Embed Size (px)
Citation preview

Clinical assessment of heart chamber size and valve motion during cardiopulmonary resuscitation by two-dimensional echocardiography
It has been generally accepted that enhanced blood flow during closed-chest CPR is generated from compression of the heart between the sternum and the spine. To visualize the heart during closed- chest massage, we performed two-dimensional echocardiography (2DE) during resuscitation efforts in four patients who had cardiac arrest. 2DE analysis showed that (1) the LV internal dimensions dld not change appreciably with chest compression: (2) the mitral and aortic valves were open simultaneously during the compression phase; (3) blood flow into the right heart, as evidenced by saline bubble contrast, occurred during the relaxation phase; and (4) compression of the right ventricle and LA occurred In varying amounts In all patients. We conclude that stroke volume from the heart during CPR does not result from compression of the LV. Rather, CPR-induced improved cardiocirculatory dynamics appear to be principally the result of changes in intrathoracic pressure created by sternal compression. (AM HEART J 102:366, 1961.)
Stuart Rich, M.D., Hershel L. Wix, M.D., and Edward P. Shapiro, M.D. Chicago, Ill.
Since Kouwenhoven et al.’ introduced closed-chest massage in 1960,’ it has been presumed that sternal compression causes blood flow by squeezing the heart between the sternum and the spine. Recent investigations into the mechanisms of closed-chest cardiopulmonary resuscitation (CPR) have chal- lenged this notion. Weisfeldt et al.‘-” have demon- strated that in dogs blood flow during closed-chest massage is the result of the generalized increase in intrathoracic pressure,? and maneuvers that cause higher intrathoracic pressure result in an increase in blood flo~.~, 4 Although clinical studies are limited, similar maneuvers to raise intrathoracic pressure have been correlated with an increase in blood flow during cardiac arrest, presumably by the same mechanism.j To visualize the cardiac chambers dur- ing closed-chest massage, we performed two-dimen- sional echocardiography (2DE) in patients who had cardiac arrest. We were able to position the trans- ducer to obtain clear images without interfering with the resuscitation efforts. Our findings confirm
From the Department of Medicine, The University of Chicago.
Supported in part by United States Public Health Service Training Grant HL 07381.
Received for publication March 7, 1981; accepted May 12, 1981.
Reprint requests: Stuart Rich, M.D., Section of Cardiology, University of Illinois Hospital, P.O. Box 6998, Chicago, IL 60680.
that compression of the left ventricle (LV) does not occur during closed-chest massage in patients. Blood flow, both into and out of the chest, appears to be the result of the intrathoracic pressure gradients created by sternal compression.
METHODS
Study prot~ol. With approval from the Clinical Inves- tigations Committee of the University of Chicago, the present investigators were immediately notified of any cardiac arrest that occurred in the intensive care units. The clinical features of the .four patients studied are summarized in Table I. In all cases, CPR was initiated within 2 minutes of cardiac arrest, and lasted between 45 and 90 minutes per patient. The echocardiographic studies were performed within 20 minutes of onset of cardiac arrest. None of the patients survived the resusciation attempts.
Echocardiographic and hemodynamic recordings. All of the patients were supine during the study, on a hard backboard used in CPR. A Toshiba SSH-1OA phased- array sector scanner with 2.4 MHz transducer of 7%degree arc was employed, and the images were recorded on videotape for later playback and review. The operator performed the study standing at the patient’s left side while CPR was done in the conventional manner. A parasternal long-axis view of the heart was recorded with the transducer placed in the third or fourth intercostal space with the sector plane parallel to the long axis of the LV. which allowed simultaneous visualization of the
366 000%8703/81/090368 + 06$00.60/O 0 1981 The C. V. Mosby Co.

Volume102
Number3,patil 2DE assessment of LV/RV in CPR 369
Table I. Clinical features of patients studied during CPR
Patient Age/sex Clinical history Reason for admission Etiology of arrest Postmortem exam
1 76/F Chronic angina, recur- Syncopal episodes Asystole Acute MI, severe 3-
rent arrhythmias, mild vessel CAD, old aortic stenosis right atria1 infarc-
tion, AV calcifica- tion
2 84/M CHF, chronic bronchitis, Acute MI with Sudden hypotension Not done old CVA, cancer of pulmonary edema hypopharynx
3 82/F CHF, recent onset angi- Acute pulmonary ed- Recurrent ventricu- RV/LV hypertrophy,
na, COPD ema lar tachycardia acute subendocardial MI, severe emphyse- ma, multiple PE
4 58/M Cardiomyopathy with Severe CHF, abdomi- Cardiogenic shock Congestive cardiomy-
chronic CHF, mitral nal pain opathy, myxomatous regurgitation MVPS, pneumonia
CHF = congestive heart failure; CVA = cerebrovascular accident; COPD = chronic obstructive lung disease; MI = myocardial infarction; CAD = coro- nary artery disease; AV = aortic valve; PE = pulmonary emboli; MVPS = myxomatous mitral valve prolapse syndrome.
mitral and aortic valves. A short-axis view from the same position was obtained by rotating the transducer 90 degrees. An apical four-chamber view was obtained by placing the transducer at the LV apex with the sector plane directed towards the cardiac base. Rotation of the transducer 90 degrees provided a long-axis two-chamber view of the LV in a right anterior oblique equivalent position. Direct pressure recordings from either a Swan- Ganz catheter or radial artery catheter allowed objective estimations of the efficacy and constancy of chest com- pression in all patients (Fig. 1). 2DE monitoring was stopped when resuscitation efforts were terminated.
Data analysis and contrast 2DE studies. The compres- sion and relaxation phases of chest massage could be distinguished echocardiographically. Chest compression was defined as the period beginning with dorsal movement of the heart, sternum, and great vessels. The end of the compression phase and beginning of the relaxation phase occurred with return of the thoracic structures to their “resting” position. Measurements of changes in individual cardiac chambers were made when 2DE recordings of a particular view were of sufficient quality to allow 10 sequential measurements of the compression and relaxa- tion phases. The average of the values obtained are reported in Table II. Changes in LV internal dimension were measured from the parasternal long-axis and short- axis views just below the mitral valve. The right ventric- ular (RV) internal dimension was measured from the apical four-chamber view at the RV inflow tract just below the tricuspid valve. The RV outflow tract and left atrium (LA) were measured from the parasternal long- axis views. Intravenous saline infusion used for drug administration during resuscitation prodded bubble con- trast images within the right atrium (Rb) and RV. The flow of contrast within the right heart was correlated with timing of chest compressions.
RESULTS
LV during chest compression. Analysis of echocar- diograms revealed that the LV was not appreciably compressed during CPR. The change in LV diame- ter, as determined in the anteroposterior axis, aver- aged 2.9% (range 1.9% to 3.8%) in the patients studied (Table II). LV shape was not changed as seen in either the short-axis or long-axis views (Figs. 2 and 3). In one patient, the LV was seen to move laterally during the compression phase away from the sternum.
RV and LA during chest compression. In contrast to the LV, the LA and RV were compressed in all patients (Table II and Figs. 2 and 4). The RV was compressed less at the level of the tricuspid valve (range 12.6% to 16.0%) than at the outflow tract (range 40.2% to 72.6%). The LA was compressed to some degree in all patients (range 10.6% to 32.5%) (Fig. 2). The aortic root was compressed only mini- mally; 2DE visualization of the aortic root was not of sufficient quality to permit quantification of such changes. The extent of compression in these struc- tures appeared related, in part, to the depth af sternal compression achieved during CPR.
Blood flow through the right heart. Saline bubble contrast allowed assessment of blood Aow through the right heart.6 During the relaxation phase, the tricuspid valve opened widely and contrast could be seen to flow through the RA into the RV (Fig. 4). With onset of compression, the tricuspid valve closed and the RV became compressed, but more so at the outflow tract than at the apex. With release of compression the RV returned to its previous

370 Rich, Wix, and Shapiro September, 1981
American Heart Journal
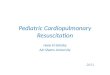
Fig. 1. Continuous pressure recording from a Swan-Ganz catheter in the pulmonary artery of one patient during CPR. The peaks in the phasic pulmonary pressure occurred with each chest compression.
I - - - .,_xll . . . . I . “ . ”
mid compression
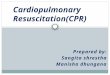
Fig. 2. Parasternal long-axis view of the heart during CPR. The panel on the left shows the mitral valve in a partially open position during the relaxation phase. With onset of chest compression (middle panel), the mitral valve opens widely, simultaneously with the aortic valve. During midcompression (rightpanel), the mitral valve remains in an open position, but the leaflets appear closer together. In this view, the right ventricular outflow tract and left atrium are seen to be compressed by the external sternal pressure. There is no appreciable change in left ventricular internal dimension throughout the CPR cycle. LV = left ventricle; LA = left atrium; RV,, = right ventricular outflow tract; MV = mitral valve; Ao = aortic root; A V = aortic valve. Because stop-frame images of the 2DE visualize only 50% of the sector plane, the quality of these images is considerably less than the actual recordings as viewed in real time. Diagrammatic representations of the stop-frame images are provided.

Volume102
Number3,partl CPR 371
relaxation compression
Fig. 3. Short-axis view of the heart during external relaxation (left) and chest compression (right) during CPR. In this view the mitral valve is seen to open (left) and close (right) while the left ventricle remained unchanged in size and shape with chest compression. RV = right ventricle; LV = left ventricle; MV = mitral valve.
shape and saline again filled both right heart cham- bers. The pulmonic valve was not well visualized.
Blood flow through the left heart. The LV was not compressed and appeared to function simply as a conduit through which blood flowed. The opening of the mitral and aortic valves was interpreted as a manifestation of blood flowing through them.’ The aortic and mitral valves opened simultaneously (Fig. 2), implying passage of blood from the atrium into the aorta. The valves were open during both com- pression and relaxation phases of CPR. The greatest excursion of the mitral and aortic valves occurred with onset of chest compression (Fig. 2). During chest midcompression, the mitral and aortic leaflets were less opened in systole but remained partially open (Figs. 2 and 3). With release of compression, the leaflets again opened widely during relaxation (Figs. 2 and 3). Quantification of blood flowing through the aortic and mitral valves was not possi- ble from these echocardiograms obtained during active CPR.
DISCUSSION
Mechanism of hemodynamic effective closed-chest CPR. Recent investigations into the mechanism of
Table II. Percent decrease in cardiac chamber size with external compression during CPR
Patient LV RV, R Vu LA
1 2.3 - 72.6 32.5
2 3.5 16.0 58.8 10.6
3 3.8 12.6 40.2 25.4 4 1.9 14.5 -
LV = percent change in LV measured just below the mitral valve in the parastemal long-axis and short-axis views; RV, = percent change in RV inflow tract measured just below the tricuspid valve in the apical four-chamber view; RV, = percent change in RV outflow tract measured in the parastemal long-axis view; LA = percent change in LA measured in the parasternal long-axis view.
cardiac output during closed-chest cardiac massage using a canine model have shown that blood flow out of the chest correlates with the amount of intrathoracic pressure created by sternal compres- sion.?-.’ Maneuvers that increase thoracic pressure during chest compression, or decrease thoracic pres- sure during relaxation, result in increased carotid artery flow.” It was concluded from these experi- ments that compression of the heart is not necessary to generate stroke output from the LV during CPR. This has now been demonstrated by ventriculogra-

372 Rich, Wix, September, 1981
American Heart Journal
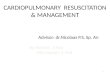
Fig. 4. Apical four-chamber view of the heart during CPR. The panel on the left shows the tricuspid valve open as bubbles rush in during the external relaxation phase. With the next external compression, the tricuspid valve shuts as the RV is compressed (right panel); the bubbles appeared to stop flowing during external compression when viewed in real time. In the apical two-chamber view (not shown), the right ventricular outflow tract was compressed more than the body of the right ventricle, suggesting that the bubbles may become trapped within the RV during external compression. This view also shows the mitral and tricuspid valves simultaneously; the AV valves moved at different times during chest compression and relaxation. LV = left ventricle; RV = right ventricle; MV = mitral valve; TV = tricuspid valve.
phy performed in dogs during CPR showing that the LV was not compressed.!’
Enhanced cardiac output during sternal pressure without LV compression. Clinical studies have been limited, but maneuvers that produce increased intrathoracic pressure and blood tlow during chest compression in dogs produce similar results in patients.j Although there are anatomical differences in the relationship of the heart to the thoracic skeleton between dogs and humans, it has been assumed that compression of the heart does not occur during CPR in patients as well.
Contrast 2DE visualized increased systemic venous return during chest relaxation. The echocardiograms obtained in this study enabled us to directly visual- ize the heart during CPR in patients, Although we did not measure cardiac output directly, the saline bubble contrast images showed that systemic venous return into the right heart occurred primari- ly during the relaxation phase (Fig. 4). The RV outflow tract was compressed to a greater degree
than the RV body, with the tricuspid valve fully closed during the compression phase, suggesting that blood may become trapped within the RV during chest compression. The forward flow of blood presumably results from the pressure gradient between the extrathoracic systemic veins and the intrathoracic vena cavae during the relaxation phase.’ Collapse of the intrathoracic veins during compression prevents backward flow of blood out of the chest.’ It should be noted that intrathoracic arterial pressures recorded during CPR do not necessarily reflect the degree of blood flow. Thus the peak pressure recorded from a pulmonary artery catheter in a patient during CPR (Fig. 1) occurred when pulmonary flow was least.
2DE evaluation of cardiac output during CPR. Blood flow through the left heart is somewhat more diffi- cult to assess. The aortic and mitral valves were open simultaneously in both the compression and relaxation phases, suggesting that blood flows out of the lungs during both phases (Fig. 2). Evaluation of

Volume 102
Number 3, part 1
the magnitude of blood flow during CPR was unable to be carried out echocardiographically, but pre- vious animal studies have shown that blood flow from the LV into the systemic circulation occurs predominantly during chest compression.‘0 Howev- er, substantive compression of the LV does not occur (Figs. 2 to 4). Instead, the LV serves as a conduit for the passage of blood. Compression of the LA and aortic root does occur, (Fig. 2) and may contribute to the forward flow of blood in some patients.?
Anatomic relation of heart to sternum. None of the patients in our study survived the resuscitation efforts. One might question whether the effects of sternal compression on the heart differ in those surviving CPR, but there is little to suggest that this may be the case. The anatomic relationship of the heart to the sternum may vary among patients but it has never been demonstrated that resuscitation is more successful in individuals with narrow anterio- posterior thoracic diameters or flexible chest walls. In fact, survival from CPR has been most closely correlated with early successful defibrillation, rather than technique or severity of underlying heart dis- ease.“. 12
Present study suggests CPR be directed to achieve increased intrathoracic pressure. The results of this study do not suggest that current techniques of CPR be abandoned or altered. However, by provid- ing insight into the mechanisms by which blood flow is created during closed-chest massage, it may lead to newer techniques which may make CPR even more effective. The focus on improving blood flow during CPR may now be shifted away from trying to achieve greater cardiac compression, and aimed toward generating higher intrathoracic pressure gra- dients.
Conclusions. We have confirmed that blood flow during CPR in patients does not result from direct
2llE assessment of LV/RV in CPR 373
compression of the LV. Rather, it appears to be the result of changes in intrathoracic pressure created by sternal compression. Blood flows into the right heart primarily during the relaxation phase and out of the lungs during the compression phase. Compres- sion of the LA and aorta does occur and may contribute to systemic blood flow in some patients.
REFERENCES
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
Kouwenhoven WB, Jude JR, Knickerbocker GG: Closed heart cardiac massage. JAMA 173:1064, 1960. Rudikoff MT. Mauehan WL. Effron M. Freund P. Weisfeldt ML: Mechanisms if blood’ flow during cardiopulmonary resuscitation. Circulation 61:345, 1980. Chandra N, Rudikoff M, Tsitlik J, Weisfeldt ML: Augmen- tation of carotid flow during cardiopulmonary resuscitation in the dog by simultaneous compression and ventilation with high airway pressure. Am J Cardiol43:422, 1979. Chandra N, Snyder L, Weisfeldt ML: Abdominal binding during CPR in man. Circulation 59 and IO(supp1 II):II-45, 1979. Chandra N, Rudikoff M, Weisfeldt ML: Simultaneous chest compression and ventilation at high airway pressure during cardiopulmonary resuscitation. Lancet 1:175, 1980. Seward JB, Tajik AJ, Hagler DJ, Ritter DG: Peripheral venous contrast echocardiography. Am J Cardiol 39:202, 1977. Rubenstein JJ, Pohost GM, Dinsmore RE: The echocardio- graphic determination of mitral valve opening and closure: Correlations with hemodynamic studies in man. Circulation 51:98, 1975. Chandra N, Cohen JM, Tsitlik J, Weisfeldt ML: Negative airway pressure between compression augments carotid flow during CPR. Circulation 59 and 6O(suppl II)II-46, 1979. Neimann JT, Garner D, Rosborough J, Criley JM: The mechanism of blood flow in closed chest cardiopulmonary resuscitation. Circulation 59 and 6O(suppl II):II-74, 1979. Cohen JM, Alderson PO, Van Aswegen A, Chandra N, Tsitlik J, Weisfeldt ML: Timing of imtrathoracic blood flow during resuscitation with high intrathoracic pressure. Circu- lation 59 and IO(supp1 II):II-196, 1979. Reichenbach DD, Moss NS, Meyer E: Pathology of the heart in sudden death. Am J Cardiol 39:865, 1977. Thompson RG, Hallstrom AP, Cobb LA: Bystander- initiated cardiopulmonary resuscitation in the management of ventricular fibrillation. Ann Intern Med 90:737, 1979.