-
7/27/2019 CNS Disorders (CD Nursing)
1/315
CNS AFFECTING THECNS
-
7/27/2019 CNS Disorders (CD Nursing)
2/315
TETANUS
-
7/27/2019 CNS Disorders (CD Nursing)
3/315
Tetanus
A neurological disease characterised by increased muscle
tospasms.
Caused by CLOSTRIDIUM TETANI
An anaerobic, motile, gram positive rod that forms oval,
colterminal spores tennis racket or drumstick shape.
-
7/27/2019 CNS Disorders (CD Nursing)
4/315
A. IMPORTANT INFORMATION
1. Infectious but not contagious2. Brought about by direct
inoculation of material containing
causative agent
3. Always a serious diseasefatal up to 60% of unimmunize
usually within 10 days of onset. When symptoms develop
days, the prognosis is poor.
-
7/27/2019 CNS Disorders (CD Nursing)
5/315
B. OTHER NAMES
Lockjaw Tetanos a Greek word to strech
First described by Hippocrates & Susruta
-
7/27/2019 CNS Disorders (CD Nursing)
6/315
C. CAUSATIVE AGENT
1. A common inhabitant of the soil especially if fertilized
wit2. Anaerobic (does not grow in the presence of free oxygen),
bacillus with round terminal spore with slender body givin
drumstick appearance
3. The organism comes in 2 forms, spore forming and the veg
form
4. Spores are extremely resistant to heat and ordinary
antisep
5. Multiplies only at the site of the wound
-
7/27/2019 CNS Disorders (CD Nursing)
7/315
2 Forms of Clostridium tetani
1.Vegetative: Slender, gram positive, nonencapsulated,
motileanaerobic
Susceptible to bactericidal effect of heat, chemical
disinfectantibiotics
Pathogenic form
2. Sporulated
Bulge at one end; drumstick appearance
Highly resistant to disinfection by chemicals or heat
-
7/27/2019 CNS Disorders (CD Nursing)
8/315
C. CAUSATIVE AGENT
6. The organism releases 2 types of toxins:
a. Tetanolysin
Dissolves/destroys the red blood cells Results to anemia
Thus, patient is pale-looking
b. Tetanospasmin
Causes muscle spasm
Acts on MYONEURAL JUNCTION of the muscles and on
INTERNUNCIALFIBERS of the spinal cord and thebrain.
Results into multiple muscle spasms
Inhibits the spastic muscle from sending transmissions to th
which would inhibit progression of spasms. Due to this, adja
muscles will also undergo spasm similar to a chain reaction
domino reaction.
-
7/27/2019 CNS Disorders (CD Nursing)
9/315
In the wound, there would be an inflammatory responscardinal
signs of local inflammation):
a. Ruborredness
b. Calorheat
c. Tumorswelling
d. Dolor
paine. Functio laesaloss of function
-
7/27/2019 CNS Disorders (CD Nursing)
10/315
It is found worldwide in soil, in inanimate environment, in
afeces & occasionally human feces.
-
7/27/2019 CNS Disorders (CD Nursing)
11/315
-
7/27/2019 CNS Disorders (CD Nursing)
12/315
D. PREDISPOSING FACTORS
1. More in the tropics2. Newborns whose method of delivery and
umbilical cor
not aseptic
3. Compound fracture
4. Following surgeries; any punctured wound; infected w
burns; tooth decay5. Bites/scratches
6. Women are poorer risks than men, so are the very youn
the very old
-
7/27/2019 CNS Disorders (CD Nursing)
13/315
E. EPIDEMIOLOGY
Occurs sporadically Affects unimmunized, partially immunized
& fully immunize
to maintain adequate immunity with booster doses of vacci
Although it is an entirely preventable disease by
immunizatiburden of disease worldwide is great.
-
7/27/2019 CNS Disorders (CD Nursing)
14/315
As reporting is inaccurate & incomplete, particularly
in devoleping countries, W.H.O considers reportedcases to be an
underestimate & takes case/deathestimates to assess the burden
of disease.
In 2002, the estimated deaths in all age groups2,13,000 of which
1,80,000 were attributable toneonatal tetanus.
More common in areas where soil is cultivated, inrural areas, in
warm climates, during summer, amonmales.
-
7/27/2019 CNS Disorders (CD Nursing)
15/315
F. INCUBATION PERIOD
1. Commonly 5-10 days but may vary from 2 days to severallonger,
depending on the extent, location, and character of
wound (3-21-28 days)
2. A short incubation period gives a bad prognosis
3. The longer the incubation period, the greater the
probabilit
recovery
-
7/27/2019 CNS Disorders (CD Nursing)
16/315
CONCEPT
The shorter the incubation period, the poorer the progn Shorter
incubation period is 2-3 days.
An incubation period of one month has a better prognos
incubation period of 2-3 days.
-
7/27/2019 CNS Disorders (CD Nursing)
17/315
F. SOURCES OF INFECTION
1. Animal and human feces (manure). The organisms are
fouintestinal wall of herbivorous animals, including man.
2. Soil and dust
3. Plaster of Paris, unsterile sutures, pins, rusty metals,
scisso
-
7/27/2019 CNS Disorders (CD Nursing)
18/315
G. MODE OF TRANSMISSION
1. Break in skin integrity
through punctured wound that is contaby dust, soil, or animal
excreta containing spores of Clostridum
a. Rugged traumatic wounds and burns
b. Umbilical cord stump in newborn especially for babies
deliv
home with faulty cord dressing; babies delivered to mothers
Tetanus toxoid immunizationc. Unrecognized wounds (cleaning of
the ears with sharp mate
d. Dental extraction, circumcision, ear piercing
-
7/27/2019 CNS Disorders (CD Nursing)
19/315
G. MODE OF TRANSMISSION
Range of injuries & accidentstrivial pin prick, skin
abrasiopuncture wounds, burns, human bites, animal bites &
stingunsterile surgery, IUD, bowel surgery, dental extractions,
inunsterile division of umbilical cord, compound #, otitis
mechr.skin ulcers, eye infections, gangrene
NOT TRANSMITTED FROM PERSON TO PERSON
-
7/27/2019 CNS Disorders (CD Nursing)
20/315
H. PATHOPHYSIOLOGY
C. tetanienters body through a wound
causes local and tissue necrosis in anaerobic conditions spores
g(reproduce) toxins produced (TETANOSPASMIN &TETANOLYSIN)
disseminated via blood and lymphaacts at several sites:
1. Central nervous system
2. Spinal cord
3. Brain
4. Sympathetic nervous system
-
7/27/2019 CNS Disorders (CD Nursing)
21/315
H. PATHOPHYSIOLOGY
While reproducing, they also release toxins that enter the
blooand the lymphatics and eventually spread into the central
nerv
system, or absorbed by the motor nerve ending and passes up
the axon cylinder, to the anterior horn cells of the spinal
cord.
stimulates contraction of the muscles supplied by the
neurons
the toxin diffuses.
-
7/27/2019 CNS Disorders (CD Nursing)
22/315
H. PATHOPHYSIOLOGY
Contamination of wounds with spores of C.tetani.
Germination & toxin production in wounds with low
oxidreduction potential (devitalized tissues, active infection
)
Tetanospasmin (neurotoxin)
Tetanolysin (hemolysin)
-
7/27/2019 CNS Disorders (CD Nursing)
23/315
Tetanospasmin (exotoxi) produced locally , released into blo
Binds to peripheral motor neuron terminals & nerve cells
ofof spinal cord
The toxin after entering axon , transported to nerve cell
bodstem & spinal cordretrograde intraneuronal transport
Toxin migrates across synapse presynaptic terminals- blorelease
ofGlycine & GABA from vesicles.
-
7/27/2019 CNS Disorders (CD Nursing)
24/315
The blocking of neurotransmitter release by
Tetanospasmincleavage of Synaptobrevin essential for proper fn of
synaprelease apparatus
With diminished inhibition resting firing rate of alpha
motneurons increasesrigidity
Lessened activity of reflexes which limit polysynaptic
spreadimpulses, agonists & antagonists recruited - spasms
-
7/27/2019 CNS Disorders (CD Nursing)
25/315
-
7/27/2019 CNS Disorders (CD Nursing)
26/315
Loss of inhibition of preganglionic sym neurons
sympathethyperactivity
-
7/27/2019 CNS Disorders (CD Nursing)
27/315
Diagnosis
1. Clinical Observation - based entirely on clinical
findings
a. Assess patient physicallyb. Assess for the presence of
lockjaw
c. If lockjaw is positive, a logical question would beDo you
have a
wound?
2. Examine all cases with wound infection & muscle
stiffness
3. Wound cultures in suspected cases, C. tetani can be isolated
from wpts without tetanus & frequently cannot be isolated from
wounds of thotetanus. If there is afresh wound, microorganisms are
still present ther4. Electromyograms continous discharge of motor
units, shortening / silent interval seen after AP.
5. Muscle enzymes raised
-
7/27/2019 CNS Disorders (CD Nursing)
28/315
SIGNS & SYMPTOMS
1. Spinal Cord
a. Striated musclesLockjaw
b. Trigeminal nervesTrismus
c. Facial nervesRisus Sardonicus
d. Spinal nerves - Opisthotonus
2. Brain
Respiratory Center Pharyngeal SpasmAbdominalGeneral Rigidity
(Tonic)
-
7/27/2019 CNS Disorders (CD Nursing)
29/315
TYPES OF TETANUS
Traumatic
Puerperal
Otogenic
Idiopathic
Tetanus neonatorum
Generalized
Neonatal
Local
-
7/27/2019 CNS Disorders (CD Nursing)
30/315
Clinical Features
May begin from 2 days to several weeks after the injury
UWEEK
Remember
Shorter the incubation period
More severe the attack
Worse the prognosis
-
7/27/2019 CNS Disorders (CD Nursing)
31/315
Clinical features
GENERALIZED TETANUS
Most common
Increased muscle tone & generalized spasms
Median time of onset after injury7 days
Pt 1st notices increased tone in masseter ( Trismus, lock
jaw
Dysphagia Stiffness / pain in neck, shoulder, back muscles
appear conc
or soon thereafter
Rigid abd & stiff prox.limb muscles . Hands, feet
spared.
-
7/27/2019 CNS Disorders (CD Nursing)
32/315
trismus
-
7/27/2019 CNS Disorders (CD Nursing)
33/315
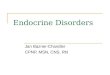
Risus Sardonicus : Spasm of facial muscles ( frontalis &
angl
mouth muscles ) producing grinning facies Opisthotonus : Painful
spasms of neck, trunk and extremity
producing characteristic bowingand arching of back Some pts
devolep paroxysmal, violent, painful, generalized
spasms cyanosis . Spasms occur repetitively & may be spo
/provoked by slightest stimulation. Constant threat during
general spasm is reduced ventilation
laryngospasm.
-
7/27/2019 CNS Disorders (CD Nursing)
34/315
Risus sardonicus
-
7/27/2019 CNS Disorders (CD Nursing)
35/315
-
7/27/2019 CNS Disorders (CD Nursing)
36/315
-
7/27/2019 CNS Disorders (CD Nursing)
37/315
Mild ds ( muscle rigidity , no / few spasms )
Moderate ds (trismus, dysphagia, rigidity, spasm)
Severe ds ( freq explosive paroxysms )
Autonomic dysfn complicates severe cases - labile
htn,hyperpyrexia, profuse sweating, peripheral vasoconstriction
catecholamines.
-
7/27/2019 CNS Disorders (CD Nursing)
38/315
Neonatal Tetanus
Usually fatal if untreated
Children born to inadequately immunized mothers, after
untreatment of umbilical stump
During first 2 weeks of life.
Poor feeding ,rigidity and spasms
-
7/27/2019 CNS Disorders (CD Nursing)
39/315
-
7/27/2019 CNS Disorders (CD Nursing)
40/315
-
7/27/2019 CNS Disorders (CD Nursing)
41/315
Local Tetanus
Uncommon form
Manifestations are restricted to muscles near the wound.
Cramping and twisting in skeletal muscles surrounding the w
local rigidity
Prognosis excellent
-
7/27/2019 CNS Disorders (CD Nursing)
42/315
Cephalic Tetanus
A rare form of local tetanus
Follows head injury / ear infection
Involves one / more facial cranial nerves
Trismus and localised paralysis, usually facial nerve,
oftenunilateral.
Incubation period : few days Mortality : high
-
7/27/2019 CNS Disorders (CD Nursing)
43/315
-
7/27/2019 CNS Disorders (CD Nursing)
44/315
Diagnosis
1. Clinical Observation - based entirely on clinical
findings
a. Assess patient physicallyb. Assess for the presence of
lockjaw
c. If lockjaw is positive, a logical question would beDo you
have a
wound?
2. Examine all cases with wound infection & muscle
stiffness
3. Wound cultures in suspected cases, C. tetani can be isolated
from w
pts without tetanus & frequently cannot be isolated from
wounds of thotetanus. If there is afresh wound, microorganisms are
still present ther4. Electromyograms continous discharge of motor
units, shortening / silent interval seen after AP.
5. Muscle enzymes raised
-
7/27/2019 CNS Disorders (CD Nursing)
45/315
Serum Anti toxin levels >= 0.1 IU/ml protective & makes
te
unlikely .
H MANAGEMENT
-
7/27/2019 CNS Disorders (CD Nursing)
46/315
H. MANAGEMENT1. Prevention
1.1 Active Immunization with tetanus toxoid (TT)6 weeks after
birth (togethDiphtheria and Pertussis/DPT): 0.5 ml for 3 doses (4-8
weeks interval)
DPT Immunization for Pregnant Individuals
Dose: 0.5 ml
Route: Intramuscular
Number of Doses given:a. Two (2) doses with three (3) booster
doses or;
b. Two (2) doses with booster dose given every pregnancy
When given:a. 1st Dose: Anytime during second trimester of
pregnancyb. 2nd Dose: With one (1) month interval
c. Booster Dose: Given with successive pregnancy/ies
H MANAGEMENT
-
7/27/2019 CNS Disorders (CD Nursing)
47/315
H. MANAGEMENT
1. Prevention
1.2 Tetanus Toxoid for non-pregnant women 1st Dose (TT1) given
anytime0.5 m
2nd Dose (TT2) after 1 month
3rd Dose (TT3) after 6 months
4th Dose (TT4) after 1 year 5th Dose (TT5) after another
year
Booster Dose given after 10 years
CO C
-
7/27/2019 CNS Disorders (CD Nursing)
48/315
CONCEPT
Succeeding doses of Tetanus Toxoid are given based on DA
LAST DOSE
If a person is high-risk, give booster dose every five (5)
yea
If a person is low risk, give booster dose every ten (10)
year
Effect of TT administration on the mother
Slight soreness or heaviness on site of injection
H MANAGEMENT
-
7/27/2019 CNS Disorders (CD Nursing)
49/315
H. MANAGEMENT
1. Prevention
1.3 Antitoxin is used for the treatment of clinical tetanus
an
passive immunization or prophylaxis in recently woun
individuals never previously immunized with tetanus to
P ti A ti I i ti
-
7/27/2019 CNS Disorders (CD Nursing)
50/315
Prevention Active Immunization
For partially immunized, unimmunized and recovering from It
stimulates production of protective antitoxin
2 prep : combined vaccine : DPT
monovalent vaccine : plain / formol
toxoid
tetanus vaccine , adsorbed
H MANAGEMENT
-
7/27/2019 CNS Disorders (CD Nursing)
51/315
H. MANAGEMENT
2. Control
2.1 Medical Aseptic technique
2.2 Concurrent Disinfection (all materials contaminated with
secretions should be securely wrapped in paper and burned AS
Terminal Disinfection (walls and furniture washed with soap
water, room thoroughly aired, mattress and pillows
autoclavedaired/sunned for 6-8 hours)
CONCEPT ON WOUND CARE
-
7/27/2019 CNS Disorders (CD Nursing)
52/315
CONCEPT ON WOUND CARE
Wash wound with soap and running water
Place antiseptic solution on wound
Use thin dressing
Band Aid Plastic Strips are allowable as they have air ve
holes
Do not use plasterUse only those types of plasters with air
ventilation holes
introduce oxygen to the wound
H MANAGEMENT
-
7/27/2019 CNS Disorders (CD Nursing)
53/315
H. MANAGEMENT3. Treatment
3.1 Medical Careobjectives are:a. Neutralize the toxintop
priority since the toxin is responsible for the S/Sx of
and the systemic infection
(1) Give anti-tetanus serum (ATS) ortetanus anti-toxin (TAT)
Comes from a horse serum Do SKIN TESTING first
If (-) for skin test, inject TIG 0.01 ml in 0.09 ml NSS.
Epinephrine or sterocounteract prophylaxis
(2) If (+) for skin testing, DO NOT GIVE the drug
Resort to human serumtetanus immunoglobulin (TIG)
a) Give skin test first: anti-tetanus serum (ATS)b) If skin test
is negative, inject Tetanus Anti-Toxin (TAT) 0.01 ml in 0.0
Epinephrine or steroid is given to counteract prophylaxis.
CONCEPT
-
7/27/2019 CNS Disorders (CD Nursing)
54/315
CONCEPT
In the Philippine setting, the horse serum is given despite a
(+) s
This is done by giving fractional doses.
Example: Initial administration of 0.01 of drug and 0.099 PNSS
After 30 minutes, 0.05 of the drug and 0.95 of PNSS
After another 30 minutes, another increase in the dose of the
druWhen administering tetanus horse serum, always have ready
the
a. EPINEPHRINE
b. CORTICOSTEROID These would be necessary to counteract any
delayed reaction, which ma
hypersensitivity reactions leading to anaphylaxis and eventually
the deapatient.
-
7/27/2019 CNS Disorders (CD Nursing)
55/315
NEUTRALIZE TOXIN :
Inj. Human Tetanus Immunoglobulin (TIG) 3000 6000 units IM,
usuadivided doses as volume is large.
ANTIBIOTIC THERAPY :
Although of unproven value , antibiotics adm to eradicate
vegetative csource of toxin
IV Penicillin 10 -12 million units daily for 10 days
IV Metronidazole 500mg Q 6 hrly / 1gm Q 12 hrly
Allergic to Penicillin : consider Clindamycin &
Erythromycin
H MANAGEMENT
-
7/27/2019 CNS Disorders (CD Nursing)
56/315
H. MANAGEMENT
b. Kill the microorganism
(1) Give IV Penicillin (drug of choice): antibiotic to kill the
bacter(eradicate vegetative cells) & is given 1 hour before
meals or 2meals for bioavailability. If allergic to penicillin,
considerClin& Erythromycin
(2) On the fresh wound, do daily cleansing with the use of
hydrogeperoxide.
(3) Then apply antiseptic solution like Betadine or Povidone(4)
Then cover wound with THIN DRESSING to allow air to circu
through the wound(5) It may also be good to expose the wound but
avoid contact wit
H MANAGEMENT
-
7/27/2019 CNS Disorders (CD Nursing)
57/315
H. MANAGEMENT
c. Prevent and control spasms
(1) Muscle relaxants
Given during acute phase of tetanus; done via the IV route
methocarbamol (Robaxin, Robaxisal), Lionesal (Baclofen),
Eperis
(Myonal)
May be given per orem when the patient is on his way to
recover
(2) Sedatives
Valium (diazepam); use IV push or IV drip Concept: I.V. drip
regulation is titrated based on the frequenc
spasm
The more frequent the spasm, the faster the rate of the titr
(3) Tranquilizers Thorazine
-
7/27/2019 CNS Disorders (CD Nursing)
58/315
(4) Continued spasms : intubate & ventilate
(5) Proceed with other supportive managementa. For urinary
retention, do catheterization
b. For constipation, administer laxatives as ordered.
CONCEPT: Stimuli triggers spasm
-
7/27/2019 CNS Disorders (CD Nursing)
59/315
CONCEPT: Stimuli triggers spasm
Types of Stimuli:
(1) Exteroceptive Stimuli
Comes from outside environment of the patient Examples: bright
light and noise
Place the patient in dim and quiet environment
(2) Interoceptive Stimuli
Comes from inside or within the patient Examples: stress, pain,
coughing, passage of flatus(3) Proprioceptive Stimuli
There is participation of the patient and other people Examples:
touching, turning, jarring the bed of the patient
H MANAGEMENT
-
7/27/2019 CNS Disorders (CD Nursing)
60/315
H. MANAGEMENT3.2 Nursing Caredone to prevent patient from having
spasms
a. Place the patient should be in a quiet, darkened/dimmed,
wel
ventilated, and non-stimulating environment CONCEPT: Patients
are isolated so as not to be exposed to stimuli.
b. Practice Minimal/gentle handling of patient. Touching and
Turning is not contraindicated
However, do these as gently as possible Inform the patient
before proceeding with any procedure
c. Practice Cluster Care Do all nursing activities in one
setting Proper scheduling of nursing care activities so as not to
disturb patient o
cleansing bath with warm water, change position, oral
hygiene
Do other nursing care activities with vital signs taking
H MANAGEMENT
-
7/27/2019 CNS Disorders (CD Nursing)
61/315
H. MANAGEMENT
3.2 Nursing Care
d. Liquid diet of 3,000-4,000 calories via tube feedings as ine.
Prevent injury
(1) Do not leave patient alone
(2) Siderails of bed always raised
(3) Padded tongue blades or metal spoon to guard against re
obstruction
e. Proper wound carewash with flowing water, then rinse w
antiseptic solution and cover with thin dressing
Treatment general measures
-
7/27/2019 CNS Disorders (CD Nursing)
62/315
Treatment general measures
Goal is to eliminate the source of toxin, neutralize the
unbo
& prevent muscle spasm & providing support - resp suppor
Admit in a quiet room in ICU
Continuous careful observation & cardiopulmonary monitor
Minimize stimulation
Protect airway Explore woundsdebridement
Management of autonomic dysfn
-
7/27/2019 CNS Disorders (CD Nursing)
63/315
Management of autonomic dysfn
Labetalol
Continuous infusion of esmolol
Clonidine / verapamil
Additional measures
-
7/27/2019 CNS Disorders (CD Nursing)
64/315
Additional measures
Pts recovering from tetanus should be actively immunized
Hydration
Nutrition
Physiotherapy
Prophylactic anticoagulation
Bowel, bladder, back care Treatment of intercurrent
infection
DPT (Diphtheria Pertussis Tetanus)
-
7/27/2019 CNS Disorders (CD Nursing)
65/315
VaccineWhen given:
1st Dose: 6 weeks after birth; 0.5 ml
2nd Dose: 10 weeks after birth; 0.5 ml
3rd Dose: 14 weeks after birth; 0.5 ml
Number of Doses: three (3)
Interval between Doses: Four (4) weeksAdministration Site:
Vastus lateralis muscle
Route: Intramuscular
IMPORTANT CONCEPTS IN DPTADMINISTRATION
-
7/27/2019 CNS Disorders (CD Nursing)
66/315
ADMINISTRATIONa. Expect fever to set in after administration of
DPT vaccine
Give paracetamol
Apply warm compress for better drug absorption Immediately
follow up with cold compress to avoid soreness
b. If tenderness or swelling on site of injection is
present:
Do cold compress within twenty-four (24) hours
Then do warm compress
c. Observe for signs of convulsions within seven (7) days after
DPT immun
This indicates that child has reaction with the pertussis
component of the dru Therefore, succeeding doses of DPT will NOT BE
GIVEN
Give ONLY the DT components
If DPT is given again, this predisposes the child to neurologic
disorders
d. Observe if child cries uncontrollably
IMPORTANT CONCEPTS IN DPTADMINISTRATION
-
7/27/2019 CNS Disorders (CD Nursing)
67/315
ADMINISTRATION
d. Observe if child cries uncontrollably
This is an indication of development of neurologic disorder
Monovalent vaccines
-
7/27/2019 CNS Disorders (CD Nursing)
68/315
Monovalent vaccines
Purified tetanus toxoid ( adsorbed ) supplanted the palin
tox
higher & long lasting immunity response Primary course of
immunization 2 doses
Each 0.5 ml , injected into arm given at intervals of 1-2
mon
The longer the interval b/w two doses, better is the immune
1st
booster1 yr after the initial 2 doses 2nd Booster : 5 yrs after
the 1st booster ( optional )
Freq boosters to be avoided
Passive immunization
-
7/27/2019 CNS Disorders (CD Nursing)
69/315
Passive immunization
Temp protection human tetanus immunoglobulin /ATS
Human Tetanus Hyperimmunoglobulin :
250-500 IU
Does not cause serum sickness
Longer passive protection compared to horse ATS( 30 days /
days )
Passive immunization
-
7/27/2019 CNS Disorders (CD Nursing)
70/315
Passive immunization
ATS ( EQUINE ) :
1500 IU s/c after sensitivity testing
7 10 days
High risk of serum sickness
It stimulates formation of antibodies to it , hence a person
w
once received ATS tends to rapidly eliminate subsequent do
Active & Passive Immunization
-
7/27/2019 CNS Disorders (CD Nursing)
71/315
Active & Passive Immunization
In non immunized persons
1500 IU of ATS / 250-500 units of Human Ig in one arm &
0.adsorbed tetanus toxoid into other arm /gluteal region
6 wks later, 0.5 ml of tetanus toxoid
1 yr later , 0.5 ml of tetanus toxoid
Prevention of neonatal tetanus
-
7/27/2019 CNS Disorders (CD Nursing)
72/315
Clean delivery practices
3 cleans : clean hands, clean delivery surface, clean cord car
Tetanus toxoid protects both mother & child
Unimmunized pregnant women : 2 doses tetanus toxoid
1st dose as early as possible during pregnancy
2nd
dose at least a month later / 3 wks before delivery
-
7/27/2019 CNS Disorders (CD Nursing)
73/315
Immunized pregnant women : a booster is sufficient
No need of booster in every consecutive pregnancy
Prevention of tetanus after injury
-
7/27/2019 CNS Disorders (CD Nursing)
74/315
j y
All wounds should be thoroughly cleaned soon after injury
Remove all foreign bodies, soil, dust, necrotic tissueA
completed course of toxoid/booster < 5 yrs ago
B- completed course of toxoid / booster >5 yrs ago & <
10 y
C- completed course of toxoid / booster >10 yrs ago
D- not completed course of toxoid / immunity status unkno
Wounds < 6hrs, clean, non penetrating negligible tissue
damage
-
7/27/2019 CNS Disorders (CD Nursing)
75/315
negligible tissue damage
Immunity Category
A
B
C D
Treatment
Nothing more required
Toxoid 1 dose
Toxoid 1 dose Toxoid complete cours
Other Wounds
-
7/27/2019 CNS Disorders (CD Nursing)
76/315
Immunity Category
A
B
C
D
Treatment
Nothing more required
Toxoid 1 dose
Toxoid 1 dose + HumanIg
Toxoid complete coursHuman Tetanus Ig
-
7/27/2019 CNS Disorders (CD Nursing)
77/315
MENINGITIS
-
7/27/2019 CNS Disorders (CD Nursing)
78/315
-
7/27/2019 CNS Disorders (CD Nursing)
79/315
MENINGITISMeningitis is an inflammatory process of the
leptomeninges and
Space occupying lesions
-
7/27/2019 CNS Disorders (CD Nursing)
80/315
CNS hemorrhage
Brain tumours Brain abscess
Metastatic tumours
Classification
-
7/27/2019 CNS Disorders (CD Nursing)
81/315
1. acute pyogenic (bacterial) meningitis
2.acute aseptic (viral) meningitis 3.acute focal suppurative
infection (brain abscess,subdural a
extradural empyema)
4.chronic bacterial infection (tuberculosis).
Acute pyogenic bacterial meningitis
-
7/27/2019 CNS Disorders (CD Nursing)
82/315
Most important
Can be fatal if untreated Organisms:
E.coli ---------- neonates
Streptococci B ---------- neonantes
H. influenzae-------------adolescents
Neisseria meningitidis------------- young adults
Streptococcus pneumonia--------- elderly
Clinical signs
-
7/27/2019 CNS Disorders (CD Nursing)
83/315
Signs of infection (fever,malaise,rigor.)
Signs of meningeal irritation:
1.headache
2.neck stiffness
3.photophobia
4.irritability
C.S.F by lumbar puncture shows :
a.cloudy purulent csfb.abundant neutrophils > 90,000/mm3
c.high protein level and
d.reduced glucose level.
Morphology
-
7/27/2019 CNS Disorders (CD Nursing)
84/315
Grossly , pyogenic meningitis shows a thick layer of suppura
exudate covers the leptomeninges over the surface of the b
Exudate in basal surface--- H.INFLUENZAE
Exudate in covexity surface--- P.MENINGT
Microscopically :
neutrophils in the subarachnoid space
-
7/27/2019 CNS Disorders (CD Nursing)
85/315
-
7/27/2019 CNS Disorders (CD Nursing)
86/315
-
7/27/2019 CNS Disorders (CD Nursing)
87/315
-
7/27/2019 CNS Disorders (CD Nursing)
88/315
-
7/27/2019 CNS Disorders (CD Nursing)
89/315
-
7/27/2019 CNS Disorders (CD Nursing)
90/315
Complications
-
7/27/2019 CNS Disorders (CD Nursing)
91/315
Antibiotic treatment------ full recovery
Delayed or untreated cases--- can be fatal Healing by fibrosis
cause obliteration of subarachenoid spac
HYDROCEPHALUS
Brain abscess
Septic shock and skin rashes, why ?
Skin rashes
-
7/27/2019 CNS Disorders (CD Nursing)
92/315
Is due to small skin bleed
All parts of the body are affeced
The rashes do not fade under pressure Pathogenesis:
a. Septicemia
b. wide spread endothelial damage
c. activation of coagulation
d. thrombosis and platelets aggregation
e. reduction of platelets (cosumption )f. BLEEDING 1.skin
rashes
2.adrenal hemorrhage
Arenal hemorrhage is called Waterhouse-Friderichsen Syndrome.It
cause acute adrinsufficiency and is uaually fatal
-
7/27/2019 CNS Disorders (CD Nursing)
93/315
-
7/27/2019 CNS Disorders (CD Nursing)
94/315
Acute Aseptic (Viral ) Meningitis
-
7/27/2019 CNS Disorders (CD Nursing)
95/315
Can follow any viral infection
Less danger CSF shows :
1.lymphocytes
2. mild increase in protein
3. normal glucose level
Viral meningitis is usually self-limiting and treated
symptoma
Brain abscess
-
7/27/2019 CNS Disorders (CD Nursing)
96/315
Causes :
1. complication of bacterial meningitis2. bacterial
endocarditis
3. pulmonary sepsis : peumoniaetc
4. other sepsis
Brain abscess cause a space occupying lesion in the brain
-
7/27/2019 CNS Disorders (CD Nursing)
97/315
-
7/27/2019 CNS Disorders (CD Nursing)
98/315
Neisseria meningitidis
(meningococcus)
-
7/27/2019 CNS Disorders (CD Nursing)
99/315
MENINGOCOCCEMIA
Encapsulated small, gram-negative diplococci
Second most common cause (behind S. pneumonia
it i d i iti i i l h lth
General Overview of Neisseria meningitidis
-
7/27/2019 CNS Disorders (CD Nursing)
100/315
community-acquired meningitis in previously health
adults; swift progression from good health to life-
threatening disease Pathogenicity:
Pili-mediated, receptor-specific colonization of
nonciliated cells of nasopharynx
Antiphagocytic polysaccharide capsule allows
systemic spread in absence of specific immunity Toxic effects
mediated by hyperproduction of
lipooligosaccharide
Serogroups A, B, C, Y, W135 account for about 90%
all infections
Diseases Associated with Neisseriameningitidis
-
7/27/2019 CNS Disorders (CD Nursing)
101/315
Following dissemination of virulent
organisms from the nasopharynx: Meningitis
Septicemia (meningococcemia) with or with
meningitis
Meningoencephalitis
Pneumonia
Arthritis
Urethritis
Neisseria meningitidis inCerebrospinal Fluid
-
7/27/2019 CNS Disorders (CD Nursing)
102/315
Humans only natural hosts
Person-to-person transmission by aerosolizatio
respiratory tract secretions in crowded condition
Epidemiology of Meningococcal Disease
-
7/27/2019 CNS Disorders (CD Nursing)
103/315
respiratory tract secretions in crowded condition
Close contact with infectious person (e.g., famil
members, day care centers, military barracks,prisons, and other
institutional settings)
Highest incidence in children younger than 5 ye
and particularly those younger than 1 year of ag
passive maternal antibody declines and as infan
immune system matures Commonly colonize nasopharynx of
healthy
individuals; highest oral and nasopharyngeal
carriage rates in school-age children, young ad
and lower socioeconomic groups
Age Distribution of Meningococcal Dise
in USA
Lacking maternal antibody
-
7/27/2019 CNS Disorders (CD Nursing)
104/315
Specific receptors (GD1 ganglioside) for bacterial fimbri
nonciliated columnar epithelial cells in nasopharynx of h
O
Pathogenesis of Meningococcal Disease
-
7/27/2019 CNS Disorders (CD Nursing)
105/315
Organisms are internalized into phagocytic vacuoles, av
intracellular killing in absence of humoral immunity and
complement system (patients with late complementdeficiencies are
particularly at risk)
Replicate intracellularly and migrate to subepithelial spa
where excess membrane fragments are released
Hyperproduction of endotoxin (lipid A of LOS) and blebb
into surrounding environment (e.g., subepithelial
spacesbloodstream) mediates most clinical manifestations inclu
diffuse vascular damage (e.g., endothelial damage, vas
(inflammation of vessel walls), thrombosis (clotting),
disseminated intravascular coagulation (DIC)
Skin Lesions of Meningococcemia
-
7/27/2019 CNS Disorders (CD Nursing)
106/315
NOTE:Petechiaehave coalesced into
hemorrhagic bullae.
Following colonization of the nasopharynx, prote
humoral immunity develops against the same or
Immunogenicity of Neisseria meningitidis
-
7/27/2019 CNS Disorders (CD Nursing)
107/315
humoral immunity develops against the same or
closely related organisms of the same serogroup
not against other serogroupsBactericidal activity of the
complement system is
required for clearance of the organisms
Cross-reactive protective immunity acquired with
colonization by closely related antigenic strains a
with normal flora of other genera (e.g., E. coliK1progressive
disease can occur in absence of
serogroup-specific immunity
Large numbers (e.g., >107cells/ml) of encapsula
Laboratory Characterization of Neisseria meningitidis
-
7/27/2019 CNS Disorders (CD Nursing)
108/315
g ( g , ) p
small, gram-negative diplococci (flattened along
adjoining side) and polymorphonuclear leukocy(PMNs) can be seen
microscopically in
cerebrospinal fluid (CSF)
Transparent, non-pigmented nonhemolytic colo
on chocolate blood agar with enhanced growth
moist atmosphere with 5% CO2 Oxidase-positive
Acid production from glucose and maltose but n
from other sugars
Prevention and Treatment of Meningococcal Disease
Penicillin is drug of choice for treatment in adjunct
supportive therapy for meningeal symptoms
-
7/27/2019 CNS Disorders (CD Nursing)
109/315
Increasing MIC mediated by genetic alteration o
target penicillin binding proteins is being monito
Chloramphenicol or cephalosporins as alternati
Chemoprophylaxis of close contacts with rifampin
sulfadiazine (if susceptible)
Polyvalent vaccine containing serogroups A, C, Y,
W135 is effective in people older than 2 years of a
for immunoprophylaxis as an adjunct tochemoprophylaxis
Serogroup B is only weakly immunogenic and
protection must be acquired naturally from expo
to cross-reacting antigens
-
7/27/2019 CNS Disorders (CD Nursing)
110/315
VIRAL ENCEPHALITIS
-
7/27/2019 CNS Disorders (CD Nursing)
111/315
Introduction
-
7/27/2019 CNS Disorders (CD Nursing)
112/315
Encephalitis is an acute inflammatory process affecting the
brain
Viral infection is the most common and important cause, with
over 10
implicated worldwide
Symptoms Fever
Headache
Behavioral changes
Altered level of consciousness
Focal neurologic deficits
Seizures
Incidence of 3.5-7.4 per 100,000 persons per year
Causes of Viral Encephalitis
H i HSV 1 HSV 2 i ll t i t l i E t i B
-
7/27/2019 CNS Disorders (CD Nursing)
113/315
Herpes viruses HSV-1, HSV-2, varicella zoster virus,
cytomegalovirus, Epstein-Barr herpes virus 6
Adenoviruses
Influenza A
Enteroviruses, poliovirus
Measles, mumps, and rubella viruses
Rabies
Arboviruses examples: Japanese encephalitis; St. Louis
encephalitis virus; West Nivirus; Eastern, Western and Venzuelan
equine encephalitis virus; tick borne enceph
Bunyaviruses examples: La Crosse strain of California virus
Reoviruses example: Colorado tick fever virus
Arenaviruses example: lymphocytic choriomeningitis virus
What Is An Arbovirus?
A b i h d b i
-
7/27/2019 CNS Disorders (CD Nursing)
114/315
Arboviruses = arthropod-borne viruses
Arboviruses are maintained in nature through biological
trabetween susceptible vertebrate hosts by blood-feeding arth
Vertebrate infection occurs when the infected arthropod takblood
meal
-
7/27/2019 CNS Disorders (CD Nursing)
115/315
http://www.cdc.gov/ncidod/dvbid/arbo
Major Arboviruses That Cause Encepha
Fl i i id
-
7/27/2019 CNS Disorders (CD Nursing)
116/315
Flaviviridae Japanese encephalitis
St. Louis encephalitis
West Nile
Togaviridae Eastern equine encephalitis
Western equine encephalitis
Bunyaviridae La Crosse encephalitis
-
7/27/2019 CNS Disorders (CD Nursing)
117/315
-
7/27/2019 CNS Disorders (CD Nursing)
118/315
West Nile Virus
West Nile Virus
Flavivirus
-
7/27/2019 CNS Disorders (CD Nursing)
119/315
Primary host wild birds
Principal arthropod vectormosquitoes
Geographic distribution - Africa,Middle East, Western
Asia,Europe, Australia, North America,
Central America
http://www.walgreens.com/images/library/healtht
History of West Nile Virus
1937 West Nile virus isolated from woman in Uganda
-
7/27/2019 CNS Disorders (CD Nursing)
120/315
1937 - West Nile virus isolated from woman in Uganda
1950s First recorded epidemics in Israel (1951-1954, 1957
1962 Epidemic in France
1974 Epidemic in South Africa. Largest ever West Nile epi
1996 Romanian epidemic with features similar to those ofAmerican
outbreak. 500 cases and 50 deaths.
1999 Russian outbreak. 40 deaths.
West Nile Virus: 1999 New York Outbrea
Crows dying in and around Queens in latesummer
-
7/27/2019 CNS Disorders (CD Nursing)
121/315
summer
27 deaths among captive birds in the Queens
and Bronx zoos Concomitant human infection of apparent
encephalitis in the same area
Outbreak was first attributed to St. Louisencephalitis, but
tissue samples from deadcrows confirmed that it was West Nile
virus
59 human cases requiring hospitalization,including 7 deaths
Spread of West Nile Virus in the US
2000 spread throughout New England andMid-Atlantic regions.
-
7/27/2019 CNS Disorders (CD Nursing)
122/315
g
18 new human cases reported
2001 spread throughout the entire easternhalf of the US
64 cases reported, with NY, FL and NJaccounting for 60%
2002 spread westward across Great Plainsinto Western US. Reached
California by LaborDay.
By end of 2002 cumulative human cases > 3900,with > 250
deaths
2003 US, Canada, Mexico 9,858 cases reported to CDC, including
262
deaths in 45 states and D.C.
West Nile Activity in the US Reports aApril 7, 2004
-
7/27/2019 CNS Disorders (CD Nursing)
123/315
West Nile Activity in the US CountiesReporting Cases as of March
24, 2004
-
7/27/2019 CNS Disorders (CD Nursing)
124/315
West Nile Virus 2004:BREAKING NEWS
April 13, 2004 Ohio may have first 2004 West Nile Case 79 year
old man from Scioto County OH was admitted April 1 with v
-
7/27/2019 CNS Disorders (CD Nursing)
125/315
79 year old man from Scioto County, OH was admitted April 1 with
vmeningitis and encephalitis which rapidly progressed to coma over
2
days. Initial IgM antibody titers were positive for West Nile
virus and he
complained of itching from insect bites upon admission
Has been treated with blood-pressure drugs to control
over-responsby the immune system to West Nile virus, causing brain
inflammatio
Previously unresponsive and paralyzed.
Can now open his eyes and shake his head in response to
questions, bstill cannot talk.
-
7/27/2019 CNS Disorders (CD Nursing)
126/315
St. Louis Encephalitis
St. Louis Encephalitis
Flavivirus
-
7/27/2019 CNS Disorders (CD Nursing)
127/315
Most common mosquito-
transmitted human pathogen inthe US
Leading cause of epidemicflaviviral encephalitis
History of St. Louis Encephalitis
1933 virus isolated during St. Louis and Kansas City, MO ep
-
7/27/2019 CNS Disorders (CD Nursing)
128/315
g y, p
1940s virus spread to Pacific Coast
1959-1971 virus spread to Southern Florida
1974-1977 last major epidemic. Over 2,500 cases in 35 st
1990-1991 South Florida epidemic. 226 cases and 11 dea
1999 New Orleans outbreak. 20 reported cases.
St. Louis Encephalitis
-
7/27/2019 CNS Disorders (CD Nursing)
129/315
-
7/27/2019 CNS Disorders (CD Nursing)
130/315
Japanese Encephalitis
Japanese Encephalitis
Flavivirus related to St. Louis encephalitis
Most important cause of arboviral encephalitis
-
7/27/2019 CNS Disorders (CD Nursing)
131/315
Most important cause of arboviral encephalitisworldwide, with
over 45,000 cases reported
annually Transmitted by culex mosquito, which breeds in
rice fields
Mosquitoes become infected by feeding ondomestic pigs and wild
birds infected withJapanese encephalitis virus. Infectedmosquitoes
transmit virus to humans andanimals during the feeding process.
History of Japanese Encephalitis
1800s recognized in Japan
-
7/27/2019 CNS Disorders (CD Nursing)
132/315
1924 Japan epidemic. 6125 cases, 3797 deaths
1935 virus isolated in brain of Japanese patient who died
encephalitis
1938 virus isolated from Culex mosquitoes in Japan
1948 Japan outbreak
1949 Korea outbreak
1966 China outbreak Today extremely prevalent in South East
Asia. 30,000-50,0reported each year.
Distribution of Japanese Encephalitis in1970-1998
-
7/27/2019 CNS Disorders (CD Nursing)
133/315
Eastern Equine
-
7/27/2019 CNS Disorders (CD Nursing)
134/315
Eastern Equine
Encephalitis
Eastern Equine Encephalitis
Togavirus
Caused by a virus transmitted to humans and
-
7/27/2019 CNS Disorders (CD Nursing)
135/315
horses by the bite of an infected mosquito.
200 confirmed cases in the US 1964-present Average of 4 cases
per year
States with largest number of cases Florida,Georgia,
Massachusetts, and New Jersey.
Human cases occur relatively infrequently,largely because the
primary transmission cycle
takes place in swamp areas where populationstend to be
limited.
History of Eastern Equine Encephalitis
1831 First recognized as a disease in horses. Over 75 hors3 i i
M h
-
7/27/2019 CNS Disorders (CD Nursing)
136/315
3 counties in Massachusetts.
1845-1912 epizootics in Northeast and Mid-Atlantic region
1933 virus isolated from horse brains
1938 association of human disease with epizootics. 30
caencephalitis in children living in same area as equine cases.
1947 largest recorded outbreak in Louisiana and Texas. 13cases
and 11,722 horse deaths
-
7/27/2019 CNS Disorders (CD Nursing)
137/315
Western Equine
-
7/27/2019 CNS Disorders (CD Nursing)
138/315
Western Equine
Encephalitis
Western Equine Encephalitis
Togavirus
Mosquito-borne
-
7/27/2019 CNS Disorders (CD Nursing)
139/315
Mosquito borne
639 confirmed cases in the USsince 1964
Important cause of encephalitis inhorses and humans in
NorthAmerica, mainly in the Western
parts of the US and Canada
History of Western Equine Encephalitis
Early 1900s epizootics of viral encephalitis in horses
descrArgentina
-
7/27/2019 CNS Disorders (CD Nursing)
140/315
Argentina
1912 25,000 horses died in Central Plains of US
1930 San Joaquin Valley, CA outbreak. 6000 cases in
horseisolated from horse brains
1938 virus isolated from brain of a child
-
7/27/2019 CNS Disorders (CD Nursing)
141/315
-
7/27/2019 CNS Disorders (CD Nursing)
142/315
La Crosse Encephalitis
La Crosse Encephalitis Bunyavirus
On average 75 cases per year reported to the CDC
Most cases occur in children under 16 years old
-
7/27/2019 CNS Disorders (CD Nursing)
143/315
Most cases occur in children under 16 years old
Zoonotic pathogen that cycles between the daytimebiting treehole
mosquito, and vertebrate amplifierhosts (chipmunk, tree squirrel)
in deciduous foresthabitats
Most cases occur in the upper Midwestern state, butrecently
cases have been reported in the Mid-Atlantic region and the
Southeast
1963 isolated in La Crosse, WI from the brain of achild who died
from encephalitis
-
7/27/2019 CNS Disorders (CD Nursing)
144/315
Summary Confirmed and Probable Human in the US
Virus Years Total cases
-
7/27/2019 CNS Disorders (CD Nursing)
145/315
Eastern Equine 1964-2000 182
Western Equine 1964-2000 649
La Crosse 1964-2000 2,776
St. Louis 1964-2000 4,482
West Nile 1999-present > 9,800
Molecular Biology of Virusethat can Cause Viral
-
7/27/2019 CNS Disorders (CD Nursing)
146/315
that can Cause Viral
Encephalitis Flaviviridae: West Nile Virus
Togaviridae: Eastern and Western EquiEncephalitis
Bunyaviridae: La Crosse Virus
Flavivirus
-
7/27/2019 CNS Disorders (CD Nursing)
147/315
Flavivirus Japanese Encephalitis Virus
St. Louis encephalitis virus
West Nile Virus
Flavivirus: Virus Classification
Family Flaviviridae
3 G
-
7/27/2019 CNS Disorders (CD Nursing)
148/315
3 Genera Flavivirus, Pestivirus, Hepacivirus
Flavivirus - 12 Serogroups Japanese encephalitis virus
serogroup
Includes West Nile Virus (WNV), St. Louis Encephalitis, and
othe
Scanned images of West Nile virus isolated from tissue from a
crow found in New York.
-
7/27/2019 CNS Disorders (CD Nursing)
149/315
Viral Replication Cycle
http://arjournals.annualreviews.org/na101/home/literatum/ar/journals/production/micro/2002/56/1/annurev.micro.56.012302.160654/images/large/mi56_0371_2.jpeg
-
7/27/2019 CNS Disorders (CD Nursing)
150/315
Genome Structure
http://arjournals.annualreviews.org/na101/home/literatum/ar/journals/production/micro/2002/56/1/annurev.micro.56.012302.160654/images/large/mi56_0371_2.jpeghttp://arjournals.annualreviews.org/na101/home/literatum/ar/journals/production/micro/2002/56/1/annurev.micro.56.012302.160654/images/large/mi56_0371_1.jpeg
-
7/27/2019 CNS Disorders (CD Nursing)
151/315
Viral Genome
Positive Strand RNA Genome
1 ORF Genome encodes single polyprotein which is subseq
http://arjournals.annualreviews.org/na101/home/literatum/ar/journals/production/micro/2002/56/1/annurev.micro.56.012302.160654/images/large/mi56_0371_1.jpeg
-
7/27/2019 CNS Disorders (CD Nursing)
152/315
1 ORF Genome encodes single polyprotein which is subseq
cleaved 5 portion
3 structural proteins
3 portion 7 non-structural proteins
Genome also includes 5 and 3 noncoding regions which
hafunctional importance
Secondary structure loops
-
7/27/2019 CNS Disorders (CD Nursing)
153/315
3 Stem Loop of Plus Strand
Tertiary interactions of 3 non-coding region serve to
stabilizcompact the 3 region of the genome and may also create
b
-
7/27/2019 CNS Disorders (CD Nursing)
154/315
sites for cellular and/or viral proteins PseudoknotsFormed by
interactions between 3 stem loo
adjacent nucleotides
PK1 May be important for minus strand replication
Interacts with cellular proteins
P104, EF-1, and p84
Conserved Secondary and TertiaryTerminal RNA Structures in
MinusStrand
Stem loop structures at 5 and 3 ends are conserved
-
7/27/2019 CNS Disorders (CD Nursing)
155/315
Stem loop structures at 5 and 3 ends are conserved
across flavivirus species suggesting a functionalimportance for
these groups.
Minus strand stem loops may play a role in facilitatinthe
formation of replication complexes and inreleasing newly
synthesized minus strands from plus
strands. In addition, its interaction with cellular proteins
is
important for replication.
Viral Proteins: Structural and Non-Structural Structural
Proteins
Capsid (C), Membrane (M), Envelope (E)
-
7/27/2019 CNS Disorders (CD Nursing)
156/315
The envelope - receptor binding Dimers of E protein arrange
their sheets in a head to tail formati
flat on top of the lipid bilayer. The distal portions of these
proteinanchored in the membrane
Non-Structural Multifunctional Proteins NS1, NS2A, NS2B, NS3,
NS4A, NS4B, NS5
Many functions of non-structural proteins have yet to be de
Viral Non-Structural Proteins
NS1- may play a role in flavivirus RNA synthesis; it has been
shown to be essential fostrand synthesis
NS2A NS2B NS4A NS4B - may facilitate the assembly of viral
replication complexes
-
7/27/2019 CNS Disorders (CD Nursing)
157/315
NS2A, NS2B, NS4A, NS4B - may facilitate the assembly of viral
replication complexes
unknown mechanism NS3: Multifunctional
Proteolytic function upon association with NS2B
RNA triphosphatase function thought to be important for the
synthesis of the 5
Helicase and NTPase activity
Its activity may be upregulated through interaction with
phosphorylated NS5
NS5 RNA dependent RNA polymerase
Methyltransferase domain thought to be required for formation of
the 5 cap
Model for Closed-Loop Complex FormaFlaviviruses
-
7/27/2019 CNS Disorders (CD Nursing)
158/315
-
7/27/2019 CNS Disorders (CD Nursing)
159/315
Togavirus Eastern Equine Encephalitis Virus
Western Equine Encephalitis Virus
Venezuelan Equine Encephalitis Virus
Togavirus
Family: Togaviridae Genus: Alphavirus
-
7/27/2019 CNS Disorders (CD Nursing)
160/315
49S Single Stranded Genome ~11700 Nucleotides
3 end: Five potential structural proteins C, E3, E2, 6K, and
E1
5 end: Unknown number of non-structural proteins probab
involved in replication Genome has an opposite orientation from
the Flaviviruses
Alphavirus Structure
-
7/27/2019 CNS Disorders (CD Nursing)
161/315
http://www.cdc.gov/ncidod/dvbid/arbor/alphavir.htm
Alphaviruses: Protein Function
E1and E2 glycoprotein heterodimers form trimers that appear as
knobsurface of the virion
E1 transmembrane glycoprotein with 2 to 3 N-linked glycosylation
sites
-
7/27/2019 CNS Disorders (CD Nursing)
162/315
E2 - glycoprotein with 1 to 2 N-linked glycosylation sites,
contains short intracyand hydrophobic stretch of amino acids that
serves as the fusion peptide for vir
Capsid protein has a conserved N-terminal region which binds RNA
anterminal region which interacts with the cytoplasmic tail of E2
as well proteins
E3 and 6K proteins are signal sequences for E2 and E1,
respectively, anlargely cleaved off from the mature virion
Replication Cycle
Proposed Model: E1 glycoprotein interacts with proteins on the
cell subinds to cellular proteins and receptor-mediated endocytosis
takes pl
In acidified endosomal compartment glycoproteins fuse with
membra
-
7/27/2019 CNS Disorders (CD Nursing)
163/315
In acidified endosomal compartment, glycoproteins fuse with
membranucleocapsid is released.
Virion RNA serves as mRNA, translation of non-structural
proteins beg
Structural proteins are transcribed as polyprotein
E2 and E1 travel from ER to the Golgi
At cellular membrane regions containing E1 and E2 heterodimers
intenucleocapsids and viral particles bud from the cell surface
-
7/27/2019 CNS Disorders (CD Nursing)
164/315
BunyaviridaeLa Crosse Virus
La Crosse Virus
http://www.wadsworth.org/databank/lacrosse.htm/
-
7/27/2019 CNS Disorders (CD Nursing)
165/315
http://www.virology.net/Big_Virology/BVRN
Bunyaviruses
Genome - single strand of negative sense RNA
Four structural proteins
http://www.wadsworth.org/databank/lacrosse.htm/
-
7/27/2019 CNS Disorders (CD Nursing)
166/315
Two external proteins Two associated with RNA to form
nucleocapsid
Matrix proteins absent from Bunyaviruses, therefore capsid and
envelope glycoproteins directly interact prior to buddin
Bioweaponization
-
7/27/2019 CNS Disorders (CD Nursing)
167/315
http://www.cdc.gov/ncidod/dvbid/arbor/index.htm
Mosquito vector
T
ransmission Cycle is Key to
Weaponization
Incidental infection
-
7/27/2019 CNS Disorders (CD Nursing)
168/315
West Nile virus
Bird reservoir hosts Incidental infections
http://www.cdc.gov/ncidod/dvbid/westnile/conf/February_20
Bioweaponization
Vector, Vector, Vector In areas around NYC mosquitoes are
extremely ubiquitous during
months
-
7/27/2019 CNS Disorders (CD Nursing)
169/315
months
Mosquitoes are already virulent, further genetic
engineeringunnecessary
A fully effective cure is not available
Diagnosis is difficult
Widespread Panic would be generated as the outbreak prog
The Iraq Connection
The US shipped various pathogens, including WNV, to Iraq
in1980s
-
7/27/2019 CNS Disorders (CD Nursing)
170/315
In 1999 following the West Nile Virus outbreak in NYC therefears
that Iraqi bioterrorism was involved
Investigations by the CDC and the CIA found no evidence
ofbioterrorism in the 1999 outbreak
WNV as a low-tech Bioweapon:Possible Connection to 1999
outbreak
Gather mosquitoes in an endemic area
Incubate mosquitoes with a food source
-
7/27/2019 CNS Disorders (CD Nursing)
171/315
Put them to sleep Place mosquitoes in a matchbox
Board plane to US
Take bus from airport; Release mosquitoes from buswindow
Wait for outbreak
Source: Dr. Ilya Tr
-
7/27/2019 CNS Disorders (CD Nursing)
172/315
Clinical Considerations
Case Study
In August 2002, a 91 year old male from Northern Staten Island
who pinitially with sudden onset of fever, left lower extremity
weakness, inawalk, and possibly some transient and mild AMS, was
admitted to a Sthospital.
-
7/27/2019 CNS Disorders (CD Nursing)
173/315
hospital.
He was not considered to have aseptic meningitis or encephalitis
and infection was not considered at that time. After being
discharged, he evaluated by a neurologist for persistent left leg
weakness and inabilit
In April 2003, the neurologist reported this case to the DOHMH
as a ppolio case. Serological specimens were forwarded to the
NYSDOH whtested positive for WN virus.
-
7/27/2019 CNS Disorders (CD Nursing)
174/315
Clinical ConsiderationsDiagnosis
Patient History
Detailed history critical to determine the likely cause of
encephalitis.
Prodromal illness, recent vaccination, development of few days
Acute DisseminatEncephalomyelitis (ADEM) .
-
7/27/2019 CNS Disorders (CD Nursing)
175/315
Biphasic onset: systemic illness then CNS disease Enterovirus
encephalitis. Abrupt onset, rapid progression over few days
HSE.
Recent travel and the geographical context: Africa Cerebral
malaria
Asia Japanese encephalitis
High risk regions of Europe and USA Lyme disease
Recent animal bites Tick borne encephalitis or Rabies.
Occupation Forest worker, exposed to tick bites
Medical personnel, possible exposure to infectious diseases.
History cont.
Season Japanese encephalitis is more common during the rainy
season.
Arbovirus infections are more frequent during summer and
fall.
-
7/27/2019 CNS Disorders (CD Nursing)
176/315
Predisposing factors: Immunosuppression caused by disease and/or
drug treatment.
Organ transplant Opportunistic infections
HIV CNS infections
HSV-2 encephalitis and Cytomegalovirus infection (CMV)
Drug ingestion and/or abuse
Trauma
Initial Signs
Headache
Malaise
-
7/27/2019 CNS Disorders (CD Nursing)
177/315
Anorexia Nausea and Vomiting
Abdominal pain
Developing Signs
Altered LOC mild lethargy to deep coma.
AMS confused, delirious, disoriented.
-
7/27/2019 CNS Disorders (CD Nursing)
178/315
Mental aberrations: hallucinations agitation personality change
behavioral disorders occasionally frank psychosis
Focal or general seizures in >50% severe cases. Severe
focused neurologic deficits.
Neurologic Signs
Virtually every possible focal neurological disturbance has
breported.
-
7/27/2019 CNS Disorders (CD Nursing)
179/315
Most Common Aphasia Ataxia
Hemiparesis with hyperactive tendon reflexes
Involuntary movements
Cranial nerve deficits (ocular palsies, facial weakness)
Other Causes of Encephalopathy
Anoxic/Ischemic conditions
Metabolic disorders
Nutritional deficiency
-
7/27/2019 CNS Disorders (CD Nursing)
180/315
Toxic (Accidental & Intentional) Systemic infections
Critical illness
Malignant hypertension
Mitochondrial cytopathy (Reyes and MELAS syndromes)
Hashimotos encephalopathy
Traumatic brain injury Epileptic (non-convulsive status)
CJD (Mad Cow)
Differential Diagnosis
Distinguish Etiology (1) Bacterial infection and other
infectious conditions
(2) Parameningeal infections or partially treated bacterial
meningitis
(3) Nonviral infectious meningitides where cultures may be
negative (e.g., fung
-
7/27/2019 CNS Disorders (CD Nursing)
181/315
tuberculous, parasitic, or syphilitic disease) (5) Meningitis
secondary to noninfectious inflammatory diseases
MRI Can exclude subdural bleeds, tumor, and sinus thrombosis
Biopsy Reserved for patients who are worsening, have an
undiagnosed lesion after sca
response to acyclovir. Clinical signs cannot distinguish
different viral encephalitides
Differential Diagnosis cont.
Encephalopathy Encephalitis
Fever Uncommon Common
Headache Uncommon Common
-
7/27/2019 CNS Disorders (CD Nursing)
182/315
AMS Steady deterioration May fluctuate
Focal Neurologic Signs Uncommon Common
Types of seizures Generalized Both
Blood: Leukocytosis Uncommon Common
CSF: Pleocytosis Uncommon Common
EEG: Diffuse slowing Common +Focal
MRI Often normal Focal Abn.
Cli i l C id ti
-
7/27/2019 CNS Disorders (CD Nursing)
183/315
Clinical ConsiderationsRadiology
MRI
-
7/27/2019 CNS Disorders (CD Nursing)
184/315
MRI
-
7/27/2019 CNS Disorders (CD Nursing)
185/315
Cli i l C id ti
-
7/27/2019 CNS Disorders (CD Nursing)
186/315
Clinical ConsiderationsLaboratory Diagnosis
Laboratory Diagnosis
Diagnosis is usually based on CSF Normal glucose
Absence of bacteria on culture.
Vi i ll i l t d di tl f CSF
-
7/27/2019 CNS Disorders (CD Nursing)
187/315
Viruses occasionally isolated directly from CSF Less than half
are identified
Polymerase Chain Reaction techniques Detect specific viral DNA
in CSF
NYSDOH PCRNEW YORK STATE DEPARTMENT OF HEALTH (NYSDOH)
Viral Encephalitis Letter of Agreement for
Physician Ordered Testing by Polymerase Chain Reaction (PCR)
NYSDOH's Wadsworth Center offers the following tests on CSF for
viral encephalitis:
PCR testing for a panel of viruses including: herpes simplex
varicella zoster cytomegalovirus( ) ( )
-
7/27/2019 CNS Disorders (CD Nursing)
188/315
PCR testing for a panel of viruses, including: herpes simplex,
varicella zoster, cytomegalovirus,Epstein-Barr virus,
enteroviruses, St. Louis encephalitis (SLE), eastern equine
encephalitis (EEE),California encephalitis (including LaCrosse and
Jamestown Canyon viruses), Powassan and West N(WN) viruses, and
Enzyme-linked immunoassay (ELISA) for WN virus.
If there is insufficient quantity of CSF (less than 1.0 ml) to
conduct both ELISA and PCR for WN virplease consider the following
in determining which test is most appropriate for your patient:
ELISA is more sensitive than PCR for WN viral testing and should
be considered when there isstronger suspicion of WN virus than
other viruses.
PCR is less sensitive for WN virus, but tests for a wide range
of viruses. PCR should be considered
viruses other than WN virus are suspected.
Please note your testing priority below or on the viral
encephalitis/meningitis case report form. IPCR testing is desired,
the agreement below must be completed.
Viral Encephalitis PCR Panel West Nile Virus ELISA Antibody
Testing
Cli i l C id ti
-
7/27/2019 CNS Disorders (CD Nursing)
189/315
Clinical ConsiderationsDisease Progression
Disease Progression
Worsening neurologic symptoms
Vascular collapse and shock May be due to adrenal
insufficiency.
-
7/27/2019 CNS Disorders (CD Nursing)
190/315
Loss of tissue fluid may be equally important.
Homeostatic failure
Decreased respiratory drive
Cli i l C id ti
-
7/27/2019 CNS Disorders (CD Nursing)
191/315
Clinical ConsiderationsTreatment
Treatment
When HSE cannot be ruled out, Acyclovir must be started p(before
the patient lapses into coma) and continued at leastfor maximal
therapeutic benefit.
Rocky Mountain spotted fever should also be considered an
-
7/27/2019 CNS Disorders (CD Nursing)
192/315
Rocky Mountain spotted fever should also be considered,
antreatment with Doxycycline is indicated.
Suspected HSE Treatment Plan
-
7/27/2019 CNS Disorders (CD Nursing)
193/315
Acyclovir
Acyclovir is a synthetic purine nucleoside analogue with
inhactivity against HSV-1 and HSV-2, varicella-zoster virus
(VZVBarr virus (EBV) and cytomegalovirus (CMV)
In order of decreasing effectiveness
-
7/27/2019 CNS Disorders (CD Nursing)
194/315
In order of decreasing effectiveness
Highly selective
Acyclovir Action Thymidine Kinase (TK) of uninfected cells does
not use acyclovir as a substrate.
TK encoded by HSV, VZV and EBV2 converts acyclovir into
acyclovir monophosphate
The monophosphate is further converted into diphosphate by
cellular guanylate kintriphosphate by a number of cellular
enzymes.
Acyclovir triphosphate interferes with Herpes simplex virus DNA
polymerase and inh
-
7/27/2019 CNS Disorders (CD Nursing)
195/315
Acyclovir triphosphate interferes with Herpes simplex virus DNA
polymerase and inhDNA replication.
Acyclovir triphosphate incorporated into growing chains of DNA
by viral DNA polym
When incorporation occurs, the DNA chain is terminated.
Acyclovir is preferentially taken up and selectively converted
to the active triphosphHSV-infected cells.
Thus, acyclovir is much less toxic in vitro for normal
uninfected cells because: 1) less2) less is converted to the active
form.
Supportive Therapy Fever, dehydration, electrolyte imbalances,
and convulsions require treatment.
For cerebral edema severe enough to produce herniation,
controlled hyperventilatioand dexamethasone.
Patients with cerebral edema must not be overhydrated.
If these measures are used, monitoring ICP should be
considered.
-
7/27/2019 CNS Disorders (CD Nursing)
196/315
, g If there is evidence of ventricular enlargement,
intracranial pressure may be monito
conjunction with CSF drainage.
Outcome is usually poor.
For infants with subdural effusion, repeated daily subdural taps
through the sutures usu
No more than 20 mL/day of CSF should be removed from one side to
prevent sudden shintracranial contents.
If the effusion persists after 3 to 4 weeks of taps, surgical
exploration for possible excisio
membrane is indicated.
Dexamethasone
Synthetic adrenocortical steroid
Potent anti-inflammatory effects
Dexamethasone injection is generally administered
initiallyIM
-
7/27/2019 CNS Disorders (CD Nursing)
197/315
Dexamethasone injection is generally administered initially
IM
Side effects: convulsions; increased ICP after treatment;
verheadache; psychic disturbances
Clinical Considerations
-
7/27/2019 CNS Disorders (CD Nursing)
198/315
Clinical ConsiderationsPatient Prognosis
Prognosis The mortality rate varies with etiology, and epidemics
due to the sam
in severity in different years.
Bad: Eastern equine encephalitis virus infection, nearly 80% of
survivors have seneurological sequelae.
Not so Bad: EBV, California encephalitis virus, and Venezuelan
equine encephal
-
7/27/2019 CNS Disorders (CD Nursing)
199/315
, p , q psevere sequelae are unusual.
Approximately 5 to 15% of children infected with LaCrosse virus
have a residuadisorder, and 1% have persistent hemiparesis.
Permanent cerebral sequelae are more likely to occur in infants,
but ychildren improve for a longer time than adults with similar
infections.
Intellectual impairment, learning disabilities, hearing loss,
and other lasting seqbeen reported in some studies.
Prognosis w/ Treatment Considerable variation in the incidence
and severity of sequelae.
Hard to assess effects of treatment.
NIAID-CASG trials: The incidence and severity of sequelae were
directly related to the age of the patient an
consciousness at the time of initiation of therapy. Patients
with severe neurological impairment (Glasgow coma score 6) at
initiation of the
-
7/27/2019 CNS Disorders (CD Nursing)
200/315
Patients with severe neurological impairment (Glasgow coma score
6) at initiation of thedied or survived with severe sequelae.
Young patients (
-
7/27/2019 CNS Disorders (CD Nursing)
201/315
Verbal Incomprehensible words 2
Response Inappropriate words 3
Disoriented conversation 4
Oriented conversation 5
Best None 1
Motor Abnormal extension 2
Response Abnormal flexion 3
Flexion withdrawal 4
Localizes pain 5
______________Obeys commands _________6 _
Total score 3-15
Clinical Considerations
-
7/27/2019 CNS Disorders (CD Nursing)
202/315
Clinical ConsiderationsVaccination
Vaccination
None for most Encephalitides
JE Appears to be 91% effective
There is no JE-specific therapy other than supportive care
-
7/27/2019 CNS Disorders (CD Nursing)
203/315
p py pp
Live-attenuated vaccine developed and tested in China Appears to
be safe and effective
Chinese immunization programs involving millions of children
Vero cell-derived inactivated vaccines have been developed in
Chi 2 millions doses are produced annually in China and Japan
Several other JE vaccines under development
Public Health
Considerations
-
7/27/2019 CNS Disorders (CD Nursing)
204/315
ConsiderationsEndemic Prevention
Infection Control CDCs Three Ways to Reduce your West Nile Virus
Risk
Avoid mosquito bites
Mosquito-proof your home
Help your community
-
7/27/2019 CNS Disorders (CD Nursing)
205/315
Avoid Mosquito Bites Apply Insect Repellent Containing DEET
Clothing Can Help Reduce Mosquito Bites Cover up
Be Aware of Peak Mosquito Hours
-
7/27/2019 CNS Disorders (CD Nursing)
206/315
Be Aware of Peak Mosquito Hours
Dusk to dawn are peak mosquito biting times for many
species.
Mosquito-Proof Home Drain Standing Water
Install or Repair Screens
-
7/27/2019 CNS Disorders (CD Nursing)
207/315
Community-Wide Efforts Clean Up Breeding Grounds
Ensure Safe Blood Supply
Mosquito Control Programs
Controversial
-
7/27/2019 CNS Disorders (CD Nursing)
208/315
Controversial
Surveillance
Blood Supply NYC Policy Statement reflecting FDA policy:
To reduce WN transmission through blood components. donations
will be screened for WN virus RNA using nucleic
amplification tests (NAT). In the event of a NAT-reactive donbl
d ll d ll bl d
-
7/27/2019 CNS Disorders (CD Nursing)
209/315
blood centers will remove and quarantine all blood
componassociated with the donation and notify the state or local
hedepartment. In addition, blood testing centers have added
questions to identify and exclude persons with fever and he
the week prior to donation.
Mosquito Control ProgramsNYC DOHMH Statement:
We hope that spraying of adulticides will not be required
thsummer. However, if there is a threat of an outbreak of hum
and spraying is deemed necessary, targeted adult mosquito ( i d
i l i f i id ) b
-
7/27/2019 CNS Disorders (CD Nursing)
210/315
measures (via ground or aerial spraying of pesticides) may
brequired.
Mosquito Control But wait, theres more:
Same Memo:
Confirmed or suspected cases of pesticide poisoning must
breported to the New York State Department of Healths Pest
-
7/27/2019 CNS Disorders (CD Nursing)
211/315
p pPoisoning Registry at (800)-322-6850, and to the New York
CControl Center at (212)-764-7667.
Whats Being Sprayed The adulticides used during the last three
seasons in New Yo
Sumithrin, a pyrethroid.
Although pyrethroids are among the least toxic
insecticides,nerve poisons, and act upon the sodium ion channels in
ner
membranes.I h li th id i ti id hi h i
-
7/27/2019 CNS Disorders (CD Nursing)
212/315
Inhaling pyrethroid insecticides can cause coughing,
wheezishortness of breath, runny or stuffy nose, chest pain, or
diffbreathing.
Skin contact can cause a rash, itching, or blisters.
Sumithrin is not very toxic to mammals, but it is highly
toxicand fish.
-
7/27/2019 CNS Disorders (CD Nursing)
213/315
Crop-Dusting NYC? Aerosolized liquids sprayed over large areas
of the city.
Terrorism concern?
New vector for urban area.
-
7/27/2019 CNS Disorders (CD Nursing)
214/315
Public Health
Considerationsll
-
7/27/2019 CNS Disorders (CD Nursing)
215/315
ConsiderationsSurveillance
SurveillanceSince 2000, the NYC DOHMH has conducted
comprehensive arthropodisease surveillance and control. In 2003,
efforts will again focus on mcontrol through reduction of breeding
sites and application of larvicidaddition, comprehensive mosquito,
avian and human data collected d
2000-2002 seasons have allowed NYC DOHMH to develop more
sensitsurveillance criteria for determining the level of WN viral
activity in bi
-
7/27/2019 CNS Disorders (CD Nursing)
216/315
surveillance criteria for determining the level of WN viral
activity in bimosquitoes that may indicate a significant risk for a
human outbreak. indicators will be monitored citywide to identify
areas at risk for humatransmission.
Standing Water ReportingThe Department of Health & Mental
Hygiene is now acceptiof standing water. However, we will not be
able to visit and treported nuisances. Therefore we are encouraging
City resid
business owners to take immediate action to eliminate stanon
their property.
-
7/27/2019 CNS Disorders (CD Nursing)
217/315
p p y
Dead-Bird Reporting Online form
http://www.nyc.gov/html/doh/html/wnv/wnvbird.html
The Department of Health & Mental Hygiene is now accepti
of dead birds. Only a sample of dead birds that meet specifiwill
be picked up and tested for the West Nile virus. Howeve
http://www.nyc.gov/html/doh/html/wnv/wnvbird.htmlhttp://www.nyc.gov/html/doh/html/wnv/wnvbird.html
-
7/27/2019 CNS Disorders (CD Nursing)
218/315
will be picked up and tested for the West Nile virus.
Howevereport of a dead bird is extremely important to us because
dreports may indicate the presence of West Nile virus. If you
receive a call back from the Department of Health within twbusiness
days of making your report, please dispose of the b
Mosquito TestingFive pools of mosquitoes collected in New York
City have tested positWest Nile (WN) virus. These include a pool
ofCulex salinarius, a humamosquito, collected on July 15, in the
Willowbrook Park area of Statenpool of Culex restuans, primarily a
bird-biting mosquito, collected fro
Park, Queens on July 17, a pool ofCulex pipiens, a mosquito that
bitesand humans, collected from the Hunts Point area of the Bronx
on July
-
7/27/2019 CNS Disorders (CD Nursing)
219/315
and humans, collected from the Hunts Point area of the Bronx on
July ofCulexspecies collected from Jamaica Bay, Queens on July 16,
and a Culex salinarius collected from Greenwood Cemetery, Brooklyn
on Julpositive pools are the first evidence of West Nile (WN) virus
in New Yo2003
Disease ReportingThe New York City Department of Health and
Mental HygieDOHMH) is again requesting that during the peak adult
mosseason, from June 1 October 31, 2003, all suspected cases
encephalitis (all ages) and viral meningitis (adults only) be
rimmediately by telephone or facsimile and that appropriate
-
7/27/2019 CNS Disorders (CD Nursing)
220/315
laboratory specimens (cerebrospinal fluid and sera) be
submpromptly for testing for West Nile (WN) virus.
POLIOMYELITIS
-
7/27/2019 CNS Disorders (CD Nursing)
221/315
POLIOMYELITIS
-
7/27/2019 CNS Disorders (CD Nursing)
222/315
What is Poliomyelitis? polio= gray matter
Myelitis= inflammation of the spinal cord
This disease result in the destruction of motor neurons
causpoliovirus.
f
-
7/27/2019 CNS Disorders (CD Nursing)
223/315
Polio is causes by a virus that attacks the nerve cells of the
bspinal cord although not all infections result in sever
injuriesparalysis.
When was it reported? Poliomyelitis was recorded in the late
1700s with the first e
the late 1800s.
The cases that were reported in 1979 where mild and self-li
do not result in paralysis.
-
7/27/2019 CNS Disorders (CD Nursing)
224/315
How is polio transmitted? Poliovirus is transmitted through both
oral and fical routes w
implantation and replication occurring in either the orapgarand
or in the intestine of mucosa. Polio cases are most infec
10 days before and after clinical symptoms begin.
-
7/27/2019 CNS Disorders (CD Nursing)
225/315
What are the symptoms? Many include fever, pharyngitis,
headache, anorexia, nausea
vomiting. Illness may progress to aseptic meningitis
andmenigoencephalitis in 1% to 4% of patients. These patients
higher fever, myalia and sever headache with stiffness of
theback.
-
7/27/2019 CNS Disorders (CD Nursing)
226/315
Polio in children
http://tm.wc.ask.com/r?t=an&s=p&uid=0D84491B2F2231504&sid=124738D5C207A8804&qid=338CF7577F473C4AB3248DDD86845A21&io=12&sv=za5cb0de8&o=0&ask=polio&uip=cdbc74c9&en=is&eo=-100&pt=&ac=7&qs=1&pg=8&u=http://pictures.ask.com/redir?bpg=http%3a%2f%2fpictures.ask.com%2fpictures%3fq%3dpolio%26o%3d0%26page%3d8&q=polio&u=http%3a%2f%2fwww.rds-online.org.uk%2fmilestones%2fpolio.html&s=p&bu=http%3a%2f%2fwww.rds-online.org.uk%2fmilestones%2fpolio.html&qte=0&o=0&isimageSearch=true&fromImagePage=False&iskey=&thumbsrc=http%3a%2f%2fimages.picsearch.com%2fis%3f32355078933&imagesrc=http%3a%2f%2fwww.rds-online.org.uk%2fimages%2fpolio.jpg&thumbwidth=128&thumbheight=108http://tm.wc.ask.com/r?t=an&s=p&uid=0D84491B2F2231504&sid=124738D5C207A8804&qid=338CF7577F473C4AB3248DDD86845A21&io=7&sv=za5cb0dc6&o=0&ask=polio&uip=cdbc74d2&en=is&eo=-100&pt=&ac=7&qs=1&pg=6&u=http://pictures.ask.com/redir?bpg=http%3a%2f%2fpictures.ask.com%2fpictures%3fq%3dpolio%26o%3d0%26page%3d6&q=polio&u=http%3a%2f%2fwww.mumbai.de%2ffpage_01.htm&s=p&bu=http%3a%2f%2fwww.mumbai.de%2ffpage_01.htm&qte=0&o=0&isimageSearch=true&fromImagePage=False&iskey=&thumbsrc=http%3a%2f%2fimages.picsearch.com%2fis%3f489110965089&imagesrc=http%3a%2f%2fwww.mumbai.de%2ffpage_01.jpg&thumbwidth=128&thumbheight=108http://tm.wc.ask.com/r?t=an&s=p&uid=0D84491B2F2231504&sid=124738D5C207A8804&qid=338CF7577F473C4AB3248DDD86845A21&io=7&sv=za5cb0dc6&o=0&ask=polio&uip=cdbc74d2&en=is&eo=-100&pt=&ac=7&qs=1&pg=6&u=http://pictures.ask.com/redir?bpg=http%3a%2f%2fpictures.ask.com%2fpictures%3fq%3dpolio%26o%3d0%26page%3d6&q=polio&u=http%3a%2f%2fwww.mumbai.de%2ffpage_01.htm&s=p&bu=http%3a%2f%2fwww.mumbai.de%2ffpage_01.htm&qte=0&o=0&isimageSearch=true&fromImagePage=False&iskey=&thumbsrc=http%3a%2f%2fimages.picsearch.com%2fis%3f489110965089&imagesrc=http%3a%2f%2fwww.mumbai.de%2ffpage_01.jpg&thumbwidth=128&thumbheight=108http://tm.wc.ask.com/r?t=an&s=p&uid=0D84491B2F2231504&sid=124738D5C207A8804&qid=338CF7577F473C4AB3248DDD86845A21&io=7&sv=za5cb0dc6&o=0&ask=polio&uip=cdbc74d2&en=is&eo=-100&pt=&ac=7&qs=1&pg=6&u=http://pictures.ask.com/redir?bpg=http%3a%2f%2fpictures.ask.com%2fpictures%3fq%3dpolio%26o%3d0%26page%3d6&q=polio&u=http%3a%2f%2fwww.mumbai.de%2ffpage_01.htm&s=p&bu=http%3a%2f%2fwww.mumbai.de%2ffpage_01.htm&qte=0&o=0&isimageSearch=true&fromImagePage=False&iskey=&thumbsrc=http%3a%2f%2fimages.picsearch.com%2fis%3f489110965089&imagesrc=http%3a%2f%2fwww.mumbai.de%2ffpage_01.jpg&thumbwidth=128&thumbheight=108http://tm.wc.ask.com/r?t=an&s=p&uid=0D84491B2F2231504&sid=124738D5C207A8804&qid=338CF7577F473C4AB3248DDD86845A21&io=7&sv=za5cb0dc6&o=0&ask=polio&uip=cdbc74d2&en=is&eo=-100&pt=&ac=7&qs=1&pg=6&u=http://pictures.ask.com/redir?bpg=http%3a%2f%2fpictures.ask.com%2fpictures%3fq%3dpolio%26o%3d0%26page%3d6&q=polio&u=http%3a%2f%2fwww.mumbai.de%2ffpage_01.htm&s=p&bu=http%3a%2f%2fwww.mumbai.de%2ffpage_01.htm&qte=0&o=0&isimageSearch=true&fromImagePage=False&iskey=&thumbsrc=http%3a%2f%2fimages.picsearch.com%2fis%3f489110965089&imagesrc=http%3a%2f%2fwww.mumbai.de%2ffpage_01.jpg&thumbwidth=128&thumbheight=108http://tm.wc.ask.com/r?t=an&s=p&uid=0D84491B2F2231504&sid=124738D5C207A8804&qid=338CF7577F473C4AB3248DDD86845A21&io=7&sv=za5cb0dc6&o=0&ask=polio&uip=cdbc74d2&en=is&eo=-100&pt=&ac=7&qs=1&pg=6&u=http://pictures.ask.com/redir?bpg=http%3a%2f%2fpictures.ask.com%2fpictures%3fq%3dpolio%26o%3d0%26page%3d6&q=polio&u=http%3a%2f%2fwww.mumbai.de%2ffpage_01.htm&s=p&bu=http%3a%2f%2fwww.mumbai.de%2ffpage_01.htm&qte=0&o=0&isimageSearch=true&fromImagePage=False&iskey=&thumbsrc=http%3a%2f%2fimages.picsearch.com%2fis%3f489110965089&imagesrc=http%3a%2f%2fwww.mumbai.de%2ffpage_01.jpg&thumbwidth=128&thumbheight=108http://tm.wc.ask.com/r?t=an&s=p&uid=0D84491B2F2231504&sid=124738D5C207A8804&qid=338CF7577F473C4AB3248DDD86845A21&io=3&sv=za5cb0dc1&o=0&ask=polio&uip=cdbc74c9&en=is&eo=-100&pt=&ac=7&qs=1&pg=2&u=http://pictures.ask.com/redir?bpg=http%3a%2f%2fpictures.ask.com%2fpictures%3fq%3dpolio%26o%3d0%26page%3d2&q=polio&u=http%3a%2f%2fwww.ibabydoc.com%2fonline%2fimages%2fillnesses%2fpolio9.htm&s=p&bu=http%3a%2f%2fwww.ibabydoc.com%2fonline%2fimages%2fillnesses%2fpolio9.htm&qte=0&o=0&isimageSearch=true&fromImagePage=False&iskey=&thumbsrc=http%3a%2f%2fimages.picsearch.com%2fis%3f393472259799&imagesrc=http%3a%2f%2fwww.ibabydoc.com%2fonline%2fimages%2fillnesses%2fimg0009.jpg&thumbwidth=85&thumbheight=128
-
7/27/2019 CNS Disorders (CD Nursing)
227/315
Can it cause paralyzes? Paralytic disease occurs 0.1% to 1% of
those who become in
with the polio virus.
Paralysis of the respiratory muscles or from cardiac arrest
if
neurons in the medulla oblongata are destroyed. Patients have
some or full recovery from paralysis usually a
http://tm.wc.ask.com/r?t=an&s=p&uid=0D84491B2F2231504&sid=124738D5C207A8804&qid=338CF7577F473C4AB3248DDD86845A21&io=12&sv=za5cb0de8&o=0&ask=polio&uip=cdbc74c9&en=is&eo=-100&pt=&ac=7&qs=1&pg=8&u=http://pictures.ask.com/redir?bpg=http%3a%2f%2fpictures.ask.com%2fpictures%3fq%3dpolio%26o%3d0%26page%3d8&q=polio&u=http%3a%2f%2fwww.rds-online.org.uk%2fmilestones%2fpolio.html&s=p&bu=http%3a%2f%2fwww.rds-online.org.uk%2fmilestones%2fpolio.html&qte=0&o=0&isimageSearch=true&fromImagePage=False&iskey=&thumbsrc=http%3a%2f%2fimages.picsearch.com%2fis%3f32355078933&imagesrc=http%3a%2f%2fwww.rds-online.org.uk%2fimages%2fpolio.jpg&thumbwidth=128&thumbheight=108http://tm.wc.ask.com/r?t=an&s=p&uid=0D84491B2F2231504&sid=124738D5C207A8804&qid=338CF7577F473C4AB3248DDD86845A21&io=3&sv=za5cb0dc1&o=0&ask=polio&uip=cdbc74c9&en=is&eo=-100&pt=&ac=7&qs=1&pg=2&u=http://pictures.ask.com/redir?bpg=http%3a%2f%2fpictures.ask.com%2fpictures%3fq%3dpolio%26o%3d0%26page%3d2&q=polio&u=http%3a%2f%2fwww.ibabydoc.com%2fonline%2fimages%2fillnesses%2fpolio9.htm&s=p&bu=http%3a%2f%2fwww.ibabydoc.com%2fonline%2fimages%2fillnesses%2fpolio9.htm&qte=0&o=0&isimageSearch=true&fromImagePage=False&iskey=&thumbsrc=http%3a%2f%2fimages.picsearch.com%2fis%3f393472259799&imagesrc=http%3a%2f%2fwww.ibabydoc.com%2fonline%2fimages%2fillnesses%2fimg0009.jpg&thumbwidth=85&thumbheight=128
-
7/27/2019 CNS Disorders (CD Nursing)
228/315
Patients have some or full recovery from paralysis usually awith
proximally 6 months
Physical therapy is recommended for full recovery.
Treatment Bed rest with close monitoring of respiratory and
cardiovasc
functioning is essential during the acute stage of
poliomyeliwith fever control and pain relievers for muscle
spasms.
Mechanical ventilation, respiratory therapy may be
neededdepending of the severity of patients.
-
7/27/2019 CNS Disorders (CD Nursing)
229/315
Vaccine Polio vaccine first appeared to be licensed in the
United Stat
1955.
Advantages:
Ease to administration
Good local mucosal immunity
http://tm.wc.ask.com/r?t=an&s=p&uid=0D84491B2F2231504&sid=124738D5C207A8804&qid=338CF7577F473C4AB3248DDD86845A21&io=0&sv=za5cb0d89&o=0&ask=polio&uip=cdbc7493&en=is&eo=-100&pt=&ac=7&qs=1&pg=5&u=http://pictures.ask.com/redir?bpg=http%3a%2f%2fpictures.ask.com%2fpictures%3fq%3dpolio%26o%3d0%26page%3d5&q=polio&u=http%3a%2f%2fwww.polioplus.us%2f&s=p&bu=http%3a%2f%2fwww.polioplus.us%2f&qte=0&o=0&isimageSearch=true&fromImagePage=False&iskey=&thumbsrc=http%3a%2f%2fimages.picsearch.com%2fis%3f911523601502&imagesrc=http%3a%2f%2fwww.polioplus.us%2fImages%2fvaccine.jpg&thumbwidth=85&thumbheight=128
-
7/27/2019 CNS Disorders (CD Nursing)
230/315
Good local mucosal immunity
Disadvantage:
Strict cold shipping & storage requirements
Multiple doses required to achieve high humeral
conservatiagainst all virus types
Vaccine (continuation)
Babies are given 4 doses through out their infancy.
Adolescents and adults should get vaccinated as weAdolescents
younger than 18 should receive theroutine four doses.
You should get it if you travel outside places wherepolio id
still an epidemic
http://tm.wc.ask.com/r?t=an&s=p&uid=0D84491B2F2231504&sid=124738D5C207A8804&qid=338CF7577F473C4AB3248DDD86845A21&i