Embed Size (px)
Citation preview

PROPERTIESAllow user to leave interaction: AnytimeShow ‘Next Slide’ Button: Show alwaysCompletion Button Label: View Presentation

Slide 2
Cardiogenic Shock, Acute Coronary Syndromes
and Heart Failure
Fredric Ginsberg, M.D.
Joseph Parrillo, M.D.

Slide 3
Cardiogenic Shock
• Inadequate tissue perfusion resulting from cardiac dysfunction
• Clinical definition: decreased cardiac output and tissue hypoxia in the presence of adequate intravascular volume
• Hemodynamic definition: Sustained systolic BP<90 mmHg, cardiac index <2.2 L/min/m2, PCWP > 15 mm Hg
Parrillo, J. 2005

Slide 4
Causes of Cardiogenic Shock
• Acute MI– Pump failure
– Mechanical complications
– Right ventricular infarction
• Other conditions– End-stage cardiomyopathy
– Myocarditis (Fulminant Myocarditis)
– Myocardial contusion
– Prolonged cardiopulmonary bypass
– Septic shock with myocardial depression
– Valvular disease
– Stress cardiomyopathy

Slide 5
CARDIOGENIC SHOCK
• Frequently, shock develops after presentation for myocardial infarction.
- SHOCK Registry • At presentation 25% in shock • Within 24 hours 75%
(median delay = 7 hours)
- GUSTO Trial • At presentation 11% in shock • After admission 89%
SHOCK Registry, Circulation 1995;91:873-81GUSTO J Amer Coll Cardiol 1995;26:668-74
Evolution of the Disease
Slide 6
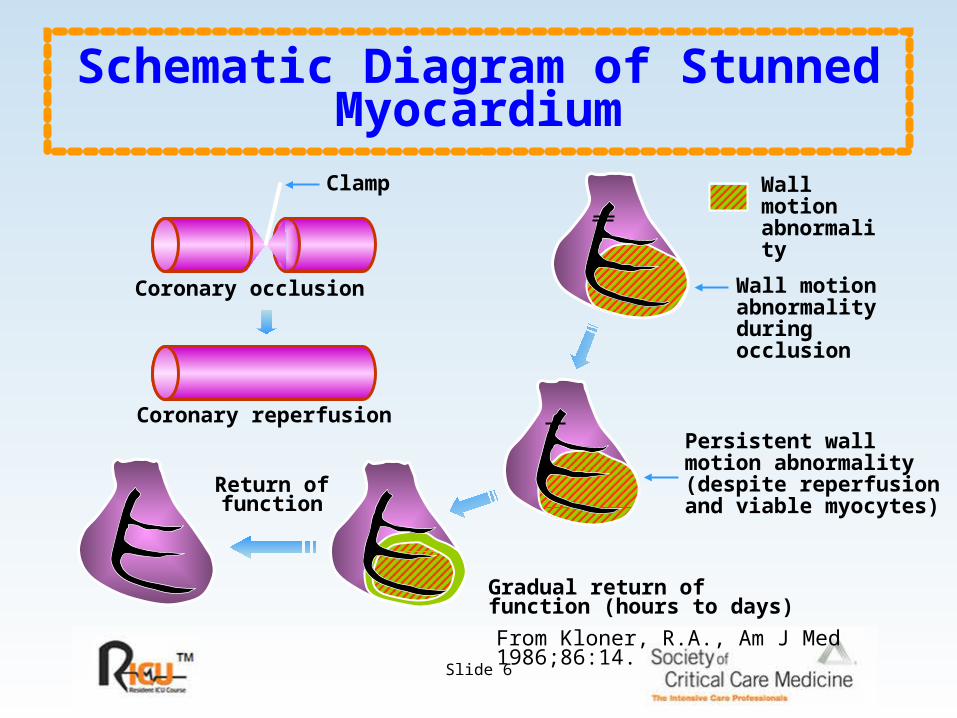
Schematic Diagram of Stunned Myocardium
Wall motion abnormalityduringocclusion
Wall motionabnormality
From Kloner, R.A., Am J Med 1986;86:14.
Gradual return offunction (hours to days)
Persistent wall motion abnormality(despite reperfusionand viable myocytes)
Coronary occlusion
Coronary reperfusion
Return offunction
Clamp

Slide 7
Hibernating Myocardium
Atherosclerotic narrowing
Wall motion abnormalitydue to chronic ischemiawithout infarction
Wall motion abnormality
From Kloner, R.A., Am J Med 1986;86:14.

Slide 8
Cell death Significant residual stenosis
Reperfusion
Segments withmyocardialstunning
Segments withboth stunningand hibernation
Segments withhibernatingmyocardium
Relief of ischemia
Inotropicsupport
No returnof function Return of
myocardial function
Ischemic Myocardium

Slide 9
Initial Approach: Management
• Assure Oxygenation
– Intubation and ventilation if needed
• Venous access
• Pain relief
• Continuous EKG monitoring
• Hemodynamic support
– Fluid challenge if no pulmonary edema
– Vasopressors for hypotension• Dopamine
• Norepinephrine

Slide 10
Intra-Aortic Balloon Counterpulsation
• Reduces afterload and augments diastolic perfusion pressure
• Beneficial effects occur without increase in oxygen demand
• No improvement in blood flow distal to critical coronary stenosis
• No improvement in survival when used alone
• May be essential support mechanism to allow for definitive therapy

Slide 11
Overall 30-Day Survival in the Study
Hochman, J.S., et al, N Engl J Med 1999;341:625-34.
Pro
po
rtio
n A
live
0Days after Randomization
0.6
0.2
0.0
0.8Revascularization (n=152)
Medical therapy (n=150)
1.0
0.4
5 10 15 20 25 30
Survival = 53%
Survival = 44%
p =0.11
Revascularization in Acute Myocardial Infarction
Early revacularization in Acute Myocardial Infarction complicated by cardiogenic shock

Slide 12
46.7 50.354.356
63.166.4
0
20
40
60
80
100
%
P = 0.11 P = 0.027 P < 0.03
30 days 6 months 1 year
RevascMed Rx
SHOCK Trial Mortality
Slide 13
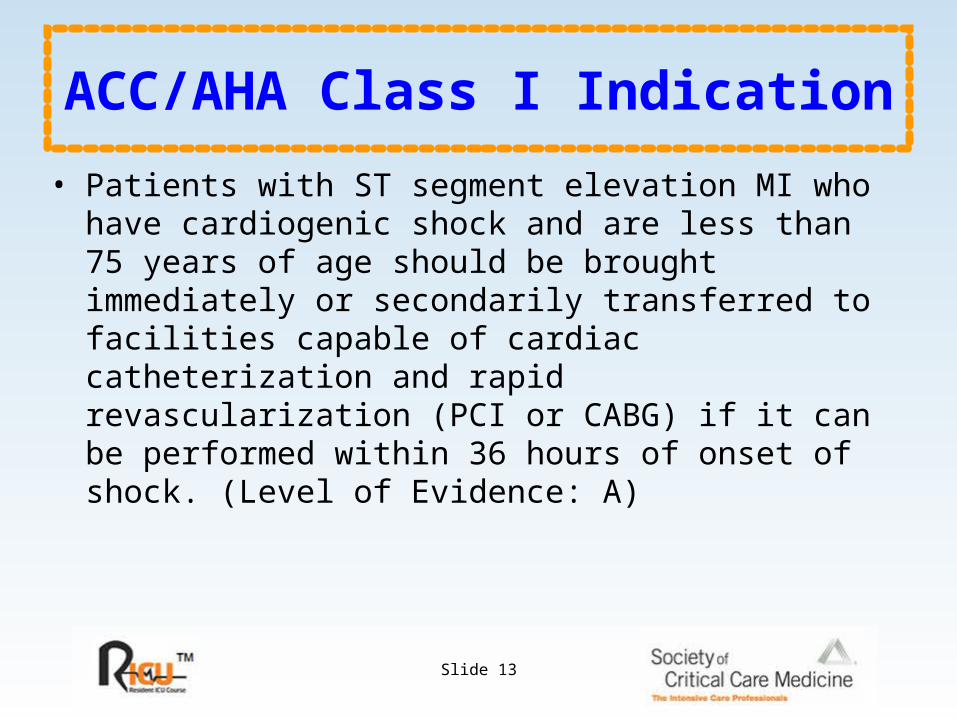
ACC/AHA Class I Indication
• Patients with ST segment elevation MI who have cardiogenic shock and are less than 75 years of age should be brought immediately or secondarily transferred to facilities capable of cardiac catheterization and rapid revascularization (PCI or CABG) if it can be performed within 36 hours of onset of shock. (Level of Evidence: A)

Slide 14
National Registry of MI
• National Registry of MI early Revascularization is Underutilized in Cardiogenic Shock
– Despite ACC/AHA recommendation to treat patients <75 years of age aggressively with early mechanical revascularization,
– In 2001, 2 years after the guidelines were published, only 41% of patients with cardiogenic shock complicating AMI were treated with primary PTCA and only 3.1% underwent early CABG.
– These data demonstrate significant underutilization of guideline recommended therapy.
Babaev A et al Circ 2002 106(19):1811 (abstract)

Slide 15
Pathophysiology of Cardiogenic Shock
• The following are observations from the SHOCK Trial and Registry that Challenge the Classic Paradigm
– LVEF is only moderately depressed (30%), with a wide range of EFs and LV sizes noted.
– Systemic vascular resistance (SVR) on vasopressors is not elevated (~ 1350), with a very wide range of SVRs measured.
– A clinically evident systemic inflammatory response syndrome is often present in patients with CS.
– Most survivors (85%) have NYHA functional Class I-II CHF status.
Hochman JS. Circ .2003;107:2998-3002.

Slide 16
Overproduction of Nitric Oxide
Thus, excess nitric oxide and peroxy nitrites may be a major contributor to cardiogenic shock complicating MI.
The Overproduction of Nitric Oxide May Cause Both Myocardial Depression and
Inappropriate Vasodilatation.
Cotter, Eur Heart J. 2003:24:1287-1295

Slide 17
Acute Coronary Syndromes: Definitions
Acute coronary syndrome:
Constellation of clinical symptoms compatible with acute myocardial ischemia
1. ST-segment elevation MI (STEMI)
2. Non-ST-segment elevation MI (NSTEMI)
3. Unstable angina
Unstable angina:
1.angina at rest (usually >20 minutes)
2.new-onset of class III or IV angina
3.increasing angina (from class I or II to III or IV)
Braunwald. Circulation 2002; 106:1893-2000.www.acc.org/clinical/guidelines/unstable/unstable.pdf

Slide 18
Hospitalizations in the US Due to Acute Coronary Syndromes
Acute Coronary Syndromes
~1.8 Million Hospital Admissions
UA/NSTEMI
1.42 Million
Admissions
Per Year
STEMI
0.41 Million
Admissions
Per Year
National Hospital discharge survey 1999. National Center for health Statistics/Centers for Disease Control and Prevention. Series 13, No. 14. September 20000.

Slide 19
Plaque rupture
Platelet adhesion
Platelet activation
Partially occlusive arterial thrombosis & unstable angina
Microembolization & non-ST-segment elevation MI
Totally occlusive arterial thrombosis & ST-segment elevation MI
Pathogenesis of Acute Coronary Syndromes
White HD. Am J Cardiol 1997;80 (4A):2B-10B.

Slide 20
Structure of ThrombusFollowing Plaque Disruption
UA/NSTEMI:Partially-occlusive thrombus
(primarily platelets)
Intra-plaque thrombus (platelet-dominated)
Plaque core
STEMI:Occlusive thrombus (platelets,
red blood cells, and fibrin)
Intra-plaque thrombus
(platelet-dominated)
Plaque core
SUDDEN DEATH
White HD. Am J Cardiol 1997;80 (4A):2B-10B.
UA = Unstable AnginaNSTEMI = Non-ST-segment Elevation Myocardial InfarctionSTEMI = ST-segment Elevation Myocardial Infarction

Slide 21
Diagnostic Algorithm
Braunwald E, et al. 2002. http://www.acc.org/clinical/guidelines/unstable/unstable.pdf.
Therapeutic goal: rapidly break apart fibrin mesh to quickly restore blood flow
ST-segment elevation MI Non-ST Elevation ACS* Non-ST Elevation MI
+ Troponinor + CK-MB
Consider fibrinolytic therapy, if indicated, or primary percutaneous coronary
intervention (PCI)
Therapeutic goal: prevent progression to complete occlusion of coronary artery and
resultant MI or death
Consider GP IIb-IIIa inhibitor + aspirin + heparin before early diagnostic catheterization
&/or

Slide 22
0.00
0.05
0.10
0.15
0.20
0.25
0 3 6 9 12
Pro
bab
ilit
yo
f D
eath
or
MI
Placebo
Aspirin 75 mg
Risk ratio 0.5295% CL 0.37 - 0.72
Wallentin LC, et al. J Am Coll Cardiol, 1991;18:1587-93.
Months
Risk of MI & Death During Treatment
The following graph displays the risk of MI and death during treatment with low-dose aspirin and iv heparin in men with unstable cad

Slide 23
Braunwald. Circulation. 2002;106:1893-2000. www.acc.org/clinical/guidelines/unstable/unstable.pdf
Low Molecular Weight Heparin (LMWH) vs. Unfractionated Heparin (UFH)
Trial:
FRIC(Dalteparin; n = 1,482)
FRAXIS(nadroparin; n = 2,357)
ESSENCE(enoxaparin; n = 3,171)
TIMI 11B(enoxaparin; n = 3,910)
.75 1.01.51.5
.75 1.01.51.5
(p= 0.032)
(p= 0.029)
LMWHBetter
UFHBetter
6
14
14
14
Day:
The following chart displays the low molecular weight heparin (LMWH) vs. unfractionated heparin (Ufh) in non-st elevation ACS: effect on death, MI, recurrent ischemia.

Slide 24
0
2
4
6
8
10
12
14
Dea
th,
MI,
or
Str
oke
Clopidogrel
+ ASA
3 6 9
Placebo + ASA
Months of Follow-Up
11.4%
9.3%
20% RRRP < 0.001
N = 12,562
0 12
%%
N Engl J Med. 2001;345:494-502.
Effects of ClopidogrelThis graph demonstrates the effects of Clopidogrel in addition to Aspirin in patients with ACS without ST-Segment Elevation

Slide 25
II IIaIIa IIbIIb IIIIII
Braunwald. Circulation 2002;106:1893-2000.www.acc.org/clinical/guidelines/unstable/unstable.pdf
Immediate aspirin
Clopidogrel,if ASA contraindicatedAspirin + Clopidogrel, for up to 1 month, if medical therapy or PCI is planned
Heparin (IV unfractionated, LMW) with antiplatelet agents listed above
Enoxaparin preferred over UFH unless CABG is planned within 24 hours
Hospital Care Anti-Thrombotic Therapy

Slide 26
II IIaIIa IIbIIb IIIIII
Braunwald. Circulation 2002;106:1893-2000.www.acc.org/clinical/guidelines/unstable/unstable.pdf
Any GP IIb/IIIa inhibitor + ASA/Heparin for all patients, if cath/PCI planned
Eptifibatide or tirofiban + ASA / Heparin for high risk * patients in whom early cath/PCI is not planned.
Any GP IIb/IIIa inhibitor for patients already on ASA + Heparin + clopidogrel, if cath/PCI is planned
Hospital Care Platelet GP IIb/IIIa Inhibitors (1)

Slide 27
II IIaIIa IIbIIb IIIIII
Braunwald. Circulation 2002;106:1893-2000.www.acc.org/clinical/guidelines/unstable/unstable.pdf
Eptifibatide or tirofiban + ASA / Heparin for patients without continuing ischemia in whom PCI is not planned.
Abciximab for patients in whom PCI is not planned.
Hospital Care Platelet GP IIb/IIIa Inhibitors (2)

Slide 28
II IIaIIa IIbIIb IIIIII
Braunwald. Circulation 2002;106:1893-2000.www.acc.org/clinical/guidelines/unstable/unstable.pdf
β -blocker (IV►oral) if not contraindicated
Non-dihydropyridine Ca2+ antagonist if β -blocker contraindicated and no LV dysfunction, for reccurrent ischemia
ACE inhibitor if ↑ BP persists with NTG+ β –blocker, for patients with CHF or diabetes.
Hospital Care Anti-ischemic Therapy (1)

Slide 29
II IIaIIa IIbIIb IIIIII
Braunwald. Circulation 2002;106:1893-2000.www.acc.org/clinical/guidelines/unstable/unstable.pdf
ACE inhibitor for all ACS pts
Extended-release CA2+ blocker instead of β-blocker
Immediate-release Ca2+ blocker with β-blocker
Long-acting Ca2+ blocker for recurrent ischemia, if no contraindications and NTG + β-blocker used fully
Hospital Care Anti-Ischemic Therapy (2)
C

Slide 30
ST-segment Depression Predicts Higher Risk of Mortality in
ACS
30 60 90 120 150 180
10%
8%
6%
4%
2%
T-wave inversion3.4%
ST-segment elevation6.8%
ST-segment depression8.9%
Days from randomization
% Cumulative Mortality at 6 Months
Savonitto S. J Am Med Assoc 1999; 281: 707-711.

Slide 31
Mortality Rates According to Level of Cardiac Troponin

Slide 32
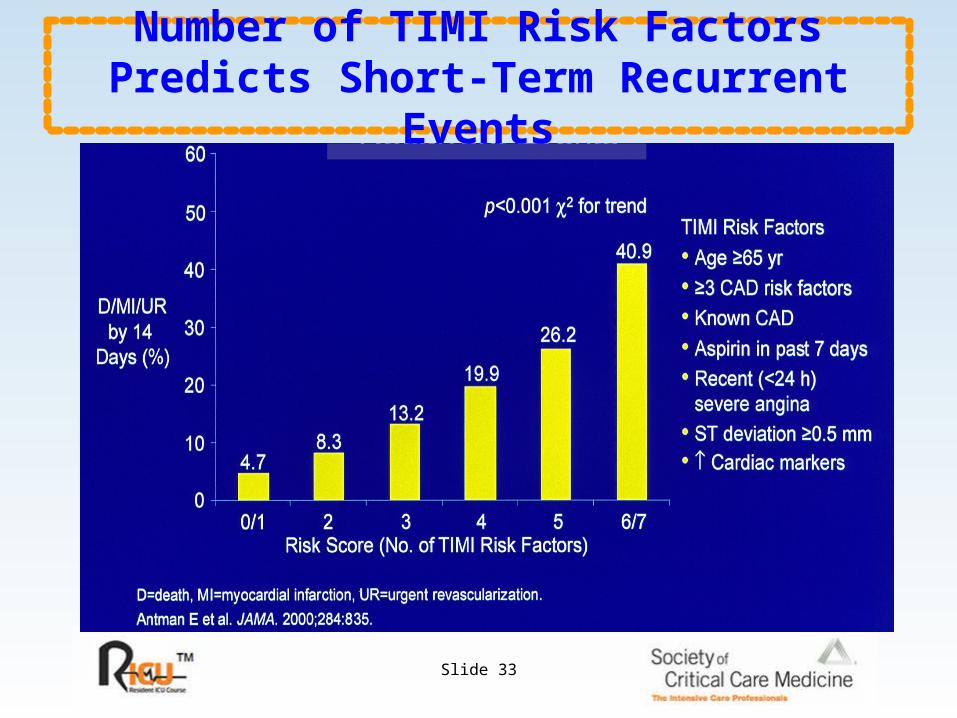
Variables Used in the TIMI Risk Score
• Age >65 years
• At least 3 risk factors for CAD
• Known prior coronary stenosis of >50%
• ST segment deviation on presenting ECG
• At least 2 anginal events in prior 24 hours
• Use of aspirin in prior 7 days
• Elevated serum cardiac biomarkers
Slide 33
Number of TIMI Risk Factors Predicts Short-Term Recurrent Events

Slide 34
De
ath
/MI/A
CS
Re
ho
sp (
%) CONS
TIMI UA Risk Score: Primary Endpoint at 6 mos
% of Pts: 25% 60% 15%
INV
OR=0.75CI (0.57, 1.00)
OR=0.55CI (0.33, 0.91)
11.8
20.3
12.816.1
19.5
30.6
0
5
10
15
20
25
30
35
Low 0-2 Intermed. 3-4 High 5-7
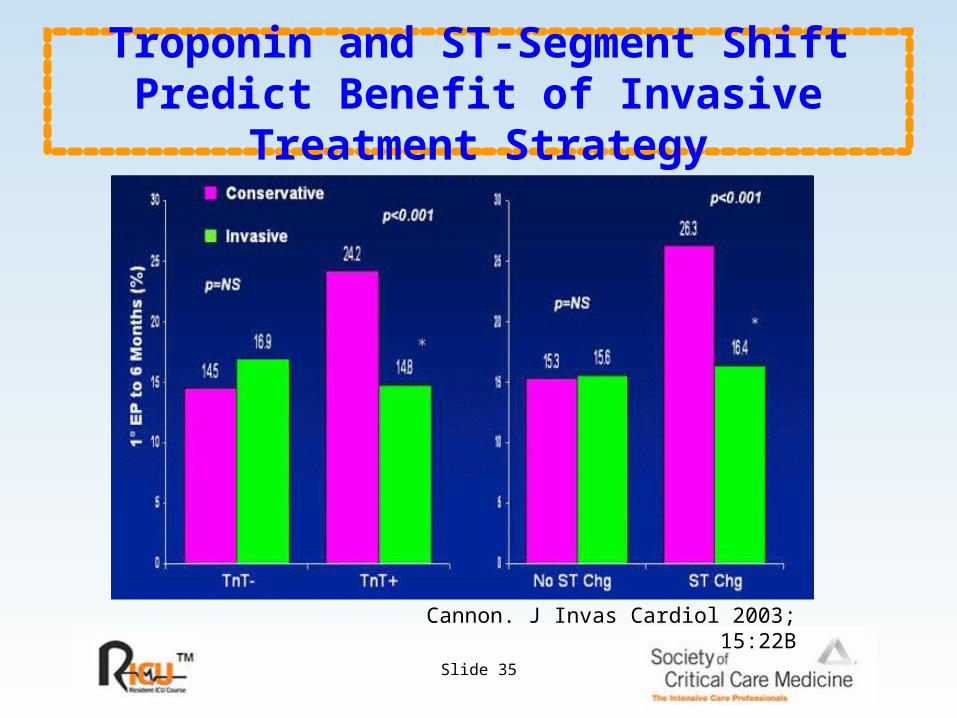
Slide 35
Troponin and ST-Segment Shift Predict Benefit of Invasive Treatment Strategy
Cannon. J Invas Cardiol 2003; 15:22B
Slide 36
Management of Patients with Unstable Angina
• ACC/AHA Guideline Update for the Management of Patients with Unstable Angina and Non-ST-Segment Elevation MI Class I
• An early invasive strategy in patients with a high-risk indicator:
– Recurrent angina/ischemia despite intensive anti-ischemic rx
– Elevated troponin-T or troponin-I
– New or presumably new ST-segment depression
– Recurrent angina/ischemia with CHF sx, S3, pulmonary edema, worsening rales, or new or worsening MR
– High-risk findings on noninvasive stress testing
– Depressed LV systolic function (EF <40%)
– Hemodynamic instability
– Sustained ventricular tachycardia
– PCI within 6 months
– Prior CABG
• Either early invasive or early conservative strategy if not high risk
Braunwald, Circulation. 2002:106:1893-2000. www.acc.org/clinical/guidelines/unstable/unstable.pd

Slide 37
Start immediate Aspirin Heparin or low-molecular-weight heparin GP IIb-IIIa inhibitor
Adapted from Braunwald E, et al. 2002. http://www.acc.org/clinical/guidelines/unstable/unstable.pdf.
At presentationST-segment depression &/or elevated cardiac troponin
Need to immediately arrest thrombus progression
Need to eliminate occlusive ruptured plaque
Send for catheterization & revascularization within 24-48 hours
Cautionary information No clopidogrel within 5-7 days prior to CABG surgery No enoxaparin within 24 hours prior to CABG surgery No abciximab, if PCI is not planned
2002 ACC/AHA Guidelines for theManagement of High-risk NSTE ACS

Slide 38
Ongoing Evaluation in an Early Conservative Strategy
Braunwald E, et al. 2002. http://www.acc.org/clinical/guidelines/unstable/unstable.pdf.
Recurrent Symptoms/ischemia
Heart failureSerious arrhythmia
Patient stabilizes
EF .40Stress Test
Not low risk
Follow on Medical Rx
Evaluate LV function
EF < .40
Low risk
Immediate angiography
Early medical management

Slide 39
Guideline Update
• ACC/AHA Guideline Update for the Management of Patients with Unstable Angina and on-ST-Segment Elevation MI - Class I indications for revascularization with PCI or CABG
• CABG for > 50% stenosis of the left main coronary artery
• CABG for 3 vessel CAD
• CABG for 2 vessel CAD including proximal LAD stensoes & EF < 50%
• PCI or CABG for 1 or 2 vessel CAD, no proximal LAD large area of viability, high-risk noninvasive test
• PCI for patients with multivessel CAD, normal EF, no diabetes
• IV platelet GP IIb/IIIa inhibitior in ACS patients undergoing PCIBraunwald, Circulation. 2002:106:1893-2000. www.acc.org/clinical/guidelines/unstable/unstable.pd

Slide 40
Guideline Update
• ACC/AHA Guideline Update for the Management of Patients with Unstable Angina and Non-ST-Segment Elevation MI Class IIa indications for revascularization with PCI or CABG
• Repeat CABG for patients with multiple saphenous vein graft stenoses especially if LAD graft
• PCI for focal saphenous vein graft lesions or multiple lesions if poor surgical candidate
• PCI or CABG for patients with 1 or 2 vessel CAD, not proximal LAD, but moderate area of viability and ischemia
• PCI or CABG for patients with 1 vessel CAD with proximal LAD
• CABG with Internal Mammary artery for patients with multivessel CAD and diabetes Braunwald, Circulation. 2002:106:1893-2000.
www.acc.org/clinical/guidelines/unstable/unstable.pd
Slide 41
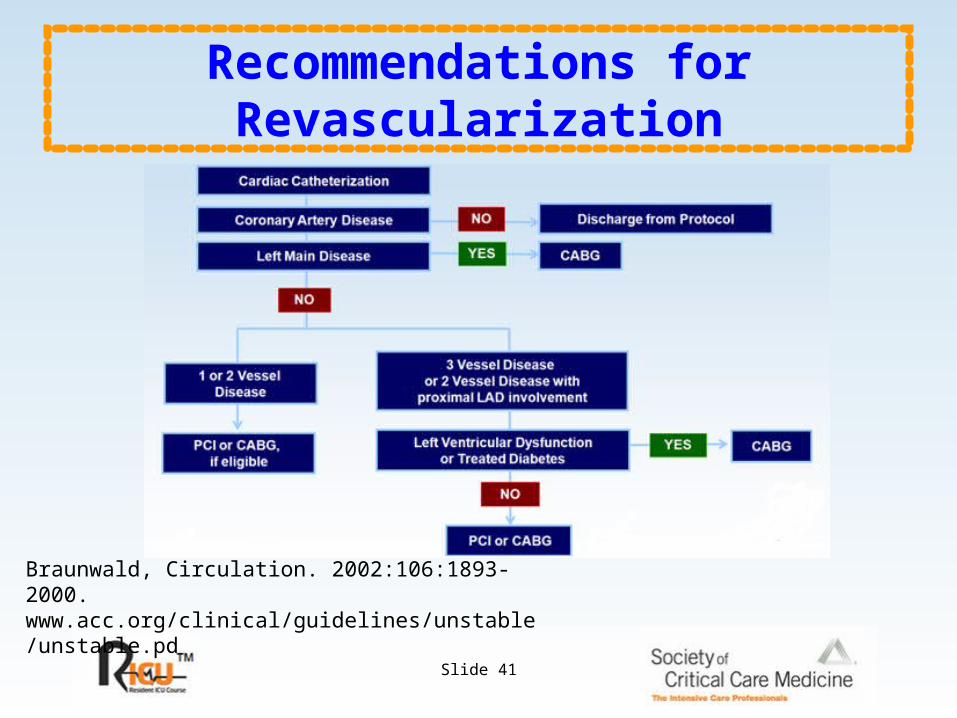
Recommendations for Revascularization
Braunwald, Circulation. 2002:106:1893-2000. www.acc.org/clinical/guidelines/unstable/unstable.pd

Slide 42
UA/NSTEMIUA/NSTEMI
High Risk High Risk **
ASA, Heparin/ASA, Heparin/Enox.Enox., , block., Nitrates, Clopidogrelblock., Nitrates, Clopidogrel
RISK STRATIFY
Low RiskLow Risk
Braunwald E, et al. Circ. 2002;106:1893.
* Recurrent ischemia; Trop; ST; LV failure/dysf.; hemodynamic instability; VT; prior CABG
Enoxeparin. Preferred to UFH (IIa)
If coronary arteriography >24 hours
ACC/AHA REVISED GUIDELINES

Slide 43
Braunwald E, et al.Circ. 2002;106:1893.
LMCD, 3VD+LV Dys., LMCD, 3VD+LV Dys., or Diab. Mell.or Diab. Mell.
CABGCABG
High RiskHigh Risk
Cor. ArteriographyCor. Arteriography
1 or 2VD, Suitable 1 or 2VD, Suitable for PCIfor PCI NormalNormal
Clopidogrel, Clopidogrel, IIb/IIIa inhib.IIb/IIIa inhib.
Consider Alternative Consider Alternative DiagnosisDiagnosis
Discharge on ASA, Clopidogrel, Statin, ACEIDischarge on ASA, Clopidogrel, Statin, ACEI
PCIPCI
ACC/AHA REVISED GUIDELINES
Braunwald E, et al. Circ. 2002;106:1893.

Slide 44
II IIaIIa IIbIIb IIIIII
Braunwald. Circulation 2002;106:1893-2000.www.acc.org/clinical/guidelines/unstable/unstable.pdf
ASA, if not contraindicated
Clopidogrel, when ASA contraindicated
Aspirin + Clopidogrel, for up to 9 months
-blocker, if not contraindicated
Lipid agents (statins) + diet
ACE Inhibitor: CHF, EF < 40%, DM, or HTN
Discharge Medications
Braunwald, Circulation. 2002:106:1893-2000. www.acc.org/clinical/guidelines/unstable/unstable.pd

Slide 45
Death or Major Cardiovascular Events
Cannon CP, et al. N Engl J Med. 2004:350:1495-1504.
This graph displays the all-cause death or major cardiovascular events in all randomized subjects

Slide 46
Reductions in Major Cardiac End Points
Cannon CP, et al N Engl J Med. 2004:350:1495-1504

Slide 47
Risk Factor Modification
Braunwald, Circulation. 2002:106:1893-2000. www.acc.org/clinical/guidelines/unstable/unstable.pd

Slide 48
Heart Failure due to LV Systolic Dysfunction
• Approximately 5 million Americans have Heart Failure (male to female ratio 1:1)
• 550,000 new cases annually
• Hospital discharges 1,000,000 annually
• 80% of men and 70% of women under the age of 65 with HF will die within 8 years
Numbers based on 2000 data.American Heart Association. 2003 Heart and Stroke Statistical Update. Dallas,
Tex: AHA; 2002.

Slide 49
RAS, renin-angiotensin system; SNS, sympathetic nervous system.
Myocardial injury to the heart (CAD, HTN, CMP, Valvular disease)
Morbidity and mortalityArrhythmiasPump failure
Peripheral vasoconstrictionHemodynamic alterations
Heart failure symptoms
Remodeling and progressiveworsening of LV function
Initial fall in LV performance, wall stress
Activation of RAS and SNS
Fibrosis, apoptosis,hypertrophy, cellular/molecular alterations,
myotoxicity
FatigueActivity altered Chest congestionEdemaShortness of breath
Neurohormonal Activation in Heart Failure

Slide 50
LV Remodeling After Anteroseptal MI
1 week 3 months
EDV 137 mL ESV 80 mLEF 41%
EDV 189 mL ESV 146 mLEF 23%
Apical 4 Chamber View

Slide 51
Drugs for Heart Failure
• ACE-inhibitors
• Beta-blockers
• Angiotensin receptor blockers
• Aldosterone antagonists
• Loop diuretics
• Nitrates with hydralazine
• Digoxin
• Nesiritide, inotropic agents

Slide 52
ACE-Inhibition and CHF Trials
• SAVE--captopril, 1992. Post-MI (not CHF) with EF<40%, f/u 42 mos, 2231 pts. Mortality reduced from 25% to 20% NEJM 1992;327:669
• SOLVD--enalapril, 1991. CHF pts, class II-III, EF<35%,f/u 41 mos, 2569pts. Mortality reduced from 39% to 35% NEJM 1991;325:293
• SOLVD--enalapril, 1992. Asymptomatic LV dysfunction, EF<35%, f/u 37 mos, 4228 pts Non-significant reduction in mortality, significant reduction in CHF and hospitalization NEJM 1992;327:685

Slide 53
ACE-I and CHF: Meta-analysis
• Captopril, enalapril, ramipril, quinapril, lisinopril
• 32 trials, 7105 patients, FC II-III
• 2 mortality trials
• Combined: total mortality reduced 21.9% to 15.8% and total mortality plus CHF hosp reduced 32.6% to 22.4%
• Summary:
– 1. Improvement in risk of death or MI or CHF hospitalization
– 2. Class effect
• JAMA. 1995. 273:1450

Slide 54
Beta Blockade-Rationale
• Catecholamine levels are increased in CHF
• Higher levels correlate with more severe disease
• Catecholamines contribute to myocyte hypertrophy and necrosis (apoptosis)
• More ischemia, arrhythmia, vasoconstriction and LV dilatation

Slide 55
Metoprolol
• MERIT-HF: Metoprolol tartrate
• Preceded by 2 previous trials in CHF (MDC, RESOLVD)
• 3,991 patients, mean f/u 12months, class II-III
• Mean EF 28%
• Results: stopped early as total mortality + all cause hospitalization was reduced 38% to 32% (p=.00012) and total mortality reduced 10.8% to 7.2 % (p<.0001)
• JAMA.2000;283:1295

Slide 56
CAPRICORN
YearsThe CAPRICORN Investigators. Lancet. 2001;357:1385–1390.
0 0.5 1 1.5 2 2.5
Carvedilol n=975
Placebo n=984
Pro
po
rtio
n E
ven
t-fr
ee
23%P=.031
Risk reduction
Mortality rates: Placebo 15%; Carvedilol 12%
0
1.00
0.90
0.70
0.60
0.80
Carvedilol in post-MI patients with Reduced EF: All-Cause Mortality
Slide 57
COPERNICUS
• Carvedilol in Class III-IV Heart Failure
• Inclusion: EF<25%, class III-IV,euvolemic
• 2,289 patients, mean f/u 10.4 months, stopped early
• Mortality 18.5% (placebo) vs. 11.4% with carvedilol 35% reduction (p<.00013)
• No difference in withdrawal rates
• Mortality curves diverge within 3 weeks; thus, beneficial effects are not delayed and can occur at low dose
NEJM 2001; 344:1651

Slide 58
COPERNICUS All-cause Mortality
Packer M et al. N Engl J Med. 2001;344:1651–1658.Coreg (carvedilol) Prescribing Information. GlaxoSmithKline, Research Triangle Park, NC. Mar 2003.
P=.0014
% S
urv
ival
Carvedilol
Placebo
0 3 6 9 12 15 18 21
Months
100
90
80
60
70
0
Risk reduction
35%
n=115
n=113
Mortality rates: Placebo 19.7%; Carvedilol 12.8%

Slide 59
COMET
• First head-to-head mortality study comparing two beta-blocking agents in CHF--carvedilol vs. short-acting metoprolol titrate
• 3,029 patients, class II-III, EF<35%, 80% male, 99% Caucasian
• Carvedilol compared to metoprolol reduced annual mortality from 10.0% to 8.3% and prolonged median survival by 1.4 years
• Lancet 2003;362:7

Slide 60
Beta Blockers for CHF: Summary
• Ischemic or non-ischemic CMP
• All symptomatic CHF patients
• Class II - IV
• Hemodynamically stable and euvolemic
• Even in “compensated” patients as there is a high likelihood of symptoms progression in 12 months
• Beneficial effects are in addition to effects of other therapies

Slide 61
Angiotensin Receptor Blockers in CHF
Trial Drugs Baseline EFMortality vs.
ACE-I Notes
RESOLVD 1999candesartan vs.
enalaprilAvg 27% 6.1 vs 3.7 (p=NS)
ELITE II 2000 losartan vs. captopril <40% 17.7 vs. 15.9 (p= NS)
ValHeft 2001 valsartan <40% 19.9 vs. 19.4 (p= NS)33% increased
mortal if not on ACE-I
CHARM 2003 candesartanSmall decrease in
mortality when added to ACE-I
No increased mortality w/ beta-
blocker

Slide 62
Angiotensin Receptor Blockers in CHF
• ARBs should be used in patients intolerant of ACE inhibitors
• ARBs can be added on in patients receiving ACE-inhibitors and beta blockers with a small added benefit
• Increased risk of hypotension, hyperkalemia and renal insufficiency when added on to ACE-I and beta-blocker therapy

Slide 63
Aldosterone Blockers in CHF
Study Drug Patients Added therapy Mortality vs. placeboHyper-
kalemia
RALES 1999 spironolactoneClass III and IV
CHFACE-I, no beta-
blockerReduced from 46.3%
to 35% (p<.001)2%
EPHESUS 2003 eplerenonePost-MI w/ EF<40% or
diabetes
ACE-I and beta-blocker
Reduced from 14.6% to 8.5% (p=.008)
5.5%

Slide 64
Aldosterone Blockers
• Aldosterone blockers should be used in patients with chronic heart failure with low EF (spironolactone) and in patients post-MI with heart failure with EF<40% or diabetes mellitus (eplerenone)
• Contraindications: renal insufficiency (creat >2.5 mg%) or hyperkalemia (over 5.0)
• Patients on aldosterone blockers must have renal function and electrolytes carefully and frequently monitored

Slide 65
Digoxin and CHF: “Dig Trial”
• 1997, CHF with EF<45%, NSR, class II-III
• 6,800 patients, 94% ACE-I, little beta-blocker, f/u 37 months
• Total and CV mortality: No significant differences
• Decreased need for hospitalization for CHF, 2% hospitalized for dig toxicity
• Summary: Use digoxin for symptomatic benefit, not mortality benefit
• NEJM.1997;336:525

Slide 66
Vasodilators and CHF
• V-HeFT I: 1986: preceded use of ACE-I and beta blockers for CHF
• Placebo vs. prazosin vs. combined isosorbide dinitrate (avg 136 mg) with hydralazine (avg 270 mg)
• 642 pts, EF<45%
• All cause mortality improvement only with ISDN+Hydralazine (p=.04)
• Recommend: Use for patients unable to take ACE-I or ARB
• NEJM.1986;314:1547

Slide 67
Vasodilator Therapy: A-Heft
• Therapy with ISDN and hydralazine added on to standard CHF therapy.
• 1050 black patients; class III-IV heart failure, EF<45%
• 76% on ACE-I/ARB, 74% on beta-blocker
• Mortality reduced from 10.2% to 6.2% at 10 month follow-up (p=0.02)
• NEJM 2004; 351:2049

Slide 68
NESIRITIDE (BNP)
• Inpatient intravenous infusion
• Arterial and venodilator
• Natriuresis and diuresis
• No tolerance or proarrhythmia
• Associated with hypotension
• Rapid fall in PCWP
• No adverse effect on mortality

Slide 69
Intravenous Inotropic Agents
• ACC/AHA Guidelines (Circ. 2001; 104:2996.)
• 1. For symptomatic systolic dysfunction (Stage C):
• Class III (i.e. NOT indicated): Long term intermittent use of an infusion of a positive inotropic drug (level of evidence C)
• 2. For refractory end-stage CHF (Stage D):
• Class IIb: Continuous intravenous infusion of a positive inotropic agent for palliation of symptoms (level of evidence C)
• Class III (NOT indicated): Routine intermittent infusions (level of evidence B)

Slide 70
Search for Aggravating Medical Conditions
• Ischemia, arrhythmias, conduction abnormalities
• Worsening valve regurgitation
• Hypertension, bilateral renal artery stenosis
• Anemia, thyroid disease, infection, renal failure, obstructive sleep apnea, medication noncompliance
Slide 71
Patients Refractory to Pharmacologic Therapy
• Resynchronization therapy to improve heart failure (biventricular pacemaker)
• Revascularization if documented ischemia
• ICD implant to reduce risk of sudden arrhythmic death
• Surgery: CABG, valve repair, transplant
Slide 72
Case Studies
•The following are case studies that can be used for review of this presentation.
Review Cases
End

Slide 73
Case #1
• A 49-year-old female presented to the emergency department of a community hospital with a 5-day history of chest pain. The pain was retrosternal, radiated to both arms, and was brought on by mild exertion. Chest pains increased in frequency over the 5 days.

Slide 74
Case #1
• Past medical history: No cardiovascular illness
• Cardiac Risk Factors:– chronic cigarette smoker
– Multiple family members with MI at age 50-60
• Physical exam: BP 120/80, HR 80 per min, Lungs clear, normal cardiac exam
• ECG: normal sinus rhythm, normal
• Laboratory: – total cholesterol 177mg%
– triglycerides 247 mg%
– HDL 27mg%
– LDL 101mg% FBS 109mg%
– TROPONIN=0.52 (nl< .05)

Slide 75
Case #1
• Hospital course:
• Patient was treated with aspirin, low molecular weight heparin (enoxaparin) and nitroglycerin topically
• On day 2, patient was transferred to a tertiary hospital for cardiac catheterization
• Coronary angiography showed significant single vessel coronary artery disease with a 95% stenosis of the mid-right coronary artery. There was also a 30% stenosis of the LAD and a 40% stenosis of the mid circumflex coronary artery.
• Patient underwent successful and uncomplicated stenting of the RCA.

Slide 76
Case #1
• Discharge medications:
– aspirin 325 mg daily
– clopidogrel 75 mg daily
– atorvastatin 80 mg daily
– metoprolol 50 mg bid
– lisinopril 10 mg daily
• Patient counseled regarding cessation of cigarette smoking

Slide 77
Case #2
• A 58-year-old female presents to the emergency department with severe dyspnea, awakening her from sleep.
• HPI: two-month history of gradually worsening exertional dyspnea without chest pain
• PMH: Hypertension, hyperlipidemia; non-smoker, no alcohol use
• Medication on admission: amlodipine 5 mg daily

Slide 78
Case #2
• Physical exam: marked respiratory distress HR 110 per min, BP 160/105, Chest: rales in all fields, Heart: regular tachycardia, S3 gallop, no murmur, Extremities: no edema
• ECG: sinus tachycardia, voltage criteria for LVH, ST segment depression laterally.
• CXR: cardiomegaly, pulmonary edema
• Laboratory: Normal CBC. Normal electrolytes, renal function and liver enzymes

Slide 79
Case #2
• Hospital course: Initially treated with intravenous furosemide and intravenous nitroglycerin with resolution of signs and symptoms of pulmonary edema and lowering of BP to 110/80 in 24 hours.
• Echocardiogram: Markedly dilated LV with severe global hypokinesis and calculated LV ejection fraction of 20%. Normal appearance of mitral and aortic valves. Mild mitral regurgitation.
• Coronary angiography: No significant coronary artery stenoses.

Slide 80
Case #2
• Diagnosis: Congestive heart failure due to idiopathic dilated cardiomyopathy in the setting of chronic hypertension.
• Patient discharged feeling well on the following medications:
– lisinopril 10 mg daily
– carvedilol 12.5 mg bid
– spironolactone 25 mg daily
– digoxin 0.125 mg daily

Slide 81
Case #3
• 60-year-old male presents to the emergency room of a community hospital with a two-hour history of severe chest pain associated with severe diaphoresis, dizziness and presyncope
• PMH: type 2 diabetes mellitus, no previous cardiac illness

Slide 82
Case #3
• Examination: HR 80 per min BP 78/54
– Pale, diaphoretic, Lungs clear
– Heart: No murmur or S3 gallop
• ECG: NSR, marked ST segment elevation in leads II, III and aVF
• CXR: Normal heart size, clear lung fields
Slide 83
Case #3
• Course: Patient was emergently transferred to a tertiary hospital for cardiac catheterization
• Hemodynamics: RA=22 mmHg PA=32/22 PCWP mean=23 mmHg
• Coronary Angiography: total occlusion of proximal right coronary artery. Treated with successful and uncomplicated angioplasty and stenting. Intra-aortic balloon pump placed.

Slide 84
Case #3
• Diagnosis: Acute inferior wall myocardial infarction complicated by cardiogenic shock due to right ventricular infarction
• Hospital course: Patient’s BP improved to 110/78 post-procedure, with resolution of chest pain. Hospital course was uncomplicated. IABP removed on day #2, patient discharged on hospital day #5.

Slide 85
Selected References
• Hochman JS, Sleeper LA, Webb JG, et al. Early Revascularization in Acute Myocardial Infarction Complicated by Cardiogenic Shock.. N Eng J Med. 1999;341:625-634
• Anderson JL, Adams CD, Antman EM, Bridges CM, et al. ACC/AHA 2007 Guidelines for the Management of Patients with Unstable Angina/ Non-ST Elevation Myocardial Infarction-2002: Executive Summary. A Report of the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Unstable Angina/Non-ST-Elevation Myocardial Infarction). J Am Coll Cardiol 2007; 50: 652-726.

Slide 86
Selected References
• Adams KF, Lindenfeld J, Arnold JMO, et al. Executive Summary: HFSA 2006 Comprehensive Heart Failure Practice Guidelines. J Cardiac Failure. 2006;12:10-38.
• Packer M, Coats AJ, Fowler MB, et al, Carvedilol Prospective Randomized Cumulative Survival Study Group. Effect of Carvedilol on Survival in Severe Chronic Heart Failure. N Eng J Med. 2001;344:1651-1658.