Embed Size (px)
Citation preview

CNS PathologyCNS Pathology
RT 91 RT 91
Spring 2012Spring 2012
11

INFLAMMATORY INFLAMMATORY DISEASE OF CNSDISEASE OF CNS
22

MeningitisMeningitis Inflammation fo the meningeal coverings of the brain and Inflammation fo the meningeal coverings of the brain and
spinal cordspinal cord
Can be caused by Can be caused by Bacteria, virus and other organisms via blood or lymphBacteria, virus and other organisms via blood or lymph Trauma, pentrating wounds or adjacent structures infectedTrauma, pentrating wounds or adjacent structures infected
Bacterial is most common (can cause hydrocephalus)Bacterial is most common (can cause hydrocephalus) Three types pus forming bacteria:Three types pus forming bacteria:
Meningococci - infantsMeningococci - infants Streptococci - childrenStreptococci - children Pneumococci- adultsPneumococci- adults
Tubercle bacillusTubercle bacillus
33

Different Pathogens causing Different Pathogens causing MeningitisMeningitis
FungiFungi Chronic meningitisChronic meningitis Often associated with AIDS and immunodepressant Often associated with AIDS and immunodepressant
drug therapydrug therapy VirusVirus
Viral meningitis can be caused by mumps, poliovirus Viral meningitis can be caused by mumps, poliovirus and herpes simplexand herpes simplex
BacteriaBacteria Most commonMost common Bacteria release toxins that destroy meningeal cells Bacteria release toxins that destroy meningeal cells
stimulating immune & inflammatory reactionsstimulating immune & inflammatory reactions
44

Acute Meningitis Acute Meningitis Clinical SymptomsClinical Symptoms
FeverFever HeadacheHeadache Stiff neckStiff neck VomitingVomiting Changes in LOCChanges in LOC Severely ill in 24 hoursSeverely ill in 24 hours RashRash Chronic symptoms are Chronic symptoms are
the same but occur over the same but occur over weeksweeks
55

Diagnosis of MeningitisDiagnosis of Meningitis Brain CTBrain CT
Rule out contraindications to do a spinal tapRule out contraindications to do a spinal tap
Spinal tapSpinal tap LP to remove CSF to send to labLP to remove CSF to send to lab
Sometimes MRI is used Sometimes MRI is used
Is most sensitive modality for demonstrating pia and Is most sensitive modality for demonstrating pia and arachnoid arachnoid
Treatment includes antibiotics and if secondary Treatment includes antibiotics and if secondary to encephalitis: antiviral drugsto encephalitis: antiviral drugs
66

Radiographic AppearanceRadiographic Appearance
Initially meninges Initially meninges show vascular show vascular congestion, edema congestion, edema and minute and minute hemorrhageshemorrhages
MRI and CT scans MRI and CT scans could appear normal could appear normal if appropriate therapy if appropriate therapy is done right awayis done right away Meningitis as a result of a Staph infection
77

EncephalitisEncephalitis
Infection of the brain tissue that is viralInfection of the brain tissue that is viral May occur subsequent to chickenpox, small May occur subsequent to chickenpox, small
pox, influenza and measlespox, influenza and measles May be caused by mosquitoes and herpesMay be caused by mosquitoes and herpes
Survival rates depend of cause of the Survival rates depend of cause of the disease (can be fatal)disease (can be fatal) 30% of cases in children30% of cases in children When caused by herpes it is often fatalWhen caused by herpes it is often fatal
88

EncephalitisEncephalitis
MRI is modality of MRI is modality of choicechoice
Results in cerebral Results in cerebral edema and edema and hemorrhagic lesionshemorrhagic lesions
More serious than More serious than meningitis because it meningitis because it frequently develops frequently develops permanent neurologic permanent neurologic disabilitiesdisabilities
99

Encephalitis:Encephalitis:Symptoms and TreatmentSymptoms and Treatment
Symptoms:Symptoms: HeadacheHeadache
MalaiseMalaise
ComaComa
FeverFever
SeizuresSeizures
Treatment:Treatment: Treated with antiviral Treated with antiviral
medicationsmedications
Herpes induced is Herpes induced is treated with Acyclovirtreated with Acyclovir
• Interferes with DNA Interferes with DNA synthesis and inhibits synthesis and inhibits viral replicationviral replication
1010

CONGENITAL CONGENITAL DISEASES OF CNSDISEASES OF CNS
1111

Spinal BifidaSpinal Bifida Is a congenital diseaseIs a congenital disease
Bony neural arch that not completely closedBony neural arch that not completely closed
Most common in lumbar regionMost common in lumbar region May or may not herniate through openingMay or may not herniate through opening
Can range in risk from treatable to life threateningCan range in risk from treatable to life threatening
Can be diagnosed in utero Can be diagnosed in utero With amniocentesisWith amniocentesis UltrasoundUltrasound Elevated beta fetoprotein in mother’s bloodElevated beta fetoprotein in mother’s blood
1212

Types of Spinal BifidaTypes of Spinal Bifida
MeningoceleMeningocele Only the meninges protrudeOnly the meninges protrude Local defect of bone & duraLocal defect of bone & dura
MyeloceleMyelocele Protrusion of spinal cordProtrusion of spinal cord
MeningomyeloceleMeningomyelocele Protrusion of meninges and Protrusion of meninges and
spinal cord into the skin of the spinal cord into the skin of the backback
Most seriousMost serious
Spinal bifida occultaSpinal bifida occulta No protrusion of spinal No protrusion of spinal
contentscontents Least severeLeast severe 1313

Radiographic AppearanceRadiographic Appearance
Can be demonstrated Can be demonstrated with CT, MRI and with CT, MRI and myelographymyelography Prenatally with Prenatally with
ultrasound (in utero)ultrasound (in utero)
Large bony defectsLarge bony defects
Herniated spinal Herniated spinal contentscontents
Meningomyelocele
Meningocele
1414

MeningomyeloceleMeningomyelocele
Most serious Most serious Affected PT’s have Affected PT’s have
severe neurologic severe neurologic deficitsdeficits ParaplegiaParaplegia Diminished control of Diminished control of
lower limbs, bladder lower limbs, bladder and bowelsand bowels
Hydrocephalus is Hydrocephalus is commoncommon
1515

Spinal Bifida ImagingSpinal Bifida Imaging
1616

Spinal Bifida TreatmentSpinal Bifida Treatment
Can be surgically repairedCan be surgically repaired Neurological damage is permanent still and cannot be Neurological damage is permanent still and cannot be
reversedreversed
Most measures are supportive rather than Most measures are supportive rather than correctivecorrective Physical therapyPhysical therapy Physical supportsPhysical supports BracesBraces SplintsSplints
1717

CRANIAL AND SPINAL CRANIAL AND SPINAL FRACTURESFRACTURES
1818

Cranial FracturesCranial Fractures Cerebral fractures usually occurs to Cerebral fractures usually occurs to
fractures of the calvaria of the skullfractures of the calvaria of the skull 3 types of cranial fractures3 types of cranial fractures
Linear- straight and sharply definedLinear- straight and sharply defined• Is 80% of all cranial fracturesIs 80% of all cranial fractures
Depressed- curvilinear densityDepressed- curvilinear density
Basilar- Air fluid levels are indicative Basilar- Air fluid levels are indicative • Hard to diagnosis radiographicallyHard to diagnosis radiographically
1919

Cranial FracturesCranial Fractures
Location of FX is more important that the Location of FX is more important that the extent of the FXextent of the FX If FX crosses artery a bleed can occur If FX crosses artery a bleed can occur
causing a hematomacausing a hematoma
Fx that enters mastoid air cells or sinus can Fx that enters mastoid air cells or sinus can cause an infection that can result incause an infection that can result in• Meningitis Meningitis • EncephalitisEncephalitis
2020

Linear FracturesLinear Fractures Non branching lines that Non branching lines that
are intensely radiolucentare intensely radiolucent
Vascular markings are Vascular markings are occasionally mistaken for occasionally mistaken for fracturesfractures
Fracture appears more Fracture appears more translucent and translucent and transverses the full transverses the full thickness of skullthickness of skull
SuturesSutures
2121

Linear Skull FXLinear Skull FX
2222

Depressed FractureDepressed Fracture The fractured edges The fractured edges
overlapoverlap
Usually caused by a high Usually caused by a high velocity impact with a velocity impact with a small objectsmall object
Can cause bleeding into Can cause bleeding into subarachnoid spacesubarachnoid space
Best demonstrated with Best demonstrated with CR tangential to the FXCR tangential to the FX
2323

Depressed Skull FXDepressed Skull FX
2424

Basilar FractureBasilar Fracture Very difficult to demonstrate with x-rayVery difficult to demonstrate with x-ray
Air fluid levels in sphenoid sinusesAir fluid levels in sphenoid sinuses Clouding of mastoid air cellsClouding of mastoid air cells
Often X-table lateral is done to demonstrate thisOften X-table lateral is done to demonstrate this CT & MRI are most often used for this type CT & MRI are most often used for this type
2525

Compression Fracture of spineCompression Fracture of spine
Most frequent type of injury involving Most frequent type of injury involving vertebral bodyvertebral body
Generally occurs in T and L-spineGenerally occurs in T and L-spine T11- T12 and T12 – L1T11- T12 and T12 – L1
Damage is usually limited to the upper Damage is usually limited to the upper portion of the vertebral body, particularly to portion of the vertebral body, particularly to the anterior marginthe anterior margin
2626

Compression FX of SpineCompression FX of Spine
2727

Compression FX of SpineCompression FX of Spine
2828

Hangman’s FractureHangman’s Fracture
FX of the arch of the 2FX of the arch of the 2ndnd c-spine vertebrae c-spine vertebrae Usually accompanied by anterior Usually accompanied by anterior
subluxation of the 2subluxation of the 2ndnd and 3 and 3rdrd cervical cervical vertebraevertebrae
Sometimes called traumatic spondylosisSometimes called traumatic spondylosis Resulting from acute hyperextension of Resulting from acute hyperextension of
the head & neckthe head & neck Originally seen commonly in hangingsOriginally seen commonly in hangings
Now seen more for MVANow seen more for MVA
2929

Hangman’s FractureHangman’s Fracture
3030

Hangman’s FractureHangman’s Fracture
3131

Jefferson’s FractureJefferson’s Fracture
Comminuted FX of the ring of the atlasComminuted FX of the ring of the atlas First described as a “burst FX” First described as a “burst FX”
Generally occurs as a result of severe axial Generally occurs as a result of severe axial force such as a MVAforce such as a MVA
With this FX particular attn needs to be With this FX particular attn needs to be paid to the transverse longitudinal paid to the transverse longitudinal ligament by reviewing lateral masses on ligament by reviewing lateral masses on the open mouth odontoidthe open mouth odontoid
MRI is preferred method for this ligamentMRI is preferred method for this ligament
3232

Jefferson’s FractureJefferson’s Fracture
3333

Jefferson’s Jefferson’s Fracture Fracture
3434

TRAUMATIC DISEASETRAUMATIC DISEASE
3535

Cerebral ContusionCerebral Contusion Is an injury to the brain tissue caused by a Is an injury to the brain tissue caused by a
movement of the brain within the calvaria movement of the brain within the calvaria after blunt traumaafter blunt trauma
Occurs when brain contacts rough skull Occurs when brain contacts rough skull surfaces such as orbital floor and petrous surfaces such as orbital floor and petrous ridgesridges PT usually loses consciousness and cannot PT usually loses consciousness and cannot
remember traumatic eventremember traumatic event Persitent LOC over 24 hrs is a coma and can Persitent LOC over 24 hrs is a coma and can
be fatalbe fatal3636

CT appearance of CT appearance of Cerebral ContusionCerebral Contusion
CT scans appear as low density areas of edema CT scans appear as low density areas of edema and tissue necrosisand tissue necrosis With or without homogenous density zones reflecting With or without homogenous density zones reflecting
areas of hemorragheareas of hemorraghe Most common sites of injury are frontal and anterior Most common sites of injury are frontal and anterior
temporal regions.temporal regions.
When IV contrast is used it will enhance several When IV contrast is used it will enhance several weeks after injuryweeks after injury
Plays an important role in diagnosisPlays an important role in diagnosis
3737

MR of Cerebral ContusionMR of Cerebral Contusion
Cerebral edema causes high signal Cerebral edema causes high signal intensity on T2 scansintensity on T2 scans
T1 scans may produce high signal regionsT1 scans may produce high signal regions
Diagnosis can also include CT, MRI and Diagnosis can also include CT, MRI and PETPET
3838

Cerebral Cerebral ContusionContusion
Clinical symptoms:Clinical symptoms: DrowsinessDrowsiness ConfusionConfusion AgitiationAgitiation HemiparesisHemiparesis Unequal pupil sizeUnequal pupil size
Treatment:Treatment: PT is hospitalizedPT is hospitalized
• Prevent shockPrevent shock
If there is swelling If there is swelling medication is given to medication is given to decrease cranial decrease cranial pressurepressure
• Control edemaControl edema• Drainage of hematomaDrainage of hematoma
Surgery is usually not Surgery is usually not necessarynecessary
3939

Cerebral ContusionCerebral Contusion
4040

HematomasHematomas Brain trauma often resulting in a hemorrhaging Brain trauma often resulting in a hemorrhaging
from a ruptured vein or arteryfrom a ruptured vein or artery Venous bleeding occurs more slowly than arterial Venous bleeding occurs more slowly than arterial
bleedingbleeding Arterial bleed accumulates fast & causes neurologic Arterial bleed accumulates fast & causes neurologic
symptoms & comasymptoms & coma Both can cause edema in the brain and cause an Both can cause edema in the brain and cause an
increase in intracranial pressureincrease in intracranial pressure
Skull does not allow for expansion and pressure Skull does not allow for expansion and pressure forces brain toward open space (foramen forces brain toward open space (foramen magnum)magnum)
Can result in major consequences & death if not Can result in major consequences & death if not treated quicklytreated quickly
4141

Epidural HematomasEpidural Hematomas
Highest mortality rate of the hematomasHighest mortality rate of the hematomas Even when treated quickly mortality rate is 30%Even when treated quickly mortality rate is 30%
Results from a torn artery and its branchesResults from a torn artery and its branches Most often occurs from a FX of the temporal boneMost often occurs from a FX of the temporal bone 80% of cases conventional radiograph shows fracture80% of cases conventional radiograph shows fracture
Usually meningeal artery with blood pooling Usually meningeal artery with blood pooling between bones of the skull & dura materbetween bones of the skull & dura mater
http://www.youtube.com/watch?v=cVUofakFIyw&feature=related
4242

Epidural HematomaEpidural Hematoma
Usually a shift of midlineToward opposite side
CT shows increased density
Emergency surgicaldecompression is required to relieve cranial pressure 4343

Subdural HematomasSubdural Hematomas
Between the dura mater & arachnoid Between the dura mater & arachnoid meningeal layersmeningeal layers Caused by blunt trauma to frontal or occipital Caused by blunt trauma to frontal or occipital
lobes and can tear subdural veinslobes and can tear subdural veins
Pushes brain away from skull across Pushes brain away from skull across midline (including ventricles)midline (including ventricles)
4444
http://www.youtube.com/watch?v=qO16QXMxBLY&feature=related

Subdural HematomaSubdural Hematoma
Occurs more slowlyBecause it is a venousHemorrhage.
On CT appears as a curvilinear area of Iincreased density on portions or all of the cerebral hemispheres4545

Subdural HematomasSubdural Hematomas
Subacute stage (up to several days)Subacute stage (up to several days) Appears on CT as a decreased density or Appears on CT as a decreased density or
isodense fluid collectionisodense fluid collection
In chronic state (2-3 weeks)In chronic state (2-3 weeks) The surface of the hematoma becomes The surface of the hematoma becomes
concaveconcave Delayed coma con occurDelayed coma con occur
4646

Symptoms of HematomasSymptoms of Hematomas
HeadachesHeadaches
AgitationAgitation
DrowsinessDrowsiness
Gradual radiograph deficitsGradual radiograph deficits
4747

Treatment of HematomasTreatment of Hematomas In small hematomas without inclination to In small hematomas without inclination to
rebleedrebleed the hemorrhage is reabsorbed naturally the hemorrhage is reabsorbed naturally no treatment is necessaryno treatment is necessary
Severe casesSevere cases Require surgical ligationRequire surgical ligation Evacuation of hematoma to prevent herniationEvacuation of hematoma to prevent herniation
Less invasive treatment may includeLess invasive treatment may include Drug therapyDrug therapy Intraventricular catheter to remove CSF, which may Intraventricular catheter to remove CSF, which may
cause herniationcause herniation 4848

Degenerative DiseasesDegenerative Diseases
4949

Herniated DiskHerniated Disk Disks act as shock Disks act as shock absorbersabsorbers
When young nucleus When young nucleus pulposus contains pulposus contains large amount of fluid large amount of fluid to cushion spineto cushion spine
With increased age With increased age the fluid & elasticity the fluid & elasticity decrease leading to decrease leading to degenerative disease degenerative disease and back painand back pain
5050

Herniated DiskHerniated Disk May result from either degenerative disease or May result from either degenerative disease or
traumatrauma
A weakened or torn annulus is subject to ruptureA weakened or torn annulus is subject to rupture Nucleus pulposus protrudes & compresses spinal Nucleus pulposus protrudes & compresses spinal
nerve rootsnerve roots Can prolapse in any direction, sometimes without painCan prolapse in any direction, sometimes without pain When it projects posteriorly there is pain and When it projects posteriorly there is pain and
weakening of muscles supplied by those nervesweakening of muscles supplied by those nerves Most commonly occurs is lower cervical & lumbarMost commonly occurs is lower cervical & lumbar
• Lumbar: Most at L4-L5 and L5 – S1Lumbar: Most at L4-L5 and L5 – S1• Cervical: Most at C6 – C7Cervical: Most at C6 – C7• Thoracic: T9-T12Thoracic: T9-T12
5151

Herniated DiskHerniated Disk
5252

Herniated DiskHerniated Disk
MRI is modality of choiceMRI is modality of choice CT and Myelography can also be usedCT and Myelography can also be used
5353

Symptoms of Herniated DiskSymptoms of Herniated Disk
Sudden weak & severe onset of painSudden weak & severe onset of pain Weakened musclesWeakened muscles
Compression of nerve roots in C-spine:Compression of nerve roots in C-spine: Cause pain and weakness in neck & upper Cause pain and weakness in neck & upper
extremitiesextremities Compression in lumbar in L-spine:Compression in lumbar in L-spine:
Causes pain in hip, posterior thigh, calf and Causes pain in hip, posterior thigh, calf and foot (sciatica)foot (sciatica)
5454

Treatment: Herniated DiskTreatment: Herniated Disk
Conservative treatment:Conservative treatment: Bed rest, analgesics and muscle relaxantsBed rest, analgesics and muscle relaxants Followed by physical therapyFollowed by physical therapy 95% recover is 3 months without surgery95% recover is 3 months without surgery
Surgical interventionSurgical intervention DiskectomyDiskectomy Surgical decompressionSurgical decompression Spinal fusionSpinal fusion LaminectomyLaminectomy
5555

Herniated Disk: FusionHerniated Disk: Fusion
5656

Brain & Spinal Brain & Spinal TumorsTumors
5757

Spinal TumorsSpinal Tumors
Primary tumors are less common is spinal Primary tumors are less common is spinal cord than those of the braincord than those of the brain
Divided into extradural and intraduralDivided into extradural and intradural Intradural further divided intoIntradural further divided into
• Intramedullary (within spinal cord)Intramedullary (within spinal cord) Most common are: Astrocytoma & EpenymomaMost common are: Astrocytoma & Epenymoma
• Extramedullary (outside spinal cord)Extramedullary (outside spinal cord) Most common types of primary spinal neoplasm's Most common types of primary spinal neoplasm's
(>60%) are: Meningiomas and Neurofibromas(>60%) are: Meningiomas and Neurofibromas
5858

Symptoms of Spinal TumorsSymptoms of Spinal Tumors
ExtramedullaryExtramedullary
Similar symptoms as a Similar symptoms as a herniated nucleus herniated nucleus pulposuspulposus
Compress nerve roots Compress nerve roots leading to pain and leading to pain and muscle weaknessmuscle weakness
IntramedullaryIntramedullary
Can cause Can cause progressive progressive paraparesisparaparesis
Sensory lossSensory loss
5959

Extramedullary Spinal TumorsExtramedullary Spinal Tumors
NeurofibromaMeningioma
6060

Intramedullary Spinal tumorsIntramedullary Spinal tumors
Astrocytoma Ependymoma 6161

Imaging of Spinal TumorsImaging of Spinal Tumors
MRI is the modality of choiceMRI is the modality of choice
Conventional radiographyConventional radiography Can demonstrate bony destructionCan demonstrate bony destruction Widening of the vertebral pediclesWidening of the vertebral pedicles CT myelo may be necessary to identify CT myelo may be necessary to identify
extradural tumorsextradural tumors
6262

Treatment of Spinal TumorsTreatment of Spinal Tumors
Both intramedullary and extramedullary Both intramedullary and extramedullary can be removed surgicallycan be removed surgically 50% of patients who have surgery experience 50% of patients who have surgery experience
a reverse of clinical anomaliesa reverse of clinical anomalies
In cases where surgery is contraindicatedIn cases where surgery is contraindicated Radiation therapy is the primary means of Radiation therapy is the primary means of
treating a tumortreating a tumor
6363

Brain TumorsBrain Tumors Gliomas acct for 50% of all brain tumorsGliomas acct for 50% of all brain tumors
Types of gliomas include: Astrocytoma & Types of gliomas include: Astrocytoma & ependymomaependymoma
Ependymomas predominate in 3-4 yr oldsEpendymomas predominate in 3-4 yr olds
Meningiomas are the most frequently occurring Meningiomas are the most frequently occurring nonglial tumorsnonglial tumors Primarily affecting adults around 50 yrs oldPrimarily affecting adults around 50 yrs old They are non-aggressiveThey are non-aggressive
All tumors have greater incidence in malesAll tumors have greater incidence in males
Interfere with circulation of the CSF causing a Interfere with circulation of the CSF causing a hydrocephalushydrocephalus 6464

Brain TumorsBrain Tumors In children 20% of all tumors are brain In children 20% of all tumors are brain
tumorstumors 60 – 70% are located in the cerebellum & 60 – 70% are located in the cerebellum &
posterior fossaposterior fossa Most common are astrocytomas, Most common are astrocytomas,
medulloblastomas, glioblastomas and medulloblastomas, glioblastomas and craniopharyngliomascraniopharyngliomas• 30% of primary ped. Tumors are medulloblastoma30% of primary ped. Tumors are medulloblastoma
In adults most prevalent are:In adults most prevalent are: Astrocytomas, glioblastomas, metastatic Astrocytomas, glioblastomas, metastatic
tumors and menigiomastumors and menigiomas6565

Astrocytomas of BrainAstrocytomas of Brain
Usually treated with surgery and radiation therapy
Have good 5 year survival rate
6666

Ependymoma of BrainEpendymoma of Brain
Usually treated with surgical removal 6767

Medulloblastomas of BrainMedulloblastomas of Brain
6868

Craniopharyngliomas of BrainCraniopharyngliomas of Brain
6969

Metastatic Tumor of BrainMetastatic Tumor of Brain
7070

Meningiomas of BrainMeningiomas of Brain
Usually benign
More frequent in women
Rare in children
Less common to see in brain than spinal cord
7171

Symptoms of Brain TumorsSymptoms of Brain Tumors
HeadacheHeadache Nausea and VomitingNausea and Vomiting LethargyLethargy SeizuresSeizures ParalysisParalysis AphasiaAphasia BlindnessBlindness DeafnessDeafness Abnormal changes in personality & behaviorAbnormal changes in personality & behavior
7272

Treatment of Brain TumorsTreatment of Brain Tumors
Surgical resectionSurgical resection Radiation therapyRadiation therapy
Survival rate for surgery & Radiation therapy Survival rate for surgery & Radiation therapy combined is 80% over a 5 year periodcombined is 80% over a 5 year period
Rate of survival decrease to 3% over a Rate of survival decrease to 3% over a 10 year period10 year period
7373

HydrocephalusHydrocephalus
Can be congenital or acquiredCan be congenital or acquired Refers to an excessive amount of fluid in the Refers to an excessive amount of fluid in the
ventriclesventricles Two typesTwo types
Non- communicatingNon- communicating• Interferes or blocks normal CSF circulation from the Interferes or blocks normal CSF circulation from the
ventricles to the subarachnoid spaceventricles to the subarachnoid space CommunicatingCommunicating
• Poor absorption of the CSF by the arachnoid VilliPoor absorption of the CSF by the arachnoid Villi Least common cause is from overproduction of CSFLeast common cause is from overproduction of CSF
7474

HydrocephalusHydrocephalus
Non-communicatingNon-communicating Can be congenitalCan be congenital Can be from tumor Can be from tumor
growthgrowth Trauma (hemorrhage)Trauma (hemorrhage) InflammationInflammation
CommunicatingCommunicating Can come with Can come with
increased cranial increased cranial pressurepressure
Raised intrathoracic Raised intrathoracic pressure impairing pressure impairing venous flowvenous flow
Inflammation from Inflammation from meningitismeningitis
Subarachnoid Subarachnoid hemorrhagehemorrhage
7575

Radiographic AppearanceRadiographic Appearance
Generalized enlargement of the ventricular systemGeneralized enlargement of the ventricular system
PA radiograph can reveal separation of the suturesPA radiograph can reveal separation of the sutures
CT clearly demonstrates ventricular dilatation CT clearly demonstrates ventricular dilatation
MRI is more specific in demonstrating the underlying MRI is more specific in demonstrating the underlying cause of obstruction or in excluding obstructioncause of obstruction or in excluding obstruction
Ultrasound is useful in utero and in infantsUltrasound is useful in utero and in infants Sound waves transverse open fontanelsSound waves transverse open fontanels
7676

HydrocephalusHydrocephalus
7777

HydrocephalusHydrocephalus
7878

Hydrocephalus Clinical SymptomsHydrocephalus Clinical Symptoms
The cranial size is The cranial size is enlargedenlarged
Scalp veins distendedScalp veins distended Skin of scalp thin, Skin of scalp thin,
fragile and shinyfragile and shiny Neck muscles Neck muscles
underdevelopedunderdeveloped Severe casesSevere cases
Orbital roofs are Orbital roofs are depresseddepressed
Eyes displaced Eyes displaced downwardsdownwards
•In adults •ALOC•Ataxia•Incontinence•Decreased intellectual capabilities 7979

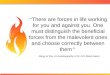
Treatment of HydrocephalusTreatment of Hydrocephalus Placement of a shuntPlacement of a shunt
Internal jugular, heart or Internal jugular, heart or peritoneumperitoneum
Contains one way valve to Contains one way valve to prevent backflow of blood prevent backflow of blood into ventriclesinto ventricles
Radiographs taken to Radiographs taken to verify shunt placementverify shunt placement
CT or MRI done to CT or MRI done to evaluate success of evaluate success of treatmenttreatment Ventricularjugular Shunt
8080
http://www.youtube.com/watch?v=Qmym2iFVNw8
http://www.youtube.com/watch?v=0h7Xa-Lsnac

Hydrocephalus in InfantsHydrocephalus in Infants
Affects 1 of every Affects 1 of every 1000 newborns1000 newborns
Long maturation of Long maturation of CNSCNS
Can be caused by Can be caused by maternal & fetal maternal & fetal infections, fetal infections, fetal hypoxia, irradiation, hypoxia, irradiation, chemical agents and chemical agents and mechanical forcesmechanical forces
8181

Hydrocephalus In UteroHydrocephalus In Utero
X-ray used to be taken for fetal age and X-ray used to be taken for fetal age and positionposition
With hydrocephalic fetus- hard to deliver With hydrocephalic fetus- hard to deliver vaginallyvaginally
Pelvimetry was ordered to determine Pelvimetry was ordered to determine measurements of inlet and outletmeasurements of inlet and outlet Very uncomfortable Very uncomfortable Three exposuresThree exposures
8282

Fetal HydrocephalusFetal Hydrocephalus
CommunicatingCommunicating The flow of CSF is free The flow of CSF is free
between ventricles & between ventricles & subarachnoid space subarachnoid space about cauda equinaabout cauda equina
Infants head is normal Infants head is normal size but there is size but there is bulging of the frontal bulging of the frontal fontanellesfontanelles
Caused by poor Caused by poor absorption of CSFabsorption of CSF
Non-communicatingNon-communicating Obstruction between Obstruction between
ventricles and cauda ventricles and cauda equinaequina
Most common form of Most common form of obstructive obstructive hydrocephalus is from hydrocephalus is from abnormalities between abnormalities between the 3the 3rdrd and 4 and 4thth ventriclesventricles
8383

Multiple SclerosisMultiple Sclerosis
Chronic progressive disease of the Chronic progressive disease of the nervous systemnervous system Affects women more than men at approx 20-Affects women more than men at approx 20-
40 years of age40 years of age
There is no cure and its origin is unknownThere is no cure and its origin is unknown Treatment only slows the processTreatment only slows the process Some research indicates it may come from Some research indicates it may come from
herpes or retrovirusherpes or retrovirus Appears more in temperate climates than Appears more in temperate climates than
tropical climatestropical climates8484

Multiple SclerosisMultiple Sclerosis Demyelination of the myelin sheath covering Demyelination of the myelin sheath covering
nervous tissue of spinal cord & white matter nervous tissue of spinal cord & white matter within the brainwithin the brain
It has episodes of relapses and remissionIt has episodes of relapses and remission
Eventually leads to neurological damageEventually leads to neurological damage Impairment of nerve conductionImpairment of nerve conduction
Patients life is not shortenedPatients life is not shortened Quality of life is diminishedQuality of life is diminished
8585

Symptoms Of Multiple SclerosisSymptoms Of Multiple Sclerosis
Difficulty speaking Difficulty speaking clearlyclearly
Bladder dysfunctionBladder dysfunction
Muscle impairmentMuscle impairment
Loss of balanceLoss of balance
Poor coordination Poor coordination
TremorsTremors Muscle weakness Muscle weakness
Double visionDouble vision
Nystagmus (rapid eye Nystagmus (rapid eye movement)movement)
8686

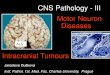
DEMYELINATION AREAS
DEMYELINATION AREAS
BRAINBRAIN
SPINAL CORDSPINAL CORD
HALLMARKS OF MS :
HALLMARKS OF MS :
8787

Imaging of Multiple SclerosisImaging of Multiple Sclerosis Scars from areas of Scars from areas of
demyelinated nervesdemyelinated nerves Sclerotic lesions Sclerotic lesions
throughout nervous systemthroughout nervous system Called MS plaquesCalled MS plaques
MRI is modality of choiceMRI is modality of choice Contrast enhanced can Contrast enhanced can
differentiate active differentiate active inflammation from older inflammation from older brain plaquesbrain plaques
Functional MRI assesses Functional MRI assesses alterations in normal CSF alterations in normal CSF functionfunction
8888

Multiple Sclerosis: MRIMultiple Sclerosis: MRI
8989

CT imaging of Multiple SclerosisCT imaging of Multiple Sclerosis
CT shows old inactive diseaseCT shows old inactive disease Well defined areas of decreased attenuationWell defined areas of decreased attenuation
With contrast, in an acute phaseWith contrast, in an acute phase Shows a mixture of decreased density (old)Shows a mixture of decreased density (old) Enhancing regions (active)Enhancing regions (active)
9090

Treatment for MSTreatment for MS Immunosuppressive Immunosuppressive
agentsagents Limit the autoimmune Limit the autoimmune
attackattack
AntiviralAntiviral Slows the progress of the Slows the progress of the
diseasedisease
Beta interferonBeta interferon Immunomodulatory agents Immunomodulatory agents
that reduce the severity of that reduce the severity of the attacksthe attacks
Given subcutaneouslyGiven subcutaneously
Corticosteroids (short Corticosteroids (short term)term)
Shortens the symptomatic Shortens the symptomatic periodsperiods
Delays progression of Delays progression of diseasedisease
Reduces frequency of Reduces frequency of attacksattacks
Regular exerciseRegular exercise Reduces spasms and Reduces spasms and
increases ROMincreases ROM
9191

Cerebrovascular Accident (CVA)Cerebrovascular Accident (CVA) Is an atherosclerotic disease affecting blood supply to the Is an atherosclerotic disease affecting blood supply to the
brainbrain 33rdrd leading cause of death in U.S. leading cause of death in U.S. 2 types of stroke:2 types of stroke:
Ischemic and HemorrhagicIschemic and Hemorrhagic Both CT and MRI distinguish between the two typesBoth CT and MRI distinguish between the two types
MRI is especially sensitive to infarction within hours of onsetMRI is especially sensitive to infarction within hours of onset CT, at times appears negative for a day or soCT, at times appears negative for a day or so
Carotid duplex and MRA are also useful in the diagnosis Carotid duplex and MRA are also useful in the diagnosis of a strokeof a stroke
http://www.youtube.com/watch?v=pcmrgwNCPwM&feature=relmfu
9292

Ischemic StrokeIschemic Stroke Blood clot blocks a blood vessel in the brainBlood clot blocks a blood vessel in the brain Is the majority of strokesIs the majority of strokes
Two types:Two types: Thrombosis of cerebral arteryThrombosis of cerebral artery
• Blood clot that blocks a blood vesselBlood clot that blocks a blood vessel Embolism of the brainEmbolism of the brain
• Is a mass of undissolved matter (solid, liquid or gas) present Is a mass of undissolved matter (solid, liquid or gas) present in a blood vessel brought there by blood currentin a blood vessel brought there by blood current
Diagnosed with CT and MRIDiagnosed with CT and MRI Angiography can be used if other modalites are Angiography can be used if other modalites are
questionablequestionable9393

Symptoms of Thrombotic Symptoms of Thrombotic Ischemic StrokeIschemic Stroke
Sypmtoms come on over horus to daysSypmtoms come on over horus to days ConfusionConfusion HemiplegiaHemiplegia AphasiaAphasia
May be preceded by a temporary episode of May be preceded by a temporary episode of nerurologic dysfunction called transient ischemic nerurologic dysfunction called transient ischemic attack (TIA)attack (TIA) Includes hemiparesis, monocular blindness- clears up Includes hemiparesis, monocular blindness- clears up
in about 2 hoursin about 2 hours
9494

Ischemic Stroke: from EmbolismIschemic Stroke: from Embolism
Sudden onset of symptoms without warningSudden onset of symptoms without warning
Mortality rate is 20%Mortality rate is 20%
Prognosis depends on location, extent, age, and Prognosis depends on location, extent, age, and general healthgeneral health Complete recovery is rareComplete recovery is rare Deficits remaining after 6 months are likely to be Deficits remaining after 6 months are likely to be
permanentpermanent
TreatmentTreatment Bed rest Bed rest Clot blockers within 3 hours (recombinant tissue Clot blockers within 3 hours (recombinant tissue
plasminogen activator (rtPA)plasminogen activator (rtPA) 9595

Ischemic StrokeIschemic Stroke
9696

Imaging of Ischemic StrokeImaging of Ischemic Stroke Non-contrast CT scans are most commonly usedNon-contrast CT scans are most commonly used
Before treatment with thrombolytic agentsBefore treatment with thrombolytic agents Best success if within 45 minutes of strokeBest success if within 45 minutes of stroke Follow up CT or transcranial US used after meds to monitor Follow up CT or transcranial US used after meds to monitor
success or medssuccess or meds
MRI is also excellent for imagingMRI is also excellent for imaging In some cases more accurate than CT in identifying EARLY In some cases more accurate than CT in identifying EARLY
infarct signsinfarct signs
CT, MRA and US may offer info regarding patency in the CT, MRA and US may offer info regarding patency in the brain and carotid arteriesbrain and carotid arteries
PET may be used in the future to identify decreased PET may be used in the future to identify decreased Oxygen flow and consumption within the brainOxygen flow and consumption within the brain
Shows promise but not currently used freqentlyShows promise but not currently used freqently
9797

Hemorrahgic StrokeHemorrahgic Stroke Occurs from a weakening in the diseased blood Occurs from a weakening in the diseased blood
vesselvessel Typically weakened from atherosclerosis from Typically weakened from atherosclerosis from
hypertensionhypertension
Sudden and often lethal because it comes on so Sudden and often lethal because it comes on so suddenlysuddenly
Accounts for 10-15% of all CVA’s Accounts for 10-15% of all CVA’s
Two types:Two types: Subarachnoid and IntracerebralSubarachnoid and Intracerebral
9898

Hemorrahgic StrokeHemorrahgic Stroke
Most occur in the cerebrum and bleed into Most occur in the cerebrum and bleed into lateral ventriclelateral ventricle
Most often preceded by an intense headache Most often preceded by an intense headache and vomitingand vomiting
LOC follows in minutes and leads to LOC follows in minutes and leads to contralateral hemiplegia or deathcontralateral hemiplegia or death
Prognosis is poorPrognosis is poor 35% die day after stroke35% die day after stroke 15% die within a few weeks, usually from another 15% die within a few weeks, usually from another
vessel rupturevessel rupture9999

Imaging of Hemorrahgic StrokesImaging of Hemorrahgic Strokes
CT is modality of choiceCT is modality of choice Can demonstrate high density blood in the Can demonstrate high density blood in the
subarachnoid space in more than 95% of subarachnoid space in more than 95% of casescases
Can demonstrate aneurysms greaeter than Can demonstrate aneurysms greaeter than 3mm3mm
With contrast is contraindicated because With contrast is contraindicated because surgeon will not operate without an angiogramsurgeon will not operate without an angiogram
MRI is relatively insensitive for MRI is relatively insensitive for subarachoid bleedssubarachoid bleeds
100100

Treatment ofTreatment ofHemorrahgic StrokesHemorrahgic Strokes
SurgerySurgery Preceded by a surgical angiogramPreceded by a surgical angiogram
If surgical intervention is postponed so will If surgical intervention is postponed so will the angiogramthe angiogram
101101

Hemorrahgic StrokeHemorrahgic Stroke
102102

Pathology Summary and Pathology Summary and Modality of ChoiceModality of Choice
Pathology Summary: Central Nervous Pathology Summary: Central Nervous SystemSystem
Pathology Imaging Modalities of Pathology Imaging Modalities of Choice Additive or Subtractive Choice Additive or Subtractive PathologyPathology
Hydrocephalus Hydrocephalus CT, MRI, sonography in the neonateCT, MRI, sonography in the neonate
MeningitisMeningitis MRIMRI
EncephalitisEncephalitis MRIMRI
Brain abscessBrain abscess CT, MRICT, MRI
Herniated nucleus pulposusHerniated nucleus pulposus MRI, CT, myelographyMRI, CT, myelography
Cervical spondylosisCervical spondylosis Radiography SubtractiveRadiography Subtractive Multiple sclerosisMultiple sclerosis
MRIMRI CVACVA
MRI, CT, sonography, PETMRI, CT, sonography, PET
GliomaGlioma MRI, CTMRI, CT
MedulloblastomaMedulloblastoma MRI, CTMRI, CT
MeningiomaMeningioma CT, MRICT, MRI
Pituitary adenomaPituitary adenoma CT, MRICT, MRI
CraniopharyngiomaCraniopharyngioma CTCT
Acoustic neuromaAcoustic neuroma MRIMRI
Spinal tumorSpinal tumor MRI, radiography, CT, myelographyMRI, radiography, CT, myelography
Both Metastases from other sitesBoth Metastases from other sites MRI, radiography, CTSubtractiveMRI, radiography, CTSubtractive
103103