Embed Size (px)
Citation preview

Clinical Anatomy of the Periocular RegionPari N. Shams, BSc, MRCP, FRCOphth1 Santiago Ortiz-Pérez, MD2 Naresh Joshi, FRCOphth1
1Oculoplastic and Craniofacial Service, Department ofOphthalmology, Chelsea and Westminster Hospital, London, UnitedKingdom
2Department of Oculoplastic, Institut Clinic Oftalmologia, HospitalClinic, Barcelona, Spain
Facial Plast Surg 2013;29:255–263.
Address for correspondence Pari N. Shams, BSc, MRCP, FRCOphth,Department of Ophthalmology, Chelsea and Westminster Hospital,369 Fulham Road, London, United Kingdom SW10 9NH(e-mail: [email protected]).
The primary function of the eyelids is to protect the globethrough voluntary and reflex eyelid closure. They also play animportant role in maintaining good vision by providingimportant elements of the precorneal tear film, the mostimportant refractive surface of the eye, and helping to dis-tribute the tear film evenly over the surface of the eye.Additionally the lacrimal pump function of the eyelids actsto propel the tears to themedial canthus, to enter the lacrimaldrainage system. We aim to provide the reader with acomprehensive and up-to-date overview of periocular anat-omy; however, the reader is encouraged to refer to recentreviews and peer reviewed articles and to textbooks ofoculoplastic surgery for greater detail and understanding ofthe anatomy of the periocular region.1–10
Superficial Topography of the Eyelids
The interpalpebral fissure or palpebral aperture measures 10to 11 mm vertically in young adults and decreases to 8 to10 mm with advancing age (►Fig. 1). The peak of the uppereyelid usually lies just nasal to the midline of the pupil. Thehorizontal length of the fissure is 31 � 1 mm. The upper andlower eyelids meet at an angle of �60 degrees medially andlaterally. In primary position, the upper eyelid margin lies at
the superior corneal limbus in children and 1.5 to 2 mmbelow it in adults. The lower eyelidmargin rests at the inferiorcorneal limbus. When operating on the lateral canthus, it isworth remembering that the normal lateral canthal angle lies�2 to 3 mm higher than its medial counterpart.
The Skin
There is a marked transition from the thin eyelid skin to thethicker skin of the eyebrow and cheek. The redundancy andelasticity of the eyelid skin and other eyelid structures allowfor primary closure of large defects of up to 30% of the eyelidin older patients. Increased redundancy and laxity of eyelidskin and muscle with age is known as dermatochalasis.Prominence of the lower eyelids may result from prolapseof the orbital fat, malar bags, or hypertrophic or overridingorbicularis oculi muscle. Eyelid skin is the thinnest in thebody, often less than 1 mm thick, and unique in having nosubcutaneous fat.
The upper eyelid skin crease is created by attachmentsfrom the superficial aspect of the levator aponeurosis into theorbicularis muscle and the subcutaneous tissue. The skincrease, although variable in height and subject to genderand racial differences, usually lies 5 to 6 mm above the eyelid
Keywords
► anatomy► eyelid► periocular► oculoplastic surgery► brow► midface► orbital septum► facial nerve
Abstract The aims of this article are twofold: (1) to provide the facial plastic surgeon with acomprehensive and up-to-date overview of periocular anatomy including the brow,midface, and temporal region and (2) to highlight important anatomical relationshipsthat must be appreciated in order to achieve the best possible functional and aestheticsurgical outcomes.
Issue Theme Periocular AestheticRejuvenation; Guest Editor, Naresh Joshi,FRCOphth
Copyright © 2013 by Thieme MedicalPublishers, Inc., 333 Seventh Avenue,New York, NY 10001, USA.Tel: +1(212) 584-4662.
DOI http://dx.doi.org/10.1055/s-0033-1349365.ISSN 0736-6825.
255
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.

margin centrally in males and 7 to 8 mm in females (►Fig. 1).When marking the desired position of the upper lid skincrease, note that the crease descends to within 3 to 4 mm ofthe eyelidmarginmedially and 5 to 6 mm laterally. The lowereyelid skin crease is 3 to 4 mm blow the eyelid margincentrally and 5 to 6 mm laterally.
In Asian patients, the upper lid skin crease is typicallypoorly developed or absent because the orbital septuminserts onto the levator aponeurosis in a lower position.This anatomical arrangement allows the preaponeurotic fatto extend further into the eyelid.
These are condensations of fibrous tissue, known asretaining ligaments, that run from deeper structures to theoverlying dermis and help to anchor the skin and mobile softtissues to the underlying skeleton. The orbital retainingligaments are located over the zygomaticofrontal sutureand over the malar eminence. With aging fascial and liga-mentous laxity, in combinationwith dermal elastosis, there isdescent of all soft tissues of the face contributing to thecharacteristic brow ptosis, submalar hollowing, and theprominence of the nasolabial fold.
Orbicularis Oculi
The orbicularis oculi may be divided into the orbital andpalpebral parts, with the latter being divided further into thepreseptal and pretarsal portions (►Fig. 2). The palpebralportion functions in voluntary and involuntary eyelid closure,and the orbital portion is used in forced eye closure.
The orbital portion overlies the bony orbital margins. Itarises from insertions on the frontal process of the maxillarybone, the orbital process of the frontal bone, and the medialcanthal tendon. Its fibers pass around the orbital rim to form acontinuous ellipse without interruption at the lateral canthusand insert just below the points of origin. The muscle fibersextend superiorly to interdigitatewith the frontalismuscle andcorrugator supercilii muscle, laterally to cover the anteriortemporalis fascia, and inferiorly to cover the origins of the lipelevators. The palpebral portion of the orbicularis muscleoverlies the mobile eyelid from the orbital rims to the eyelid
margins. Themuscle fibers pass circumferentially around eacheyelid, fixed medially and laterally at the canthal tendons.
The fibers of the preseptal orbicularis originate perpen-dicularly along the upper and lower borders of the medialcanthal tendon, arc around the eyelids, and insert along thelateral horizontal raphe. An overriding preseptal orbicula-ris muscle in the lower eyelid is associated with epible-pharon. The weight of the skin fold and the orbicularismuscle may rotate the lower eyelid margin inward, creatingan entropion.
The pretarsal portion of the muscle originates from themedial canthal tendon via separate superficial and deepheads, arc around the lids, and inserts onto the lateral canthaltendon and raphe. Additional bundles of thin muscle fibersrun along the upper and lower eyelid margins. These arereferred to as muscles of Riolan. Contraction of these fibersaids in the lacrimal pump mechanism. Medially, the deepheads of the pretarsal fibers fuse to form a prominent bundleof fibers, the Horner muscle, which extends just behind theposterior limb of the canthal tendon and inserts onto theposterior lacrimal crest. As the Horner muscle passes to theposterior lacrimal crest, it is joined by the medial horn of thelevator aponeurosis, the posterior layer of the orbital septum,and the medial rectus check ligament. Contraction of theHorner muscle draws the eyelids (especially the lower)medially and posteriorly. The resulting lateral pull on thelacrimal sac creates a relative negative pressurewithin the sacand draws the tears from the canaliculi into the sac.
An avascular fascial plane composed of loose connectivetissue exists between the orbicularis muscle and the orbitalseptum-levator aponeurosis fascial complex, which extendsto themargin of the eyelid at the gray line. The gray line is alsoreferred to as themuscle of Riolan and represents the pretarsalorbicularis muscle on the eyelid margin. The gray line itselfmarks the anatomical separation of the anterior skin–musclelamella from the posterior tarsoconjunctival lamella. Thispostorbicularis fascial plane allows bloodless surgical dissec-tion down to the septum and approach to the superior andinferior orbital margins.
Fig. 1 The topography of the eyelids in relation to one another and theglobe.
Fig. 2 The anatomy of the pretarsal, preseptal, and orbital parts of theorbicularis oculi, the other brow depressors (corrugator and procerus),the brow elevator (frontalis), and other periocular muscles.
Facial Plastic Surgery Vol. 29 No. 4/2013
Clinical Anatomy of the Periocular Region Shams et al.256
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.

The postorbicularis fascial plane also allows slight move-ment between the orbicularis muscle and the underlyingorbital septum while maintaining an integrated lamellarstructure. Surgical disruption of the fibrous connectionswithin the postorbicularis fascial plane can cause an inferiorslippage of the anterior lamella. This can be prevented byfixating the orbicularis muscle and skin edges to the levatoraponeurosis during the skin closure.
The Orbital Septum
The orbital septum is a thin, fibrous, multilayered sheath thatbegins at the arcus marginalis along the orbital rim (►Fig. 3);it represents a continuation of the orbital fascial system. Theorbital septum can be readily identified during surgery bynoting the firm resistance to traction applied to it because ofits attachment to the arcus marginalis.
Distal fibers of the orbital septum merge into the anteriorsurface of the levator aponeurosis. The point of insertionusually is �3 to 5 mm above the tarsal plate, but it may be asmuch as 10 to 15 mm above it. In the lower eyelid the septumfuses with the capsulopalpebral fascia several millimetersbelow the tarsus (►Fig. 4). In young patients, the orbitalseptum is usually relatively thick and quite easily identified atsurgery. In contrast, the orbital septum may be very thin anddehiscent in older patients. Functionally, the septummay actas a barrier to infection and hemorrhage.
The orbital septum is continuous with the inner layers ofthe periorbita. Within the orbit, the periorbita lines the bonyorbital walls and is composed of an outer layer of periosteumand an inner layer continuous with the orbital fascia. Theselayers separate at the arcus marginalis, and the outer perios-teum continues over the orbital margins as the periosteum ofthe forehead and facial bones. In the upper eyelid the inner
fascial layer separates into two layers at the arcus marginalis.The superficial layer continues over the brow where it iscontinuous with the deep fascia over the frontalis muscle andthe galea aponeurotica above the eyebrow. The deep layerbecomes the orbital septum in the upper eyelid. In the lowereyelid the inner fascial layer extends into the eyelid as theorbital septum. Medially, the septum attaches to the anteriorand posterior lacrimal crests, and laterally it inserts into thelateral canthal tendon and also passes behind the tendoninserting onto the lateral retinaculum together with thelateral horn of the levator aponeurosis.
Periocular Fat Compartments
Fat is located within the eyelid, subbrow, and orbitalcompartment. Eyelid fat is interconnected and contiguouswith deeper orbital fat and both serve as a protectivecushion for the globe and facilitate movement of the globe.Because the eyelid fat pads are in direct communicationwith the deep extraconal fat of the orbit, caution must beexercised when handling orbital fat in the anterior orbit.Traction on the fat pad may injure deep orbital vesselscausing orbital hemorrhage.
The central preaponeurotic fat pad is an important surgicallandmark, as it lies immediately posterior to the orbitalseptum and anterior to the levator aponeurosis in the upperlid (►Fig. 3) and lower lid retractors in the lower eyelid(►Fig. 4). Fine connective tissue septa extend anteriorly fromthe capsule of preaponeurotic fat to the orbital septum andposteriorly to the levator aponeurosis. The preaponeurotic fatpad is yellow as compared with the whiter, more fibrousmedial fat pad. The medial fat pad is derived from orbital fatdeep to the levatormuscle and ismore vascular because of thelocation of the palpebral arterial arcade that courses throughit. The lacrimal gland lies lateral to the central preaponeuroticfat pad, isolated within its own fascial sheath. If the latterbecomes lax, the gland can prolapse into the lateral aspect of
Fig. 3 Sagittal cross section through the upper eyelid. Abbreviations:PAFP, preaponeurotic fat pad; ROOF, retro-orbicularis oculi fat.
Fig. 4 Sagittal cross section through the lower eyelid. Abbreviation:SOOF, suborbicularis oculi fat.
Facial Plastic Surgery Vol. 29 No. 4/2013
Clinical Anatomy of the Periocular Region Shams et al. 257
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.

the eyelid where it must be differentiated from preaponeur-otic fat by its firm, pink, vascular, lobulated structure to avoidperioperative injury.
Although the so-called fat pads of the lower eyelid are notdistinct anatomic entities, they have been divided into threeclinically useful divisions: medial, central, and lateral(►Fig. 5). The medial and central fat pads are divided bythe inferior oblique muscle, and the boundaries of the middleand lateral fat pads are defined by the arcuate expansion,which extends from Lockwood’s ligament to the inferolateralorbital margin. A small lobule from the precapsulopalpebralfat pad extends superiorly between the orbital septum andthe lateral canthal tendon, known as the Eisler pocket, whichis thought to act as a bursa to the lateral canthal tendonduring eyelid movements.
A deep plane of fat, the retro-orbicularis oculi fat (ROOF),lies posterior to the orbital part of the orbicularis musclesuperiorly over the superior orbital margin (►Fig. 3) andinferiorly the suborbicularis oculi fat (SOOF) lies over theinferior orbital margin (►Fig. 4). Subbrow fat can form aredundant upper eyelid skin fold and undergoes gravitationaldescent during aging. In females, the eyebrow is generallyarched and above the level of the supraorbital rim. The maleeyebrow is flatter and at the level of the supraorbital rim. Theposition of the eyebrow can affect the height and excursion ofthe upper eyelid and must be considered in a patient beingevaluated for ptosis repair or blepharoplasty. Resection of theROOF in conjunctionwith aesthetic blepharoplasty can softenand flatten heaviness and bulkiness in the lateral upperorbital and brow region.
It is extremely important not to confuse an extension ofthe brow fat pad into the postorbicularis fascial plane of theupper eyelid with the preaponeurotic fat pads. If the orbitalseptum is incorrectly identified as the levator aponeurosis, aninadvertent advancement of this septal layer will result inmarked lagophthalmos. Likewise advancement of the capsu-
lopalpebral fascia in the lower eyelid without first separatingthe orbital septum will result in lower eyelid retraction.Suturing the orbital septum without adequate traction ofthe eyelid in the opposite direction also risks shorteningresulting in lagophthalmos or eyelid retraction.
The midfacial fat compartments include the SOOF andmalar fat pads. These fat compartments are bound to theorbicularis muscle by the superficial muscular aponeuroticsystem (SMAS) of the cheek. In the aging lower eyelid,pseudoherniation of orbital fat may result in contourirregularities. The SOOF can become apparent with thegravitational descent seen in the midface with aging andcontributes to the aesthetic deformity of the lower lids.Malar bags may also develop from descent of the malar fatpad.
The Tarsal Plates
The tarsal plates are made up of dense fibrous tissue andprovide the main structural integrity to the eyelids. Theupper and lower tarsal plates are �25 mm in length hori-zontally and 1 to 1.5 mm in thickness, and centrally thevertical height of the tarsal plate varies from 8 to 12 mm inthe upper lid and 3.5 to 4 mm in the lower eyelid. The medialand lateral aspects of the tarsal plates taper to 2 mm in heightas they pass into the medial and lateral canthal tendons. Theposterior surface of both tarsal plates is covered by conjunc-tiva. Only 4 to 5 mm of tarsus is needed for upper eyelidstability, when the tarsus is used in eyelid reconstruction.Within the tarsal plates, 20 to 30 vertically aligned meibo-mian glands lie, which are multilobulated holocrine seba-ceous glands, opening onto the posterior eyelid marginbehind the gray line and secreting the lipid layer of theprecorneal tear film.
The Canthal Tendons
Medially, the tarsal plates pass into fibrous bands that formthe crura of the medial canthal tendon. These lie between theorbicularis muscle anteriorly and the conjunctiva posteriorly.The superior and inferior crura fuse to form a common tendonthat inserts via three limbs, anterior, posterior, and superior.The anterior limb inserts onto the orbital process of themaxillary bone in front of and above the anterior lacrimalcrest. It provides the major support for the medial canthalangle. The posterior limb arises from the common tendonnear the junction of the superior and inferior crura and passesbetween the canaliculi. It inserts onto the posterior lacrimalcrest just in front of the Horner muscle. The posterior limbdirects the vector forces of the canthal angle backward tomaintain close approximation with the globe. The superiorlimb of the medial canthal tendon arises as a broad arc offibers from both the anterior and posterior limbs. It passesupward to insert onto the orbital process of the frontal bone.The posterior head of the preseptal orbicularis muscle insertsonto this limb, and the unit forms the soft tissue roof of thelacrimal sac fossa. This tendinous extension may providevertical support to the canthal angle but it also appears to
Fig. 5 The fat compartments of the upper and lower eyelid and theirrelationship to adjacent structures.
Facial Plastic Surgery Vol. 29 No. 4/2013
Clinical Anatomy of the Periocular Region Shams et al.258
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.

play a significant role in the lacrimal pump mechanism. It isthe posterior arm of the medial canthal tendon inserting intothe posterior lacrimal crest that must be repaired meticu-lously when a lower eyelid has been avulsed to avoid ananterior malposition of the lower eyelid.
Laterally, the tarsal plates pass into not very well-devel-oped fibrous strands that become the crura of the lateralcanthal tendon. The lateral canthal tendon is a distinct entityseparate from the orbicularis muscle; it measures �1 mm inthickness, �5 to 7 mm in length, and 3 mm in width at thepoint where the superior and inferior crura unite but itbroadens to a width of �6 to 7 mm as it inserts into thelateral orbital tubercle 1.5 mm inside the lateral orbitalmargin. The lateral horn of the levator aponeurosis blendswith the superior border of the lateral canthal tendon. Theinsertion of these fibrous strands extends posteriorly alongthe lateral orbital wall, where it blends with strands of thelateral check ligament from the sheath of the lateral rectusmuscle. Along with the lateral canthal tendon complex, theinferolateral fibers of the Whitnall superior suspensory liga-ment and the lateral portion of the Lockwood inferior sus-pensory ligament insert onto the lateral tubercle, forming thelateral retinaculum. The lateral canthal tendon and the lateralhorn of the levator aponeurosis extend superiorly to a posi-tion 4 to 5 mmbelow the frontozygomatic suture line forminga broad tendonlike insertion. Division of the superior crus ofthe lateral canthal tendon can be associated with significantmorbidity due to the proximity of important adjacent struc-tures (i.e., the lateral horn of the levator, the Whitnall liga-ment, and the lacrimal gland). The inferior crus of the lateralcanthal tendon is divided during the course of a lateral tarsalstrip procedure and in the management of an acute orbitalhemorrhage.
The Eyelid Retractors
The upper eyelid retractor muscles include the levator palpe-brae superioris (LPS) muscle and the superior tarsal muscle,called the Müller muscle, in the upper eyelid. The LPS is askeletal muscle innervated by the oculomotor nerve (thirdcranial nerve), whereas the inferior tarsal muscle and theMüller muscle are both composed of smooth muscle andsympathetically innervated.
The LPSmuscle arises from the lesser wing of the sphenoidbone just above the annulus of Zinn and superolateral to theoptic canal. The muscle is �35 mm in length. At its origin it is�4 mm in width, widening to �8 mm in the midsection ofthe orbit. As the muscle passes forward, it lies in intimatecontact with the superior rectus muscle (►Fig. 3). The levatorand the superior rectus muscles are connected by fine fibrousstrands of the superior orbital fascial system, which functionas check ligaments but permit coordinated movement of theupper eyelid with vertical ocular movements. Immediatelyposterior to the superior orbital margin, the LPS musclewidens to �18 mm where a condensation of horizontallyoriented connective tissue is seen running along the musclesheath in a horizontal direction known as the Whitnallsuperior transverse ligament. The Whitnall ligament marks
the junctionwhere the LPS changes from a skeletalmuscle to afibrous sheath, the levator aponeurosis. The levator aponeu-rosis continues inferiorly �15 to 20 mm to insert onto thesuperior two-thirds of the anterior tarsal surface but alsosend fibers to the septum, the pretarsal orbicularis muscle,and the skin, which act to prevent overhang of these struc-tures on elevation of the eyelid and form the upper lid skincrease. The dehiscence of the levator aponeurosis thereforeresults in a superior displacement of the skin crease.
The Whitnall ligament attaches to the trochlear fascia andsuperior oblique tendon medially and sends fibrous connec-tions to the medial retinaculum. It attaches laterally to thefascia surrounding the orbital portion of the lacrimal glandand at the frontozygomatic suture. The ligament is firmlyattached to the levator muscle sheath medially and laterallybut only very loosely attached to the levator muscle centrally.A very thin sheet of fascia passes from the Whitnall ligamentto insert into the superior orbital margin. The Whitnallligament appears to function as a check ligament againstposterior movement of the levator and superior rectusmuscles. The Whitnall ligament forms a circumorbital fascialring in conjunction with the Lockwood ligament. Duringptosis surgery the Whitnall ligament should be maintainedintact wherever possible. If the Whitnall ligament is severed,the levator muscle can prolapse. This loss of support results inthe need for a greater resection than would otherwise berequired. The ligament can also be used as an internal slingduring ptosis surgery.
The levator aponeurosis widens to form the medial andlateral levator horns as it passes inferiorly from the Whitnallligament. The medial and lateral levator horns help to dis-tribute the forces generated by the levator muscle along thelevator aponeurosis, allowing the central aspect of the eyelidto elevate to the greatest extent. The medial horn is moretenuous, accounting for a lateral shift of the superior tarsus inolder patients. The lateral horn is a better-defined structureand separates the lacrimal gland into orbital and palpebrallobes. The lateral levator horn inserts onto the lateral orbitaltubercle of the zygomatic bone and joins the fibers of thecapsulopalpebral fascia of the lower eyelid. The medial hornof the levator aponeurosis inserts onto the posterior limb ofthe medial canthal tendon and the posterior lacrimal crest.The lateral levator aponeurosis horn is divided during levatorrecession procedures for upper eyelid retraction. The levatorhorns should be preserved during ptosis surgery to advancethe dehisced levator aponeurosis but may need to be dividedto allow adequate levator resection of the dysgenic LPS incongenital ptosis.
The Müller muscle is joined to the overlying levatoraponeurosis by a very loose avascular connective tissue layer,allowing separation of these structures during ptosis surgery.The origin of the Müller muscle is from the under surface ofthe levator muscle, 20 to 22 mm above the superior tarsalborder at the origin of the aponeurosis. The Müller muscleruns inferiorly posterior to the levator aponeurosis. It meas-ures�8 to 12 mm in length and has a variable thickness of 0.1to 0.5 mm. The Müller muscle inserts onto the anterior edgeof the superior border of the tarsus.
Facial Plastic Surgery Vol. 29 No. 4/2013
Clinical Anatomy of the Periocular Region Shams et al. 259
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.

Full excursion of the upper eyelid from depression to fullelevation is �15 to 20 mm, which is primarily the action ofthe LPS, with the Müller muscle responsible for �2 mm. Themuscles of the forehead and brow also play a role in elevatingthe eyelid; the frontalis muscle is the primary elevator of theforehead and brow and innervated by the seventh cranialnerve, the facial nerve; the corrugator muscle draws the headof the eyebrows to the nose and is responsible for verticalfurrows on the bridge of the nose. Depression of the head ofthe eyebrow is a result of contraction of the procerus muscle,which can result in horizontal furrows in the skin of theglabellar region of the forehead overlying the bridge of thenose. When examining patients with upper eyelid ptosis, it isimportant to immobilize the forehead and eyebrows toaccurately measure the severity of the ptosis.
The lower eyelid retractors are composed of the capsu-lopalpebral head, capsulopalpebral fascia (CPF), and thesmooth muscle fibers, also known as the inferior tarsalmuscle analogous to the Müller muscle described previously.The capsulopalpebral head originates from the inferior rectusmuscle fascia and as it passes anteriorly from its origin, itsplits to envelop the inferior oblique muscle and reunites asthe inferior transverse or Lockwood ligament (►Fig. 4). Thinfascial extensions from the Lockwood ligament pass forwardto unite with the Tenon capsule and the inferior fornixconjunctiva with additional fibers coursing forward as theCPF. The thinner anterior part of the CPF joins the orbitalseptum, 4 to 5 mm below the inferior border of the tarsalplate, and the suborbicularis fascial layer and extends to theanterior lamellae of the lower eyelid through the orbicularisoculimuscle. This anterior layer does not attach to the inferiormargin of the tarsus but passes forward to the subcutaneoustissues forming the lower eyelid skin crease. The posterior andthicker part of the CPF consists of dense fibers containingscattered smooth muscle fibers and inserts into the lowertarsal plate. The main role of this posterior layer is to pull thelower eyelid inferoposteriorly.
In the Asian lower lid, the line of fusion of the orbitalseptum to the CPF is often higher, or indistinct, with anteriorand superior orbital fat projection, and overriding of thepreseptal orbicularis oculi over the pretarsal orbicularis.
The Conjunctiva
The conjunctiva is a mucous membrane composed of non-keratinizing stratified squamous epithelium, clinically divid-ed into palpebral, forniceal, and bulbar portions. The bulbarconjunctiva is loosely attached to the globe and the palpebralportion firmly adheres to the posterior surface of the tarsalplates (►Figs. 3 and 4). It is also closely applied to the Müllermuscle in the upper lid and the equivalent smooth musclefibers in the lower lid and continues into the forniceal portion.The superior fornix is situated �10 mm above the superiorcorneal limbus. The superior fornix is supported by a finefibrous suspensory ligament, which arises from the fascia ofthe levator muscle and the superior rectus muscle. Theinferior fornix is situated �8 mm below the inferior corneallimbus and is supported by a fine suspensory ligament that
arises from the Lockwood ligament. This is situated justposterior to the CPF and functions to retract the fornixinferiorly during downgaze. The conjunctiva contains a seriesof small accessory lacrimal glands as well as mucous-secret-ing goblet cells. At the medial canthus lies the caruncle,containing multiple sebaceous glands and hair follicles, anda vertical fold of conjunctiva, the plica semilunaris, immedi-ately lateral to it. Access to the medial orbital wall can begained via the transcaruncular approach, through the planebetween the caruncle and the plica semilunaris.
Sensory Nerve Supply of the Eyelids
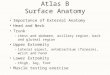
Branches of the ophthalmic and maxillary divisions of thetrigeminal nerve provide the sensory innervation of theeyelids (►Fig. 6). The upper eyelid is innervated by thesupraorbital, supratrochlear, and lacrimal nerves. The medialaspect of the upper and lower eyelids is supplied by theinfratrochlear nerve. Branches of the infratrochlear nerve alsosupply parts of the adjacent eyebrow, forehead, and nose. Thelateral aspect of the upper eyelid and temple is supplied bythe zygomaticotemporal branch of the maxillary nerve. Thecentral aspect of the lower eyelid is supplied by infraorbitalnerve, a branch of the maxillary nerve, and the lateral aspectof the lower eyelid is supplied by the zygomaticofacial branchof the maxillary nerve.
Vascular Supply to the Eyelids
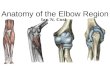
A network of vessels derived from two major sources, theinternal and the external carotid arteries, richly vascularizesthe eyelids (►Fig. 7). Collateralization between the internaland external systems contributes to the rapid wound healingand the low incidence of infection following eyelid surgery.The internal carotid arterial supply is from the supraorbital,supratrochlear, and dorsal nasal branches, which are terminalbranches of the ophthalmic artery medially and the lacrimal
Fig. 6 The sensory innervation of the eyelids and periorbital region.
Facial Plastic Surgery Vol. 29 No. 4/2013
Clinical Anatomy of the Periocular Region Shams et al.260
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.

artery laterally. Two medial palpebral arteries arise from theophthalmic artery as the superior and inferior marginalarcades and pass horizontally and laterally, one to supplythe upper lid and one to supply the lower lid, lying on theanterior tarsal surface�4 mm and 2 mm from the upper andlower eyelid margin, respectively. In the upper lid, a periph-eral arcade arises from the marginal arcade and lies on theanterior surface of the Müller’s muscle, just above the supe-rior tarsal border.
Laterally, the lacrimal artery pierces the orbital septum togive rise to two lateral palpebral arteries, which pass medial-ly, one to the upper eyelid and one to the lower eyelid, andanastomose with the marginal arcades.
The facial artery, the superficial temporal artery, andinfraorbital artery are branches of the external carotid artery.The facial artery continues up to the medial canthal region asthe angular artery, anastomosing with the dorsal nasal artery.The superficial temporal artery supplies the eyelid via thetransverse facial and zygomatic branches. The infraorbitalartery, a terminal branch of the maxillary artery, exits theinfraorbital foramen to anastomose with vessels of the lowereyelid.
The lymphatic drainage from the lateral two-thirds of theupper eyelid and the lateral one-third of the lower eyeliddrains laterally and inferiorly into the deep and superficialparotid and submandibular lymph nodes. Lymph from themedial one-third of the upper eyelid and the medial two-thirds of the lower eyelid drains medially and inferiorly intothe anterior cervical lymph nodes. Extensive disruption ofthese lymphatic channels results in lymphedema.
The Scalp
The central scalp consists of five layers: skin, subcutaneousfibrofatty tissue, galea aponeurotica, loose areolar tissue, andpericranium. The galea aponeurotica links the frontalis andoccipitalis muscles. The subgaleal plane is relatively avascularand the forehead can be peeled forward in this plane aftermaking a bicoronal scalp incision. The pericranium is very
vascular and a pericranial flap can be used to reconstructdeep medial canthal defects in conjunction with a full-thickness skin graft. The pericranium can be lifted from theunderlying bone very easily, and the space thus created isavascular. This space is accessed for endoscopic browliftsurgery.
The Brow
The frontalis muscles are paired extensions of the galeaaponeurotica and insert into the supraorbital dermis byinterdigitating with the orbicularis oculi muscle. The su-perficial and deep galea layers continue to the upperpalpebral margin as the anterior and posterior sheaths ofthe frontalis and orbicularis muscles. A fat pad developswithin a split in the posterior muscle sheath at the brow.The galea is continuous with the superficial temporal fascialaterally, which is continuous with the SMAS inferiorly. Atthe temporal crest there is a fusion plane between thegalea, temporalis, and periosteum. The depressors of thebrow are the procerus, corrugator supercilii, depressorsupercilii, and orbicularis oculi muscles. The procerusmuscles originate from the upper lateral cartilages andnasal bones and insert into glabellar skin at the medialedges of the frontalis. Contraction produces transversewrinkling at the radix of the nose.
The corrugator muscle has both a transverse and anoblique head. The procerus, depressor supercilii, and theoblique head of the corrugators muscle originate from thesuperomedial orbital rim and share a parallel course beforeinserting into the dermis under the medial eyebrow. Thetransverse head of the corrugator supercilii muscle originatesfrom the medial-superior orbital rim and inserts into thedermis just superior to the middle third of the eyebrow. Thistransverse head of the muscle moves the entire eyebrowmedially, producing both vertical and oblique glabellar skincreases. The procerus supercilii muscle and the oblique headof the corrugator supercilii muscle produce oblique glabellarskin lines. The orbital portion of the orbicularis oculi muscleinterdigitates with the corrugators medially and is continu-ous around the lateral canthus into the zygomatic area.Contraction of the orbicularis results in downward displace-ment of the lateral brow. Contraction of the medial head ofthe orbital portion depresses the level of the medial eyebrowbut does not uniformly contribute to the formation of obliqueglabellar skin lines.
The sensory nerves of the forehead are the supraorbitaland supratrochlear nerves. These nerves typically exit fromthe supraorbital notch or foramen; however, in up to 10% ofcases one or both of these nerves may arise from a trueforamen 1 to 2 cm superior to the orbital rim are at risk ofinjury. The supraorbital nerve splits into a deep branch,whichpasses between the galea and periosteum, and a superficialbranch, which enters the frontalis 2 to 3 cm above thesupraorbital rim. The supratrochlear nerve enters the sub-stance of the corrugator and then the frontalis. The motornerve of the forehead is the temporal branch of the facialnerve.
Fig. 7 The vascular anatomy of the eyelids and periorbital region.
Facial Plastic Surgery Vol. 29 No. 4/2013
Clinical Anatomy of the Periocular Region Shams et al. 261
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.

The Temporal Region
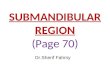
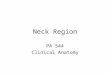
Generally, there are nine layers in the temporal region(►Fig. 8), including the skin, the subcutaneous tissue, thesuperficial temporal fascia (temporoparietal fascia), the looseareolar layer, the superficial layer of the deep temporal fascia,the superficial temporal fat pad, the deep layer of the deeptemporal fascia, the deep temporal fat pad, and the temporalismuscle. The superficial temporal fascia in the temporal regionis the most superficial layer beneath the subcutaneous tissue.It is continuouswith the galea superiorly, the frontalis muscleanteriorly, and the SMAS inferiorly. It contains the frontalbranch of the facial nerve and the superficial temporal artery.Deep to the superficial temporal fascia is a loose areolarfascial layer, otherwise known as the intermediate temporalfascia or subaponeurotic plane. Deep to this fascia is the deeptemporal fascia that covers the temporalis muscle. It is easilyrecognized by its thick white glistening surface and can beconfirmed by making a small cut in the fascia to expose theunderlying temporalis muscle. For an endoscopic browlift thedissection from the temple to the orbital margin should bemade along this layer, with the frontal branch of the facialnerve lying protected above this layer in the superficialtemporal fascia. A few centimeters above the zygomaticarch, the deep temporal fascia splits into two layers: thesuperficial and the deep layers of the deep temporal fascia.These insert onto the anterosuperior and posterosuperioraspects of the zygomatic arch, respectively. Between thesetwo layers lies the temporal fat pad.
The Facial Nerve
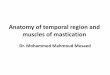
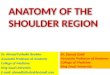
The facial nerve supplies most of the muscles of facialexpression and motor function of the eyelids. The twobranches of the nerve, the upper (temporozygomatic) andthe lower (cervicofacial) branches, pass within the substanceof the parotid gland before dividing into the main distalbranches. The upper division divides into the frontotemporaland zygomatic branches (►Fig. 9), which innervate the
frontalis muscle, superior orbicularis muscle, transversehead of the corrugator supercilii muscle, and superior endof the procerus muscle. The lower cervicofacial division givesrise to the buccal, mandibular, and cervical branches, whichinnervate muscles of the lower face and neck.
At the anterior border of the parotid gland, these brancheslie on the surface of the masseter muscle deep to theparotidomasseteric fascia. The temporal nerve is the smallestof the branches, has the fewest number of interconnections,and in the majority of individuals is a terminal branch, oftenshowing the least degree of recovery following a facial palsy.
The frontotemporal branch of the facial nerve divides intotwo to four branches that exit the parotid gland within theparotid-masseteric fascia and continue within the interme-diate temporal fascia across the zygomatic arch. The fronto-temporal branch becomes superficial once it crosses thezygomatic arch where the nerve is most vulnerable to injury.
Between 1.5 to 3.0 cm above the superior border of thezygomatic arch and 0.9 to 1.4 cm posterior to the lateralorbital rim the frontotemporal branches transition from theintermediate temporal fascia to run on the undersurface ofthe superficial temporal fascia before entering the frontalis ororbicularis oculimuscle. A series of bridging vessels, includingone larger sentinel vein, are encountered between the super-ficial and deep temporal fascia during the dissection in thetemporal region. These bridging vessels point to the frontalbranch of the nerve as it courses through the superficialtemporoparietal fascia.
In the temple, the nerve runs within the superficialtemporoparietal fascia and supplies the frontalis muscle,the superior fibers of the orbicularis muscle, the procerusand corrugator supercilii muscles (►Fig. 8). It is important tostay on the glistening fibers of the deep temporal fascia deepto the temporoparietal fascia to avoid injury to the nerveduring surgical dissections in this area. In the brow region, thefrontal branch runs �2 cm above the brow.
Fig. 9 Branches of the facial nerve
Fig. 8 The fascial planes of the temporal region and the path of thefrontal branch of the facial nerve in this region. Abbreviation: DTF,deep temporalis fascia.
Facial Plastic Surgery Vol. 29 No. 4/2013
Clinical Anatomy of the Periocular Region Shams et al.262
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.

The zygomatic branch of the facial nerve supplies theinferior orbicularis oculi muscle, inferior end of the procerusmuscle, depressor supercilii muscle, oblique head of thecorrugator supercilii muscle, and medial head of the orbicu-laris oculi muscle.
SMAS and Midface Anatomy
The SMAS is a superficial continuous fibromuscular layer ofthe face and neck, which invests and interlinks all thesuperficial muscles of facial expression. The SMAS can bedivided and repositioned or plicated to augment or contourthe elevation of the malar fat pad. It extends from the malarregion superiorly to become continuous with the galeaaponeurotica, inferiorly to join the platysma, and laterallyto invest in the parotid fascia. In the temporal region, theSMAS blends into the superficial temporoparietal fascia. TheSMAS invests the superficial mimetic muscles, including theplatysma muscle, orbicularis oculi muscle, occipitofrontalismuscle, zygomaticus muscles, and the levator labii superiorismuscle. The SMAS attaches to the skin via ligamentousextensions. It varies in thickness and becomes much thinnerand less distinct as it extends toward the nasolabial fold.
The malar fat pad is a collection of fat overlying the malareminence, which lies on andwithin the anterior surface of theSMAS. In the lower part of the face, the facial nerve branchesare deep to the SMAS and innervate the facialmuscles on theirundersurface. The deep facial muscles are an exception to thisrule: the levator anguli oris, the buccinator, and the mentalisare all innervated on their superficial surface. These facialnerve branches are protected if a dissection is kept superficialto the SMAS in this location.
The malar soft tissues are suspended from the malareminence and maxilla by the zygomatic retaining ligamentslaterally and buccomaxillary ligaments medially. The malarprominence descends inferomedially with aging to deepenthe nasolabial crease and expose the lateral orbital rim. It iscomposed of a subcutaneous malar fat pad with underlyingorbicularis oculi muscle. Deep to this is the SOOF, which is
intimately associated with the periosteum of the infraorbitalrim and maxilla and the insertions of the zygomaticus majorand minor muscles. Motor nerve supply to the muscles of themidface comes from the zygomatic and buccal branches of thefacial nerve traveling along the deep surface of the muscles.Sensory innervation of the midface comes from the seconddivision of the trigeminal nerve, the infraorbital nerve, whichexits the infraorbital foramen, and the zygomaticotemporalbranch of the trigeminal nerve that exits through the body ofthe zygoma. The zygomaticotemporal nerve supplies thelateral temple region of the scalp and is encountered in amidfacial dissection, although it is rarely visualized.
Summary
Understanding the anatomy of the periocular region is aprerequisite to successful oculoplastic and oculofacial surgeryand essential in minimizing adverse outcomes.
References1 Most SP, Mobley SR, Larrabee WF Jr. Anatomy of the eyelids. Facial
Plast Surg Clin North Am 2005;13:487–492, v2 Ridgway JM, Larrabee WF. Anatomy for blepharoplasty and brow-
lift. Facial Plast Surg 2010;26:177–1853 Oh SR, Priel A, Korn BS, Kikkawa DO. Applied anatomy for the
aesthetic surgeon. Curr Opin Ophthalmol 2010;21:404–4104 Kakizaki H, Malhotra R, Selva D. Upper eyelid anatomy: an update.
Ann Plast Surg 2009;63:336–3435 Kakizaki H, Malhotra R, Madge SN, Selva D. Lower eyelid anatomy:
an update. Ann Plast Surg 2009;63:344–3516 Lam VB, Czyz CN, Wulc AE. The brow-eyelid continuum: an
anatomic perspective. Clin Plast Surg 2013;40:1–197 Babakurban ST, CakmakO, Kendir S, Elhan A, Quatela VC. Temporal
branch of the facial nerve and its relationship to fascial layers. ArchFacial Plast Surg 2010;12:16–23
8 Ghassemi A, Prescher A, Riediger D, Axer H. Anatomy of the SMASrevisited. Aesthetic Plast Surg 2003;27:258–264
9 Leatherbarrow B. Oculoplastic Surgery, 2nd ed. London: InformaHealthcare; 2010
10 Yanoff M, Duker JS. Ophthalmology, 3rd ed. London: Mosby; 2008
Facial Plastic Surgery Vol. 29 No. 4/2013
Clinical Anatomy of the Periocular Region Shams et al. 263
Dow
nloa
ded
by: W
orld
Hea
lth O
rgan
izat
ion
( W
HO
). C
opyr
ight
ed m
ater
ial.