Embed Size (px)
Citation preview
IronDeficiencyandNeurologicalConsequencesforChildren
ClinicalPediatrics&PediatricSurgeryJune2017
DawnSHartfieldBScMed,MPH,MD,FRCPCAssociateProfessor
DepartmentofPediatricsCollegeofMedicineandDentistry
UniversityofAlbertaEdmonton,Alberta,Canada
PresenterDisclosure
• Relationshipswithcommercialinterests:• Grants/ResearchSupport:None• SpeakersBureau/Honoraria:None• ConsultingFees:None• Other:None

Objectives:• Understandtheepidemiology,etiology,andconsequences
ofirondeficiency
• Understandbrainironmetabolismandtheimpactofitsdeficiencyonthedevelopingbrain
• Identifyneurologicalconditionswhichareassociatedwithirondeficiencytoensurepromptdiagnosisandtreatment
• 24.8%ofpopulation(1.62billion)• Highestinpre-schoolagedchildren47.4%(CI:45.7-49.1)• School-agedchildren25.4%(CI:19.9-30.9)• Pregnantwomen41.8%(CI:39.0–43.8)
• CanadianEstimates:• Pre-schoolagedchildren7.6%(CI:1.6–28.9%)• Pregnantwomen11.5%(CI:2.4-40.9%)
deBenoistBetal.,eds.Worldwideprevalenceofanaemia 1993-2005.WHOGlobalDatabaseonAnaemia Geneva,WorldHealthOrganization,2008.http://www.who.int/vmnis/anaemia/prevalence/summary/anaemia_data_status_t2/en/
GlobalEpidemiologyofAnemia
HowCommonisIronDeficiency?
• Morecommonindevelopingcountries• Alsooccursinindustrializednations
• Edmontonstudyof32,06912to59montholdchildrenMay2002-June2008
• 7.69%of19month-oldchildrenhadIDA;11.65%IDPaediatricsandChildHealth.2009May/June;Vol14Suppl14A:44A
• Canadianhighriskpopulations- excessof50%• Mostvulnerable- poorest,youngest,leasteducated,female-athighestrisk
WhatCausesofIronDeficiency?• Life-stages
• Menarche• Infancy/earlychildhood
• Nutritionaldeficiency• Culturalpractices• Parasites
• Hookworm• H.Pylori
HowisIronUtilized?• Ironexistsastwopools:
• Storediron(2/3)• Functionaliron(1/3)
• Hemoglobin70%• Transportiron25%• Myoglobin4%• Enzymerelated1%
• BiochemicaleffectsofID• DECREASED:
• Hemeproteins• Ironcontainingenzymes• Ironascofactor
WhyisIronImportant?
• Vitalmicronutrient• Hormones• Neurotransmitters• RNAandDNAmetabolism• Myelinproduction• energymetabolism
• Productionofhemoglobin
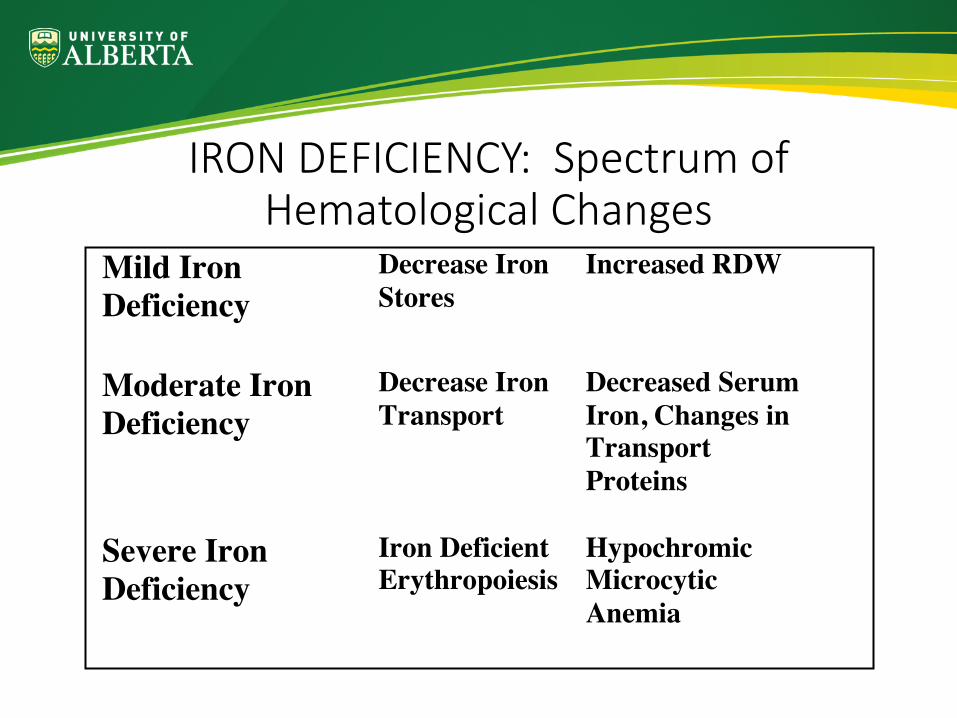
IRONDEFICIENCY:SpectrumofHematologicalChanges
Mild Iron Deficiency
Decrease Iron Stores
Increased RDW
Moderate Iron Deficiency
Decrease Iron Transport
Decreased Serum Iron, Changes in Transport Proteins
Severe Iron Deficiency
Iron Deficient Erythropoiesis
Hypochromic Microcytic Anemia
EnsuringAdequateIronIntakeisImportant
• Ironmaintainsnormalcellularfunction
• Deficiencyeffectseveryorgansystem
• Mostobviousclinicaleffectisanemia
• Criticaltodiagnoseandtreatearlyinchildren
IRONINTHEDEVELOPINGBRAIN
BrainIron• Ironentersbrainviareceptormediatedendocytosis• 50%ofbrainironisacquiredduringthefirst3weeksoflife• Transportwithinbrainpoorlyunderstood
• Mostassociatedwithtransferrin,ferritin,lactoferrin,enzymes• “Free”ironhasbeenimplicatedinthepathophysiologyofanumberofbraindiseases
• Distributionisuneven• Presentingreyandwhitematter• Mostcommonlyfoundinoligodendrocytes
• Normaloligodendrocytes,brainiron,andirontransportarerequiredformyelinproductionandmaintenance
IronDeficiencyandtheDevelopingBrain• Decreasedbrainironandferritin
• Compensatoryincreaseintransferrin• Non-homogeneousdecreaseinbrainiron
• AbnormalMyelination• Ironisacofactorforlipidandcholesterolbiosynthesis• Ratswithprenatalandlactational irondeficiencyhaveadelayedrateofmyelinationandhypomyelination
• NeurochemicalAbnormalities• GABA,dopamine,serotonin,phenylalanine
• AbnormalNeurodevelopment• Ratandmurinemodels- irreversible changesinmotorandcognitivedevelopment
• Ratmodel- associationbetweenirondeficiencyandSNHL• Hippocampus– disruptedplasticity
NeurologicalConsequencesofIronDeficiencyinChildren
DEVELOPMENTALDELAY
DEVELOPMENTALABNORMALITIES
• IDnegativeimpactoncognition,behaviorandmotorskills• ID,IDAandnon-IDanemiacancausecognitivedefectsatanyage
• Hemoglobinlevelcorrelatestocognitiveperformance• Impactofirontherapytoimprovecognitivefunctionisunclear
• LozoffandcolleaguesfollowedacohortofCostaRicanchildrenfrominfancytoadolescencetodeterminetheearlyeffectsofirondeficiencyonchildhooddevelopment
FIRSTSTUDY:Infantsandtoddlers• 191wellinfants12to23months• Baseline,1&12wk posttherapylabworkandBSID• InfantswithmoderatetosevereIDAhadlowerbaselineMDIandPDIscores
• 1week- nochangeinMDIorPDIscores• 12weeks- moderatetosevereIDA
• lackofcorrectionofironstoreswithcorrectionofanemia(25/34patients)correlatedwithpersistenceoflowerMDIandPDIscores
• Irontherapytocorrectanemiaaloneisnotadequatetocorrectneurodevelopmentaldisturbances
Conclusion:Early,severe,chronicirondeficiencyismorelikelytoresultinneurodevelopmentalabnormalitiesPediatrics1987;79:981-995
SECONDSTUDY:School-AgeChildren• Follow-upstudyat5yearsofagetodetermineeffectsofirondeficiencyininfancyonlaterdevelopment
• Retentionrate:85%•Allhadnormalgrowthandnutritionalstatus•moderatelysevereanemiaininfancyresultedinsignificantlylowerscoresonmentalandmotortesting
CONCLUSION:Childrenwithirondeficiencyanemiaininfancyareatriskforlong-lastingdevelopmentalsequelaeNEJM1991;325:687-694
THIRDSTUDY:Adolescents• Longitudinalfollow-uptodetermineeffectsofirondeficiencyininfancyonlaterintellectualfunctioning
• Retentionrate:87%• Adolescencewithmoderatelysevereirondeficiencyininfancy:
• hadlowertestscoresinnumerousareas• morelikelytohaverepeatedagrade/receivedtutoring• morebehaviorproblems
CONCLUSION:Severechronicirondeficiencyininfancyidentifieschildrenatriskforabnormalitiesinbehavior,cognitionandmotorskillsmorethantenyearsafterirontherapyPediatrics2000;105(4):1-11
HOWDOESIRONDEFICIENCYRESULTINDEVELOPMENTALDELAY?
• Alterationsinhippocampus• Mitochondrialdamage• Abnormalmyelination• Neurotransmitterabnormalities
• Braindopaminemetabolism• Behavioralabnormalitiesduetoirondeficiencyimpairlearningcapability
NeurologicalConsequencesofIronDeficiencyinChildren
CEREBROVASCULAREVENTS
HowCommonareCerebrovascularEventsinChildren?
• Incidence:2- 3/100000childrenperyear• Noetiologyfound
• 20- 36%ischemicstroke• 16%hemorrhagicstroke
• Manycasereportsandlargerstudiesdemonstrateanassociationbetweenirondeficiencyandpediatricstrokeinotherwisewellchildren
IRONDEFICIENCY:ACAUSEOFSTROKEINCHILDREN• Retrospectivereviewofchildrenfromtheneonatalperiodtoage15yearswhopresentedwithstrokebetween1985and1995.
• 53patientsdiagnosed• 2.5/100000childrenperyear
• 16/53(30.2%)noetiologyfound• 6/16(37.5%)withetiologyundeterminedwereirondeficient(p<0.01)
• Ofthesechildren:• Allwere6- 18months• Allhadamildviralillness• Notallwereanemic• Notallhadthrombocytosis
CONCLUSION:• Anassociationbetweenirondeficiencyandpediatricstrokeexistsinchildren6to18monthsofageinthesettingofanonspecificviralillness
Hartfield et al. Pediatric Neurology 1997;16(1)50-53
Furtherworkinthisarea:• Azabetal.AnnHematol2014;93(4):57:1-6
• Case-controlstudyof21patientswith100controls• Healthychildrenwithstrokewere3.8timesmorelikelytohaveIDA(p=0.005)• RecommendearlydetectionofIDAforpreventionofhealthproblems
• Maguireetal.Pediatrics2007;120:1053-1057• Case-controlstudyof53patients12-38months• otherwisehealthchildrenwere10timesmorelikelytobeirondeficient• accountedformorethan50%ofstrokeinthecohort• Concludedthatirondeficiencyisariskfactorforstrokeinchildren
• Sebireetal.Brain2005;128:477-489• Studyof42patientswithSVTfrom4strokeregistries• 55%hadanemia;50%hadID• Morecommoninotherwisehealthchildren(p=0.07)• Concluded- nutritionaldeficiencymodifiableriskfactor
MechanismofIDandStroke
• Thrombocytosissecondarytoirondeficiency• Irondeficiencyleadstoahypercoagulablestate• AnemicHypoxia• Abnormalitiesinmitochondrialfunction
NeurologicalConsequencesofIronDeficiencyinChildren
FEBRILESEIZURE
FebrileSeizures
• 2-5%ofchildrenupto5yearsofage• Peakageis18months- similartoID
• Knownriskfactors:• Genetics,fever>39.4celsius,particularinfections,day-careattendance,lowbirthweight,neonatalstay>30days,maternalsmokinginpregnancy
• Susceptibilityofdevelopingbraintoseizuresrelatedtomaturationalchangesinexcitatoryandinhibitoryneurotransmitters
• Inappropriateresponsetocytokinesassociatedwithinfection
RoleofIronDeficiencyinFebrileSeizures
RelevantStudies:• OnestudyfoundIDtodecreasetheriskoffebrileseizuresinchildren
• KobrinskyNL,YagerJY,CheangMS,etal.JChildNeurol.1995(2):105-109
• SixstudiesfoundIDtoincreasetherisk• SharifM,etal.GlobalJofHealthSci20168(2):185-189• PapageorgiouV,etal.EurJPaediatrNeurol201519(5):591-6• Hartfieldetal.ClinicalPediatricsFebruary200948(4):420-426• RehmanN,BillooSG.JCPSP,2005(5):338-340• DaoudAS,BatiehaA,Abu-EkteishF,etal.Epilepsia,2002(7):740-74• PisacaneA,SansoneR,ImpagliazzoN,etal.BMJ,1996(313):343-344
• Difficultieswiththesestudies:• Somearesmallstudies• DiagnosticcriteriausedtodiagnoseID/IDA
• Ironstudiesinaccurateinthesettingoffebrileillness
Consensus:
• Irondeficiencyisariskfactorforfebrileseizure• ChildrenwithfebrileseizuresshouldbescreenedforID/IDA
• Avoidironstudieswhileacutelyunwell
NeurologicalConsequencesofIronDeficiencyinChildren
BREATHHOLDINGSPELLS
BreathHoldingSpells• Occurin27%ofchildren• Proposedtobeduetoautonomicdysregulationandvagallymediatedcardiacarrestwithcerebralanoxia
• IronDeficiencyexacerbatesBHSas:• Anemiadecreasesoxygencarryingcapacitycausingcerebralanoxia• IDchildrenaremoreirritablewhichincreaseslikelihoodofaBHS• Ironisacofactorintheenzymesthatdegradecerebralcatecholamines
• Autonomicdysregulation• Abnormalityinneurotransmitterfunction
IronTherapyandBreathHoldingSpells• Consideredrandomised/quasi-randomised studies• Comparedironsupplementationwithplaceboornotherapyforchildren<18yearswithBHS
• Reductioninfrequencyorseverityorboth• RESULTS:
•2studieswith87children• Irondecreasedfrequency(OR76.4895%CI:15.65-373.76,P<0.00001)
•Meta-analysissolelyexaminedironcausingcompleteresolutionmaintainsignificance(OR53.45:95%CI6.57-434.57,P=0.0002)
• CONCLUSION:• IrontherapyiseffectiveinthetreatmentofBHS
Cochranereview:Zehetner Aetal.CochraneDatabaseSyst Rev201012(5)
• Prospectivestudyof100children6-26monthswithBHS
• 73%resolutionand23%had50%reductioninBHS
• 3mg/kg/dayofironfor12weeks• Factorspredictingpoorresponseonunivariateanalysis:
• Frequencyofattacksandintoleranceofiron• Responseratenotpredictedbypresenceofanemiaorironstatus
Conclude:IrontherapyiseffectivetherapyinBHSregardlessofironstatusJain R et al. J of Paediatr Child Health 2017 June 1 ePub
IsIronTherapyAppropriateforBHSforChildrenWithoutAnemia?
• Investigate for IDA
• Treat those with IDA and ID
• For those without ID/IDA• More research needed!• Discuss risks/benefits of therapy• Trial 3 mg/kg/day• Monitor side-effects
How to Approach Children with BHS?
NeurologicalConsequencesofIronDeficiencyinChildren
OtherLessCommonProblems
IronandDysphagia• Plummer-VinsonSyndromeiswelldescribedinadults
• Rarereportsinchildren- youngest5years• Treatmentisiron• Dysphagiaresolvespriortowebs/rings
• AdultscomplainoforalpainwhenID• Esophagealmanometry(adults)
• AbnormalinIDadultswithdysphagiawithoutwebs/rings
• AnimalmodelsofID• AbnormalesophagealmusclestructureinID• NitricOxide
• requiredfornormalsmoothmusclefunction/peristalsis• decreasedasproductionisirondependent
IDANDDYSPHAGIA:IMPLICATIONSFORINFANTS
• ToddlersdevelopIDAasconsumeexcessivemilk• Typicallyrefusesolids• Mostlythoughtofasa“parenting”issue
• Newhypothesis:MildIDresultsinoralpainanddysphagia.Thiscausesfeedingdysfunction,whichperpetuatestheIDstate.Rapidlyreversiblewithirontherapy
• Supportedbyadultandanimalstudies• WarrantsfurtherstudyHartfield.ClinicalPediatrics,February2010
RecognizedandRare
•Pseudotumorcerebri• Irondeficiencyrecognizedcauseofpseudotumorcerebrisincethe1800’s
• Pathophysiologyuncertain• Tissuehypoxialeadstocerebraledema• AbnormalhemodynamicsresultinincreasedCBFresultinginincreasedICP
• Depletioniniron-containingenzymesmayhaveeffect
• Reversiblewithirontherapy•Cranialnervepalsy
NewandEmerging
•ADHD• Abnormalitiesindopaminergicfunction• Metaanalysis- lowserumferritinandnotironassociatedwithADHD
WangYetal.PLoS One201712(1)
•RestlessLegSyndrome• PublicationsimplicateIDasacontributortoRLS• Meta-analysisofirontherapy– insufficientevidencetodeterminebenefit
Trotti LMetal.CochraneDatabaseSysRev2012May16(5)
Conclusions• Ironisrequiredfor:
• Braindevelopment• Myelination• Neurotransmitterproduction• Hemoglobinsynthesis
• Deficiencyassociatedwithavarietyofneurologicalproblems
Preventionofirondeficiencythroughoutgestation,infancyandchildhoodisimperativefornormalneurodevelopment
andtopreventotherimportantcomplicationsofirondeficiency
StrategiestoPreventIronDeficiency• ScreenandtreatpregnantwomenforID
• Moreprevalentinwomenofchildbearingage• Delayedcordclamping• Ensureappropriatedietatearlycheck-ups
• Ironcontainingfoodintroducedby6months• Avoidcow’smilkuntil1yearofage• Breastfeedorformulawithironbeforethen
• Screenhighriskinfantsandchildren• Indigenous,immigrants,prematureinfants
• Remember- parasitesandH.Pyloricontribute• Timelytherapywithdiagnosis





























