Embed Size (px)
Citation preview

Co-sponsored by
September 26 – 28, 2013 | Westin Tampa Harbour Island
Interactive Case Challenge: A Patient With Bipolar Disorder and Residual Symptoms
W. Vaughn McCall, MD, MS Medical College of Georgia at Georgia Regents University Augusta, GA Robert M. A. Hirschfeld, MD University of Texas Medical Branch Galveston, TX

Learning Objective
Initiate and maintain a solid communication dynamic with patients with bipolar depression so that they understand the role of sleep in bipolar disorder outcomes
1

Learning Objective
Accurately and routinely administer validated questionnaires to improve the detection of residual symptoms in patients with bipolar depression
2
W. Vaughn McCall, MD, MS
● Research/Grants: Merck; National Institute of Mental Health (NIMH)
● Scientific Advisor: Luitpold Pharmaceuticals, Inc.
Disclosures

Robert M. A. Hirschfeld, MD
● Consultant: bioStrategies Group; Grey Healthcare Group, Inc.; Merck Manual Editorial Board
● Other Financial Interest: Jones and Bartlett Publishers
● Honoraria: bioStrategies Group; CMEology; Health and Wellness Partners; Physicians Post Graduate Press, Inc.
Disclosures
Meet Ms. Patty Ericsson
● 42-year-old woman ● Divorced ● No children ● High school education ● Unemployed, on
unemployment benefits for 12 months, wanting to return to work

Chief Complaint
“I thought I was getting better, but now I just don’t feel like doing anything again”

Recent Psychiatric History
● One year ago ! Experienced a full-blown manic attack,
including delusions of grandeur, and requiring a 3-week psychiatric hospitalization
! Had resolution of psychosis, hyperactivity, and sleep loss after her psychotropic treatments were changed during that hospitalization
! Has had no more manic symptoms since that time and seemed to be euthymic and in remission

Recent Psychiatric History
● Over past six months ! Has had significant weight gain, attributed to
use of psychotropic medications ! Has had an increase in morning blood glucose
from 100 to 140 and was placed on metformin, leading to renormalization of her glucose level
Past Psychiatric History
● Diagnosed with bipolar I disorder ! First manic attack at age 20 ! Three psychiatric hospitalizations ! More time in depressed episodes than in
manic episodes ● Family psychiatric history is remarkable for ! Multiple members affected with depressive
illness ! None with mania, schizophrenia, or substance
abuse

Medical and Social History
● Medical ! Prediabetes ! S/P appendectomy and tonsillectomy
● Social ! Longest period of employment has been 15 months as
a sales clerk ! Married a man she met in her outpatient support
group, whom she divorced after two years ! She is active in her church and in her bipolar support
group ! She does not use alcohol, tobacco, or illicit drugs
S/P = Status post

Psychiatric Interview
● This is your first visit with this patient, and you are 15 minutes late seeing her!
● She is lightly dozing in the waiting room, but rouses when you walk up
● She reports: ! “I am depressed that I am so out of it.” ! Being so tired that she has not felt like seeing friends or going to
church for the last month, and takes pleasure from nothing ● Appears sluggish with no psychomotor-retardation,
and is not tearful ● Has normal speech ● Is fully oriented with intact recent memory ● Denies psychotic symptoms, suicidal or homicidal ideation
Beck Depression Inventory–I (BDI-1)
● Asks about how the subject has been feeling in last week ! 21 questions ! Each question has a set of at least four possible answer choices
! (0) I do not feel sad ! (1) I feel sad ! (2) I am sad all the time and I can't snap out of it ! (3) I am so sad or unhappy that I can't stand it
● Scoring: standard cut-offs ! 0 – 9: indicates minimal depression ! 10 – 18: indicates mild depression ! 19 – 29: indicates moderate depression ! 30 – 63: indicates severe depression
Beck AT, et al. Arch Gen Psychiatry. 1961;4:561-571. PMID: 13688369.
BDI Score
● She completes a BDI-1 ● Her score is 11
BDI-1 = Beck Depression Inventory–I
Medications
● Olanzapine 20 mg qhs (for 12 months)
● Lithium 900 mg qhs (for 5 years)
● Lamotrigine 100 mg qam (for 2 years)
● Metformin 500 mg bid (for 3 months)
qhs = at each bedtime; qam = each morning; bid = twice daily

● Overweight, BMI 35 ● Posterior pharynx not visualized ● Heart sounds and breath sounds are
distant ● Otherwise normal
Physical Exam
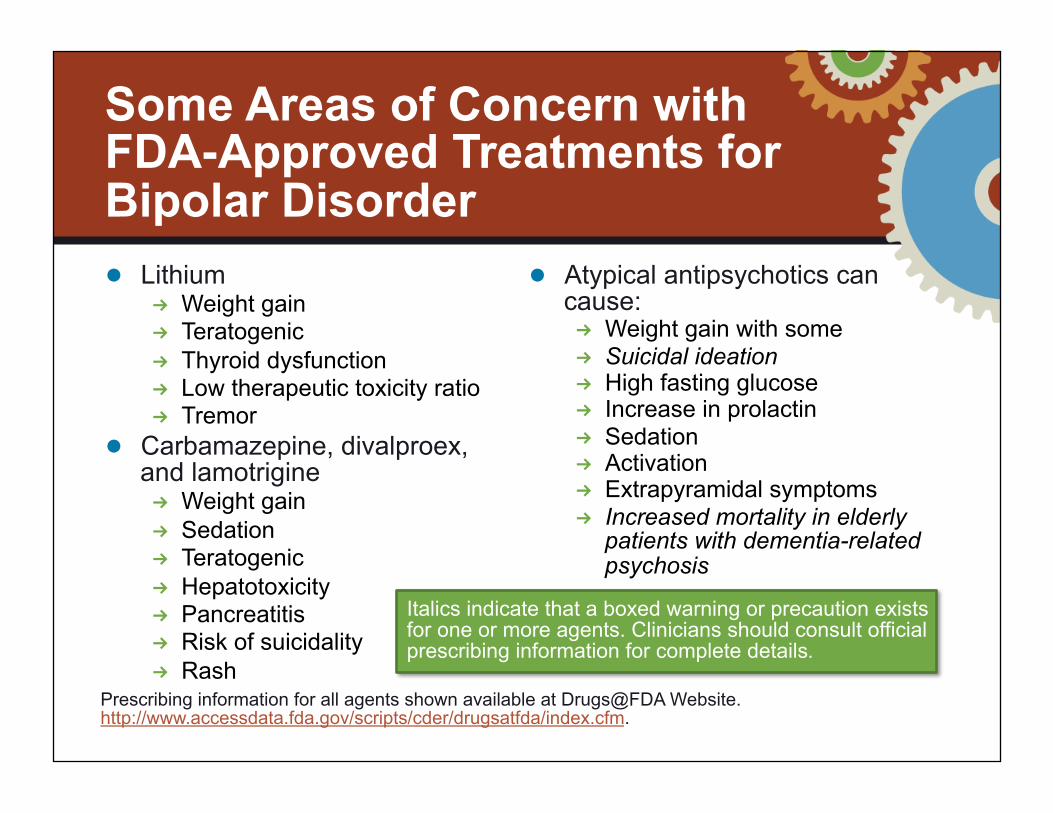
Some Areas of Concern with FDA-Approved Treatments for Bipolar Disorder ● Lithium
! Weight gain ! Teratogenic ! Thyroid dysfunction ! Low therapeutic toxicity ratio ! Tremor
● Carbamazepine, divalproex, and lamotrigine ! Weight gain ! Sedation ! Teratogenic ! Hepatotoxicity ! Pancreatitis ! Risk of suicidality ! Rash
● Atypical antipsychotics can cause: ! Weight gain with some ! Suicidal ideation ! High fasting glucose ! Increase in prolactin ! Sedation ! Activation ! Extrapyramidal symptoms ! Increased mortality in elderly
patients with dementia-related psychosis
Prescribing information for all agents shown available at Drugs@FDA Website. http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm.
Italics indicate that a boxed warning or precaution exists for one or more agents. Clinicians should consult official prescribing information for complete details.

Recent Labs
● You note recent labs done by her PCP ! Comprehensive metabolic panel:
Normal ! Glycosylated hemoglobin: Normal ! TSH and T4: Normal ! Lithium level: 0.6 mmol/L ! Total cholesterol: 225 mg/dL ! Remainder of lipid panel not done
TSH = thyroid stimulating hormone; T4 = thyroxine
Plan
● You have her ! Taper off olanzapine ! Start lurasidone 20 mg/day ! Returns for follow-up in two weeks

Sleep History
● Describes her sleep as fitful, more so in the last six months
● Reports that her mouth is dry upon awakening, and sometimes she has a headache
● Has fallen asleep while driving in the last three months, narrowly avoiding a car crash
● Unknown whether she snores: she lives alone and has had no bed partner in a year
MVA = motor vehicle accident
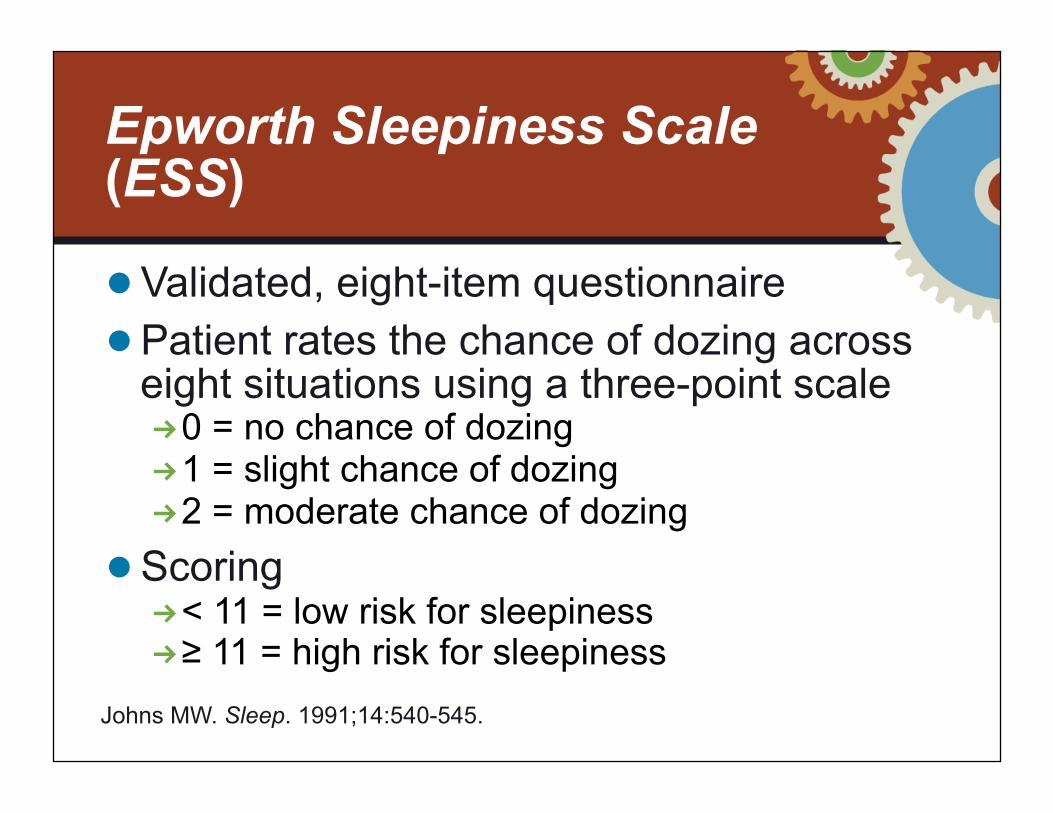
Epworth Sleepiness Scale (ESS)
● Validated, eight-item questionnaire ● Patient rates the chance of dozing across
eight situations using a three-point scale ! 0 = no chance of dozing ! 1 = slight chance of dozing ! 2 = moderate chance of dozing
● Scoring ! < 11 = low risk for sleepiness ! ≥ 11 = high risk for sleepiness
Johns MW. Sleep. 1991;14:540-545.

ESS Score
● She completes an ESS ● Her score is 15
ESS = Epworth Sleepiness Scale

Excessive Sleepiness (ES)
● A cardinal symptom of ! Insufficient time allocated for sleep ! Sleep-wake disorders ! Medical and psychiatric comorbidities ! Sedating medications
● Often described by patients as fatigue or feeling tired ● Associated with
! Reduced cognitive performance ! Increased risk of motor vehicle accidents ! Increased risk of errors on the job occupational injury
● Underdetected
Roth T, et al. Curr Med Res Opin. 2010 Dec;26 Suppl 2:S3-S24. PMID: 21077746.
Sleep Affects Mood; Mood Affects Sleep ● Although the mechanisms are unclear, there appears to
be a strong association between the circadian system and mood regulation, as supported by the following lines of evidence1,2
! Genetic studies have identified polymorphisms in individual circadian genes in humans which associate particularly with bipolar disorder, and to a lesser extent for recurrent depressive disorders2
! Some therapies used for the treatment of mood disorders are known to modulate circadian rhythms2
! Example: Lithium, produces a strong, phase delay in rhythms, and there is evidence suggesting that its therapeutic actions are dependent upon this circadian effect
Harvey AG. Annu Rev Clin Psychol. 2011;7:297-319. PMID: 21166537. McClung CA. Eur Neuropsychopharmacol. 2011;21(Suppl 4):S683-S693. PMID: 21835596.
Strategies to Address ES
● Sleep hygiene ● Alerting agents
Sleep Hygiene: AASM “Healthy Habits of Good Sleep”
American Academy of Sleep Medicine [AASM]. http://yoursleep.aasmnet.org/Hygiene.aspx.
● Don’t go to bed unless you are sleepy.
● If you are not asleep after 20 minutes, then get out of the bed.
● Begin rituals that help you relax each night before bed.
● Get up at the same time every morning; even on weekends and holidays.
● Get a full night’s sleep on a regular basis.
● Avoid taking naps if you can. ● Keep a regular schedule. ● Don’t read, write, eat, watch TV, talk
on the phone, or play cards in bed.
● Do not have any caffeine after lunch.
● Do not have a beer, a glass of wine, or any other alcohol within six hours of your bedtime.
● Do not have a cigarette or any other source of nicotine before bedtime.
● Do not go to bed hungry, but don’t eat a big meal near bedtime either.
● Avoid any tough exercise within six hours of your bedtime.
● Avoid sleeping pills, or use them cautiously.
● Try to get rid of or deal with things that make you worry.
● Make your bedroom quiet, dark, and a little bit cool.

Alerting Agents for ES
1. PI for modafinil. Drugs@FDA Website. 2011. 2. PI for armodafinil. Drugs@FDA Website. 2012.
● For patients with excessive sleepiness, alerting agents can be considered ● Modafinil1 and armodafinil2 are FDA-
approved to improve wakefulness in adult patients with excessive sleepiness associated with treated obstructive sleep apnea (OSA), narcolepsy, or shift work disorder (SWD)

Polysomnography (PSG)
● Sleep efficiency over a 7-hour recording: 75%
● Apnea-hypopneas index (AHI): 35 obstructive breathing events per hour of sleep
● 200 arterial oxygen desaturations below 90%
● Absent slow-wave sleep and excess stage 1 sleep

Correct Diagnosis
● Obstructive sleep apnea (OSA)
Clinical Pearl Avoid assuming that sleepiness in a patient with bipolar disorder is a residual symptom that is related to just the mood disorder or its therapy. Work up these patients for a sleep-wake disorder – just as you would any other patient.

Clues to OSA Diagnosis
● Dosing in the waiting room ● Physical exam showed posterior pharnyx
not visible ● Dry mouth upon awakening ● Near MVA ● ESS score high

OSA in Bipolar Disorder
● A large, telephone-based survey showed that in populations with severe and moderate daytime sleepiness, both bipolar disorder (6.0% and 3.9%, respectively) and OSA (6.7% and 4.8%, respectively) occurred significantly more frequently than in populations with no daytime sleepiness
● Obesity is a major risk factor for the development of OSA and may be critically important in bipolar populations who are taking medications that can cause weight gain
OSA = obstructive sleep apnea Ohayon MM, et al. Arch Intern Med. 1997;157(22):2645-2652. PMID: 9531234.

Follow-Up
● Treated with an alerting agent ● Placed on CPAP, with good adherence and
complete resolution of her chief complaint of “just don’t feel like doing anything”
● Now she feels well enough that she has returned to work delivering pizza late at night: ! Job requires her to work until 2:00 a.m. ! She has been working this job for two weeks already
CPAP = continuous positive airway pressure

CPAP Compliance
● Up to 50% of patients with OSA reject CPAP treatment option or discontinue use within the first week
● 12% – 25% of the remaining patients may be expected to have discontinued its use at 3 years
● CPAP compliance ! Improves health outcomes ! Improves quality of life indicators ! Reduces healthcare utilization ! Improves chronic conditions, e.g., CHF, COPD, HTN
CPAP = continuous positive airway pressure; OSA = obstructive sleep apnea; CHF = congestive heart failure; COPD = chronic obstructive pulmonary disease; HTN = hypertension. Englemen HM, Wild MR. Sleep Med Rev. 2003;7(1):81-99. PMID: 12586532.

Conclusion
● After recognizing how connected her sleep and her mood are, she agrees to start looking for another job
● She continues to do so well at her current job that when there is an opening for a daytime shift manager, she takes it
● She continues to do well for the next 12 months

Clinical Connections
● Work-up sleep complaints in patients with mood disorders just as you would in any other patient
● Use validated tools to measure the severity of sleep symptoms and their impact on functioning
● Counsel patients with bipolar disorder on how poor sleep can affect their mood symptoms
● Manage sleep disorders in patients with bipolar disorder in accordance with recommendations from the American Academy of Sleep Medicine
Questions & Answers

Co-sponsored by