Embed Size (px)
Citation preview

Utsislchfwssmfbtffta
L
S
A
0©
S
Evaluation of the Kidney Stone Patient
John R. Asplin, MD
Summary: Kidney stones are one of the most common chronic disorders in industrializedcountries. In patients with kidney stones, the goal of medical therapy is to prevent theformation of new kidney stones and to reduce growth of existing stones. The evaluation ofthe patient with kidney stones should identify dietary, environmental, and genetic factors thatcontribute to stone risk. Radiologic studies are required to identify the stone burden at thetime of the initial evaluation and to follow up the patient over time to monitor success of thetreatment program. For patients with a single stone an abbreviated laboratory evaluation toidentify systemic disorders usually is sufficient. For patients with multiple kidney stones24-hour urine chemistries need to be measured to identify abnormalities that predispose tokidney stones, which guides dietary and pharmacologic therapy to prevent future stoneevents.Semin Nephrol 28:99-110 © 2008 Elsevier Inc. All rights reserved.Keywords: Nephrolithiasis, hypercalciuria, hyperoxaluria, hypocitraturia
st
H
Wfdscircmto
oicsrreotl(s
rolithiasis is one of the most commondisorders of the urinary tract. Approxi-mately 12% of men and 6% of women in
he United States will have at least one kidneytone during their lifetime.1 In fact, recent stud-es have shown that the prevalence of kidneytones in industrialized societies is increasing,ikely because of dietary changes and the in-reasing rate of obesity. Once an initial stoneas formed, more than 50% of patients willorm additional stones over the next 10 years,ith some patients forming multiple kidney
tones.2,3 The medical evaluation of the kidneytone patient is focused on identifying abnor-alities of urine composition that cause stone
ormation. Urine composition can be affectedy systemic disease, dietary habits, environmen-al factors, and genetic traits. Once urine riskactors have been identified, the clinician canormulate a selective therapeutic plan aimed athat patient’s specific metabolic problem. Thisrticle reviews the evaluation of the kidney
itholink Corporation, Chicago, IL, and the Department of Medicine, Univer-sity of Chicago Pritzker School of Medicine, Chicago, IL.
upported in part by National Institutes of Health grants R44 DK071375-01and R43 DK078409-01.
ddress reprint requests to John R. Asplin, MD, Medical Director, LitholinkCorporation, 2250 W Campbell Park Dr, Chicago, IL 60612. E-mail:[email protected]
270-9295/08/$ - see front matter
p2008 Elsevier Inc. All rights reserved. doi:10.1016/j.semnephrol.2008.01.001eminars in Nephrology, Vol 28, No 2, March 2008, pp 99-11
tone patient to prevent recurrent stone forma-ion.
ISTORY
hen obtaining the medical history, it is help-ul to quantify the number of stones and theuration of stone disease. Knowing the rate oftone formation (stones/year) will allow clini-ians to gauge the success of their therapeuticnterventions. In addition, the stone formationate will guide the aggressiveness of the medi-al intervention; a patient who passes stonesonthly likely will require more aggressive
herapy than a patient who is forming stonesnce every few years.
The medical history also should identifyther comorbid conditions such as urinary tract
nfection, bowel disease, and diseases that alteralcium homeostasis, all of which can affecttone risk. Urinary tract infection may be theesult of stone disease, particularly from recur-ent instrumentation of the urinary tract. How-ver, recurrent infection also can be the causef stones. If a patient has a urinary tract infec-ion with Proteus or Klebsiella species, whichikely possess the enzyme urease, then struvitemagnesium ammonium phosphate) kidneytones are likely.4 This is a common problem in
atients requiring chronic indwelling or inter-0 99

mmwaraospwtaCsapcpbfsccl
E
TfiewEsthetbastirpsadabad
aasm
raehwlgw3aitfljltiaromh
D
ActphfgttmddiCqPntdb
100 J.R. Asplin
ittent catheterization. Bowel disease is a com-on contributor to kidney stone formation asell. Chronic diarrhea leads to loss of fluid and
lkali from the gastrointestinal (GI) tract, whichesults in low urine flow rates, hypocitraturia,nd acidic urine; these factors enhance the riskf both calcium oxalate (CaOx) and uric acidtone formation.5 Patients with an ileostomy arearticularly prone to these problems. Patientsho have extensive small-bowel disease or mul-
iple small-bowel resections, leading to fat mal-bsorption, may develop hyperoxaluria andaOx stones.6 Bariatric surgery also has beenhown to cause hyperoxaluria and nephrolithi-sis7 (see the article by Lieske et al in this issue,. 163). Any disorder than can cause hypercal-iuria may lead to nephrolithiasis. Certainly,rimary hyperparathyroidism is well known toe a cause of kidney stone disease, accountingor 2% to 5% of stone formers referred to kidneytone centers.8,9 Other mineral disorders thatause overproduction of calcitriol, such as sar-oid and other granulomatous diseases, canead to hypercalciuria and stone formation.
nvironmental Factors
he major environmental factors to be identi-ed as stone risk factors include heat exposure,mployment, and exercise. Heat exposure is aell-recognized risk factor for stone disease.
pidemiologic data from the United Stateshow a greater incidence of nephrolithiasis inhe Southern states, which of course have theighest mean temperatures.10,11 The southeast-rn United States has the highest stone forma-ion rate, and often is referred to as the “stoneelt,” although it is likely that other factors suchs diet also play a role in stone risk because thetone rates are higher than equally hot areas inhe southwest portion of the United States. Themportance of environment is highlighted in aecent study of stone formation in US militaryersonnel deployed to the hot, arid climate ofouthwest Asia.12 The mean time to a symptom-tic stone event, in 182 previously healthy sol-iers who formed stones, was 93 days afterrrival to the new environment. Stones mayecome symptomatic long after they formed. Inddition to the patient’s current area of resi-
ence, past habitats should be considered in lssessing stone risk. A patient who had lived inhot, dry environment may no longer have the
ame risk for recurrent stones after moving to aore temperate area.A patient’s employment can influence stone
isk owing to effects on insensible water loss orlterations in fluid intake. If the employmentnvironment is hot, then stone risk will beigher. Borghi et al13 investigated the effect ofork environment by determining the preva-
ence of nephrolithiasis for men employed in alass factory in Italy. They found that menorking in the area of the glass furnace were
.5 times more likely to have stones than ange- and weight-matched group of men work-ng for the same company in a climate-con-rolled environment. Employment also can in-uence stone risk by altering fluid intake. Some
obs limit the availability of water, but just asikely an occupation will limit the availability ofoilet facilities, leading patients to reduce liquidntake to keep urine volume low. Leisure timectivities also can play a significant role in stoneisk. Patients who engage in vigorous exerciser any outdoor activity in the summer monthsay dehydrate themselves regularly, leading toighly concentrated urine.14
iet
patient’s diet will greatly influence their urinehemistries and their risk of kidney stones. Al-hough low-calcium diets once were common-lace in the treatment of kidney stones andigh calcium intake was thought to be a riskactor, recent epidemiologic data have sug-ested otherwise. In 3 large prospective cohortrials, Curhan et al15-17 found that subjects withhe highest dietary calcium intake (�1,100g/d) had the lowest rate of forming an inci-
ent kidney stone. The mechanism for the re-uction of kidney stone risk by high calcium
ntake has not been determined definitively.alcium intake can be assessed quickly byuantifying intake of dairy products in the diet.atients who are on a chronic low-calcium dietot only may increase their stone risk, but alsohe risk of osteopenia. Alternatively, excessiveietary calcium can increase kidney stone risky increasing intestinal calcium absorption,
eading to hypercalciuria. A calcium intake of

1p
nt3opavntoppa
tflhgobiWpiwfscj
aTlsiiftprgotwtDf
itiqceptd
F
ArclsH5htptccgpiawwLbmcapaoDectstipiw
Kidney stone patients 101
,000 to 1,200 mg/d seems a reasonable com-romise in kidney stone patients.Oxalate in the urine is derived from endoge-
ous production of oxalate and from absorp-ion of oxalate from foodstuffs. Approximately0% to 50% of urine oxalate is of dietary originn a normal diet.18 Because oxalate is an end-roduct of human metabolism, the net oxalatebsorbed from the intestine must be excretedia the kidney. Urine oxalate can increase sig-ificantly as diet oxalate content increases. Ahorough history of a patient’s intake of high-xalate foods, both frequency and amount, mayrovide important insight into the cause of aatient’s kidney stones. Food oxalate content isvailable from numerous sources.19,20
An estimate of fluid intake should be ob-ained from the patient as well as the types ofuids they consume. Epidemiologic studiesave suggested that some beverages conferreater protection against kidney stones thanthers.21,22 Regular ingestion of coffee, tea,eer, and wine were associated with a lower
ncidence of forming an incident stone.hether specific beverages are beneficial in
reventing recurrent stones is not known. Ofnterest, daily consumption of grapefruit juice
as associated with an increased risk of stoneormation. Although the mechanism of this as-ociation is not known,23 it is prudent to dis-ourage regular consumption of grapefruituice in patients with kidney stones.
Excessive dietary intake of animal proteinnd sodium affects urinary stone risk factors.he increased metabolic acid load from protein
owers urine pH, increasing risk of uric acidtones, and also lowers urine citrate excretion,ncreasing CaOx stone risk.24 Protein loads willncrease urine calcium excretion, a further riskor CaOx stones.25-27 In addition, purine intakeends to correlate with protein intake, so high-rotein diets may lead to hyperuricosuria. Aeasonable goal for protein intake is 1 to 1.2rams of protein per kg body weight. The levelf sodium intake plays a significant role in de-ermining urine calcium excretion, and patientsith hypercalciuria may be more sensitive to
he calciuric effects of high sodium intake.28-30
iet sodium intake often is difficult to quantify
rom history. Patients who add salt to food after at is prepared invariably have excess sodium inheir diet. Easily identified high-sodium foodsnclude canned foods, prepared meats, and fre-uent consumption of restaurant meals. Urinehemistries also can be helpful in assessing di-tary habits of patients, particularly sodium androtein intake, and should be used in conjunc-ion with the history to estimate the impact ofiet on stone disease.
amily History
lthough diet and environment clearly play aole in stone formation, there is a strong geneticomponent as well. Stone formers are moreikely to have first-degree relatives with kidneytones than are non–stone-forming patients.31
ypercalciuria is familial because it is found in0% of first-degree relatives of patients withypercalciuria.32 Although the inheritance pat-ern has similarities to an autosomal-dominantattern, it likely is inherited as a polygenicrait.33 For other stone risk factors, such asitrate and oxalate, inheritance patterns are lesslear. There are a number of uncommon mono-enic disorders that include nephrolithiasis asart of the phenotype. Primary hyperoxaluria is
nherited as an autosomal-recessive disordernd will show a horizontal inheritance patternith siblings being affected but neither parentith disease (see the article by Bobrowski and
angman in this issue, p. 152). Cystinuria maye inherited as a recessive disorder but it alsoay present as autosomal dominant with in-
omplete penetrance (see the article by Mattoond Goldfarb in this issue, p. 181). It usuallyresents within a generation but if it is theutosomal-dominant form, parents or childrenf a proband may have the stone phenotype.istal renal tubular acidosis can be inherited asither autosomal dominant or recessive and in-ludes nephrolithiasis as part of the pheno-ype.34 Finally, a strong family history of kidneytones and renal failure in males within a familyree suggests Dent disease, a disorder character-zed by hypercalciuria, low-molecular-weightroteinuria, and renal disease, which is inher-
ted as an X-linked recessive trait in which theomen in a family are asymptomatic carriers
nd the men have the disease.35

M
Atprcitafdrcslcwhaimsttma
iwlmtrsstbwtt
mdisfbhsrthfpmttvaelimttcsetDcOawpd
102 J.R. Asplin
edications and Supplements
thorough survey of current and past medica-ions, vitamins, and supplements taken by theatient is critical to identify modifiable stoneisks. Medications and supplements can in-rease stone risk by either altering urine chem-stries to promote stones or by crystallizing inhe urinary tract (Table 1). Medications thatlter urine chemistries often affect renal tubularunction. A prime example is carbonic anhy-rase inhibitors, which cause abnormalities inenal acidification and increase the risk of cal-ium stones, particularly calcium phosphatetones. Carbonic anhydrase inhibitors willower urine citrate, increase urine pH, and in-rease urine calcium excretion.36 Topiramate,hich is used to treat epilepsy and migraineeadaches, has significant carbonic anhydrasectivity and has been linked to stone formationn a number of studies.37,38 Vitamin C can be
etabolized to oxalate and therefore has beenuspected to be a risk factor for stone forma-ion. However, there are conflicting reports aso the extent of oxalate formation during vita-in C therapy.39-41 In general, it is wise to limit
Table 1. Medications That CauseNephrolithiasis
Drugs ThatCrystallize
Drugs That CauseMetabolic Stones
Triamterene Calcium supplementsProtease inhibitors Vitamin D supplements
IndinavirAtazinirNelfinavir
AntimicrobialsSulfonamidesQuinolones
GuaifenesinEphedrineAllopurinol
(oxypurinol)
Carbonic anhydraseinhibitor
AcetazolamideTopiramate
LaxativesProbenecidAscorbic acidAlkali
AntacidsMagnesium
trisillicateAluminum
hydroxide
scorbic acid intake to no more than 500 mg/d b
n kidney stone patients. Calcium supplementsill increase urine calcium and one epidemio-
ogic study suggested that calcium supplementsay increase stone risk.16 In addition, a recent
rial of vitamin D and calcium supplements toeduce bone loss and fractures in womenhowed that the women randomized to calciumupplements had higher rates of stone forma-ion.42 It has been postulated that risk will note the same if calcium supplements are takenith meals to slow their absorption and to get
he benefit of reduced oxalate absorption, buthis theory has not been tested rigorously.
Some drugs have low solubility in urine anday form a pure stone composed only of the
rug or its metabolites, or the drug may bencorporated as a component of more routinetones such as CaOx. Protease inhibitors usedor human immunodeficiency virus (HIV) haveeen associated with stone formation.43,44 De-ydration and volume depletion frequentlyeen in HIV patients as a result of chronic diar-hea and fever enhance the risk for crystalliza-ion of these drugs. However, Nadler et al45
ave shown that a significant number of stonesrom HIV patients on indinavir are not com-osed of the drug and likely are related to otheretabolic causes.45 It is important to determine
he composition of stones in patients with HIVo prevent an unnecessary change in antiretro-iral therapy. Over-the-counter preparationslso may lead to stone formation. Both guaifen-sin and ephedrine have been found to crystal-ize and cause kidney stones when taken chron-cally in high doses.46,47 Finally, mention must be
ade of triamterene, a potassium-sparing diuretichat can crystallize in the urinary tract.48,49 It of-en is used as a combination pill with hydro-hlorothiazide (Dyazide, GlaxoSmithKline, Re-earch Triangle Park, NC) and therefore it isasy to overlook in a patient’s list of medica-ions. It also is important to avoid prescribingyazide as a treatment for hypercalciuria be-ause of the risk of triamterene crystallization.ther potassium-sparing drugs, such as amiloride,
re preferred if needed to control potassiumasting from diuretic therapy in a kidney stoneatient. A comprehensive review of drug-in-uced nephrolithiasis was published recently
y Daudon and Jungers.50
R
Maopnsoiwsonhrttusaf
fgoduvtqomacdbsstwwti
tiiegf
Sstmptttam
L
IwNciRargOrmsasew(snbicp(nncametwtycp
Kidney stone patients 103
ADIOLOGY
ost patients will have had a radiologic evalu-tion when presenting with their first episodef renal colic. A helical computerized tomogra-hy (CT) scan of the abdomen and pelvis isow the standard radiologic study for a patientuspected of having renal colic. The advantagesf CT are that it does not require radiocontrast,
t can identify stones smaller than often seenith an abdominal radiograph or ultrasound, all
tones are radio-opaque, and it allows diagnosisf other causes of abdominal pain if stones areot present.51,52 CT has been shown to have aigher sensitivity and specificity in detectingenal stones than abdominal radiograph and ul-rasound.53,54 CT scan is significantly betterhan ultrasound in the detection of stones in thereter. Reduced-dose CT scans have beenhown to be accurate in detecting nephrolithi-sis, but with much lower radiation exposureor the patient.54
If a patient who has passed a stone presentsor a medical evaluation without any radio-raphs having been performed, then some formf kidney imaging needs to be performed toetermine the number of stones present in therinary tract because the distinction of singleersus multiple stones will determine the ex-ent of metabolic evaluation the patient re-uires. CT is the gold standard for the detectionf stones, but cost and radiation exposure mayake radiographs and ultrasound reasonable
lternatives in certain situations.55 Ninety per-ent of stones will be radio-opaque on an ab-ominal radiograph, although small stones maye missed. Ultrasound can detect all types oftones, shown as echogenic images with backhadowing. An advantage of using ultrasound ishat it does not expose the patient to radiation,hich makes it the preferred test in pregnantomen and may make it a useful study in pa-
ients who are expected to require frequentmaging.
In addition to differentiating single versus mul-iple stone formers, the radiologic evaluation ismportant in charting the success of therapeuticnterventions to prevent new stones. Once di-tary or pharmacologic therapy is initiated, theoal of therapy is to prevent new stones from
orming and pre-existing stones from growing. merial radiographs are required to determine iftones are growing, but, more importantly, anyime a patient passes a stone it must be deter-ined if the stone is new or if the patient isassing a pre-existing stone. If the stone is old,hen there may be no reason to alter medicalherapy. This knowledge also must be impartedo the patient, lest they become discouragednd give up on what may be an effective treat-ent regimen.
ABORATORY EVALUATION
n a patient with a single kidney stone, a limitedork-up has been recommended by the lastational Institutes of Health nephrolithiasisonsensus conference.56 The evaluation shouldnclude serum electrolyte levels to evaluate forTA, creatinine level to assess renal function,nd calcium level to screen for hyperparathy-oidism. If a stone has been captured, crystallo-raphic stone analysis should be performed.ptical microscopy, infrared spectroscopy, or
adiograph crystallography all are acceptableethods for stone analysis. Although most
tones are CaOx, crystallographic stone analysisllows identification of the less common stonesuch as cystine and struvite that require differ-nt evaluation. Also, stone analysis is the onlyay to diagnose stones composed of drugs
Table 1) and the very uncommon stonesuch as 2,8-dihydroxyadenine stones. A uri-alysis should be obtained to screen for possi-le infection, and if pyuria or other findings
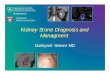
ndicative of infection are present then a urineulture should be performed. Urinalysis alsorovides an opportunity to evaluate crystalluriaFig. 1). Although calcium crystals are moreumerous and larger in stone formers than inormal subjects, the identification of CaOx andalcium phosphate crystals by itself has no di-gnostic significance. Uric acid crystals alsoay be seen in normal subjects and stone form-
rs, and usually form in acidic urine. However,he finding of cystine or struvite crystals is al-ays abnormal and provides a diagnosis even in
he absence of a stone analysis. If a stone anal-sis is not available, a qualitative screen forystinuria should be performed to rule out thisotentially devastating disease because treat-
ent needs to be initiated after the initial stone
agftbea
sblsps
Fcm rystals
104 J.R. Asplin
nd not wait for a recurrence. Although theeneral recommendation is a limited evaluationor single stone formers, children should have ahorough evaluation after the initial stone eventecause they have a higher likelihood of inbornrrors of metabolism, such as primary hyperox-
igure 1. Light microscopy of urine crystals. (A) Hexarystals (200�); (C) pyramid-shaped calcium oxalate dehonohydrate crystal (400�); (E) rectangular uric acid c
luria and cystinuria, as the cause of their s
tones. Some patients also require an evaluationased on their employment, such as airline pi-
ots. If the limited evaluation of the kidneytone patient reveals no abnormalities, then theatient should receive standard dietary and life-tyle advice that would be beneficial for all
cystine crystals (200�); (B) coffin-lid–shaped struvitee crystals (200�); (D) dumbbell-shaped calcium oxalate(400�); and (F) rhomboidal uric acid crystals (400�).
gonalydrat
tone patients, such as high fluid intake to keep

ulpnp
pfsufgbilntmifdAohfwmt
nbwcc
nmatsuosstatbbwttvsiSthbdftw
esi
Kidney stone patients 105
rine volume greater than 2.5 L/d, as well as aow-sodium, moderate-protein diet.57,58 Theatient also should be instructed to maintainormal dietary calcium levels because manyatients will reduce calcium on their own.A more extensive evaluation is needed for
atients with recurrent nephrolithiasis. Twenty-our–hour urine chemistries should be mea-ured to identify the abnormalities that contrib-te to stone formation and to identify dietaryactors that may modulate excretion of litho-enic substances. The chemistries that shoulde included in a 24-hour urine analysis are listed
n Table 2. The measurements listed in theeft-hand column provide the minimal work-upeeded for a stone-forming patient, allowinghe clinician to assess the factors that relateost directly to stone risk. The measurements
n the right-hand column provide additional in-ormation on stone risk itself, as well as theietary factors that influence urine stone risk.lso, calculation of urine supersaturation (SS)f the common stone-forming salts can be aelpful guide in the treatment of patients.59 Allactors included in Table 2, except creatinine,ould be included in the calculation of SS, theore chemistries included in the SS calculation,
he more accurate it will be.One issue that has not been resolved is the
umber of 24-hour urine collections that shoulde performed as part of the initial kidney stoneork-up. Unlike serum tests, urine chemistries
an change significantly from day to day based onhanges in environment, activities, and diet. A
Table 2. 24-Hour Urine Chemistries forEvaluation of Nephrolithiasis
MinimalEvaluation
CompleteEvaluation
Calcium SodiumOxalate PotassiumCitrate ChlorideUric acid Urea nitrogenVolume PhosphorouspH MagnesiumCreatinine Ammonia
Sulfate
o
umber of investigators have suggested thatultiple measurements are required to identify
bnormalities in urine chemistries, althoughhere is not universal agreement.60-62 Table 3hows the results of a comparison of 2 consec-tive pretreatment 24-hour urine collectionsbtained from a database of a clinical laboratorypecializing in kidney stone disease. Table 3hows the percentage of paired urine sampleshat have deviations of at least 25% or 50% inny of the major urine chemistries. The chancehat any of these critical chemistries will varyy 100% from one day to the next is 9%. Ielieve such variability is worth noting becauseithout having a sound knowledge of the pa-
ient’s baseline status it is impossible to judgehe effectiveness of any given therapeutic inter-ention. It seems prudent to obtain 2 urinepecimens when evaluating a patient, one dur-ng a weekday and one during the weekend.uch an evaluation will help uncover risk fac-ors that may be unique to the work and/orome environment. Many patients will need toe told specifically to perform the collectionuring a workday because most prefer to per-orm collections during the weekend to avoidhe embarrassment of collecting urine at theorkplace.A brief description of the clinical utility of
ach of the common measurements in a kidneytone evaluation is provided later. In consider-ng urine chemistries it should be noted that all
Table 3. Variability of 24-Hour UrineChemistries
25% VariabilityBetween 2
Consecutive24-Hour Urines
50% VariabilityBetween 2
Consecutive24-Hour Urines
Volume 36% 15%Calcium 20% 12%Oxalate 20% 6%Citrate 24% 10%Uric acid 15% 3%Any of the
above67% 36%
f these tests are continuous variables with a

wswpicst
C
MhaGcoctcistuesttscufit
O
Hphuoiaopwuso
C
H3lkcftiLsaphmwa
U
Ha1mlcdftemfwCrcttiwLcffl
U
Aps
106 J.R. Asplin
ide range of normal values.63 An increase intone risk can occur when values are stillithin the 95% confidence interval for a normalopulation. Strict cut-off values often are used
n research studies of nephrolithiasis but clini-ians caring for a patient need to recognize thatome urine chemistries require treatment, evenhough the results are in the normal range.
alcium
ost stones are composed of calcium andypercalciuria is the most common metabolicbnormality found in calcium stone formers.enerally, hypercalciuria is defined as a urinealcium level greater than 300 mg/d in a manr 250 mg/d in a woman on their usual diet,ompared with a mean urine calcium of 150o 170 mg/d in non–stone formers. Urine cal-ium levels greater than the mean, although notn the hypercalciuric range, may contribute totone disease and bringing high-normal valueso the low-normal level may be of benefit. Lowrine calcium levels can be found in stone form-rs, and although not a direct risk for kidneytones, hypocalciuria may indicate other pa-hology. Bowel disease may lead to malabsorp-ion of calcium and yet still be associated withtones because of other abnormalities fromhronic diarrhea such as low urine volume, lowrine citrate, and low urine pH. Vitamin D de-ciency also should be considered in any pa-ient with low urine calcium levels.
xalate
yperoxaluria is found in 30% of kidney stoneatients. In the vast majority of patients theyperoxaluria is of mild to moderate level and issually the result of dietary overindulgence ofxalate. It also may be related to other dietary
ssues such as a low-calcium diet, which allowsgreater percentage of oxalate to be absorbed,r because of a high intake of oxalate metabolicrecursors as might occur in some patientsith a high protein intake. If very high levels ofrine oxalate (�90 mg/d) are found, the patienthould be evaluated for enteric hyperoxaluria
r primary hyperoxaluria. Witrate
ypocitraturia generally is defined as less than25 mg/d, although there is considerable over-
ap between normal subjects and patients withidney stones.64 Citrate reduces stone risk byomplexing calcium in the urine, lowering theree calcium concentration.65 In addition, ci-rate is a direct inhibitor of CaOx crystallizationndependent of its ability to complex calcium.ow urine citrate level may be caused by con-umption of a high dietary acid load, metaboliccidosis, secondary to hypokalemia or idio-athic in origin.66 Because hypokalemia causesypocitraturia, it is particularly important toonitor the serum potassium level in patientshose hypercalciuria is being treated with thi-
zide.
ric Acid
yperuricosuria may contribute to both uriccid and CaOx stone formation. It is present in0% to 25% of stone formers. Hyperuricosuriaay be caused by metabolic abnormalities that
ead to overproduction, but most often isaused by excessive ingestion of purine in theiet.67 Generally, purine in human diets comesrom animal protein, and thus markers of pro-ein intake also will guide the clinician as to thextent of purine intake. Hyperuricosuria pro-otes stone formation by salting out CaOx
rom the urine.68 Lowering uric acid excretionith allopurinol has been shown to reduceaOx stone formation in patients with hyperu-
icosuria.69 Increased excretion obviously canontribute to uric acid stone formation, al-hough uric acid excretion rate is not as impor-ant as urine pH or urine flow rate in determin-ng the risk of uric acid stones. Some patients
ith severe metabolic derangements, such asesch-Nyhan syndrome, will have uric acid ex-retion rates so high that uric acid stones mayorm even with normal urine pH and urineow.
rine pH
lthough CaOx stones are independent of urineH, both uric acid and calcium phosphatetones are critically dependent on urine pH.
ith a pK of 5.4, uric acid becomes protonated

asmccHopauIcecg6soawtis
sudpbtcs
V
UsrisrTurflurplti
pta
E
Imtedditmwwhspvelucaisabwi
U
Duusuosmpf
A
Aat
Kidney stone patients 107
t low urine pH; protonated uric acid is poorlyoluble, with a maximal solubility of approxi-ately 100 mg/L in urine.70 As urine pH in-
reases above 6.0, uric acid risk decreases butalcium phosphate stone risk increases as
2PO4 is converted to HPO4, increasing the SSf calcium monohydrogen phosphate. A urineH of 6.0 is the double-minimum point for uriccid and calcium phosphate SS. Urine pH isseful in monitoring the effect of alkali therapy.f alkali is given to increase either urine pH oritrate, the urine pH should be measured tonsure an adequate response and prevent ex-essive alkalinization. Uric acid stone formersenerally need a urine pH in the range of 6.0 to.5, higher urine pH does not lower uric acidaturation significantly but will increase the riskf calcium phosphate crystallization. Excessivelkalinization should be avoided for patientsith hypocitraturia and hypercalciuria being
reated with alkaline citrate because an increasen urine pH may lead to calcium phosphatetones.
Urine pH varies from 5 to 7.5 in normalubjects, so a single random urine pH is not aseful clinical guide in the evaluation of stoneisease. The time averaging of 24-hour urine pHrovides a much better indicator of stone riskecause uric acid stone formers will have urinehat persistently is acidic and those with cal-ium phosphate stones usually will have a per-istently high urine pH.71
olume
rine volume is required in any timed urinepecimen to allow calculation of excretionates, and flow rate shows if the patient is drink-ng an adequate amount of fluid. Borghi et al57
howed that high fluid intakes reduce stoneecurrence in a prospective, randomized trial.heir work also provided a goal for urine vol-me: 2.5 L/d significantly reduced stone recur-ence. Patients should be instructed to increaseuid intake so that this goal is reached. A goal ofrine flow seems a more reasonable end pointather than a fixed fluid intake because everyatient has different rates of extrarenal fluid
oss via the GI tract and skin, which will affectheir rate of urine flow independent of fluid
ntake. Certainly, higher urine flow rates should irovide even greater therapeutic benefits, al-hough few patients can keep urine volumebove 3 L/d consistently.
lectrolytes
n patients without chronic diarrheal states, al-ost all dietary sodium is absorbed from the GI
ract. To stay in balance, the absorbed sodium isxcreted by the kidney, allowing the urine so-ium excretion to act as an excellent marker ofiet sodium intake. Because dietary salt load
nfluences urine calcium excretion, and an es-imate of diet sodium by patients is unreliable,easurement of sodium excretion is a practicalay to confirm that the patient is complyingith their diet therapy. Low potassium intakeas been associated with an increased risk oftones and can be estimated from the urineotassium excretion. A diet rich in fruits andegetables will increase the urine potassiumxcretion and seems to be associated withower stone risk. Urine potassium is particularlyseful in monitoring therapy with potassiumitrate. If the patient is taking their potassiumlkali, then urine potassium excretion shouldncrease by approximately the amount of potas-ium that was prescribed. Changes in urine pHnd urine citrate excretion during therapy maye variable, but the change in urine potassiumill confirm the patient is compliant with med-
cation.
rea Nitrogen/Sulfate
ietary protein intake may be assessed by urinerea and sulfate excretion. Urea is an end-prod-ct of amino acid metabolism and in the steadytate protein intake can be estimated by therea excretion rate.72 Sulfate is the end-productf metabolism of sulfur-containing amino acidsuch as methionine. As such, sulfate may beonitored to estimate dietary intake of animalrotein and provides insight into the acid load
rom a patient’s diet.
mmonium
mmonium levels change with the amount ofcid that the kidneys need to excrete to main-ain acid-base equilibrium. As diet acid load
ncreases, ammonium will increase, roughly
mtusowattaihnutt
M
Huaclmdb
P
Uomstnww
C
Tacvibtsaas
S
AbstcaISiwmKCoFu
C
Tramestlr
ATa
R
108 J.R. Asplin
irroring the changes in urine sulfate excre-ion. If ammonium greatly exceeds sulfate andrine pH is less than 6.5 it suggests an acidotictate such as a chronic diarrhea. In the settingf an alkali load, urine ammonium excretionill be suppressed as urine pH increases, the
mmonium excretion can be monitored to de-ermine the effectiveness of alkali therapy initrating the dietary acid load. If urine pH isbove 6.5 and urine ammonium excretion alsos high, it is a state incompatible with normaluman physiology. This situation suggests uri-ary tract infection with bacteria that possessrease activity. If this finding occurs, the pa-ient will need to be treated for infection andhe urine study will need to be repeated.
agnesium
ypomagnesuria has been suggested to contrib-te to stone risk.73 Magnesium complexes ox-late in the urine and lowers urine saturation ofalcium salts; diets low in magnesium may al-ow overabsorption of dietary oxalate. If urine
agnesium is very low, it suggests magnesiumeficiency, often seen in patients with small-owel disease and malabsorption.
hosphate
rine phosphate provides a rough estimatef dietary phosphate intake because approxi-ately 60% to 70% of dietary phosphate is ab-
orbed. Although excess urine phosphate con-ributes to calcium phosphate stone risk, it isot as important a risk factor as urine pH,hich determines how much of the phosphateill be in the form of HPO4.
reatinine
he creatinine excretion should be measured inll 24-hour urine specimens to ensure that theollection has been performed properly. Urineolume is not an adequate marker to determinef a urine collection was performed properlyecause urine flow may be as low as 500 mL/do more than 3 L/d. Urine creatinine levelshould be 18 to 25 mg/kg body weight in mennd 15 to 22 mg/kg body weight in women,lthough it can vary with muscle mass and obe-
ity.upersaturations
ll the earlier-described urine chemistries cane used to calculate urine SS using a programuch as EQUIL2.59 SS is the ratio of the concen-ration of a salt in solution to the salt’s solubilityoncentration, a value greater than 1 indicates SS,value less than 1 is an undersaturated solution.
n the absence of a crystallographic stone analysis,S values can predict the type of stone the patients most likely to form because SS values correlate
ith known stone types. SS is also a useful way toonitor therapy. At the University of Chicagoidney Stone Clinic we have found that reducingaOx SS by 50% from baseline led to a reductionf stone rates to 21% of the pretreatment rate.74
or uric acid stones, the goal is to keep the urinendersaturated.
ONCLUSIONS
he evaluation of the kidney stone patientequires a careful history to determine dietarynd environmental risk factors that can beodified as well as a thorough laboratory
valuation for patients with recurrent kidneytones to identify abnormalities that can bereated by dietary, lifestyle, and pharmaco-ogic interventions. Medical intervention caneduce stone recurrence by up to 80%.
cknowledgmenthe author would like to acknowledge the invalu-ble editorial assistance of Susan Donahue.
EFERENCES1. Stamatelou KK, Francis ME, Jones CA, et al. Time trends
in reported prevalence of kidney stones in the UnitedStates: 1976-1994. Kidney Int. 2003;63:1817-23.
2. Sutherland JW, Parks J, Coe F. Recurrence after asingle renal stone in a community practice. MinerElectrolyte Metab. 1985;11:267-9.
3. Ljunghall S, Danielson BG. A prospective study ofrenal stone recurrences. Br J Urol. 1984;56:122-4.
4. Schwartz BF, Stoller ML. Nonsurgical management ofinfection-related renal calculi. Urol Clin North Am.1999;26:765-78, viii.
5. Worcester EM. Stones from bowel disease. Endocri-nol Metab Clin North Am. 2002;31:979-99.
6. Parks JH, Worcester EM, O’Connor RC, et al. Urinestone risk factors in nephrolithiasis patients with andwithout bowel disease. Kidney Int. 2003;63:255-65.
7. Asplin JR, Coe FL. Hyperoxaluria in kidney stone

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
3
3
3
3
4
4
4
4
Kidney stone patients 109
formers treated with modern bariatric surgery. J Urol.2007;177:565-9.
8. Coe FL, Parks JH. Nephrolithiasis: pathogenesis andtreatment. 2nd ed. Chicago: Year Book Medical Pub-lishers, Inc., 1988.
9. Levy FL, Adams-Huet B, Pak CY. Ambulatory evalua-tion of nephrolithiasis: an update of a 1980 protocol.Am J Med. 1995;98:50-9.
0. Soucie JM, Thun MJ, Coates RJ, et al. Demographicand geographic variability of kidney stones in theUnited States. Kidney Int. 1994;46:893-9.
1. Curhan GC, Rimm EB, Willett WC, et al. Regionalvariation in nephrolithiasis incidence and prevalenceamong United States men. J Urol. 1994;151:838-41.
2. Evans K, Costabile RA. Time to development of symp-tomatic urinary calculi in a high risk environment.J Urol. 2005;173:858-61.
3. Borghi L, Meschi T, Amato F, et al. Hot occupationand nephrolithiasis. J Urol. 1993;150:1757-60.
4. Milvy P, Colt E, Thornton J. A high incidence ofurolithiasis in male marathon runners. J Sports MedPhys Fitness. 1981;21:295-8.
5. Curhan GC, Willett WC, Rimm EB, et al. A prospec-tive study of dietary calcium and other nutrients andthe risk of symptomatic kidney stones. N Engl J Med.1993;328:833-8.
6. Curhan GC, Willett WC, Speizer FE, et al. Comparison ofdietary calcium with supplemental calcium and othernutrients as factors affecting the risk for kidney stones inwomen. Ann Intern Med. 1997;126:497-504.
7. Curhan GC, Willett WC, Knight EL, et al. Dietaryfactors and the risk of incident kidney stones inyounger women: Nurses’ Health Study II. Arch InternMed. 2004;164:885-91.
8. Holmes RP, Goodman HO, Assimos DG. Contributionof dietary oxalate to urinary oxalate excretion. Kid-ney Int. 2001;59:270-6.
9. Harvard School of Public Health Nutrition Depart-ment’s File Download Site. Updated October 2007.Oxalate table of foods. [cited 2007 October 23] Avail-able from: https://regepi.bwh.harvard.edu/health/Oxalate/files/.
0. Oxalosis and Hyperoxaluria Foundation. The oxalatecontent of food. Updated May 2004. [cited 2007October 23] Available from: http://www.ohf.org/diet.html/.
1. Curhan GC, Willett WC, Rimm EB, et al. Prospectivestudy of beverage use and the risk of kidney stones.Am J Epidemiol. 1996;143:240-7.
2. Curhan GC, Willett WC, Speizer FE, et al. Beverageuse and risk for kidney stones in women. Ann InternMed. 1998;128:534-40.
3. Goldfarb D, Asplin JR. Effect of grapefruit juice onurinary lithogenicity. J Urol. 2001;166:263-7.
4. Breslau NA, Brinkley L, Hill KD, et al. Relationship ofanimal protein-rich diet to kidney stone formationand calcium metabolism. J Clin Endocrinol Metab.1988;66:140-6.
5. Allen LH, Oddoye EA, Margen S. Protein-induced hy-
percalciuria: a longer term study. Am J Clin Nutr.1979;32:741-9.
6. Robertson WG, Heyburn PJ, Peacock M, et al. Theeffect of high animal protein intake on the risk ofcalcium stone-formation in the urinary tract. Clin Sci(Lond). 1979;57:285-8.
7. Licata AA, Bou E, Bartter FC, et al. Effects of dietaryprotein on urinary calcium in normal subjects and inpatients with nephrolithiasis. Metabolism. 1979;28:895-900.
8. Sakhaee K, Harvey JA, Padalino PK, et al. The poten-tial role of salt abuse on the risk for kidney stoneformation. J Urol. 1993;150:310-2.
9. Silver J, Rubinger D, Friedlaender MM, et al. Sodium-dependent idiopathic hypercalciuria in renal-stoneformers. Lancet. 1983;2:484-6.
0. Muldowney FP, Freaney R, Moloney MF. Importanceof dietary sodium in the hypercalciuria syndrome.Kidney Int. 1982;22:292-6.
1. Curhan GC, Willett WC, Rimm EB, et al. Family his-tory and risk of kidney stones. J Am Soc Nephrol.1997;8:1568-73.
2. Coe FL, Parks JH, Moore ES. Familial idiopathic hy-percalciuria. N Engl J Med. 1979;300:337-40.
3. Goodman HO, Holmes RP, Assimos DG. Genetic fac-tors in calcium oxalate stone disease. J Urol. 1995;153:301-7.
4. Karet FE. Inherited distal renal tubular acidosis. J AmSoc Nephrol. 2002;13:2178-84.
5. Knohl SJ, Scheinman SJ. Inherited hypercalciuric syn-dromes: Dent’s disease (CLC-5) and familial hypomag-nesemia with hypercalciuria (paracellin-1). SeminNephrol. 2004;24:55-60.
6. Ahlstrand C, Tiselius HG. Urine composition andstone formation during treatment with acetazol-amide. Scand J Urol Nephrol. 1987;21:225-8.
7. Lamb EJ, Stevens PE, Nashef L. Topiramate increasesbiochemical risk of nephrolithiasis. Ann Clin Bio-chem. 2004;41:166-9.
8. Welch BJ, Graybeal D, Moe OW, et al. Biochemicaland stone-risk profiles with topiramate treatment.Am J Kidney Dis. 2006;48:555-63.
9. Hatch M, Mulgrew S, Bourke E, et al. Effect of mega-doses of ascorbic acid on serum and urinary oxalate.Eur Urol. 1980;6:166-9.
0. Urivetzky M, Kessaris D, Smith AD. Ascorbic acidoverdosing: a risk factor for calcium oxalate nephro-lithiasis. J Urol. 1992;147:1215-8.
1. Auer BL, Auer D, Rodgers AL. The effect of ascorbicacid ingestion on the biochemical and physical chem-ical risk factors associated with calcium oxalate kid-ney stone formation. Clin Chem Lab Med. 1998;36:143-8.
2. Jackson RD, LaCroix AZ, Gass M, et al. Calcium plusvitamin D supplementation and the risk of fractures.N Engl J Med. 2006;354:669-83.
3. Saltel E, Angel JB, Futter NG, et al. Increased preva-lence and analysis of risk factors for indinavir neph-
rolithiasis. J Urol. 2000;164:1895-7.
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
7
7
7
110 J.R. Asplin
4. Wu DS, Stoller ML. Indinavir urolithiasis. Curr OpinUrol. 2000;10:557-61.
5. Nadler RB, Rubenstein JN, Eggener SE, et al. The etiol-ogy of urolithiasis in HIV infected patients. J Urol.2003;169:475-7.
6. Powell T, Hsu FF, Turk J, et al. Ma-huang strikes again:ephedrine nephrolithiasis. Am J Kidney Dis. 1998;32:153-9.
7. Assimos DG, Langenstroer P, Leinbach RF, et al.Guaifenesin- and ephedrine-induced stones. J En-dourol. 1999;13:665-7.
8. Ettinger B, Oldroyd NO, Sorgel F. Triamterene neph-rolithiasis. JAMA. 1980;244:2443-5.
9. Sica DA, Gehr TW. Triamterene and the kidney.Nephron. 1989;51:454-61.
0. Daudon M, Jungers P. Drug-induced renal calculi:epidemiology, prevention and management. Drugs.2004;64:245-75.
1. Rao PN. Imaging for kidney stones. World J Urol.2004;22:323-7.
2. Sheafor DH, Hertzberg BS, Freed KS, et al. Nonen-hanced helical CT and US in the emergency evalua-tion of patients with renal colic: prospective compar-ison. Radiology. 2000;217:792-7.
3. Ulusan S, Koc Z, Tokmak N. Accuracy of sonographyfor detecting renal stone: comparison with CT. J ClinUltrasound. 2007;35:256-61.
4. Kluner C, Hein PA, Gralla O, et al. Does ultra-low-doseCT with a radiation dose equivalent to that of KUBsuffice to detect renal and ureteral calculi? J ComputAssist Tomogr. 2006;30:44-50.
5. Brenner DJ, Hall EJ. Computed tomography—an in-creasing source of radiation exposure. N Engl J Med.2007;357:2277-84.
6. Consensus conference: prevention and treatment ofkidney stones. JAMA. 1989;260:978-81.
7. Borghi L, Meschi T, Amato F, et al. Urinary volume,water and recurrences in idiopathic calcium neph-rolithiasis: a 5-year randomized prospective study.J Urol. 1996;155:839-43.
8. Borghi L, Schianchi T, Meschi T, et al. Comparisonof two diets for the prevention of recurrent stonesin idiopathic hypercalciuria. N Engl J Med. 2002;346:77-84.
9. Werness PG, Brown CM, Smith LH, et al. EQUIL 2: abasic computer program for the calculation of urinary
saturation. J Urol. 1985;134:1242-4.0. Parks JH, Goldfisher E, Asplin JR, et al. A single24-hour urine collection is inadequate for the med-ical evaluation of nephrolithiasis. J Urol. 2002;167:1607-12.
1. Pak CY, Peterson R, Poindexter JR. Adequacy of asingle stone risk analysis in the medical evaluation ofurolithiasis. J Urol. 2001;165:378-81.
2. Strohmaier WL, Holz K, Bichler KH. Is metabolicevaluation based on one urine specimen reliable? In:Rodgers AL, Hibbert BE, Hess B, Khan SR, PremingerGM, editors. Urolithiasis. Cape Town: University ofCape Town, 2000.
3. Curhan GC, Willett WC, Speizer FE, et al. Twenty-four-hour urine chemistries and the risk of kidneystones among women and men. Kidney Int. 2001;59:2290-8.
4. Nikkila M, Koivula T, Jokela H. Urinary citrate excre-tion in patients with urolithiasis and normal subjects.Eur Urol. 1989;16:382-5.
5. Nicar MJ, Hill K, Pak CYC. Inhibition by citrate ofspontaneous precipitation of calcium oxalate in vitro.J Bone Miner Res. 1987;2:215-20.
6. Hamm LL. Renal handling of citrate. Kidney Int. 1990;38:728-35.
7. Coe FL, Kavalach AG. Hypercalciuria and hyperurico-suria in patients with calcium nephrolithiasis. N EnglJ Med. 1974;291:1344-50.
8. Ryall R, Grover P, Marshall V. Urate and calciumstones—picking up a drop of mercury with one’sfingers? Am J Kidney Dis. 1991;27:426-30.
9. Ettinger B, Tang A, Citron JT, et al. Randomized trialof allopurinol in the prevention of calcium oxalatecalculi. N Engl J Med. 1986;315:1386-9.
0. Coe F, Strauss AL, Tembe V, et al. Uric acid saturationin calcium nephrolithiasis. Kidney Int. 1980;17:662-8.
1. Parks JH, Worcester EM, Coe FL, et al. Clinical impli-cations of abundant calcium phosphate in routinelyanalyzed kidney stones. Kidney Int. 2004;66:777-85.
2. Maroni BJ, Steinman TI, Mitch WE. A method forestimating nitrogen intake of patients with chronicrenal failure. Kidney Int. 1985;27:58-65.
3. Preminger GM, Baker S, Peterson R, et al. Hypomag-nesiuric hypocitraturia: an apparent new entity forcalcium nephrolithiasis. J Lithotripsy Stone Dis. 1989;1:22-5.
4. Parks J, Coe F. The financial effects of kidney stone
prevention. Kidney Int. 1996;50:1706-12.