Embed Size (px)
Citation preview

CLINICAL GASTROENTEROLOGY
GEORGE Y. WU, SERIES EDITOR
For further volumes:http://www.springer.com/series/7672

ChronicViral HepatitisDIAGNOSISAND THERAPEUTICS
Second Edition
Edited by
KIRTI SHETTY, MDGeorgetown UniversityMedical Center, Washington, DC
and
GEORGE Y. WU, MDUniversity of ConnecticutHealth Center, Farmington, CT, USA

EditorsKirti Shetty, MD George Y. Wu, MDGeorgetown University Hospital, 2 Main University of Connecticut3800 Reservoir Road, NW Health CenterWashington DC 20007 236 Farmington [email protected] Farmington CT 06030-1845
ISBN 978-1-934115-81-7 e-ISBN 978-1-59745-565-7DOI 10.1007/978-1-59745-565-7Springer Dordrecht Heidelberg London New York
Library of Congress Control Number: 2009921504
c© Humana Press, a part of Springer Science+Business Media, LLC 2001, 2009All rights reserved. This work may not be translated or copied in whole or in part without thewritten permission of the publisher (Humana Press, c/o Springer Science+Business Media, LLC,233 Spring Street, New York, NY 10013, USA), except for brief excerpts in connection withreviews or scholarly analysis. Use in connection with any form of information storage andretrieval, electronic adaptation, computer software, or by similar or dissimilar methodology nowknown or hereafter developed is forbidden.The use in this publication of trade names, trademarks, service marks, and similar terms, even ifthey are not identified as such, is not to be taken as an expression of opinion as to whether or notthey are subject to proprietary rights.While the advice and information in this book are believed to be true and accurate at the date ofgoing to press, neither the authors nor the editors nor the publisher can accept any legal responsi-bility for any errors or omissions that may be made. The publisher makes no warranty, express orimplied, with respect to the material contained herein.
Printed on acid-free paper
Springer is part of Springer Science+Business Media (www.springer.com)

I wish to dedicate this book to mystudents and patients who have taughtme so much and to my family who makethis all worthwhile. K.S.
I would like to dedicate this book to myfamily for their patience, our studentswho inspire us, and especially RoyLopata, Sigmund, and Jenny Walder whohave been so supportive for our efforts inresearch, teaching, and treating liverdisease. G.Y.W.

PREFACE
Since the publication of the first edition in 1991, a great deal of newinformation has become available regarding pathogenesis and treatmentof chronic viral hepatitis. While the armamentarium for use againstviral hepatitis has expanded, especially for the treatment of hepatitisB, in many ways the evaluation and therapeutic decision making hasbecome more complex. Problematic issues not previously addressedinclude the appearance of resistance, side effects some of which are irre-versible, and their management. Chronic viral hepatitis still affects hun-dreds of millions of people worldwide, and millions more new infec-tions occur every year. This edition is intended to provide the read-ership with the most current information, concentrating on clinicallyuseful practical information and new advances in diagnostic and ther-apeutic technology. Special attention is devoted to reactivation of hep-atitis B with chemotherapy and immunosuppression, herbal and non-traditional therapies, HCV extrahepatic manifestations and their treat-ment, chronic viral hepatitis in the pediatric population, and immunol-ogy and immunotherapy of HCV.
As in the previous edition, the authors have strived to make thisvolume focused on clinically relevant information, presented in apractical and convenient format. It has been a pleasure to work withthis group of expert authors in producing this volume. We hope thereaders will find the information useful and helpful.
Kirti ShettyGeorge Y. Wu
vii

CONTENTS
Preface . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . vii
Contributors . . . . . . . . . . . . . . . . . . . . . . . . . . . . xi
Molecular Virology of Hepatitis B and C: Clinical Implications . . . 1Marcy Coash and George Y. Wu
Epidemiology, Risk Factors, and Natural History of ChronicHepatitis C . . . . . . . . . . . . . . . . . . . . . . . . . . . . 33
Nalini K. Sharma and Averell H. Sherker
Current and Future Therapy of Chronic Hepatitis C . . . . . . . . 71Mohammad Ashfaq and Gary Davis
Hepatitis C in Special Populations . . . . . . . . . . . . . . . . . 97Douglas Dieterich, Marie-Louise Vachon
and Damaris Carriero
Extrahepatic Manifestations of Chronic Hepatitis C Infection . . . . 135Douglas Meyer and Henry C. Bodenheimer Jr.
Anti-HCV Agents in Development . . . . . . . . . . . . . . . . . . 159Ketan Kulkarni and Ira M. Jacobson
Epidemiology, Screening, and Natural History of ChronicHepatitis B Infection . . . . . . . . . . . . . . . . . . . . . . . 185
Shiv K. Sarin and Manoj Kumar
Current Treatment of Chronic Hepatitis B . . . . . . . . . . . . . 243Walid S. Ayoub and Emmet B. Keeffe
Management of Patients Co-Infected with ChronicHepatitis B (CHB) and the Human ImmunodeficiencyVirus (HIV) . . . . . . . . . . . . . . . . . . . . . . . . . . . 259
Edward Doo and Marc Ghany
Management of Antiviral Resistance in Chronic Hepatitis B . . . . . 273Edward Doo and Marc Ghany
ix

x Contents
Herbal and Non-Traditional Therapies for Viral Hepatitis . . . . . . 289Veronika Gagovic and Paul Kwo
Hepatitis B Reactivation in the Setting of Chemotherapyand Immunosuppression . . . . . . . . . . . . . . . . . . . . . 307
Halim Charbel and James H. Lewis
Support of Patients During Antiviral Therapyfor Hepatitis B and C . . . . . . . . . . . . . . . . . . . . . . 337
Alyson N. Fox and Thomas W. Faust
Viral Hepatitis, A Through E, In Pregnancy . . . . . . . . . . . . 353Eashen Liu and Jacqueline Laurin
Chronic Viral Hepatitis and Liver Transplantation . . . . . . . . . 375Kirti Shetty
Treatment of Viral Hepatitis in Children – 2008 . . . . . . . . . . . 405Zachary R. Schneider and Parvathi Mohan
Viral Hepatitis and Hepatocellular Carcinoma . . . . . . . . . . . 431Jorge A. Marrero
Hepatitis B Vaccines . . . . . . . . . . . . . . . . . . . . . . . . 449Oren Shibolet and Daniel Shouval
T-Cell-Mediated Immunity and Immunotherapy of ChronicHepatitis C . . . . . . . . . . . . . . . . . . . . . . . . . . . . 471
Richard C. Duke, Alex Franzusoff and David Apelian
Index . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 491

CONTRIBUTORS
DAVID APELIAN, MD, PHD • GlobeImmune, Louisville, COMOHAMMAD ASHFAQ, MD • Baylor University Medical Center,
Dallas, TXWALID S. AYOUB, MD • Stanford University, Palo Alto, CAHENRY C. BODENHEIMER • Albert Einstein College of Medicine,
New York, NYDAMARIS CARRIERO, MD • Mount Sinai School of Medicine,
New York, NYHALIM CHARBEL, MD • Georgetown University Medical Center,
Washington, DCMARCY COASH, MD • University of Connecticut Health Center,
Farmington, CTGARY DAVIS, MD • Baylor University Medical Center, Dallas, TXDOUGLAS DIETERICH, MD • Mount Sinai School of Medicine,
New York, NYEDWARD DOO, MD • National Institutes of Health, Bethesda, MDRICHARD C. DUKE, PHD • GlobeImmune, Louisville, COTHOMAS W. FAUST • University of Pennsylvania, Philadelphia, PAALYSON N. FOX • University of Pennsylvania, Philadelphia, PAALEX FRANZUSOFF, PHD • GlobeImmune, Louisville, COVERONIKA GAGOVIC • Indiana University School of Medicine,
Indianapolis, INMARC GHANY, MD • National Institutes of Health, Bethesda, MDIRA M. JACOBSON, MD • Weill Medical College of Cornell
University, New York, NYEMMETT B. KEEFFE, MD • Stanford University, Palo Alto, CAKETAN KULKARNI, MD • Weill Medical College of Cornell
University, New York, NYMANOJ KUMAR, MD • G. B. Pant Hospital, New Delhi, IndiaPAUL KWO • Indiana University School of Medicine, Indianapolis, INJACQUELINE LAURIN, MD • Georgetown University Medical Center,
Washington, DCJAMES H. LEWIS, MD, FACP, FACG • Georgetown University Medical
Center, Washington, DC
xi

xii Contributors
EASHEN LIU, MD • Georgetown University Medical Center,Washington, DC
JORGE A. MARRERO, MD, MS • University of Michigan, AnnArbor, MI
DOUGLAS MEYER, MD • Albert Einstein College of Medicine,New York, NY
PARVATHI MOHAN • Children’s National Medical Center,Washington, DC
SHIV K. SARIN, MD • G.B. Pant Hospital, New Delhi, IndiaZACHARY R. SCHNEIDER • Children’s National Medical Center,
Washington, DCNALINI K. SHARMA, MD • Washington Hospital Center,
Washington, DCKIRTI SHETTY, MD, FACG • Georgetown University Medical Center,
Washington, DCAVERELL H. SHERKER, MD, FRCP (C) • Washington Hospital
Center, Washington, DCOREN SHIBOLET, MD • Hadassah-Hebrew University Hospital,
Jerusalem, IsraelDANIEL SHOUVAL, MD • Hadassah-Hebrew University Hospital,
Jerusalem, IsraelMARIE-LOUISE VACHON, MD • Mount Sinai School of Medicine,
New York, NYGEORGE Y. WU, MD, PHD • University of Connecticut Health Center,
Farmington, CT

Molecular Virology of HepatitisB and C: Clinical Implications
Marcy Coash, MD and George Y. Wu,MD, PhD
CONTENTS
INTRODUCTION
HEPATITIS B VIRUS
HEPATITIS C VIRUS
CONCLUSION: FUTURE TREATMENT
STRATEGIES
ACKNOWLEDGMENTS
REFERENCES
Key Principles
• HBV and HCV are hepatotropic, noncytotoxic viruses.• Both viruses mutate rapidly to produce quasispecies.• HBV, but not HCV, can integrate into the host genome.• Both viruses require viral and host proteins for replication.• Few animal models for HBV and HCV are available.• Specialized features of viral replication may offer targets for new
antiviral agents.
1. INTRODUCTION
Despite fundamental differences in genome structure, hepatitis B(HBV) and C (HCV) viruses use many of the same strategies to achieve
From: Clinical Gastroenterology: Chronic Viral Hepatitis,Edited by: K. Shetty and G. Y. Wu, DOI 10.1007/978-1-59745-565-7 1,
C© Humana Press, a part of Springer Science+Business Media, LLC 2001, 2009
1

2 Coash and Wu
high-level replication and persistence of infection in hepatocytes. Thelimited genome size of these viruses necessitates an efficient use ofhost cell machinery to carry out viral gene expression. This strongdependence on virus–host interactions restricts HBV and HCV celltropism to the hepatocytes of higher primates and previously precludedtheir reliable and reproducible propagation in cell culture. Recent stud-ies have begun to overcome this experimental limitation, so as to permita more complete understanding of the molecular basis for viral repli-cation, and the concomitant induction or evasion of the host antiviralimmune response. Some of the important molecular biological proper-ties of these viruses, as well as how they are reflected in the clinicalmanifestations of viral infection, are presented below.
2. HEPATITIS B VIRUS
HBV is a member of the Hepadnavirus family, a group of hepa-totropic mammalian and avian DNA viruses, which replicate via reversetranscription of a full-length genomic RNA intermediate carried outby reverse transcriptase activity present in the viral DNA polymerase(1–3). The frequency of mutation during HBV genome replication is10-fold higher than the normal rate for DNA viruses due to the fact thatRTs do not correct errors of transcription. HBV populations may evolvemore quickly than most DNA viruses as a result of environmental fac-tors allowing the development of viral HBV mutants. Diversification ofHBV strains has produced genotypes, subgenotypes, and HBsAg sub-types. They have emerged in specific populations and migrated withtheir hosts to other areas of the world. Based on sequence divergence inthe entire genome of >8%, human HBV strains have been classified intoeight genotypes (A–H), further divided into 24 subgenotypes that differby at least 4% from each other. Additionally, nine different serologicsubtypes exist as determined by HBsAg epitopes. Each of the variousgenotypes exhibits a characteristic serotype profile and geographicaldistribution, allowing an evaluation of HBV phylogenetic evolution andpossible genotypic influence on the natural course of HBV infection (4).The sequencing of clinical isolates has even been used as an epidemio-logical marker to trace routes of transmission.
HBV infection is highly cell type- and species-specific: hepatocytesof the great apes are the only confirmed site of HBV replication.Reported infection of other cell types, e.g., lymphocytes, is controver-sial and generally thought to be of little clinical relevance. The lackof infection models to study the mechanisms of hepadnaviral entryand disease has been a significant problem in the past. Other hepad-naviruses, particularly duck and woodchuck hepatitis viruses, provided

Molecular Virology of Hepatitis B and C: Clinical Implications 3
convenient model systems for HBV infection and associated liver dis-ease. With regard to cell culture models for HBV, recently primaryhepatocytes from tree shrews, i.e., Tupaia belangeri, and a humanhepatoma cell line (HepaRg) have been demonstrated to have suscep-tibility for HBV infection, the latter upon induction of differentiationin vitro (5). Besides the chimpanzees, which are extremely expensiveand in short supply, a SCID mouse model based on primary humanhepatocytes (PHH) and more recently an immunocompetent humanhepatocyte-tolerant rat model have been described (6–8).
2.1. Structure of HBVHBV is a 42-nm-coated DNA virus with a partially double-stranded
3.2-kb genome. The virion is composed of a nucleocapsid covered withthe envelope proteins. The nucleocapsid, or core particle (also knownas Dane particle), is a 27-nm icosahedron made up of the core proteinHBcAg, an incomplete double-stranded viral DNA, and a DNA poly-merase. The envelope is composed of lipids derived from the host incombination with the viral surface antigen (HBsAg), which is madeup of three related proteins (S, M, L), variably glycosylated. ExcessHBsAg can aggregate to form noninfectious quasispherical particles20 nm in diameter as well as tubular structures 22 nm in diameter(9, 10).
2.2. Replication CycleHBV commonly achieves infection in virtually 100% of the hep-
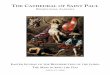
atocyte population. The HBV replication cycle is complicated. Viralentry involves various components of the large and middle HBsAg pro-teins and annexins as well as other hepatocellular membrane proteins.Following entry into the host cell, the virus uncoats and the 3.2-kbpartially double-stranded (pdsDNA) HBV genome is transported tothe nucleus and converted by host RNA polymerase to a covalentlyclosed circular (cccDNA) template, which is then organized intoviral minichromosomes from which all viral mRNAs are transcribed,including the pregenomic RNA (pgRNA), which is essential for HBVreplication (Fig. 1). Although the viral genome is a 3.2-kb partiallydouble-stranded DNA molecule, it is generated by the reverse tran-scription of a longer-than-genome length 3.5-kb pregenomic RNA (11).The pgRNA is translated to produce the core protein and DNA poly-merase and plays a role in nucleocapsid formation. The viral pgRNAtranscript, encompassing the entire genome sequence, is subsequentlyencapsidated and reverse-transcribed into the pdsDNA form by a viralDNA polymerase, which functionally resembles that of a retrovirus.

4 Coash and Wu
Fig. 1. HBV life cycle. After cell entry, HBV nucleocapsids transport the par-tially double-standed circular genomic HBV DNA to the nucleus, where theDNA is converted into covalently closed circular (ccc) DNA. The cccDNAfunctions as the template for the transcription of four viral RNAs, which areexported to the cytoplasm and used as mRNAs for the translation of the HBVproteins. The longest pregenomic RNA also functions as the template for repli-cation, which occurs within nucleocapsids in the cytoplasm. Nucleocapsidsare enveloped during their passage through the ER or Golgi complex and aresecreted through the cell. Adapted from Rehermann et al. (45).
Although direct cytopathic liver injury is seen under conditions of veryhigh viral load—as in fibrosing cholestatic hepatitis, a rare conditionobserved in some patients with recurrent posttransplantation hepatitisB—the virus itself is generally noncytolytic. Rather, HBV-associatedinjury is attributed to the lysis of infected hepatocytes by the hostimmune response (12).
2.3. Cellular EntryVirion endocytosis, uncoating, and nuclear transport of the pdsDNA
genome remain poorly understood, although the host cell contribu-tion to these events is believed to be a major determinant of HBV-cell

Molecular Virology of Hepatitis B and C: Clinical Implications 5
tropism. Interaction of the viral envelope protein with a specific cellsurface receptor is considered the initial step of HBV infection. Asidefrom host-derived phospholipids, the envelope of an HBV virion con-tains virus-derived (S), (M), and (L) surface proteins that are translatedfrom distinct initiation codons, but share a common carboxyl domain.A generally accepted view is that the pre-S domain which resides on theN-terminal domain of the LHBs of the HBV envelope protein, specif-ically residues 21–47, is involved in mediating HBV attachment to aviral receptor on hepatocytes. The putative cellular receptor of HBV isstill an enigma in the field of HBV research although studies with duckhepatitis B virus suggest the involvement of a carboxypeptidase recep-tor. More than 10 proteins including interleukin-6, human squamouscell carcinoma antigen 1, immunoglobulin A receptor, asialoglycopro-tein receptor, transferrin receptor, apolipoprotein H, polymerized serumalbumin, annexin V, fibronectin and more recently lipoprotein lipasehave been demonstrated to interact with the HBV PreS or S proteins invitro and may be potential receptor candidates although none of themhas been experimentally proven to be the true receptor (13). Nuclearimport of pdsDNA may be facilitated by the covalently attached HBVpolymerase, or by the noncovalently associated capsid protein, whichbears a nuclear localization signal. Host components involved in thisnucleocytoplasmic transport have yet to be determined. Interestingly,the translocation event does not occur in transgenic mouse models ofHBV infection, despite the ability of mouse hepatocytes to support sub-sequent steps in HBV replication.
2.4. cccDNAThe mechanism by which HBV pdsDNa is converted to covalently
closed circular form is not known, but presumably involves hostcell DNA-repair pathways. Conversion of the relaxed circular DNAgenomes of the incoming virus to covalently closed circular (ccc) DNAwithin the nucleus of an infected hepatocyte is the first marker of aproductive infection, but is difficult to detect (14). Once formed, thecccDNA does not undergo semiconservative replication in the nucleus,as the intracellular HBV DNA pool can be supplemented only by reversetranscription in the cytoplasm, as described below. In contrast to serumHBV DNA which has a half-life of just 1–3 d, cccDNA is a remark-ably stable species in hepatocyte nuclei despite the fact that it is notintegrated into the cellular genome. It is resistant to direct elimina-tion by antiviral agents and serves as a reservoir for viral reactivationwhen antiviral therapy is interrupted. The half-life of infected hep-atocytes is quite long, 10–100 d or more, depending on the extentof liver injury. Accordingly, antiviral therapy with reverse transcrip-tase inhibitors requires an extended course of treatment to achieve

6 Coash and Wu
complete clearance, especially in mild disease with a relatively low rateof hepatocyte turnover.
2.5. TranscriptionIn contrast to other DNA viruses, HBV appears not to utilize posttran-
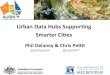
scriptional alternative mRNA splicing to maximize its coding capacity.Instead, HBV makes exquisitely economical use of its genome at thetranscriptional level by embedding regulatory elements—even overlap-ping open-reading frames (ORFs) (C, P, S, and X)—within concise pro-tein coding sequences for seven viral proteins (Fig. 2). Despite its smallsize, the HBV cccDNA genome is sufficient to direct the synthesis offour classes of RNA transcripts by host RNA polymerase II. A pair of–3.5-kb RNAs, differentially regulated by the core promoter, functionas templates for HBV DNA synthesis and serve as mRNAs for pre-core (HBeAg) which contains the full amino acid sequence of the coreprotein, and is not incorporated into the virus particle, but is secreted
Fig. 2. Structure of HBV DNA and genes. Four genes (S, C, X, and P)are encoded and these partially overlap. The pre-S gene is located upstream ofthe S gene and consists of the pre-S1 and pre-S2 genes. The precore region isupstream of the core gene.

Molecular Virology of Hepatitis B and C: Clinical Implications 7
in a soluble form by the infected cell, core (HBcAg), and polymerase(DNA-pol) proteins. The 2.4-kb and 2.1-kb pre-S1/pre-S2/S mRNAsencode the three envelope proteins. A 0.7-kb transcript directs the syn-thesis of the HBV X protein (HBxAg), which is a transactivator of virusreplication that is not incorporated into the virion. The mature viral par-ticle is composed of a single core protein, three envelope glycoproteins,and the viral DNA polymerase (2).
Transcription of each HBV RNA initiates from one or more uniquepromoters, which are regulated by two shared enhancer elements,EN I and II. Activity of liver-enriched transcription factors (TFs) atthese sites is thought to contribute to tissue specificity of HBV infec-tion, as the observed multifactorial cis-regulation of viral promoterstakes place only in well-differentiated liver cells (15). Additionally,the HBV genome also contains two 11-base direct repeats (DR1 andDR2) located at the 5′-end of both strands, a polyadenylation signal,and a site for glycocorticoid response (GRE). All transcripts termi-nate at a common polyadenylation signal, which is located in the coreORF. This signal is read-through during transcription of the prege-nomic RNA, generating a terminally redundant greater-than-genomelength transcript. Hepatitis delta RNA selectively inhibits transcriptionof pregenomic HBV RNA in vitro. This effect likely contributes to thefrequently observed precore antigen seroconversion in carriers superin-fected with HDV.
2.6. TranslationEfficient use of coding sequences, the hallmark of HBV biology, is
also apparent during translation. The surface antigens are generated bythree different in-phase start codons. Translation of the precore/coreORF originates from one of two in-frame start codons; initiation fromthe upstream site generates the precore polypeptide containing a signalfor secretion, which is posttranslationally modified to form the hepatitisB e-antigen. Translation of the polymerase gene initiates from an out-of-frame start codon located in the C-terminal coding region of the coreORF. The inefficiency of this unconventional and, as yet, poorly under-stood process yields a core:polymerase molar ratio of 250:1. Interac-tion between the HBV polymerase and the 5′-end of its own mRNA issufficient to block further translation and to precipitate the events ofgenomic replication.
2.7. Encapsidation and Reverse TranscriptionHBV RNA packaging and reverse transcription have been well char-
acterized (16). Among the viral transcripts made from cccDNA, the

8 Coash and Wu
3.5-kb pregenomic RNA (pgRNA) encodes the core and polymeraseproteins, and carries at its 5′-end a stem and loop structure known asepsilon that directs its encapsidation into the viral replication complex.The N-terminal domain of the polymerase protein binds to “epsilon”and is facilitated by host cell chaperones, such as p23 and heat-shockprotein (Hsp)70; inhibitors of Hsp90 have been shown to block HBVRNA packaging and subsequent DNA synthesis. Formation of thepolymerase–RNA complex triggers assembly of the viral nucleocap-sid. The capsid is composed of 120 disulfide-linked core dimers, whichcollectively bind RNA via a C-terminal domain of the core polypeptide.The N-terminal domain is responsible for core protein dimer formationand capsid assembly (17).
Reverse transcription occurs within the nucleocapsid, which con-tains small pores to allow influx of deoxynucleotides and othersmall molecules. Initiation of reverse transcription is accomplishedby a protein-priming mechanism, utilizing an amino-terminal tyrosineresidue of the polymerase and the epsilon structure as a replicationorigin. The C-terminal catalytic domains of the HBV polymerase pro-tein exhibit reverse transcriptase, DNA-dependent DNA polymerase,and RNase H activities. In the presence of requisite host cell chaper-ones, and possibly other cofactors, the polymerase carries out synthesisof viral pdsDNA and nearly complete degradation of the pregenomicRNA template. Phosphorylated metabolites of the antiviral compoundslamivudine, famciclovir, lobucavir, and adefovir dipivoxil inhibit thisstep of HBV replication by competing with deoxynucleotide triphos-phates for incorporation into HBV DNA, thereby causing prematuretermination of nascent polynucleotide chains.
One notable feature of the HBV polymerization process is its dis-continuous nature. pdsDNA synthesis requires dissociation of the poly-merase, and nascent DNA from the RNA template, and annealing toa homologous direct repeat sequence on the 3′-end of the pregenome.Polymerization from primers that fail to undergo template switching(“in situ priming”) results in the formation of double-stranded linear(dslDNA) genomes. Although illegitimate recombination events canconvert dslDNA into cccDNA, they may also cause integration of HBVsequences into host DNA.
2.8. IntegrationThe integration of the HBV DNA is apparently a common event that
occurs early during HBV infection even after acute self-limiting hepati-tis. It is not essential for the viral replication, but it allows persistenceof the viral genome. Transcription from integrated DNA accounts for

Molecular Virology of Hepatitis B and C: Clinical Implications 9
hepatitis B surface antigen HBsAg secretion observed in the absence ofviral replication. Even in the majority of patients who develop sponta-neous or treatment-induced HBeAg seroconversion and normalizationof aminotransferase (ALT) levels and histology, HBV DNA sequencescan be detected by PCR-based diagnostic tests. HBV dslDNA is likelythe predominant integrating species, although the gap structure in thepdsDNA may facilitate integration of this form as well. Commonly, thecore and polymerase genes are disrupted by integration, whereas theX and pre-S2/envelope ORFs remain intact. It has been demonstratedthat the regulatory proteins HBx and the pre-S2 activators that can beencoded by the integrant can exert a tumor promoter-like effect and leadto a selection of cells that produce a functional regulatory protein.
Integrated HBV DNA is found in the majority of HBsAg-positivehepatocellular carcinomas (HCCs). As with other viruses, these inte-grated viral genomes are characterized by rearrangements or partialdeletions. HBV integration can induce deletions in the host chromosomeat the integration site, as well as cause insertional mutagenesis, leadingto activation of a proto-oncogene or inactivation of a tumor suppressorgene in cis. In woodchuck hepatitis virus, there is evidence of specificactivation of the myc family of genes by this mechanism. In isolatedcases of human HCC, HBV insertion has been observed near cyclinA, retinoic acid receptor �, mevalonate kinase gene, sarco/endoplasmicreticulum calcium ATPase1 gene, and p53 loci. Integration in thesegenes can cause alterations in cellular signal transduction cascades, pro-liferation control, and cell viability. However, the HBV integration siteis apparently random, and integration of full-length HBV genomes doesnot commonly lead to transformation of cultured cells.
2.9. X Protein and HepatocarcinogenesisThe oncogenic potential of HBV integration likely derives from the
activation of host gene transcription in trans, rather than in cis (18).Truncated forms of the HBV pre-S/S envelope proteins may be formedas a result of integration. These exhibit potent transactivation in vitroand can stimulate the c-myc promoter, as seen in woodchuck hepatitisvirus-related HCC. Integrated HBV DNA isolated from tumor nodulespreferentially encompasses the X protein ORF. X is required for infec-tion in vivo, but is dispensable for viral replication in transfection-basedcell culture models. The X protein regulates transcription from viral andhost RNA polymerase I, II, and III promoters in vitro (19). AlthoughX has been shown to dimerize—a feature common to DNA-bindingTFs—it likely acts as a coactivator. X associates with a myriad ofhost cell proteins, including transcriptional regulators such as NF-�B,

10 Coash and Wu
AP-1, AP-2, c-EBP, ATF/CREB, and the calcium-activated factorNF-AT (20). It influences other TFs without binding them directly andso is thought to act by more global mechanisms, such as interactionwith general transcription factors (TFIIB, RNA polymerase subunit 5).
Among the multitude of cis-acting genetic elements responsive toX activity is HBV enhancer I: thus X may regulate its own syn-thesis. Enh I is responsive to many extracellular signals including12-O-tetradecanoylphorbol-13-acetate (TPA), okadaic acid, IL-6, andgenotoxic stimuli that are important in an acute inflammatory responseand cell proliferation in the liver. X-responsive host genes include manyinvolved in acute inflammatory and immune responses [e.g., majorhistocompatibility complex (MHC), tumor necrosis factor (TNF)-�1,interleukin (IL)-6, signal transduction, cell proliferation, and apopto-sis]. HBxAg sensitizes cells to TNF-� and is suspected to influenceother apoptotic pathways. Overall, the transcriptional regulatory effectsof X may contribute to viral persistence, increased cell turnover, andHBV-related hepatocarcinogenesis.
Distinct from its transactivation function, HBxAg may disrupt DNArepair and normal cell-growth regulation by direct interaction withhost regulatory proteins. X associates with a cellular factor called UV-damaged DNA-binding protein and downregulates nucleotide excisionrepair pathways. Sequestration by X protein also inhibits p53 nucleartranslocation and tumor suppressor activities, disrupting transcription-coupled repair mechanisms. Consequently, X may sensitize cells togenotoxic stimuli and promote integration events and overall geneticinstability common in HCC. Interestingly, HBxAg has been reported toexhibit endogenous adenosine monophosphate (AMP) kinase/ATPaseactivities and to colocalize with proteasome subunits, which may bemechanistically relevant to its observed effects on growth regulators.Stimulation of the Ras-Raf-mitogen-activated protein kinase pathwayand activation of protein kinase C, c-Src, and c-Fyn have been reportedin cell culture models of X expression. The retinoblastoma (Rb) tumorsuppressor is inactivated by hyperphosphorylation in the presence ofHBxAg.
In vitro and transgenic studies indicate that X promotes cell trans-formation and carcinogenesis, but only upon overexpression to levelswell beyond those typical of infected cells. Integration of X may leadto such overexpression, as subcellular localization studies indicate thatexpression of X from integrated templates leads to its accumulationand redistribution. Notably, an X-responsive bZip-family TF was foundto be overexpressed in HCCs. However, cell transformation has beenobserved with the expression of the X gene product N-terminal domain,which lacks the transactivation function altogether. Indeed, most of the

Molecular Virology of Hepatitis B and C: Clinical Implications 11
proposed actions of X have not been demonstrated in the context ofHCC-derived cells; it is possible that HBV-associated carcinogenesis issolely due to the induction of chronic hepatocellular necrosis and regen-eration. Given that HBV-related HCC is closely associated with cirrho-sis and that the peak incidence occurs 30–50 years after HBV infection,it is likely that the contribution of X expression alone is limited, relativeto other factors, such as the extent of immune-mediated pathogenesis.
2.10. Virion ProductionNewly synthesized pdsDNA may be imported into the nucleus,
resulting in the replenishment of the cccDNA pool, or secreted fromthe cells in virions. Completion of pdsDNA synthesis in some wayfacilitates nucleocapsid translocation into the endoplasmic reticulum(ER) and entry into the secretory pathway. The mechanism of this cou-pled maturation process is unknown, but may involve a conformationalshift in the nucleocapsid exterior. Other factors, such as a core proteinphosphorylation state or regulation by HBeAg, may influence the rel-ative rate of cccDNA accumulation and virion production. HBeAg hasbeen shown to slow HBV DNA replication in vitro by reducing HBcAgdimerization, thereby reducing encapsidation of pregenomic RNA andmay induce immunological tolerance. Secretion is also dependent onthe concentration of L envelope protein as the pre-S1 domain mediatesassociation of the envelope with core particles. Through budding, thenucleocapsid acquires a coating of the S, M, and L transmembrane pro-teins. Transport of virions through the Golgi apparatus results in thematuration of envelope proteins into N-glycosylated disulfide-linkedmultimers.
HBV is continuously released into the bloodstream, with a dailyproduction of up to 1011 enveloped virions. HBV surface proteinsare not only incorporated into virion envelopes, but they also budvery efficiently from intracellular post-ER pre-Golgi membranes. Theseenvelopes lacking enclosed nucleocapsids can be secreted at more thana 100-fold excess over virions, resulting in very high serum concentra-tions of “surface antigen particles” or subviral particles. Subviral par-ticles and virions have identical surface antigens (HBsAg), but theirprotein composition is not identical. Presumably the overproductionof HBsAg can influence the host immune response such that it isadvantageous for the virus acting as immunological decoys (17–20).Extrahepatic symptoms may result from deposition of antigen–antibodycomplexes formed when these particles are neutralized by anti-HBsAgantibodies.

12 Coash and Wu
2.11. Immune System EvasionInfection of a high percentage of hepatocytes is observed even in
acute, resolved cases, suggesting a delayed immune response to HBVantigens. Patients recovering from acute HBV infection exhibit humoralresponse to pre-S and S antigens, as well as vigorous, polyclonal cyto-toxic T lymphocyte (CTL) activity against multiple epitopes of HBVenvelope, core, and polymerase proteins. This response involves humanleukocyte antigen class II-restricted CD4+ helper T lymphocytes andCD8+ cytotoxic T lymphocytes However, given the large quantity ofhepatocytes infected and the rapid rate of clearance following transientinfection, it has been proposed that HBV nucleic acids can be eliminatedfrom infected hepatocytes by means other than direct CTL killing andreplacement by noninfected cells. cccDNA may be lost from cell nucleiduring mitosis. Additionally, the activation of an intracellular antiviralresponse by cytokines, such as TNF-�, interleukin-12, and interferons(IFNs) alpha and gamma, is known to induce noncytocidal loss of viralRNA and proteins. At high doses, TNF and interferons downregulatethe core promoter.
Immunotolerance of HBV antigens may play a central role in viralpersistence. Most infections in immunocompromised adults, and 90%of perinatal infections, progress to chronicity. These patients exhibitgenerally less severe liver disease than immunocompetent adults,despite higher viral load. The CTL and CD4+ T cell response in chron-ically infected patients is weak and restricted to relatively few epi-topes. Hepatitis B e-antigen is not essential for infection in vivo, butappears to play an immunosuppressive role contributing to the mainte-nance of high-level viremia. HBeAg bears an N-terminal signal peptideand is actively secreted. It has been proposed to cross-react with anti-bodies to core or antagonize the inflammatory Th1 response, therebysuppressing the host’s ability to generate a sufficient CTL attack oninfected hepatocytes. HBeAg may cross the placenta to establish T-celltolerance to HBV e- and core antigens setting the stage for perina-tally acquired chronic infection. Consistent with these proposed inter-actions, clearance of HBeAg during primary and chronic infections isfrequently associated with ALT flare-ups. HBV mutant strains defec-tive for e-antigen expression generally induce more severe immune-mediated liver injury than wild-type and are more likely to be clearedduring the acute phase of infection.
2.12. Viral MutationThe genetic stability of HBV is evidenced by the fact that each of
the major genotypes exhibits only a few of the possible HBsAg sub-

Molecular Virology of Hepatitis B and C: Clinical Implications 13
types. The development of effective anti-HBV vaccines has been greatlyfacilitated by the high degree of sequence conservation in neutraliza-tion epitopes (e.g., the “a” determinant, amino acids 99–169) of theHBV envelope proteins. Even the most divergent genotype, F, retainsapproximately 85% genomic sequence identity with other genotypes.Despite this, viral reverse transcriptases lack a proofreading functionand are inherently error prone, leading to frequency of HBV mutationsestimated to be 1.4–3.2 ×10–5 nt substitutions per site per year.
The remarkably low tolerance for mutations is most likely a con-sequence of the overlapping nature of the HBV genome, which dic-tates that a single-point mutation can affect multiple coding sequencesand/or regulatory elements. HBV quasispecies variability is prone tostronger conservatory constraints than RNA viruses that do not havenonoverlapping reading frames such as HCV and poliovirus. Nonethe-less, mutations in each of the four HBV genes have been clinically iso-lated, and these variants frequently arise in response to immune systemselection and antiviral therapy (21, 22). In several cases, the emergenceof a particular mutant is known to be contingent upon nearby wild-type sequences; therefore, HBV genotyping is valuable for the predic-tion and assessment of the clinical implications of viral mutation. Thisquasispecies distribution implies that if a newly generated mutationleads to a selective advantage for the virus, this will allow the corre-sponding viral population to overtake the other variants in a Darwinianmanner.
2.13. Immune-Escape MutantsThe emergence of HBV mutants has been implicated in vaccine fail-
ure and immune system evasion. Two major groups of mutations thatlead to a reduction or a blockade of HBeAg expression have been iden-tified. The common G-to-A transition at nucleotide 1896 results in astop-codon mutation causing premature translation termination of theprecore ORF, thereby preventing synthesis of HBeAg. Notably, thismutation is found in association with T1858, a sequence characteris-tic of HBV genotypes B–E, possibly because this pairing maintains sta-bility of the pregenomic RNA encapsidation signal. This mutation israrely found in genotypes A or F or in certain strains of HBV genotypeC. The relative rarity of this mutation in genotype A may contributeto the observed low perinatal transmissibility of HBV from healthyHBsAg carrier mothers in Northwestern Europe where genotype A pre-dominates. Precore mutants may replicate more efficiently than wild-type, but are most likely selected due to their ability to escape anti-HBe surveillance. Their pathogenic significance is unclear, as mixed

14 Coash and Wu
viremia brings about a complex set of dynamic interactions with thehost immune response (22).
The second group of mutations resulting in alteration of HBeAgexpression involves mutations affecting the basal core promoter occur-ring at nt 1762 and nt 1764. This results in reduced binding ofliver-specific transcription factors, transcribing fewer precore and coremRNA transcripts and, therefore, less precore protein (HBeAg). Thesemutations, however, do not affect the transcription of pregenomic RNAor the translation of the core or polymerase. Genotype A-infected indi-viduals often express this pattern of mutation and, therefore, haveenhanced viral replication by suppression of precore and core mRNArelative to pregenomic RNA (23).
Mutations in the X region lead to alteration in the regulatory ele-ments that control replication and can include mutations in the basalcore promoter and enhancer II. The basal core promoter spans nt 1742–1802 and overlaps the reading frame of the X gene. The nt 1762 and thent 1764 mentioned above are core promoter mutations that can causechanges in the X gene leading to production of truncated X proteins,which lack the amino acid domains required for transactivation activityof the HBxAg.
Most hepatitis B vaccines contain the major HBsAg protein andinduce an immune response to the major hydrophilic region at residues99–170. The anti-HBsAg response produces protective immunity.Mutations within this epitope have been selected during vaccination.Envelope gene mutations are detected in roughly half of all individ-uals who develop postvaccination HBV infection and are particularlyprevalent in infants born to carrier mothers. The most common of theseso-called “vaccine-escape” mutants is G145R in the “a” determinant ofHBsAg. Mutations here can lead to conformational alterations affect-ing the binding of neutralizing antibodies. These HBV mutants havebeen shown to escape vaccine-induced or passively transferred neu-tralizing responses allowing the propagation of a true HBsAg-positiveHBV infection despite the high titer of anti-HBsAb (23, 14). Mutationswithin this locus have also been found in orthotopic liver transplantrecipients who developed reinfection despite human immunoglobulinprophylaxis. The presence of escape variants correlated with a highincidence of graft failure, nearly double the percentage observed forpatients lacking variants. The S140 residue, unique to HBV E and Fgenotypes, may predispose patients to a vaccine escape mutation at anadjacent locus, as K141E has been observed only in West Africa, wheregenotype E predominates.
Pre-S1/S2 deletions and start codon mutants have been detectedin patients with chronic and fulminant hepatitis, perhaps arising in

Molecular Virology of Hepatitis B and C: Clinical Implications 15
response to strong humoral and T-cell activity against this highlyimmunogenic region. Selection of emergent mutations in CTL epi-topes of the envelope and core genes has been observed, though escapeis incomplete due to the multispecific nature of the CTL response.Some of these mutant-derived core sequences act as antagonists ofCTL response against the wild-type epitope and may contribute to viralpersistence.
2.14. Polymerase MutantsHBV integration typically yields replication-deficient integrated
genomes. Therefore, inhibition of reverse transcriptase for a sufficientlylong duration should permit eventual immune-mediated clearance ofthe preexisting cccDNA pool. The advent of treatment with nucleo-side and nucleotide analogues has resulted in the production of minorquasispecies containing mutations in the HBV Pol gene (23). Stud-ies have shown that long-term monotherapy with lamivudine or otherpolymerase inhibitors is often unsuccessful due to breakthrough infec-tion by drug-resistant polymerase gene mutants after approximately 1year of therapy (21, 25). Polymerase mutants are absent from untreatedpatients and exhibit generally lower virulence than wild-type, due tolower catalytic activity or possible missense disruption of the over-lapping S gene. Clinical manifestations of breakthrough infection arevariable: most patients sustain lower-than-pretreatment serum DNAand ALT levels; but, in rare occasions, emergence is accompanied byALT flares and hepatic decompensation. Upon therapy withdrawal,the reemergence of wild-type HBV typically yields further bouts ofhepatitis.
Lamivudine resistance increases progressively during treatment to14–32% annually and can reach 70% after 48 months of treatment.Several mutations which confer resistance to lamivudine have beenshown to cause substitutions within or adjacent to the “YMDD” motifat the catalytic site of the polymerase. A protein structure-based modelby which these mutated residues block drug action has been pro-posed (24, 26). Famciclovir-associated polymerase gene mutations,commonly affecting upstream domains of the protein, have been iden-tified in immunocompromised patients. Upstream mutations are morelikely to affect immune epitopes on HBsAg, although the effect on anti-genicity has yet to be determined. Unfortunately, the two most commonfamciclovir-resistant mutations, L528M and V521L, are also observedwith lamivudine treatment, suggesting that patients who developlamivudine-resistant mutants may not respond favorably to famci-clovir treatment and vice versa. HBV resistance to adefovir occurs less

16 Coash and Wu
frequently—around 20% after 2 years—than lamivudine resistance.Adefovir resistance is conferred primarily by a mutation at codon 236 inthe D motif of HBV Pol gene as well as a B motif mutation at 181. Ente-cavir resistance has been observed in two patients who were resistant tolamivudine with mutations mapped to the B motif at 184, the C motif at202, and the D motif at 250 (23). Recent in vitro and in vivo studies indi-cate that YMDD gene variants resistant to lamivudine remain sensitiveto adefovir, suggesting that the antiviral effects of these drugs will beadditive. However, mutations that confer resistance to lamivudine havebeen shown to give partial resistance to entecavir in vitro. The identi-fication of such mutually exclusive resistance profiles may be useful inthe design of effective sequential or combination therapy regimens.
3. HEPATITIS C VIRUS
One of the most remarkable features of hepatitis C virus is the fre-quency with which a chronic infection can be established, occurringin 55–85% of patients (27). In contrast to HBV, HCV exhibits extremevariability in nucleotide sequence. HCV, a member of the Flaviviridaefamily, has a single-stranded positive RNA genome with high geneticdiversity. The diversity is due to defective repair activity of the RNA-dependent RNA polymerase, which results in nucleotide substitution,as well as the absence of 5′ to 3′ exonuclease activity causing a lackof editing (28). At least six HCV genotypes and a large number ofsubtypes have been identified, some with different clinical outcomes.More recently, chimeric viruses generated by intergenotypic homol-ogous recombination events in the NS2 gene have been described.For a genotype 1a strain, the complete ∼9600 nucleotide (nt) RNAgenome has been verified by in vivo chimpanzee transfection, usingtranscripts derived from consensus cDNA clones. During the course ofan infection, HCV mutations accrue at the rate of 1.4×103 to 1.9×103
substitutions per nucleotide per year. Variants reflecting slight mod-ifications to the coding sequence, so-called “quasispecies”, are com-monly found to coexist simultaneously within a patient, and any givenserum-derived HCV inoculum contains a population of closely relatedviruses. The regions of the genome corresponding to essential viralfunctions such as those involved in translation or replication, as well asthe noncoding 5′- and 3′-ends, are highly conserved. The most variablepart of the genome is the region encoding the envelope glycoproteinsE1 and E2, and certain strains have shown more than 50% variability(28). The observed “hypervariability” in HCV-envelope proteins is oneexplanation for the exceptional ability of HCV inocula to reinfect thesame host following seroconversion and resolution of acute infection.

Molecular Virology of Hepatitis B and C: Clinical Implications 17
The absence of protective immunity against HCV continues to thwartvaccine development, and the emergence of drug-resistant strains willlikely pose a future obstacle to long-term efficacy of inhibitors designedto target the enzymes responsible for viral replication.
3.1. Replication Cycle and Experimental SystemsChimpanzee infection studies revealed the principal etiologic agent
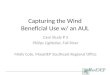
of HCV hepatitis to be an enveloped, 9.6-kb linear single-strandedpositive-sense RNA virus and has been characterized extensively invitro (29, 30). The genome serves as a template for translation as wellas for replication and is composed of a 5′-noncoding region (NCR),which includes an internal ribosome entry site (IRES), a single open-reading frame that encodes structural and nonstructural proteins, and a3′-NCR (31). The 5′-untranslated region (UTR) of virion RNA directsthe cap-independent translation of a polyprotein, which is cleavedinto structural (C,E1,E2,p7) and nonstructural (NS2,3,4A,4B,5A,5B)viral proteins (32). Replication of the viral RNA is carried out by anHCV-encoded RNA-dependent RNA polymerase, through a full-lengthnegative-strand RNA intermediate without evidence of DNA formation(33) (Fig. 3). Nascent positive-strand RNAs can be utilized for transla-tion, subsequent rounds of RNA replication, or packaging into virions.Although development of hepatitis in immunocompromised individualssuggests that HCV proteins may be directly cytopathic, the replicationprocess is generally noncytolytic. In most cases, chronic infection con-tinues for many years without evidence of hepatocyte injury.
Since the discovery of the HCV in 1989, the difficulty in the devel-opment of a cell culture model has been a major obstacle for HCVresearch. Previous attempts using primary hepatocyte culture systemsderived from resected liver tissue and inoculated with HCV-positivesera were only able to sustain low levels of viral RNA. One of theimportant milestones for HCV research was the development of repli-con systems which supported HCV replication inside permissive cul-tured cells. Replicon systems have been used for screening antiviralcompounds, studying host–viral interactions, RNA replication, and cel-lular innate immune responses. A shortcoming of this system is the lackof viral packaging and infectious viral release as would occur in infec-tion. In 2005, several groups were able to establish complete viral cellculture systems. A genotype 1b HCV DNA was transfected into Huh7cells, a cell line derived from a man with hepatocellular cancer. Anothersystem developed included the JFH1 genotype 2a clone-based infec-tious cell culture system, which was cloned from a Japanese patientwho had fulminant hepatitis caused by HCV. The viral replicons derived

18 Coash and Wu
Fig. 3. HCV life cycle. After HCV entry into the cell, the nucleocapsids aredelivered to the cytoplasm, where the viral RNA acts as an mRNA for transla-tion of a long polyprotein. RNA-dependent RNA replication converts the (+)into (−), which serves as a template for further (+) synthesis. Cytoplasmicreplication occurs via membrane-associated replication complexes in a perin-uclear membranous web. Genomic RNA-containing plasmids bud into cyto-plasmic vesicles through intracellular membranes, which fuse with the plasmamembrane. Adapted from Rehermann et al. (45).
from the JFH1 clone replicated much more efficiently without the needfor adaptive mutation. It was later shown that infectious viral particlescould be released from Huh7 cells when JFH1 full-length RNA wastransfected into the cells and that these viral particles could reinfectother naı̈ve cells (33).
Humans and chimpanzees are the only hosts able to support thecomplete viral life cycle, and the chimpanzee is still the only proveninfection animal model. However, studies on chimpanzees are limiteddue to constraints on availability and cost. The development of othersmall animal models for HCV infection has been a priority. Tree shrews(T. belangeri) have been shown to be susceptible to infection with HCV.However, they must first be irradiated to reduce the immune response.Several lines of HCV transgenic mice have been established. These ani-mals do produce circulating virus, but the lack of host immune toleranceto viral proteins does not simulate the normal immune response that

Molecular Virology of Hepatitis B and C: Clinical Implications 19
results in liver damage. A mouse model in which mouse hepatocyteswere repopulated by human liver cells has also recently been demon-strated, and an even more successful model using a uPA-SCID trans-genic mouse has shown potential applications in a model for HCVresearch (33). A rat model for HCV has recently been establishedthrough induction of tolerance of human hepatoma cell line Huh7. Ratlivers transplanted with Huh7 cells were shown to develop HCV repli-cation, gene expression, and biochemical as well as histological evi-dence of hepatitis. However, levels of virus were low, much lower thanin average patients with HCV infection (34).
3.2. Viral EntryRecent studies have identified viral and host cell components
involved in HCV cell entry. Hepatocytes are the main target cells forHCV infection. However, HCV has also been found in B cells, den-dritic cells, and other cell types. The HCV envelope integral membraneproteins are glycosylated noncovalent heterodimers of two polypep-tides, E1 and E2. The latter of these is apparently responsible for viralattachment, as E2-specific antisera can prevent HCV binding to cul-tured cells. Circulating HCV virions have been shown to associate with�-lipoproteins. The capsid protein, core, colocalizes with apolipopro-tein AII and intracellular lipid droplets; this interaction may contributeto hepatic steatosis observed in core transgenic mice. Notably, theexpression of LDL receptor in some cell types was shown to induceHCV binding, which does not otherwise occur. The endocytosis ofHCV particles appears to be mediated by LDL receptor, but may beassisted by other interactions. E2 was shown to bind a human cellsurface membrane protein, CD81. This interaction may contribute toentry of HCV virions into hepatocytes, although expression of CD81is a protein that has been found on the surface of many cell types.Other proposed HCV receptors in addition to LDL and CD81 includescavenger receptor class B type I (SR-BI), dendritic cell-specificintercellular adhesion molecule-3-grabbing nonintegrin (DC-SIGN),liver/lymph node-specific intercellular adhesion molecule-3-grabbingintegrin (L-SIGN), and more recently, claudin-1 which has been foundto be essential for HCV entry into hepatic cells and has been termed acoreceptor (31).
HCV replication has been reported to occur in extrahepatic sites, mostnotably peripheral blood mononuclear cells (PBMCs) from chronicallyinfected patients. High HCV RNA titers are observed in lymph nodesand approx. 50% of patients develop circulating HCV-associated cryo-globulins. An association with lymphoproliferative disorders such as

20 Coash and Wu
non-Hodgkin’s lymphoma has been reported. Lymphotropic variants ofHCV have been isolated from passage in cell culture and chimpanzeePBMCs. Comparison of HCV RNA sequences isolated from virusespropagated in lymphocytes vs. hepatocyte cell lines revealed that themajority of amino acid positions which putatively influence cell tropismare located in E2.
Events following HCV cell attachment remain to be elucidated. Itis known that HCV enters by clathrin-mediated endocytosis via transitthrough an endosomal low pH compartment and presumably by endo-somal membrane fusion. The actual mechanisms involved in activatingthe low pH-induced fusion as well as the fusion peptides still remainunknown (31). The E2 glycoprotein is insufficient for membrane fusion,and a hydrophobic region of the E1 glycoprotein has been proposedto mediate fusion of the viral envelope to the cell membrane. Uponcell entry, core associates with 60S ribosomal subunits, which maycontribute to uncoating of RNA and initiation of IRES-mediated HCVtranslation and RNA replication (31).
3.3. TranslationThere is no evidence that HCV positive-strand RNA bears the
5′-methylguanidine cap and 3′-polyadenylate tail typical of eukaryoticmessenger RNAs; but, it is nonetheless sufficient to direct translationof the ∼3000 amino acid-long HCV open-reading frame. The 5′-UTRsequence folds into a complex secondary and tertiary RNA structure.Notably, it is one of the few regions of the genome exhibiting lit-tle sequence variation among all HCV genotypes. The ∼300-nt regionupstream of the initiator codon functions as an internal ribosome entrysite (IRES). It directly recruits 40s ribosomal subunits to the start codonand can do so even in the absence of any canonical eukaryotic initia-tion factors. The IRES–40S ribosome complex then recruits eukaryoticinitiation factor eIF-3 followed by Met-tRNA-eIF2-GTP to produce a48S rRNA complex at the AUG initiation codon, which is then con-verted into an 80S complex in a rate-limiting step involving GTP-dependent association of the 60S subunit (31). The formation of thiscomplex is accelerated by the host NS1-associated protein-1 (NSAP-1),which binds to an adenosine-rich region within the HCV RNA (35). Theunique internal entry and factor independence of HCV ribosome bind-ing stand in marked contrast to cap-dependent translation initiation ofhost cell genes, making IRES a potential target for specific inhibition.
Sequences adjacent to the minimal IRES element are thought toinfluence its activity either by preventing disruption of RNA sec-ondary structure or possibly by recruiting host cell factors. Various host

Molecular Virology of Hepatitis B and C: Clinical Implications 21
RNA-binding proteins have been isolated via their direct interactionwith the HCV UTRs, although in many cases their identity and contribu-tion to translation initiation remain obscure. Disruption of these interac-tions might destabilize the IRES structure or diminish ribosome entryand could be explored as a treatment strategy. Indeed, the inhibitionof translation and/or the direct cleavage of positive-strand RNA maybe essential components of an effective antiviral therapeutic regime.Because HCV translation does not require the preexistence of virallyencoded factors, any remaining RNA is sufficient to initiate new roundsof replication, even if all HCV enzymes are simultaneously inhibited.
3.4. Protein ProcessingTranslation results in the production of a fusion protein which needs
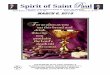
to be processed into each of its 10 proteins. Additionally an 11th pro-tein is also produced by ribosomal frame-shifting within the core geneand is called alternative reading frame protein (ARFP) (35). Prote-olytic processing of the HCV polyprotein is co- and posttranslationaland mediated by both host and viral proteases (Fig. 4). The host signalpeptidase, resident in the ER lumen, is responsible for cleavage between
Fig. 4. Structure of the HCV gene. A long single open-reading frameencodes a polyprotein of ∼3010 amino acids. The structural proteins are core,E1, and E2, the envelope proteins. The rest of the genome contains nonstruc-tural proteins. Another protein known as ARFP (alternative reading frame pro-tein) may be expressed from the core region of the genome as a result of trans-lational frameshift.