-
J7ournal ofNeurology, Neurosurgery, and Psychiatry
1994;57:7-15
NEUROLOGICAL MANAGEMENT
Clinical genetics in neurological disease
John C MacMillan, Peter S Harper
Inherited neurological disorders have tradi-tionally engendered
feelings of therapeuticnihilism in the medical community: not
onlyare these conditions often difficult to diag-nose with any
certainty, they are also per-ceived as "untreatable" whether or not
a firmdiagnosis has been reached. This negativeresponse is due in
part to a lack of knowledgeconcerning the underlying pathological
basisfor these disorders.The 1980s and early 1990s have seen a
rapid increase in our understanding of themolecular mechanisms
behind many of thesedebilitating conditions, largely due toadvances
in recombinant DNA technology.This article aims to summarise the
role ofclinical genetic and molecular genetic practicein the
management of the major inheritedneurological diseases. We consider
diagnosticissues as they pertain to the individual case-that is,
the specific disorder affecting thepatient and its likely
prognosis-and coun-selling issues for the family, such as the
iden-tification of individuals who may developsymptoms in later
life (presymptomatic test-ing) or risks for the inheritance of the
disor-der by a future family member (prenataltesting and carrier
detection). To date therehave not been equivalent advances in
ourtherapeutic options in the management ofthese conditions
although experimental pro-tocols have been initiated with this in
mind,some of which show promising results in ani-mal models.The
disorders and the relevant molecular
genetic analyses under consideration are dis-cussed in two
groups: those for which one ormore genetic loci have been
identified but thegene(s) not yet cloned; and those for whichthe
genes have been isolated and the relevantproduct characterised. We
begin by reviewingthe available data from epidemiological andfamily
studies on the frequency of thesedisorders.
Institute ofMedicalGenetics, UniversityofWales College
ofMedicine, Heath Park,CardiffCF4 4XN, UKJ C MacMillanP S
HarperCorrespondence to:Dr MacMillan
EpidemiologyIndividual genetic neurological diseases arenot
common but as a group they account fora significant burden of
disability in a generallyyounger age group than affected by
otherneurological diseases. In a review of reportspublished
throughout the world, Emery' esti-mated a population prevalence for
the inher-ited neuromuscular diseases of over 1 in3000. The
authors' study in southeast Wales2suggests a minimum prevalence for
the majorinherited neurological disorders of over 58per 100 000
population (approximately 1 in1700 population). Table 1 shows the
disor-ders and the prevalence of symptomatic indi-viduals in the
southeast Wales population.
These figures do not take into accountasymptomatic gene carriers
who may developclinical disease in the future; nor do theyallow for
the unaffected but "at-risk" familymembers who are also likely to
request infor-mation on the disease (this latter group aremore
likely to seek guidance from a geneticsunit but a not insignificant
number may beseen initially by the neurologist dealing withthe
index case).
Linkage analysisDISORDERS LOCALISED TO SPECIFICCHROMOSOMAL SITES
BUT NOT YET CLONEDThe number of disorders in this groupdecreases
monthly as a result of the continualisolation of new genes for
specific diseases.The technology used in "linkage analysis"merits a
brief description as it needs to beappreciated that there are
limitations to itsusefulness in many clinical situations.
Linkage analysis has been the first stage inthe localisation of
a gene responsible formany genetic disorders. It makes use
ofrestriction fragment length polymorphisms(RFLPs). These are
lengths of DNA thathave been cut at each end at a specific site
Table 1 Prevalence of major, single-gene neurological disorders
in southeast Wales
Disorder Prevalence (/100 000) 95% confidence interval
Hereditary motor and sensory neuropathy types I,JI,JII and V
12-9 10-7-15-4Myotonic dystrophy 7-1 5-5-9-1Duchenne muscular
dystrophy 9-6* 7-0-12-9Becker muscular dystrophy 5.0*
3-2-7-6Facioscapulohumeral muscular dystrophy 2-9 1-9-4-1Spinal
muscular atrophy (all types) 1-3 0-7-2-2Huntington's disease 8-4
6-6-10-5Tuberous sclerosis 1-6 0-9-2-6Von Hippel Lindau disease 0-6
0-2-1-4Hereditary spastic paraplegia 3-4 2-3-4-8Neurofibromatosis
type 1 13-3 11 1-158
*Per 100 000 males.
7
on March 29, 2021 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.57.1.7 on 1
January 1994. D
ownloaded from
http://jnnp.bmj.com/
-
MacMillan, Harper
recognised by a bacterial restriction endonu-clease enzyme.
Different enzymes recogniseand cleave at different DNA sequence
motifsof variable numbers of base pairs. The greatvariability in
human DNA results in differ-ences in the length of sequence
betweencleavage sites in unrelated individuals. Withina family,
however, these anonymous DNAsegments (RFLPs) are inherited in
amendelian fashion and can be trackedthrough a family pedigree
using standard lab-oratory techniques. Botstein et al3 first
sug-gested the use of these in the construction ofgenetic linkage
maps for the localisation ofdisease genes to particular segments of
chro-mosomes and they have superseded the bloodgroup polymorphisms
used in early studies.
In a family linkage analysis, each memberof the family is
assessed for the presence ofthe disease of interest and their
status(RFLP) for the marker locus is ascertained. Ifthe disease
locus and the marker locus areclose together on the same
chromosome(linked) then independent assortment atmeiosis will be
rare and both traits will beinherited in the offspring. The closer
they areto each other the less likely it is that they willseparate
during the pairing of homologouschromosomes at meiosis-in other
words,that a recombination will occur. The recom-bination fraction,
known as theta (0) gives anindication of the genetic distance
between thetwo loci. Genetic distance is expressed incentiMorgans
where 1 cM is defined as a seg-ment of chromosome with a 1% chance
ofrecombination per meiosis4 and this is equiva-lent to a 0 of
0.01. A recombination fractionof 0 5 means either that the two loci
are ondifferent chromosomes or that they are farapart on the same
chromosome.The successful application (accuracy) of
linkage analysis in the clinical situation isdependent on
several factors: it is crucial thatthe diagnosis is correct; and
the disease musthave been localised (mapped to a segment
ofchromosome) with close polymorphic mark-ers available. Affected
individuals should beheterozygous for the marker
polymorphisms("informative"), there should not (ideally) begenetic
heterogeneity (more than one diseaselocus for the clinical
phenotype), and thefamily relationships, especially paternity,must
be clearly established. The disease sta-tus for each individual
typed must be accu-rate (especially where the disease is of
lateonset and "unaffected" individuals are crucialto the analysis).
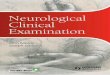
The figure shows a familytyped for a hypothetical two-allele
polymor-phism known to be linked to the disease ofinterest.
Individual I2 is affected by the disor-der and is heterozygous for
the polymorphism(she types 2-1); her unaffected spouse ishomozygous
(2-2) as is her unaffected sonIIL. Individual 13 is clinically
affected and hasinherited allele 1 from his mother, and
hassubsequently transmitted this allele to indi-vidual III,. This
three-generation situation isideally suited to linkage analysis as
phase isknown-that is, the chromosome carrying themutant gene can
be identified-and affected
i
LLanePerson
4..
i -
Figure The lanes in the autoradiograph contain DNAfrom the
individuals indicated in the pedigree. The DNAhas been digested
using a restriction endonuclease enzyme,subjected to
electrophoresis on an agarose gel andtransferred to a nylon
membrane. The DNA probe ofinterest has been labelled with
radioisotope and incubatedovernight with the membrane. The membrane
has beenstored at -200C adjacent to radiographic film for
sevendays. Bands are assigned numbers with the largest
banddesignated 1.
individuals are heterozygous for the polymor-phisms of interest.
It is possible to predict forindividual III3, who may be too young
for thedisease to have manifested, the likelihood thatthey will
develop the disease from a knowl-edge of their genotype. In this
situation thepresence of allele 1 indicates a high risk, theactual
value of which would depend on therecombination fraction between
the markerand the disease. In general it is unlikely that amarker
would be used whose rate of recombi-nation with the disease was
greater than 3%.In the example shown the actual value wouldbe 97%,
using a marker with 3% recombina-tion, as it is a fully informative
situation. Thisapproach can also be used to increase
thereproductive options for couples at risk bypermitting prenatal
diagnosis through linkageanalysis and, where affected, termination
ofan affected pregnancy. Individual III, in thefigure could
represent a conceptus fromwhich chorionic villus sampling would
pro-vide appropriate tissue for analysis in earlypregnancy.
Specific disordersTable 2 lists those diseases linked to
specificchromosomes, but with the gene not yet iso-lated, for which
family linkage studies canplay a useful role in patient and family
man-agement. It is not intended to be a compre-hensive list of all
mapped neurogeneticdiseases; the interested reader should
consultsources such as the bimonthly listings inNeuromuscular
disorders (Pergamon Press),the summaries of the Human GenomeMapping
Project annual meetings,
8
t.7---,
on March 29, 2021 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.57.1.7 on 1
January 1994. D
ownloaded from
http://jnnp.bmj.com/
-
Clinical genetics in neurological disease
Table 2 Chromosomal localisations for major genetic neurological
disorders for which thegene has notyet been cloned
Disorder Localisation(s)
Emery-Dreifuss muscular dystrophy Xq27 3-28Facioscapulohumeral*
muscular dystrophy 4q35Familial spastic paraplegia (one dominant
type) 14qFriedreich's ataxia 9ql3-21Limb-girdle muscular dystrophy
(dominant) 5q22-3-31-3Spinal muscular atrophy recessive types I, II
and III 5ql 1-2-13*3Tuberous sclerosis (see also table 3) 9q34
Gene locations are identified by the chromosome number followed
by an indication of whicharm (p = short, q = long) and the
sub-band.*But see below for comments on the molecular rearrangement
reported in this disorder.
McKusick's Mendelian inheritance in man(published and "online"
versions) and peri-odic reviews.5
It may be possible to provide presympto-matic testing for these
disorders for relativesat risk if the family structure is suitable
butthe presence of genetic heterogeneity, as intuberous sclerosis,
can make even this verydifficult in all but the largest families.
VariousBayesian approaches have been proposed totake such
additional factors into accountwhen counselling individuals in
these situa-tions.6
Although the gene for facioscapulohumeral(FSH) muscular
dystrophy has not yet beencloned, it is possible to make diagnostic
useof molecular DNA analysis where it isthought that an affected
individual representsa new dominant mutation for the disorder.This
paradoxical situation arises as the resultof the presence of
detectable rearrangementsassociated with a series of 3-2 kb
tandemrepeat elements in the subtelomeric region ofthe long arm of
chromosome 4.7 (1 kb =1000 base pairs.) The DNA probe pl3E-1
1(locus D4F104S1) detects bands over 50 kbin size after EcoRI
digestion in normal indi-viduals and a band less than 35 kb in
lengthin individuals with FSH dystrophy. In mostcases thought to
represent new mutations, itis possible to show that both parents
possesstwo normal-sized alleles whereas the affectedindividual has
one normal-sized and onerearranged fragment.Some disorders, mostly
rare, have not yet
been mapped to a specific chromosome(s)and genetic management is
confined to coun-selling families on the inheritance and natureof
the disease.
Mutation analaysisOnce a gene associated with a particular
dis-ease has been isolated it becomes possible totest DNA samples
from affected individualsfor mutations within that gene. These
maytake the form of point mutations that substi-tute alternative
nucleic acid bases and resultin changes in the amino-acid sequence
(mis-sense mutations) or introduce stop codonswith premature
truncation of the translationproduct (nonsense mutations). Other
muta-tions may involve the insertion or deletion ofa number of base
pairs (from one to manythousands) resulting in disruption of the
nor-mal function of the gene. Occasionally dele-
tions or duplications of whole chromosomesegments are found in
association with spe-cific disorders. In addition to these
"classical"types of mutation, we have seen in the pasttwo years,
the identification of a new class ofmutation that is often unstable
in its trans-mission between generations. This is the
trin-ucleotide repeat, the principal characteristicof which is
instability, giving varying molecu-lar and clinical changes in the
differentaffected members of a single kindred, as dis-cussed more
fully below.
Mutation analysis has the advantage (overlinkage analysis) that
it is not dependent onfamily structure and can therefore be
appliedto an isolated case of a disorder suspected tobe genetic. A
variety of laboratory techniquesare used in the detection of
mutations8 and itmay take several weeks for a specific defect tobe
identified, depending on whether themethod is in regular service
use or still at theresearch stage.
DISORDERS FOR WHICH THE RESPONSIBLEGENE HAS BEEN
CHARACTERISEDTable 3 lists some of those disorders forwhich the
gene responsible has been identi-fied and mutation analysis is
feasible (thespecial situation for facioscapulohumeralmuscular
dystrophy has been mentionedabove). The number of disorders in this
cate-gory is increasing rapidly and individualgenetic units cannot
be expected to provideevery analysis. In the United Kingdom,
theclinician primarily responsible for the individ-ual patient's
care should consult their localgenetics unit for information on
which molec-ular services are available locally and thosewhich can
be obtained elsewhere (usuallyfrom other genetic laboratories in
theNational Health Service). It should bestressed that a
comprehensive genetic coun-selling service should be available to
all indi-viduals on whom a molecular genetic analysisis undertaken.
This is particularly relevantwhere specific mutation analysis is
requestedbut the individual has not been aware that thedisorder may
be hereditary. The analyses mayhave significant implications for
siblings oroffspring. Examples of these difficulties aregiven below
in respect of specific disorders.
In several disorders listed, a single, or verysmall number, of
distinct mutations in thesame gene are responsible for the same
phe-notype: thus in Leber's hereditary optic neu-ropathy (LHON) a
point mutation at basepair 11 778 (in the gene for subunit 4 of
thereduced nicotinamide adenine dinucleotide(NADH) dehydrogenase
(ND4) complex inthe respiratory chain) of the mitochondrialgenome
accounts for 50% of cases, whereasother causative mutations giving
an identicalclinical picture occur at base pairs 3460 (inND1), 4160
(ND1) and 15 257 (cytochromeb).9 Mutation analysis in this
situation there-fore requires careful planning and interpreta-tion.
Recent work has suggested that somemitochondrial mutations may be
synergistic-for example, mutations at base pairs 13 708,15 257, 15
812 and 5244-and the accumu-
9
on March 29, 2021 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.57.1.7 on 1
January 1994. D
ownloaded from
http://jnnp.bmj.com/
-
MacMillan, Harper
Table 3 Cloned genes, their products, functions and
mutations
Disease Chromsonal Gene Mutationslocalisation product Function
Mutation identified (%/6)
DMB/BMD Xp21 Dystrophin Cytoskeletal protein Deletions,
duplications 50Point mutations
Neurofibromatosis type 1 17ql 1-2 Neurofibromin Tumour
suppressor Deletions 20Point mutations
Neurofibromatosis type 2 22ql 1 Merlin Tumour suppressor
Deletions 50Point mutations
Tuberous sclerosis (one type) 16pl3 Tuberin Tumour suppressor
Deletions UncertainMyotonic dystrophy l9q13 2 Myotonin Protein
kinase Expanded trinucleotide
repeat sequence 100Huntington's disease 4pl6-3 Huntingtin
Unknown Expanded trinucleotide
repeat sequence 99Charcot-Marie-Tooth disease
type 1A 17pll 2 PMP-22 Myelin protein Duplication
-
Clinical genetics in neurological disease
X mental retardation syndrome associatedwith a cytogenetically
detectable fragile site atXq27T3 (FRAXA), the expanded sequencelies
5' (upstream) to the coding sequence. Itappears that in this
disorder there is a criticaldegree of expansion beyond which there
issilencing of gene expression'6 possibly due tohypermethylation
within the gene'7 and it isthis deficiency that is responsible for
the dis-ease phenotype. In the fragile X syndromewith a fragile
site at Xq28 (FRAXE), there isamplification of a GCC repeat with
associ-ated hypermethylation of the neighbouringCpG island (a
region associated with anactive gene) implying a similar disease
mech-anism to that seen in FRAXA.18 In myotonicdystrophy it has
been shown that the level ofmyotonin protein kinase messenger mRNA
isreduced when the mutant allele has less than200 repeats and very
low when there are 800repeats.'9 In congenital cases it has
beenreported that not only is no mutant mRNAdetectable but also
that there is a reducedlevel of the normal paternal mRNA.20Another
group has, however, reported anincrease in the level of mutant mRNA
in con-genital cases.2' This conflict needs to beresolved.A
specific characteristic of this type of
mutation is its instability; the length of therepeat sequence
tends to increase as it under-goes successive meiotic passages (as
it passesfrom one generation to the next). Inmyotonic dystrophy
this successive expansionaccounts for the long debated phenomenonof
anticipation whereby the clinical manifes-tations (phenotype)
become more severe insubsequent generations. It does not,
however,account for the observation that congenitalcases of
myotonic dystrophy are always bornof affected mothers.
These trinucleotide repeat amplificationsare quantitative
mutations and have been thesubject of several studies examining
correla-tions between degree of amplification and theage at onset
of symptoms.22 The questionarises as to whether it is possible to
predictthe age at disease onset and severity of thedisease
phenotype knowing the degree ofexpansion in the DNA sequence.2' We
wouldcaution against attempting this in a specificclinical
situation. Although there is a cleardistinction between the degree
of expansionin congenital cases of myotonic dystrophyand late
onset/minimal manifesting individu-als, such as cataract only,
there is consider-able overlap in other situations, even withinthe
same family.
Phenotype prediction on the basis ofdegree of sequence expansion
inHuntington's disease is fraught with evenmore difficulties: we
have shown that theindividual variation in age at onset for a
givenrepeat number can range over a span of20-30 years24 and, in
addition, that the size ofthe repeat sequence on the normal
paternalallele has an effect in maternally transmitteddisease.25
This may account for the largervariability in age at onset in
sibships with dis-ease of maternal compared with paternal ori-
gin. As with any inherited disorder, the dis-ease-specific
mutation is acting within theindividual's unique (with the
exception ofidentical twins) genetic background whichmay contain
several modifying loci. It couldwell be argued that the lack of a
clinically use-ful correlation has potential benefits to
anindividual requesting presymptomatic testing:the psychological
well being of an individualand his or her family would be unlikely
to behelped by foreknowledge of a precise age atonset of this
devastating disorder.
HEREDITARY MOTOR AND SENSORYNEUROPATHY TYPE IIn considering the
applicability of moleculargenetic testing, the case of type I
hereditarymotor and sensory neuropathy (HMSN I)illustrates some of
both the benefits and limi-tations of using direct mutational
analysis inthe clinical situation. HMSN type I (alsoknown as
Charcot-Marie-Tooth disease type1) is an autosomal dominant
condition withextreme variability in phenotype. The mani-festations
range from significantly reducedperipheral nerve conduction
velocity (medianmotor conduction velocity
-
MacMillan, Harper
sis). One situation that has been clarified withmutation
analysis for CMT1/HMSN I is thecase of the isolated, affected
individual whomay be considered to have the autosomalrecessive form
of HMSN I. Hoogendijk et aP9have shown that in nine out of 10
isolatedcases of HMSN I (in whom both parentswere clinically and
electrophysiologically nor-mal), the disorder had arisen from a de
novoduplication occurring in one of the parentalgerm cells. The
risk to subsequent offspringof such an affected individual is
clearly 50%(and not "minimal" as may previously havebeen
counselled) whereas the risk to siblingsof such patients would be
minimal (this maybe modified in some cases by gonadalmosaicism in
the parent) rather than the pre-viously counselled 25%. Counselling
of aduplication-negative isolated male caseremains difficult in
view of the possibility thathe has the X-linked form of CMT.
Hayasakaet alP0 have recently reported the identificationof point
mutations in the gene for Po, anotherintegral membrane protein of
peripheral ner-vous system myelin, in individuals withCMTlb. Where
this complexity of situationoccurs there is much to be said for the
con-tinued application of standard clinical screen-ing protocols
(measurement of motor nerveconduction velocities and sensory
nerveaction potentials) for individuals at risk inaddition to
direct molecular analysis.
Considerations when requestingmutation analysisIn myotonic
dystrophy, Huntington's diseaseand Charcot-Marie-Tooth type 1 (HMSN
I)the success of mutation analysis makes ittempting to expand the
range of the clinicalpicture that prompts the dispatch of a
bloodsample for "DNA analysis". We have alreadystated our view
that, before any sample istaken, the patient should be made aware
ofthe potential genetic implications of a "posi-tive" result. This
may not cause undue anxi-ety if the individual believes other
familymembers show similar signs already, or he orshe perceives the
disorder not to be undulyserious.
Three disorders merit closer examinationin considering the
clinical spectrum thatshould prompt a "DNA analysis":Huntington's
disease; Alzheimer's disease;and prion dementia. All may manifest
withprogressive dementia with or without addi-tional features.
Should we therefore screen allcases of dementia for the specific
mutationsassociated with these disorders? Several prob-lems arise
in considering this.
Firstly, there is the question of consent.Can the patients be
made aware of the impli-cations of a positive result or should
theirfamilies make the decision on their behalf?After all it is
they (the family) who will bemost affected by such a result.
Secondly, the sensitivity of the analysisshould be considered.
In those situationswhere we believe this to be approaching
100% (Huntington's disease) the family canbe reassured by a
negative result. In familialAlzheimer's disease, however, there is
geneticheterogeneity, and the available molecularanalysis (looking
for point mutations in theAPP gene) would screen only one
geneaccounting for a small proportion of cases.3'A negative result
would not therefore excludea diagnosis of familial Alzheimer's
disease.Screening DNA from patients with dementiafor mutations in
the prion protein gene asso-ciated with Gerstmann-Straussler
syndromeand familial Creutzfeldt-Jakob disease would,superficially,
seem reasonable in view of thereported cases where dementia is the
onlymanifestation.'2The implications for the siblings and off-
spring of a patient with an identifiable prionmutation are,
however, less clear. Whereas anasymptomatic gene carrier for
Huntington'sdisease has approaching a 100% likelihood ofdeveloping
clinical manifestations (barringother causes of death), there are
currentlyonly limited data with which to counsel anasymptomatic
carrier of a prion gene muta-tion; Collinge et al give an empiric
risk of95%." Any reservations on the application ofthese mutation
analyses in a dementedpatient would be removed should an
effectivetreatment become available.
There have been no reservations, however,in applying molecular
analyses of the dys-trophin gene and its product, despite
theknowledge that a positive result identifies anuntreatable
disorder. Hoffman et al34 haveshown that at least 10% of women with
amyopathy and raised plasma creatine kinaseconcentration have an
identifiable abnormal-ity in the dystrophin gene or the
dystrophinprotein, or both. The perceived benefit thatthese women
and their families can now becounselled on the appropriate risks of
recur-rences would appear to have been justifica-tion enough for
testing.The availability of analyses for the trinu-
cleotide repeat amplification in the androgenreceptor gene in
bulbospinal neuronopathy35and mutations in the copper/zinc
superoxidedismutase gene (SOD 1)36 in some familieswith autosomal
dominant motor neuron dis-ease, makes feasible the screening of
isolatedindividuals (especially males) with motorneuron disease. We
are of the opinion that,whereas screening for the androgen
receptorgene trinucleotide repeat expansion is valu-able (a normal
result excludes Kennedy's dis-ease), SOD1 analysis in the absence
of asignificant family history is not an appropriateuse of
laboratory services.
Table 4 shows the mutation analyses thatwe consider should be
available to neurolo-gists as part of a regional molecular
geneticservice and the clinical situations in which wefeel the
request is appropriate. Fragile X (typeA) mutation analysis is
usually requested bypaedialricians when faced with a child
withdevelopmental delay but could be added tothis list. It would
however, add considerablyto the workload and would require
appropri-ate additional staff.
12
on March 29, 2021 by guest. P
rotected by copyright.http://jnnp.bm
j.com/
J Neurol N
eurosurg Psychiatry: first published as 10.1136/jnnp.57.1.7 on 1
January 1994. D
ownloaded from
http://jnnp.bmj.com/
-
Clinical genetics in neurological disease
Table 4 Clinical indications for specified mutation analyses
Mutation analysis Clinical indication
Dystrophin gene "Limb girdle" dystrophy with raised CK*Raised
neonatal creatine kinase
CMT1A duplication Demyelinating neuropathyMyotonin-kinase CTG
repeat Muscular dystrophy with myotoniaIT1 5 CAG repeat Adult onset
chorea
Juvenile rigid syndromeLHON mutations Acute bilateral optic
atrophyMELAS/MERRF mutationst Myoclonic epilepsy, proximal myopathy
with appropriate
histology, young stroke victims
*Ethically approved research protocol.tOn DNA extracted from
blood and muscle.LHON = Leber's hereditory optic neuropathy; MELAS
= mitochondrial myopathy,encephalopathy, lactic acidosis,
stroke-like episodes; MERRF = myoclonus epilepsy withragged-red
fibres.
The issue of which cases should be referredto a clinical
geneticist in conjunction with therequest for a specific mutation
analysis shouldbe addressed locally, taking into considera-tion the
available staffing levels (see below)and the specific interests of
the clinicians.Access to diagnostic molecular servicesshould not be
limited by the availability of aclinical geneticist, although it
should be astandard of acceptable practice that theappropriateness
of the request for mutationanalysis should be discussed with a
geneticscolleague whenever possible.Once a positive result has been
generated
the clinician is duty bound to transmit thisinformation to the
patient and, with his or herconsent, to the family. Clinical
neurologistswill often find this a most useful time toengage the
help of their clinical genetics col-leagues, if they were not
approached initiallyto advise on what molecular test may havebeen
applicable. Extended family counsellingon the nature and
implications of a specificdiagnosis is often time consuming and
mayinvolve other health professionals such as spe-cialist genetics
nurses and clinical psycholo-gists if presymptomatic testing is
requested bysiblings or offspring.
SITUATIONS WHERE MUTATION ANALYSIS ISINAPPROPRIATEWe are also
aware of the situations where amolecular DNA test should not be
under-taken. The most obvious situation is wherethe patient does
not want it. This is no differ-ent from an individual declining a
test forHIV carrier status. Most other situationsoccur where
presymptomatic testing isrequested and these will usually be
directedtowards the geneticist. Practising neurologistsshould be
aware of these situations, however,as family members may approach
them ini-tially, following the diagnosis of a heritabledisorder in
the patient. Occasionally, an indi-vidual at risk for an inherited
disorder mayapproach a neurologist with symptoms unre-lated to the
genetic disease. In this situation itwould not be appropriate to
offer specificmutation analysis. What is less clear is themerit of
mutation analysis in the presence ofvague symptoms which may be
diseaserelated, such as clumsiness or forgetfulness,where there is
a family history ofHuntington's disease. The identification of
adisease-specific mutation in this situation may
not offer a definitive explanation for the indi-vidual's
symptoms.Many inherited neurological disorders have
onset in mid to later life and presymptomatictesting of children
for these is not appropri-ate.37 This would change should
effectivetherapy to prevent clinical disease becomeavailable.
Individuals should not be underpressure from third parties, such as
insurancecompanies, to test and those requesting test-ing should be
made aware of the possibleinterests of such parties in the outcome.
Itmay be useful to consider what impact a posi-tive test would have
on one's own family andsocial situation to gain an appreciation of
thepossible consequences for the individual inquestion.
Susceptibility genesThis article has focused on those
neurologicaldisorders whose aetiology is primarily "singlegene" and
where advances in our knowledgehave followed the isolation of that
gene. Inmany of the most prevalent neurological dis-orders
(multiple sclerosis, idiopathic epilepsy,stroke) there may be a
significant geneticcomponent, as recognised from familial
clus-tering of cases or from twin studies, butwhere true mendelian
inheritance is not seen.Attention is now focusing on the
identifica-tion of "susceptibility genes" which may pre-dispose an
individual to the development ofthese conditions. Harding et aP8
have pro-posed that mitochondrial loci may be impli-cated in the
susceptibility to develop multiplesclerosis. It has long been
recognised thatthere is a higher frequency of specific
HLAhaplotypes in individuals with multiple scle-rosis, suggesting
additional immunologicalfactors (reviewed in reference 39). It is
notknown how relevant any single susceptibilitylocus will turn out
to be, nor how amenableto modification this predisposition will be
inan individual.We are in no doubt, however, that individ-
uals with these disorders and their familieswill in future
expect to receive counselling onthe genetic contribution to disease
suscepti-bility and advice on strategies for modifyingtheir risks.
We are equally convinced thatsociety will require considerable
education onthe relevance of these factors, if individualswho have
been identified to be at increasedrisk are not to be discriminated
against ineducation, employment, and insurance.Legislative
intervention may be necessary toavoid the creation of a genetically
stigmatisedsubpopulation.
Applying molecular analysisSAMPLESMost analyses are carried out
on DNA iso-lated from peripheral blood lymphocytescollected in
containers with EDTA as an anti-coagulant. A sample of 20 ml of
bloodprovides sufficient DNA for all analyses.Where polymerase
chain reaction technologyis used, considerably less is required, so
that
13 on M
arch 29, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.57.1.7 on 1 January
1994. Dow
nloaded from
http://jnnp.bmj.com/
-
MacMillan, Harper
the dried blood spot on a Guthrie card maybe adequate. Some
mutations may be tissuespecific (such as some mitochondrial
genemutations) and the appropriate sample willbe required if a
false-negative result is to beavoided. Transportation of blood
using thefastest available postal service (approximatelytwo days
delay) is adequate provided thatarrangements have been made with
the recip-ient laboratory to expect the sample. Tissuesuch as
muscle biopsy specimens may requiresnap freezing in liquid
nitrogen, especially ifRNA analysis is required, and again
thisshould be discussed with the unit undertakingthe analysis.
SERVICESThe availability of a comprehensive moleculargenetic
laboratory service is essential if one isto make optimal clinical
use of the advancesoutlined in this review. The pace at
whichmutation analysis is becoming feasible forgenetic disorders in
general, precludes anysingle diagnostic unit from providing such
aservice and many laboratories have imple-mented consortium
arrangements to enablethe widest possible range of services to
beavailable. Single gene neurological disordersdo, however, account
for 54% of all clinicalreferrals to regional genetic units40 and
itwould seem appropriate that a core molecularneurogenetic
diagnostic service should beavailable at a regional level.We feel
that the minimal provision should
include molecular analyses for the trinu-cleotide repeat
expansions associated withmyotonic dystrophy and Huntington's
dis-ease, the CMT1A duplication, a deletionscreening protocol for
Duchenne and Beckermuscular dystrophies, a core
mitochondrialmutation screen (see table 4) and linkageanalysis for
the autosomal recessive spinalmuscular atrophies of childhood. The
work-load generated at a regional level should beable to be handled
by two trained laboratoryscientific officers working alongside
col-leagues carrying out other analyses.Additional analyses will
generally be availableby negotiation with other units.
TheLaboratory and National ConsortiumDirectory, compiled by the
ClinicalMolecular Genetics Society, lists by diseaseand centre the
services available throughoutthe United Kingdom. This publication
alsoindicates the target times by which a resultshould be available
(these vary by disease andcentre).The provision of a clinical
service to com-
plement the molecular analyses is essential.As we discussed
above, it will often be neces-sary to undertake extended family
counsellingwhen a genetic diagnosis is made. Most dis-tricts will
have access to the services of a clini-cal geneticist and a
specialist genetic nurse,who will be able to provide such a
service. Wefeel that, in addition, there should be, at aregional
level, the provision of a clinical spe-cialist with training in
both clinical neurologyand clinical and molecular genetics.
Thisindividual would be able to offer an optimal
clinical service for patients and colleagues andprovide informed
interpretation of relevantmolecular DNA analyses.
ConclusionsMolecular genetic studies have begun to elu-cidate
the pathobiological mechanisms under-lying many of the inherited
neurologicaldisorders. Improved diagnostic accuracyenables a more
accurate prognosis to be givento the patient and facilitates
appropriategenetic counselling for the family unit. It islikely
that more effective therapy will followfor some of these disorders
but the prospectof a "cure", as perceived by the patient,remains a
matter of speculation. This shouldnot prevent individuals and their
familiesbenefiting from the advances made to date.
We wish to thank Dr M Upadhyaya for useful discussions onthe
molecular genetics of facioscapulohumeral musculardystrophy, S
Cochran, unpublished data on CMTX, Dr LLazarou for the
autoradiograph used in the figure and Mr PDavies for discussions on
the feasibility of the estimatedlaboratory workload. JC MacMillan
is supported through agrant from the Muscular Dystrophy Group of
Great Britainand Northern Ireland.
1 Emery AEH. Population frequencies of inherited neuro-muscular
diseases-a world survey. Neuromusc Disord1991;1: 19-30.
2 MacMillan JC, Harper PS. Single gene neurological disor-ders
in South Wales; an epidemiological study. AnnNeurol
1991;30:411-4.
3 Botstein D, White RL, Skolnick M, Davis RW.Construction of a
genetic linkage map in man usingrestriction fragment length
polymorphisms. Am Jf HumGenet 1980;32:314-31.
4 Haldane JBS. The combination of linkage values and
thecalculation of distances between loci of linked factors. JGenet
1919;8:299-309.
5 Harding AE. The DNA laboratory and neurological prac-tice. J
Neurol Neurosurg Psychiatry 1993;56:229-33.
6 Daniels RJ, Suthers GK, Morrison KE, et al. Prenatal
pre-diction of spinal muscular atrophy. JT Med Genet1992;29:
165-70.
7 Wijurenga C, Frants R, Hewitt J, et al. Molecular geneticsof
facioscapulohumeral muscular dystrophy. NeuromuscDTsord, 1993, in
press.
8 Rossiter BJF, Caskey CT. Molecular studies of humangenetic
disease. FASEBJ_ 1991;5:21-7.
9 Shoffner JM, Wallace DC. Mitochondrial genetics:Principles and
practice. Am J Hum Genet 1992;51:1179-86.
10 Brown MD, Voljavec AS, Lott MT, MacDonald I,Wallace DC.
Leber's hereditary optic neuropathy: Amodel for mitochondrial
neurodegenerative disease.FASEB J 1992;6:2791-9.
11 Koenig M, Beggs AH, Moyer M, et al. The molecularbasis for
Duchenne versus Becker muscular dystrophy:Correlation of severity
with type of deletion. Am J HumGenet 1989;45:498-506.
12 Bradley DM, Parsons EP, Clarke AJ. Experience withscreening
newborns for Duchenne muscular dystrophyin Wales. BMJ
1993;306:357-60.
13 Matsumura K, Tome FMS, Collin H, et al. Deficiency ofthe 50K
dystrophin-associated glycoprotein in severechildhood autosomal
recessive muscular dystrophy.Nature 1992;359:320-2.
14 Matsumura K, Nonaka I, Campbell KP. Abnormalexpression of
dystrophin-associated proteins inFukuyama-type congenital muscular
dystrophy. Lancet1993;341:521-2.
15 Upadhyaya M, Shen M, Cherryson A, et al. Analysis ofmutations
at the neurofibromatosis 1 (NFI) locus. HumMol Genet
1993;1:735-40.
16 Pieretti M, Zhang F, Fu YH, et al. Absence of expressionof
the FMR-1 gene in fragile X syndrome. Cell199 1;66:817-22.
17 Scott Hansen R, Gartler SM, Scott CR, Chen S, LairdCD.
Methylation analysis of CGG sites in the CpGisland of the human
FMR1 gene. Hum Mol Genet1992;1:571-8.
18 Knight SJL, Flannery AV, Hirst MC, et al. Trinucleotiderepeat
amplification and hypermethylation of a CpGisland in FRAXE mental
retardation. Cell 1993;74:127-34.
19 Fu YH, Friedman DL, Richards S, et al. Decreasedexpression of
myotonin-protein kinase messanger RNAand protein in adult form of
myotonic dystrophy.
14 on M
arch 29, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.57.1.7 on 1 January
1994. Dow
nloaded from
http://jnnp.bmj.com/
-
Clinical genetics in neurological disease
Science 1993;260:235-8.20 Hofmann-Radvanyi H, Lavedan C, Rabes
J-P, et al.
Myotonic dystrophy: absence of CTG enlargedtranscript in
congenital forms, and low expression of thenormal allele. Hum Mol
Genet 1993;2:1263-6.
21 Sabouri LA, Mahadevan MS, Narang M, Lee DSC, SurhLC, Korneluk
RG. Effect of the myonic dystrophy(DM) mutation on mRNA levels of
the DM gene.Nature Genet 1993;4:233-8.
22 Harley HG, Rundle SA, MacMillan JC, et al. Size of
theunstable CTG repeat sequence in relation to phenotypeand
parental transmission in myotonic dystrophy. Am 7Hum Genet
1993;52:1164-74.
23 Suthers GK, Huson SM, Davies K. Instability versus
pre-dictability: the molecular diagnosis of myotonic dystro-phy. J
Med Genet 1992;29:761-5.
24 MacMillan JC, Snell RG, Tyler A, et al. Molecular analy-sis
and clinical correlations of the Huntington's diseasemutation.
Lancet 1993;342:954-8.
25 Snell R, MacMillan JC, Cheadle JP, et al. Relationshipbetween
trinucleotide repeat expansion and phenotypicvariation in
Huntington's disease. Nature Genet 1993;4:393-7.
26 MacMillan JC, Upadhyaya M, Harper PS. Charcot-Marie-Tooth
disease type la (CMT1A): evidence fortrisomy of the region pl 12 of
chromosome 17 in southWales families. J Med Genet 1992;29:12-3.
27 Suter U, Welcher AA, Ozcelik T, et al. Trembler mousecarries
a point mutation in a myelin gene. Nature 1992;356:241-4.
28 Valentijn LJ, Baas F, Wolterman RA, et al. Identical
pointmutations of PMP-22 in Trembler-J mouse andCharcot-Marie-Tooth
disease type 1A. Nature Genet1992;2:288-9 1.
29 Hoogendijk JE, Hensels GW, Gabreels-Festen AAWM, etal.
De-novo mutation in hereditary motor and sensoryneuropathy type I.
Lancet 1992;339:1081-2.
30 Hyasaka K, Takada G, Ionasescu V. Mutation of the
myelin Po gene in Charcot-Marie-Tooth neuropathytype 1 B. Hum
Mol Genet 1993;2:1369-72.
31 Fidani L, Rooke K, Chartier-Harlin M-C, et al. Screeningfor
mutations in the open reading frame and promoterof the ,B-amyloid
precursor protein gene in familialAlzheimer's disease:
identification of a further familywith APP717 Val-Ile. Hum Mol
Genet 1992;1:165-8.
32 Collinge J, Harding AE, Owen F, et al. Diagnosis
ofGerstmann-Straussler syndrome in familial dementiawith prion
protein gene analysis. Lancet 1989;334: 15-7.
33 Collinge J, Poulter M, Davis MB, et al.
Presymptomaticdetection or exclusion of prion protein gene defects
infamilies with inherited prion diseases. Am J Hum
Gent1991;49:1351-4.
34 Hoffman EP, Arahata K, Minetti C, et al.Dystrophinopathy in
isolated cases of myopathy infemales. Neurology 1992;42:967-75.
35 La Spada AR, Wilson M, Lubahn DB, Harding AE,Fischbeck KH.
Androgen receptor gene mutations in X-linked spinal and bulbar
muscular atrophy. Nature199 1;352:77-9.
36 Rosen DR, Siddique T, Patterson D, et al. Mutations inCu/Zn
superoxide dismutase gene are associated withfamilial amyotrophic
lateral sclerosis. Nature 1993;362:59-62.
37 Harper PS, Clarke A. Should we test children for
"adult"genetic diseases? Lancet 1990;335:1205-6.
38 Harding AE, Sweeny MG, Miller DH, et al. Occurrenceof a
multiple sclerosis-like illness in women who have aLeber's
hereditary optic neuropathy mitochondrialDNA mutation. Brain
1992;115:979-89.
39 Jersild C, Grunnet N. Demyelinating disease. In Thegenetic
basis of common diseases. King RA, Rotter JI,Motulsky AG, eds.
Oxford: Oxford University Press,1992; 753-74.
40 Rona RJ, Swan AV, Wilson OM, et al. DNA probetechnology:
implications for service planning in Britain.Clin Genet
1992;42:186-95.
15 on M
arch 29, 2021 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.57.1.7 on 1 January
1994. Dow
nloaded from
http://jnnp.bmj.com/