Embed Size (px)
Citation preview
Clinical Alarm Management
“Stop the Nuisance” Maria Carpenter MSN, RN, AG CNS-BC, CCRN
Laura Solano MSN, RN, CCNS, PCCN, CCRN K

Objectives
• Discuss aspects of alarm safety
• Discuss implications of alarm fatigue
• Discuss changing culture of alarm management
• Discuss tools and methods used to improve clinical alarm management
• Discuss widening default parameters in cardiac monitoring and the impact it has had at PPMC

Alarm Safety Recognized
2005-2009 linked 566 deaths to
monitor alarms

Research shows:
• Response rate improves with alarm reliability, low work load conditions and trust in the alarms
• 68 – 99% of all alarms are false or nonactionable
• Nurses spend 16-35% of their time answering alarms

Alarm Fatigue
• Occurs when device alarms sound frequently or without a sign of emergent patient danger.
▫ Nurses stop recognizing the alarm as a sign of emergent danger
▫ Alarm responders become desensitized delaying recognition and response to alarms
▫ Sentinel events have occurred
Clinically Relevant Alarm
• Definition:
▫ Alarm for which a diagnostic or therapeutic decision is required to be made. Actionable alarm

Nuisance alarm
• Definition
▫ an alarm that indicates a parameter has been violated, but does not require clinical intervention.
▫ “cry wolf” effect

Alarm Management
• Alarm committee
• Changing the culture
• Healthy work environment
• Consequences:
▫ Clinical effects on patients and families
▫ Affects quality and patient safety
▫ Effects staff

Stop the Nuisance
• Where to begin?
• Start with the basics
▫ Patient education
▫ Change electrodes daily
▫ Skin prep, lead selection, proper storage
▫ Proper fitting SpO2 finger sensors
▫ Stability of capnography cannulas

Education and Staff Competency
• Proactive use of pause
▫ Suctioning, Drawing blood from aline
• When to use ST segment detection
• When to turn off pacemaker detection
• When to turn off irregular alarms
• Alarm customization, individualization
• Clinical Alarm Management Policy
▫ Guide to safe practice

Inoperable Alarms
• INOP alarm (such as leads off)
▫ Sentinel events
▫ Considered a priority
▫ Treat with an immediate response!
▫ Change the culture!
Alarms must be audible
• Respond in a timely manner.
• All alarms must be ‘on’ and audible to staff.
• Does your technology allow for alarms to be turned off in the room yet audible at the desk?
• Can the volume be turned down in the room : sleep mode / comfort mode?

Alarm Customization
• Individualize to your patient’s condition
▫ Known afib – turn off irregular alarm / afib alarm
▫ Patient on a ventilator – turn off RR alarm
▫ Adjust parameters

Alarm Champions (staff)
• Involve all staff
• Seek out nuisance alarms and work to find solutions
• Assist coworkers to customize alarms
• Conduct huddles on alarm management
• Implement initiatives such as ‘no pass zone’

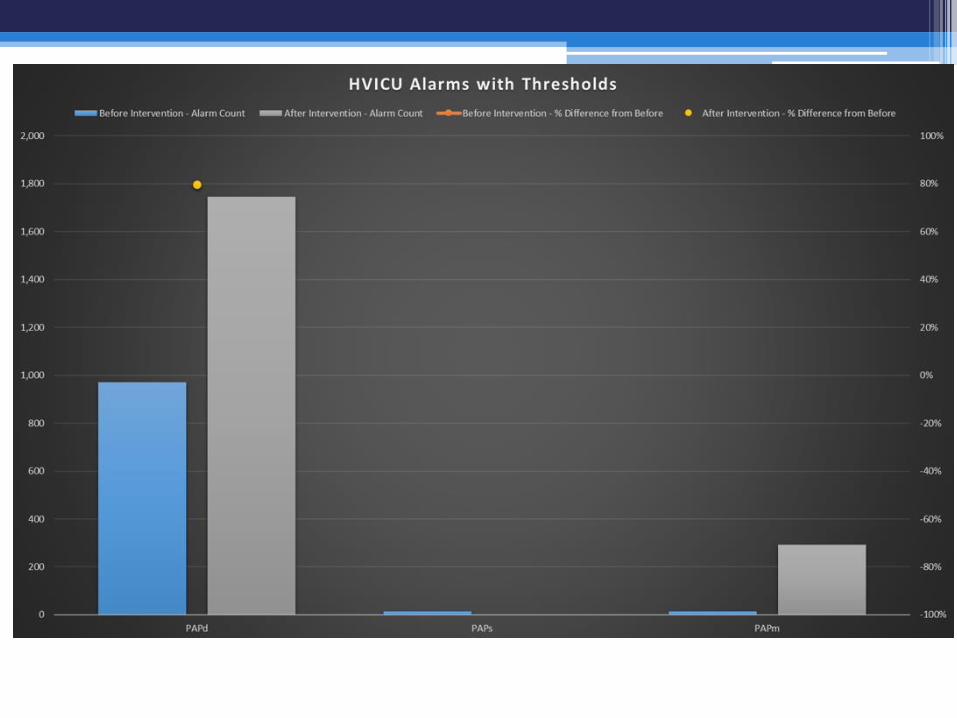
Effects of customization


Rethinking defaults
• Widen default parameters so that alarms are actionable • Add delay so that false alarms have a chance to
autocorrect prior to sounding • Eliminate duplicative alarms • Turn off alarms for conditions that we no longer treat • For some signals, a visual alarm can work better than
another beeping sound

Analyze your data
• Pareto diagram to determine highest areas of impact
• Evaluate where the violators lie within those areas
• Utilize unit level data to determine comfort level of default changes against their impact


What if:



Pre – 6/20/17 - 6/27/17 Post - 5/22/2017-5/29/2017

4/1/17-5/1/17 10/7/17- 11/6/17

Post default changes: RR in TSICU

Widen defaults
unit by unit
Previous Defaults HR 55 to 120 RR 8 to 30 SBP 90 to 160 Mean 60 to 90 SPO2 90 to 100% PVCs >10



References
.
Cvach, M., Monitor Alarm Fatigue: An integrative Review”, Biomedical Instrumentation & Technology, July/Aug 2012,
268-277.
Cvach, M., Graham, KC. (2010) Monitor alarm fatigue: standardizing use of physiological monitors and decreasing
nuisance alarms. Am J Crit Care. 19(1):28-34
Cvach MM, Biggs M, Rothwell KJ, Charles-Hudson C. (2012) Daily electrode change and effect on cardiac alarms: an
evidence-based practice approach. J Nurs Care Qual. 28(3): 265-271
Cvach, M., Monitor Alarm Fatigue: An integrative Review”, Biomedical Instrumentation & Technology, July/Aug 2012,
268-277.
Cvach, M., Graham, KC. (2010) Monitor alarm fatigue: standardizing use of physiological monitors and decreasing
nuisance alarms. Am J Crit Care. 19(1):28-34
Cvach MM, Biggs M, Rothwell KJ, Charles-Hudson C. (2012) Daily electrode change and effect on cardiac alarms: an
evidence-based practice approach. J Nurs Care Qual. 28(3): 265-271
Gross, B., et al. “Physiologic monitoring alarm load on medical/surgical floors of a community hospital”, Biomedical
Instrument Technology, Spring 2011, Sppl., pp 29-36.
Gross, B., et al. “Physiologic monitoring alarm load on medical/surgical floors of a community hospital”, Biomedical
Instrument Technology, Spring 2011, Sppl., pp 29-36.
Hsu, T., Ryherd, E. Waye, K.P., & Ackerman. (2013) Noise pollution in hospitals: impact on patients. J Clin Outcomes
Manage 19(7): 301-309
Hsu, T., Ryherd, E. Waye, K.P., & Ackerman. (2013) Noise pollution in hospitals: impact on patients. J Clin Outcomes
Manage 19(7): 301-309