Embed Size (px)
Citation preview
Clinical ReviewClinical Review AbioCor® Implantable Replacement HeartAbioCor® Implantable Replacement Heart
H040006H040006
Julie Swain M.D.
Cardiovascular Surgeon
Ileana Piña M.D.
Heart Failure Cardiologist
DRAFT
2
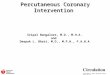
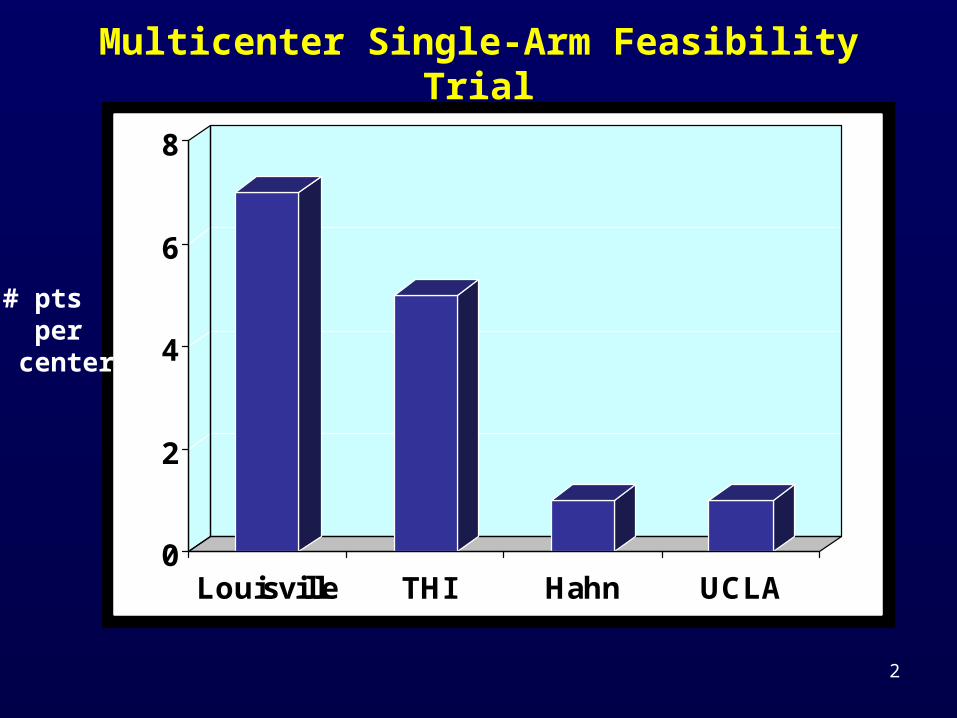
Multicenter Single-Arm Feasibility Trial
0
2
4
6
8
Louisville THI Hahn UCLA
# pts per center
3
Indication For Use
The AbioCor is designed to serve a subset of transplant-ineligible end-
stage heart failure patients with biventricular failure not treatable by drugs, pacing devices, or approved
cardiac assist devices.
4
Approved HUD Inclusion
Heart failure patients who are on optimal medical therapy and meet all of the following:
• < 75 years old • not transplant candidates • estimated 30-day survival of <30%• in biventricular failure not supportable by an
implantable left ventricular assist device (LVAD) alone
• multiple inotropes OR those not weanable from a temporary BIVAD
5
Proposed Additional Inclusions(page 69, Post Approval Study)
The Sponsor claims patients with contraindications to LVAD placement would be included in the indications for the device:
• refractory arrhythmias• aortic regurgitation• prosthetic aortic valve• “Massive MI”: patients who are “…at risk of inlet cannula
dislodgement due to fragility of the infarcted ventricular tissue.”• Mural thrombus in the ventricles• Ventricular septal rupture• Transplant rejection
** It should be noted that none of the 14 patients in the feasibility study had any of the above conditions
6
Post Hoc Proposed Controls
• REMATCH control pts– Changes in medical care – Different patients (LV failure, gatekeeper, OMM)– Subset analysis (61 pts, many withdrew from care)
• AMI-SHOCK Index– No pts had acute MI
• AbioScore– 42 prospective and retrospective records– ICD-9 codes for heart failure and CPT and NDC
codes for inadequate hemodynamics – age 20 - 79 years – 26% were female – 38% were on LVAD’s for bridge-to-transplant
7
AbioScore
• used to estimate survival for inclusion of > 70% mortality in 30 days
• 27 clinical items (renal function, NYHA class, etc.)
• components include items normally used by clinicians
• validation unproven• No known predictive system• Very ill, malnourished patients
8
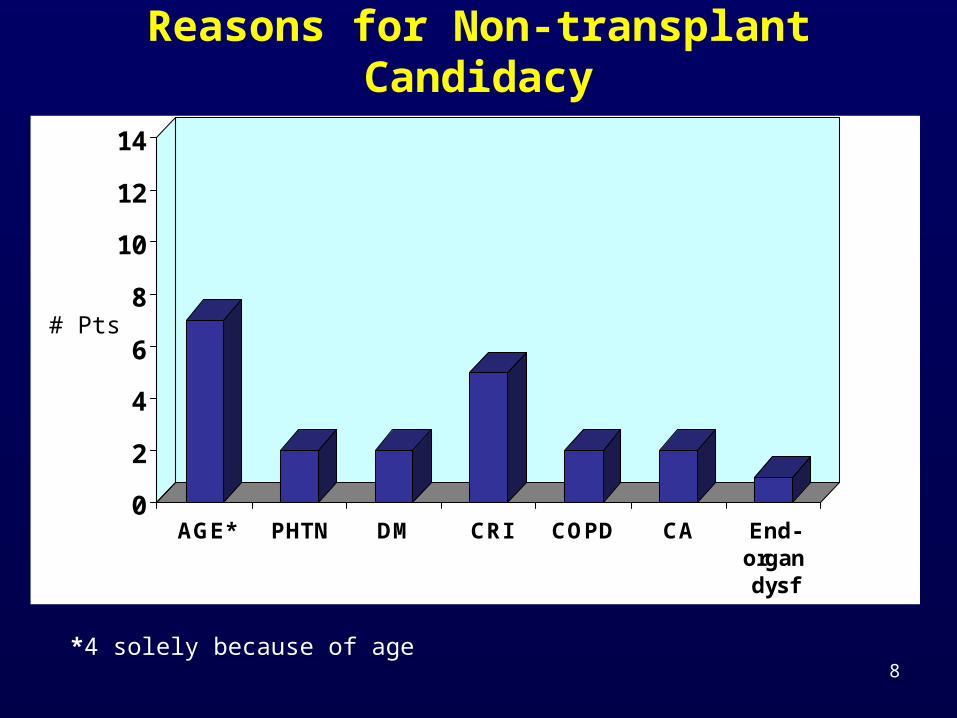
Reasons for Non-transplant Candidacy
0
2
4
6
8
10
12
14
AGE* PHTN DM CRI COPD CA End-organdysf
# Pts
*4 solely because of age
9
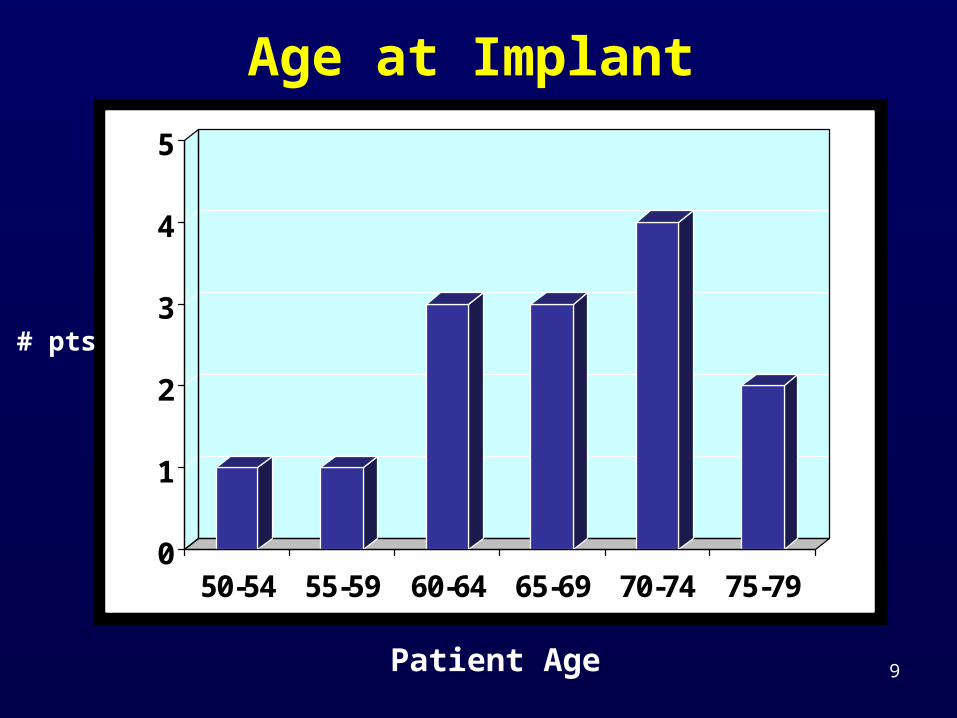
Age at Implant
0
1
2
3
4
5
50-54 55-59 60-64 65-69 70-74 75-79
# pts
Patient Age
10
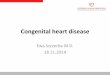
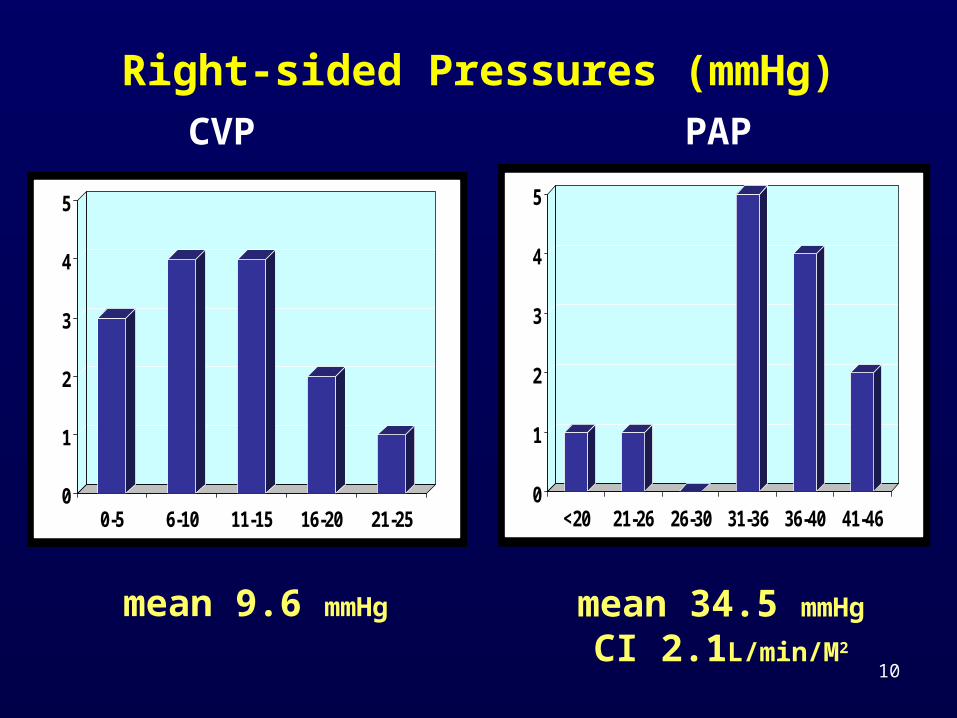
Right-sided Pressures (mmHg)
0
1
2
3
4
5
0-5 6-10 11-15 16-20 21-250
1
2
3
4
5
<20 21-26 26-30 31-36 36-40 41-46
CVP PAP
mean 9.6 mmHg mean 34.5 mmHg
CI 2.1L/min/M2
11
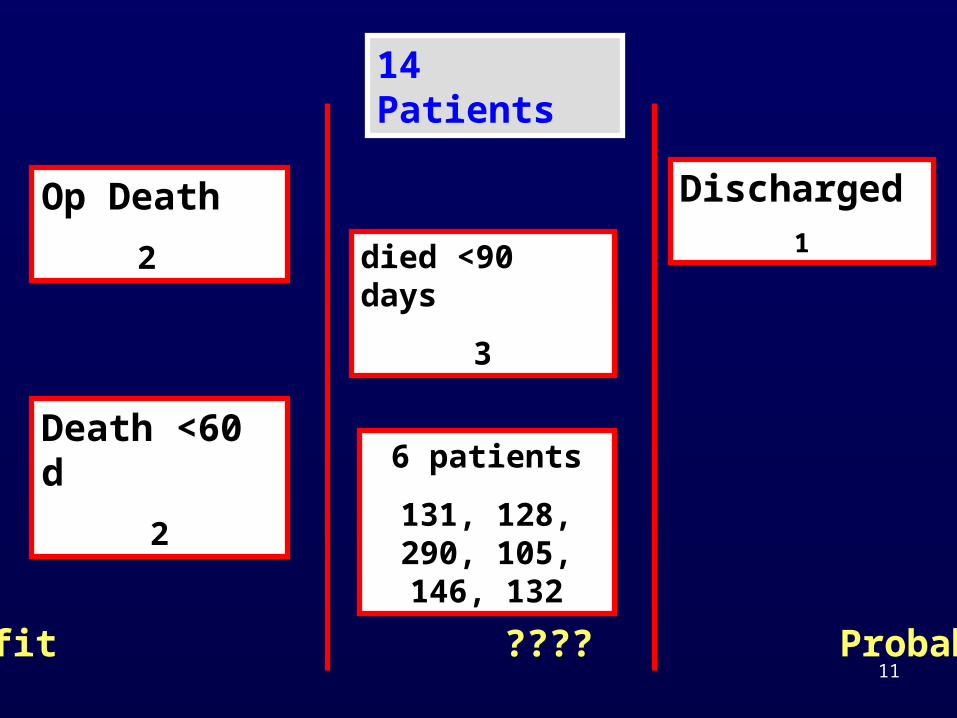
14 Patients
6 patients
131, 128, 290, 105, 146, 132
Death <60 d
2
Op Death
2
Discharged1
No Benefit ???? Probable Benefit
died <90 days
3
12
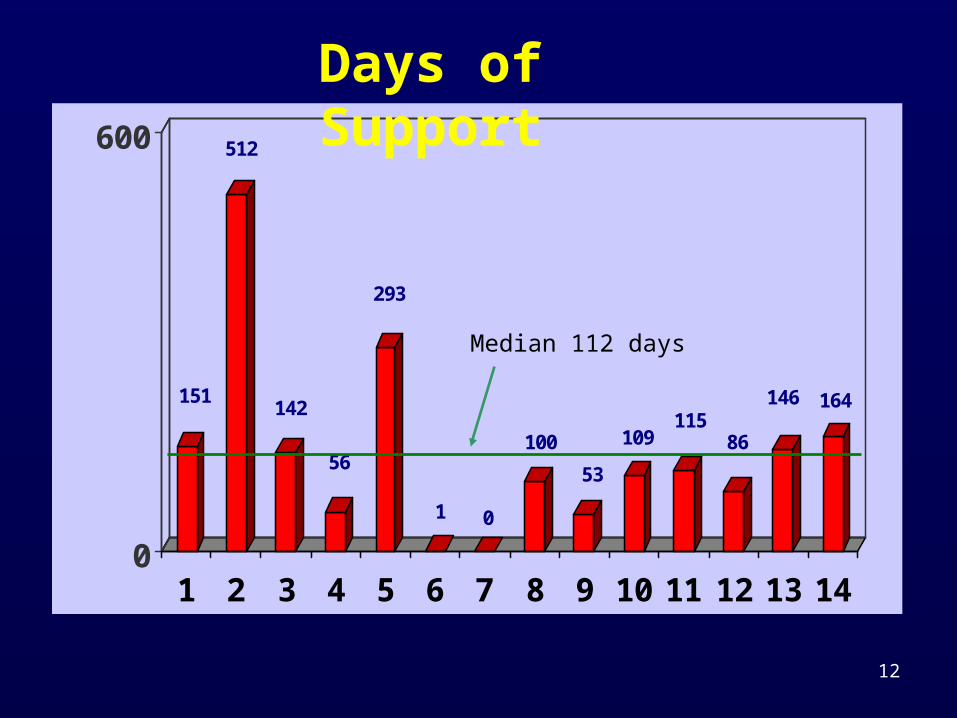
151
512
142
56
293
1 0
100
53
109115
86
146 164
0
600
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Days of Support
Median 112 days
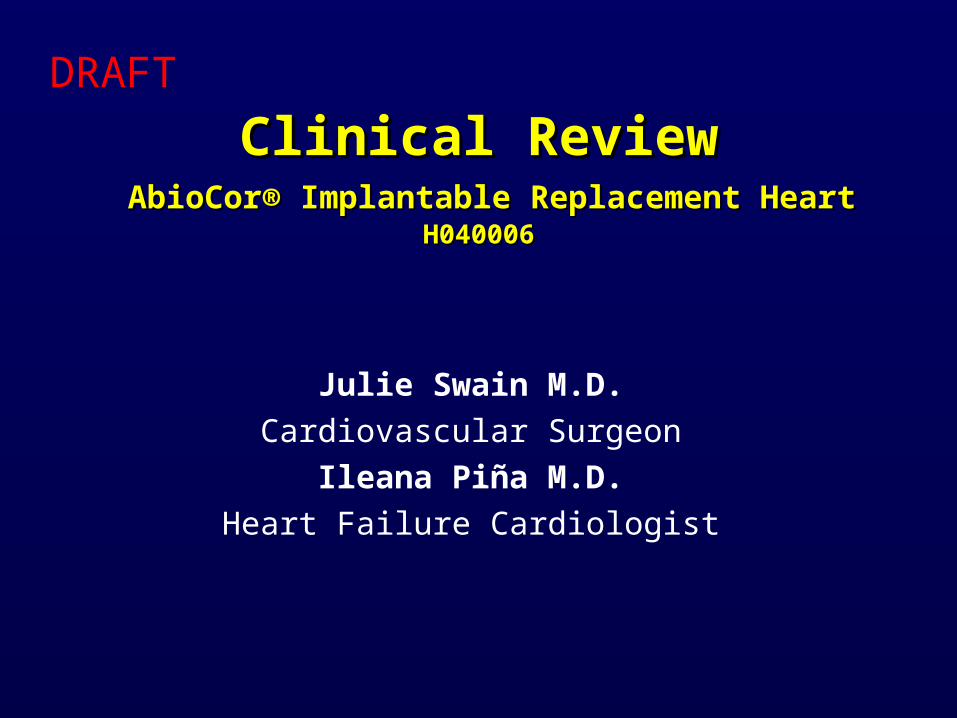
13
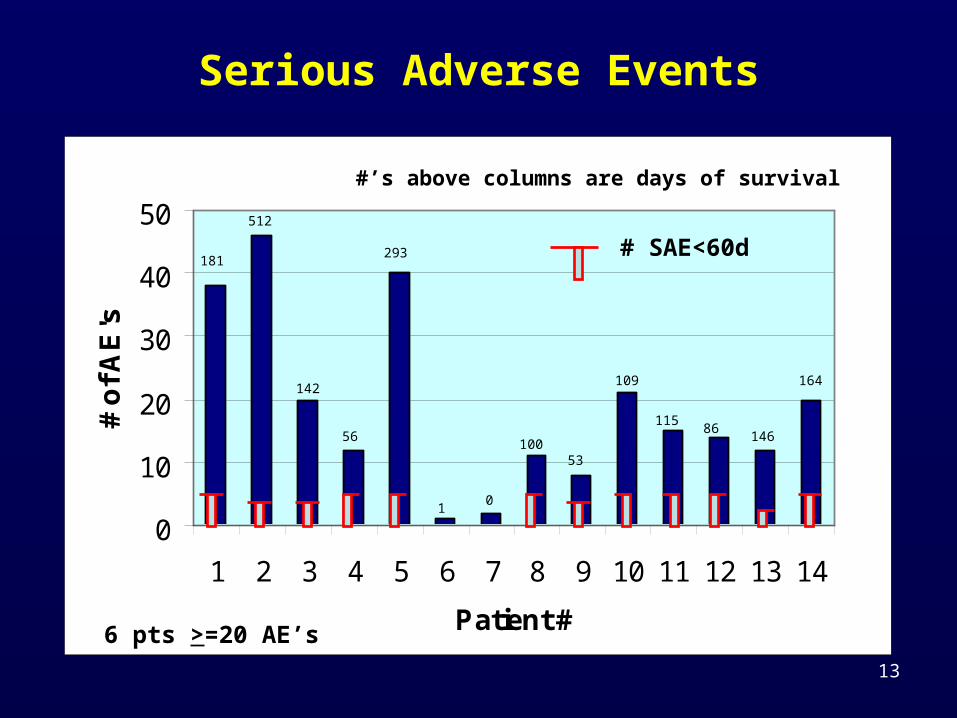
Serious Adverse Events
0
10
20
30
40
50
1 2 3 4 5 6 7 8 9 10 11 12 13 14
Patient #
# o
f AE
's
6 pts >=20 AE’s
# SAE<60d181
512
293
10
10053
109
11586
146
164142
56
#’s above columns are days of survival
14
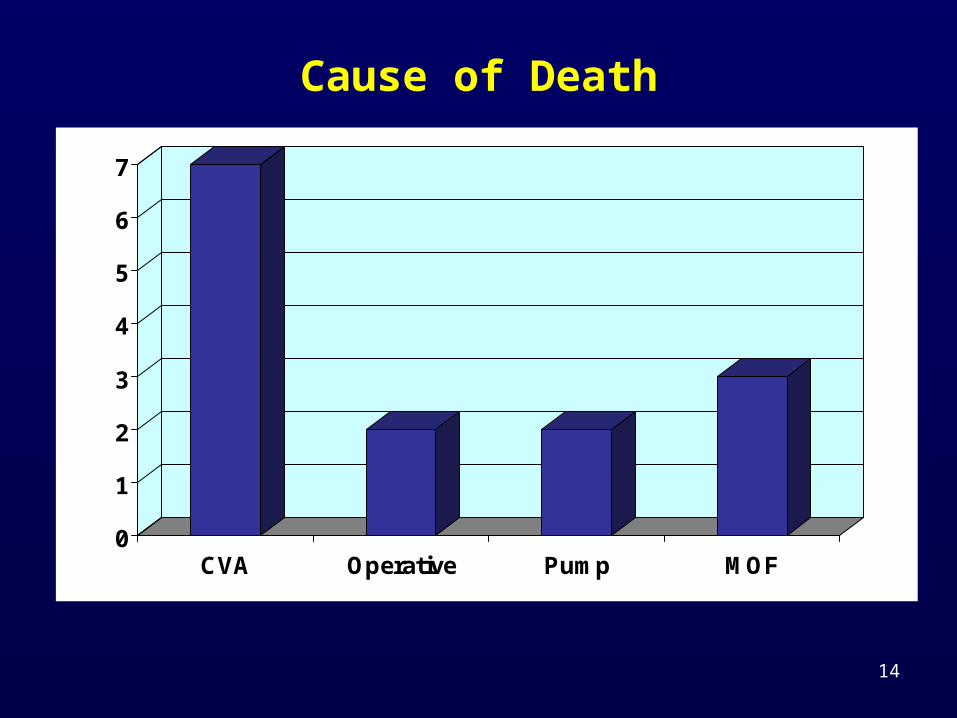
Cause of Death
0
1
2
3
4
5
6
7
CVA Operative Pump MOF
15
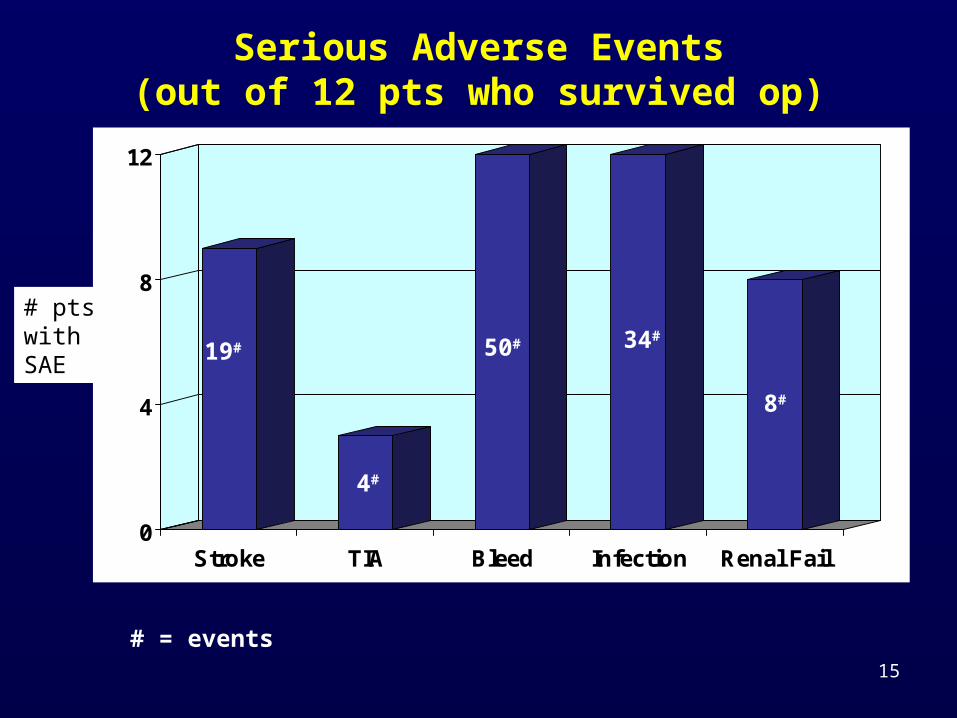
Serious Adverse Events(out of 12 pts who survived op)
0
4
8
12
Stroke TIA Bleed Infection Renal Fail
# ptswith SAE
19#
4#
50# 34#
8#
# = events
16
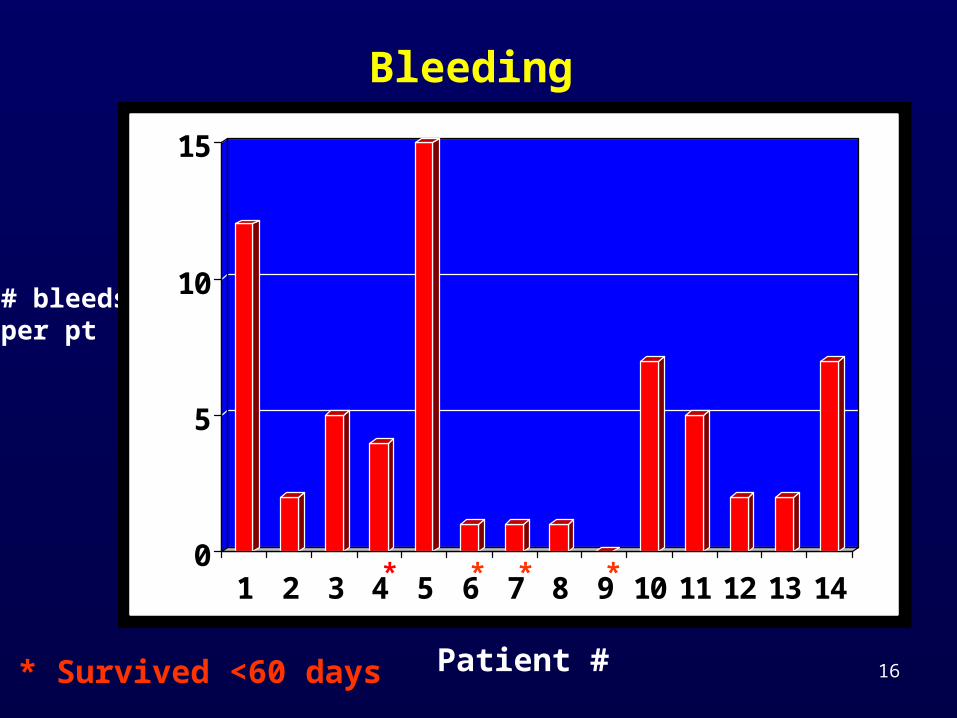
Bleeding
# bleedsper pt
Patient #* Survived <60 days
0
5
10
15
1 2 3 4 5 6 7 8 9 10 11 12 13 14* * **
17
Functional Measurements
• QOL– No validated measures– Occasional notes on walking or taking excursions
out of the hospital• No functional measurements (6 min walk or MVO2
postop)
• Difficult to understand functional level and to balance high mortality and SAE’s
18
Summary of Clinical Data
• Implanted in patients who, in the judgment of the investigator, appeared not to have any other options to prolong survival
• Provided physiological cardiac outputs and pressures
• Some had improvement and/or stabilization of end-organ function
• Some patients could sit, stand, walk, and take excursions outside of the hospital
19
Conclusion from Clinical Data
The risk/benefit determination for this device is difficult due to the lack of validated QOL and functional data
20
Post Market Study Inclusion (page 69, Post Approval Study)
The Sponsor claims patients with contraindications to LVAD placement would be included in the indications for the device:
• refractory arrhythmias• aortic regurgitation• prosthetic aortic valve• “Massive MI”: patients who are “…at risk of inlet cannula
dislodgement due to fragility of the infarcted ventricular tissue.”• Mural thrombus in the ventricles• Ventricular septal rupture• Transplant rejection
It should be noted that none of the 14 patients in the feasibility study had any of the above conditions
21
Post Market Study-Items for Discussion
• What should be measured?– Pre-implant status (demographics, hemodynamics,
reason not Tx candidate)– Survival– Major adverse events (bleeding, stroke, renal
failure, hepatic failure, infection)– Validated Function/QOL measurements– Rankin score
• For how long?– To death or device removal
• In how many patients?– 20 (no statistics possible)