Embed Size (px)
Citation preview

Clinical Oncology for Medical Dosimetrists
DOS 431/531University of Wisconsin –
La Crosse

Nasopharynx

Epidemiology Uncommon in most countries
Highest incidence: China, Southeast Asia, and in Eskimos
Peaks in 4th-5th decade of life 3 major etiologic factors:
Viral: Ebstein-Barr virus (EBV) Genetic: human leukocyte antigen (HLA) Environmental: poor ventilation, occupational
exposures to smoke or dusts, and diet

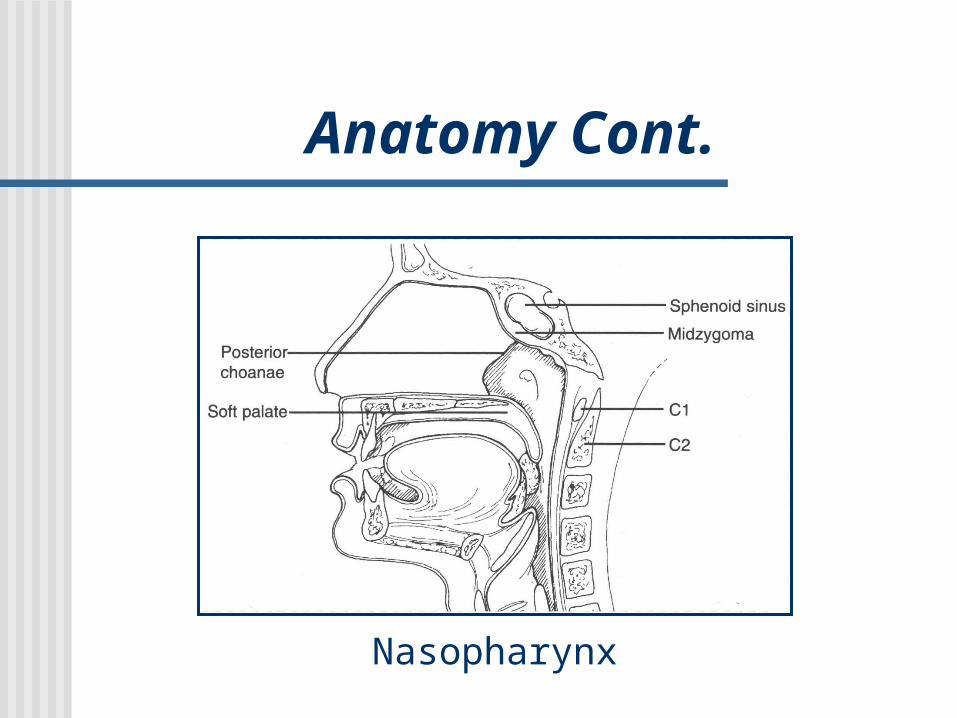
Anatomy The nasopharynx is a roughly cuboidal,
open chamber located below the base of the skull and behind the nasal cavity.
Borders of the nasopharynx: Ant. border: posterior choanae Post. border: first 2 cervical vertebrae and the
clivus Sup. border: body of the sphenoid Inf. border: soft palate
Anatomy Cont.
Nasopharynx

Pathology and Lymphatics Epidermoid or undifferentiated carcinomas make
up about 90% of malignant nasopharynx tumors Lymphoma, plasmacytoma, melanoma,
rhabdomysarcoma, chordoma, and tumors of minor salivary gland origin make up the remaining 10%
Commonly involved lymph nodes: Cervical lymph nodes Jugulodigastric lymph nodes Supraclav nodes

Staging and Management Many staging systems may be used;
however, the most common system used is the TNM staging system. See Table in Chao
Radiation therapy is the treatment of choice for nasopharynx tumors Chemoradiotherapy has shown to increase
survival as well Surgical resection with acceptable
margins is not possible

Radiation Therapy Techniques Opposed lateral fields with a 5 degree posterior angle (to
help avoid direct ipsilateral dose to the external and middle ear, as well as the contralateral lens)
Volumes included: nasopharynx, adjacent parapharyngeal tissues, cervical lymphatics (jugular, spinal accessory, and supraclav nodes), post. ethmoid cells, sphenoid sinus, and basosphenoid, base of skull, post. nasal cavity and maxillary antrum, and lateral and post. pharyngeal wall to the lower pole of tonsil, in addition to the retropharyngeal, upper cervical, mastoid, and posterior cervical lymph nodes
Bilateral anterior supraclav field is always included Midline block is used

Radiation Therapy Techniques Cont.
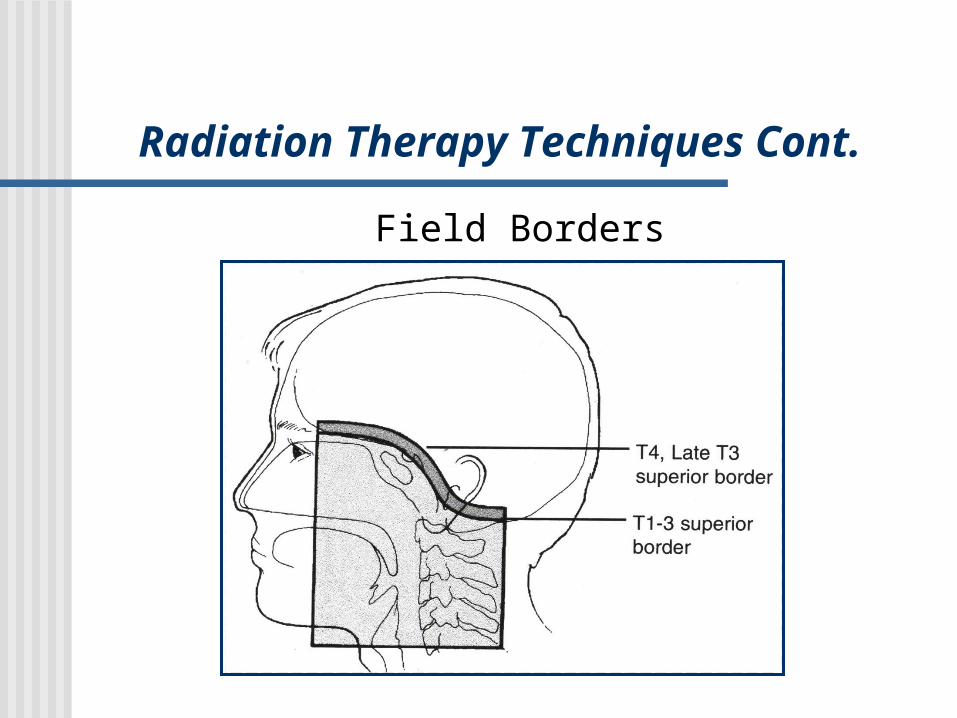
Field Borders Ant: posterior 2cm of nasal cavity; posterior 1/3
of maxillary sinus; posterior ethmoid sinuses; posterior ¼ of orbit
Post: behind spinous processes
Sup: entire sphenoid sinus; cavernous sinus; base of skull
Inf: thyroid notch or above the larynx
Radiation Therapy Techniques Cont.
Field Borders

Radiation Therapy Techniques Cont.
Doses Full field dose: 45Gy
Reduce fields and use 9MeV electrons to take post. neck nodes to 50-60Gy
Nasopharynx: 65-75Gy Last 20-25Gy may use high-energy photons
(18MV) to reduce dose to the mandible and TMJ
Low neck and supraclav fossa: 50Gy

Radiation Therapy Techniques Cont.
Brachytherapy Brachytherapy can be used to treat
nasopharyngeal tumors. These can be interstitial or intracavitary
implants. More recently, HDR afterloading units
have been used to treat intracavitary nasopharynx tumors.

Radiation Therapy Techniques Cont.
Nasopharynx BrachytherapyHDR technique





























