Embed Size (px)
Citation preview

IhgtcTsucaliusd©
Immwmtmppavlbhsssaaelnp
tG
UR
2
Clinical Presentation, Natural History, and Treatment of CrescenticProliferative IgA Nephropathy
By James A. Tumlin and R. A. Hennigar
gA nephropathy is one of the most common causes of glomerulonephritis in the world and is characterizedistologically by the deposition of polymeric forms of IgA within the mesangium and in some cases along thelomerular capillary wall.1 Proliferative and crescenteric forms of IgA are associated with nephrotic range pro-einuria, accelerated hypertension, and a more rapid decline toward end-stage renal disease. Previous attempts toategorize the incidence and clinical significance of proliferative IgA nephropathy have given conflicting results.his is in part the result of the lack of a uniform nomenclature and the failure of clinical therapies to prolong renalurvival in specific subgroups. In the present study, we performed a prospective open-label trial of pulse sol-medrol and intravenous cyclophosphamide in 20 patients with IgA nephropathy and at least 10% cellularrescents or endocapillary proliferation on renal biopsy. Seventeen patients underwent repeat kidney biopsiesfter 6 months of therapy, and the morphologic response to treatment was assessed using a modified systemic
upus erythematosis (SLE) histologic activity and chronicity index score. To determine the long-term efficacy ofntravenous cyclophosphamide on renal survival, the results of the treated patients were compared with 12ntreated historical controls. Pulse solumedrol and intravenous cyclophosphamide effectively reduced peakerum creatinine, degree of proteinuria, the rate of decline in renal function, and the incidence of end-stage renalisease at 36 months.2004 Elsevier Inc. All rights reserved.
wcsp1mu(elcfmt
S
apwpifefmopgPm
gA NEPHROPATHY IS a complex disorderwith disease manifestations ranging from mild
esangial matrix expansion and hematuria to ful-inate rapidly progressive glomerulonephritisith endocapillary proliferation and crescent for-ation.2 The binding of IgA to putative Fc recep-
ors on the surface of mesangial cells leads toesangial hypercellularity and production of
roinflammatory cytokines. In addition, IgA com-lexes can indirectly stimulate cell proliferationnd mesangial matrix deposition through the acti-ation of compliment through the mannan-bindingectin and/or alternative pathway.3 An increasingody of literature suggests that this broad array ofistologic and clinical manifestations results inpecific subgroups with different risks for end-tage renal disease (ESRD) and disease progres-ion.4-6 Although mesangial cell hypercellularitynd matrix expansion are common in IgA nephrop-thy, additional glomerular pathology can includendocapillary proliferation, karryhorexis, and cel-ular crescents.2,7-9 The incidence and clinical sig-ificance of these lesions are unknown. In theresent study, we prospectively treated 20 patients
From the Division Nephrology and the Department of Pa-hology and Laboratory Medicine, Emory University, Atlanta,A.Address reprint requests to Dr. James A. Tumlin, Emoryniversity School of Medicine, Renal Division, 1364 Cliftond., NE, Atlanta, GA 30322. E-mail: [email protected]© 2004 Elsevier Inc. All rights reserved.0270-9295/04/2403-0007$30.00/0
idoi:10.1016/j.semnephrol.2004.01.006
56 Semina
ith IgA nephropathy and at least 10% cellularrescents or endocapillary proliferation with pulseolumedrol, oral steroids, and intravenous cyclo-hosphamide. A repeat biopsy was performed in7 of 20 patients after 6 months of therapy, and theorphologic response to treatment was assessed
sing a modified National Institutes of HealthNIH) Systemic Lupus Erythematosis (SLE) dis-ase activity and chronicity index score. When theong-term outcomes of the treated patients wereompared with 12 untreated historical controls, weound that steroids and intravenous cyclophospha-ide reduced peak serum creatinine, level of pro-
einuria, and the incidence of ESRD at 36 months.
METHODS
tudy Criteria and Patient Population
Twenty consecutive patients with IgA nephrop-thy and at least 10% crescents or endocapillaryroliferation referred to Emory University Hospitalere enrolled in a prospective, open-label study ofulse solumedrol, oral prednisone, and monthlyntravenous cyclophosphamide after signing in-ormed consent. Histologic criteria for studynrollment included the presence of incipient-to-ulminate cellular crescents with or without seg-ental endocapillary proliferation in 10% or more
f glomeruli. Clinical entry criteria included theresence of hypertension (�140/90 mm Hg) andreater than 1.0 g of proteinuria per 24 hours.atients were also considered eligible for enroll-ent if IgA nephropathy was associated with clin-
cal signs of Henoch-Schonlein purpura (HSP). All
rs in Nephrology, Vol 24, No 3 (May), 2004: pp 256-268

dweaPpaotclpvasa
S
ndp0mmtopmmt2tmpmDmd1Uca
H
ttuwst
apepftnswdcpiampfdnpr
H
atodcstfsnIlswttcuvgibigccn
CRESCENTIC IgA NEPHROPATHY: CLINICAL COURSE AND TREATMENT 257
rugs, including antihypertensive medications,ere allowed to continue throughout the study
xcept for alternative immunosuppressives (e.g.,zathioprine, mycophenolate, or cyclosporin A).atients were excluded from the study if IgA ne-hropathy was present in a transplanted kidney orssociated with cirrhosis and other secondary eti-logies. Patients were also considered ineligible ifhe initial biopsy demonstrated greater than 50%ortical scarring or if the patient was pregnant oractating. A repeat biopsy was performed in allatients after the completion of 6 months of intra-enous cyclophosphamide. A histologic activitynd chronicity scoring system was used to comparecores in the initial biopsies with those obtainedfter 6 months of therapy.
tudy Protocol
Patients enrolled in the study received intrave-ous methylprednisolone (15 mg/kg per day) for 3ays in conjunction with oral prednisone (1 mg/kger day) for 60 days. Patients were then tapered to.6 mg/kg per day for 60 days followed by 0.3g/kg per day prednisone for 60 days and 0.15g/kg per day for an additional 60 days. At the
ime of repeat biopsy, all patients were maintainedn 10 mg prednisone per day. Intravenous cyclo-hosphamide was given at 0.5 to 0.75 g per squareeter body surface area (m2 BSA) monthly for 6onths. Cyclophosphamide dosages were titrated
o achieve a nadir white blood cell count between500 and 3000 cells/mL3. All patients enrolled inhe study underwent a repeat kidney biopsy 1onth after completion of six courses of cyclo-
hosphamide. Omega-3 fatty acid fish oil supple-entation was then initiated at 12.0 g per day.uring the follow-up period, oral prednisone wasaintained at 0.15 mg/kg per day and systolic and
iastolic blood pressure was maintained between20 and 130 and 60 and 70 mm Hg, respectively.nless clinically contraindicated, all patients re-
eived angiotensin-converting enzyme inhibitorss part of their antihypertensive regimen.
istorical Controls
To determine the long-term clinical response toherapy, changes in the slope of the reciprocal ofhe serum creatinine (1/serum Cr), 24-hour protein-ria, and incidence of ESRD in the treated patientsere compared with 12 untreated patients with
imilar degrees of histologic activity. The surgical
issue archives of The Department of Pathology tnd Laboratory Medicine, Emory University Hos-ital, Atlanta, Georgia, were searched by comput-rized SnoMed codes for a diagnosis of IgA ne-hropathy. Approximately 4500 biopsies datingrom 1992 through mid-2001 were screened. Aotal of 331 cases were found in which the diag-osis of IgA nephropathy was confirmed or con-idered. Of the 331 cases of IgA nephropathy, 28ere identified with histologically active disease asefined by the presence of incipient-to-fulminateellular crescents with or without endocapillaryroliferation in 10% or more of glomeruli. Thencidence of crescentic/proliferative IgA nephrop-thy at Emory University Hospital was approxi-ately 8.5%. Of the 28 patients with crescentic
roliferative IgA nephropathy, 12 patients matchedor age, baseline creatinine, proteinuria, and inci-ence of hypertension but managed without immu-osuppressive therapy were analyzed and com-ared with the treatment group. Biopsies fromenal allografts were excluded.
istology
To determine whether intravenous cyclophosph-mide improves glomerular histopathology, pa-ients underwent repeat renal biopsies and the levelf cellular proliferation and cortical scarring wasetermined using a modified SLE disease activity/hronicity scoring system. Tissue for light micro-copic examination was prepared in the conven-ional manner. A portion of each biopsy was snap-rozen for immunofluorescence studies. Frozenections were stained with fluorescein isothiocya-ate (FITC)-labeled antisera against human IgG,gA, IgM, C3, C4, C1q, and, sometimes, kappa/ambda light chains. The portions of each specimeneparated for electron microscopic examinationere fixed in glutaraldehyde, postfixed in osmium
etroxide, and embedded in epoxy resin. Thin sec-ions were stained with uranyl acetate and leaditrate. Each biopsy contained at least 13 glomer-li. An experienced renal pathologist (RAH) re-iewed the glass slides and electron photomicro-raphs in blinded fashion. Each biopsy was gradedn terms of histologic activity and chronicity (Ta-le 1). Basic grading criteria for histologic activityncluded degree of (1) mesangial proliferation, (2)lomerular endocapillary proliferation, (3) extra-apillary proliferation in the form of cellular cres-ents, (4) karyorrhexis with or without fibrinoidecrosis of glomeruli, (5) subendothelial “immune-
ype” dense deposits, and (6) interstitial inflamma-
toclai
C
tfka
a(2rpb1catoc
M0123E01234C012345K012345S0235I012345
TUMLIN AND HENNIGAR258
ion. Grading criteria for chronicity included extentf (1) global glomerular sclerosis (i.e., obsoles-ence), (2) partial glomerular sclerosis and/or col-apse, (3) fibrous crescents, (4) tubular atrophy,nd (5) interstitial fibrosis. Activity and chronicityndices were then calculated for each biopsy.
linical Data and Statistical Analyses
A detailed chart review for patients in the con-rol and treatment groups was performed and theollowing clinical data determined: (1) time ofidney biopsy, (2) age, (3) sex, (4) race, (5) basal
Table 1. Histologic Grading Criteria Usedin Patients Wi
Histologic Activity
esangial proliferation (0-3 points)� minimal� mild to moderate focal (�50%) segmental� marked segmental accentuation in one or more glom� diffuse (�50%) globalndocapillary proliferation (0-4 pts)� none� mild focal segmental� moderate focal segmental� marked focal segmental� global diffuseellular crescents (0-5 pts)� none� between 1-10% of all glomeruli� between 11-20%� between 21-30%� between 31-40%� �40%aryorrhexis/fibrinoid necrosis (0-5 pts)� none� between 1-10% of all glomeruli� between 11-20%� between 21-30%� between 31-40%� �40%ubendothelial “immune-type” dense deposits (0, 2, 3, 5� none� rare� scattered/occasional� many
nterstitial inflammation (0-5 pts)� none� involving 1-20% of renal parenchyma� 21-40%� 41-60%� 61-80%� �80%
Total pts (activity score)Activity index (out of a possible 27 pts)
nd peak serum creatinine, (6) basal and nadir w
lbumin, (7) systolic and diastolic blood pressures,8) presence of microscopic or gross hematuria, (9)4 hour proteinuria, and (10) and time to renaleplacement therapy. Data was obtained on all 32atients included in the study. Data of aggregateasal and peak serum creatinines (Cr), slope of/serum Cr, proteinuria, and pre- and postactivity/hronicity scores were included in the statisticalnalyses for the study group and historical con-rols. Data are expressed as mean � standard errorf mean for continuous variable or number (per-entage) for dichotomous variable unless other-
termining Activity and Chronicity IndicesNephropathy
Chronicity
Glomerular obsolescence (0-5 pts)0 � none1 � between 1-20% of glomeruli2 � between 21-40%3 � between 41-60%4 � between 61-80%5 � �80%Partial glomerular sclerosis and/or collapse (0-5 pts)0 � none1 � between 1-20% of glomeruli2 � between 21-40%3 � between 41-60%4 � between 61-80%5 � �80%Fibrous crescents (0-5 pts)0 � none1 � between 1-20 of glomeruli2 � between 21-40%3 � between 41-60%4 � between 61-80%5 � �80%Tubular atrophy (0-5 pts)0 � none1 � between 1-20% of glomeruli2 � between 21-40%3 � between 41-60%4 � between 61-80%5 � �80%Interstitial fibrosis (0-5 pts)0 � none1 � 1-20% scaring of renal cortex2 � 21-40%3 � 41-60%4 � 61-80%5 � �80%
Total pts (chronicity score)Chronicity index (out of a possible 25 pts)
for Deth IgA
eruli
pts)
ise stated. Differences within the treatment group

wstcsagcWIc
cotctaidcmd1dHwt(tup
ipPsiC
1c21ar1f1brmtmpbmt
recafco
crwIcaamusco1almuil
CRESCENTIC IgA NEPHROPATHY: CLINICAL COURSE AND TREATMENT 259
ere calculated using a Student t test and a two-ample paired analysis. Differences between thereatment group and historical controls were cal-ulated using a Student t test and a two-sampleeparate variance analysis. The incidence of ESRDt 36 months was calculated using a 2 � 2 contin-ency table and chi-squared analysis. Statisticalalculations were conducted using GB Stat forindows, version 5.0 (Dynamic Microsystems,
nc, Silver Spring, MD). A P value of �0.05 wasonsidered to be statistically significant.
RESULTS
To determine the efficacy of corticosteroid andyclophosphamide therapy on the progressionf crescentic/proliferative IgA nephropathy, 20reated patients were compared with 12 historicalontrols matched for age, gender, baseline Cr, pro-einuria, and histologic severity. The clinical char-cteristics of the patients in both groups are listedn Table 2. There were no statistically significantifferences between the two groups in age, serumreatinine, or serum albumin. Male patients wereore frequent in the control group, but this trend
id not reach statistical significance. Although 5 of2 patients in the control group had systolic andiastolic blood pressures greater than 140/90 mmg, all patients (20 of 20) in the treatment groupere hypertensive. This difference was not statis-
ically significant. Clinically significant proteinuria�1.0 g/24 hour) was present in 100% of thereatment group, whereas nephrotic range protein-ria (�3.0 g/24 hours) was observed in 50% of
Fig 1. Steroids and cy-lophosphamide stabilizesenal function in patientsith crescentic/proliferative
gA nephropathy. Serumreatinine was averaged forll 20 patients at study entry,t peak levels, and afterean of 28 months of follow
p (6–60 months). Serum Crignificantly (P < 0.01) in-reased during the coursef therapy from a baseline of.70 mg/dL to 2.64 mg/dLnd returning to baseline
evels by 6 months. After aean of 28 months of follow
p, serum Cr was not signif-cantly different than base-ine levels.
atients. Serum complement levels were depressed a
n patient no. 5 and normal in the remaining 19atients. All patients were tested for C-ANCA and-ANCA positivity at the time of enrollment. Aingle patient tested positive for P-ANCA antibod-es, but none of the 20 patients were positive for-ANCA.The mean serum creatinine before treatment was
.70 � 0.24 mg/dL, rising significantly during theourse of induction therapy to a peak value of.64 � 0.32 mg/dL (P � 0.01 vs. baseline) (Fig.). After 6 months of treatment with solumedrolnd intravenous cyclophosphamide, the mean se-um creatinine fell from a peak of 2.64 � 0.32 to.63 � 0.10 mg/dL. After a mean of 28 months ofollow up, the mean serum creatinine rose to.77 � 0.32 mg/dL. At the time of the initialiopsy, the mean proteinuria was in the nephroticange (3.78 � 0.54 g/24 hours) and reached aaximum value of 4.93 � 0.71 g/24 hours during
he first 6 months of therapy. At the end of 6onths, proteinuria decreased significantly from a
eak of 4.93 � 0.71 g/ 24 hours (P � 0.01 vs.aseline) to 1.38 � 0.37 g/24 hours. After 28onths follow up, proteinuria was further reduced
o 1.15 � 0.43 g/24 hours (Fig. 2).All patients in the treatment group underwent a
epeat biopsy at 6 months to determine (1) theffectiveness of combined corticosteroids and cy-lophosphamide in reducing histologic activity,nd (2) to delay the progression of chronicity. Weound that pulse solumedrol and intravenous cy-lophosphamide significantly reduced the numberf crescents and degree of endocapillary prolifer-
tion without significantly increasing chronicity.
Shgcagd
woitcKt
Nhbsbts
TUMLIN AND HENNIGAR260
tatistical analysis revealed a significant drop inistologic activity in the post- versus pretreatmentroup (P � 0.004) and not significant difference inhronicity (Fig. 3). The level of histologic activitynd chronicity in the initial biopsies of treatmentroup and historical controls were significantlyifferent (Fig 3). Activity in follow-up biopsies
Fig 3. Steroids and cyclophosphamide reduces gloIH SLE histologic activity/chronicity index was appistorical controls. There were no significant differeetween the two groups. After 6 months of cyclophospignificantly lower than pretreatment levels (P < 0.00etween baseline levels in the treatment group orreatment group, it did not change significantly after
tandard error of means.ere decreased in all of the treated patients exceptne (patient no. 5) and fell to one-half or more ofts original value in 50% of patients. To determinehe efficacy of corticosteroids and intravenous cy-lophosphamide on the incidence of ESRD, aaplan-Meier survival plot was calculated for both
he treatment group and historical controls. Figure
Fig 2. Steroids and cy-clophosphamide reducesproteinuria in patients withcrescentic/proliferative IgAnephropathy. At study entry,50% of treated patients hadnephrotic-range proteinuriawith a mean proteinuria of3.78 g/24 hours. Proteinuriasignificantly (P < 0.01) in-creased from 3.78 to 4.93 g/24 hours but was signifi-cantly (P < 0.01) lower thanbaseline levels after 6months of therapy. After amean of 28 months of followup, proteinuria was reducedfurther to a mean of 1.15g/24 hours (P < 0.01 vs.baseline).
r activity and minimizes cortical scarring. A modifiedbaseline renal biopsies in the treatment group and
in the initial average activity and chronicity scorese, the mean activity score in the treatment group wasan chronicity scores were not significantly differente levels among the historical controls, and in the
months of therapy. Values are reported as means �
merulalied tonceshamid4). Mebaselinthe 6
4ortsrvwaFli5ACTplbssaascupipnbgtw
ramppdoitmbIetpoDmrtmcifmmapptis
crImsmc3t9htc0nfm
CRESCENTIC IgA NEPHROPATHY: CLINICAL COURSE AND TREATMENT 261
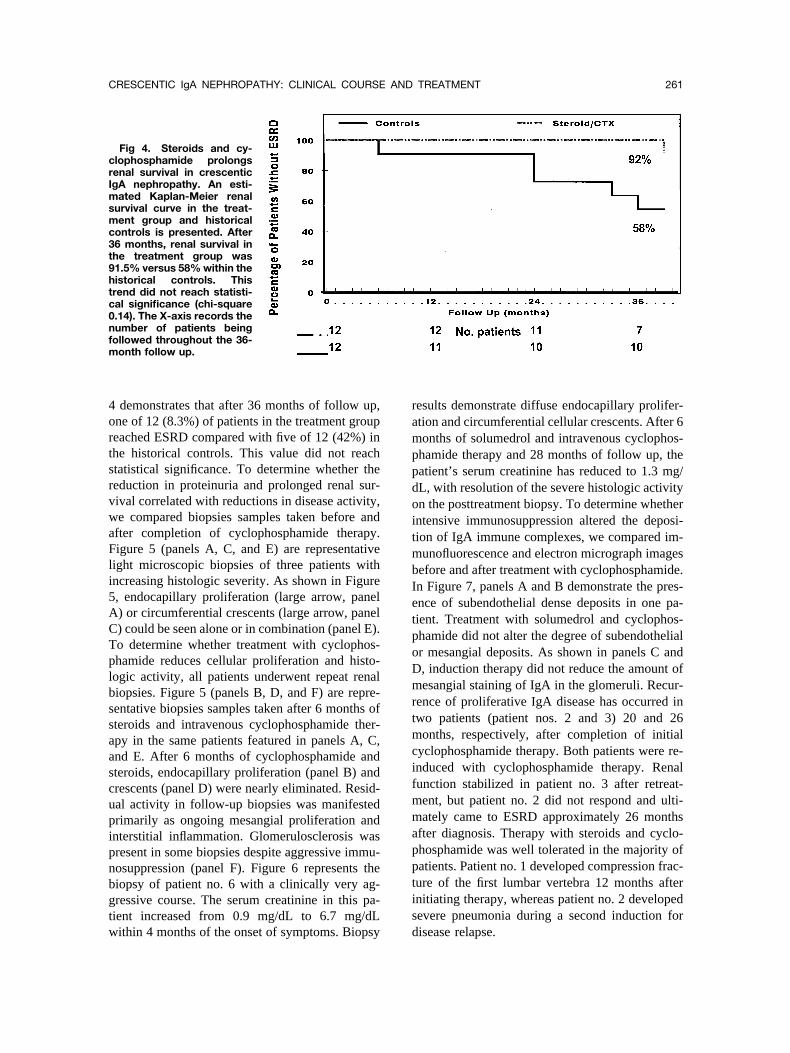
demonstrates that after 36 months of follow up,ne of 12 (8.3%) of patients in the treatment groupeached ESRD compared with five of 12 (42%) inhe historical controls. This value did not reachtatistical significance. To determine whether theeduction in proteinuria and prolonged renal sur-ival correlated with reductions in disease activity,e compared biopsies samples taken before and
fter completion of cyclophosphamide therapy.igure 5 (panels A, C, and E) are representative
ight microscopic biopsies of three patients withncreasing histologic severity. As shown in Figure, endocapillary proliferation (large arrow, panel) or circumferential crescents (large arrow, panel) could be seen alone or in combination (panel E).o determine whether treatment with cyclophos-hamide reduces cellular proliferation and histo-ogic activity, all patients underwent repeat renaliopsies. Figure 5 (panels B, D, and F) are repre-entative biopsies samples taken after 6 months ofteroids and intravenous cyclophosphamide ther-py in the same patients featured in panels A, C,nd E. After 6 months of cyclophosphamide andteroids, endocapillary proliferation (panel B) andrescents (panel D) were nearly eliminated. Resid-al activity in follow-up biopsies was manifestedrimarily as ongoing mesangial proliferation andnterstitial inflammation. Glomerulosclerosis wasresent in some biopsies despite aggressive immu-osuppression (panel F). Figure 6 represents theiopsy of patient no. 6 with a clinically very ag-ressive course. The serum creatinine in this pa-ient increased from 0.9 mg/dL to 6.7 mg/dL
Fig 4. Steroids and cy-lophosphamide prolongsenal survival in crescenticgA nephropathy. An esti-
ated Kaplan-Meier renalurvival curve in the treat-ent group and historical
ontrols is presented. After6 months, renal survival inhe treatment group was1.5% versus 58% within theistorical controls. Thisrend did not reach statisti-al significance (chi-square.14). The X-axis records theumber of patients beingollowed throughout the 36-
onth follow up.
ithin 4 months of the onset of symptoms. Biopsy d
esults demonstrate diffuse endocapillary prolifer-tion and circumferential cellular crescents. After 6onths of solumedrol and intravenous cyclophos-
hamide therapy and 28 months of follow up, theatient’s serum creatinine has reduced to 1.3 mg/L, with resolution of the severe histologic activityn the posttreatment biopsy. To determine whetherntensive immunosuppression altered the deposi-ion of IgA immune complexes, we compared im-unofluorescence and electron micrograph images
efore and after treatment with cyclophosphamide.n Figure 7, panels A and B demonstrate the pres-nce of subendothelial dense deposits in one pa-ient. Treatment with solumedrol and cyclophos-hamide did not alter the degree of subendothelialr mesangial deposits. As shown in panels C and, induction therapy did not reduce the amount ofesangial staining of IgA in the glomeruli. Recur-
ence of proliferative IgA disease has occurred inwo patients (patient nos. 2 and 3) 20 and 26onths, respectively, after completion of initial
yclophosphamide therapy. Both patients were re-nduced with cyclophosphamide therapy. Renalunction stabilized in patient no. 3 after retreat-ent, but patient no. 2 did not respond and ulti-ately came to ESRD approximately 26 months
fter diagnosis. Therapy with steroids and cyclo-hosphamide was well tolerated in the majority ofatients. Patient no. 1 developed compression frac-ure of the first lumbar vertebra 12 months afternitiating therapy, whereas patient no. 2 developedevere pneumonia during a second induction for
isease relapse.
CN
iopeciaulnwrw
ssimdpwpnsctdmwh
rsatcEm�gpa
TUMLIN AND HENNIGAR262
DISCUSSION
linical Presentation of Crescentic IgAephropathy
The question of whether patients with histolog-cally aggressive forms of IgA nephropathy dem-nstrate clinical features consistent with a rapidlyrogressive glomerulonephritis is unknown. How-ver, several investigators have reported an in-reased incidence of hypertension and proteinurian patients with crescentic forms of IgA nephrop-thy.4-8,10-12 For example, Wistam-Attorps et al.sed 51 Cr-EDTA clearance to measure glomeru-ar filtration rate (GFR) in 54 patients with IgAephropathy and demonstrated that in patients withorsening proteinuria, GFR was proportionately
educed. As noted in other trials,7,13 patients with
Fig 5. Histologic response to intravenous cyclophoesentative lesions of crescentic/proliferative IgA neteroids and intravenous cyclophosphamide are shorrow) is superimposed on mesangial hypercellularityreatment (hematoxylin and eosin [H&E] stain, �400rescents and endocapillary proliferation are absent farly extracapillary proliferation is manifested as incental endocapillary proliferation (small arrows) in pat400]. D depicts the posttreatment biopsy results in wlomeruli (PAS, �400). (E and F) A fulminant cellular crresent in patient no. 12 before treatment (PAS, �400bsence of extra- and endocapillary proliferative lesio
orsening glomerulosclerosis or interstitial fibro- t
is presented with higher levels of proteinuria andelective loss of IgG immunoglobulins.10 Interest-ngly, although mesangial matrix expansion andesangial cell proliferation correlated with re-
uced GFR, these features did not correlate withroteinuria or other clinical parameters associatedith disease progression.10 In a review of 112atients, Boyce et al. divided patients with IgAephropathy into three different classes based onpecific histopathologic criteria and attempted toorrelate histologic severity with clinical presenta-ion and the risk for ESRD. Patients whose biopsyemonstrated only IgA deposition or expansion ofesangial matrix was subdivided into class I,hereas patients with focal or diffuse mesangialypercellularity were grouped into class II. Pa-
ide in crescentic/proliferative IgA nephropathy. Rep-athy before and after treatment with 6 months ofand B) Segmental endocapillary proliferation (largeatrix expansion (small arrows) in patient no. 4 beforeposttreatment biopsy is shown in panel B where
lomeruli (Periodic acid-Schiff [PAS], �400). (C and D)cellular crescent (large arrow) accompanied by seg-. 1 (Jones’ methenamine silver with PAS counterstain,xtra- and endocapillary proliferation are absent from(arrow) and acute necrotizing glomerulonephritis areosttreatment biopsy is shown in panel F. There is an
h scattered with obsolete glomeruli (PAS, �200).
sphamphrop
wn. (Aand m). Therom gipientient nohich e
escent). The pns wit
ients in class III had more aggressive lesions,

itpbawwptqa[osnhiaMetsci(ta
htrprr
CH
pfrD3autowwuqrff
rspma
CRESCENTIC IgA NEPHROPATHY: CLINICAL COURSE AND TREATMENT 263
ncluding focal or diffuse endocapillary prolifera-ion with the presence of crescents.13 In contrast torevious studies, Boyce et al. found no correlationetween the presence of the nephrotic syndromend worsening histopathology. However, patientsith class III changes or the presence of crescentsere more likely to be hypertensive and torogress to ESRD. Welch et al. reported that pa-ients with proliferative IgA nephropathy were fre-uently hypertensive at the time of biopsy, whereasccelerated hypertension (mean arterial pressureMAP] �150) was the presenting symptom in 20%f patients with IgA nephropathy.5 In a similartudy, Subias et al. examined 66 patients with IgAephropathy and noted that 24 of 66 (36%) wereypertensive (MAP �114 mm Hg) at the time ofnitial presentation, whereas 15% had malignant orccelerated hypertension (MAP �163 mm Hg).oreover, Subias et al. noted that crescents or
ndocapillary proliferation were present in 70% ofhe patients presenting with accelerated hyperten-ion.6 We studied 20 patients with 10% cellularrescents with or without the presence of endocap-llary proliferation and found that hypertensionMAP �107) was present in 50% of patients at theime of biopsy. Although none of our patients had
Fig 6. Histologic response to intravenous cyclophoepresentative photomicrograph of patient no. 6 withecondary to IgA nephropathy (Serum Cr 0.9–6.7 mroliferation and circumferential cellular crescents. (Bonths of solumedrol and intravenous cyclophospham
nd endocapillary proliferation. Mild increase in inters
ccelerated hypertension, nonnephrotic (�1.0 g/24 e
ours) and nephrotic (�3.0 g/24 hours) range pro-einuria were present in 100% and 50% of patients,espectively. We found no correlation between theresence of nephrotic range proteinuria and theesponse to therapy or development of progressiveenal disease.14
rescentic IgA Nephropathy: Prevalence, Naturalistory, and Risk for End-Stage Renal Disease
Early reports of the natural history of IgA ne-hropathy demonstrated an overall benign courseor IgA nephropathy with only 10% of patientseaching ESRD within 10 years.11 More recently,’Amico et al. examined the renal survival rates in620 patients compiled from 18 different studiesnd found an average of 19% ESRD after a followp of 10 years.15 Previous attempts to determinehe prevalence of proliferative or crescentic formsf IgA nephropathy have been slowed by the un-illingness of some clinicians to biopsy patientsith suspected IgA nephropathy and the lack of aniform system of nomenclature. As a conse-uence, the prevalence in previously reported se-ies varies from 1.5% to 55%.7,12 The explanationor the broad range in the prevalence of crescenticorms of IgA is unknown but could reflect differ-
ide in crescentic/proliferative IgA nephropathy. (A) Aical course of rapidly progressive glomerulonephritisover 4 months). Arrows show diffuse endocapillaryresentative photomicrograph of patient no. 6 after 6
reatment resulted in complete resolution of crescentscarring and sclerotic glomerular lesions were noted.
sphama cling/dL) A repide. Ttitial s
nces in ethnic groups or deficiencies in tissue

ptusbiflnnetscnasnt
pssdvpwpcgrsrwsttr
Tatid
TUMLIN AND HENNIGAR264
rocessing. For example, Shouno et al. found thathe presence of proliferative lesions within glomer-lar capillaries was underreported because of in-ufficient number of tissue sections. When serialiopsy sections are increased from 20 to 100, thencidence of endocapillary proliferation increasedrom 7% to 30%.16 The significance of these pro-iferative lesions are unknown, but an increasingumber of authors suggest that proliferative IgAephropathy should be viewed as a different dis-ase with therapies directed at the underlying his-ology. For example, Nicholls et al. reported a caseeries of three patients with an average of 22%rescents on initial biopsy (range, 4–50%) andoted that all patients reached ESRD within anverage of 27 months of initial presentation.4 In aimilar prospective study of 80 children with IgAephropathy, Hogg et al. noted that 12 of 80 pa-
Fig 7. Electron microscopy and immunofluorescenwo representative photomicrographs of patient no. 5nd after 6 months of intravenous cyclophosphamidehelial dense deposits. (C and D) Two representative intense mesangial staining with IgA. Six months of inteposition in patient no. 5.
ients (15%) reached ESRD within 4 years. Of the (
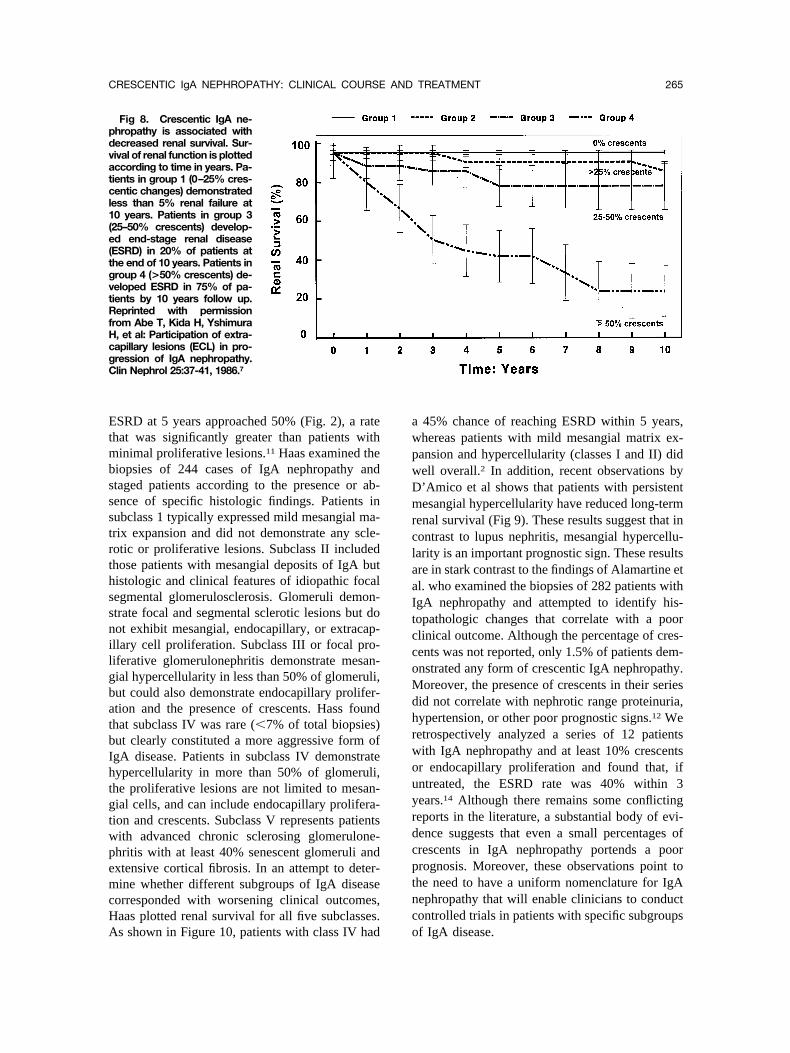
atients reaching ESRD, light microscopy demon-trated that 42% had crescents at the time of pre-entation, whereas 93% had evidence of focal oriffuse endocapillary proliferation.17 Abe et al. re-iewed the biopsies of 205 patients with IgA ne-hropathy and found that over 55% of patientsere found to have 25% or more crescents.7 Whenatients were stratified according to percentage ofrescents and histologic severity, those withreater than 50% crescents demonstrated moreapid decline of renal function and reduced overallurvival (Fig. 8).7 D’Amico et al. found a similareduction in renal survival among IgA patientsith proliferative glomerular lesions. In a large
tudy of 365 patients, D’Amico et al. semiquanti-atively graded endocapillary proliferation from 0o �3 severity and correlated these findings withenal survival. Among patients with diffuse
sponse to intravenous cyclophosphamide. (A and B)nstrating large subendothelial dense deposits beforese treatment did not alter the presence of subendo-ofluorescence images of patient no. 5 demonstratingus cyclophosphamide did not alter the degree of IgA
ce redemo
. Intenmmunraveno
�50%) endocapillary proliferation, the rate of
EtmbssstrthssnilgbatbIhtgtwpemcHA
awpwDmrclaaItccoMdhrwouyrdcptnc
pdvatcl1(e(tgvtRfHcgC
CRESCENTIC IgA NEPHROPATHY: CLINICAL COURSE AND TREATMENT 265
SRD at 5 years approached 50% (Fig. 2), a ratehat was significantly greater than patients withinimal proliferative lesions.11 Haas examined the
iopsies of 244 cases of IgA nephropathy andtaged patients according to the presence or ab-ence of specific histologic findings. Patients inubclass 1 typically expressed mild mesangial ma-rix expansion and did not demonstrate any scle-otic or proliferative lesions. Subclass II includedhose patients with mesangial deposits of IgA butistologic and clinical features of idiopathic focalegmental glomerulosclerosis. Glomeruli demon-trate focal and segmental sclerotic lesions but doot exhibit mesangial, endocapillary, or extracap-llary cell proliferation. Subclass III or focal pro-iferative glomerulonephritis demonstrate mesan-ial hypercellularity in less than 50% of glomeruli,ut could also demonstrate endocapillary prolifer-tion and the presence of crescents. Hass foundhat subclass IV was rare (�7% of total biopsies)ut clearly constituted a more aggressive form ofgA disease. Patients in subclass IV demonstrateypercellularity in more than 50% of glomeruli,he proliferative lesions are not limited to mesan-ial cells, and can include endocapillary prolifera-ion and crescents. Subclass V represents patientsith advanced chronic sclerosing glomerulone-hritis with at least 40% senescent glomeruli andxtensive cortical fibrosis. In an attempt to deter-ine whether different subgroups of IgA disease
orresponded with worsening clinical outcomes,aas plotted renal survival for all five subclasses.
Fig 8. Crescentic IgA ne-hropathy is associated withecreased renal survival. Sur-ival of renal function is plottedccording to time in years. Pa-ients in group 1 (0–25% cres-entic changes) demonstrated
ess than 5% renal failure at0 years. Patients in group 325–50% crescents) develop-d end-stage renal diseaseESRD) in 20% of patients athe end of 10 years. Patients inroup 4 (>50% crescents) de-eloped ESRD in 75% of pa-ients by 10 years follow up.eprinted with permission
rom Abe T, Kida H, Yshimura, et al: Participation of extra-apillary lesions (ECL) in pro-ression of IgA nephropathy.lin Nephrol 25:37-41, 1986.7
s shown in Figure 10, patients with class IV had o
45% chance of reaching ESRD within 5 years,hereas patients with mild mesangial matrix ex-ansion and hypercellularity (classes I and II) didell overall.2 In addition, recent observations by’Amico et al shows that patients with persistentesangial hypercellularity have reduced long-term
enal survival (Fig 9). These results suggest that inontrast to lupus nephritis, mesangial hypercellu-arity is an important prognostic sign. These resultsre in stark contrast to the findings of Alamartine etl. who examined the biopsies of 282 patients withgA nephropathy and attempted to identify his-opathologic changes that correlate with a poorlinical outcome. Although the percentage of cres-ents was not reported, only 1.5% of patients dem-nstrated any form of crescentic IgA nephropathy.oreover, the presence of crescents in their series
id not correlate with nephrotic range proteinuria,ypertension, or other poor prognostic signs.12 Weetrospectively analyzed a series of 12 patientsith IgA nephropathy and at least 10% crescentsr endocapillary proliferation and found that, ifntreated, the ESRD rate was 40% within 3ears.14 Although there remains some conflictingeports in the literature, a substantial body of evi-ence suggests that even a small percentages ofrescents in IgA nephropathy portends a poorrognosis. Moreover, these observations point tohe need to have a uniform nomenclature for IgAephropathy that will enable clinicians to conductontrolled trials in patients with specific subgroups
f IgA disease.
CH
pdthuiIusffatpmsmfitmIdtpoois
bceaacetptgarspc
amlIalav6ctbp
TUMLIN AND HENNIGAR266
rescentic IgA Nephropathy: Role of Steroidormones and Cyclophosphamide
The lack of uniform definitions for specific sub-opulations of IgA nephropathy has slowed theevelopment of effective treatments for prolifera-ive forms of IgA nephropathy. Because of theeterogeneity of IgA nephropathy, early studiessing steroid hormone therapy have given conflict-ng results. In a prospective trial of 86 patients withgA nephropathy and moderate to severe protein-ria, Pozzi et al. demonstrated that pulse cortico-teroids for 6 months slowed the loss of renalunction compared with control subjects matchedor clinical severity.18 A recent analysis of trialsssessing the efficacy of glucocorticoids in thereatment of IgA nephropathy concluded that foratients with preserved renal function (CrCl �70L/min), prolonged therapy (�2 years) effectively
lows the loss of renal function.19 However, in theajority of these studies, patients were not classi-ed by pathologic changes or histologic severity,
hus the efficacy of glucocorticoids in patients withore severe pathologic changes was not assessed.
n an attempt to address this question, Lai et al.ivided 34 patients with IgA nephropathy intohree groups based on the degree of mesangialroliferation, glomerulosclerosis, and percentagef crescents and prospectively studied the efficacyf short-term steroid therapy. In patients random-zed to oral prednisone, 4 months of treatment
tabilized renal function and reduced proteinuria tut only in those patients with greater than 20%rescents on initial biopsy.20 Recently, Hotta et al.xamined the effects of pulse methylprednisolonend tonsillectomy in 35 patients with hematuriand known IgA nephropathy. Although the per-entage was not recorded, over 91% of patients hadvidence of crescents on initial biopsy. To assesshe response to steroid hormone therapy, all 35atients underwent repeat biopsy after 1 year ofherapy. Interestingly, mesangial cell proliferation,lomerular sclerosis, and crescent formation werell significantly reduced on repeat biopsy.21 Theseecent data supports the finding of Pozzi et al. anduggest that even in the face of epithelial cellroliferation, steroid therapy can have a positivelinical and histologic result.
Several small trials have studied whether theddition of oral cyclophosphamide to steroid treat-ent improves renal survival. For example, Bal-
ardie et al. treated 38 patients with progressivegA nephropathy with a combination of steroidsnd oral cyclophosphamide for 34 months fol-owed by 2 additional years of prednisone andzathioprine. Kaplan-Meier analysis of renal sur-ival showed a 72% 5-year survival compared with% for matched controls.22 Although histologichanges, including mesangial hypercellularity, in-erstitial fibrosis, and tubular atrophy were similaretween groups, patients were not controlled forresence of crescents or endocapillary prolifera-
22
Fig 9. Differential renalsurvival among patients withincreasing mesangial cell pro-liferation. Kaplan-Meier sur-vival curves of renal survivalamong patients with worsen-ing mesangial cell prolifera-tion. Renal survival among pa-tients with minimal mesangialcell hypercellularity was 100%after 12 years follow up. Re-nal survival among patientswith focal mesangial hyper-cellularity (<50%) decreased70%, whereas patients withdiffuse (>50%) mesangial hy-percellularity was reduced to50% after 12 years follow up.Reprinted with permissionfrom D’Amico G: The com-monest glomerulonephritis inthe world: IgA nephropathy. QJ Med 64:709-727,2001.24
ion. Ferrario et al. treated six patients with focal

gcdts
ppciatdLomi
hbiatlsgbfHcUoecm
foMtfar5rymt1drpm8yscNlK©F
APP
PPSS
CRESCENTIC IgA NEPHROPATHY: CLINICAL COURSE AND TREATMENT 267
lomerular necrosis and 20% or more cellular cres-ents with steroids and oral cyclophosphamide andemonstrated that when compared with eight his-orical controls, 6 months of combination therapyignificantly prolonged renal survival.8
We examined the effect of intense immunosup-ression in 20 patients with progressive IgA ne-hropathy and histologic evidence of 10% or moreellular crescents. In our hands, prednisone andntravenous cyclophosphamide reduced proteinuriand stabilized renal function after 6 months ofherapy. Both proteinuria and serum creatinine re-uced to near-baseline levels within 6 months.ong-term follow up in the treatment group dem-nstrated that proteinuria and renal function re-ained stable over an average of 36 months. To
nvestigate the response to treatment of glomerular
Fig 10. Renal survival asunction of Haas classificationf IgA nephropathy. Kaplan-eier renal survival was plot-
ed against time for each of theour IgA subgroups. Class Ind II demonstrated excellentenal survival with less than% progressing to end-stageenal disease (ESRD) over 10ears. Class III demonstrated aore rapid loss of renal func-
ion with a 35% ESRD rate at0 years. Classes IV and Vemonstrate very rapid loss ofenal function with over 40%atients reaching ESRD by 36onths with approximately
0% achieving ESRD by 10ears. Reprinted with permis-ion from Haas M: Histologi-al subclassification of IgAephropathy: A clinicopatho-
ogic study of 244 cases. Am Jidney Dis 29:829-842, 1997.2
1997 by National Kidneyoundation, Inc.
Table 2. Emory University Protocol:
Clinical Data
ge (years)ercent Maleercent hypertension (�140/90 mm Hg)Percent accelerated (�210/130 mm Hg)
ercent proteinuria (�1.0 gm/24 hrs)ercent nephrotic (�3.0 g/24 hrs)erum creatinine (mean, mg/dL)erum albumin g/dLMean � standard error mean
istopathology, 17 of 20 patients underwent repeatiopsy. The percentage of crescents and endocap-llary proliferation was compared between the pre-nd postbiopsies after induction therapy. Duringhe preliminary analysis of our clinical and histo-ogic data, we determined that early nomenclatureystems designed to identify specific IgA sub-roups were not sensitive enough to discriminateetween our treatment and control groups. There-ore, we applied a modified version of the Worldealth Organization SLE disease activity and
hronicity indices to our population of patients.sing this system, we demonstrated that 6 monthsf steroids and intravenous cyclophosphamideliminated all active cellular crescents and endo-apillary proliferation. In addition, intensive im-unosuppression using intravenous cyclophosph-
entic Proliferative IgA Nephropathy
ontrol (N � 12) Steroids/CTX (N � 20)
43 4464% (7/12) 40% (8/20)41% (5/12) 85% (17/20)40% (2/5) 075% (9/12) 100% (20/20)42% (5/12) 55% (11/20)
1.85 1.70
3.5 � 0.2 3.2 � 0.2
Cresc
C

aaNnbtsscpmosanpshht(wtreacrmfsiahs
ip
t2
m
l
I
MN
Hg
l
Gs
PC
i5
FeK
CA
lmr
aK
Yas
SaG
I8
ME7
It
Rs
oJ
pc1
w
TUMLIN AND HENNIGAR268
mide minimized the amount of cortical scarringnd tubular dropout in the majority of patients.umerous studies have documented the poor prog-osis with crescentic forms of IgA nephropathy,ut few had used follow-up biopsies to prospec-ively assess a response to treatment. In a similartudy, McIntyre et al. treated nine patients withevere crescentic IgA nephropathy (cellular cres-ents involving 20% to 70% of glomeruli) withrednisone and oral cyclophosphamide for up to 6onths followed by 2 years with prednisone and
ral azathioprine. Long-term follow up demon-trated that steroids in conjunction with alkylatinggents reduced proteinuria and improved creati-ine clearance. On repeat biopsy, three of the eightatients showed an increased in glomerulosclero-is.23 In our series, we compared the clinical andistologic response of the treated patients with 12istorical controls receiving conventional medicalherapy but no immunosuppression. Five of 1242%) patients in this control group reached ESRDithin 36 months compared with only 8.5% among
he treatment group. The recent data of Hotta et al.aises the question of whether treatment of prolif-rative IgA nephropathy with steroid hormoneslone is as effective as therapy combined withyclophosphamide. Moreover, these observationsaise the question of whether attempts should beade to create a unified histologic nomenclature
or subgroups of IgA nephropathy that parallels theystem in widespread use in SLE. Ultimately, annternational application of such a system wouldllow for more precise definition of the naturalistory of specific subgroups and facilitate the de-ign of clinical therapies to treat these patients.
REFERENCES
1. Kobayashi Y, Fujii K, Hiki Y, Tateno S: Steroid therapyn IgA nephropathy: a prospective pilot study in moderateroteinuric cases. Q J Med 61:935-943, 19862. Haas M: Histological subclassification of IgA Nephropa-
hy: A clinicopathologic study of 244 cases. Am J Kidney Dis9:829-842, 19973. Floege J, Feehally J: IgA nephropathy: Recent develop-ents. J Am Soc Nephrol 11:2395-2403, 20004. Nicholls K, Walker R, Dowling J, Kincaid-Smith P: “Ma-
ignant” IgA nephropathy. Am J Kidney Dis 5:42-46, 19855. Welch TR, McAdams AJ, Berry A: Rapidly progressing
gA nephropathy. Am J Dis Child 142:789-793, 19886. Subias R, Botey A, Darnell A, Montoliu J, Revert L:alignant or accelerated hypertension in IgA nephropathy. Clinephrol 27:1-7, 1987
7. Abe T, Kida H, Yshimura H, Koshino Y, Tomosugi N,attori N: Participation of extracapillary lesions (ECL) in pro-ression of IgA nephropathy. Clin Nephrol 25:37-41, 19868. Ferrario F, Napodano P, Rastaldi M, D’Amico G: Capil-
aritis in IgA nephropathy. Contrib Nephrol 111:8-12, 19959. D’Amico G, Napodano P, Ferrario F, Rastaldi MP, Arrigo
: Idiopathic IgA nephropathy with segmental necrotizing le-ions of the capillary wall. Kidney Int 59:682-692, 2001
10. Widstam-Attorps U, Berg U, Bohman S, Lefvert A:roteinuria and renal function in relation to renal morphology.lin Nephrol 38:245-253, 199211. D’Amico G, Minetti L, Ponticelli C, et al: Prognostic
ndicators in idiopathic IgA mesangial nephropathy. Q J Med9:363-378, 198612. Alamartine E, Sabatier J, Guerin C, Baerliet J, Berthoux
: Prognostic factors in mesangial IgA glomerulonephritis: Anxtensive study with univariate and multivariate analyses. Am Jidney Dis 18:12-19, 199113. Boyce NW, Holdsworth SR, Thomson NM, Atkins RC:
linicopathological associations in mesangial IgA nephropathy.m J Nephrol 6:246-252, 198614. Tumlin JA, Lohavichan V, Hennigar R: Crescentic pro-
iferative IgA nephropathy: Clinical and histologic response toethyl prednisolone and intravenous cyclophosphamide. Neph-
ol Dial Transplant 18:1321-1328, 200315. D’Amico G: Natural history of idiopathic IgA nephrop-
thy: Role of clinical and histological prognostic factors. Am Jidney Dis 36:227-237, 200116. Shouno Y, Shimokama T, Sakemi T, Harada A,
amaguchi M, Wantanabe T: Segmental glomerular necrosis asn active index of IgA nephropathy: A study with 100 serialections of 128 cases. Acta Pathol Jpn 43:723-729, 1993
17. Hogg RJ, Silva FG, Wyatt RJ, Reisch JS, Argyle JC,avino DA: Prognostic indicators in children with IgA nephrop-thy: Report of the Southwest Pediatric Nephrology Studyroup. Pediatr Nephrol 8:15-20, 199418. Pozzi C, Bolasco P, Fogazzi G, et al: Corticosteroids in
gA nephropathy: A randomized controlled trial. Lancet 353:83-887, 199919. Waldo FB, Wyatt RJ, Kelly DR, Herrera GA, BenfiledR, Kohaut EC: Treatment of IgA nephropathy in children:
fficacy of alternate day oral prednisone. Pediatr Nephrol:529-532, 199320. Lai K, Lai F, Ho C, Chan W: Corticosteroid therapy in
gA nephropathy with nephrotic syndrome: A long-term con-rolled trial. Clin Nephrol 26:174-180, 1986
21. Hotta O, Furuta T, Chiba S, Tomioka S, Toguma Y:egression of IgA. Regression of IgA nephropathy: a biopsy
tudy. Am J Kidney Dis 39:493-502, 200222. Ballardie FW, Roberts ISD: Controlled prospective trial
f prednisolone and cytotoxics in progressive IgA nephropathy.Am Soc Nephrol 13:142-148, 200223. McIntyre CW, Fluck RJ, Lambie SH: Steroid and cyclo-
hosphamide therapy for IgA nephropathy associated with cres-entic change: An effective treatment. Clin Nephrol 56:193-98, 200124. D’Amico G: The commonest glomerulonephritis in the
orld: IgA nephropathy. Q J Med 64:709-727, 2001

















