 1980 Not a randomised controlled trial.
Rodger 1985 The number of multiple insulin injections per day is less than three
85Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Rodger 1988 The number of multiple insulin injections per day is less than three
Saibene 1981 Not a randomised controlled trial.
Schaepelynck-Belicar 2003 Not a randomised controlled trial.
Schiffrin 1982 Following all reasonable attempts to contact the authors, we were unable to confirm the number of
multiple injections per day
Schiffrin 1982a Following all reasonable attempts to contact the authors, we were unable to confirm the number of
multiple injections per day
Schiffrin 1983 Following all reasonable attempts to contact the authors, we were unable to confirm the number of
multiple injections per day
Schiffrin 1984 Following all reasonable attempts to contact the authors, we were unable to confirm the number of
multiple injections per day
Schiffrin 1984a Following all reasonable attempts to contact the authors, we were unable to confirm the number of
multiple injections per day
Schiffrin 1985 Following all reasonable attempts to contact the authors, we were unable to confirm the number of
multiple injections per day
Schiffrin 1987 Following all reasonable attempts to contact the authors, we were unable to confirm the number of
multiple injections per day
Schmitz 1987 Inappropriate interventions.
Schottenfeld-Naor 1985 Not a randomised controlled trial.
Scuffham 2003 Not a randomised controlled trial.
Service 1985 The number of multiple insulin injections per day is less than three
Siebenhofer 2004 Inappropriate interventions.
Simonson 1985 Not a randomised controlled trial.
Skare 1986 Following all reasonable attempts to contact the authors, we were unable to obtain extractable data
Skyler 1982 Following all reasonable attempts to contact the authors, we were unable to confirm whether the trial
was randomised
Sleightholm 1986 The number of multiple insulin injections per day is less than three
Slijper 1990 The number of multiple insulin injections per day is less than three
86Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Steno 1982 The number of multiple insulin injections per day is less than three
Sulli 2003 Not a randomised controlled trial.
Tamborlane 1979 Not a randomised controlled trial.
Tamborlane 1979a Not a randomised controlled trial.
Tamborlane 1981 Not a randomised controlled trial.
Tamborlane 1982 Not a randomised controlled trial.
Testa 1985 The number of multiple insulin injections per day is less than three
Thuesen 1986 The number of multiple insulin injections per day is less than three
Tilvis 1986 The number of multiple insulin injections per day is less than three
Toni 2004 Not a randomised controlled trial.
Turk 1996 The number of multiple insulin injections per day is less than three
van Ballegooie 1985 Not a randomised controlled trial.
Viberti 1981 The number of multiple insulin injections per day is less than three
Viberti 1984 The number of multiple insulin injections per day is less than three
Warmolts 1987 Not a randomised controlled trial.
Weinzimer 2004 Not a randomised controlled trial.
Willi 2003 Not a randomised controlled trial.
Wilson 2005 The number of multiple insulin injections per day is less than three
Wredling 1997 Not a randomised controlled trial.
Yki-Jarvinen 1984 Not a randomised controlled trial.
Ziegler 1988 Following all reasonable attempts to contact the authors, we were unable to obtain extractable data
87Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. CSII versus MI
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 HbA1c 20 Mean Difference (Random, 95% CI) -0.25 [-0.40, -0.10]
1.1 Cross-over trials 10 Mean Difference (Random, 95% CI) -0.25 [-0.45, -0.05]
1.2 Parallel trials 10 Mean Difference (Random, 95% CI) -0.26 [-0.52, -0.00]
2 HbA1c subgroup analysis - age 20 Mean Difference (Random, 95% CI) -0.25 [-0.40, -0.10]
2.1 < 18 years 8 Mean Difference (Random, 95% CI) -0.22 [-0.41, -0.03]
2.2 > 18 years 12 Mean Difference (Random, 95% CI) -0.29 [-0.52, -0.06]
3 HbA1c subgroup analysis - study
duration
20 Mean Difference (Random, 95% CI) -0.25 [-0.40, -0.10]
3.1 Short term (< 1 month) 1 Mean Difference (Random, 95% CI) 0.2 [-1.94, 2.34]
3.2 Medium term (> 1 month
≤ 6 months)
12 Mean Difference (Random, 95% CI) -0.32 [-0.52, -0.11]
3.3 Long term (> 6 months) 7 Mean Difference (Random, 95% CI) -0.17 [-0.44, 0.10]
4 HbA1c small study bias 6 Mean Difference (Random, 95% CI) -0.72 [-1.55, 0.10]
5 Daily mean blood glucose 13 Mean Difference (Random, 95% CI) Subtotals only
6 Daily mean blood glucose
subgroup analysis - age
13 Mean Difference (Random, 95% CI) -15.26 [-23.37, -7.
14]
6.1 < 18 years 3 Mean Difference (Random, 95% CI) -3.70 [-14.38, 6.98]
6.2 > 18 years 10 Mean Difference (Random, 95% CI) -17.60 [-26.71, -8.
48]
7 Daily mean blood glucose
subgroup analysis - study
duration
13 Mean Difference (Random, 95% CI) -15.26 [-23.37, -7.
14]
7.1 Short term (< 1 month) 1 Mean Difference (Random, 95% CI) -3.0 [-80.47, 74.47]
7.2 Medium term (> 1 month
≤ 6 months)
10 Mean Difference (Random, 95% CI) -14.12 [-23.11, -5.
13]
7.3 Long term (> 6 months) 2 Mean Difference (Random, 95% CI) -21.41 [-29.40, -13.
43]
8 Daily mean blood glucose small
study bias
4 Mean Difference (Random, 95% CI) -29.33 [-51.36, -7.
31]
9 Fasting blood glucose 11 Mean Difference (Random, 95% CI) -14.02 [-24.42, -3.
61]
10 Fasting blood glucose subgroup
analysis - age
11 Mean Difference (Random, 95% CI) -14.02 [-24.42, -3.
61]
10.1 < 18 3 Mean Difference (Random, 95% CI) -7.67 [-23.88, 8.53]
10.2 >18 8 Mean Difference (Random, 95% CI) -16.25 [-29.07, -3.
42]
11 Fasting blood glucose subgroup
analysis - study duration
11 Mean Difference (Random, 95% CI) -14.02 [-24.42, -3.
61]
11.1 Short term (< 1 month) 1 Mean Difference (Random, 95% CI) -20.0 [-35.48, -4.52]
11.2 Medium term (> 1
month ≤ 6 months)
8 Mean Difference (Random, 95% CI) -8.48 [-19.35, 2.39]
88Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

11.3 Long term (> 6 months) 2 Mean Difference (Random, 95% CI) -37.04 [-73.46, -0.
62]
12 Fasting blood glucose small
study bias
3 Mean Difference (Random, 95% CI) -13.71 [-50.37, 22.
96]
13 Post prandial blood glucose 5 Mean Difference (Random, 95% CI) -4.44 [-10.91, 2.03]
14 Post prandial blood glucose
subgroup analysis - age
5 Mean Difference (Random, 95% CI) -4.44 [-10.91, 2.03]
14.1 < 18 2 Mean Difference (Random, 95% CI) -3.23 [-12.37, 5.90]
14.2 >18 3 Mean Difference (Random, 95% CI) -7.51 [-23.03, 8.00]
15 Post prandial blood glucose
subgroup analysis - study
duration
5 Mean Difference (Random, 95% CI) -4.44 [-10.91, 2.03]
15.1 Short term (< 1 month) 1 Mean Difference (Random, 95% CI) -24.0 [-41.44, -6.56]
15.2 Medium term (> 1
month ≤ 6 months)
4 Mean Difference (Random, 95% CI) -2.03 [-4.34, 0.27]
15.3 Long term (> 6 months) 0 Mean Difference (Random, 95% CI) 0.0 [0.0, 0.0]
16 Post prandial blood glucose
small study bias
2 Mean Difference (Random, 95% CI) 0.67 [-14.52, 15.86]
17 Non-severe hypoglycaemic
events
Other data No numeric data
18 Severe hypoglycaemic events Other data No numeric data
19 Quality of life Other data No numeric data
20 Weight 8 Mean Difference (Random, 95% CI) -0.37 [-1.98, 1.25]
21 Weight subgroup analysis -
study duration
8 Mean Difference (Random, 95% CI) -0.37 [-1.98, 1.25]
21.1 Short term (< 1 month) 0 Mean Difference (Random, 95% CI) 0.0 [0.0, 0.0]
21.2 Medium term (> 1
month ≤ 6 months)
6 Mean Difference (Random, 95% CI) -0.24 [-1.94, 1.46]
21.3 Long term (> 6 months) 2 Mean Difference (Random, 95% CI) -1.58 [-7.65, 4.50]
22 Weight small study bias 3 Mean Difference (Random, 95% CI) 1.74 [-4.24, 7.72]
23 Daily insulin requirement (U) 9 Mean Difference (Random, 95% CI) -6.98 [-10.77, -3.19]
24 Daily insulin requirement (U)
subgroup analysis - age
9 Mean Difference (Random, 95% CI) -6.98 [-10.77, -3.19]
24.1 < 18 1 Mean Difference (Random, 95% CI) -12.2 [-25.08, 0.68]
24.2 > 18 8 Mean Difference (Random, 95% CI) -6.59 [-10.66, -2.52]
25 Daily insulin requirement
(U) subgroup analysis - study
duration
9 Mean Difference (Random, 95% CI) -6.98 [-10.77, -3.19]
25.1 Short term (< 1 month) 1 Mean Difference (Random, 95% CI) -5.2 [-9.71, -0.69]
25.2 Medium term (> 1
month ≤ 6 months)
7 Mean Difference (Random, 95% CI) -8.68 [-14.34, -3.02]
25.3 Long term (> 6 months) 1 Mean Difference (Random, 95% CI) -3.0 [-11.41, 5.41]
26 Daily insulin requirement (U)
small study bias
5 Mean Difference (Random, 95% CI) -6.01 [-13.98, 1.96]
27 Daily insulin requirement (U/
kg)
13 Mean Difference (Random, 95% CI) Subtotals only
28 Daily insulin requirement (U/
kg) subgroup analysis - age
12 Mean Difference (Random, 95% CI) -0.12 [-0.19, -0.05]
28.1 < 18 6 Mean Difference (Random, 95% CI) -0.16 [-0.31, -0.01]
28.2 > 18 6 Mean Difference (Random, 95% CI) -0.08 [-0.15, -0.01]
89Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

29 Daily insulin requirement (U/
kg) subgroup analysis - study
duration
12 Mean Difference (Random, 95% CI) -0.12 [-0.19, -0.05]
29.1 Short term (< 1 month) 1 Mean Difference (Random, 95% CI) 0.1 [-0.12, 0.32]
29.2 Medium term (> 1
month ≤ 6 months)
6 Mean Difference (Random, 95% CI) -0.12 [-0.21, -0.03]
29.3 Long term (> 6 months) 5 Mean Difference (Random, 95% CI) -0.14 [-0.32, 0.04]
30 Daily insulin requirement (U/
kg) small study bias
3 Mean Difference (Random, 95% CI) -0.04 [-0.13, 0.05]
A D D I T I O N A L T A B L E S
Table 1. Overview of study populations
study ID intervention [n] screened [n]
randomised
[n] safety [n] ITT [n] finishing
study
comments
Bak 1987 &
Husted 1989
CSII (I1)
MI (I2)
For de-
tails about the
inter-
ventions, see ’
Characteris-
tics
of included
studies’.
Not reported Total: 20 Not reported Not reported Total: 16 Four par-
ticipants failed
to com-
plete the study
due to incom-
patibility with
CSII
Botta 1986 Not reported I1: 5
I2: 5
Total: 10
Not reported Not reported I1: 5
I2: 5
Total: 10
Drop outs not
reported
Bruttomesso
2008
I1: 24
I2: 18
Total:42
I1: 24
I2: 18
Total: 42
Not reported Not reported I1: 24
I2: 15
Total: 39
Chiasson
1984 & 1985
Not reported I1: 6
I2: 6
Total: 12
Not reported Not reported I1: 6
I2: 6
Total: 12
Drop outs not
reported
Cohen 2003 Not reported Total: 16 Not reported Not reported Total: 12 Three partici-
pants were sat-
isfied with
pump and so
didn’t want to
start MI, one
who started
with MI re-
fused to con-
nect to pump
DeVries 2002 To-
tal: 150 (asked
to participate)
I1: 39
I2: 40
Total: 79
Not reported I1: 39
I2: 40
I1: 34
I2: 21
It is impor-
tant to note
90Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Overview of study populations (Continued)
To-
tal: 89 (quali-
fication phase)
Total: 79 Total: 55 that at the
design phase,
the study
investigators
anticipated
the possibility
that they
would have
to analyse the
study as a
parallel RCT
(rather than
a cross-over)
because of the
demanding
nature of the
protocol and
an expected
high drop out
rate. However,
at the point
of cross over,
there had been
no drop outs
so the study
investigators
continued
with a cross-
over design
and stopped
inclusion at
79 partic-
ipants (48
participants
per arm were
calculated to
be required
to have an
80% chance
of detecting
a 0.75%
difference in
HbA1c with
an assumed
SD of 1.3%)
91Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Overview of study populations (Continued)
. Finally, the
study investi-
gators decided
that due to
the drop out
rate after cross
over, they
would analyse
the data as a
parallel study
using only pre
cross over data
Doyle 2004 Total: 32 I1: 16
I2: 16
Total: 32
Not reported I1: 16
I2: 16
Total: 32
I1: 16
I2: 15
Total: 31
Hanaire-
Broutin 2000
Not reported I1: 20
I2: 21
Total: 41
Not reported Not reported I1: 20
I2: 20
Total: 40
Hirsch 2005 Not reported I1: 50
I2: 50
Total: 100
Not reported Not reported I1: 45
I2: 46
Total: 91
Home 1982 Total: 12 Total: 11 Not reported Not reported Total: 10 The study in-
vesti-
gators have not
provided clear
infor-
mation about
what stage the
drop out oc-
curred
Hoogma 2005 Not reported Total: 272 Not reported Total: 229 Total: 223
Lepore 2003 Not reported I1: 16
I2: 16
Total: 32
Not reported Not reported I1: 16
I2: 16
Total: 32
Meschi 1982 Not reported I1: 8
I2: 8
Total: 16
Not reported Not reported I1: 8
I2: 8
Total: 16
Nathan 1982 Not reported Total: 5 Not reported Not reported Total: 5
Nosadini
1988
Not reported I1: 19 FBR
10 HOR
I2: 15
Not reported Not reported I1: 19 FBR
10 HOR
92Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Overview of study populations (Continued)
Total: 44 I2: 15
Total: 44
Nuboer 2008 Total: 39 I1: 19
I2: 19
Total: 38
Not reported Not reported I1: 19
I2: 19
Total: 38
Oslo Study
1985-1992
Total: 180 I1: 15
I2: 15
Total: 30
Not reported Not reported I1: 15
I2: 15
Total: 30
Pozzilli 2003 I1: 11
I2: 12
Total: 23
I1:11
I2:12
Total: 23
Not reported Not reported I1: 7
I2: 12
Total: 19
Four dropped
out of CSII be-
fore treatment
started.
Saurbrey 1988 Not reported I1:15
I2: 6
Total: 21
Not reported Not reported I1:13
I2: 6
Total: 19
Schmitz 1989 Not reported Total: 10 Not reported Not reported Total: 10
Skogsberg
2008
Not reported I1: 34
I2: 38
Total: 72
Not reported Not reported I1: 34
I2: 33
Total: 67
Tsui 2001 Total: 28 I1: 13
I2: 14
Total: 27
Not reported Not reported I1: 12
I2: 14
Total: 26
Weintrob
2004
Total: 24 I1: 11
I2: 12
Total: 23
Not reported Not reported I1: 10
I2: 12
Total: 22
Total 976 867
C O N T R I B U T I O N S O F A U T H O R S
MARIE MISSO (MM): co-ordinated each stage of the review and was responsible for: design of the review (in collaboration with
DOC); developing the protocol (in collaboration with DOC, JS and KE); developing the search strategy; undertaking the searches for
studies (independently of, but in addition to KE); screening the search results (independently of, but in addition to KE); organising
retrieval of papers; screening retrieved papers against inclusion/exclusion criteria (independently of, but in addition to KE); appraising
the quality of papers (independently of, but in addition to KE and MP); extracting data from papers (independently of, but in addition
to KE and MP); writing to study investigators for additional information; providing additional data about papers; summarising the risk
of bias of the studies (rated independently by MM, KE and MP); compiling the summary of comparisons, tables of included, excluded
awaiting and ongoing studies; entering data into RevMan 5; performing analysis of data; interpreting the findings; writing the review
(with contribution from DOC, JS, KE and MP); final approval of the version to be published.
93Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

DENISE O’CONNOR (DOC): was involved in the following stages of the review: the design of the review (in collaboration with
MM); developing the protocol (in collaboration with MM, JS & KE); contributing to the writing of the review (in collaboration with
MM, JS, KE and MP).
KRISTINE EGBERTS (KE): was involved in the following stages of the review: contributing to the drafting of the protocol (in
collaboration with MM, JS & DOC); screening the search results (independently of, but in addition to MM); screening retrieved
papers against inclusion/exclusion criteria (independently of, but in addition to MM); appraising the quality of papers (independently
of, but in addition to MM and MP); extracting data from papers (independently of, but in addition to MM and MP); contributing to
the writing of the review (in collaboration with MM, DOC, JS and MP).
MATTHEW PAGE (MP): was involved in the following stages of the review: appraising the quality of papers (independently of, but
in addition to MM and KE); extracting data from papers (independently of, but in addition to MM and KE); assisting MM with
compiling the table of included studies; contributing to the writing of the review (in collaboration with MM, DOC, JS and MP).
JONATHAN SHAW (JS): was involved with the following stages of the review: developing the protocol (in collaboration with MM,
DOC & KE) and contributing to the writing of the review (in collaboration with MM, DOC, KE and MP).
D E C L A R A T I O N S O F I N T E R E S T
JONATHAN SHAW: Received honoraria for lectures and for advisory boards; his department has received funding for research and
for organizing educational activities from NovoNordisk, Eli Lilly, Sanofi Aventis and Medtronic.
D I F F E R E N C E S B E T W E E N P R O T O C O L A N D R E V I E W
Matthew Page has been added as an author. The background has been updated. Study quality assessment methodology has been replaced
with risk of bias methodology as recommended for adapting the review to Review Manager 5 and the Cochrane Handbook for SystematicReviews of Interventions Version 5.0.0 (Higgins 2008).
Subgroup analysis regarding sex and type of insulin was not performed. We also conducted post-hoc analyses where we explored studies
that included less than 20 participants in subgroup analyses for each outcome.
I N D E X T E R M SMedical Subject Headings (MeSH)
Diabetes Mellitus, Type 1 [∗drug therapy]; Hypoglycemic Agents [∗administration & dosage]; Infusions, Subcutaneous; Insulin
[∗administration & dosage]; Randomized Controlled Trials as Topic
MeSH check words
Adolescent; Adult; Child; Humans
94Continuous subcutaneous insulin infusion (CSII) versus multiple insulin injections for type 1 diabetes mellitus (Review)
Copyright © 2010 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.