Embed Size (px)
Citation preview

Clearance of pathological antibodies usingbiomimetic nanoparticlesJonathan A. Coppa,b, Ronnie H. Fanga,b, Brian T. Luka,b, Che-Ming J. Hua,b, Weiwei Gaoa,b, Kang Zhanga,c,and Liangfang Zhanga,b,1
aDepartment of Nanoengineering, bMoores Cancer Center, and cDepartment of Ophthalmology and Shiley Eye Center, University of California, San Diego,La Jolla, CA 92093
Edited by Robert Langer, Massachusetts Institute of Technology, Cambridge, MA, and approved August 8, 2014 (received for review July 1, 2014)
Pathological antibodies have been demonstrated to play a key role intype II immune hypersensitivity reactions, resulting in the destructionof healthy tissues and leading to considerable morbidity for thepatient. Unfortunately, current treatments present significant iatro-genic risk while still falling short for many patients in achieving clinicalremission. In the present work, we explored the capability of targetcell membrane-coated nanoparticles to abrogate the effect of patho-logical antibodies in an effort to minimize disease burden, without theneed for drug-based immune suppression. Inspired by antibody-drivenpathology, we used intact RBC membranes stabilized by biodegrad-able polymeric nanoparticle cores to serve as an alternative target forpathological antibodies in an antibody-induced anemia disease model.Through both in vitro and in vivo studies, we demonstrated efficacy ofRBC membrane-cloaked nanoparticles to bind and neutralize anti-RBCpolyclonal IgG effectively, and thus preserve circulating RBCs.
nanomedicine | immune therapy | type II hypersensitivity reaction |autoantibody
Type II immune hypersensitivities are driven by pathologicalantibodies targeting self-antigens, either naturally occurring
or due to exposure to an exogenous substance present on the cel-lular exterior or ECM. This disease type makes up many of the mostprevalent autoimmune diseases, including pernicious anemia, Gravedisease, and myasthenia gravis, as well as autoimmune hemolyticanemia (AIHA) and immune thrombocytopenia (1–4). In addition,these diseases may occur after the administration of a new drug orfollowing certain infections. Currently, therapies for these immune-mediated diseases remain relatively nonspecific via broad immunesuppression (5). For instance, comprehensive immune suppressionthrough systemic glucocorticoids (i.e., prednisone, methylpredniso-lone), cytotoxic drugs (i.e., cyclophosphamide, methotrexate, aza-thioprine), and monoclonal antibodies (i.e., rituximab, belimumab,infliximab) dominate treatment regimens to prevent further tissuedestruction (6–8). Although this approach to therapy is effective forsome patients in achieving remission, its efficacy remains variableand there is a well-established risk of adverse side effects, high-lighting the need for better tailored therapies (9, 10).The development of nanoparticle therapeutics has sparked
new hope for the treatment of various important human dis-eases. Herein, we demonstrate the application of a biomimeticnanoparticle for the clearance of pathological antibodies usingan established murine model of antibody-induced anemia (11).This disease may be idiopathic, as in AIHA, or drug induced, asin drug-induced anemia (DIA). In both cases, however, auto-antibodies attack surface antigens present on RBCs. Therapy forAIHA is relatively standardized, with patients starting on sys-temic steroids and escalating to cytotoxic drugs and B cell-depleting monoclonal antibodies, and then possibly splenectomybased on patient response to therapy (12, 13). The shortcomingof suppressing the immune system with drug-based therapiesis the considerable iatrogenic risk associated with nonspecifictherapy and heightened susceptibility to severe infections fol-lowing spleen removal (9, 10, 14). DIA, which can be the resultof drug-hapten antibodies or drug-independent autoantibodies,
is treated much the same way, with discontinuance of the offendingdrug and, much more often than in AIHA, performance of bloodtransfusions (15, 16). A subsequent limitation of repeated trans-fusions of packed RBCs is that although they revive tissue perfu-sion, they carry the risks of hemolytic transfusion reactions, theformation of alloantibodies, and iron toxicity (17–19).It has previously been shown that mammalian cellular mem-
brane, from both nucleated and nonnucleated cells, can be fusedonto polymeric nanoparticle substrates to form stable core/shellstructures (20, 21). These particles have been shown to retain andpresent natural cell membrane and surface antigens (22), whichbare the target epitopes involved in antibody-mediated cellularclearance found in AIHA and DIA. To demonstrate the in-terception of pathological antibodies, we used RBC membrane-cloaked nanoparticles, herein denoted RBC antibody nanosponge(s)(ANS), to serve as alternative targets for anti-RBC antibodiesand preserve circulating RBCs (Fig. 1). Unlike conventional im-mune therapy, these biomimetic nanoparticles have no drug pay-load to suppress normal lymphocytes or immune effector cells.Additionally, unlike blood transfusions, which serve as a replace-ment therapy, the RBC-ANS serves to deplete circulating anti-body levels, without contributing further toxic metabolites due tothe hemolysis of transfused cells. Moreover, it has been demon-strated in animal models of autoimmune diseases that the primarytarget antigens can vary and shift over the course of the diseases(23). Exploiting target cell membranes in their entirety over-comes the varying antigen specificities and presents a previouslyunidentified approach in intercepting the autoreactive antibodymechanism of type II immune hypersensitivity reactions.
Significance
The selective depletion of disease-causing antibodies usingnanoparticles offers a new model in the management of type IIimmune hypersensitivity reactions. The demonstration of patho-physiologically inspired nanoengineering serves as a valuableprototype for additional therapeutic improvements with the goalof minimizing therapy-related adverse effects. Through the useof cell membrane-cloaked nanoparticles, nanoscale decoys withstrong affinity to pathological antibodies can be administered todisrupt disease processes in a minimally toxic manner. Thesebiomimetic nanoparticles enable indiscriminate absorption ofpathological antibodies regardless of their epitope specificities.This particular approach offers much promise in treating anti-body-mediated autoimmune diseases, in which target antigenson susceptible cells can vary from patient to patient.
Author contributions: J.A.C., R.H.F., B.T.L., C.-M.J.H., and L.Z. designed research; J.A.C., R.H.F.,B.T.L., C.-M.J.H., and W.G. performed research; J.A.C., R.H.F., B.T.L., C.-M.J.H., W.G., K.Z., andL.Z. analyzed data; and J.A.C., R.H.F., B.T.L., C.-M.J.H., W.G., K.Z., and L.Z. wrote the paper.
The authors declare no conflict of interest.
This article is a PNAS Direct Submission.1To whom correspondence should be addressed. Email: [email protected].
www.pnas.org/cgi/doi/10.1073/pnas.1412420111 PNAS | September 16, 2014 | vol. 111 | no. 37 | 13481–13486
MED
ICALSC
IENCE
SEN
GINEE
RING

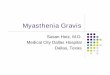
ResultsWe constructed RBC-ANS following a previously reportedprotocol (21), in which purified mouse RBC membrane wasmechanically extruded with 100 nm of poly(lactic-co-glycolic acid)(PLGA) polymeric cores. The resulting nanoparticles revealeda core/shell structure under transmission electron microscopy(TEM) that corresponds to unilamellar membrane coatings overthe nanoparticle cores (Fig. 2A). Physicochemical characterizationsshowed that upon RBC membrane coating, the nanoparticles hadan ∼20-nm increase in diameter and a 10-mV increase in surfacezeta-potential (Fig. 2B), which were consistent with the addition ofRBC membrane to the particle surface (24). A mixture of RBC-ANS with rabbit anti-mouse RBC IgG antibodies (anti-RBCs)resulted in a diameter increase of ∼26 nm, which can be attributedto the association of the IgG with the RBC-ANS. Such associationalso resulted in surface charge shielding, as was evidenced by the10-mV increase in the particle zeta-potential (Fig. 2B). To in-vestigate the binding capacity of RBC-ANS for anti-RBC better,250 μg of RBC-ANS was incubated with fluorescently labeled anti-RBCs ranging from 1.75 to 500 μg. This titration assay demon-strated a plateau in particle-bound antibody fluorescent signal, orbinding maximum, corresponding with an antibody mass of ∼27 μg,yielding a particle-to-antibody mass ratio of ∼9:1 (Fig. 2C). Toevaluate the specificity of antibody–antigen binding, RBC-ANSwas incubated with fluorescently labeled anti-RBCs or goat anti-mouse Fc IgG (anti-Fc, as a negative control) for 10 min at 37 °C.Fig. 2D shows that significantly higher binding signal was observedbetween RBC-ANS and anti-RBCs with very little nonspecificbinding with anti-Fc. PEGylated (PLGA) nanoparticle(s) (PEG-NP) incubated with anti-RBCs served as a negative control andshowed little retention of the antibody. Furthermore, binding af-finity of anti-RBCs to RBC-ANS was nearly identical to that of anequivalent amount of RBC ghosts (Fig. 2E). In the presence ofserum proteins, RBC-ANS still retained greater than 60% of itsanti-RBC binding capacity compared with when the incubation wasperformed in buffer alone (Fig. 2F). These results are indicative ofrelatively low nonspecific antibody–nanoparticle binding inter-actions and demonstrate the necessity for antigen–antibody con-cordance to achieve neutralization.To characterize the binding stability and competitive binding
capacity further, we varied the amounts of RBC-ANS mixed witha constant amount of fluorescent anti-RBCs in 5 vol% RBC solu-tion. To assess in vitro binding stability, RBC-ANS was pre-incubated with anti-RBCs before mixing with 5 vol% RBC solution(Fig. 3 A and B), and to test competitive binding capacity, RBC-
ANS was added simultaneously with anti-RBCs to 5 vol% RBCsolution (Fig. 3 C and D). After separating the RBCs from anyunbound antibodies and RBC-ANS, we measured fluorescent sig-nal associated with the RBCs using flow cytometric analysis.Both preincubation and coincubation studies showed dose-dependent antibody neutralization. High binding ability andstability of RBC-ANS to anti-RBCs was shown in the pre-incubation neutralization experiment, which demonstrated an∼60% reduction in RBC-bound antibodies with 100 μg of RBC-ANS and an ∼95% reduction with 1 mg of RBC-ANS comparedwith the negative control. Competitive coincubation showed
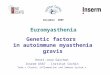
Fig. 1. Schematic representation of RBC-ANS neutralizing anti-RBC anti-bodies (anti-RBCs). (A) Anti-RBCs opsonize RBCs for extravascular hemolysis,via phagocytosis, as observed in AIHA and DIA. (B) RBC-ANS absorbs andneutralizes anti-RBCs, thereby protecting RBCs from phagocytosis.
Fig. 2. In vitro characterization of RBC-ANS. (A) TEM image demonstratesthe core/shell structure of RBC-ANS. (Scale bar: 150 nm.) (B) Size and surfacezeta-potential of pure PLGA cores, RBC-ANS, and RBC-ANS bound with anti-RBCs. (C) RBC-ANS (250 μg) incubated with five serial dilutions of fluorescentanti-RBCs demonstrated particle saturation at ∼27 μg of antibody, corre-sponding to a particle/antibody mass ratio of ∼9:1. (D) Equivalent amountsof RBC-ANS incubated with anti-RBCs or anti-Fc demonstrated significantlygreater specific binding compared with nonspecific binding. The corre-sponding PEG-NP incubated with anti-RBCs served as a negative control. (E)Comparison of anti-RBC binding kinetics with a fixed amount of RBC-ANS orRBC ghosts. (Inset) Relative binding capacity of RBC-ANS vs. RBC ghosts atsaturation. (F) Relative binding capacity of RBC-ANS in PBS vs. RBC-ANS inserum at saturation.
13482 | www.pnas.org/cgi/doi/10.1073/pnas.1412420111 Copp et al.

a reduction of RBC-bound antibody signal by ∼40% and ∼80% atequivalent RBC-ANS doses, respectively. To correlate dose de-pendence to relevant diagnostic parameters clinically, we com-pleted an Ig agglutination test, which is equivalent to the qualitativedirect antiglobulin test that is a gold standard laboratory diagnostictest often used in the diagnosis of AIHA (25, 26). By varying thedose of RBC-ANS from 0 to 250 μg, we demonstrated a dose-dependent neutralization of anti-RBCs (primary antibody) as evi-denced by the progressive decrease of RBC agglutination uponaddition of an agglutinating secondary antibody (Fig. 3 E–I).After confirming in vitro that RBC-ANS could selectively bind
anti-RBCs, we next assessed the ability of the particles to retainantibodies durably in vivo. A previously described anemia diseasemodel, induced through i.p. injection of anti-RBCs, was used inthe study (11). Five hundred micrograms of anti-RBCs, a suffi-cient amount to induce acute anemia, was injected i.p. into mice inthe control group. Following the injection, the antibodies coulddiffuse across the peritoneal membrane, bind to circulating RBCs,and induce their clearance. Mice in the treatment group receivedthe same dose of anti-RBCs incubated beforehand for 5 min at37 °C with 5 mg of RBC-ANS. The relevant clinical parametersused for monitoring anemia responses, including RBC count, he-moglobin level, and hematocrit, of each group were then assesseddaily for 4 d. Comparison of the hematological parameters
between the control and treatment groups showed that anti-RBCs preincubated with RBC-ANS was less effective in inducingan anemic response (Fig. 4). Mice in the treatment group pos-sessed a higher RBC count, hemoglobin content, and hemat-ocrit throughout the duration of the study. All parameters wereconsistent with control mice that had not been challenged withanti-RBCs but had their blood drawn daily. This result suggeststhat the anti-RBCs were trapped by the RBC-ANS and wereprecluded from binding to circulating RBCs. The experimentdemonstrates the feasibility of using target cell-mimickingnanoparticles to neutralize pathological antibodies.To validate the clinical relevance of the RBC-ANS further, we
administered daily injections of low-dose anti-RBCs i.p. to main-tain a sustained level of the antibodies for anemia progression.RBC-ANS was injected i.v. with the aim of neutralizing the cir-culating antibodies and retarding anemia development. PEG-NPof analogous size was also administered as a control. Mice weredivided into RBC-ANS plus anti-RBC, PEG-NP plus anti-RBC,and PBS plus anti-RBC groups. All mice received 200 μg of anti-RBCs daily through i.p. injection, followed by i.v. injection of 2 mgof either RBC-ANS, PEG-NP, or PBS daily for 4 d. Blood wasobtained daily for the duration of the experiment to assess RBCcount, hemoglobin level, and hematocrit. Starting from day 2, sig-nificant benefit in anemia-related parameters was observed in the
Fig. 3. In vitro dose-dependent neutralization and stability of RBC-ANS/anti-RBC binding. (A) Flow cytometry histograms of RBC-ANS (from left to right:1,000 μg, 500 μg, 250 μg, 100 μg, 50 μg, and 0 μg) preincubated with 50 μg of FITC–anti-RBCs before mixing with 5 vol% RBC solution demonstrated dose-dependent neutralization of anti-RBCs. (B) Mean fluorescence intensity of samples in A. (C ) Flow cytometry histograms of RBC-ANS (from left to right:1,000 μg, 500 μg, 250 μg, 100 μg, 50 μg, and 0 μg) coincubated with 50 μg of FITC–anti-RBCs and 5 vol% RBC solution demonstrated dose-dependent,competitive neutralization of anti-RBCs. (D) Mean fluorescence intensity of samples in C. (E–I) Varying amounts of RBC-ANS (from E to I: 0 μg, 25 μg, 50 μg,100 μg, and250 μg) were coincubated with 15.6 μg of anti-RBCs (primary antibody) and 5 vol% RBC solution, followed by adding an equivalent dose of anti-Fc(agglutinating secondary antibody). The samples were then imaged by light microscopy at 10× magnification, demonstrating dose-related inhibition of RBCagglutination by RBC-ANS. (Scale bar: 100 μm.)
Fig. 4. In vivo binding stability of RBC-ANS and anti-RBCs. Mice (n = 6) were i.p. injected with 500 μg of anti-RBCs preincubated with 5 mg of RBC-ANS (red),500 μg of anti-RBCs alone (blue), or PBS (black). Blood was collected daily to monitor RBC count (A, million cells per microliter), hemoglobin level (B, gramsper deciliter), and hematocrit (C, %) of the mice.
Copp et al. PNAS | September 16, 2014 | vol. 111 | no. 37 | 13483
MED
ICALSC
IENCE
SEN
GINEE
RING

RBC-ANS–treated group compared with PEG-NP control miceand vehicle-only mice (Fig. 5). The inability of PEG-NP to preventanemia further supports the antigen-specific clearance of anti-RBCsmediated by RBC-ANS as opposed to the preservation of RBCs viasaturation of the mononuclear phagocyte system (27, 28). To helpassess the safety of the RBC-ANS approach, we also examined theautologous anti-RBC serum titers in mice 6 wk following RBC-ANStreatment. ELISA assessment of autoantibodies against mouseRBCs showed no observable elevation of autologous anti-RBCresponses in mice receiving RBC-ANS treatment compared withthe controls. The result confirms that the RBC-ANS/anti-RBCcomplex does not potentiate a humoral immune response againstparticle-associated membrane antigens (Fig. 6).
DiscussionAutoimmune diseases, which include type II, type III, and typeIV immune hypersensitivity reactions, are known to attack al-most every body tissue, make up over 50 diseases, and contributeto over $65 billion in health care costs annually (29). AIHA wasattributed to an autoantibody in 1904 by Donath and Land-steiner, and the mechanism of extravascular hemolysis was de-scribed by Metchinkoff in 1905, making it the first disease knownto be caused by this mechanism (30). Although the etiology isoften idiopathic, it can be induced by drugs (cephalosporins,chemotherapies, and quinines), as well as by malignancies andviral infections (25, 26, 30). Despite the differences in etiology,the final common disease pathway is the generation of antibodiesagainst RBC membrane components, typically rhesus group andglycophorins, by a B-lymphocyte population that has lost self-tolerance to RBC surface antigen(s) (31). Most commonly, thepathological mechanism is IgG-mediated attack that leads to theopsonization of RBCs for extravascular destruction by phagocytes.Alternatively, AIHA can also be induced by IgM-mediatedattack on RBCs, which causes RBC intravascular hemolysis viaactivation of the complement system (26, 30, 32, 33). Eventhough autoantibodies have long been recognized to play a sig-nificant role in the disease, to our knowledge, therapies specifi-cally directed at these pathological antibodies were not pre-viously explored. Existing AIHA therapy continues to targetupstream disease mechanisms through reliance on broad im-mune suppression, blood transfusions, or splenectomy for re-fractory cases (12, 15). This treatment paradigm holds true forother type II immune hypersensitivities, which are also man-aged with broad immune suppression, such as using systemicglucocorticoids or cytotoxic drugs (3, 34).Although efficacious for many patients, systemic steroids carry
some of the highest risks of iatrogenic illness. Adverse effects oftherapy include steroid myopathy, nosocomial infection, asepticbone necrosis, accelerated osteoporosis, weight gain, metabolicderangements, and Cushingoid appearance (35, 36). In additionto these side effects, if steroid therapy fails, a patient may need toundergo surgery or systemic B-cell depletion with monoclonal
antibodies or cytotoxic drugs, with side effects of severe infection,antibody transfusion reactions, and even the development ofmalignancies (10, 37). Given this landscape, it is meaningful tocontinue development of innovative therapeutic strategies tomanage disease burden while minimizing iatrogenic risk. Nano-particles have already shown promise in reducing the risk of sys-temic toxicity of chemotherapy while increasing efficacy both inemerging literature and clinically (38–40). We demonstrated thatnanoparticles can be engineered to intercept binding betweenpathological antibodies and their target cells to have a favorableimpact on disease status. This particular approach offers a uniquetherapeutic intervention for type II immune hypersensitivityreactions by targeting a final pathological mechanism and presentsan attractive alternative to broad-spectrum immune suppression.Through the stabilization of biological membrane on a poly-
meric nanoparticle substrate, we unveiled the ability of cellmembrane-coated nanoparticles to serve as an antibody decoy toimprove disease parameters. Our results indicate the ability ofRBC-ANS to bind to anti-RBCs effectively and preclude its in-teraction with RBCs. The therapeutic potential of the proposedapproach was validated in vivo with separate administration ofanti-RBCs and RBC-ANS via i.p. and i.v. routes, respectively.Although the RBC-ANS reduced the antibody-mediated anemicresponse, equivalent doses of PEG-NP of analogous physico-chemical properties failed to moderate the effect of the anti-RBCs. The outcome of the in vivo study further indicates that theimproved hematological status upon RBC-ANS treatment wasmediated by specific antibody–antigen interaction, rather thanparticle-mediated saturation of phagocytic cells (27, 28). We alsoestablished a lack of humoral response against the RBC mem-brane antigens following administration of RBC-ANS and anti-RBCs, which validates the safety of the approach, because theRBC-ANS, in the presence of anti-RBCs, did not potentiate anRBC autoantibody immune response. It has been previouslyreported that RBC membrane-coated nanoparticles are primarilymetabolized in the liver (21, 41), where particulate metabolismgenerally promotes a tolerogenic immune response (42, 43). Inaddition, several reports have shown that antigen-laden polymericnanoparticles, in the absence of immune adjuvants, are immune-tolerizing (44–46). Although rigorous immunological studies inmore faithful AIHA animal models are warranted, the presentstudy exhibits the feasibility of applying cell membrane-coatednanoparticles for clearing pathological antibodies. Adding prom-ise to the approach is the demonstration of both nucleated andnonnucleated mammalian cell membranes that have been suc-cessfully stabilized by nanoparticle cores (20, 21). This capacity tofunctionalize particles, with a variety of multiantigen membranes,offers a platform for the development of a robust line of therapiesagainst additional type II immune hypersensitivities.Currently, the paradigm in targeted nanomedicine revolves
around high-throughput screening for ligand-receptor recognitionand the subsequent nanoparticle functionalization with specific
Fig. 5. In vivo neutralization of anti-RBCs by RBC-ANS. Mice (n = 10) were i.p. injected with 200 μg of anti-RBCs on days 0, 1, 2, and 3. After each dose of theantibody, the mice received 2 mg of RBC-ANS (red), PEG-NP (black), or PBS (blue) via tail vein i.v. injection. Blood was collected daily to monitor RBC count(A, million cells per microliter), hemoglobin level (B, grams per deciliter), and hematocrit (C, %) of the mice.
13484 | www.pnas.org/cgi/doi/10.1073/pnas.1412420111 Copp et al.

targeting molecules (47, 48). With regard to type II immune hy-persensitivity reactions, such a functionalization process could provelimited owing to the varying antigen specificities among pathologicalantibodies from patient to patient, such as in the case of AIHA (11,23, 45). Through the appropriate application of biological mem-branes, which possess the diversity of surface antigens susceptible topathological antibodies, biomimetic nanoparticles can be preparedin a facile manner for selective immunomodulation. Furthermore,drug-loaded cores or those made from different materials, such asmetallic or inorganic nanoparticles, can be used to create multi-functional formulations. We believe the demonstration of patho-physiologically inspired nanoengineering serves as a valuableprototype for additional therapeutic advances, offering the oppor-tunity for selective disease intervention while minimizing iatrogenicrisks associated with many traditional drug-based therapies.
Materials and MethodsPreparation of RBC-ANS. RBC-ANSwas prepared following previously describedmethods (21). Briefly, ∼100-nm PLGA polymeric cores were prepared using0.67 dL/g of carboxy-terminated 50:50 poly(DL-lactide-co-glycolide) (LACTELAbsorbable Polymers) in a nanoprecipitation process. The PLGA polymer wasfirst dissolved in acetone at a concentration of 10 mg/mL. One milliliter of thesolution was then added rapidly to 3 mL of water. For fluorescently labeledformulations, 1,1′-dioctadecyl-3,3,3′,3′-tetramethylindodicarbocyanine per-chlorate (DiD; excitation/emission = 644/665 nm; Life Technologies) was loadedinto the polymeric cores at 0.1 wt%. The mixture was then stirred in open airfor 1 h and placed in a vacuum for another 3 h. The resulting nanoparticlesolution was filtered using Amicon Ultra-4 Centrifugal Filters with a molecularmass cutoff of 10 kDa (Millipore). RBC membrane coating was then completedby fusing RBC membrane vesicles with PLGA particles via sonication using anFS30D bath sonicator at a frequency of 42 kHz and a power of 100 W for2 min. The size and the zeta-potential of the resulting RBC-ANS were obtainedfrom three dynamic light scattering measurements using a Malvern ZEN 3600Zetasizer, which showed an average hydrodynamic diameter of ∼100 nm and∼115 nm before and after the membrane coating process, respectively. Thestructure of RBC-ANS was examinedwith TEM. A drop of the RBC-ANS solutionat 100 μg/mL was deposited onto a glow-discharged, carbon-coated grid for10 s and then rinsed with 10 drops of distilled water. A drop of 1 wt% uranylacetate stain was added to the grid. The sample was then imaged using an FEI200 kV Sphera microscope. PEG-NP was prepared using poly(ethylene glycol)methyl ether-block-poly(lactide-co-glycolide) (PEG-PLGA; Sigma–Aldrich). ThePEG-PLGA polymer was dissolved in acetone at 10 mg/mL, and 1 mL of solutionwas added to 3 mL of water. For fluorescently labeled formulations, DiD wasloaded into the polymeric cores at 0.1 wt%. The mixture was then stirred inopen air for 1 h and subsequently placed in a vacuum for another 3 h.
RBC-ANS Binding Capacity and Specificity Studies. Antibodies were first la-beled with FITC. Specifically, 100 μL of polyclonal rabbit anti-mouse RBC IgG
(anti-RBCs; Rockland Antibodies and Assays) at 10 mg/mL was mixed with3.0 μL of 10 mg/mL FITC (Thermo Scientific) in DMSO. The mixture was in-cubated at room temperature in the dark for 1 h and then run througha Sephadex G-25 column (Sigma–Aldrich) with deionized water to purifyconjugated FITC–anti-RBCs for subsequent experiments. For the antibodyretention study, 250 μg of DiD-loaded RBC-ANS was combined with six serialdilutions (500 μg, 250 μg, 125 μg, 31.25 μg, 7.81 μg, and 1.95 μg) of FITC-labeled antibody in triplicate in a Costar 96-well plate (Corning Unlimited).Before incubation, the samples’ fluorescence intensities were measured us-ing a Tecan Infinite M200 reader (TeCan) to determine 100% signal of FITC(515 nm) and DiD (670 nm). Solutions were then incubated for 30 min at37 °C, followed by spinning down in a Legend 21R Microcentrifuge (ThermoScientific) at 21,200 × g for 5 min to collect pelleted RBC-ANS/anti-RBCcomplex. Samples were then washed three times in 1 mL of water, and theirfluorescence intensity was remeasured to determine the signal intensity ofFITC in relation to DiD. All DiD signals were greater than 90% of the originalsignal, ensuring minimal loss during washing steps. These steps were re-peated at optimum concentrations of 250 μg of DiD-loaded RBC-ANS or250 μg of DiD-loaded PEG-NP, combined with 7.8 μg of FITC–anti-RBC and7.8 μg of FITC-conjugated anti-Fc (Rockland Antibodies and Assays) to de-termine the specificity of RBC-ANS against anti-RBCs compared with controlsamples. To compare binding kinetics, serially diluted concentrations ofFITC–anti-RBCs (1, 0.5, 0.25, 0.125, 0.063, and 0.031 mg/mL) were incubatedwith a constant substrate concentration (0.25 mg/mL RBC-ANS or an equiv-alent amount of RBC ghosts). Final values were normalized to the maximumbinding observed at saturation. Binding capacity was expressed as a ratio ofthe fluorescent signals at saturation. To test binding capacity in serum, RBC-ANS was incubated with a saturated amount of FITC–anti-RBCs in PBS or inthe presence of 50 vol% FBS (Thermo Scientific). Values were expressed asa ratio of the fluorescent signals.
Competitive Binding Studies. RBC-ANS was prepared at 1 mg/mL in 1× Dulbecco’sPBS (Gibco) and serially diluted to make five solutions (1 mg/mL, 500 μg/mL,250 μg/mL, 100 μg/mL, and 50 μg/mL) with 1× PBS as a control. For thepreincubation study, these solutions were combined with 50 μg of anti-RBCsand incubated for 2 min at 37 °C before the addition of 1 mL of washed 5 vol%mouse RBC solution. For the competitive coincubation study, RBC-ANS andanti-RBCs were added simultaneously to 1 mL of 5 vol% RBC solution. Eachexperiment was done in triplicate. Samples were allowed to incubate for10 min at 37 °C and then washed three times in 1× PBS to remove supernatantthoroughly and collect RBC pellets. Flow cytometry was used to measure theFITC signal of the collected RBC population using a Becton Dickinson FACSCantoII. Flow cytometry data were analyzed using FlowJo software from Treestar.
RBC Agglutination Titration. The experiment was carried out per the manu-facturer’s instructions (Rockport Antibodies and Assays). Briefly, 100 μL ofanti-RBCs (primary antibody) at 156 μg/mL was added to 100 μL of 5 vol%washed RBCs in 1× PBS, along with 62.5 μL of RBC-ANS (250 μg, 100 μg,50 μg, 25 μg, or 0 μg) and incubated for 45 min at 37 °C. The RBC solutionwas then washed three times by centrifuging the sample at 3,500 × g for1 min and exchanging the supernatant with 1× PBS each time. One hundredmicroliters of anti-Fc (agglutinating secondary antibody) at 156 μg/mL wasadded to each sample, which was then placed in an analog vortex mixer(Fisher Scientific) at 625 rpm for 5 min and then spun down at 3,500 × g for20 s. The sample was then resuspended using a pipette to disrupt the pellet.For the negative control, 100 μL of 6% (wt/vol) BSA was used in lieu ofsecondary antibody. All samples were then viewed via a light microscope at10× magnification and imaged via mounted camera.
In Vivo Stability of RBC-ANS and Anti-RBC Binding. Following induction ofanemia via i.p. injection of anti-RBCs, we randomly assorted 12 CD-1 mice(Charles River Laboratories) into two groups of six. The treatment groupreceived 500 μg of anti-RBCs incubated with 5 mg of RBC-ANS for 5 min at37 °C before injection, and anti-RBC only mice received anti-RBCs incubatedin 1× PBS for 5 min. A control group of mice received injections of PBS only.A few drops of blood were collected from each mouse before injections onday 0 to establish starting blood counts, and this procedure was repeated oneach day of the experiment. Samples were stored in potassium-EDTAMicrovette tubes (Sarstedt) and vigorously mixed to prevent clotting. Sam-ples were then run on the same day using a Drew Scientific Hemavet 950(Erba Diagnostics), and RBC count, hemoglobin level, and hematocrit wererecorded daily.
In Vivo Neutralization of Circulating Anti-RBCs by RBC-ANS. Using the esta-blished i.p. model for antibody delivery, 30 mice were randomized to three
Fig. 6. RBC-ANS does not elicit autoimmune antibodies against RBCs. Sixweeks following administration, ELISA analysis of serum from mice receivingRBC-ANS plus anti-RBCs, anti-RBCs alone, or PBS (Blank) showed no observ-able elevation of anti-RBC titer compared with the positive control.
Copp et al. PNAS | September 16, 2014 | vol. 111 | no. 37 | 13485
MED
ICALSC
IENCE
SEN
GINEE
RING

groups of 10 mice. Each group of mice received a 100-μL i.p. injection of2 mg/mL anti-RBCs on days 0, 1, 2, and 3. The treatment group also receiveda tail vein i.v. injection of 200 μL of RBC-ANS (10 mg/mL) in 1× PBS within30 min of i.p. antibody delivery. The PEG-NP group received an equivalenti.v. dose of PEG-NP, and the anti-RBC only group received 200 μL PBS via i.v.injection. The RBC count, hemoglobin level, and hematocrit of each samplewere recorded on days 0, 1, 2, 3, and 4.
Anti-RBC Autoimmune Study. Six weeks after the in vivo neutralization studies,serumwas collected from 12mice (six in each group) and a standard ELISAwasperformed. Washed CD-1 mouse RBCs were plated at 1 × 106 RBCs per wellonto a Costar 96 well plate. One hundred microliters of collected serum was
added in a sequence of six 1:5 dilutions. HRP-conjugated goat anti-mouseantibody IgG (Biolegend) was used to probe for bound antibodies. The platewas developed using 3,3′,5,5′-tetramethylbenzidine substrate, and 1 M HClwas used to stop the reaction. Absorbance was measured at 450 nm.
ACKNOWLEDGMENTS. This work is supported by the National Institute ofDiabetes and Digestive and Kidney Diseases of the National Institutes ofHealth (NIH) under Award R01DK095168. J.A.C. is supported by a HowardHughes Medical Institute Medical Research Fellowship. R.H.F. is supported bythe Department of Defense through the National Defense Science andEngineering Graduate Fellowship Program. B.T.L. is supported by NIH TrainingGrant R25CA153915 from the National Cancer Institute.
1. Jacobson DL, Gange SJ, Rose NR, Graham NMH (1997) Epidemiology and estimatedpopulation burden of selected autoimmune diseases in the United States. Clin Im-munol Immunopathol 84(3):223–243.
2. Wakayama H, et al. (2000) Abolition of anti-glomerular basement membrane anti-body-mediated glomerulonephritis in FcRgamma-deficient mice. Eur J Immunol 30(4):1182–1190.
3. Hudson BG, Tryggvason K, Sundaramoorthy M, Neilson EG (2003) Alport’s syndrome,Goodpasture’s syndrome, and type IV collagen. N Engl J Med 348(25):2543–2556.
4. Weetman AP (2000) Graves’ disease. N Engl J Med 343(17):1236–1248.5. Edwards JCW, Cambridge G (2006) B-cell targeting in rheumatoid arthritis and other
autoimmune diseases. Nat Rev Immunol 6(5):394–403.6. Wallace DJ, et al. (2009) A phase II, randomized, double-blind, placebo-controlled,
dose-ranging study of belimumab in patients with active systemic lupus eryth-ematosus. Arthritis Rheum 61(9):1168–1178.
7. Worlledge SMBM, Brain MC, Cooper AC, Hobbs JR, Dacie JV (1968) Immmunosuppressivedrugs in the treatment of autoimmune haemolytic anaemia. Proc R Soc Med 61(12):1312–1315.
8. Emilia G, Messora C, Longo G, Bertesi M (1996) Long-term salvage treatment by cy-closporin in refractory autoimmune haematological disorders. Br J Haematol 93(2):341–344.
9. Tabas I, Glass CK (2013) Anti-inflammatory therapy in chronic disease: Challenges andopportunities. Science 339(6116):166–172.
10. Hansel TT, Kropshofer H, Singer T, Mitchell JA, George AJT (2010) The safety and sideeffects of monoclonal antibodies. Nat Rev Drug Discov 9(4):325–338.
11. Meyer D, et al. (1998) FcgammaRIII (CD16)-deficient mice show IgG isotype-dependentprotection to experimental autoimmune hemolytic anemia. Blood 92(11):3997–4002.
12. Lechner K, Jäger U (2010) How I treat autoimmune hemolytic anemias in adults. Blood116(11):1831–1838.
13. Arnold DM, et al. (2012) A pilot randomized trial of adjuvant rituximab or placebo fornonsplenectomized patients with immune thrombocytopenia. Blood 119(6):1356–1362.
14. Kyaw MH, et al. (2006) Evaluation of severe infection and survival after splenectomy.Am J Med 119(3):276.e1–276.e7.
15. Crowther M, et al. (2011) Evidence-based focused review of the treatment of idio-pathic warm immune hemolytic anemia in adults. Blood 118(15):4036–4040.
16. Petz LD (2004) A physician’s guide to transfusion in autoimmune haemolytic anaemia.Br J Haematol 124(6):712–716.
17. Salama A, Berghöfer H, Mueller-Eckhardt C (1992) Red blood cell transfusion in warm-type autoimmune haemolytic anaemia. Lancet 340(8834-8835):1515–1517.
18. Ahrens N, Pruss A, Kähne A, Kiesewetter H, Salama A (2007) Coexistence of auto-antibodies and alloantibodies to red blood cells due to blood transfusion. Transfusion47(5):813–816.
19. Shander A, Cappellini MD, Goodnough LT (2009) Iron overload and toxicity: Thehidden risk of multiple blood transfusions. Vox Sang 97(3):185–197.
20. Fang RH, et al. (2014) Cancer cell membrane-coated nanoparticles for anticancervaccination and drug delivery. Nano Lett 14(4):2181–2188.
21. Hu CMJ, et al. (2011) Erythrocyte membrane-camouflaged polymeric nanoparticles asa biomimetic delivery platform. Proc Natl Acad Sci USA 108(27):10980–10985.
22. Hu CMJ, et al. (2013) ‘Marker-of-self’ functionalization of nanoscale particles througha top-down cellular membrane coating approach. Nanoscale 5(7):2664–2668.
23. Hall AM, et al. (2007) Deletion of the dominant autoantigen in NZB mice with au-toimmune hemolytic anemia: Effects on autoantibody and T-helper responses. Blood110(13):4511–4517.
24. Hochmuth RM, Evans CA, Wiles HC, McCown JT (1983) Mechanical measurement ofred cell membrane thickness. Science 220(4592):101–102.
25. Bass GF, Tuscano ET, Tuscano JM (2014) Diagnosis and classification of autoimmunehemolytic anemia. Autoimmun Rev 13(4-5):560–564.
26. Packman CH (2008) Hemolytic anemia due to warm autoantibodies. Blood Rev 22(1):17–31.
27. Crow AR, Song S, Semple JW, Freedman J, Lazarus AH (2001) IVIg inhibits re-ticuloendothelial system function and ameliorates murine passive-immune throm-bocytopenia independent of anti-idiotype reactivity. Br J Haematol 115(3):679–686.
28. Samuelsson A, Towers TL, Ravetch JV (2001) Anti-inflammatory activity of IVIG me-diated through the inhibitory Fc receptor. Science 291(5503):484–486.
29. Persidis A (1999) Autoimmune disease drug discovery. Nat Biotechnol 17(10):1038–1039.30. Mack P, Freedman J (2000) Autoimmune hemolytic anemia: A history. Transfus Med
Rev 14(3):223–233.31. Leddy JP, et al. (1994) Erythrocyte membrane proteins reactive with IgG (warm-
reacting) anti-red blood cell autoantibodies: II. Antibodies coprecipitating band 3and glycophorin A. Blood 84(2):650–656.
32. König AL, Kather H, Roelcke D (1984) Autoimmune hemolytic anemia by coexistinganti-I and anti-Fl cold agglutinins. Blut 49(5):363–368.
33. Semple JW, Freedman J (2005) Autoimmune pathogenesis and autoimmune hemo-lytic anemia. Semin Hematol 42(3):122–130.
34. Daniel BS, Borradori L, Hall RP, 3rd, Murrell DF (2011) Evidence-based management ofbullous pemphigoid. Dermatol Clin 29(4):613–620.
35. Buttgereit F, Burmester GR, Straub RH, Seibel MJ, Zhou H (2011) Exogenous andendogenous glucocorticoids in rheumatic diseases. Arthritis Rheum 63(1):1–9.
36. Saag KG, Caldwell JR, Brasington R, Furst DE (1995) Serious adverse events with low-dose, long-term corticosteroid-therapy in rheumatoid-arthritis—Reply. Am J Med99(6):693–694.
37. Lenz HJ (2007) Management and preparedness for infusion and hypersensitivity re-actions. Oncologist 12(5):601–609.
38. Karve S, et al. (2012) Revival of the abandoned therapeutic wortmannin by nano-particle drug delivery. Proc Natl Acad Sci USA 109(21):8230–8235.
39. Green MR, et al. (2006) Abraxane, a novel Cremophor-free, albumin-bound particleform of paclitaxel for the treatment of advanced non-small-cell lung cancer. AnnOncol 17(8):1263–1268.
40. O’Byrne KJ, et al. (2002) A phase I dose-escalating study of DaunoXome, liposomaldaunorubicin, in metastatic breast cancer. Br J Cancer 87(1):15–20.
41. Hu CMJ, Fang RH, Copp J, Luk BT, Zhang L (2013) A biomimetic nanosponge thatabsorbs pore-forming toxins. Nat Nanotechnol 8(5):336–340.
42. Crispe IN (2003) Hepatic T cells and liver tolerance. Nat Rev Immunol 3(1):51–62.43. Klugewitz K, et al. (2002) Immunomodulatory effects of the liver: Deletion of acti-
vated CD4+ effector cells and suppression of IFN-gamma-producing cells after in-travenous protein immunization. J Immunol 169(5):2407–2413.
44. Basarkar A, Singh J (2009) Poly (lactide-co-glycolide)-polymethacrylate nanoparticlesfor intramuscular delivery of plasmid encoding interleukin-10 to prevent auto-immune diabetes in mice. Pharm Res 26(1):72–81.
45. Getts DR, et al. (2012) Microparticles bearing encephalitogenic peptides induce T-celltolerance and ameliorate experimental autoimmune encephalomyelitis. Nat Bio-technol 30(12):1217–1224.
46. Kim WU, et al. (2002) Suppression of collagen-induced arthritis by single adminis-tration of poly(lactic-co-glycolic acid) nanoparticles entrapping type II collagen:A novel treatment strategy for induction of oral tolerance. Arthritis Rheum 46(4):1109–1120.
47. Fang RH, et al. (2013) Lipid-insertion enables targeting functionalization of erythro-cyte membrane-cloaked nanoparticles. Nanoscale 5(19):8884–8888.
48. Hu CMJ, Fang RH, Luk BT, Zhang L (2014) Polymeric nanotherapeutics: Clinical de-velopment and advances in stealth functionalization strategies. Nanoscale 6(1):65–75.
13486 | www.pnas.org/cgi/doi/10.1073/pnas.1412420111 Copp et al.