Embed Size (px)
Citation preview
Renal “Pot Pourri”:CKD, proteinuria, anaemia, bone disease and
stones
Cambridge Medical SeminarsDr Elaine Jolly
Consultant in Nephrology and Acute Medicine24 November 2018
Outline of talk
• Define CKD• eGFR calculation and interpretation
• Referral guidelines for CKD
• ACRs: how to interpret and when to act
• Potential scenarios on the medical take– Case vignettes
• Issues arising as a consequence of CKD– Anaemia management
– Renal bone disease
• Stone disease
Chronic kidney disease (CKD)
• Common: affects 5.5 - 8.5% of UK population• Expensive: £1.44 billion in 2009-2010 (NHSE)• Not a specific diagnosis - further assessment to
establish cause and individualise treatment• Asymptomatic in early stages
• Management has 4 key aims:– Manage risk factors for cardiovascular disease– Slow CKD progression– Detect and treat CKD-related complications (Stage 3b
onwards)– Allow timely preparation for renal replacement therapy
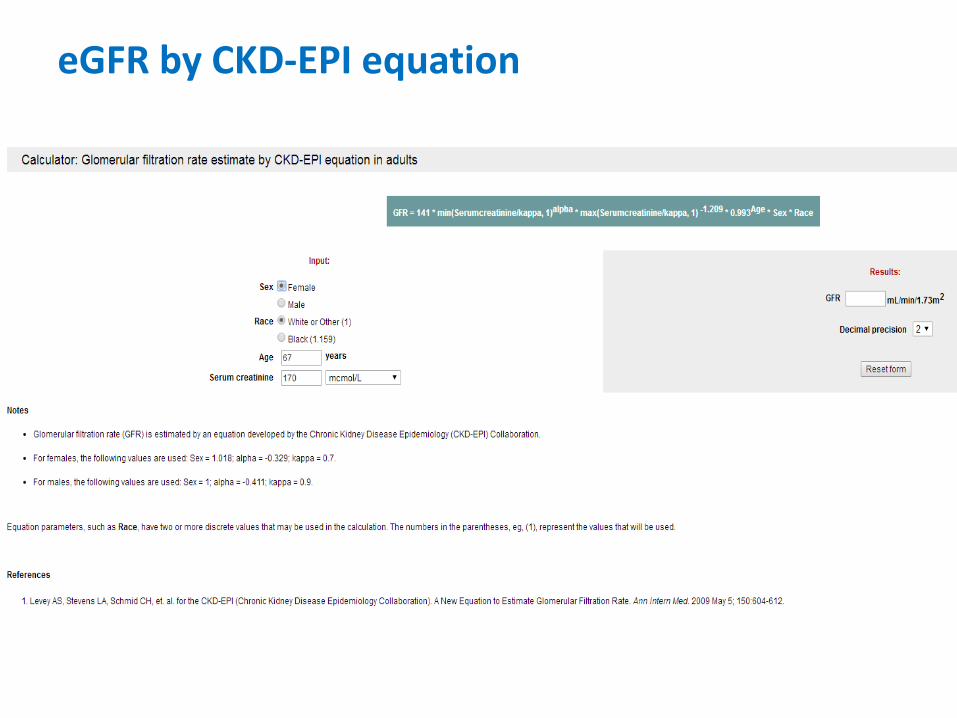
eGFR by CKD-EPI equation
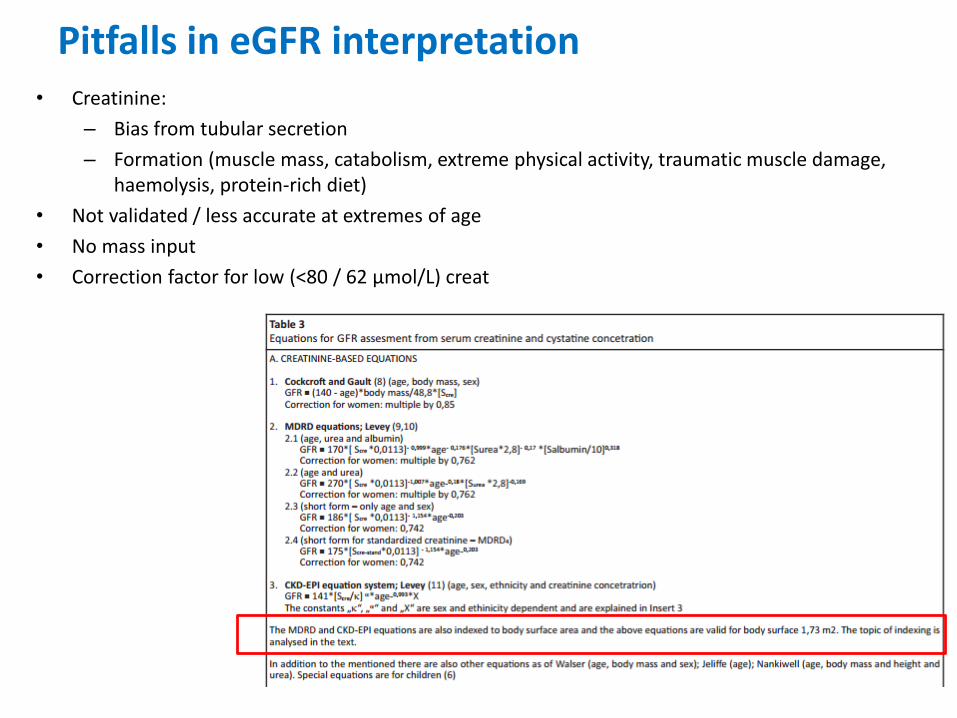
Pitfalls in eGFR interpretation• Creatinine:
– Bias from tubular secretion
– Formation (muscle mass, catabolism, extreme physical activity, traumatic muscle damage, haemolysis, protein-rich diet)
• Not validated / less accurate at extremes of age
• No mass input
• Correction factor for low (<80 / 62 µmol/L) creat
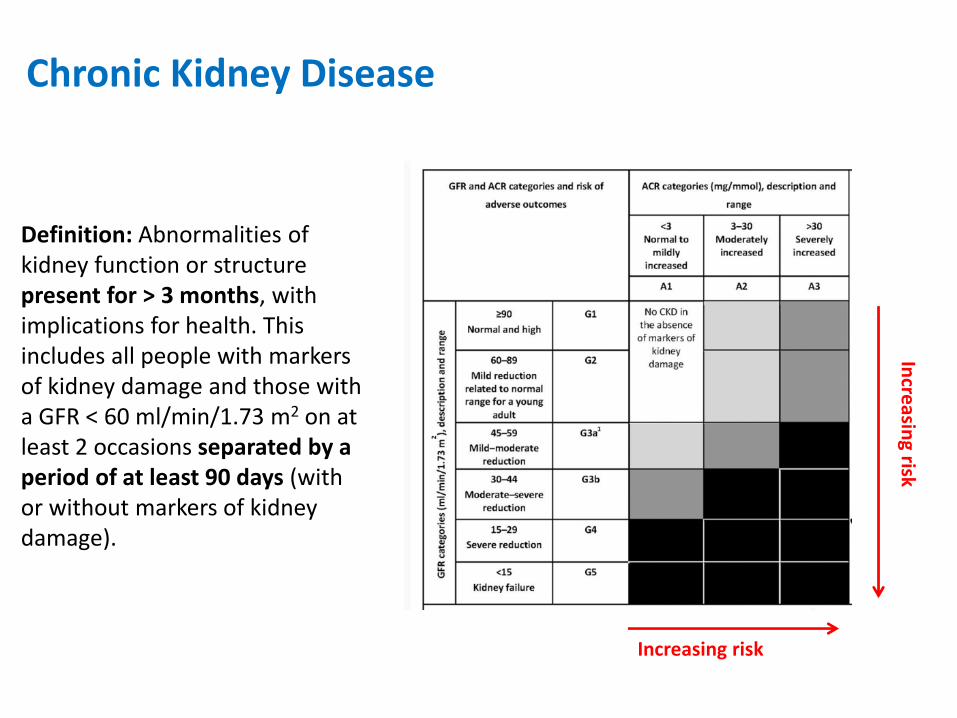
Chronic Kidney Disease
Definition: Abnormalities of kidney function or structure present for > 3 months, with implications for health. This includes all people with markers of kidney damage and those with a GFR < 60 ml/min/1.73 m2 on at least 2 occasions separated by a period of at least 90 days (with or without markers of kidney damage).
Increasing risk
Incre
asing risk
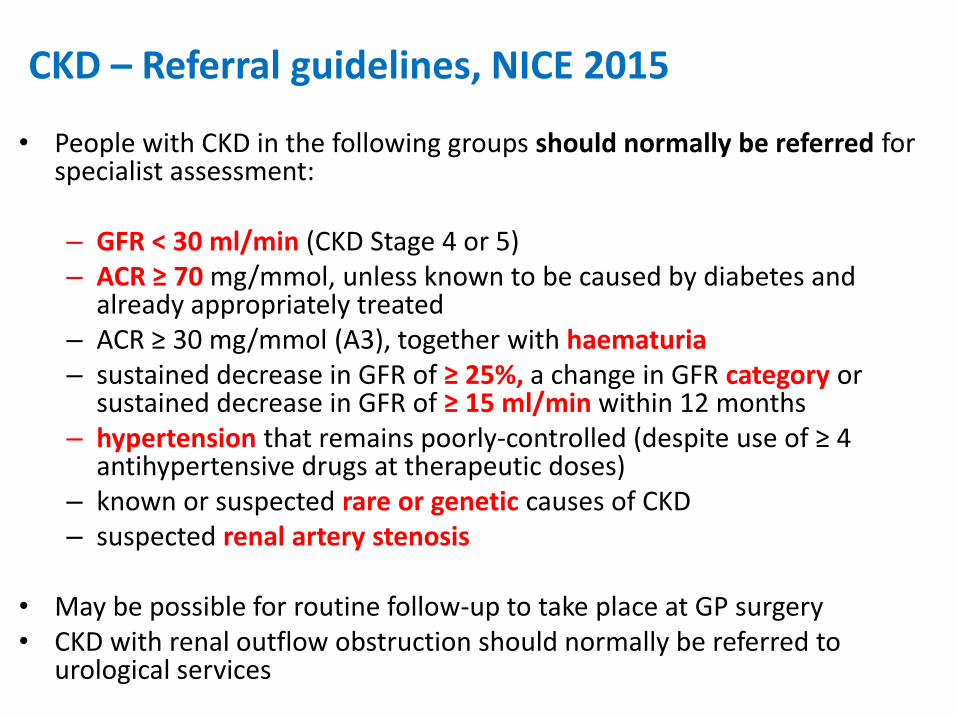
CKD – Referral guidelines, NICE 2015
• People with CKD in the following groups should normally be referred for specialist assessment:
– GFR < 30 ml/min (CKD Stage 4 or 5)– ACR ≥ 70 mg/mmol, unless known to be caused by diabetes and
already appropriately treated– ACR ≥ 30 mg/mmol (A3), together with haematuria– sustained decrease in GFR of ≥ 25%, a change in GFR category or
sustained decrease in GFR of ≥ 15 ml/min within 12 months– hypertension that remains poorly-controlled (despite use of ≥ 4
antihypertensive drugs at therapeutic doses) – known or suspected rare or genetic causes of CKD– suspected renal artery stenosis
• May be possible for routine follow-up to take place at GP surgery• CKD with renal outflow obstruction should normally be referred to
urological services
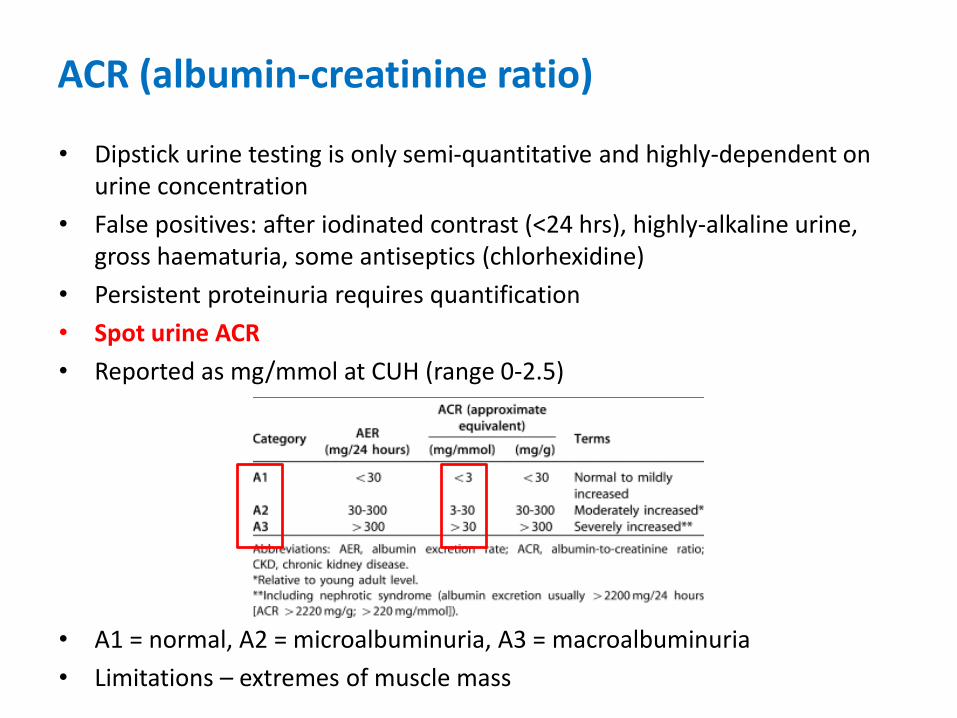
ACR (albumin-creatinine ratio)
• Dipstick urine testing is only semi-quantitative and highly-dependent on urine concentration
• False positives: after iodinated contrast (<24 hrs), highly-alkaline urine, gross haematuria, some antiseptics (chlorhexidine)
• Persistent proteinuria requires quantification
• Spot urine ACR
• Reported as mg/mmol at CUH (range 0-2.5)
• A1 = normal, A2 = microalbuminuria, A3 = macroalbuminuria
• Limitations – extremes of muscle mass
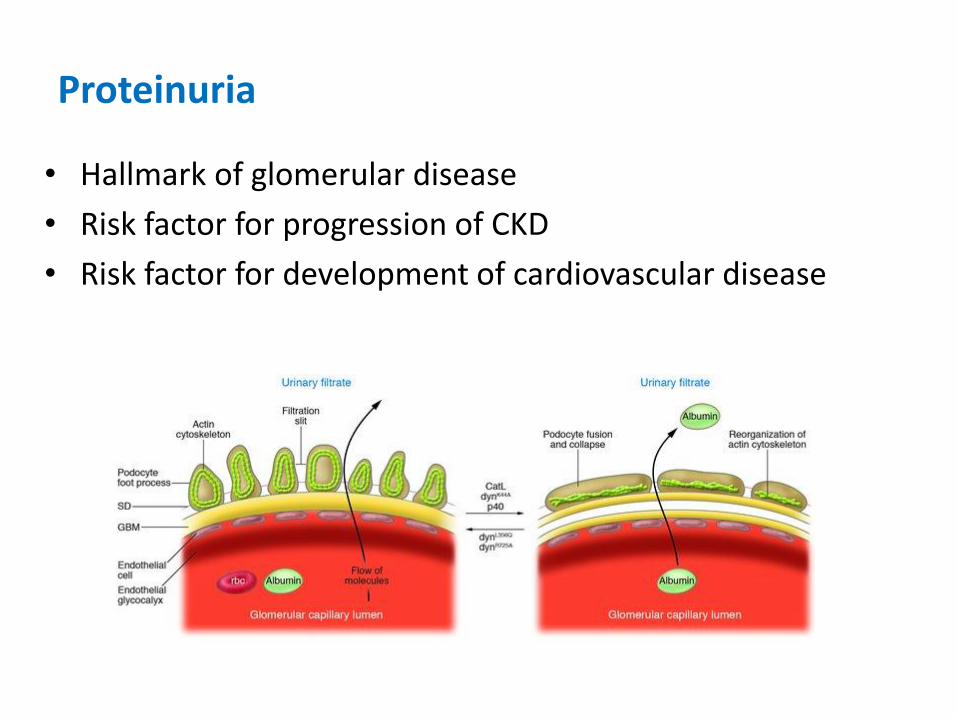
Proteinuria
• Hallmark of glomerular disease
• Risk factor for progression of CKD
• Risk factor for development of cardiovascular disease
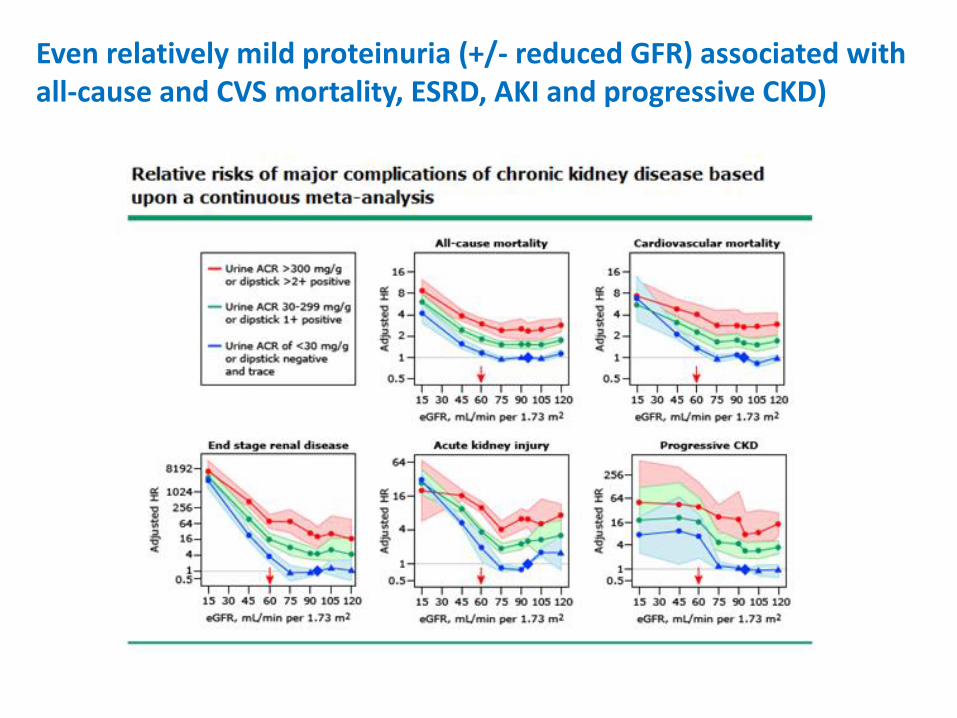
Even relatively mild proteinuria (+/- reduced GFR) associated with all-cause and CVS mortality, ESRD, AKI and progressive CKD)
Proteinuria
• Nephrotic-range: discuss with nephrology (renal biopsy usually indicated)
• Exclude post-renal proteinuria
• Non-nephrotic (isolated) proteinuria:
– Medical history and exam
– Measure serum creat / eGFR
– Exclude transient (fever, exercise, UTI, young) or orthostatic
– May reflect an underlying renal or systemic disorder:
• ANA, ANCA, C3/C4, immunoglobulins, hepatitis/HIV serology
• Urine for monoclonal light chains
• Renal US (reflux, ADPKD)
• Nephrology referral if A3
• Kidney biopsy usually indicated for non-nephrotic proteinuria with active urinary sediment or decreased GFR or if proteinuria persistently >1g/day or new NVH, hypertension, drop in GFR

Case 1 – CKD and Medication
• AB, 65Y, male
• 2/7 history of dysuria, fever, right loin discomfort
• PMH: IHD (PCI 2016, LVEF 45%), hypertension, CKD Stage 3a (baseline eGFR 45 ml/min, Creat 140), OA knees
• DH: aspirin, ramipril, amlodipine, frusemide, bisoprolol, (diclofenac)
• O/E: T 38.5, BP 95/60, HR 90 bpm, mild suprapubic and right renal angle tenderness
• Ix: WCC 15 (neutrophilia), CRP 247, Creat 165, lactate 3.1
Urine: Protein / blood / leucocytes / nitrites +
• Blood and urine cultures taken, IV fluids prescribed, IV augmentinand gentamicin (5mg/kg) given
What is your next step in management?https://designer.voxvote.com/Event/EditQuestion/78eb0fc1-0d29-437d-982c-a99a00dd93ca
• Continue regular medication unaltered
• Stop everything (just in case…)
• Stop the frusemide as giving IV fluids but continue everything else
• Stop ramipril and frusemide but continue bisoprolol and amlodipine
• Stop all antihypertensives and frusemide
• Stop ramipril, amlodipine and frusemide
• None of the above
ACEI / ARB
• Overwhelming evidence is positive (CKD / CCF / diabetes)
• Reduction in GFR is seen in some patients:
– Following the introduction / dose increase of RAS antagonists
– do not modify the dose if either:• GFR decrease is < 25% or
• Serum creatinine increase from baseline is < 30%
– May be severe in those with bilateral renal artery stenosis, hypertensive nephrosclerosis, heart failure, ADPKD or CKD
• May precipitate AKI in situations of reduced renal perfusion
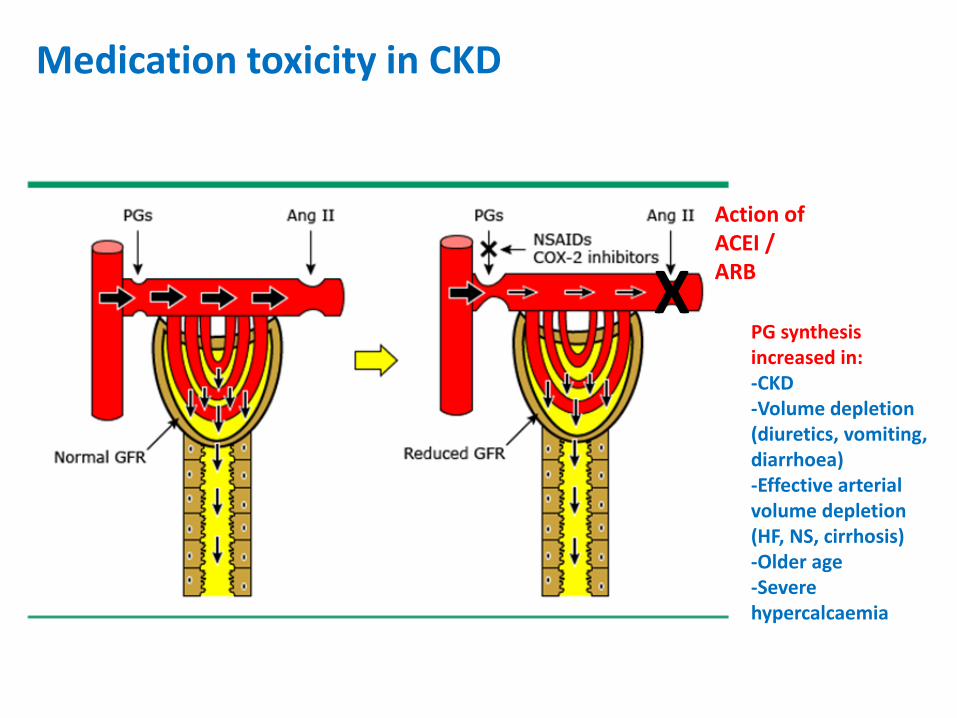
PG synthesis increased in:-CKD-Volume depletion (diuretics, vomiting, diarrhoea)-Effective arterial volume depletion (HF, NS, cirrhosis)-Older age-Severe hypercalcaemia
Medication toxicity in CKD
Action of ACEI / ARB
X

Case 2 – CKD and Anaemia
• CD, 35Y, female• Referred to ambulatory care with tiredness, GP checked bloods 1
week previously: Hb 88• PMH: ADPKD, CKD Stage 4 (baseline eGFR 20 ml/min, Creat 250,
DNA’d last 2 nephrology clinic visits), frequent UTIs, hypertension• DH: ramipril, trimethoprim / cefalexin, ferrous sulphate
• O/E: BP 125/70, HR 72 bpm, slightly pale, no abdominal pain, DRE: no melaena
• Ix: Hb 90 (MCV normal), Creat 300, K 5.8Historical results (Hb >100 when last seen in clinic 4/12 previously)Pregnancy test: negative
• Iron studies / folate / Vit B12 / TSH / blood film taken• Serum iron 4.0 / ferritin 10.3 / transferrin 2.98 / transferrin
saturation: 7%
What is your next step in management?https://designer.voxvote.com/Event/EditQuestion/65c4dc32-2a47-468c-980b-a99a00e02814
• Arrange urgent blood transfusion as symptomatically anaemic
• Nothing - I have no idea how to interpret iron indices
• Change iron preparation from oral to IV infusion
• Check EPO level and consider starting ESA (recombinant erythropoeitin)
• Contact the renal unit for advice
• None of the above
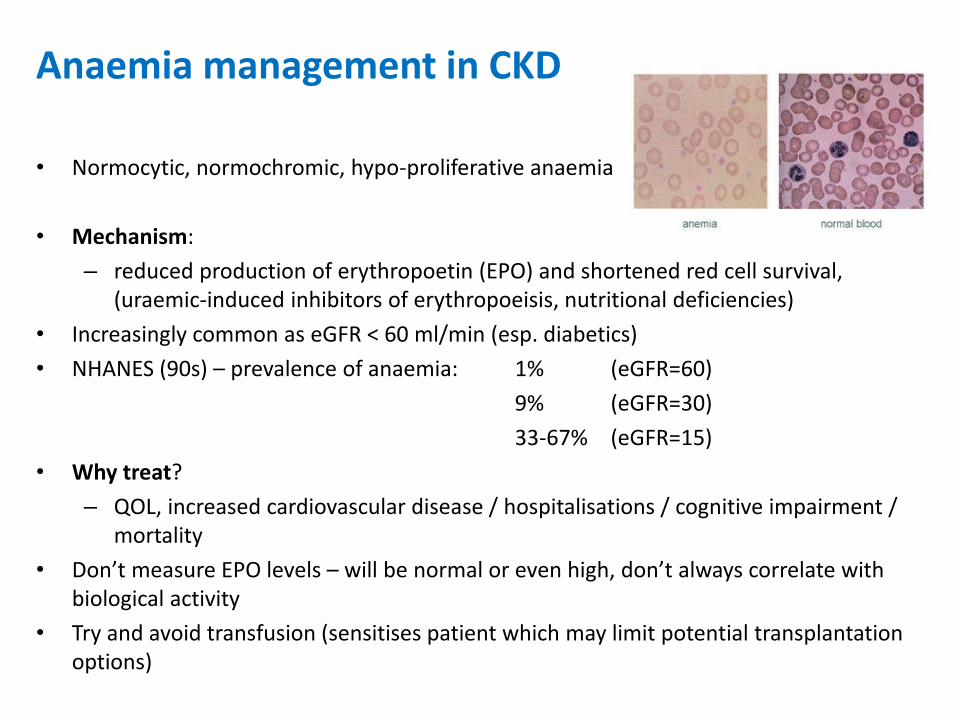
Anaemia management in CKD
• Normocytic, normochromic, hypo-proliferative anaemia
• Mechanism:
– reduced production of erythropoetin (EPO) and shortened red cell survival, (uraemic-induced inhibitors of erythropoeisis, nutritional deficiencies)
• Increasingly common as eGFR < 60 ml/min (esp. diabetics)
• NHANES (90s) – prevalence of anaemia: 1% (eGFR=60)
9% (eGFR=30)
33-67% (eGFR=15)
• Why treat?
– QOL, increased cardiovascular disease / hospitalisations / cognitive impairment / mortality
• Don’t measure EPO levels – will be normal or even high, don’t always correlate with biological activity
• Try and avoid transfusion (sensitises patient which may limit potential transplantation options)
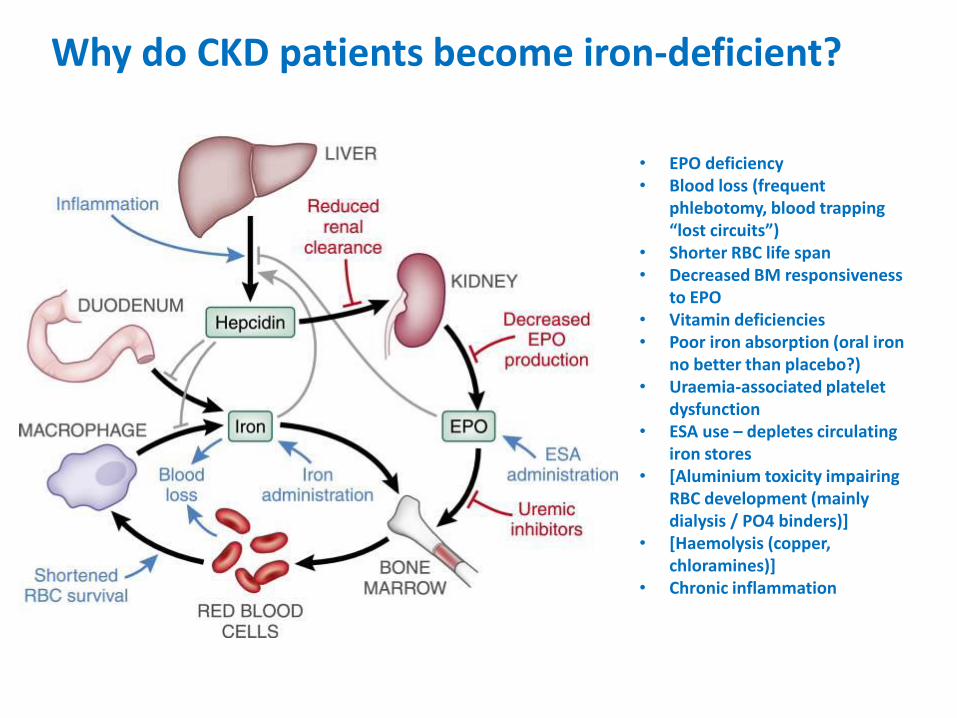
• EPO deficiency• Blood loss (frequent
phlebotomy, blood trapping “lost circuits”)
• Shorter RBC life span• Decreased BM responsiveness
to EPO• Vitamin deficiencies• Poor iron absorption (oral iron
no better than placebo?)• Uraemia-associated platelet
dysfunction• ESA use – depletes circulating
iron stores• [Aluminium toxicity impairing
RBC development (mainly dialysis / PO4 binders)]
• [Haemolysis (copper, chloramines)]
• Chronic inflammation
Why do CKD patients become iron-deficient?
NICE guidelines 2017 (CKD)
• Screening– eGFR < 60ml/min, 6-12 monthly– Assess iron status: % HRC (>6%) or reticulocyte haemoglobin content
(<29pg) or combination of transferrin saturation (<20%) and serum ferritin (<100 µg/L)
– Exclude non-renal causes of anaemia
• Management– Hb <110 g/L or symptoms, aiming to maintain Hb 100-120– Correct iron deficiency first: consider trial of oral iron before offering
IV iron (high-dose, low frequency)– Offer ESA if on-going anaemia despite iron sufficiency (eGFR <
30ml/min)– Correct hyperparathyroidism
–PIVOTAL trial

Case 3 – CKD and bone disease
• EF, 70Y, female
• 2/12 history of constipation, thirst, abdominal pain and nausea
• PMH: COPD, CKD Stage 4 (baseline eGFR 19 ml/min, Creat 220), PVD, hypertension
• DH: aspirin, amlodipine, bendroflumethiazide, doxazosin, seretide / salbutamol, alfacalcidol, sevelamer, aranesp
• O/E: BP 150/80, HR 95 bpm, clinically dry, mild generalised abdominal pain
• Ix: Creat 320, Ca 3.1, K 4.2, PO4 1.3, ALP 170
PTH 28 pmol/L
CXR: slightly prominent right hilum
What is your next step in management?https://designer.voxvote.com/Event/EditQuestion/ec6ee2a7-76f8-4aa6-a89a-a99a00e4e9de
• Consult a BNF………
• Check a serum ACE to confirm a putative diagnosis of sarcoidosis
• Rehydrate with IVI but continue all medication
• Rehydrate with IVI and stop alfacalcidol and bendroflumethiazide
• Rehydrate and prescribe pamidronate
• None of the above
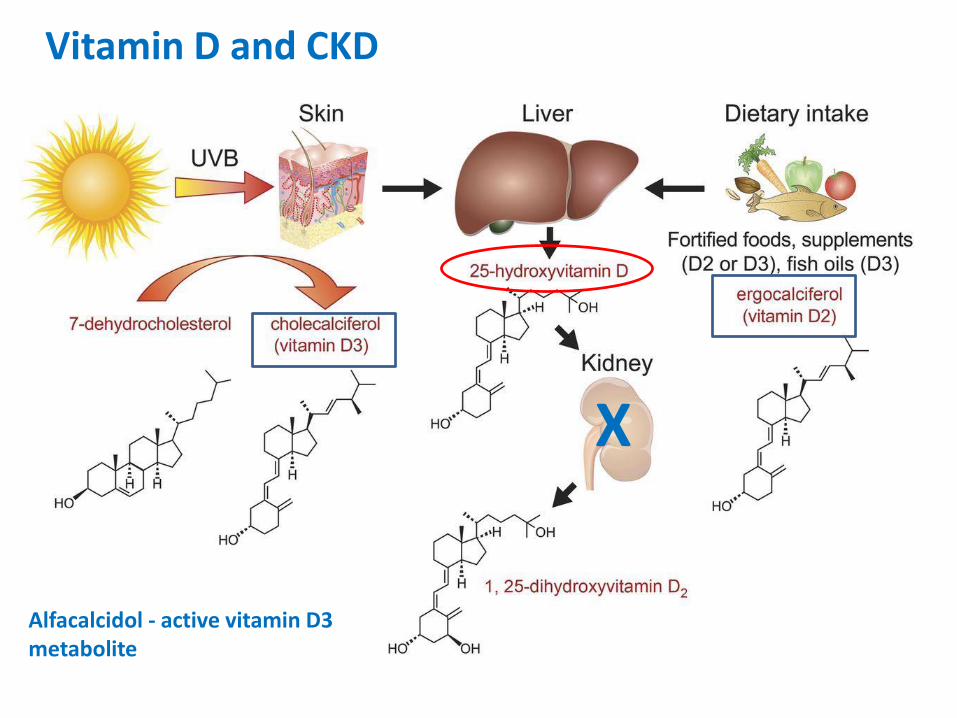
Alfacalcidol - active vitamin D3 metabolite
X
Vitamin D and CKD
Vitamin D deficiency
• Low serum 25(OH)D (calcidiol) level <20 ng/ml (50nmol/L)
• Very common in general pop. (> 40% of adults, NHANES 2006)
• In CKD population – pretty well ubiquitous
• Routine use of Vit D in CKD for the past 30 years to try to prevent / reverse the impact of hyperparathyroidism on the skeleton
• But does replacing deficiency guarantee benefit?
• Supplementation generally increases Vit D levels (and suppresses PTH) but less focus on clinical end-points (fracture risk, hospitalisations, mortality)
• Unresolved issues:– what should we be measuring
– what replacement protocol works best
– which end-points to use for titration
– role of monitoring and screening
Vitamin D supplements in the management of CKD-MBD, NICE 2014
• “Detailed advice on the management of CKD–MBD is beyond the scope of this guideline. If uncertain, seek advice from your local renal service.”
• Do not routinely offer vitamin D supplementation to manage or prevent CKD–mineral and bone disorders
• Offer cholecalciferol or ergocalciferol to treat vit D deficiency in people with CKD and vit D deficiency (“Native” Vit D, eGFR >30 ml/min, Normal PTH/PO4)
• If vit D deficiency has been corrected and symptoms of CKD–MBD persist, offer alfacalcidol (1-alpha-hydroxycholecalciferol) or calcitriol (1-25-dihydroxycholecalciferol) to people with a GFR <30 (G4 or G5) (“Synthetic or active” Vit D, eGFR <30 ml/min)
• Monitor serum Ca2 + PO4 in people receiving alfacalcidol or calcitriolsupplements

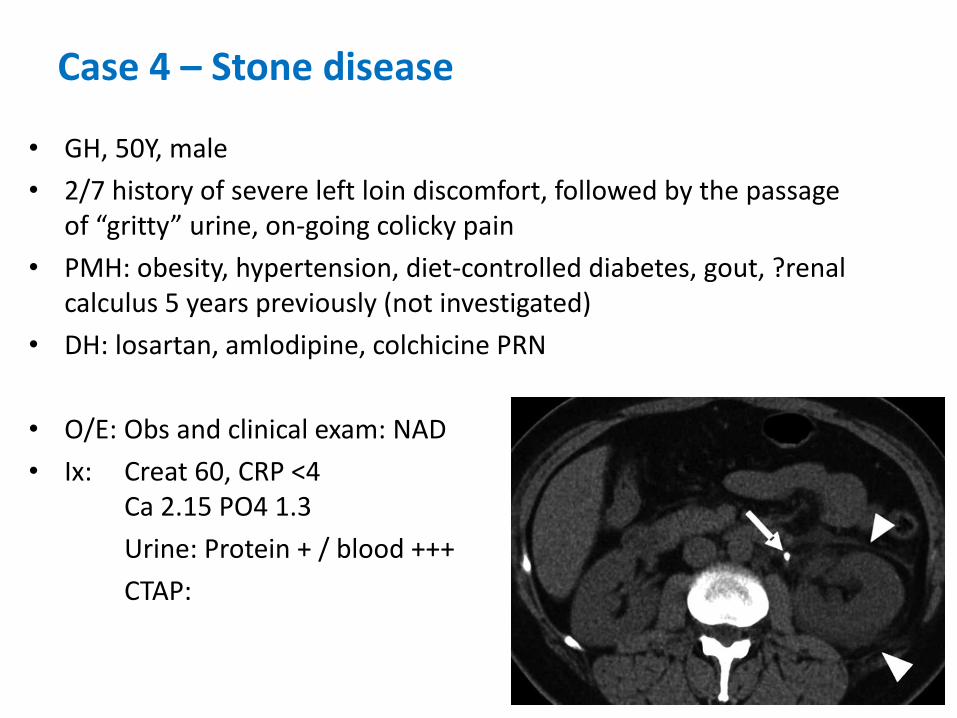
Case 4 – Stone disease
• GH, 50Y, male
• 2/7 history of severe left loin discomfort, followed by the passage of “gritty” urine, on-going colicky pain
• PMH: obesity, hypertension, diet-controlled diabetes, gout, ?renal calculus 5 years previously (not investigated)
• DH: losartan, amlodipine, colchicine PRN
• O/E: Obs and clinical exam: NAD
• Ix: Creat 60, CRP <4 Ca 2.15 PO4 1.3
Urine: Protein + / blood +++
CTAP:
What is your next step in management?https://designer.voxvote.com/Event/EditQuestion/449e7e32-bf19-4d3e-897a-a99a00e99a21
• Contact urology
• 24 hour urine collections x2
• Measure serum urate
• Check urinary pH
• Consider switching antihypertensive medication
• Refer to renal stone clinic
• All of the above
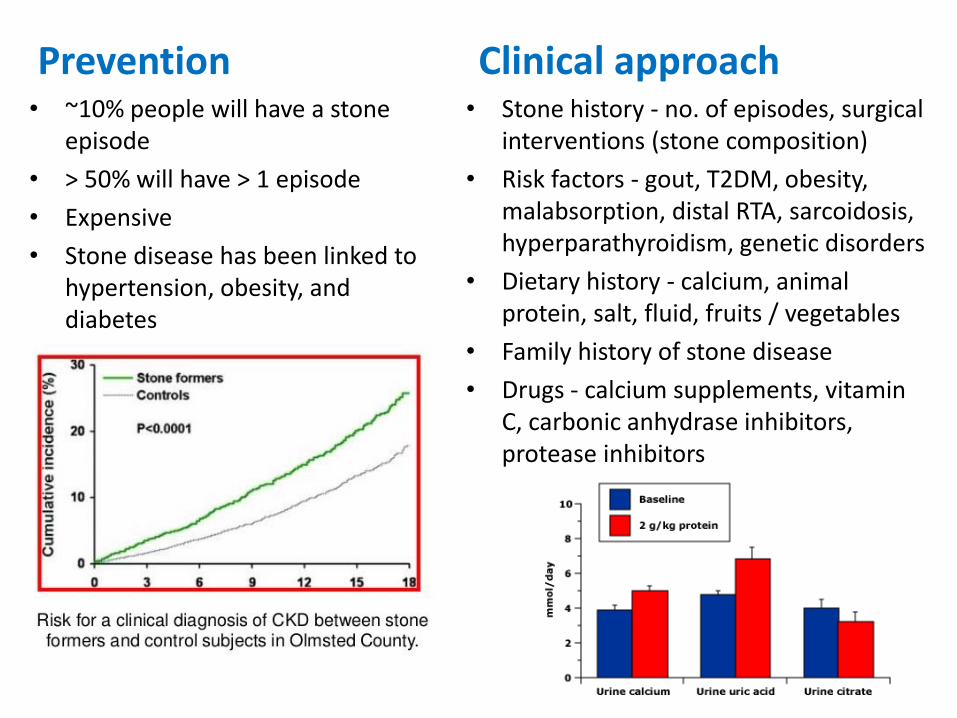
Prevention Clinical approach• ~10% people will have a stone
episode
• > 50% will have > 1 episode
• Expensive
• Stone disease has been linked to hypertension, obesity, and diabetes
• Stone history - no. of episodes, surgical interventions (stone composition)
• Risk factors - gout, T2DM, obesity, malabsorption, distal RTA, sarcoidosis, hyperparathyroidism, genetic disorders
• Dietary history - calcium, animal protein, salt, fluid, fruits / vegetables
• Family history of stone disease
• Drugs - calcium supplements, vitamin C, carbonic anhydrase inhibitors, protease inhibitors
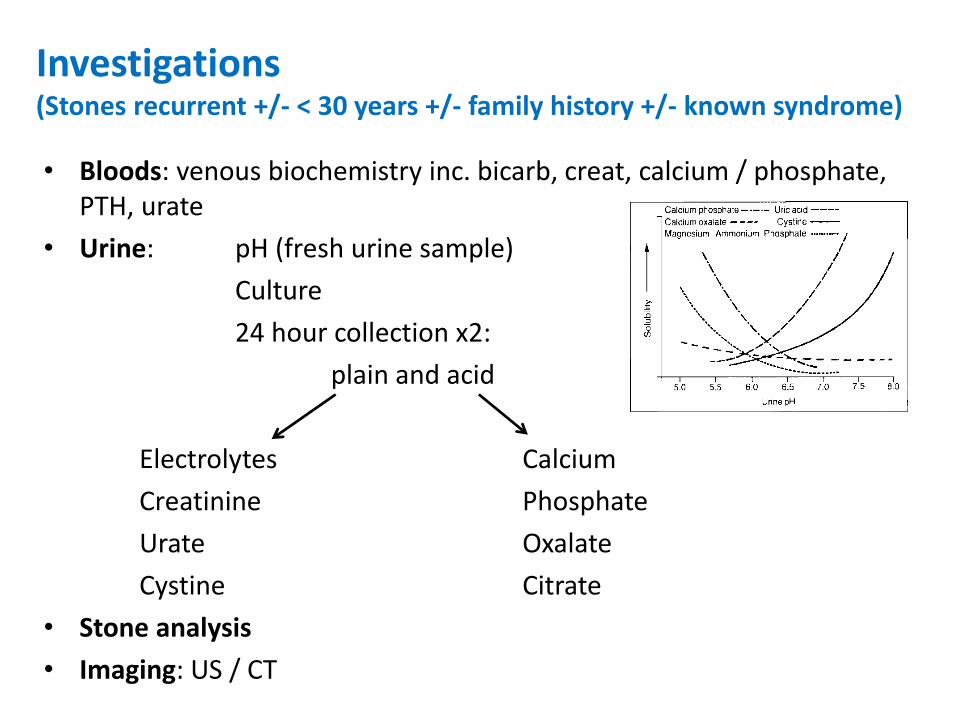
Investigations(Stones recurrent +/- < 30 years +/- family history +/- known syndrome)
• Bloods: venous biochemistry inc. bicarb, creat, calcium / phosphate, PTH, urate
• Urine: pH (fresh urine sample)
Culture
24 hour collection x2:
plain and acid
Electrolytes Calcium
Creatinine Phosphate
Urate Oxalate
Cystine Citrate
• Stone analysis
• Imaging: US / CT
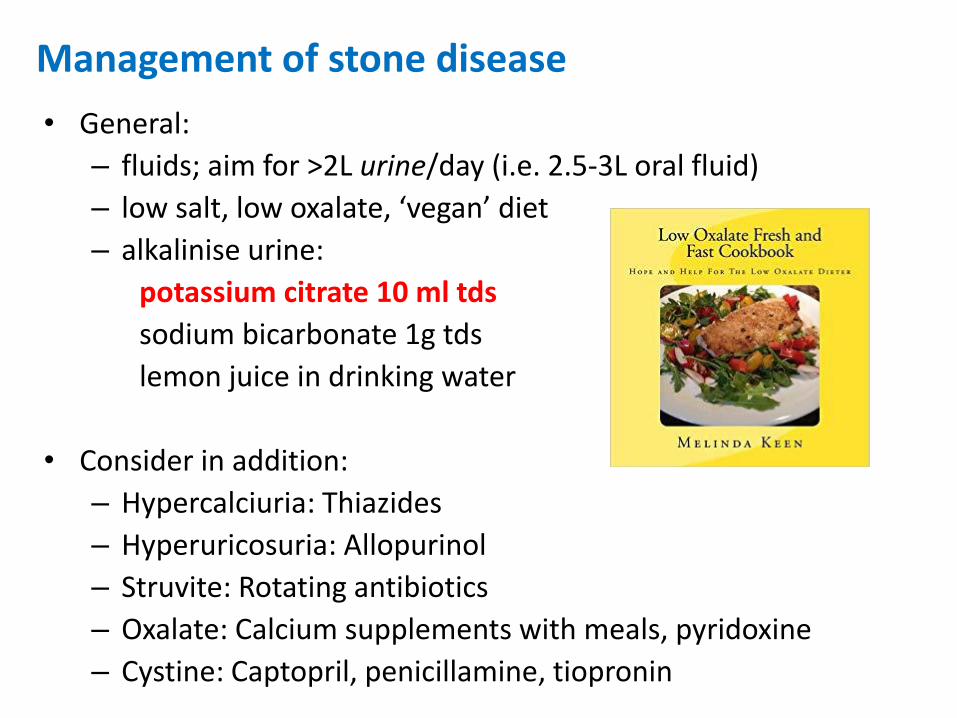
Management of stone disease
• General:
– fluids; aim for >2L urine/day (i.e. 2.5-3L oral fluid)
– low salt, low oxalate, ‘vegan’ diet
– alkalinise urine:
potassium citrate 10 ml tds
sodium bicarbonate 1g tds
lemon juice in drinking water
• Consider in addition:
– Hypercalciuria: Thiazides
– Hyperuricosuria: Allopurinol
– Struvite: Rotating antibiotics
– Oxalate: Calcium supplements with meals, pyridoxine
– Cystine: Captopril, penicillamine, tiopronin
Summary
• CKD is a frequently-occurring comorbid condition and has wide-reaching clinical implications
• eGFR and ACR calculations - how to interpret and act on results
• Importance of medication management in CKD
• Anaemia and bone mineral disorder management in CKD
• Stone disease

Thank you!






![Renal Association Clinical Practice Guideline on Anaemia ... · Guidelines for Anaemia Management in Chronic Kidney Disease (CKD) 2006 [3]. These guidelines are an updated version](https://img.pdfslide.us/doc/110x75/5f78865f477b47546236ac28/renal-association-clinical-practice-guideline-on-anaemia-guidelines-for-anaemia.jpg)








![UnderstandingtheMechanismsofProteinuria ...downloads.hindawi.com/journals/ijn/2012/546039.pdf · proteinuria, an important marker of CKD that is associated withadverseoutcomes[5–8]](https://img.pdfslide.us/doc/110x75/5f0775a37e708231d41d16a7/understandingthemechanismsofproteinuria-proteinuria-an-important-marker-of.jpg)