Embed Size (px)
DESCRIPTION
CLHIN Hospitals ALC Rehab Steering Committee Phase One Report – Orthopedics. July 13, 2012 - FINAL Malcolm Moffat, Co-Chair Helena Hutton, Co-Chair Zenita Hirji, Executive Project Lead. Presentation Outline. Provincial Context/Background Overview of ALC Rehab Project Purpose - PowerPoint PPT Presentation
Citation preview

CLHIN Hospitals ALC Rehab Steering CommitteePhase One Report –
OrthopedicsJuly 13, 2012 - FINAL
Malcolm Moffat, Co-ChairHelena Hutton, Co-Chair
Zenita Hirji, Executive Project Lead

2
Provincial Context/Background
Overview of ALC Rehab Project◦ Purpose◦ Key areas of focus◦ Steering Committee composition◦ Draft workplan
Overview of Current State of Rehab in CLHIN◦ Draft ALC Rehab Survey Results◦ Performance Targets
Orthopedic Symposium
Draft Recommendations on Orthopedics
Presentation Outline

3
Three of the four conditions, knee replacements excepted, contribute significantly to the ALC challenges faced by acute care hospitals.
Collectively, they consume a significant amount of rehabilitative resource (55% of rehab provincial patient days)
They have well developed, recognized best practice guidelines for rehabilitative patient care
Uptake of the best practices across the continuum has been inconsistent throughout the province.
Challenges faced in the implementation of these best practices are indicative of systemic challenges in rehabilitative care.
Total Joints, Hip Fracture and Stroke

4
Ontario studies provide strong evidence on the effectiveness of home-based rehab protocols following TKR/THR
“IP compared with home-based rehab following primary unilateral THR or TKR: a randomized controlled trial” N. Mahomed et al, 2008CONCLUSIONS: Despite concerns about early hospital discharge, there was no difference in pain, functional outcomes, or patient satisfaction between the groups. We recommend the use of a home-based rehab protocol following elective primary joint replacement as it is the more cost-effective strategy.

5
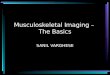
Correlation of % Joint Replacements Discharged Home & Readmissions/Revisions (2009/10)
…with no observed relation to quality measures or length of stay
Hospital Name Total CasesAvg LOS of Patients
Discharged to Inpatient / LTC / transfers
Avg LOS of Patients Discharged Home Proportion of Patients
Discharged Home
Rate of Readmission within 30 days after
surgery
SUNNYBROOK HEALTH SCIENCES 2,053 5.3 5.1 60.2% 3.9%
HAMILTON HEALTH SCIENCES 1,548 10.4 5.1 88.7% 3.9%OTTAWA HOSPITAL 1,466 6.4 4.2 66.8% 5.3%SCARBOROUGH HOSPITAL (THE) 1,253 5.2 3.9 74.5% 2.5%LONDON HLTH SCIENCES CTR 1,247 10.0 4.5 85.6% 8.0%QUEENSWAY-CARLETON HOSPITAL 1,098 2.7 4.3 27.6% 4.7%NIAGARA HEALTH SYSTEM 1,087 9.1 5.6 93.7% 4.0%UNIVERSITY HEALTH NETWORK 980 5.2 4.5 60.1% 4.7%WILLIAM OSLER HEALTH CENTRE 963 4.5 4.9 56.0% 2.5%ST MICHAEL'S HOSPITAL 887 4.7 4.0 45.2% 5.1%GRAND RIVER HOSPITAL CORP 861 9.1 4.5 90.2% 4.5%NORTH YORK GENERAL HOSPITAL 776 5.0 4.6 43.8% 3.2%TRILLIUM HEALTH CENTRE 773 5.3 5.3 87.6% 2.8%HOTEL-DIEU GRACE HOSPITAL 706 13.1 5.0 97.0% 3.1%
Top 15 Hospitals by Volume (2009/10)
5

6
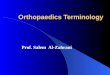
In January, the Orthopedic Expert Panel made recommendations to the Ministry on provincial targets for discharge disposition and length of stay for THR / TKR patients

7
Goal: To reduce ALC days related to lack of access to Rehab by developing a systematic approach to facilitate equitable access to appropriate rehab at the appropriate time
Four clinical areas that are identified as being the greatest contributors to the ALC challenges: ◦ hip replacement, knee replacement, stroke, and
hip fracture.
Overview of ALC Rehab Project

8
ALC Rehab Steering Committee Steering Committee established in January 2012
◦ Reports up to CLHIN Hospital/LHIN/CCAC CEO Leadership Forum
Malcolm Moffat – Co-chair, CEO, St. John’s Rehab Helena Hutton – Co-chair, VP, Southlake Regional HC
◦ Alexis Dishaw, HRRH◦ Annette Marcuzzi, CLHIN◦ Dr. Brian Berger, YCH◦ Dr. Daniel Wong, NYGH◦ Dr. Roshan Shafai, SRHC◦ Julie Sullivan, MSH◦ Shannon Landry, SMH◦ Val Thompson, NYGH◦ Winston Cheuk, YCH◦ Yvonne Ashford, CCAC◦ Zenita Hirji, Executive Project Lead

9
Phase One – Orthopedics (TJR and Hip Fractures) Focus of phase one report will be on:
Reviewing the current state of TJR and Hip Fractures care management in CLHIN hospitals
Identify of gaps in best practice guidelines and achievement of performance targets, in this patient population
Capacity assessment and recommendations on strategies aimed at reducing ALC days for rehab and improving hospital performance on key metrics for TJR and Hip Fractures
Phase Two – Stroke Focus of phase two report will be on:
Reviewing the current state of stroke care management in CLHIN hospitals Identify of gaps in best practice guidelines and achievement of performance
targets, in this patient population Capacity assessment and recommendations on strategies aimed at reducing ALC
days for rehab and improving hospital performance on key metrics on stroke care
Workplan

10
CURRENT STATE ANALYSIS OF CLHIN
REHAB CARE

11
Purpose - To develop a Central LHIN snapshot of:
◦ Inflow into IP Rehab - Patients designated as ALC and awaiting placement in an inpatient rehabilitation bed/facility (Survey One)
◦ Outflow from Rehab - Patients in designated rehab beds awaiting placement in another care setting (Survey Two)
2 surveys to be completed over two separate weeks: Week One - Jan. 30th to Feb. 5th) and Week Two (Feb.13th to 19th)◦ Total of 156 patients during two week period◦ Similar response rates for each week
Survey was designed by (and has previously been used in another study conducted by) the GTA Rehab Network
HOSPITAL ALC REHAB SURVEY RESULTS

12
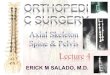
• Top 70% of Primary Diagnoses associated with patients designated as ALC awaiting IP Rehab care - summarized in table
• Stroke and Hip Fractures
comprise 31% of survey diagnoses
• No major ALC issues regarding access to IP rehab for primary hip and knee replacements
Summary of Primary Diagnoses – ALC Rehab
Primary Diagnosis No. of Pts.Stroke 34 Hip Fracture 15CVA 4pneumonia 4spinal cord injury 3acute renal failure 2CDA 2C-Difficile 2Cellulitis 2Hip 2Hyponatremia 2ischemic leg 2L 45 Lesion 2left femur # 2OA left hip 2pyelonephritis 2Respiratory Failure, West Nile Encephalitis 2Sepsis 2Sepsis/ C-Diff 2A. Fib. 1Acute Cholecystitis 1ARF/obstruction cause 1Bilateral Knee Replacement 1Biliary Sepsis 1Bowel Obstruction 1Bradycardia 1C.diff colitis, urinary retension, ARF 1CAD 1CAD-Left card. endocar. 1CHF 1Cholecystitis 1Colon Cancer 1Community Axquired Pneumonia 1Complete Heart Block 1COPD Exacerbation 1COPD, Pleural effusions, Chronic A.Fib 1Diabetic Foot 1Dialysis Line Sepsis 1Diarrhea/,# ankle, syncope 1Failure to Cope 1

13
Referral to Rehab Reasons for “no referral”
included the following:
◦ Awaiting nursing and PT forms to be completed
◦ Waiting nursing/PT/medical forms to be done
◦ Pt. already applied to LTC -also applying to LTLD as per family's request
◦ Application in process (waiting for medical, nursing, and PT forms)
◦ RMR initiated. Forms being completed by team & MRP. Will "send" RMR as soon as all forms completed by team & MRP
47% of patients were referred to more than one rehab facility Majority of patients referred to
only one rehab facility
Have you received any response to the rehab referrals?Yes - accepted 61%No 10%(blank) 9%Decision is pending 8%Yes - referral declined 6%Yes - referral is waitlisted 5%Other 1%

14
Waits associated with ALC Rehab…
Wait One
Wait Two

15

16
Variation in wait times by facility

17
Referral Response Time (in Days) – Wait Two

18
Survey Results Summary• Hip Fractures and Stroke comprise 31% of the patient population designated ALC and awaiting
placement in an IP Rehab facility• No major ALC issues regarding access to IP rehab for primary hip and knee replacements
For the most part, we know that the following special care needs comprise the highest volume of ALC patients waiting IP Rehab care
• Incontinence• Wound Care • IV Peripheral
Wait times vary by age group and significant variation exists in wait times by facility (for both wait 1 and wait 2)
Wait 1 (ALC Designation to Rehab Referral)◦ 70% of Patients are referred to an IP Rehab facility within 3 days of being designated as ALC◦ 58% are referred within 1 day
Wait 2 (Rehab Referral to Acceptance)◦ 80% of Patients had referral response times of 2 days or less
Geriatric, Stroke, and MSK represent 62% of the most common type of rehab being referred to
Low volume of Rehab patients that are designated ALC and awaiting placement◦ average number of days waiting varies by facility◦ Longer waits for Home care and LTC placement from IP Rehab units/facilities

CLHIN Hospitals Rehab Current State & Performance Indicator Results

20
IP Acute - Overall TJR Volumes by Hospital
• Majority of discharges (65%) are TKR patients
THR TKR Ttl Joints THR TKR Ttl Joints THR TKR Ttl Joints
HRRH - Church 137 275 412 111 311 422 116 352 468
HRRH - Finch 58 170 228 60 172 232 59 201 260
MSH 134 328 462 160 304 464 164 313 477
NYGH 253 365 618 255 363 618 287 388 675
SRRH 182 343 525 212 315 527 239 353 592
YCH 121 211 332 118 192 310 121 220 341
Total 885 1,692 2,577 916 1,657 2,573 985 1,828 2,813
2009/10 2010/11 2011/12 (YTD_Q3_Annualized)
Data Source: CIHI DAD – TJR includes primary, unilateral ,elective hip/knee replacements

21
Inflow-Central LHIN TJR Surgeries by Patient Residence
• Approximately 900 to1000 patients who live outside the Central LHIN, get their TJR procedure done at a Central LHIN hospital
• Impact on CCAC and OP Rehab Services
Patient LHIN: 2009/10 2010/11 2011/12 (YTD_Q3_Annualized)
Central 1,653 1,670 1,792 Central East 324 361 385
Toronto Central 163 175 204 Central West 167 118 191 NS Muskoka 109 115 121
North East 83 57 51 M Halton 43 58 44
Other 35 19 25
Total from Other LHINs 924 903 1,021
Total 2,577 2,573 2,813 % from other LHIN 36% 35% 36%Data Source: CIHI DAD – TJR includes primary, unilateral ,elective hip/knee replacements

22
Outflow – Central LHIN Residents who go Outside LHIN for TJR surgery
• Over 1000 patients per year that live in the Central LHIN get their TJR procedure at a hospital outside the Central LHIN
• Inflow/Outflow almost balance – net zero effect
2009/10 2010/11 2011/12 (YTD_Q3_Annualized)
Sunnybrook 287 305 291Scarborough Hospital 175 182 173UHN 131 141 151St Michaels 108 117 112Mt Sinai 86 107 97Toronto East 96 89 80St Joseph's 47 45 57William Osler 38 49 44Rouge Valley 29 24 40Other 87 86 80
Total 1,084 1,145 1,125 Data Source: CIHI DAD – TJR includes primary, unilateral ,elective hip/knee replacements

23
% of Patients Discharged Home by LHIN
Data Source: CIHI DAD – TJR includes primary, unilateral ,elective hip/knee replacements. Includes patients discharged home with or without services as per Orthopaedic Scorecard /HSAA definition

24
IP Rehab - TJR Average Admission Age by LHIN
Data Source: CIHI NRS, 2010/11

25
IP Rehab - TJR Median Admission FIM by LHIN
Data Source: CIHI NRS, 2010/11

26
IP Rehab – Hip Fracture Avg Admission Age by LHIN (2010/11)
Data Source: CIHI NRS, 2010/11

27
IP Rehab–Hip Fracture Median Admission FIM by LHIN
Data Source: CIHI NRS, 2010/11

Results of Orthopaedic Stakeholder Engagement – ALC Rehab Symposium on Orthopaedic Care

29
Two Symposiums:
Physician Stakeholder Session – April 24th
◦ Raise awareness amongst physicians of provincial efforts◦ Discuss impact of provincial initiatives on care planning◦ Provide an opportunity for physicians to render their input to
how to implement the proposed changes
Administrative Stakeholder Session – April 25th
◦ Raise awareness of provincial efforts◦ Provide an opportunity to hear about other LHIN-based efforts ◦ Discuss potential impact of MOHLTC funding reform ◦ Provide an opportunity for input on how to implement the
proposed changes
Stakeholder Engagement Sessions

30
Series of recommendations arising out of stakeholder engagement sessions and steering committee deliberations
Key Areas:1. System right-sizing2. Standardized Care Plans3. Patient Flow4. Location of OP Rehab5. Communication6. Funding Reform
Recommendations

31
1. Primary, Unilateral Hip & Knee Replacements◦ In accordance with Ontario Bone & Joint Network best-practice guidelines and
MOHLTC/Orthopedic Scorecard performance targets for orthopaedic care, the acute care system will reduce its reliance on inpatient rehabilitation for TJR patients, and move towards a 90% (+ 9) rate for discharge home (with appropriate supports)
◦ Therapy for the 90% discharged home will include a combination of in-home CCAC services, hospital, community based outpatient services (details on patient care guidelines to follow)
◦ In addition, a target ALOS of 4.4 days will be implemented for this patient population
2. Hip Fractures◦ Changes in management of TJRs will provide earlier access to inpatient rehabilitation for Hip
Fracture patients◦ Increased use of inpatient rehabilitation for Hip Fracture patients, in accordance with best
practice guidelines and standardized care pathways (to be developed)
These changes combined should create additional IP Rehab capacity for stroke patients (CLHIN Phase Two report on Stroke to be released in Fall 2012)
A Rehab Capacity and Sizing Working Group will be established to consider the implications for the siting of MSK and Stroke services within the Central LHIN.
System Right-sizing

32
3. Need to develop standardized care pathways that can be used consistently across all CLHIN Hospitals in management of TJRs and Hip Fractures
◦ Lack of existing documentation in current system is creating variation in care management of these patients
◦ Need to build on existing best practice guidelines and care pathways developed in other LHINs i.e. TC LHIN toolkit
◦ Pathway should include guidelines for home-based and/or hospital-based/other OP physiotherapy
◦ Standardization of processes is required and clear targets need to be established throughout episode of care. For example, what should we expect with regards to patient outcomes at day 1, day 2, etc…
◦ Messaging needs to be multi-lingual
4. Standardized pathways for TKR should include post-surgical guidelines for flexion and extension. For example,◦ If flexion does not reach 90 degrees within 4 weeks post surgery surgeons should
be notified◦ flexion of 110-120 degrees at the end of the therapy◦ full extension of the knee prior to being discharged from therapy
Standardized Care Pathway

33
5. Care pathways need to delineate clear decision-making criteria for pathway algorithms
◦ For example, factors such as patient age, weight-bearing status, cognitive impairment, and other co-morbidities need to be factored into creation of pathway algorithms
◦ Standardized way of triaging patients based on early and timely access to rehab◦ Should involve other members of clinical team in application of discharge criteria
6. Creation of implementation plan to ensure pathway adoption and necessary allocation/re-allocation of resources, where necessary
◦ Resources may need to be re-allocated both within organizations and system-wide to meet pathway care requirements
◦ Augmentation of OP physiotherapy/rehab will be required to ensure timely access to post-acute care
◦ Impact on rehab skill mix also needs to be considered as more TJRs are referred to OP settings
Standardized Care Pathway (cont.)

34
7. Need to improve timeliness of rehab referrals and response times◦ ALC Rehab survey results showed that significant variation exists in wait times by
facility (for both wait 1 and wait 2) 70% of Patients are referred to an IP Rehab facility within 3 days of being designated as ALC 80% of Patients had referral response times of 2 days or less
◦ Weekend resources may need to be augmented to ensure timely referrals and improve overall patient flow effectively to establish 7 day a week business processes
◦ Relatively efficient in overall management of ALC days for wait one and wait two (majority are short stay discharges)
◦ Findings suggest that while rehab does account for substantial number of ALC cases, they are not the long stay ALC patients
8. Strong support for ensuring adherence to GTA Rehab Network protocols on referral to sub-acute system
◦ Different standards are being applied on acceptance of referrals; even under RMR sub-acute facilities are asking for additional information
◦ Inconsistencies and lack of standardization in application process ◦ Some facilities have noted that it takes anywhere between 60-90 min per patient
to issue out referral
Patient Flow

35
9. CCAC requirements for “medically stable” patient needs to be re-visited◦ Messaging that patient has to be identified as ALC before CCAC RAI-HC
assessment can be undertaken is not correct◦ CCAC requirements state patient must be “medically stable” before assessments
can be done◦ However, this does not facilitate efficient patient flow because patients often end
up waiting (post ALC designation) for assessment to be completed◦ Need to investigate feasibility of implementing parallel processes so that
assessments can be undertaken earlier in acute care episode to allow for effective discharge planning
10. RMR electronic referral must include TCLHIN rehab facilities and CLHIN acute hospital based rehabilitation units
◦ Current system doesn’t necessarily ensure timely and transparent access to patients awaiting placement in IP Rehab
◦ Hospitals with designated rehab beds/units often give preferential access to their patients
◦ Enabling electronic referral to any rehab bed within the CLHIN system would create a level-playing field and ensure access to the “right bed at the right time”
◦ At a minimum, standardized response times should be set for responses to referral requests and compliance to response time targets should be monitored
Patient Flow (cont.)

36
11. Location of OP Rehab should leverage existing capacity and ensure equitable access across Central LHIN
◦ TCLHIN report recommends using hospital based OP physio clinics to maximize cost –efficiency and facilitate standardized approach to rehab care
◦ However, CLHIN geography is different; key principle needs to be geographical equity ◦ CLHIN may not be able to locate OP rehab exclusively at Hospital sites due to rural geography,
but also need to consider issues of critical mass in more rural areas; need to strike a balance between patient travel times and critical mass and possibly leverage home-based physio in more rural areas of CLHIN
◦ Is it a possible for CCAC to have congregate care type clinics in more rural settings? can LHIN contract services from private clinics?
◦ Parking discounts at hospital-based settings is a fundamental requirement to equitable access◦ Investigate access to care in evenings and weekends; clinic access should not just be Monday
to Friday, but also on weekends and evenings – want to encourage people to get back to work◦ Optimize LTC facilities for those patients who came from LTC
Location of OP Rehab

37
12. Irrespective of OP Rehab setting, there needs to be standardized outcome measures collected at standardized times and LT follow-up is encouraged
◦ Need to ensure that appropriate communication processes are set up with surgeon
◦ Consider creation of accredited OP rehab care providers/facilities which are appropriately trained on care pathway and required physiotherapy regimen
◦ Facility/providers should not be paid until outcome measures are achieved◦ Strengthen relationship outside of traditional rehab model –relationship to active
facilities i.e. fitness centres? Community centres?
Location of OP Rehab (cont.)

38
13. Consistent strategy and messaging required to manage patient expectations regarding access to IP rehab post-surgery
◦ no legislative requirement for patient to identify 3 choices for placement in IP rehab – only applies to LTC home placement
◦ Need for consistent patient education strategy and information pamphlets and/or letters identifying OP rehab options and locations of OP physiotherapy clinics (within and outside of the hospital setting
14. Need for strong relationship between care provider and surgeons post-discharge
◦ Consider establishment of clinic days where OP physio care providers and surgeon meet to discuss patient progress and treatment plans
◦ Strong recommendation for IT communication enablers between CCAC, Surgeon’s offices, and hospital
Communication

39
15. Need for further clarity on MOHLTC Funding Reform and impact of newly proposed Quality Based Procedure funding on the delivery of orthopaedic care in Central LHIN◦ General belief that new funding model will create less variation and more
standardized pathways and perhaps even Increase quality◦ Focus on outcomes will become paramount◦ Concern regarding double dipping (private funding under insurance plans for some
patients vs. MOH public funding; Private funding options should be exhausted first prior to use of public funds
16. Impact of new funding model on hospitals and physicians not clearly understood ◦ Will new funding model lead to creation of centres of excellence in certain
procedures?◦ What impact will funding model have on use of Ortho implants? Hospitals may
want to consider developing tighter protocols for when certain high-cost implants are used
◦ Hospital Decision Support, Health Records and IT resources will be key to measuring hospital performance in new era of funding
◦ Will we be re-distributing OR time depending on physician efficiency? Re-allocation of blocks due to funding mechanism, volume, quality, etc…?
Funding Reform

40
Communicate and obtain feedback on draft Phase One report to CLHIN system leadership and symposium attendees
Finalize Phase One report
Establish necessary working groups (revise workplan, as necessary) and focus on Implementation of recommendations◦ Capacity & Sizing Working Group◦ Pathway & Flow Working Group
Proceed into Phase Two review of Stroke services within CLHIN
Next Steps…