Embed Size (px)
Citation preview

Annals of Clinical and Laboratory ResearchISSN 2386-5180
2016Vol. 4 No. 1: 71
1© Copyright iMedPub | www.aclr.com.es
iMedPub Journalshttp://www.imedpub.com
Research Article
Rosemarie Fröber1, Karl-Heinz Eichhorn2, Ekkehard Schleußner3 and Dietmar Schlembach4
1 InstituteofAnatomyI,JenaUniversityHospital,07740Jena,Germany
2 CenterforPrenatalDiagnosis,Gerhart-Hauptmann-Strasse6,99423Weimar,Germany
3 DepartmentofObstetrics,JenaUniversityHospital,Bachstrasse18,07743Jena,Germany
4 DepartmentofObstetrics,Vivantes-Clinics,RudowerStraße48,12351Berlin,Germany
Corresponding author: Dr.RosemarieFröber
ClinicalAnatomyIandTeratology,InstituteofAnatomy,JenaUniversityHospital, Teichgraben7,07740Jena,Germany.
Tel: 0049-3641-938520Fax:0049-3641-938634
Citation:FröberR,EichhornKH,SchleußnerE,etal. HeterotaxySyndrome:AnEmbryologicStudy.AnnClinLabRes.2016,4:1.
IntroductionHeterotaxyisararemalformationsyndromewithanincidenceof1-1.5/10,000livebirthsandahighmortalityrate[1-3].Itisdefinedasanabnormalarrangementofvisceraacrosstheleft/rightaxisprimarilyinducedbydisordersoflateralitydeterminationduringearlyembryonicdevelopment.Thepresenceofbilateralright-orleft-sided “situs ambiguous” should be differentiated from theusual “situs solitus” and themirror image “situs inversus”. Theclassicterm“bilateralsidedness”impliesthepresenceofbilateralequivalent lungs and bronchi as well as bilateral symmetricatria. Inthiscontext thearrangementof thebronchopulmonartract and the atrial appendages is of particular importance forcorrectclassification.Heterotaxycanbeclassified intobilateralright-sided -“right isomerism”-and left-sided -“left isomerism”-[4].Typicalprenatalfindingsinbothvarietiesareviscerocardiac
Heterotaxy Syndrome: An Embryologic Study
Received: February25,2016; Accepted: March09,2016; Published: March14,2016
AbstractHeterotaxy isaclinicallyandgeneticallyheterogeneousdisorderwithtwomainsettings-leftorrightisomerism.Importantdiagnosticpointerslikeviscerocardiacheterotaxy,complexcardiacmalformations,anomaliesoftheinferiorvenacava,orbradyarrhythmiamayprovidetheprenataldiagnosis.
Specialsignsofheterotaxyweresonographicallydetectedin5humanfoetuses.Followingtheterminationofthepregnancyadetailedexaminationaccordingtotheguidelinesof thesequential segmentalapproachwasperformed.Themainfindingsincludemultiplefailuresintheformationoftheheartresultingfromthedysfunctional viscerocardiacarrangement.Thediscontinuityandmalpositionofthe inferior vena cava aswell as theduplicationof the superior vena cava arebasedondisordersof the left-rightdeterminationof thepairedprimitiveveinsinearlyembryonicdevelopment.Themalrotationandmalfixationof thebowelseemtobeinducedbytheabnormalprocessoftheembryonicduodenalloopwithsubsequentmalpositioningoftheportalveinandthesuperiormesentericvessels.
We demonstrate the wide variety of cardiac and extracardiac congenitalmalformations with considerable overlap in left and right isomerism. As aconsequence, the differentiation between left or right isomerism may besometimes difficult. Highly skilled sonographers and radiologists should befamiliarwith the corresponding embryonic development,which is essential forunderstanding thecomplexmalformationpattern.Completeevaluationofeachindividual case is mandatory for adequate parental counselling with regard tofurtherdiagnosticstepsandtheplanningofperinatalmanagement.
Keywords: Left/right isomerism, Heterotaxy, Situs ambiguous, Congenitalmalformation,Humanfoetus,Foetalautopsy,Embryology
heterotaxy,complexcardiacmalformationsandanomaliesofthecavalveins[5].Inmostcases,however,awidevarietyofcardiacandextracardiaccongenitalmalformations,withaconsiderableoverlapoftheanatomicalfeatures,canoccur.Asaconsequence,the prenatal differentiation between the two main settings issometimesunclear.Adetailedknowledgeofthemorphogenesisincasesofheterotaxyisessentialforunderstandingthecommonvarietiesofdifferentorgansystemsinviewofanexactprenataldiagnosis. This ismandatory for adequate parental counsellingregardingfurtherdiagnosticstepsandtheplanningofperinatalmanagement[6].
Material and MethodsSpecific signs of heterotaxy were prenatally detected in 5

2016Annals of Clinical and Laboratory Research
ISSN 2386-5180 Vol. 4 No. 1: 71
2 This Article is Available in: www.aclr.com.es
human foetuses.The4 foetuseswith suspected left isomerismwere female, and the foetus with right isomerism was male.Following the termination of the pregnancy in the secondtrimester(14weeks/4days,16weeks/0days,17weeks/3days;20weeks/2days;22weeks/6days)adetailedanatomicalsurveyin accordancewith the guidelines of the sequential segmentalapproachwasperformed[7].Wereportthecompletespectrumofautopticfindingswith respect totheunderlyingdisorders intheearlyembryonicdevelopment.
ResultsOfthe5foetuseswithprenatallysuspected leftisomerism,thediagnosiswas confirmedbypostmortem in4 cases, in1 case,however,rightisomerismwasdetected.
Table 1displaysthesonographicfindingsofthe4foetuseswithleft isomerism. Structuralheartdisease, in combinationwith acompleteatrioventricularseptal defect,wasprenatallyobservedin 3 and with an isolated ventricular septal defect in 1 of thecases.Persistentbradyarrhythmiaanddysfunctionatthelevelofventriculoarterialconnections–forexampletetralogyofFallot,commonarterialtrunkandaorticstenosis-weresuspectedin3andcommonatriumin2casesbutdextrocardiain1case.Typical
extracardiacprenatalfindingswererightsidedabdominalviscerain3cases.
A summary of the autoptic findings is given in Table 2. Thestructuralheartdiseasecouldbeconfirmedbypostmortem inall4casesofleft isomerism.Asseeninthetable,themajorityofallsegmentsofthefoetalheartwereaffectedbypartialsevereanomalies.
At the precardial venous level (S1) we diagnosed a lack ofcontinuityof the IVCinallcaseswithaspecificdiscontinuitybelow the liver (Figure 1B and 1C). As a consequence, itsupperhepaticportionhadaseparateopeningatthebottomoftheatrium,andthelowerportiondrainedintotheenlargedhemiazygos or azygos vein (Figure 2A and 2B). The inferiorportionoftheIVC,therefore,couldnotbeidentifiedinitsusualpositionbutrathertotheleftofthespine.ThevenousdrainageoftheSVCwasregularlyfoundtobeontherightsideofthecommonatrium in2 cases. In theother2 cases,however, a persistent SVCwas additionally (Figure 1B) observedonthe left (Figure 1C). At venoatrial level (S2) a commonatriumwas confirmed in 2 cases. Moreover, bilateral sickle-shapedappendages and left configured atria were diagnosed (Figure 2A-2D).Bothatrialappendageswereelongatedandattachedbyanarrow junction to the smooth-walledportionof theatrium,whichpresentsasmorphologicalleftatrialappendages.Therewasabsolutelynoterminalcrest.Thepectinatemuscleswereconfinedtotheappendagesandnotextendedaroundtheatrioventricularjunctionas in themorphologic right atrium.Within theatriumwefoundonlyathinbandoftissue,characteristicofaremnantof theatrial septum.Thepulmonaryveins joined the commonatriumatthecentralpartoftheposterioratrialwall.Anomaliesatthelevelofatrioventricularconnection(S3)werealsodetectedin all cases. Commonly, theundividedAV canal openedwith adysplasticAVvalveintoabifidventricle.Attheventricularlevel(S4)inthemainfunctionalanomalieshavepriority.Analysingtheventriculoarterialconnection(S5)adoubleoutletrightventriclewasdiagnosedin2of4cases.Withregardtotherelationshipofthe great arteries toone another, theascendingaorta left theheart rightand infrontof thepulmonarytrunk (Figure 2C and 2D).Wediagnosed, therefore, a complete transpositionof thegreatarterieswith theaorticvalveanteriorand to the rightofthe pulmonary valve. Structural defects were also seen in thepostcardialarterialsegment(S6) in3ofthe4cases. Itreferredto hypoplasia of one of the great arteries and coarctation ormalpositionoftheaorticarchaswellasanomaliesoftheductusarteriosusBotalli.
With reference to extracardial post mortem findings in casesof left isomerism, the bronchial morphology corresponded tothat of the bilateral left configured atria because both lungswere bilobed with two symmetrical hyparterial morphologicleftbronchi.Theliverwasbilateralsymmetrical,andinonecasethe extrahepatic biliary structures, such as the biliary bladder,were atretic.Multiple spleens (polysplenia) and thepancreatictail were found in the right upper abdomen (Figure 3B). Theright sided stomach continued in a distorted malpositionedduodenumontheleftsideandtheduodeno-jejunaljunction,aswellastheligamentofTreitz,werefoundrightofthespine.The
Foetussex/gestational age
Echocardiographic Findings
Extracardiac Findings
A612♀17weeks+3days
•dextrocardia•commonatrium•completeAVSD•hyperplasiaofbothventricles•severebradyarrhythmia
•visceroatrialsitusinversus•right-sidedstomach
A799♀22weeks+6days
•dextrocardia•commonatrium•completeAVSD•hyperplasiaofbothventricles•severebradyarrhythmia
•visceroatrialsitusinversus•right-sidedstomach
A973♀16weeks+0days
•levocardia•completeAVSD•commonarterialtrunc•sinusrhythm(158bpm)
•abdominalsitusinversus•right-sidedstomach
A1079♀14weeks+4days
•levocardia•mitralvalveatresia•hypoplasticleftventricle•VSD•aorticstenosis•bradyarrhythmia(44bpm)
•visceroatrialsitussolitus
Left Isomerism(sonographicallysuspectedandpostmortemconfirmed)
A722♂20weeks+2days
•levocardia•completeAVSD•commonarterialtrunc•sinusrhythm
•incompletesitusinversus•right-sidedstomach
Left Isomerism(sonographicallysuspectedbutpostmortemdiagnosedright
isomerism)AV =AtrioVentricluar;AVSD = AtrioVentricluar SeptalDefect;VSD = VentricluarSeptalDefect;IVC=InferiorVenaCava
Table 1Sonographicfindingsin5foetuseswithheterotaxy

3© Under License of Creative Commons Attribution 3.0 License
Annals of Clinical and Laboratory Research ISSN 2386-5180 Vol. 4 No. 1: 71
2016
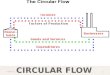
Figure 1 Embryonaldevelopmentofthesuperiorandinferiorvenacava-normallyandincasesofleftandrightisomerism(drawings).A) Normally:Developmentofsuperiorandinferiorvenacava(SVC/IVC)on6to8weekofpregnancy.Notethepairedcranialandcaudalprecursorveins:cardinalveins(blue),subcardinalveins(yellow),supracardinalveins(orange),connectingsub-/supracardinalanastomoses(green).TheprecursorsofthehepaticsegmentofIVC(violet)arevitellineveins,whichalsogiverisetohepaticveins,portalveinandsuperiormesentericvein.B) Leftisomerism(e.g.A612):SingleSVCoriginatedfromrightsidedcranialcardinalvein.NotethediscontinuityofIVCbelowitssuperiorpart(sp-IVC)respectivelyhepaticsegment(violet)andtheleft-sidedmalpositionofitsinferiorpart(ip-IVC):prerenal(orange),renal(green),postrenal(yellow)segmentandtheazygos-vein-continuation(azV).C) Leftisomerism(e.g.A799,A973,A1079):BilateralSVCoriginatedfromrightandleftsidedcranialcardinalvein.NotethediscontinuityofIVCbelowitssuperiorpart(sp-IVC)respectivelyhepaticsegment(violet)andtheleft-sidedmalpositionofitsinferiorpart(ip-IVC)-prerenal(orange)renal(green)andpostrenal(yellow)segmentandthehemiazygos-vein-continuation(hazV).D) Rightisomerism(e.g.A722):BilateralSVCoriginatedfromrightandleftsidedcranialcardinalvein.Notetheleft-sidedmalpositionofthewholeIVC(l-IVC).
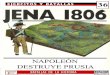
Figure 2 Leftisomerism-postmortalcardiacfindingsinafemalefoetus(A612;17weeks/3days).(A,B) Photographanddrawingoftheprecardialvenousinflow;rightsidedview:discontinuedinferiorvenacava(IVC);inferiorpart(ip-IVC)totheleftoftheabdominalaorta(ab-Ao)andoesophagus(Oe)withazygosvein(azV)-continuation;superiorpart(sp-IVC)withusualopeningonthebottomofthecommonatrium;bilateralleftconfigured(sickleshaped)atrialappendages(lc-aA).(C,D) Photographanddrawingofthepostcardialarterialoutflow;leftsidedview:doubleoutletrightventriclewithdextro-transpositionofthegreatarteries(d-TGA)-ascendingaorta(as-Ao)rightandinfrontofthepulmonarytrunk(pT);preductalaorticcoarctation(CoA).
portalveinwasfoundbelowthesuperiorpartofduodenumandthe superiormesenteric vesselsbehind itsdescendingpart.Asaconsequencethesmallbowelwaslocatedontheleftandthewholelargeintestineontherightoftheabdomen.Withregardto this malpositioned colon we were not able to detect anymesentericattachement (commonmesenterium).Moreover, in3foetusesofleftisomerismanincoherentlateralitybetweentheleftsidedheartaxis(levocardia)andthepartialsitusinversusintheupperabdomenwasdiagnosed,alsoknownasviscerocardiacheterotaxyorsitusambiguous.
Asummaryofthesonographicfindingsofthefoetuswithright isomerism is also given in Tables 1. Structural heart diseaseconcerningcompleteatrioventricularseptaldefectandcommonarterial trunk was prenatally diagnosed. Other extracardiacfindingswerearightsidedstomachandincompletesitusinversus.
Thestructuralheartdiseasecouldbeconfirmedatpostmortem.AsseeninTable 2,allsegmentsofthefoetalheartwereaffected.Attheprecardialvenouslevel(S1)wediagnosedapersistentleftSVCandaleftsidedIVCanteriortotheabdominalaorta(Figure
1D).Atvenoatriallevel(S2)thecommonatriumwascharacterizedby inverse configured appendages and atria (Figure 4A-4D).Thatpartof theatrialwallwhich is responsibleforpulmonary-venousreturnwashypoplastic.Thepulmonaryveinsjoinedthecommon atrium at the central part of the posterior atrialwallbetween the both SVC and the coronary sinuswasmissed. Atthelevelofatrioventricularconnection(S3)thesonographicallydetectedcompleteatrioventricularseptaldefect,withacommendysplastic atrioventricular valve, could be confirmed. At theventriculoarterial connection (S4andS5)a single ventricle andabigsemilunarvalvewithcontinuation intoacommonarterialtrunkwere diagnosed as seen in Figure 4A and 4B. Analysingthe postcardial arterial segment (S6)wedetected the route oftheaorticarchtotherightofthetracheaanddiagnosedmirror-inverted origins of its systemic branches followed by systemic

2016Annals of Clinical and Laboratory Research
ISSN 2386-5180 Vol. 4 No. 1: 71
4 This Article is Available in: www.aclr.com.es
pulmonaryarteries.
Withreferencetoextracardialpostmortemfindingsinthecaseofrightisomerism,thelungsweretrilobedwithtwosymmetricaleparterial morphologic right bronchi. The liver was invertedandthestomach,thespleenaswellasthetailof thepancreaswerefound intherightupperabdomen(Figure 3C).Moreover,therewasanabnormalrouteof theduodenumincombinationwith an abnormal position of the portal vein on the left andabnormal located the superiormesenteric vessels right to theduodenum. As a consequence, the midgut derivatives weremalrotated with the subsequent malposition and malfixation(commonmesenterium)of the large intestinebehindthesmallbowel.Finally,aviscerocardiacheterotaxy(situsambiguous)wasdiagnosedduetotheincoherentlateralitybetweentheleftsidedheartaxis(levocardia)andthepartialsitusinversusintheupperabdomen.
DiscussionThisstudyreportsthecompletespectrumofdetectedanomaliesin5foetuseswithheterotaxy-syndrome.Heterotaxyisalateralitydisturbanceassociatedwithpairedleftorrightsidednessviscera,the malpositioning of unpaired visceral organs and vessels aswellassplenicanomalies.Congenitalheartandgastrointestinalmalformations are commonly associated with this syndrome.
Some of the structural abnormalities can be recognised onlyduring autopsy. The definition of heterotaxy, however, isfundamentalfortheevaluationofthevisceroatrialarrangement,togetherwithothercharacteristicsignsofthissyndrome.
Thediagnosticcriteriaofheterotaxyincludetheisomerismofthepulmonal lobesandthebronchialbranching.Typicalfindingsinthe right isomerism arebilateralmorphological right (trilobed)lungswitheparterialbronchi. In contrast, the left isomerism ischaracterised by bilateral left (bilobed) lungs with hyparterialbronchi.Thisotherwiseveryrarebronchopulmonardysmorphismcanbedetectedonlyduringautopsydespitetheprogressmadeinprenataldiagnosticimaging.
Complex cardiac lesions are frequently diagnosed in patientswith heterotaxy in both settings [1,5,8]. Using the segmentalapproachwedetecteddistinctmalformationsatseveralcardiaclevels.Itconcernstheveno-atrial,theatrio-ventricular,andtheventriculo-arterial segment, aswell as theprecardial veinsand thegreatpostcardialarteries.
Thetypicalsignsincasesof leftisomerismincludethebilateralsickle-shaped atrial appendages and the left configured atrialwall [2]. Inmost cases of the left isomerism the sinus node isabsent resulting in a prenatal diagnosedheart block.Wehave
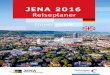
Figure 3 Finalpositionoftheabdominalorgans-normallyandincasesofleftandrightisomerism(drawings).A) Normally:Left-sidedstomach(Sto),tailofpancreas(Pa)andspleen(Sp).Notethepositionsoftheportalvein(pV)abovethesuperiorpartofduodenum(D)andofthesuperiormesentericarteryandvein(smAV)infrontoftheinferiorpartofduodenum.Notetheregularpositionandfixationofthelargeintestine–ascending,transverseanddescendingcolon(a/t/dC)-aroundthesmallbowel(ingraphsevered).B) Leftisomerism(e.g.A612):Right-sidedstomach,tailofpancreasandmultiplespleens(m-Sp).Notetheabnormalrouteoftheduodenum(D)incombinationwithanabnormalpositionoftheportalvein(pV)belowitssuperiorpartandthesuperiormesentericvessels(smAV)behind.Inconsequence,themidgut-derivativesweremalrotatedwithsubsequentdextropositionandmalfixationofthelargeintestine–ascending,transverseanddescendingcolon(a/t/dC)-followingtheleft-sidedsmallbowel(ingraphsevered).C) Rightisomerism(e.g.A722):Right-sidedstomach,tailofpancreasandspleen.Noteabnormalrouteoftheduodenum(D)incombinationwithanabnormalpositionoftheportalvein(pV)lefttothesuperiorpartofduodenumandofthesuperiormesentericvessels(smAV)righttotheduodenum.Inconsequence,themidgut-derivativesweremalrotatedwithsubsequentmalpositionandmalfixationofthelargeintestine–ascending,transverseanddescendingcolon(a/t/dC)-behindthesmallbowel(ingraphsevered).

5© Under License of Creative Commons Attribution 3.0 License
Annals of Clinical and Laboratory Research ISSN 2386-5180 Vol. 4 No. 1: 71
2016
been consistent, however,withWare et al. [9],who indicated,that the absence of the sinus node in cases of left isomerismis not mandatory. The left isomerism is frequently combinedwith a dysplastic atrioventricular connection resulting fromcomplete atrioventricular septal defects. Moreover, anomaliesatthelevelofventriculoarterialconnectionandthepostcardial
arteries, including transposition of the great arteries, left- orright-sidedobstructionsandmalpositionoftheaorticarch,mayalsooccur[2].Preductalcoarctationoftheaorticarchmayresultfromadecreasedbloodflowthroughthe leftsideof theheartin combination with ventricular anomalies. Nevertheless, it isreported,that left isomerismmayalsocoexistwithastructural
Foetus Cardiac Findings Extracardiac Findings
A612♀
•levocardia•S1:discontinuedIVCwithazygoscontinuation•S2:commonatriumwithbilateralsickle-shapedappendagesandatria
•S3:completeAVSDwithcommondysplasticAVvalve•S4:functionalsingleventricle•S5:doubleoutletrightventricle(DORV)andd-transpositiongreatarteries(d-TGA)
•S6:preductalaorticcoarctation(CoA)
•bilateralbilobarlungsandhyparterialbronchi•bilateralsymmetricliver;biliaryatresia•right-sidedstomach,pancreaticcauda,andmultiplespleens•duodenalmalposition•malpositionofportalveinandsuperiormesentericvessels•malpositionofthesmallandlargebowel,commonmesenterium
A799♀
•dextrocardia•S1:persistentleftSVC;discontinuedIVCwithhemiazygoscontinuation
•S2:commonatriumwithbilateralsickle-shapedappendagesandatria
•S3:completeAVSDwithcommondysplasticAVvalve•S4:functionalsingleventricle•S5:ordinary•S6:ordinary
•bilateralbilobarlungsandhyparterialbronchi•bilateralsymmetricliver•right-sidedstomach,pancreaticcauda,andmultiplespleens•duodenalmalposition•malpositionofportalveinandsuperiormesentericvessels•malpositionofthesmallandlargebowel,commonmesenterium
A973♀
•levocardia•S1:persistentleftSVC;discontinuedIVCwithhemiazygoscontinuation
•S2:bilateralsickle-shapedappendagesandatria•S3:dysplastic/atreticmitralvalve•S4:hypoplasticleftventricle(HLV)•S5:doubleoutletrightventricle(DORV)andd-transpositiongreatarteries(d-TGA)
•S6:hypoplasticpulmonarytrunk,aplasticductusarteriosusBotalli,right-sidedaorticarch
•bilateralbilobarlungsandhyparterialbronchi•bilateralsymmetricliver•right-sidedstomach,pancreaticcauda,andspleen•duodenalmalposition•malpositionofportalveinandsuperiormesentericvessels•malpositionofthesmallandlargebowel,commonsenterium•uterusunicornisright,left-sidedagenesiaofuterusanduterinetube
A1079♀
•levocardia•S1:persistentleftSVC;discontinuedIVCwithhemiazygoscontinuation
•S2:bilateralsickle-shapedappendagesanddilatatedatria•S3:hypoplasticmitralvalve•S4:VSD,hypoplasticleftventricle•S5:hypoplasticascendingaorta•S6:hypoplasticaorticarch
•bilateralbilobarlungsandhyparterialbronchi•bilateralsymmetricliver•right-sidedstomach,pancreaticcauda,andmultiplespleens•duodenalmalposition•malpositionofportalveinandsuperiormesentericvessels•malpositionofthesmallandlargebowel,commonmesenterium
Left Isomerism (postmortemconfirmed)
A722♂
•levocardia•S1:abnormalpulmonaryvenousreturn;persistentleftSVC;left-sidedIVCanteriortotheaorta
•S2:commonatriumwithinverseconfiguredappendagesandatria
•S3:completeAVSDwithcommondysplasticAVvalve•S4:singleventricleandsemilunarvalve•S5:commonarterialtrunc•S6:right-sidedaorticarch;mirror-invertedoriginofitsbranches;systemicpulmonalperfusion
•bilateraltrilobarlungsandeparterialbronchi•inverseliver•right-sidedstomach,pancreaticcauda,andspleen•duodenalmalposition•malpositionofportalveinandsuperiormesentericvessels•malpositionofthesmallandlargebowel,commonmesenterium
Right Isomerism (postmortemdetected)S1: precardial venous, S2: venoatrial, S3: atrioventricular, S4: ventricular, S5: ventriculoarterial and S6: postcardial arterial segment (AV = atrioventricluar;VA=ventriculoarterial;AVSD=atrioventricluarseptaldefect;VSD=ventricluarseptaldefect;SVC/IVC=superior/inferiorvenacava)
Table 2Postmortalcardiacandextracardiacfindingsinfoetuseswithheterotaxy;teratologicalevaluationaccordingtotheguidelinesofthesequentialsegmentalapproach

2016Annals of Clinical and Laboratory Research
ISSN 2386-5180 Vol. 4 No. 1: 71
6 This Article is Available in: www.aclr.com.es
normalheart[10-12].
Incontrast,rightisomerismisfrequentlyassociatedwithbilateralblunt-shaped atrial appendages and a right configured atrialwall (rightatrial isomerism).Inourstudywefoundan inversedatrialmorphologyinthefoetuswithrightisomerism.Thetypicalsigns often include multiple severe anomalies at all cardiaclevels. Commonly, there is a predominance of atrioventricularseptal defects and anomalies at the level of ventriculoarterialconnections including double outlet right ventricle, trans- ormalpositioning of the great arteries, pulmonary atresia andcommonarterialtrunk[1].ThepostcardialarteriesarefrequentlycharacterisedbyanaplasticductusarteriosusBotalliandaright-sidedaorticarchas seen inour study.Typicalfindings in casesof heterotaxy are disorders of the systemic and pulmonaryvenousreturntotheheart.Themainfeatures incasesof rightisomerism include a duplicated SVC and a malpositioned IVC,whichmaybe anterior or juxtaposed to the aorta. Commonly,there is alsoapredominanceof anomalouspulmonaryvenousreturn [5] resulting from the hypoplasia of the correspondingatrial wall. Discontinuity of IVC is an excellent marker of left
isomerism[1,5,13,14].Thereportedprevalencerangesbetween55and85%. In our study, all foetuseswith left isomerismhada termination of the IVC below its hepatic segment. Systemicvenous flow beyond this point was accommodated by dilatedazygosorhemiazygosveins,whichemptyeither intothesingleright-sidedoranaccessoryleft-sidedSVC[15].
For a clearer understanding, it should be noted that theembryonic development of the caval veins is a very complexprocess, originating from paired left- and right-sided primitiveveins [16]. As seen in Figure 1A, the IVC is composed of fourdifferent precursor segments: the hepatic, the suprarenal, therenal, and the infrarenal. The hepatic segment develops fromthevitellinevein,andthethreemorecaudallylocatedsegmentsevolvefromthesub-andsupracardinalveinsaswellasseveralconnecting anastomosis. Normally, the suprarenal segment isformed by the right subcardinal vein and subcardinal-hepaticanastomosis.DiscontinuityoftheIVCincasesof leftisomerismresults from a failure of subcardinal-hepatic anastomosis withthe consequent atrophy of the right-sided primitive veins andsubsequentdevelopmentoftheleftsidedveins(Figure 1B and
Figure 4 Rightisomerism-postmortalcardiacfindingsinamalefoetus(A722;20weeks/2days).A,B:Photographsoftheanomaliesatvenoatrialandventriculoarterialsegments;antero-superiorview:bilateralsuperiorvenacava(SVC);inverseconfiguredatrialappendages(ic-aA):blunt-shapedleftandsickle-shapedrightappendage;singleventricle(s-V)withcontinuationinacommonarterialtrunc(c-AT);right-sidedaorticarch(r-AoA).Notethesinglebigsemilunarvalve(sl-V).C,D: Drawingsofthenomaliesatvenoatrialandventriculoarterialsegments;leftandrightsidedview:rightandleftsuperiorvenacava(r-/l-SVC),leftsidedinferiorvenacava(l-IVC)anteriortotheabdominalaorta(a-Ao);hypoplasticatrialwallatpulmonaryveinsreturn(PVR);commonarterialtrunc(c-AT);right-sidedaorticarch(r-AoA);systemicperfusionofpulmonaryartery(s-PA).

7© Under License of Creative Commons Attribution 3.0 License
Annals of Clinical and Laboratory Research ISSN 2386-5180 Vol. 4 No. 1: 71
2016
1C).Thesuprarenalsegmentwasformedbythe left insteadofthe right subcardinal vein, and the renal segment by the left,instead of the right, sub-supracardinal anastomosis.Moreover,theinfrarenalsegmentderivedfromtheleftinsteadoftherightsupracardinalvein.Only,thehepaticsegment,therefore,drainedseparately into the right or the common atrium. In contrast,themalpositionof the IVC incasesof right isomerism resultedfrom a laterally reversed development (Figure 1D). Congenitalanomaliesof the ICV in casesof heterotaxy syndromewithoutcongenital cardiac defects are often discovered incidentally inadults,becausetheyareusuallyasymptomatic.Theymaycause,however, diagnostic and therapeutic difficulties in cardiology,phlebologyandsurgery[12].
A leftsidedSVC isseen in0.3 -0.5%of thenormalpopulationand in4.4%of thosewith congenitalheartdiseaseparticularlyincasesofheterotaxy.InthevastmajorityitisaccompaniedbyanormalrightsidedSVC,termedSVCduplication.Itresultsfromfailure of the embryonic left anterior cardiac vein to regress.DrainageisvariableandcanbetotherightatriumviatheobliqueveinofMarshall,thecoronarysinusortheleftatrium.Inthevastmajorityofcases(82-90%)anormal(butsmall)rightsidedSVCisalsopresent,andapersistentbridgingvein(leftbrachiocephalicvein)isseenin25-35%ofcases[16].
Oneoftheimportantdiagnosticindicatorsistheviscerocardiacheterotaxy. Mainly, the heart is left-sided with the apexorientated to the left. In all cases we found an inverted orsymmetricalliverandamirror-imagestomach.Moreover,ahighrate of congenital abnormalities of the intestine, particularlyat the level of the foregut including the hepatobiliary andpancreatic tree, is reported inheterotaxy [6,14]. Foetuseswithleftisomerismareatriskofbiliaryatresiaasshowninourstudy.Thespleenandthepancreasweredetectednearthestomachintherightupperabdomen.Itshouldbenotedthatboth,thetailofpancreasandthespleen,developinthedorsalmesogastrium.Occasionally,ahigh incidenceofshortortruncatedpancreasisreported[14].Thereweremultiplesplenulesonlyincasesofleftisomerism,inrightisomerism,however,thespleenissometimesabsent.Althoughpolyspleniaisthemostcommonfindinginleftisomerism,aspleniaoranormalspleenmayalsobepresent[13].As seen inFigure 3A, special attentionshouldbealsodirectedtowards intestinal rotationaldisorders given thepresumed riskofmidgutvolvulus[17].Thenormaldevelopmentofthehumanintestine involves two processes: the so called “rotation” ofthemidgut and the subsequent fixation of the colon and themesentery.
Anomalies of midgut derivatives are usually termed“malrotation”. It includes “nonrotation”, “incomplete rotation”and the rare “reversed completeor incomplete rotation” [18].Whiletheriskof“malrotation”inthegeneralpopulationislessthan1%,itmaybeashighas70%incasesofheterotaxyalthoughthe exact incidence is not precisely known. For patients withsitusambiguousvariousanatomicalconfigurationsof thesmallbowelandthecolonhavebeenreported[14].Ourfindingsareconsistent with those of Kluth et al. [19], who indicated thatthe normal position of the bowel is depended on the normaldevelopmentof theduodenal loop.Assuch, this loopemerges
via localized growth and lengthening of the duodenum in theearlyperiodofembryonicdevelopment.Furthergrowthpushesthe tip of the duodenojejunal loop beneath the mesentericroot,which then reaches its normal position left of the spine.Basedonourstudy,wesuggestthattheimproperformationofthe duodenal loop seems tobe the crucial factor for differentforms ofmalrotation in cases of heterotaxy. In all investigatedfoetuseswe found theduodenal loopwith an abnormal routeleftof themidlineandcontinuation inanabnormal right-sidedduodenojejunaljunction.Theabnormalrouteoftheduodenumwas associated with different malpositions of the portal vein.In right isomerism the veinwas found to the leftof theupperborder of the duodenum. In left isomerism, though, it had anabnormalinfrapyloricorigin.Followingitssubsequentascensionin front of the duodenum the vein enters the malpositionedmidline liver. The preduodenal ascension of the portal vein isoneoftheradiologicalsigndiagnosedincasesofleftisomerism[14].Embryonically,theportalvenoussystemisderivedfromthevitellineveins,whichdraintheprimitivegastrointestinaltract.Thetwoveinsareconnectedbythreeinterconnectingveins,acranial(in the liver), a middle (behind the duodenum), and a caudal(infrontoftheduodenum).Normally,theportalveinisformedby selective obliteration in early development. Atrophy of thecranialandcaudal inter-connectingveinsalongwiththecaudalsegmentoftherightandcranialsegmentoftheleftvitellineveinsresultsinanormalS-shapedportalvein.Anabnormalpositionoftheportalveinisbasedonleft-andright-sidedvariationsinthisprocess.
Moreover, the abnormal route of the duodenum was in allinvestigatedfoetusescombinedwithamalpositionofthesuperiormesentericarteryandvein.Thesevesselsprovidethecentralaxisofthemidgutloopwhichtemporarilyprojectsintotheremainsoftheextraembryoniccoelomintheproximalpartoftheumbilicalcord.Themalpositionof thesuperiormesentericvessels is theprerequisitefortheabnormalarrangementofthegutfollowingits return into the abdominal cavity. Moreover, all variants ofmalrotationareaccompaniedbyasubsequentmalfixationoftheascendinganddescendingcolon.
Withreferencetotheoverlapofcardiacandvisceralanomaliesinthetwoformsofheterotaxysyndrome,thedifferentiationofleftandright isomerismmainlyrelieson thebronchopulmonalmorphologyandtheanomaliesof the IVC.Discontinuityof theIVC represents an excellent marker for left isomerism, as thisanomaly is rare under other circumstances. In our study theIVChada lackof continuity inall foetuseswith left isomerism.Thereportedincidenceof leftisomerismincasesofheterotaxyranges between 55% and 85% and includes both infants andfoetuseswhowere the subjectof apost-mortemexamination.Theprenataldiagnosisofrightisomerismremainsadifficulttask.An importantmarker is the juxta-/anteropositionof IVC to theabdominalaorta incombinationwithviscerocardiacheterotaxyandcomplexcardiacmalformations.Specialattentionshouldbepaid to the anomalies of the pulmonary venous return as hasbeendemonstratedinourstudy.
Autopsystudieshaveshownthatrecognitionofthemorphologicalcharacteristicsoftheisomericatrialappendagesisthebestguide

2016Annals of Clinical and Laboratory Research
ISSN 2386-5180 Vol. 4 No. 1: 71
8 This Article is Available in: www.aclr.com.es
to the existenceof the2 entities in heterotaxy syndromes [9].It remains unclear, however, whether the morphology of theatria and their appendages is genetically determined by thetypeof isomerismormechanicallymodulatedbythedisturbedhaemodynamicinthesehearts.AccordingBergetal.[5],neitherthepresenceofanatrioventricularseptaldefectnorothercardiacanomalies were significantly correlated to atrial morphology,suggesting that theatrialmorphology is independent fromthemajorcardiacmalformationsinheterotaxysyndromes.
Foetuses with complex cardiac anomalies and an abnormalvisceral situs are strongly predictive of a normal karyotype.Significant progress, however, was recently achieved in theunderstandingofthegeneticpathwaysultimatelyresponsibleforleft/rightasymmetryinanimalmodels[3].Briefly,aninitialbreakin symmetryoccurs at theprimitivenode asa leftward “nodalflow”.Itprovokesasymmetricsignalsthataretransmittedtowardthe left lateral plate mesoderm. Transcription factors, Nodal,Lefty2, and Pitx2c, regulate genetic programmes on the leftsideof thebodyand createasymmetricorganmorphogenesis.Moreover, severalgenes, includingZIC3,NODAL,LEFTY2,CFC1,SHROOM3, seem to be responsible for left-right laterality andits disturbance in cases of heterotaxy [3,14,15]. Nonetheless,the mechanism of consistent left/right asymmetry duringembryogenesisremainsamajorareathatisopentoberesearch.
ConclusionsThedetailedsegmentalanalysisofthefoetuseswithheterotaxybyahighlyskilledexpertinteratologyisofextremeimportancefor the advancement of the prenatal investigation. In spite ofbeing uncommon, congenital anomalies, particularly in thecardiovascular, bronchopulmonal and gastrointestinal system,maycausedifficulties in the interpretationofprenatalfindings.A basic knowledge of embryology is required for the correctinterpretation and description of the real extent of complex
malformation pattern by sonographers and radiologists.With patience and attention to detail the specific congenitalmorphologyinbothsettingsofheterotaxymaybemadeeasierto understand. This is essential in order to effectively counselparentsonfurtherdiagnosticstepsthatmaybetakeninadditiontolikelypostnataloutcomes[6].
Left and right isomerism may have both biventricluar heartswithlargeatrioventriculardefects.Patientswithrightisomerismtendtohavecomplexcardiac lesionsmorefrequently,whereasin left isomerism only ventricular septal defects or no cardiacanomaliesmayoccur [20]. Ingeneral, themortality in foetusesandneonatesishighinthepresenceofheartblockandhydropsorpulmonaryatresiaandanomalouspulmonaryvenousreturn,andthemorbidity ismainlydeterminedbythecardiacdefects.Death in thefirst yearof life is common in right isomerism. Incontrast, theprognosisof left isomerismmaybequitegood intheabsenceofheartblock,asittendstopresentwithlessseverecardiacanomaliesorevenwithnormalintracardiacanatomy.
Although neonatal morbidity and mortality are determinedmainlybythecardiacabnormalities,thevisceralanomaliesmaystrongly affect the long-term outcome.With the improvementin long-term outlook for these patients with modern cardiacsurgerytheintra-abdominalanomalieshavebecomeincreasinglysignificant. A detailed prenatal examination to enable propercounselling in an interdisciplinary approach (i.e. obstetricians,neonatologists, cardiologists and cardiac surgeons, andvisceralsurgeons)istherebycrucial.
AcknowledgementTheauthorswishtoexpresstheirthankstoallparentsinvolvedforgivingpermissiontocollectthepresenteddata.ManythanksalsotoSabineMüllerforhertechnicalassistancethroughoutthestudyandtoJensGeilingforhisexcellentdrawings.

9© Under License of Creative Commons Attribution 3.0 License
Annals of Clinical and Laboratory Research ISSN 2386-5180 Vol. 4 No. 1: 71
2016
References1 BergC,GeipelA,SmrcekJ,KrappM,GermerU,etal.(2003)Prenatal
diagnosis of cardiosplenic syndromes: a 10-year experience.UltrasoundObstetGynecol22:451-459.
2 Pepes S, Zidere V, Allan LD (2009) Prenatal diagnosis of left atrialisomerism.Heart95:1974-1977.
3 Shiraishi I, Ichikawa H (2012) Human heterotaxy syndrome frommoleculargeneticstoclinicalfeatures,management,andprognosis.CircJ76:2066-2075.
4 JacobsJP,AndersonRH,WeinbergPM,WaltersHL III,TchervenkovCI, et al. (2007) The nomenclature, definition and classificationofcardiacstructuresinthesettingofheterotaxy.CardiolYoung2:1-28.
5 Berg C, Geipel A, Kohl T, Smrcek J, Germer U, et al. (2005) Fetalechocardiographic evaluation of atrial morphology and thepredictionoflateralityincasesofheterotaxysyndromes.UltrasoundObstetGynecol26:538-545.
6 Gottschalk I, Berg C, Heller R (2012) Disorders of laterality andheterotaxyinthefoetus.ZGeburtshilfeNeonatol216:122-131.
7 Anderson RH, Shirali G (2009) Sequential segmental analysis. AnnPediatrCardiol2:24-35.
8 Berg C, Geipel A, Kamil D, Krapp M, Breuer J, et al. (2006) Thesyndrome of right isomerism: prenatal diagnosis and outcome.UltraschallMed27:225-233.
9 WareAL,MillerDV,PorterCB,EdwardsWD(2012)Characterizationof atrial morphology and sinus node morphology in heterotaxysyndrome: an autopsy-based study of 41 cases (1950-2008).CardiovascPathol21:421-427.
10 DePaolaN,ErmitoS,NahomA,DinataleA,PappalardoEM,etal.(2009)Prenataldiagnosisofleftisomerismwithnormalheart:acasereport.JPrenatMed3:37-38.
11 DilliA,GultekinSS,AyazUY,KaplanogluH,HekimogluB(2012)Ararevariationoftheheterotaxysyndrome.CaseRepMed2012:840453.
12 HildebrandH,GunzenhauserD,WeberK,FreseW,FröberR,etal.(2007)Heterotaxiasyndromewithoutcongenitalcardiacdefects indilatedcardiomyopathy.DtschMedWochenschr132:931-937.
13 BergC,GeipelA,KamilD,KnüppelM,BreuerJ,KrappM,etal.(2005)Thesyndromeofleftisomerism:sonographicfindingsandoutcomeinprenatallydiagnosedcases.JUltrasoundMed24:921-931.
14 TawfikAM,BatoutyNM,ZakyMM,EladalanyMA,ElmokademAH(2013) Polysplenia syndrome: a review of the relationship withviscero-atrial situs and the spectrum of extra-cardiac anomalies.SurgRadiolAnat35:647-653.
15 SaitoT,WatanabeM,KojimaT,MatsumuraT,FujitaH,etal.(2011)Successful blood sampling through azygos continuation withinterrupted inferior vena cava. A case report and review of theliterature.IntHeartJ52:327-230.
16 KellmanGM,AlpernMB, SandlerMA,CraigBM (1988)Computedtomographyofvenacavalanomalieswithembryologiccorrelation.Radiographics8:533-556.
17 PapillonS,GoodhueCJ,ZmoraO,sharmaSS,WellsWJ,etal.(2013)Congenital heart disease and heterotaxy: upper gastrointestinalfluoroscopy can be misleading and surgery in an asymptomaticpatientisnotbeneficial.JPediatrSurg48:164-169.
18 StrousePJ(2004)"http://www.ncbi.nlm.nih.gov/pubmed/15378215"Disordersofintestinalrotationandfixation("malrotation").PediatrRadiol34:837-851.
19 Kluth D, Jaeschke-Melli S, Fiegel H (2003) The embryology of gutrotation.SeminPediatrSurg12:275-279.
20 LeeSE,KimHY,JungSE,LeeSC,ParkKW,etal.(2006)Situsanomaliesandgastrointestinalabnormalities.JPediatrSurg41:1237-1242.