Embed Size (px)
Citation preview

lable at ScienceDirect
Acta Anaesthesiologica Taiwanica xxx (2014) 1e3
Contents lists avai
Acta Anaesthesiologica Taiwanica
journal homepage: www.e-aat .com
Case Report
Co-presentation of Tapia’s syndrome and pressure alopeciadA rareevent after septorhinoplasty: A case report and literature review
Jahangir Ghorbani 1, Shideh Dabir 2*, Gilda Givehchi 3, Mohammadreza Najafi 4
1Department of Otolaryngology Head and Neck Surgery, Chronic Respiratory Diseases Research Center, National Research Institute of Tuberculosis and LungDiseases, Masih Daneshvari Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
2Department of Anesthesiology and Critical Care, Tracheal Diseases Research Center, National Research Institute of Tuberculosis and Lung Diseases, MasihDaneshvari Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran
3Department of Otolaryngology Head and Neck Surgery, Amir Alam Hospital, Tehran University of Medical Sciences, Tehran, Iran4Department of Otolaryngology Head and Neck Surgery, National Research Institute of Tuberculosis and Lung Diseases, Masih Daneshvari Hospital, Shahid
Beheshti University of Medical Sciences, Tehran, Iran
a r t i c l e i n f o
Article history:Received 1 June 2013Accepted 11 September 2013
Key words:alopecia;general anesthesia;hypoglossal nerve injuries;rhinoplasty;vocal cord paralysis
Conflicts of interest: All contributing authors declar* Corresponding author. Department of Anesthesio
pital, Darabad, Niavaran, Tehran 1955841452, Iran.E-mail address: [email protected] (S. Dabir).
http://dx.doi.org/10.1016/j.aat.2014.02.0011875-4597/Copyright � 2014, Taiwan Society of Anes
Please cite this article in press as: Ghorbseptorhinoplasty: A case report and literatu
a b s t r a c t
Tapia’s syndrome and pressure alopecia (PA) are two rare but distressing complications associated withorotracheal intubation and positioning of the head during surgery. To our knowledge, simultaneousoccurrence of both complications after surgery has not been previously reported. To avoid these dis-turbing complications, the mechanisms of the injury and the preventive measures should be recognizedby anesthesiologists and surgeons. We herein present the case of Tapia’s syndrome together with PAfollowing open septorhinoplasty under uncomplicated endotracheal general anesthesia in a 27-year-oldman. We review other case reports and discuss the potential underlying mechanisms of injury.
Copyright � 2014, Taiwan Society of Anesthesiologists. Published by Elsevier Taiwan LLC. All rightsreserved.
1. Introduction
Tapia’s syndrome and pressure alopecia (PA) are two rarecomplications related to anesthesia that may cause considerablepsychological distress to the patient for a long time, especiallywhen they occur after cosmetic surgeries. Therefore, both anes-thesiologists and surgeons should be aware of the possible mech-anisms of the injury and the importance of the preventivemeasures.
Tapia’s syndrome, first described in 1904 by the Spanishotorhinolaryngologist Antonio Garcia Tapia, is characterized bycombined unilateral paralysis of the hypoglossal nerve and therecurrent laryngeal branch of the vagus nerve secondary to anextracranial injury.1,2 Tapia’s syndrome is a rare consequence oforotracheal general anesthesia, with half of the cases reportedlyoccurring after rhinoplasty or septorhinoplasty.3,4 PA, firstdescribed by Abel and Lewis in 1960, is localized pressure-inducedischemia to the scalp mostly due to prolonged head immobilization
e no conflicts of interest.logy, Masih Daneshvari Hos-
thesiologists. Published by Elsevie
ani J, et al., Co-presentatiore review, Acta Anaesthesiolo
during lengthy periods of general anesthesia, and is mostcommonly reported after cardiac surgery.5,6 To our knowledge, PAafter septorhinoplasty as well as simultaneous occurrence of bothTapia’s syndrome and pressure alopecia has not been previouslydescribed. We herein present the case of Tapia’s syndrome togetherwith PA following open septorhinoplasty under uncomplicatedendotracheal general anesthesia in a 27-year-old man. Other casereports are also reviewed, and the potential underlying mecha-nisms of injury are discussed.
2. Case report
A 27-year-old man (weight: 90 kg and height: 186 cm), Amer-ican Society of Anesthesiologists physical status Class I, wasadmitted for septorhinoplasty due to nasal obstruction withexternal deformity. Administration of general anesthesia and oro-tracheal intubationwere performedwithout difficulty. AMacintoshblade Number 4 laryngoscope was used and an 8-mm armoredcuffed tracheal tube was gently placed in the trachea on the firstattempt, and was fixed to the left corner of the mouth. The cuff wasinflated with 3 mL of air where no audible leak was heard, and thelungs were easily ventilated with intermittent positive pressureventilation. A small moistened throat pack was then gently placedin the lower pharynx using laryngoscope and Magill forceps. The
r Taiwan LLC. All rights reserved.
n of Tapia’s syndrome and pressure alopeciadA rare event aftergica Taiwanica (2014), http://dx.doi.org/10.1016/j.aat.2014.02.001

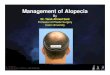
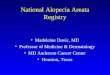
Fig. 2. Localized alopecia 1 week after septorhinoplasty.
J. Ghorbani et al.2
open septorhinoplasty was performed by otolaryngology residentsin the supine position with the head and trunk slightly elevated.Topical phenylephrine 0.25% was applied for nasal mucosaldecongestion and 10 mL solution of 1% lidocaine/1:100,000epinephrine was injected in the septum, sites of incision, andosteotomy line. Systolic arterial pressure was kept between80mmHg and 90mmHg for controlled hypotensive anesthesia. Thepatient was maintained hemodynamically stable and welloxygenated throughout the uneventful 6 hours of surgery. At theend of the surgery, the patient was extubated once fully awake.
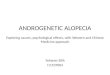
The 1st postoperative day was complicated by the patient’scomplains of pain and tenderness on the occipital area, difficulty inswallowing and speaking, hoarseness, and aspiration. A physicalexamination revealed localized swelling and tenderness in theocciput, and marked deviation of the tongue to the left side duringprotrusion (Fig. 1). Paramedian immobile true left vocal cordwithout edema or bruising was detected during laryngoscopy. Thepharynx and soft palate were normal. A complete neurologicalevaluation showed normal results. A 2 cm � 2 cm skin redness wasdetected on the buttock area. Brain magnetic resonance imaging(MRI) showed no abnormality. The patient empirically received50 mg prednisolone, and vitamins B1 and B12 daily for 7 days. Thepatient refused our recommendation for speech and swallowingtherapy. One week after the operation, he complained of progres-sive hair loss over the previously tender area, and an area of alo-pecia (3.5 cm � 1.5 cm) was detected in the occiput region (Fig. 2).
There was significant improvement in swallowing and aspira-tion problemswithin 3months after the surgery with no detectableimprovement in the tongue or vocal cord function. Six months afterthe surgery, functions of the tongue and vocal cord were alsocompletely resolved and normal hair regrowth was noted in theaffected area, and the patient was happy with the surgical outcome.
3. Discussion
Based on clinical signs, normal MRI findings, and progressiverecovery of lingual and laryngeal functions along with hairregrowth within 6 months after the surgery, our patient wasdiagnosed with concurrent Tapia’s syndrome and PA.
Tapia’s syndrome is concomitant ipsilateral paralysis of thevocal cord and muscles of the tongue that causes hoarseness, dif-ficulty in swallowing, uncontrolled tongue movements, disturbedspeech, and ipsilateral deviation of the tongue to the denervatedside on protrusion and to the contralateral side on rest.3,4 Most ofthe cases were unilateral; however, bilateral involvement of the
Fig. 1. After surgery the tongue was deviated to the left side during protrusion.
Please cite this article in press as: Ghorbani J, et al., Co-presentatioseptorhinoplasty: A case report and literature review, Acta Anaesthesiolo
nerves has also been reported.2,4 The progressive recovery oflingual and laryngeal function by our patient and in the majority ofreported cases support a neuropraxic type of nerve damage.7,8
Injury to the hypoglossal and the recurrent laryngeal nerves byendotracheal intubation or positioning of the head during surgeryis the main mechanism of Tapia’s syndrome.4,9 Anatomically, thevagus and hypoglossal nerves lie near each other at the base of thetongue and in the pyriform fossa and run on the lateral prominenceof the anterior surface of the transverse process of the first cervicalvertebra between the greater horn of the hyoid bone and the lig-amentum stylohyoideum. The crossing site of the nerves may becompressed by the endotracheal tube against these rigid anatom-ical tissues, leading to simultaneous nerve injury. Moreover, hy-perextension or excessive anterioreposterior and lateral flexion ofthe patient head during surgery may also stretch or press thesenerves between the tube and these hard tissues. The frequentlyinvolved operations were septoplasty and septorhinoplasty, maybebecause of the proximity of the surgical sites to the airway, whichcan easily displace the endotracheal tube.3,4,10 However, Tapia’ssyndrome following an orthognathic surgery,3 a shoulder surgery,11
a surgical repair of a fractured mandible,12 a cervical lam-inectomy,13 thoracotomy,14 and cardiac surgery1,15 was alsodescribed. In these cases, the most likely causes were a directcompression of the recurrent laryngeal and hypoglossal nerves bylaryngoscope or orotracheal tube, excessive pressure to the nervesby inflation of the cuff in the larynx, malposition or displacement ofthe tracheal tube, extubation with inflated cuff, or a prolongedstretch of these nerves following an excessive hyperextension orflexion of the head during surgery. Throat packing also has a verysignificant role in the nerve injury in septorhinoplasty, as itsplacement in the hypopharynx may help in compression of thenerves upon the endotracheal tube and pharyngeal wall.4,7 Teseiet al7 reported a unilateral Tapia’s syndrome following endotra-cheal intubation after rhinoplasty performed under general anes-thesia. In their opinion, compression of the nerves by theendotracheal tube upon the throat pack in the oropharynx, at thepoint where the vagus and hypoglossal cross, and also a prolongedstretching by excessive anterior and lateral flexion of the head weretwo probable mechanisms of nerve injury. Similarly, Lykoudis andSeretis4 presented another case of Tapia’s syndrome after rhino-plasty with general anesthesia due to excessive pressure fromthroat packing. Likewise, Yavuzer et al9 described a case of unilat-eral Tapia’s syndrome after septorhinoplasty caused by compres-sion of the nerves by inflation of the cuff within the larynx.9 Bo�gaand Aktas16 also presented a case of unilateral Tapia’s syndrome
n of Tapia’s syndrome and pressure alopeciadA rare event aftergica Taiwanica (2014), http://dx.doi.org/10.1016/j.aat.2014.02.001

Tapia’s syndrome together with PA 3
after septorhinoplasty performed with intratracheal intubation.Moreover, Cinar et al10 reported a case of bilateral Tapia’s syndromeafter general anesthesia following rhinoplasty. They speculated thata change in the position of the neck in combination withcompression by the endotracheal tube was a probable mechanism.Therewas also a case of Tapia’s syndrome following cardiac surgerycaused by the rhinopharyngeal hematoma at the crossing of thevagus nerve and the hypoglossal nerve due to the placement of anasogastric tube.17
Postoperative PA has been most commonly reported followingcardiac surgery the most commonly reported finding followingcardiac surgery. Cases of PA have also been reported after prolongedbreast, abdominal, orthognathic, plastic, and ophthalmic surgeryunder general anesthesia.5,6,18,19 Interestingly, we found no re-ported cases of PA after rhinoplasty or septorhinoplasty. Thepossiblemechanism of PA is localized pressure-induced ischemia tothe scalp, usually in the occiput region, due to prolonged constantpressure on the scalp as a result of prolonged head immobilizationduring long periods of general anesthesia. The constant pressure onthe scalp may cause localized ischemic injuries to the blood vesselsand hair follicles.6,20 Furthermore, intraoperative hypotension,hypoxemia, massive blood loss, the use of vasoconstrictors, Tren-delenburg position, and cardiopulmonary bypass may exacerbateischemic changes on the scalp.5,6 PA usually manifests as swelling,erythema, tenderness, or ulceration of the scalp within the first fewpostoperative days, followed by a distinct area of alopecia within afew weeks after surgery.5
In our case, we believe that the most probable predisposingfactor for the nerve palsies and PA was prolonged (6 hours)malposition of the patient’s head fixed in one position, and there-fore prolonged pressure on the scalp during the lengthy surgicalprocedure. With regard to postoperative pressure-related hair lossin the occiput region and redness on the buttock, we attribute theclinical course to the prolonged immobilization of the body of thepatient on the operating table, along with a stretching injury to therecurrent laryngeal and hypoglossal nerves due to a prolongedinadvertent hyperextension of the head probably for ease of nasalexposure during surgery. In the present case, even though oro-tracheal intubation was not traumatic or complicated, there alsomight be a possibility of a long-lasting undetected displacement ofthe tube under the surgical drapes that resulted in compression ofboth nerves between the endotracheal tube and throat pack.Moreover, the development of both complications may be aggra-vated by the use of prolonged hypotensive anesthesia, intra-operative use of topical vasoconstrictors, or forces transmitted tothe occipital area during osteotomies. Inappropriate cuff pressure isalso another important factor in the occurrence of intubation-related neuropathy. However, in our patient, because the cuff wasnot overinflated and nitrous oxide was not used, despite using anarmored tube with low-volume and high-pressure cuff, we did notcheck the intracuff pressure during anesthesia.
Both Tapia’s syndrome and PA almost always have a sponta-neous and complete recovery within a few months.2,6 However,rare cases of permanent hair loss have also been reported.18 There isno established treatment for these complications. However, in pa-tients with Tapia’s syndrome, supportive treatment with a shortcourse of systemic steroids and vitamin B complexes has been usedto reduce the duration of cranial nerve paralysis.4,16 To avoid thestressful but preventable problems, the importance of preventive
Please cite this article in press as: Ghorbani J, et al., Co-presentatioseptorhinoplasty: A case report and literature review, Acta Anaesthesiolo
measures should be recognized by anesthesiologists and surgeons.The incidence can be decreased by proper positioning of the headduring surgery, early detection and correction of the head malpo-sition, carefully performing the routine maneuvers of airwaymanagement, appropriate fixation of orotracheal tube to preventinadvertent displacement, proper placement and amount of throatpacking in the oropharynx, and a shortened operating and intu-bating time. Regular intraoperative head repositioning is also rec-ommended to avoid persistent occipital pressure and alopecia.4,5
In our case, because of early diagnosis, close follow up, constantreassurance and sympathy, and the patient’s satisfaction with sur-gical results, symptoms were well tolerated and we did notencounter legal issues.
In conclusion, in the presented case, prolonged malposition ofthe patient’s head, in combination with endotracheal tubedisplacement may have contributed to the occurrence of Tapia’ssyndrome and PA. Once septorhinoplasty is performed underendotracheal general anesthesia, both anesthesiologists and sur-geons should be aware of these complications.
References
1. Nalladaru Z, Wessels A, DuPreez L. Tapia’s syndromeda rare complicationfollowing cardiac surgery. Interact Cardiovasc Thorac Surg 2012;14:131e2.
2. Turan I, Yildirim ZK, Tan H. Bilateral Tapia syndrome secondary to oropha-ryngeal intubation. J Neurosurg Anesthesiol 2012;24:78.
3. Ota N, Izumi K, Okamoto Y, Toshitani K, Nakayama K, Fukuzawa H, et al. Tapia’ssyndrome following the orthognathic surgery under general anaesthesia. J OralMaxillofac Surg Med Pathol 2013;25:52e4.
4. Lykoudis EG, Seretis K. Tapia’s syndrome: an unexpected but real complicationof rhinoplasty: case report and literature review. Aesthetic Plast Surg 2012;36:557e9.
5. Davies KE, Yesudian P. Pressure alopecia. Int J Trichology 2012;4:64e8.6. Dominguez E, Eslinger MR, McCord SV. Postoperative (pressure) alopecia:
report of a case after elective cosmetic surgery. Anesth Analg 1999;89:1062e3.7. Tesei F, Poveda LM, Strali W, Tosi L, Magnani G, Farneti G. Unilateral laryngeal
and hypoglossal paralysis (Tapia’s syndrome) following rhinoplasty in generalanaesthesia: case report and review of the literature. Acta Otorhinolaryngol Ital2006;26:219e21.
8. Hung NK, Lee CH, Chan SM, Yeh CC, Cherng CH, Wong CS, et al. Transientunilateral hypoglossal nerve palsy after orotracheal intubation for generalanesthesia. Acta Anaesthesiol Taiwan 2009;47:48e50.
9. Yavuzer R, Basterzi Y, Ozköse Z, Yücel Demir H, Yilmaz M, Ceylan A. Tapia’ssyndrome following septorhinoplasty. Aesthetic Plast Surg 2004;28:208e11.
10. Cinar SO, Seven H, Cinar U, Turgut S. Isolated bilateral paralysis of the hypo-glossal and recurrent laryngeal nerves (bilateral Tapia’s syndrome) aftertransoral intubation for general anesthesia. Acta Anaesthesiol Scand 2005;49:98e9.
11. Boisseau N, Rabarijaona H, Grimaud D, Raucoules-Aimé M. Tapia’s syndromefollowing shoulder surgery. Br J Anaesth 2002;88:869e70.
12. Kashyap SA, Patterson AR, Loukota RA, Kelly G. Tapia’s syndrome after repair ofa fractured mandible. Br J Oral Maxillofac Surg 2010;48:53e4.
13. Lim KJ, Kim MH, Kang MH, Lee HM, Park EY, Kwon KJ, et al. Tapia’s syndromefollowing cervical laminoplastyda case report. Korean J Anesthesiol 2013;64:172e4.
14. Gelmers HJ. Tapia’s syndrome after thoracotomy. Arch Otolaryngol 1983;109:622e3.
15. Sotiriou K, Balanika M, Anagnostopoulou S, Gomatos C, Karakitsos D,Saranteas T. Postoperative airway obstruction due to Tapia’s syndrome aftercoronary bypass grafting surgery. Eur J Anaesthesiol 2007;24:378e9.
16. Bo�ga I, Aktas S. Treatment, classification, and review of Tapia syndrome.J Craniofac Surg 2010;21:278e80.
17. Rotondo F, De Paulis S, Modoni A, Schiavello R. Peripheral Tapia’s syndromeafter cardiac surgery. Eur J Anaesthesiol 2010;27:575e6.
18. Lypka MA, Yamashita DD, Urata MM. Postoperative alopecia followingorthognathic surgery. J Oral Maxillofac Surg 2008;66:1957e8.
19. Kosanin RM, Riefkohl R, Barwick WJ. Postoperative alopecia in a woman after alengthy plastic surgical procedure. Plast Reconstr Surg 1984;73:308e9.
20. Yoon TY. A clinico-pathological study of pressure alopecia. Korean J Dermatol2001;39:1370e6.
n of Tapia’s syndrome and pressure alopeciadA rare event aftergica Taiwanica (2014), http://dx.doi.org/10.1016/j.aat.2014.02.001