Embed Size (px)
Citation preview

[CANCER RESEARCH 41, 4781-4785, November 1981]0008-5472/81 /0041-OOOOS02.00
Classification of Human Leukemia by Membrane Antigen Analysis withXenoantisera1
Richard S. Metzgar,2 Barry L. Dowell,3 Lawrence B. Lachman, Nancy H. Jones, and Frederick W. George, IV
Department of Microbiology and Immunology, Duke University Medical Center, Durham, North Carolina 27710 [R. S. M., B. L. D., L. B. L., N. H. J., F. W. G.], andYerkes Primate Research Center, Emory University, Atlanta, Georgia 30322 [R. S. M.]
Abstract
Rabbit and monkey antisera after appropriate absorptionwere rendered specific for normal or leukemic lymphoid- andmyeloid-associated antigens. Antisera defining a common peripheral blood T-cell antigen, a thymus leukemia antigen, HLA-DR or la-like antigen, common acute lymphoblastic leukemiaantigen (CALLA), and a myeloid-monocyte (M) antigen wereused in a microcytotoxicity assay to classify leukemic cellsfrom 30 patients in a double blind study. The antisera to the Mantigen reacted with adherent peripheral blood cells and poly-
morphonuclear leukocytes and failed to react with nonadherentmononuclear cells and enriched T-cells and chronic lyrrtpho-
cytic leukemia cells. The M antisera also reacted with U937, amonocytic-type cell line, and with HL60, a promyelocytic-type
cell line, but failed to react with T and B lymphoblastoid celllines. The specificities of the other antisera have been described in previous reports.
Cells from three of the patients could not be phenotyped bymicrocytotoxicity testing. Cells from 25 patients had a consensus morphological or histochemical diagnosis of either acutelymphoblastic leukemia or acute nonlymphocytic leukemia. Theserological classification of these patients using the five typesof antisera listed above were consistent with the consensusdiagnosis. In addition, the lymphoid cancers were further sub-classified as to T-, B-, or thymus antigen types. There was noconsensus lymphoid versus myeloid diagnosis on cells fromtwo patients. The serological classification in both cases favored a diagnosis of myeloid rather than lymphoid leukemia.
Introduction
Xenoantisera are now widely used for the detection andclassification of types and subtypes of acute and chronicleukemia in humans (see reviews in Refs. 10 and 16). Some ofthe markers such as the CALLA4 initially described and char
acterized by Greaves ef al. (11) are leukemia associated; i.e..
' Presented at the Conference on Cell Markers in Acute Leukemia, March 4
and 5, 1980, Bethesda, Md. Supported by USPHS Grants CA 15525, CA 08975,and CA 11265 from the National Cancer Institute and Grant AM 08054 from theNational Institute of Arthritis, Metabolism, and Digestive Diseases to Duke University. Production of primate antisera was partially supported by Grant FR00165 from the Division of Research Resources to Yerkes Primate ResearchCenter.
2 To whom requests for reprints should be addressed, at Department of
Microbiology and Immunology, Duke University Medical Center, Durham, N.C. 27710.
3 Special Fellow of the Leukemia Society of America.4 The abbreviations used are: CALLA, common acute leukemia-associated
antigens; THY, thymus leukemia antigen; AMOL, acute monocytic leukemia; RIP-PAGE, radioimmunoprecipitation combined with sodium dodecyl sulfate-poly-acrylamide gel electrophoresis; ALL, acute lymphoblastic leukemia; CLL, chroniclympnocytic leukemia; PMN, polymorphonuclear leukocytes; AMML. acute mye-lomonocytic leukemia; T-ALL, thymus-derived acute lymphoblastic leukemia; E-rosette, erythrocyte-forming rosette.
the antigen is present on most leukemic cells of a given type orsubtype and either absent or found only on a small percentageof normal cell types. However, most of the antisera defineantigen(s) found on populations or subpopulations of normalcells as well as on leukemic cells. Examples of the latter typeantigens, described in previous reports from our laboratory,are the human la-like antigen (1), TLAA (1, 2), and THY (5,
18). This report is a summary of recent serological studies fromour laboratory utilizing antisera to CALLA and normal lymphoid-and myeloid-specific antigens for the classification of leukemia
by microcytotoxicity.
Materials and Methods
Antisera. The monkey and rabbit antisera used in these studies,their distribution on normal cells, and references detailing their specificity are given in Table 1. Both monkey and rabbit antisera to MSB andSB cells were appropriately absorbed to detect TLAA and la-like
antigens and have been well characterized in previous publicationsfrom this laboratory (1-4). The antisera to TLAA precipitate a M.W.
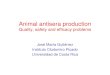
170,000 glycoprotein, while the la antisera precipitate the M.W.30,000 and 35,000 polypeptides associated with these antigens (Fig.1). The monkey and rabbit antisera to these 2 antigens precipitate thesame antigens and give similar (±20%) microcytotoxicity reactions sothat only a range of lysis is given which is representative of bothspecies of antisera. Some of the absorbed antisera (e.g., aTLAA and«-lain Fig. 1) occasionally showed additional bands with some of the
labeled antigens tested. Some of these bands were noted with thenormal serum or Staphylococcus protein A controls, while othersrepresent antigens bound by antibodies not related to the antigenicspecificity defined by cytotoxicity.
The THY antisera were produced in monkeys by immunization withhuman thymocytes and were absorbed with erythrocytes and peripheralblood leukocytes until they no longer reacted with enriched peripheralblood T- or B-lymphocytes from normal donors but still react strongly
wtih thymocytes and certain leukemic cells (5, 18). Two antisera werestudied; one was elicited to thymocytes from a single donor and theother was elicited with thymocytes from pooled donors. Essentiallysimilar percentages of cells were lysed by both antisera (±20%), sothat a range of values is given representative of both thymocyteantisera. The THY antisera precipitate 45,000 M.W. to 48,000 M.W.antigen by RIP-PAGE (Fig. 1; Ref. 5).
The rabbit antisera to CALLA have not been reported in previouspublications from this laboratory but have the same serological specificity and precipitate an antigen in the same 95,000 to 100,000molecular-weight range (Fig. 1) as that described by Greaves ef a/.(10-13). The CALLA antisera were elicited to uncultured non-T, non-B
ALL cells and were absorbed with peripheral blood leukocytes fromnormal donors and with CLL cells until they no longer reacted withenriched T- and B-cells from normal donors.
Rabbit antisera detecting myeloid-monocyte-associated antigen (M)
were elicited to cells from a patient with AMOL and to adherentperipheral blood cells from a normal donor.5 The antisera were ab-
' Unpublished data.
NOVEMBER 1981 4781
on April 7, 2019. © 1981 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

fi. S. Metzgar et al.
Table 1Characteristics of human antigens defined by xenoantisera
AntigenTLAATHYla-HLA-DRwCALLAMMolecularproper
tiesM.W.
170,000gpaM.W.
45,000-48,000M.W.
30,000and35,000gpM.W.
95,000to100,000gpNot
knownDistribution
on normalcellsThymocytes,
peripheralbloodT-lymphocytesThymocytesB-Lymphocytes,
CFU-C, 1-8%ofnormalT-lymphocytes,monocytes,
somemyeloblastsSomeantisera reported to de
tect occasional cell innormalandregeneratingmarrowGranulocytes,
monocytesSpecificity
references3,
5, 8,96,
73,8,92,
4, 10,111
2 (andseeCharts1and2)Species
ofantiseraRabbit
andmonkeyMonkeyRabbit
andmonkeyRabbitRabbit
" QP,glycoprotein; CFU-C, myeloid cell colony-forming units; M, myeloid-monocyte antigen.
sorbed with B- and T-lymphoblastoid cell lines until they no longer
reacted by microcytotoxicity with these cell lines or with enrichedperipheral blood B- or T-lymphocytes. Additional data on the specificity
of these 2 M antisera are given in the text. Both antisera had essentiallythe same titer, and the percentage of target cells lysed was ±10%.Therefore, data from both antisera are referred to collectively as a-M.
Cells. The frozen cells were obtained from Dr. David Gordon, Centerfor Disease Control, Atlanta, Ga., and many were obtained from patientsin the Southeastern Cancer Study Group. The samples were tested bymicrocytotoxicity by us without prior knowledge of the diagnosis. Thediagnosis of leukemia or lymphoma on these cells was made by aconsensus of opinions based on morphology, cytogenetics, histochem-
istry, enzymatic analysis, and certain surface marker characteristics.The properties of the cells from some of these patients have beendescribed previously (8, 9). The cells were from the peripheral blood,and only patients with 60% or more abnormal cells in the peripheralblood were studied.
The tissue culture cell lines derived from patients with leukemia andlymphoma were grown on Roswell Park Memorial Institute Medium1640 with 10% fetal calf serum. Some membrane properties of thesecell lines have been described previously (7, 17, 20).
Enriched fractions of PMN, lymphocytes, and monocytes were prepared from peripheral blood according to the procedure of English andAnderson (6). The PMN fraction was determined to be >95% PMNcells by Wright-Giemsa staining. Adherent cells containing >80%
monocytes by esterase staining properties were prepared by adherence of mononuclear cells to plastic Petri dishes for 1 hr at 37° in
Roswell Park Memorial Institute Medium 1640 containing 20% normalhuman serum. The adherent cells were removed from the Petri dishesby gentle scraping with a rubber policeman. The nonadherent cells had>2% esterase-positive cells. Enriched T-cells were prepared by removing B-lymphocytes with a goat anti-human Fab serum (14). All
enriched cell fractions were >90% viable at the time of testing.Microcytotoxicity Assay. The eosin dye exclusion microcytotoxicity
assay used in these studies has been described in detail in a previouspublication (1).
Cell Surface Labeling and RIP-PAGE Analysis. The procedure used
for analysis of the reactivity of the antisera with cell surface moleculeshas been described in detail (1, 2, 5). Viable cells were labeled with125I by the lactoperoxidase technique and solubilized with Triton X-100. Aliquots of labeled antigen (1 to 2 x 105 cpm) and antisera (5 to
20 jul) were incubated for 1 hr at room temperature followed by theaddition of 200 p.\of 10% fixed Staphylococcus áureos (15 min at roomtemperature). The samples were washed 3 times, reduced in 1%sodium dodecyl sulfate and 5% /S-mercaptoethanol, and electropho-resed in 5 to 15% discontinuous sodium dodecyl sulfate-polyacryl-
amide gradient gels. The gels were dried, and autoradiography wasperformed.
Results
Specificity of Xenoantisera to Myeloid-Monocyte-associ-ated Antigens. The microcytotoxicity titers and specificity ofthe M antisera with normal cells and tissue culture cell linesare shown in Charts 1 and 2. The M antisera react to titers>50 with adherent peripheral blood cells and PMN and fail toreact with the nonadherent cell fraction as well as enriched T-cells and CLL cells (Chart 1). The normal cell donor for thedata in Chart 1 was the immunizing normal cell donor for theantiserum to blood monocytes. The reactivity of the anti-M serawith established suspension-type tissue culture cell lines fromleukemic donors also indicates their myeloid-monocyte specificity. The antisera react with a monocytic-macrophage-like cellline U937 and with the HL60 cell line derived from a patientwith promyelocytic leukemia (7) which can be induced toterminal granulocytic differentiation (Chart 2). The antisera failto react with lymphoid-type cell lines NALM-1, SB, MOLT, and
CEM (Chart 2). Other membrane antigen properties of thesecell lines can be seen in Table 2.
Specificity of Other Xenoantisera. The molecular characteristics of the antigens, a brief summary of their distributionon normal cell types, and detailed references on the specificityof the various antisera are described in Table 1 and "Materialsand Methods." A composite of RIP-PAGE analysis of theantigens detected by the antisera utilizing various 125l-labeled
membrane antigen preparations is shown in Fig. 1 and isdescribed briefly in "Materials and Methods." The cytotoxic
reactivities of the TLAA, THY, CALLA, la, and M antisera withB, T, myeloid, and monocytic cell lines established from patients with leukemia or lymphoma are given in Table 2. TheTLAA antisera react only with the 2 T-cell lines MSB and Molt,
while the THY antisera react only with the Molt line. The laantisera react strongly with the B lymphoblastoid cell line (SB)and the NALM1 and NALM6 lines. The 30 to 40% lysis notedwith the la antisera and HL60 cells is the maximum lysis notedwith these cells on repeated testing, and the percentage oflysis varied with the degree of differentiation seen at differentpassage levels. The CALLA antisera reacted only with the 2cell lines (Nairn 1 and 6) reported to have CALLA (17). Theanti-M sera as previously shown in Chart 2 reacted only with
the U937 and HL60 cell lines.Leukemic Cell Reactivity of Xenoantisera. The rabbit and
4782 CANCER RESEARCH VOL. 41
on April 7, 2019. © 1981 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Serological Classification of Human Leukemia
100
80
40
20
T T T ±:18 54 162
TitÃr
-t—r¿D
O
T486 NRS
Control
Chart 1. Cytotoxic reactivity of M antisera with enriched cell fractions fromperipheral blood cells of a normal donor and CLL cells. O, adherent cells; A,PMN; G, nonadherent cells; •,enriched T-cells and CLL cells. NRS, normal
rabbit serum.
486 NRSControl
Chart 2. Cytotoxic reactivity of M antisera with tissue culture cell lines derivedfrom patients with leukemia or lymphoma. O, U937 and HL60; A, NALM-1 andSB; D, Molt and CEM. NRS, normal rabbit serum.
monkey antisera described in Tables 1 and 2 and Chart 2 wererecently tested on a frozen peripheral blood cell panel from 30patients with leukemia or lymphomas (see "Materials and Methods"). The microcytotoxicity analysis of these cells with the
various antisera is shown in Table 3. Three of the 30 cellsamples could not be tested because of poor viability of thecells after thawing or due to high sensitivity of the leukemiccells to rabbit complement. Three of the patients with lymphoidcancers were pediatrie, while the remaining patients wereadults. Patients 1 to 25 had a consensus diagnosis of eitherlymphoid or myeloid cancer. In a few instances, there wassome problem of subclassifying the myeloid leukemia as acutemyeloid leukemia, AMOL, or AMML (Patients 6, 12, and 15).The diagnosis for Patients 26 and 27 prior to cytotoxicitytesting was not unanimous, and there were differing opinionson a diagnosis of myeloid versus lymphoid cancer.
The anti-M sera were strongly reactive (60 to 100% lysis)with cells from Patients 1 to 15, 26, and 27. The antisera toTLAA, THY, and CALLA were negative with cells from thesepatients. The la antisera were nonreactive with cells fromPatient 1 and gave 35 to 100% lysis with the cells from theother patients in this group. On the basis of their reactivity withanti-M sera and their lack of lymphoid and CALLA antigens,the cells from Patients 1 to 15, 26, and 27 would be serologi-cally classified as being from diseases of the myeloid lineage.Since the anti-M sera also react with normal myeloid cells, thediagnosis of leukemia would have to be made by other criteria.The cells from Patient 16 reacted with the anti-TLAA, anti-la,and anti-M sera and represent a serological reaction pattern
typical of some AMML patients described in a previous report(4) showing reactivity with both TLAA and la antisera.
Cells from Patients 17 through 25 with lymphoid cancersshowed no reactivity with the anti-M sera but, with the exception of cells from Patient 17, this group did react with antiserato CALLA, TLAA, or THY. Cells from the patient with B-celllymphosarcoma (Patient 17) had surface immunoglobulins (notreported in Table 3) and la antigens. Cells from Patients 18,
Table 2
Cytotoxic reactivity of antisera to human membrane antigens with tissue culturecell lines derived from patients with leukemia or lymphoma
SBMSBMolt-4U937HL60K562Nalm-1Nalm-6a-TLAAa90-100690————u-THY_90-100—————or-la100———30-40—90-100100«-Com
monALL—————90-10090-100«-M——90-10090-100—_NTCNormalserum
controls10-2010-20<10<10<101010-2010
—.less than 10% increased percentage of lysis of antiserum over controls.6 Numbers represent percentage of cells lysed by antisera as estimated to
the nearest 10%. Control percentage of lysis is not subtracted from these values.Where more than one figure is given, it represents the ranges of percentage oflysis noted with different antisera defining the same antigen.
0 NT, not tested.
MWSTANDARD
ANTIBODYUSEDINRIP
a a a aTLAA CALLA THY ß-ZU
alo
200 K-
94 K— ,67 K-
43 K-
14K-
T-ALL
125,
C-ALL THYMUS THYMUS C-ALL
'I-Lobeled Antigen Used in RIP
Fig. 1. Sodium dodecyl sulfate-polyacrylamide gel electrophoresis analysis(5 to 15% slab gels) of immune precipitates of 125l-labeled membrane antigens
and absorbed xenoantisera to human membrane antigens. C-ALL, common ALL;K, thousands, aß-2m,rabbit anti-/?-2-microglobulin.
NOVEMBER 1981 4783
on April 7, 2019. © 1981 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

R. S. Metzgar et al.
Table 3
Cytotoxic reactivity of antisera to human membrane antigens with cells from patients with leukemia orlymphoma3
Patient1234S6789101112131415161718192021222324252627ConsensusdiagnosisAML6AMLAMI-AMI.AMLMI.'...
,MOLAMOLAMOLAMOLAMOLAMMLAMML-AMLAMMLAMMLAML-AMMLAMMLB-LSLALLALL"ALL"T-ALLTALLT-ALL"T-ALLALLAML-B-LSLAML-ALLE-rosetta
formation ratio
<4°:37°)6:18:43:113:492:NT76:503:093:8730:1012:6%
of lysis with 1:5orTLAA
THYCALLAc—
—______________________________—______—50_
__95100100100
451009510040100100
60___-- -1:10
diluted antiseratola_9580908540100100957075556510035909095100100—_———10095M8095859085951001009510060959510010070___——_———9085Control152020101020153020201020151010101020103025401015101025
a Three cells had >40% lysis in controls and were not charted.0 AML. acute myeloid leukemia; B-LSL. B-cell lymphosarcoma; NT, not tested.c -, less than 10% increased percentage of lysis over controls.a Pediatrie patients.
19, and 20 were CALLA and la antigen positive and werephenotypically the non-T, non-B ALL type. Cells from the 4patients (Patients 21 to 24) diagnosed as T-ALL or as an
unclassified ALL (Patient 25) reacted with the TLAA antisera.Cells from 4 of the 5 T-ALL patients reacted with the THYantisera. Cells from 3 of the 4 THY-positive patients showedsome E-rosette formation at 37°. Cells from Patient 24 had
strong reactivity with anti-TLAA sera, formed a high percentageof E-rosettes at 4°and 37°,but lacked the THY antigen. Cells
of Patient 24 provide additional evidence that THY antigenexpression is independent from the E-rosette receptor and is
the second example that we have seen of a cell that formsstable E-rosettes but is THY negative (5).
Cells from the 2 patients (Patients 26 and 27) with a discrepant consensus diagnosis had a serological phenotype of beingM and la antigen positive and CALLA, THY, and TLAA negative.This serological phenotype would indicate that the cancerswere myeloid rather than lymphoid.
Discussion
Since most of the antigens (TLAA, THY, la, and M) definedwith xenoantisera are not tumor specific, these reagents cannotbe used by themselves for the diagnosis of leukemia or lym-phoma. However, the use of these serologically defined anti-
genie markers have proven to be of value in the often timesdifficult task of classification of leukemia or lymphoma. Theaddition of the antisera defining a myeloid-monocyte-associ-ated antigen to our panel provided a clear-cut way to distin
guish myeloid from lymphoid cancers (Table 3). All of the acutenonlymphocytic leukemias thus far tested have reacted with
the anti-M sera, while none of the lymphoid leukemias orlymphomas have. The myeloid-type leukemia cells can be
further subclassified by the presence of la antigens. Cells fromsome AMML patients can also be subclassified by their reactivity with TLAA antisera. Our anti-M sera do not distinguishmyeloblasts or myeloblast-derived cells from monoblasts ormonocytes-macrophages, and they show the same leukemicand normal cell specificity as do the anti-M sera described by
Roberts and Greaves (19). Since the molecular nature of theantigen detected by Roberts and Greaves, anti-M serum (19),
was not described and our M antigen also is not well characterized by RIP-PAGE analysis, the identity of the M antigens
defined by the antisera from these 2 laboratories can beinferred only from comparison of the serological specificity.Future studies with monoclonal antibodies may define an antigen which is present on monocytes but not on granulocytes ormyeloblasts.
The lymphoid cancers lack M antigen but react with variouscombinations of TLAA, THY, CALLA, and la antisera (Table 3).The B-cell lymphosarcoma cells of Patient 17 have surface
immunoglobulin (data not reported here) and are la positive.The phenotype is thus similar to that noted for CLL cells (1).The other ALLs can then be subdivided into 2 major categorieson the basis of reactivity with either CALLA or TLAA antisera.The TLAA antisera gave 100% lysis of the CALLA-negativeALL cells, whereas E-rosette analysis showed percentages of3 to 93 for the "T" group. We have previously described
examples of ALL cells which serologically would be classifiedas T but which had low or intermediate E-rosette percentagesand were la antigen negative (3). The T-ALL group can be
further subdivided on the basis of reactivity with THY antisera.
4784 CANCER RESEARCH VOL. 41
on April 7, 2019. © 1981 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

Serological Classification of Human Leukemia
In this report, 5 of 6 T-ALL patients reacted with the THYantisera. In a more detailed report (5), 15 of 19 T-ALL patients
had >50% of their cells reactive with the THY antisera. Again,in this latter study, the best normal marker for classification ofleukemic cells as T-cells was the TLAA antigen (5). There isalso no direct correlation between active or stable E-rosetteformation at 37°and THY antigen expression (Table 3). This
was also noted with cells from some of the T-ALL patients
reported elsewhere (5).The advantages and disadvantages of microcytotoxicity as
an assay for leukemic cell surface antigens have been discussed in detail previously (15). In brief, the disadvantages aresensitivity of some of the cells to complement or to antibodiesin normal sera and the inability to detect minor populations ofreactive cells (less than 10%). The advantages are that a largenumber of sera or dilutions can be tested rapidly on a fewmillion target cells by one technician. Thus, although the fluorescent-activated cell sorters, radioimmunoassays, or enzyme-linked immunoassays have greater sensitivity in antigen
analysis, there are still advantages to microcytotoxicity as arapid screening assay.
Acknowledgments
The authors wish to thank Patti Tapp, Elizabeth Morton, and Melissa Gaillardtor their excellent technical assistance.
References
1. Anderson, J. K., and Metzgar, R. S. Detection and partial characterizationof human T and B lymphocyte antigens with antisera to MSB and SB celllines. J. Immunol., 120: 262-272, 1978.
2. Anderson, J. K., and Metzgar, R. S. Further characterization of a human Tlymphocyte associated antigen. Clin. Exp. Immunol., 37: 339-347, 1979.
3. Anderson, J. K., Moore, J. O., Palletta, J. M., Terry, W. F., and Metzgar, R.S. Acute lymphoblastic leukemia: classification and characterization withantisera to HSB and SB cell lines. J. Nati. Cancer Inst., 62: 293-298, 1979.
4. Anderson, J. K., Moore, J. O., and Metzgar, R. S. Detection of both T celland la like antigens on cells from patients with acute myelomonocyticleukemia and chronic myelogenous leukemia in blast crisis. Cancer Res.,39:4810-4815. 1979.
5. Dowell, B. D., Palletta, J. M., Moore, J. O., and Metzgar, R. S. Detection andpartial characterization of human thymus-leukemia antigens. J. Nati. CancerInst., 65. 691-701, 1980.
6. English, D., and Andersen, B. R. Single-step separation of red blood cells,granulocytes and mononuclear leukocytes on discontinuous density gradients of Ficoll-Hypaque. J. Immunol. Methods, 5: 249-252, 1974.
7. Gallagher, R., Collins, S., Trujillo, J., McCredie, K., Ahearn, M., Tsai, S.,Metzgar, R., Aulakh, G., Ting, R., Ruscetti, F., and Gallo, R. Characterizationof the continuous differentiating myeloid cell line (HL-60) from a patient withacute promyelocytic leukemia. Blood, 54: 713-733, 1979.
8. Gordon, D. S., and Hubbard, M. Surface membrane characteristics andcytochemistry of the abnormal cells in adult acute leukemia. Blood, 5).681-692, 1978.
9. Gordon, D. S., Mutton, J. J., Smalley, R. V., Meyer, Leon, N., and Vogler. W.Terminal deoxynucleotidyl transferase (TdT) cytochemistry and membranereceptors in adult acute leukemia. Blood, 52. 1079-1088, 1978.
10. Greaves, M. F. Clinical applications of cell surface markers. Prog. Haematol.,9: 255-303, 1975.
11. Greaves, M. F., Brown, G., Rapson, N., and Lister, T. A. Antisera to acutelymphoblastic leukemia cells. Clin. Immunol. Immunopathol., 4: 67-84,
1975.12. Greaves, M. F., and Janossy, G. Patterns of gene expression and the cellular
origins of human leukemias. Biochim. Biophys. Acta, 576: 193-230, 1978.13. Janossy, G., Francis, G. E., Capellaro, D., Goldstone, A. H., and Greaves,
M. F. Cell sorter analysis of leukemia-associated antigens on human myeloidprecursors. Nature (Lond.), 276: 176-178, 1978.
14. Metzgar, R. S., Bertoglio, J., Anderson, J. K., Bonnard, G. D., and Ruscetti,F. W. Detection of HLA-DRw (la-like) antigens of human T lymphocytesgrown in tissue culture. J. Immunol., T22: 949-953, 1979.
15. Metzgar, R. S., and Mohanakumar, T. Serologie studies of the diagnosis andnosology of human leukemia. Am. J. Clin. Pathol., 68: 699-705, 1977.
16. Metzgar, R. S., and Mohanakumar, T. Tumor associated antigens of humanleukemia cells. Seminars Hematol., 75. 139-156, 1978.
17. Minowada, J., Janossy, G., Greaves, M. F., Tsubota, T., Srivastava, B. I. S.,Morikawa, S., and Tatsumi, E. Expression of an antigen associated withacute lymphoblastic leukemia in human leukemia-lymphoma cell lines. J.Nati. Cancer Inst., 60: 1269-1277, 1978.
18. Mohanakumar, T., and Metzgar, R. S. Human thymus leukemia antigen(s):detection by a nonhuman primate antiserum. Cell. Immunol., 72: 30-36,
1974.19. Roberts, M. M., and Greaves, M. F. Maturation linked expression of a
myeloid cell surface antigen. Br. J. Haematol.. 38. 439-452, 1978.
20. Sundstrom, C., and Nilsson, K. Establishment and characterization of ahuman histiocytic lymphoma line. Int. J. Cancer, 7: 565-577, 1976.
NOVEMBER 1981 4785
on April 7, 2019. © 1981 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from

1981;41:4781-4785. Cancer Res Richard S. Metzgar, Barry L. Dowell, Lawrence B. Lachman, et al. Analysis with XenoantiseraClassification of Human Leukemia by Membrane Antigen
Updated version
http://cancerres.aacrjournals.org/content/41/11_Part_2/4781
Access the most recent version of this article at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://cancerres.aacrjournals.org/content/41/11_Part_2/4781To request permission to re-use all or part of this article, use this link
on April 7, 2019. © 1981 American Association for Cancer Research. cancerres.aacrjournals.org Downloaded from