Embed Size (px)
Citation preview

CARDIAC MAGNETIC RESONANCE (E NAGEL, SECTION EDITOR)
Clinical Applications of Aortic 4D Flow Imaging
Michael D. Hope & S. Jarrett Wrenn &
Petter Dyverfeldt
Published online: 17 January 2013# Springer Science+Business Media New York 2013
Abstract Quantitative aortic magnetic resonance (MR)blood flow imaging is a rapidly advancing technique thatis likely to impact clinical medicine in the near future. Theacquisition of comprehensive 4D velocity datasets is nowpossible in a clinically acceptable time frame. Unique andintuitive visualization methods are available. A number ofimportant hemodynamic biomarkers can be derived fromthe data, and exploited to help understand how abnormalflow is inter-related with aortic pathology. Initial data sug-gest that some of the derived biomarkers can refine theclinical assessment of aortic disease and predict diseaseprogression. We provide an overview of aortic imaging withemphasis on how flow imaging is currently used, discuss thefundamental technical aspects of multidimensional MR flowimaging, introduce key hemodynamic markers, and showhow this type of imaging may soon be used for the earlyidentification of patients at risk for the development ofpotentially devastating aortic complications.
Keywords Aorta . Magnetic resonance imaging . Phasecontrast MRI . Velocity-encodedMRI . 4D flow . Flowmeasurement . Eccentric flow . Hemodynamic imaging .
Biomarkers . Aneurysm . Aortic stenosis . Bicuspid aorticvalve . Aortic coarctation . Pulse wave velocity .
Turbulence . Pressure loss .Wall shear stress
Introduction
Imaging of the aorta is crucial for the diagnosis and man-agement of life-threatening diseases such as aneurysm anddissection. Magnetic resonance imaging (MRI) of bloodflow offers unique and valuable insights that complementconventional anatomic evaluation. This type of flow imag-ing has rapidly evolved in recent years. Here we reviewcurrent techniques and applications of quantitative MR aor-tic flow imaging, the hemodynamic biomarkers they cangenerate, and future prospects for the field.
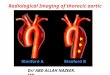
As the largest artery in the body, the aorta experiencesextreme hemodynamic forces over each cardiac cycle, re-peatedly receiving and distributing the left ventricular sys-tolic impulse. Visualization of aortic blood flow (Fig. 1) andmeasurement of associated hemodynamic parameters arenow possible with advances in MRI scanner hardware, pulsesequences, and post-processing tools. These capabilities arestarting to be used clinically to better understand vascularhomeostasis and aortic disease states.
Overview of Aortic Imaging
Aortic aneurysms are common, accounting for over 13,000deaths yearly in the United States [1]. With the increasinguse of cross-sectional imaging, the number of patients diag-nosed with aortic aneurysm is increasing. Abdominal aorticaneurysms (AAA) are more common than thoracic aorticaneurysms. Risk factors for AAA include advanced age,smoking, hypertension, atherosclerosis, and male gender;in fact, they are found in up to 5 % of men over the age of65 [2]. Thoracic aortic aneurysms are more heterogeneousthan AAAs in patient demographics, etiologies, and diseaseprogression [3]. In both cases, patients are followed withserial imaging and risk-stratified by aortic dimensions.
Electronic supplementary material The online version of this article(doi:10.1007/s12410-012-9187-8) contains supplementary material,which is available to authorized users.
M. D. Hope (*) : S. J. Wrenn : P. DyverfeldtDepartment of Radiology, University of California,San Francisco, 505 Parnassus Avenue, Box 0628,San Francisco, CA 94143-0628, USAe-mail: [email protected]
Curr Cardiovasc Imaging Rep (2013) 6:128–139DOI 10.1007/s12410-012-9187-8

The guidelines that dictate management of these patientsare based upon the strategy of surveillance imaging withelective intervention when a threshold dimension or growthrate is observed [3, 4]. This threshold is met when the risk ofleaving an aneurysm untreated (ie, the risk of dissection andrupture) equals the risk of intervention. In the ascendingaorta, for example, a diameter of 5.5 cm or a growth rateof 0.5 cm/year prompts intervention in a typical patient.Unfortunately, significant aortic disease specific morbidityand mortality are seen in patients who do not meet theseanatomic thresholds [5–9], illustrating that vessel dimen-sions alone do not capture the complexity of aortic diseaseprogression.
Two important considerations that play a role in aorticdisease progression are overlooked with a purely anatomy-based approach to aortic surveillance: (1) the structuralintegrity of the aortic wall, and (2) aortic hemodynamics.The former relates to inflammatory states, the expression ofextracellular matrix proteins, and other processes, many ofwhich can now be imaged using molecular strategies [10,11]. Hemodynamics are known to play an important role invascular disease pathogenesis and progression. For exam-ple, vessel stenoses are linked to downstream post-stenoticaneurysmal dilation, low wall shear stress promotes thedevelopment of atherosclerosis, and flow-stagnation hasbeen linked to intraluminal thrombus formation [6, 12–15].
Fig. 1 Systolic aortic bloodflow in a young man with abicuspid aortic valve and aorticcoarctation. Magnitude data a,in an oblique-sagittal orienta-tion demonstrates the coarcta-tion (arrow) and mild dilationof the ascending aorta (openarrow). Peak systolic flow isvisualized with short stream-lines generated throughout theaorta (red) and pulmonary ar-tery (blue) b. Focused flowevaluation of the thoracic aortain the same orientation (c) andin an oblique-coronal orienta-tion d, reveals eccentric veloci-ty distributions in both theascending aorta and about thecoarctation
Curr Cardiovasc Imaging Rep (2013) 6:128–139 129

Quantitative assessment of these parameters using MR flowimaging is now possible, and will provide valuable insightinto aortic disease in both research and clinical settings.
Current Clinical Flow Imaging Applications
MR blood flow imaging is routinely employed in a fewclinical scenarios. Typically, 2-dimensional (2D) cinephase-contrast (PC) MRI is used. Measurements are madewithin a plane that is prescribed according to the vessel orvalve of interest. Through-plane analysis allows for accurateflow volume quantification, but may miss peak velocitiesthat are better interrogated with analysis in the plane of avessel, or with 3-dimensional (3D) approaches. MR bloodflow imaging is commonly applied in the evaluation ofvalvular stenoses and regurgitation, cardiac output, shuntquantification, vessel stenoses, and coronary flow reserve.Here we will briefly discuss aortic valve disease and aorticcoarctation to illustrate how flow imaging is currently usedin the clinical evaluation of patients.
Aortic Valve Disease
Initial evaluation of aortic valve disease typically involvesechocardiography. MRI does offers some distinct advantagehowever, and is well accepted [16]. While MRI-derivedassessment of aortic stenosis can sometimes be limited dueto underestimation of peak velocities, the quantification ofregurgitation is accurate and not as prone to technical vari-ability as echocardiography [17]. In addition, quantitativeand reproducible measures of left ventricular size, functionand mass are obtained with MRI.
Aortic Regurgitation
Aortic regurgitation is evaluated with 2D cine PC-MRI byprescribing a plane perpendicular to the aorta in the tubularascending portion of the vessel. At multiple time pointsduring the cardiac cycle, the vessel lumen area is defined,and the measured flow through the segmented area yieldsflow volumes. The ratio of backward to forward flow is theregurgitant fraction.
Aortic Stenosis
Maximum velocity, transvalvular pressure gradient, andvalve area are routinely used for clinical evaluation of aorticstenosis. MRI permits estimation of both the anatomical andeffective orifice area (EOA), and has been shown to be lessvariable than other approaches for EOA estimation [18, 19].Estimation of the aortic valve gradient with stenosis usingMRI is performed with the modified Bernoulli equation in a
similar fashion to that employed in Doppler echocardiogra-phy, with good correlation reported [20]. The approachdiffers from flow quantification in that planes can be pre-scribed either parallel or perpendicular to the vessel in orderto identify maximal velocities. If the maximal flow veloci-ties in the vena contracta are not present in the interrogatedplanes, an underestimation of the degree of stenosis results.3D imaging techniques can avoid this problem. It shouldalso be noted that the limited temporal resolution of MRIcompared with echocardiography can also lead to underes-timation of pressure gradients.
Aortic Coarctation
Aortic coarctation refers to aortic narrowing at or near theligamentum arteriosum that restricts flow. MRI has becomethe imaging modality of choice for anatomic and hemody-namic interrogation of coarctation [21–23]. Anatomy isdelineated via high-resolution contrast-enhanced 3D-MRangiography (MRA). Hemodynamics are assessed withMR blood flow imaging. This evaluation includes (1) esti-mation of the degree of vessel stenosis, (2) quantification ofcollateral flow, and (3) assessment of dynamic flow profilesin the descending aorta. The degree of stenosis is assessed ina fashion similar to that used for aortic valve stenosis, wherepressure gradients are derived from peak velocities, andsuffers from the same limitations.
Collateral arterial flow develops as a means of bypassingthe hemodynamically significant aortic narrowing.Typically flow is measured at planes perpendicular to theaorta just beyond the coarctation and at the diaphragm.Normal flow drops over this interval [24]. However, withcollateral flow, the diaphragmatic flow is higher than thatnear the coarctation. The percentage increase can provide aquantitative measure of collateral flow [24, 25].
The hemodynamic significance of aortic coarctation isalso reflected in the flow profile of the descending aorta[21]. With significant coarctation, a slow systolic upstrokeand delayed return to baseline is seen, leading to diastolicflow persistence. This can be assessed with MR flow imag-ing in the descending aorta, including at the level of thediaphragm, where turbulence, aliasing, and stent-relatedartifact are noncontributory [26].
4D Flow
Multidimensional MR flow imaging permits the assessmentof cardiovascular hemodynamics well beyond the measure-ment of velocities through a 2D plane. It is a rapidly grow-ing field of research with a more than 10-fold increase inpublications in the last 5 years. Such attention stems fromthe numerous advantages the technique offers over 2D
130 Curr Cardiovasc Imaging Rep (2013) 6:128–139

methods: the capture of volumetric velocity data, completecoverage of the cardiovascular structures of interest, noconfinement to prospectively prescribed imaging planes,continuous breathing, and unique visualization and quanti-fication strategies.
Multidimensional MR flow imaging terminology can beconfusing. Here we will concentrate on 3D, time-resolved(cine), 3-directional PC-MRI, which is referred to as 4DFlow. The 4D component refers to 3D plus time, while“Flow” refers to the flow field information resulting from3-directional PC-MRI (Fig. 2).
Data Acquisition and Reconstruction
4D Flow acquisitions are synchronized to the cardiac cycleto obtain a cine series of images. The acquisition of acomplete data set requires many cardiac cycles (eg, 750heart beats); the reconstructed cardiac cycle thus representsan average of those cycles. The measurement of 3-directional velocities is achieved by applying motion-sensitivity in multiple directions (Fig. 2) [27]. Without ac-celeration of data acquisition, aortic 4D Flow scan time isabout an hour. However, many advances have been made toreduce scan time, with a typical Cartesian data acquisitionnow requiring 10 to 20 minutes. Data acquisition is typicallyperformed using an oblique-sagittal slab to encompass theentire thoracic aorta with spatial resolution in the 2–3 mm
range (Table 1). Further scan time reductions and improvedspatiotemporal resolution can be expected in the near future[28••, 29••, 30, 31•].
Flow Visualization
4D Flow imaging allows for unique and appealing visuali-zation of blood flow. Important abnormal flow character-istics may be revealed (Fig. 3, Movies 1 and 2) [32]. Vectorplots or particle trace methods including streamlines andpathlines can be used to visualize flow data [33]. Vectorplots allow for direct visualization of velocity fields.Streamlines represent instantaneous tangents to velocityvectors at a given time, and can reveal 3D flow patternssuch as vortices. Pathlines are calculated by integrating thevector field over time and represent actual trajectories thatparticles might take through the flow field. These visualiza-tion strategies offer a screening method for both data qualityand irregular flow patterns. However, visualization can betime-consuming and often requires considerable user-interaction. Automated approaches to standardize flow vi-sualization are needed.
Several new lines of investigation have resulted fromrecognizing global alterations in flow based on visualiza-tions: previously unsuspected pathways for arterial emboli[34•]; blood flow compartmentalization in the left ventricle[35]; altered hemodynamics in ascending aortic aneurysms
Fig. 2 Acquisition and reconstruction of aortic 4D Flow data. A 3Dimaging volume in a sagittal-oblique orientation covers the thoracicaorta a. Respiratory motion artifacts are suppressed by triggering dataacquisition only for cardiac cycles that occur during end expiration b.Data acquisition is synchronized to the cardiac cycle by ECG gating tocreate a cine series of images b. After Fourier transformation, 4complex-valued flow-encoding (FE) segments are obtained c. Onereference FEs acquired with zero first-gradient moment (FE0) and 3
FEs with motion-encoding in 3 perpendicular directions. The averageamplitude of the FEs provides a magnitude image used for anatomy d.Phase subtraction between the reference and motion-encoded segmentsprovides 3-directional velocity information. The intravoxel velocitystandard deviation (IVSD, σ) in 3 directions is obtained from theamplitude of the complex-valued FEs. Flow visualization and deriva-tion of hemodynamic biomarkers can be achieved by processing of thevelocity and IVSD data e
Curr Cardiovasc Imaging Rep (2013) 6:128–139 131

Table 1 Key aortic 4D flow imaging parameters
Parameter Typical Setting Comment
Orientation Sagittal-oblique In plane of aorta, or “candy-cane” view.
3D field-of-view (FOV, mm3) 320×320×70 Coverage in the readout, phase, and slice encoding directions.Adjusted to encompass the aorta.
3D matrix size, Nx × Ny × Nz 128×128×30 Number of frequency, phase, and slice encoding steps.
Velocity encoding range (VENC, cm/s) 150–300 Defines maximum measurable velocity. Velocities thatexceed the VENC are aliased.
Spatial resolution (mm3) 2.5×2.5×2.5 Size of the image voxels.
K-space segmentation (Nk) 2–3 k-space lines acquired per cardiac cycle. Enables a trade-offbetween temporal resolution and scan time.
Temporal resolution (ms) 35–45 (4 × TR) / Nk, where 4 is the number of encodings needed forphase reference (1) + 3-directional velocity encoding (3).
Respiratory efficiency, Reff 60 %–80 % Highly dependent on patient breathing.
parallel imaging acceleration factor 2 Degree of data undersampling. Non-acquired data is recoveredwith parallel imaging reconstruction methods.
Total scan time (min) 11–24 (HR 75 bpm) (Ny × Nz) / (Nk × Rnet × Reff × HR)
Fig. 3 4D flow visualization.a, Sagittal MRA image from ayoung female with bicuspidaortic valve and aorticcoarctation (open arrow).White bar denotes the levelthrough which cross-sectionswere obtained in panels b and c.b, Systolic velocity vector fieldthrough a cross-section of theascending aorta, illustrating aneccentric distribution of veloci-ties. c, Short streamlines at thesame level. d, Systolic stream-lines generated from a 3D gridthat spans the thoracic aortashow a helical systolic velocityfield pattern in the ascendingaorta (modified color scheme,see legend). See Movies 1 and 2for visualization of blood flowwith pathlines.
132 Curr Cardiovasc Imaging Rep (2013) 6:128–139

[36]; entry tears and resulting helical flow in chronic aorticdissection [37••]; and the relationship between eccentricflow and valve-related aortic disease [14, 38•].
Data Fidelity
Acquired 4D Flow data is representative of a specific heartrate, subject position (typically supine), and respiratory phase(typically end expiration). Flow visualization and derivedhemodynamic information should be interpreted in that phys-iologic context. The level of accuracy required of 4D Flow isapplication specific. Likewise, optimal approaches for dataprocessing and correction of known artifacts depend on theapplication in question [39•].
Validation of 4D Flow methods relies on in vitro, insilico, and animal model systems, as non-invasive methodsfor obtaining comprehensive hemodynamic parameters arelimited [40, 41]. However, due to long scan times (duringwhich subject position might change) and the fact that thereis not a standard way to correct for known artifacts, evenwell-validated 4D Flow protocols can produce low qualitydata sets. Identifying such data sets is often not trivial orstraightforward. We advocate the implementation of stan-dardized approaches to data quality control. This can beachieved by evaluation of the internal consistency of 4DFlow data. For example, pulmonary artery flow (Qp) andaortic flow (Qs) should be similar in non-shunt systems, andcan be easily extracted from the datasets and serve as acontrol for data quality. Pathline visualization can also beuseful for data validation. As pathlines are integrated overtime, they accumulate error and thus poor quality data canresult in pathlines extending beyond the vessel confines.Conservation-of-mass principles can be applied to pathlinesthrough a specified region of interest as a robust and inclu-sive method of validation [42•].
Quantitative Hemodynamic Markers
Comprehensive flow data can be used to calculate a numberof quantitative parameters referred to as hemodynamicmarkers. Although several can also be obtained from tradi-tional 2D cine PC-MRI data, all can be generated from asingle dataset with 4D Flow. We believe that the true clinicalvalue of aortic 4D Flow is likely to stem from the prognosticvalue of these markers for refined evaluation of aortic dis-ease and prediction of disease progression, rather than fromflow visualization.
Flow
In current clinical practice, flow is the most commonlymeasured hemodynamic parameter. As described above, this
is typically done with 2D cine PC-MRI through prescribedplanes. However, the 3D datasets obtained with 4D Flowprovide a unique advantage for these measurements becauseflow can be retrospectively calculated at any location in theimaging volume. This can be particularly useful in cases ofcongenital heart disease when flow measurement throughmultiple vessels is needed. Prescribing multiple imagingplanes while the patient is in the scanner is challengingand time consuming. An additional advantage of volumetriccoverage is the possibility of performing retrospective track-ing of heart valves to account for their motion during thecardiac cycle. This has been reported to enable accuratequantification of net flow volume through all heart valves[43]. Good correlation between 2D cine PC-MRI and 4DFlow has been demonstrated for aortic coarctation, correctedcomplex congenital heart disease and in the setting of type Baortic dissection [37••, 44••, 45••].
Fig. 4 Visualization of turbulence intensity with aortic stenosis. Sys-tolic flow in the ascending aorta (AA) and descending aorta (DA) for anormal subject a, and 3 patients with aortic stenosis and ascendingaortic dilation: peak/mean gradients in mm Hg of 56/30 b, 90/46 c, and75/43 d. Short streamlines (blue) generated throughout the ascendingaorta provide an overview of the systolic velocity field. Volume ren-dering of turbulent kinetic energy (TKE, red-yellow) reveal uniqueregions of elevated turbulence intensity
Curr Cardiovasc Imaging Rep (2013) 6:128–139 133

Pulse Wave Velocity
Pulse wave velocity (PWV) refers to the speed at which thesystolic impulse travels through the cardiovascular system.PWV is a measure of vascular stiffness, and has shown to bean important clinical biomarker. For example, carotid-femoral PWV is an independent predictor of mortality inthe general population and in subgroups of patients withcommon chronic illnesses [46]. PVW is also known tocorrelate well with aortic disease [46, 47] and has beenuseful in predicting progression [48] and evaluating treat-ment response [49, 50] in Marfan syndrome.
PC-MRI can measure PWV in an accurate and reproduc-ible way using transit time methods, whereby velocity-timeprofiles are measured at 2 or more locations in the vessel ofinterest [51]. The temporal differences between specific fea-tures of the flow versus time curve (eg, foot, half-maximum,or peak) are used to estimate pulse wave travel time. Thetravel distance can be reliably estimated from angiographicrepresentations of 3D MRI data. Another approach for esti-mating travel time involves using cross-correlation to estimatetime shifts between waveforms, which takes into consider-ation the entire pulse waveform [52]. This approach hasrecently been demonstrated with 4D Flow [53•]. An
Fig. 5 Abnormal systolic flow with post-stenotic aortic dilation. a,Normal blood flow in a healthy volunteer. From left to right, magneticresonance angiography (MRA), systolic streamlines in the ascendingaorta and cross-sectional analysis at the plane depicted in the proximalascending aorta are provided; this same sequence is found in eachimage panel presented. The MRA shows normal aortic geometry, thestreamlines normal laminar systolic flow, and the cross-sectional anal-ysis central fast flow and an even distribution of wall shear stress(WSS) around the aortic lumen; the green bars represent the relativemagnitude of WSS. b, A man with severe aortic stenosis and
aneurysmal dilation of the ascending aorta to 5.3 cm. Systolic flow iseccentric with streamlines that course through the ascending aorta in aright-handed helix. The cross-sectional analysis shows that flow ismarginalized to the right-anterior quadrant where WSS is focallyelevated. c, A young woman with BAV, aortic stenosis and dilation ofthe ascending aorta to 4.6 cm. Similar eccentric flow with a right-handed helix of systolic streamlines is demonstrated. WSS is againfocally elevated where flow is marginalized against the aortic wall.(With permission, Hope MD et al. Int J Cardiol. 2012;156(2):e40–42.)
134 Curr Cardiovasc Imaging Rep (2013) 6:128–139

advantage of MRI is the ability to perform focused, regionalassessment of individual vessels, which may prove moreclinically relevant than global evaluation [48].
Pressure
Pressure gradients are key to assessing the severity of ste-noses. They are routinely estimated from echocardiographyor MR velocity data using the modified Bernoulli equation.But the velocity fields acquired with 4D Flow can be ma-nipulated in more advanced ways. Pressure gradients can beintegrated along arbitrary lines, allowing the estimation ofpressure differences between selected points [54]. 3D pres-sure maps can also be calculated [55–57], but many chal-lenges exist and care must be taken to avoid systematic error[58]. A limitation of current MR pressure field mapping isthe assumption of non-turbulent flow. This is reasonable forintracardiac blood flow, but problematic for stenoses wheresignificant turbulence effects exist.
Turbulence
A hallmark of turbulent flow and related non-laminar typesof flow (eg, “transitional” or “disturbed”) is the presence ofapparently random velocity fluctuations. The standard devi-ation of the velocity fluctuations around the mean velocity isa common definition of turbulence intensity. Turbulenceintensity can be estimated by exploiting the effects of ve-locity fluctuations on the amplitude of the PC-MRI signal(Fig. 2) [59]. The turbulent kinetic energy (TKE) describesthe kinetic energy of the fluctuating velocity field, and canbe calculated from 4D Flow data [60] with good agreementwith reference methods [41, 59, 61, 62]. Application tovascular stenoses and valvular lesions has demonstratedthe potential of this extension of 4D Flow for revealingimportant information on the spatiotemporal dynamics ofdisturbed cardiovascular flows (Fig. 4) [60].
Dissipation of TKE is the primary cause of pressure lossacross stenoses, and thus may play an important role inevaluating their true hemodynamic significance. Recent datawith aortic stenosis indicate that a MR measured TKE maybe useful for the estimation of and irreversible pressure loss[63••]. Turbulence is also related to other relevant clinicalfactors including endothelial cell turnover, hemolysis andplatelet activation [64–66]. MR turbulence mappingexpands research possibilities in these areas.
Wall Shear Stress
Wall shear stress (WSS) is the frictional force exerted on avessel wall by flowing blood. 4D Flow can be used toestimate WSS and is widely applied [14, 67–69].Limitations of the method, including poor lumen-wall
contrast and partial volume effects of near wall velocitymeasurements have been addressed by combining lumenwall segmentations with line or plane fitting of velocitiesin multiple voxels [70]. Nevertheless, WSS estimates de-rived from PC-MRI underestimate true WSS in a non-linear,voxel-size dependent manner [70, 71•]. However, 4D Flowcan be used to identify areas of abnormally high or lowWSS, which may be clinically useful [14, 68, 72].
WSS is important for vascular homeostasis. Low and os-cillatory WSS is known to promote atherosclerosis by induc-ing atherogenic states of endothelial cells [12]. Goodcorrelation has been shown between aortic atherosclerosisand lowWSS observed by 4D Flow [73, 74]. WSS evaluationof abdominal aortic aneurysms, however, is often not possiblebecause of the presence of intraluminal thrombus [75].
The effect of high WSS on vessels is less well studiedthan low WSS, but has been linked to vessel remodeling[12]. High WSS can also lead to endothelial injury andweakening [76]. This has also been incorporated into alow then high WSS theory of atherosclerotic plaque rupture:low WSS leads to plaque formation and luminal narrowing,leading to elevated WSS at the upstream edge of the plaque;elevated WSS causes smooth muscle apoptosis and extra-cellular matrix degradation, weakening the vessel and pre-disposing to rupture [77]. Based on recent cell culture data,WSS gradients might be more important than absolute WSSvalues for driving aneurysm growth [78].
4D Flow has been used to evaluate WSS throughout thethoracic aorta [68, 79]. Focally elevated WSS has beencorrelated with typical areas of postoperative aneurysm
Table 2 Quantitative hemodynamic biomarkers
Hemodynamicbiomarker
Clinical Significance
Flow volume * Valve regurgitation
* Shunt quantification
* Collateral flow with aortic coarctation
Pulse wave velocity(PWV)
* Vascular stiffness
* Correlates well with disease states
* Independent predictor of mortality
Relative pressure * Driving force of blood flow
* Pressure loss across stenosis (along withturbulence)
Turbulence * Energy loss across stenosis
* Blood trauma
* Platelet activation
Wall shear stress(WSS)
* Regulator of endothelial cell function
* Low WSS promotes atherosclerosis
* High WSS linked to aortic growth
Eccentricity * Growth of aortic aneurysms
* Potential surrogate for wall shear stress
Curr Cardiovasc Imaging Rep (2013) 6:128–139 135

formation and aneurysm rupture [80, 81]. Valve-relatedaortic disease has been increasingly studied with 4D Flow,revealing distinctly abnormal hemodynamics that may un-derlie post-stenotic dilatation [67, 82–84]. For example,focally elevated WSS has been observed at the convexityof the ascending aorta in patients with bicuspid aortic valves(BAV) [14, 72], the same site where valve-related asymmet-ric aortic dilatation typically occurs in these patients (Fig. 5)[85–87] and where extracellular matrix changes have beenobserved in surgical specimens [88].
Flow Eccentricity
Normal flow in the ascending aorta is characterized by anapproximately parabolic velocity profile, where the highestvelocities are seen centrally. 4D Flow evaluation of patientswith aortic valve disease and/or aortic dilation, however,commonly demonstrates eccentric flow with highly skewedvelocity profiles. As a result, asymmetric near-wall velocitygradients are present, leading to areas of relatively highWSS. This eccentricity is well visualized and quantifiedwith 4D Flow. One approach is to calculate the angle be-tween the flow jet and the axis of the left ventricular outflowtract [89]. An alternate strategy involves calculating thedisplacement of flow from the aortic centerline [38•].
Capturing the asymmetric hemodynamics of eccentricflow with a simple, quantitative parameter such as flowdisplacement could prove clinically useful. Recently, linksbetween eccentric flow and ascending aorta growth has beenuncovered. Restricted aortic leaflet motion (which presum-ably results in flow eccentricity) was shown to correlatestrongly with increased aortic growth rate in a subset ofpatients with BAV [90•]. In a similar population of patients,4D Flow demonstrated good correlation between increasedaortic growth rates and flow displacement [91••]. Flowdisplacement is a simple parameter that is very reproducibleand better correlates with interval aortic growth than WSS(Hope MD, unpublished data, 2012). For these reasons, webelieve that eccentricity is one of the more promising he-modynamic markers for risk-stratifying patients for progres-sive valve-related aortic disease.
Conclusion
Quantitative aortic MR blood flow imaging is a rapidlyadvancing technique that is likely to impact clinical medi-cine in the near future. The acquisition of comprehensive 4Dvelocity datasets is now possible in a clinically practicaltime frame, with further scan reduction expected in the nearfuture. Unique and intuitive visualization methods are avail-able. A number of important hemodynamic markers can bederived from the data, and exploited to help understand how
abnormal flow promotes aortic pathology (Table 2). Initialdata suggest that some of the derived biomarkers can refinethe clinical assessment of aortic disease and predict aorticdisease progression. Larger, prospective studies are war-ranted to assess the potential of MR flow imaging for theearly identification of patients at risk for the development ofpotentially devastating aortic complications.
Acknowledgment Funding: Radiological Society of North AmericaResearch Scholar Grant (MDH). Swedish Heart-Lung Foundation(PD), Swedish Brain Foundation (PD), Fulbright Commission (PD).
Disclosure No potential conflicts of interest relevant to this articlewere reported.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. Elefteriades JA, Farkas EA. Thoracic aortic aneurysm clinicallypertinent controversies and uncertainties. J Am Coll Cardiol.2010;55:841–57.
2. Scott RA, Ashton HA, Kay DN. Abdominal aortic aneurysm in4237 screened patients: prevalence, development, and manage-ment over 6 years. Br J Surg. 1991;78:1122–5.
3. Isselbacher EM. Thoracic and abdominal aortic aneurysms. Circu-lation. 2005;111:816–28.
4. Hiratzka LF, Bakris GL, Beckman JA, Bersin RM, Carr VF, CaseyJr DE, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management ofpatients with Thoracic Aortic Disease: a report of the AmericanCollege of Cardiology Foundation/American Heart AssociationTask Force on Practice Guidelines, American Association forThoracic Surgery, American College of Radiology, AmericanStroke Association, Society of Cardiovascular Anesthesiologists,Society for Cardiovascular Angiography and Interventions, Socie-ty of Interventional Radiology, Society of Thoracic Surgeons, andSociety for Vascular Medicine. Circulation. 2010;121:e266–369.
5. Brown LC, Powell JT. Risk factors for aneurysm rupture inpatients kept under ultrasound surveillance.UK small aneu-rysm trial participants. Ann Surg. 1999;230:289–96. discus-sion 296–87.
6. Elefteriades JA. Thoracic aortic aneurysm: reading the enemy'splaybook. Curr Probl Cardiol. 2008;33:203–77.
7. Fillinger MF, Marra SP, Raghavan ML, Kennedy FE. Prediction ofrupture risk in abdominal aortic aneurysm during observation: wallstress versus diameter. J Vasc Surg. 2003;37:724–32.
8. Nicholls SC, Gardner JB, Meissner MH, Johansen HK. Rupture insmall abdominal aortic aneurysms. J Vasc Surg. 1998;28:884–8.
9. Pape LA, Tsai TT, Isselbacher EM, Oh JK, O'Gara PT, Evangelista A,et al. Aortic diameter > or = 5.5 cm is not a good predictor of type Aaortic dissection: observations from the International Registry ofAcute Aortic Dissection (IRAD). Circulation. 2007;116:1120–7.
10. Hope TA, Hope MD. Improved risk assessment for abdominalaortic aneurysm rupture off-the-wall imaging. J Am Coll Cardiol.2011;58:2531–2.
136 Curr Cardiovasc Imaging Rep (2013) 6:128–139

11. Osborn EA, Jaffer FA. The year in molecular imaging. JACCCardiovasc Imaging. 2010;3:1181–95.
12. Malek AM, Alper SL, Izumo S. Hemodynamic shear stress and itsrole in atherosclerosis. JAMA. 1999;282:2035–42.
13. Wilton E, Jahangiri M. Post-stenotic aortic dilatation. J Cardio-thorac Surg. 2006;1:7.
14. Hope MD, Hope TA, Crook SE, Ordovas KG, Urbania TH, AlleyMT, et al. 4D Flow CMR in assessment of valve-related ascendingaortic disease. JACC Cardiovasc Imaging. 2011;4:781–7.
15. Rayz VL, Boussel L, Ge L, Leach JR, Martin AJ, Lawton MT, etal. Flow residence time and regions of intraluminal thrombusdeposition in intracranial aneurysms. Ann Biomed Eng. 2010;38:3058–69.
16. Pennell DJ, Sechtem UP, Higgins CB, Manning WJ, Pohost GM,Rademakers FE, et al. Clinical indications for cardiovascular mag-netic resonance (CMR): consensus Panel report. Eur Heart J.2004;25:1940–65.
17. Glockner JF, Johnston DL, McGee KP. Evaluation of cardiacvalvular disease with MR imaging: qualitative and quantitativetechniques. Radiographics. 2003;23:e9.
18. Cawley PJ, Maki JH, Otto CM. Cardiovascular magnetic reso-nance imaging for valvular heart disease: technique and validation.Circulation. 2009;119:468–78.
19. Garcia J, Marrufo OR, Rodriguez AO, Larose E, Pibarot P, KademL. Cardiovascular magnetic resonance evaluation of aortic stenosisseverity using single plane measurement of effective orifice area. JCardiovasc Magn Reson. 2012;14:23.
20. Kilner PJ, Manzara CC, Mohiaddin RH, Pennell DJ, Sutton MG,Firmin DN, et al. Magnetic resonance jet velocity mapping inmitral and aortic valve stenosis. Circulation. 1993;87:1239–48.
21. Nielsen JC, Powell AJ, Gauvreau K, Marcus EN, Prakash A, GevaT. Magnetic resonance imaging predictors of coarctation severity.Circulation. 2005;111:622–8.
22. Warnes CA, Williams RG, Bashore TM, Child JS, Connolly HM,Dearani JA, et al. ACC/AHA 2008 Guidelines for the managementof adults with congenital heart disease: a report of the AmericanCollege of Cardiology/American Heart Association Task Force onPractice Guidelines (writing committee to develop guidelines onthe management of adults with congenital heart disease). Circula-tion. 2008;118:e714–833.
23. Muzzarelli S, Meadows AK, Ordovas KG, Higgins CB, MeadowsJJ. Usefulness of cardiovascular magnetic resonance imaging topredict the need for intervention in patients with coarctation of theaorta. Am J Cardiol. 2012;109:861–5.
24. Steffens JC, Bourne MW, Sakuma H, O'Sullivan M, Higgins CB.Quantification of collateral blood flow in coarctation of the aortaby velocity encoded cine magnetic resonance imaging. Circulation.1994;90:937–43.
25. Araoz PA, Reddy GP, Tarnoff H, Roge CL, Higgins CB. MRfindings of collateral circulation are more accurate measures ofhemodynamic significance than arm-leg blood pressure gradientafter repair of coarctation of the aorta. J Magn Reson Imaging.2003;17:177–83.
26. Muzzarelli S, Ordovas KG, Hope MD, Meadows JJ, Higgins CB,Meadows AK. Diagnostic value of the flow profile in the distaldescending aorta by phase-contrast magnetic resonance for pre-dicting severe coarctation of the aorta. J Magn Reson Imaging.2011;33:1440–6.
27. Pelc NJ, Bernstein MA, Shimakawa A, Glover GH. Encodingstrategies for 3-direction phase-contrast MR imaging of flow. JMagn Reson Imaging. 1991;1:405–13.
28. •• Knobloch V, Boesiger P, Kozerke S. Sparsity transform k-tprincipal component analysis for accelerating cine 3-dimensionalflow measurements. Magn Reson Med. 2012. doi:10.1002/mrm.24431. New reconstruction techniques allow accelerationfactors of up to 8 to be used with preservation of data quality.
29. •• Hsiao A, Lustig M, Alley MT, Murphy M, Chan FP, HerfkensRJ, et al. Rapid pediatric cardiac assessment of flow and ventricularvolume with compressed sensing parallel imaging volumetric cinephase-contrast MRI. Am J Roentgenol. 2012;198:W250–9. Acceler-ated 4D Flow with compressed sensing is validated in a clinicalsetting with direct comparison to standard 2D PC-MRI data.
30. Gu T, Korosec FR, Block WF, Fain SB, Turk Q, Lum D, et al. PCVIPR: a high-speed 3D phase-contrast method for flow quantifi-cation and high-resolution angiography. Am J Neuroradiol.2005;26:743–9.
31. • Sigfridsson A, Petersson S, Carlhall CJ, Ebbers T. Four-dimensional flow MRI using spiral acquisition. Magn ResonMed. 2012;68:1065–73. A new 4D Flow sequence with a non-Cartesian k-space trajectory (spiral) permits 3 times faster acqui-sition of data.
32. Sengupta PP, Pedrizzetti G, Kilner PJ, Kheradvar A, Ebbers T,Tonti G, et al. Emerging trends in CV flow visualization. JACCCardiovasc Imaging. 2012;5:305–16.
33. Buonocore MH. Visualizing blood flow patterns using streamlines,arrows, and particle paths. Magn Reson Med. 1998;40:210–26.
34. • Harloff A, Simon J, Brendecke S, Assefa D, Helbing T,Frydrychowicz A, et al. Complex plaques in the proximaldescending aorta: an underestimated embolic source of stroke.Stroke. 2010;41:1145–50. A previously unappreciated sourceof stroke is identified based on 4D Flow visualization ofretrograde flow in the descending aorta.
35. Eriksson J, Carlhall CJ, Dyverfeldt P, Engvall J, Bolger AF, Ebbers T.Semi-automatic quantification of 4D left ventricular blood flow.J CardiovascMagnReson. 2010;12:9. doi:10.1186/1532-429X-12-9.
36. Hope TA, Markl M, Wigstrom L, Alley MT, Miller DC, HerfkensRJ. Comparison of flow patterns in ascending aortic aneurysmsand volunteers using 4-dimensional magnetic resonance velocitymapping. J Magn Reson Imaging. 2007;26:1471–9.
37. •• Clough RE, Waltham M, Giese D, Taylor PR, Schaeffter T. Anew imaging method for assessment of aortic dissection using 4-dimensional phase contrast magnetic resonance imaging. J VascSurg. 2012;55:914–23. Abnormal blood flow characteristics in-cluding helicity are correlated with disease progression in a cohortof patients with chronic type B aortic dissection.
38. • Sigovan M, Hope MD, Dyverfeldt P, Saloner D. Comparison of4-dimensional flow parameters for quantification of flow eccen-tricity in the ascending aorta. J Magn Reson Imaging.2011;34:1226–30. A straightforward and reproducible hemody-namic parameter is presented that may outperform more compli-cated estimates of abnormal blood flow.
39. • Rolf MP, Hofman MB, Gatehouse PD, Markenroth-Bloch K,Heymans MW, Ebbers T, et al. Sequence optimization to reducevelocity offsets in cardiovascular magnetic resonance volume flowquantification–a multi-vendor study. J Cardiovasc Magn Reson.2011;13:18. The effects of background phase offsets in phase-contrast MRI are systematically evaluated.
40. Boussel L, Rayz V, Martin A, Acevedo-Bolton G, Lawton MT,Higashida R, et al. Phase-contrast magnetic resonance imagingmeasurements in intracranial aneurysms in vivo of flow patterns,velocity fields, and wall shear stress: comparison with computa-tional fluid dynamics. Magn Reson Med. 2009;61:409–17.
41. Petersson S, Dyverfeldt P, Gardhagen R, Karlsson M, Ebbers T.Simulation of phase contrast MRI of turbulent flow. Magn ResonMed. 2010;64:1039–46.
42. • Eriksson J, Carlhall CJ, Dyverfeldt P, Engvall J, Bolger AF,Ebbers T. Semi-automatic quantification of 4D left ventricularblood flow. J Cardiovasc Magn Reson. 2010;12:9. An inclusiveand robust approach to internal validation of 4D Flow velocitydata is presented.
43. Roes SD, Hammer S, van der Geest RJ, Marsan NA, Bax JJ, LambHJ, et al. Flow assessment through 4 heart valves simultaneously
Curr Cardiovasc Imaging Rep (2013) 6:128–139 137

using 3-dimensional 3-directional velocity-encoded magnetic res-onance imaging with retrospective valve tracking in healthy vol-unteers and patients with valvular regurgitation. Invest Radiol.2009;44:669–75.
44. •• Hope MD, Meadows AK, Hope TA, Ordovas KG, Saloner D,Reddy GP, et al. A clinical evaluation of aortic coarctation with 4DFlow MR imaging. J Magn Reson Imaging. 2010;31:711–8. 4DFlow is incorporated into the clinical scheme for evaluating aorticcoarctation and shown to be reliable.
45. •• Valverde I, Nordmeyer S, Uribe S, Greil G, Berger F, Kuehne T,et al. Systemic-to-pulmonary collateral flow in patients with palli-ated univentricular heart physiology: measurement using cardio-vascular magnetic resonance 4D velocity acquisition. J CardiovascMagn Reson. 2012;14:25. The value of a comprehensive evalua-tion of complex congenital cardiac physiology with a single 4DFlow acquisition is clearly presented.
46. Cavalcante JL, Lima JA, Redheuil A, Al-Mallah MH. Aorticstiffness: current understanding and future directions. J Am CollCardiol. 2011;57:1511–22.
47. Tzemos N, Lyseggen E, Silversides C, Jamorski M, Tong JH,Harvey P, et al. Endothelial function, carotid-femoral stiffness,and plasma matrix metalloproteinase-2 in men with bicuspid aorticvalve and dilated aorta. J Am Coll Cardiol. 2010;55:660–8.
48. Nollen GJ, Groenink M, Tijssen JG, Van Der Wall EE, Mulder BJ.Aortic stiffness and diameter predict progressive aortic dilatationin patients with Marfan syndrome. Eur Heart J. 2004;25:1146–52.
49. Ahimastos AA, Aggarwal A, D'Orsa KM, Formosa MF, White AJ,Savarirayan R, et al. Effect of perindopril on large artery stiffnessand aortic root diameter in patients with Marfan syndrome: arandomized controlled trial. JAMA. 2007;298:1539–47.
50. Groenink M, de Roos A, Mulder BJ, Spaan JA, van der Wall EE.Changes in aortic distensibility and pulse wave velocity assessedwith magnetic resonance imaging following beta-blocker therapyin the Marfan syndrome. Am J Cardiol. 1998;82:203–8.
51. Grotenhuis HB, Westenberg JJ, Steendijk P, van der Geest RJ,Ottenkamp J, Bax JJ, et al. Validation and reproducibility of aorticpulse wave velocity as assessed with velocity-encoded MRI. JMagn Reson Imaging. 2009;30:521–6.
52. Fielden SW, Fornwalt BK, Jerosch-Herold M, Eisner RL, StillmanAE, Oshinski JN. A new method for the determination of aorticpulse wave velocity using cross-correlation on 2D PCMR velocitydata. J Magn Reson Imaging. 2008;27:1382–7.
53. • Markl M, Wallis W, Brendecke S, Simon J, Frydrychowicz A,Harloff A. Estimation of global aortic pulse wave velocity by flow-sensitive 4D MRI. Magn Reson Med. 2010;63:1575–82. Globalpulse wave velocity can be reliably measured with a cross-correlation technique using 4D Flow.
54. Ebbers T, Wigstrom L, Bolger AF, Engvall J, Karlsson M. Esti-mation of relative cardiovascular pressures using time-resolved 3-dimensional phase contrast. Magn Reson Med. 2001;45:872–9.
55. Bock J, Frydrychowicz A, Lorenz R, Hirtler D, Barker AJ, JohnsonKM, et al. In vivo noninvasive 4D pressure difference mapping in thehuman aorta: phantom comparison and application in healthy volun-teers and patients. Magn Reson Med. 2011;66:1079–88.
56. Ebbers T, Wigstrom L, Bolger AF, Wranne B, Karlsson M. Non-invasive measurement of time-varying 3-dimensional relative pres-sure fields within the human heart. J Biomech Eng. 2002;124:288–93.
57. Tyszka JM, LaidlawDH,Asa JW, Silverman JM. Three-dimensional,time-resolved (4D) relative pressure mapping using magnetic reso-nance imaging. J Magn Reson Imaging. 2000;12:321–9.
58. Ebbers T, Farneback G. Improving computation of cardiovascularrelative pressure fields from velocity MRI. J Magn Reson Imaging.2009;30:54–61.
59. Dyverfeldt P, Sigfridsson A, Kvitting JP, Ebbers T. Quantificationof intravoxel velocity standard deviation and turbulence intensity
by generalizing phase-contrast MRI. Magn Reson Med.2006;56:850–8.
60. Dyverfeldt P, Kvitting JP, Sigfridsson A, Engvall J, Bolger AF,Ebbers T. Assessment of fluctuating velocities in disturbed cardio-vascular blood flow: in vivo feasibility of generalized phase-contrast MRI. J Magn Reson Imaging. 2008;28:655–63.
61. Elkins CJ, Alley MT, Saetran L, Eaton JK. Three-dimensionalmagnetic resonance velocimetry measurements of turbulencequantities in complex flow. Exp Fluids. 2009;46:285–96.
62. Binter C, Knobloch V,Manka R, SigfridssonA, Kozerke S. Bayesianmultipoint velocity encoding for concurrent flow and turbulencemapping. Magn Reson Med. 2012. doi:10.1002/mrm.24370.
63. •• Dyverfeldt P HM, Tseng EE, Saloner D. Noninvasive magneticresonance measurement of turbulent kinetic energy for the estima-tion of irreversible pressure loss in aortic stenosis. J Am CollCardiol Imaging. 2012 (in press). Noninvasive estimation of theirreversible pressure loss associated with a stenotic lesion.
64. Davies PF, Remuzzi A, Gordon EJ, Dewey Jr CF, Gimbrone JrMA. Turbulent fluid shear stress induces vascular endothelial cellturnover in vitro. Proc Natl Acad Sci U S A. 1986;83:2114–7.
65. Sallam AM, Hwang NH. Human red blood cell hemolysis in aturbulent shear flow: contribution of Reynolds shear stresses. Bio-rheology. 1984;21:783–97.
66. Stein PD, Sabbah HN. Measured turbulence and its effect onthrombus formation. Circ Res. 1974;35:608–14.
67. Barker AJ, Lanning C, Shandas R. Quantification of hemodynamicwall shear stress in patients with bicuspid aortic valve using phase-contrast MRI. Ann Biomed Eng. 2010;38:788–800.
68. Markl M, Wallis W, Harloff A. Reproducibility of flow and wallshear stress analysis using flow-sensitive 4-dimensional MRI. JMagn Reson Imaging. 2011;33:988–94.
69. Bieging ET, Frydrychowicz A, Wentland A, Landgraf BR, JohnsonKM, Wieben O, et al. In vivo 3-dimensional MR wall shear stressestimation in ascending aortic dilatation. J Magn Reson Imaging.2011;33:589–97.
70. Stalder AF, Russe MF, Frydrychowicz A, Bock J, Hennig J, MarklM. Quantitative 2D and 3D phase contrast MRI: optimized analy-sis of blood flow and vessel wall parameters. Magn Reson Med.2008;60:1218–31.
71. • Petersson S, Dyverfeldt P, Ebbers T. Assessment of the accuracyof MRI wall shear stress estimation using numerical simulations. JMagn Reson Imaging. 2012;36:128–38. Detailed investigation ofpitfalls and limitations of MR-based WSS estimation.
72. Barker AJ, Markl M, Burk J, Lorenz R, Bock J, Bauer S, et al.Bicuspid aortic valve is associated with altered wall shear stress inthe ascending aorta. Circ Cardiovasc Imaging. 2012;5:457–66.
73. Pedersen EM, Oyre S, Agerbaek M, Kristensen IB, Ringgaard S,Boesiger P, et al. Distribution of early atherosclerotic lesions in thehuman abdominal aorta correlates with wall shear stresses mea-sured in vivo. Eur J Vasc Endovasc Surg. 1999;18:328–33.
74. Wentzel JJ, Corti R, Fayad ZA, Wisdom P, Macaluso F, WinkelmanMO, et al. Does shear stress modulate both plaque progression andregression in the thoracic aorta? Human study using serial magneticresonance imaging. J Am Coll Cardiol. 2005;45:846–54.
75. Wang DH, Makaroun MS, Webster MW, Vorp DA. Effect ofintraluminal thrombus on wall stress in patient-specific mod-els of abdominal aortic aneurysm. J Vasc Surg. 2002;36:598–604.
76. Meng H, Wang Z, Hoi Y, Gao L, Metaxa E, Swartz DD, et al.Complex hemodynamics at the apex of an arterial bifurcationinduces vascular remodeling resembling cerebral aneurysm initia-tion. Stroke. 2007;38:1924–31.
77. Slager CJ, Wentzel JJ, Gijsen FJ, Schuurbiers JC, van der Wal AC,van der Steen AF, et al. The role of shear stress in the generation ofrupture-prone vulnerable plaques. Nat Clin Pract Cardiovasc Med.2005;2:401–7.
138 Curr Cardiovasc Imaging Rep (2013) 6:128–139

78. Dolan JM, Meng H, Singh S, Paluch R, Kolega J. High fluid shearstress and spatial shear stress gradients affect endothelial prolifer-ation, survival, and alignment. Ann Biomed Eng. 2011;39:1620–31.
79. Frydrychowicz A, Stalder AF, Russe MF, Bock J, Bauer S, HarloffA, et al. Three-dimensional analysis of segmental wall shear stressin the aorta by flow-sensitive 4-dimensional-MRI. J Magn ResonImaging. 2009;30:77–84.
80. Crook SE, Hope MD. Arch hypoplasia and aneurysm after aorticcoarctation repair: abnormal flow may be the link. JACC Cardio-vasc Imaging. 2011;4:685–6.
81. Hope MD, Hope TA, Urbania TH, Higgins CB. Four-dimensionalflow magnetic resonance imaging with wall shear stress analysisbefore and after repair of aortopulmonary fistula. Circ CardiovascImaging. 2010;3:766–8.
82. Hope MD, Dyverfeldt P, Acevedo-Bolton G, Wrenn J, Foster E,Tseng E, et al. Post-stenotic dilation: evaluation of ascending aorticdilation with 4D flow MR imaging. Int J Cardiol. 2012;156:e40–2.
83. Hope MD, Hope TA, Meadows AK, Ordovas KG, Urbania TH,Alley MT, et al. Bicuspid aortic valve: 4-dimensional MR evalu-ation of ascending aortic systolic flow patterns. Radiology.2010;255:53–61.
84. Hope MD, Meadows AK, Hope TA, Ordovas KG, Reddy GP,Alley MT, et al. Images in cardiovascular medicine. Evaluationof bicuspid aortic valve and aortic coarctation with 4D flow mag-netic resonance imaging. Circulation. 2008;117:2818–9.
85. Bauer M, Gliech V, Siniawski H, Hetzer R. Configuration of theascending aorta in patients with bicuspid and tricuspid aortic valvedisease undergoing aortic valve replacement with or without re-duction aortoplasty. J Heart Valve Dis. 2006;15:594–600.
86. Cotrufo M, Della Corte A. The association of bicuspid aortic valvedisease with asymmetric dilatation of the tubular ascending aorta:identification of a definite syndrome. J Cardiovasc Med.2009;10:291–7.
87. Lu MT, Thadani SR, Hope MD. Quantitative assessment of asym-metric aortic dilation with valve-related aortic disease. AcadRadiol. 2012. [Epub ahead of print].
88. Della Corte A, Quarto C, Bancone C, Castaldo C, Di Meglio F,Nurzynska D, et al. Spatiotemporal patterns of smooth muscle cellchanges in ascending aortic dilatation with bicuspid and tricuspidaortic valve stenosis: focus on cell-matrix signaling. J ThoracCardiovasc Surg. 2008;135:8–18. 18 e11–12.
89. den Reijer PM, Sallee 3rd D, van der Velden P, Zaaijer ER, ParksWJ, et al. Hemodynamic predictors of aortic dilatation in bicuspidaortic valve by velocity-encoded cardiovascular magnetic reso-nance. J Cardiovasc Magn Reson. 2010;12:4.
90. • Della Corte A, Bancone C, Conti CA, Votta E, Redaelli A, DelViscovo L, et al. Restricted cusp motion in right-left type ofbicuspid aortic valves: A new risk marker for aortopathy. J ThoracCardiovasc Surg. 2012;144:360–9, 369.e1. Restricted cusp motionwith bicuspid aortic valves correlates with ascending aorticgrowth rates, suggesting underlying flow patterns have directimpact on disease progression.
91. •• Hope MD, Wrenn SJ, Sigovan M, Foster E, Tseng E, Saloner D.Imaging biomarkers of aortic disease: increased growth rates witheccentric systolic flow. J Am Coll Cardiol. 2012;60:356–7. Eccen-tric systolic blood flow in the context of bicuspid aortic valve iscorrelated with increased aortic growth rates, suggesting a prog-nostic role for 4D Flow in the assessment of valve-related aorticdisease.
Curr Cardiovasc Imaging Rep (2013) 6:128–139 139