Embed Size (px)
Citation preview

Clinical neuroanatomy for CT1s
Dr John O’DonovanFriday 8th June

Firstly

Secondly

Thirdly

Basics
• Neurons of which there are many types, with many functions, make up the nervous system.
• The nervous system for our purposes comprises the brain, spinal cord and peripheral nerves.
• Focus for CT1 should be on both clinical and scientific but more so on clinical.
• The anatomy tends to be bottom up but clinical signs tend to be top down.

The brainin the skull Frontal lobes Temporal lobes Occipital lobes Parietal lobes Limbic lobe/system CerebellumPituitary and hypothalamus (hypophysis)Pons, midbrain, medulla oblongata-cranial nerves and nuclei.

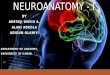
Frontal lobe
Match them UP? Look at the size of that frontal lobe!

Frontal lobe syndromes
• Orbitofrontal: disinhibition, witzelsucht, euphoria, lability, poor judgment and poor attention.
• Frontal convexity: apathetic, indifferent, retarded, perseverating
• Medical frontal: akinetic, mutism, gait problems and incontinence.
• Massive frontal lobe syndromes: combination of all four.
• All a gross oversimplification.

Worth noting the following about cortical lesions
• Less deficit per volume affected• Frequently patients are unaware of extent of deficit, “anosagnosia”• Tends to be inconsistent• Multimodal deficits eg alexia, need analysis. • There is individual variation in cortical function. • The neurology is syndrome based and therefore these are by definition
imprecise to some extent• Clinical presentation also varies by tempo and nature of damage• Cortical plasticity means that elementary functions improve better then
complex deficits.• Cortex is susceptible to global systemic fluctuation, such as delirium• Selective cortical lesions tend to cause seizures and multimodal deficits

Other signs
• Precentral gyrus: face, hand, leg and urinary incontinence if bilateral. Also with unilateral if massive.
• Mesial aspect: akinesis, perseveration, grasping, “salutatory seizures”, alien hand sign, transcortical motor aphasia, bilateral ideomotor apraxia
• Lateral aspect: impaired saccades, pure agraphia in dominant hemisphere, contralateral, arm weakness
• Frontal pole: orbitofrontal as before degree of acquired sociopathy

Frontal lobe summary
Motor problems• Eye movements on
contralateral side • Contralateral hemiparesis,
face, hand, leg (arm more then leg)
• Inability to start or stop correctly, akinesis and perseveration
• Oddities, alien hand, grasping and pure agraphia
Non motor problems• Motor aphasia: Broca’s • Incontinence if bilateral • Inability to plan ahead• Poor self monitoring and
social judgment• Acquired sociopathy • Dysexecutive
• Remember caveat about cortical lesions.

Temporal lobes
Lateral aspect Remember the hippocampus

Temporal lobe
Lanuage• Wernicke’s area, receptive
aphasia
Non language funcions • Emotion • Memory by means of the
hippocampal complex• Verbal memory is more left
based and visual is more right based. (simplification)
• Complex partial seizures NB

Temporal lobe 2
Inferomedial• Anmesia • Bilateral anterior temporal
lobe lesions can lead to Kluver-Bucy Syndrome with visual agnosia, hyperoral, tameness, hypersexual, hypomotile and hypermetamorphosis (paying attention to every visual stimulus)
Lateroinferior• Dominant: transcortical
sensory aphasia and word selection anomia, in essence receptive aphasias
• Non Dominant: Impaired recognition of facial emotional expression.

Temporal lobe 2
Laterosuperior • Dominant: pure word
deafness and sensory aphasia.
• Nondominant: sensory amusia and sensory aprosodia.
Bilateral lesions of lateral superior aspect
• Auditory agnosia

Temporal lobe 3
Eye problems• Contralateral superior
quadrantic anopsia, Meyer’s loop etc.
• Seizures• Temporal lobe both left and right,
hippocampus, amygdala and connections are frequent source of complex partial seizures-separate discussion.
Non localising signs• Auditory hallucinations • Complex visual
hallucinations

Parietal Lobe
Sensory input Making sense of it all

Parietal lobe 1
Post central gyrus• damage causes
contralateral sensory disturbance, pain and paresthesia
• Mesial aspect in dominant hemisphere can cause transcortical sensory aphasia
Lateral aspect• Dominant, parietal apraxia,
finger agnosia, acalculia, right left disorientation, literal alexia and possibly conduction aphasia. Note Gerstman Syndrome
• Non Dominant, anosognosia, autopagnosia, spatial disorientation, hemispatial neglect, constructional and dressing apraxia

To simplify
• Parietal lobes are sensory and put sensory input into context.
• Dominant lobe injury on lateral aspect can allegedly cause a Gerstman Syndrome. This is a bit of a myth, but a useful one for the MRCPsych.

Gerstman Syndrome
• Agraphia –can’t read. • Acalculia – can’t do arithmetic.• Finger agnosia –can’t recognize fingers.• Left right disorientation – left verus right• Dominant angular and marginal gyrus.
• Very debatable if it exists, beloved of post graduate examinations.

Occipital Lobes

Occipital lobe
Mesial • Visual field cut • Visual agnosia • Visual hallucinations• Anton syndrome-cortical
blindness without insight into blindness (anosagnosia)
• Alexia without agraphia-generally also with splenium involvment.
Lateral• Alexia with agraphia • Impaired optokinetic
nystagmus• Impaired scanning.

To simplify

John’s simple rules
• Frontal lobe is ultimately about doing stuff, speaking, walking, planning, studying etc.
• Temporal lobe all about memory and understanding language. Obviously the receptive language area is beside the ears!, memory is a bilateral function, anything you hear or how you hear it.
• Parietal lobe is ultimately about sensory input• Occipital lobe is about vision• Left hemisphere is dominant, any question with
language, check dominance.

MCQs Frontal lobes
Frontal lobe lesions cause• Contralateral sensory
problems. • Transcortical sensory
aphasia• Incontinence• Witzelsucht• Reckless behavior• Versive seizures• Alien hand phenomena
Frontal lobe lesions 2• Being rude to in laws • Watching TV all night • Perseveration• Grasping • Primitive reflexes • Echopraxia • Echolalia• Pure agraphia• Problems with memory

MCQs Temporal lobes
Bilateral temporal lobe lesions cause
• Disorders of memory • Transcortical motor aphasia • Amnesia • Paraamnestic phenomena• Incontinence • Contralateral motor
weakness• May if bilateral cause Kluver-
Bucy Syndrome• Emotional problems
Dominant temporal lobe lesions cause
• Inferior visual quadrantopia• Auditory agnosia • Amusia • Aprosody• Difficulty recognizing when
your wife is angry• Hallucinations?

MCQs Parietal lobes
Parietal lobe lesions cause• Motor problems • Dressing apraxia• Anosagnosia • Autopagnosia • Alexia• Finger agnosia• Visual integration problems
Dominant parietal lesions always
• Cause Gerstman Syndrome• Contralateral paresthesia • Reduced light touch, but
preserved propioception on contralteral side.
• Acalculia • Cause hemispatial neglect.

story• The four lobes of the brain were friends. • Frontal Frank was a leader. He decided what to do and how to do it. He was always talking
and always moving around. He made all the decisions and was a dominant personality. Tempermental Tim on the other hand, was always listening out for what anybody said about him and he had a prodigious memory but was prone to being moody and sometimes would seize up with odd feelings, which he could not explain very well. Frank used to go out with Pretty Parie but he broke up after being unable to satisfy her sensory needs. On top of which, despite dominating Frank, she did not read, add up, know her left from right or ever recognize her fingers and he found it hard to deal with her constant whining about her right side not being properly dressed and neglecting him all the time. Ultimately he went to tempermental Tim for advice who told him to speak with Occy who had a reputation as a bit of a visionary. Occy told Frank that he couldn’t see what was in it for him and to have a bit of a look around on the other side. Frank never took advice well and ended up beating Occy half blind, but suffered a stroke affecting his arm in particular and ended up mute and incontinent. This upset Tim so badly that he went into status epilpticus and lost his memory for everything. Pretty Parie meanwhile continued trying to make sense of it all.

Occipital lobe lesions
If dominant• Cause ipsilateral
hemianopsia • Can cause colour
desaturation.• Can cause alexia• Mean that you can no
longer drive• May cause visual
hallucinations
If bilateral• Can cause cortical blindness• Are normally caused by
pump failure. • Can occur in prion disease• Impair the pupil response• Can cause Balint Syndrome

And now for something different
• Neuroanatomy of vision• Neuroanatomy of the spinal cord• Neuroanatomy of the basal ganglia and
cerebellum• Neuroanatomy of the peripheral nerves

Diagnosis?

Diagnosis

Diagnosis

Pupils 4 parts
Optic nerve-pretectal area in midbrain
Pretectum to Edwinger Westphal nucleus (parasympathetic nucleus of !!! Occulomotor nerve)
Edwinger Westphal nucleus bilateral to ciliary ganglion
Ciliary ganglion to constrictor muscles of iris

Light near dissociationArgyll Robertson Pupil, syphilitic eye disease, very rare, lesion site around the aqueduct. “the prostitute accomodates but does not react”
Holmes-Adie tonic pupilWith arreflexia Adie Syndrome, prevalence is 1:500, degeneration of ciliary ganglion, other name is tonic pupil.
Parinaud Syndrome, rostral midbrain stroke, presumably from damage to midbrain
Remember 80% of the ciliary ganglion response is for accomodation, not light.

Dilated pupil from occulomotor palsy-occulomotor nerve, ptosis, down and out with mydriasis.
Remember parasympathetic fibres run on the outside of the nerve and are susceptible to trauma.
Coning of the brain, trauma, ptuitary lesions, PICA aneurysms.
Axonal palsies from diabetes and vasculitis tends to be pupil sparing.

Drugs that cause mydriasis
Atropine Hyoscine Scopolamine TropicamideAll anti cholinergics
Anti cholinergics-not drugs with weak anti cholinergic effects.

Horner’s Syndrome

Horner’s Syndrome
• Congenital • Anywhere in sympathetic chain• Hypothalamus • C8/T1 root• Pancoast tumours, apex of lung

Visual pathways

Visual pathways 2
• Tends not to be asked. • Generally very basic, remember to draw the
pathway. • Pituitary lesions cause bitemporal
hemianopsia • Occipital cause a contralateral field cut, left
occipital lesions cause right sided hemianopsia.

MS eye signs, optic neuritis and internculear opthalmoplegia (dissociated nystagmus)

Eye MCQs
a normal pupil response• Daylight causes mydriasis• Both pupils are equal in size• Both respond consensually• Two cranial nerves are used• Second relay centre is in the
pons• The ciliary ganglion is
sympathetic• Accomodation is to light as
2:1
Argyll Robertson pupils• Are always pathological• Can be associated with an
absent ciliospinal reflex• Don’t react to light• React quickly to
accomodation• Are common with HIV
infection• Are similar to Holmes-Adie
pupils

Eye MCQs
Match the following• Growing hands, feet and
diabetes• Young woman with weak
left leg and double vision• Smoker with a painful
armpit• Cortical blindness• Xanthochromia
Possible answers• Compressive third nerve
palsy.• Bitemporal hemianopsia • Horner’s Syndrome • Old variant CJD • Multiple sclerosis• Myasthenia gravis • Relative afferent pupil
defect.

Spinal cord and brainstem

Brainstem

Brainstem
• Use cranial nerve nuclei to find lesion level. • Remember deccusation in the pyramids of the
medulla oblongata-crossed syndromes.• Lateral medullary syndrome frequently sneaks
in and therefore must be known. • Remember pons-trigeminal nerve, pontine
pupils, CPM-central pontine myelinosis• Unlikely to be asked specifics

Cranial nerves

Spinal cord pathways
Corticospinal tract Spinothalamic

Spinal cord
Posterior columns Syringomyelia

Syringomyelia/BulbiaHole in central spinal cord filled by CSF
Results in weakness-combined lower and upper motor neuron signs
Dissociated sensory loss-meaning that it affects spinothalamic tracts with anaesthesia and absence of temperature perception.
Can result in Charcot Joints, most commonly in hands and shoulders
Classically shows a cape distribution sensory loss
Syringobulbia is when it extends into the bulbar area and causes cranial nerve and brainstem signs. Norallly lower cranial nerves and sometimes trigeminal.

Brown-Sequard SyndromeHemitransection of cord Same side as lesion UMN weakness and posterior column problems
Contralateral side loss of pain and temperature (spinothalamic)

Cord transectionRarely asked as questionIn general, below lesion spasticity and weakness
Plantar externsor and clonus
Neurogenic bladder and bowel
Lesion level guides disability
Cord level does not equate precisely to root level

Peripheral nerves
• Highly unlikely to be asked as a question. • Some basics- peripheral nerve lesions or lower
motor neruon lesions cause arreflexia at level of lesion, atrophy, weakness and fasiculations.
• Can be subdivided into many types of lesion but simply put, either axonal or demyelinating such as AIDP.
• Axonal lesions tend to occur in vascular process and cause more gross atrophy.

Peripheral neuropathies
causes Peripheral nerves

Peripheral neuropathy
• Glove and stocking • Longest nerves first (sciatic!), begins in feet. • Common causes of painful peripheral
neuropathy diabetes and drink, B12. • Commonest cause of peripheral neuropathy
worldwide is leprosy. • Acute flacid weakness-AIDP, GBS

MCQs on cranial nerves, spinal cord and peripheral nerves
• Bells palsy is a lesion of the trigeminal nerve.
• The afferent arc of the corneal reflex is in the maxillay branch of the trigeminal nerve
• Swallowing requires an intact hypoglossal nerve
• Bilateral LMN facial palsies can occur in sarcoid
• Brown Sequard syndrome results in ipsilateral spinothalamic function loss
• UMN lesions cause fasiculations • A syrinx of the thoracic cord can
cause bladder problems
• Following cause peripheral neuropathy
• Lead • Diabetes • Acute intermittent
porphyria• Metronidazole • Alcohol • B12 deficiency • Cryoglobulinaemia • Lithium

Cerebellum and basal ganglia

Basal ganglia and cerebellum
• Functions are ultimately to provide smooth and effective movements.
• Much greater role then simply movement, needed for cognition, emotion, reward networks, executive functioning.
• Multiple feedback loops between cortex and basal ganglia, allows cortex and basal ganglia to self monitor, to some extent.

Cerebellar SignsIpsilateral Ataxia Rebound Slow reflexes Nystagmus Tremor Difficulty with rapidly pronating/supinating movements-dysdiadokinesiDysarthria Hypotonia
Midline-vermian commonly from alcohol Central ataxia Dysarthria

Causes of cerebellar disease
• Alcohol • Drugs-intoxication eg phenytoin toxicity• Toxins • Hypoxia • Stroke • Trauma• Celiac disease • Paraneoplastic with breast/ovarian in particular• Congenital-SCAs, pure cerebellar degenerations• Congenital

The basal ganglia
Pathways Anatomy

Functions
• Motor • Cognitive • Emotional
• Damage in any area of basal ganglia can produce problems in those three domains.

Cognitive
• Sub cortical dementias • Slowness • Bradyphrenia • Psychomotor retardation • Apathy• Reduced language generation• Secondary frontal effects

Emotional
• Obsessional (sometimes) • Affective instability/frontal• Depression-very common and can be severe• Abulia, akinesis and apathy

Motor
• Abnormality of speed of movement, generally bradykinesia as in Parkinson’s but can be accelerated as in HD or hemibalismus
• Tremor• Chorea • Dystonia • Athetotis • Dystonia• Hemibalismus• Also dysarhtria and clumsiness

Parkinson’s Disease
tremor rest 4-6hz BradykinesiaPoor postural reflexes Festinant gait Response to dopa Presents as assymetric

Chorea
HDSCAsMedications –neuroleptics Rheumatic fever PANDASSt Vitus Dance Congenital benignStorage diseases DRPLAOdd illnessesAutoimmune Phospholipid disease Lupus OCP/pregnancy

Wilson’s DiseaseVery rareMetabolic AR genetics Check condanguinity Liver disorderCopper metabolism goes wrong
Clinically, liver disease, eye disease and dystonic, parkinsonian illness with marked axial and bulbar roblmes
Neuropsychiatric problems,global cognitive decline and personality alterations

Others
Hemibalismus Tics

MCQs
In cerebellar disease • Signs are contralateral • Reflexes are pendular• Hypertonia is the norm • DRPLA is a common cause • There may be malabsorbtion• There are cognitive and affective
changes• Alcohol should be avoided• Rebound is seen • Prosody is affected
In movement disorders• Cognition is always affected.• Depression is common • OCD may be associated with tics • Parkinson’s is normally assymetric in onset• Parkinson’s always responds to dopa • Parkinson plus syndromes have a good
prognosis • Chorea in a forty year old alcoholic with
poor impulse control is worrying• HD shows anticipation • HD is a trinucleotide repeat

The end