Embed Size (px)
Citation preview

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 1/81

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 2/81
Goal - Objective
Educate nephrology
community aboutnew Pre-ESRD classes
and current pilotprograms in the
greater Houston area

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 3/81
t the end o! this presentationthe reader will be able toanswer• "hy #idney Education is important in $hronic#idney Disease or $#D
• "hat is a community-based education program
• "hat in!ormation is included in $#D educationprogram
• How does early $#D education program bene%tpatient outcomes and the physician&s practice
• "hat patients say about early $#D education
• How one can participate or set up a program

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 4/81
$hronic #idney Disease inthe 'S
• Over () *illion mericans have some degreeo! renal insu+ciency,. in / people
• () million others are at ris0
• Hypertension 1 Diabetes are the leadingcauses o! 0idney !ailure – (23 o! all mericans have hypertension
– .4 million mericans have diabetes
• 5oth are independent ris0 !actors !orcardiovascular disease

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 5/81
CKD EDUCATION
#nowledge is Power,!or us and ourpatients 6o educate patients is thehighest !orm o! care we can give 7t
empowers our patients to ma0e changesbig and small to improve their health and8uality o! li!e 7t empowers them withcontrol and in!ormation to !eel morerela9ed in an an9iety producing situationo! $#D transition to ESRD

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 6/81

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 7/81
Projection !or ESRDPopulation
'SRDS DR ())/
8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 8/81
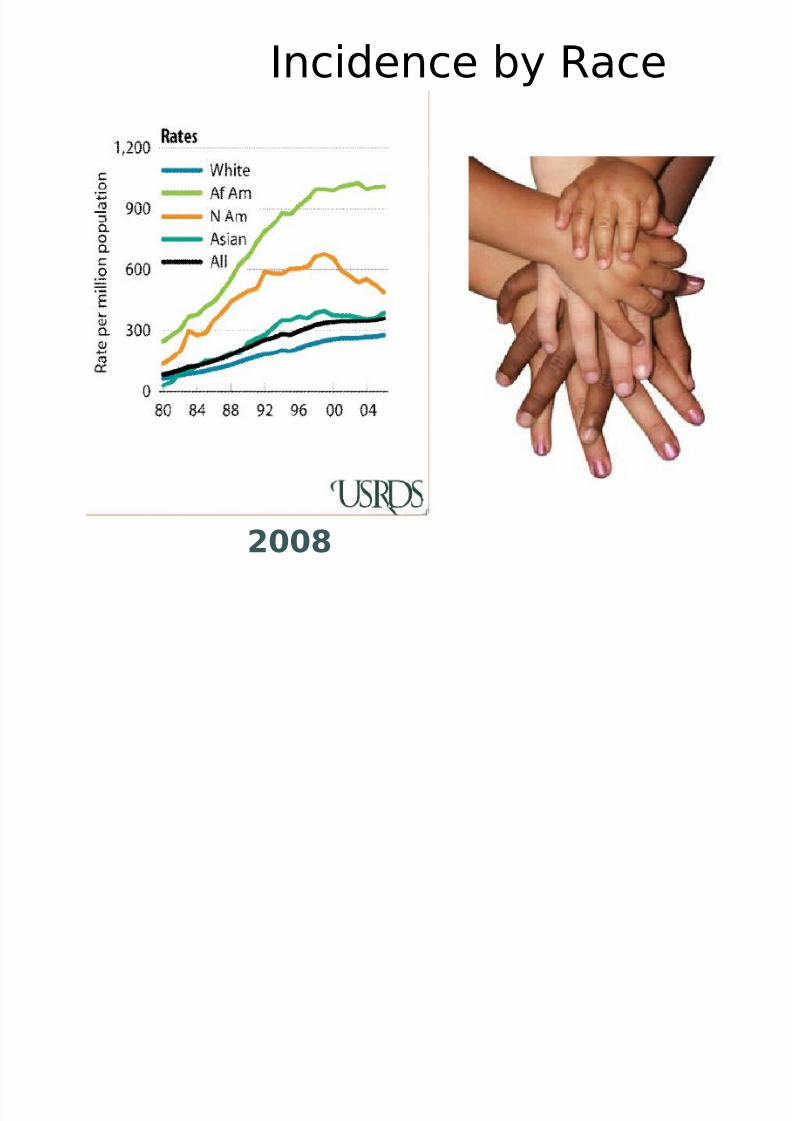
7ncidence by Race
2008

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 9/81
!rican mericans DevelopESRD at a :ounger ge

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 10/81
;ew $onditions o! $overage• ESRD *edicare Re!orm
– *edicare 7mprovements !or Patients and Providers ct o! ())/<HR 422. = *7PP>
– $#D education is recogni?ed by $*S – Reimbursement to nephrologists who provide chronic 0idney
disease education• Physicians *ust Educate $#D Patients on@
– #idney disease – ccess choices and issues – ESRD 6reatment options
• Physician per!ormance is based on – 7nAuen?e vaccine – 5lood Pressure control
– Re!erral !or an B %stula – Caboratory values = $a POE P6H Cipid pro%le
F5est physicians educate on much more

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 11/81
"hy Educate
"hy,Educate nd "hen 6he earlier the better,Starteducation by stage ( or 2 to have the biggest impact
One reason is we must 6he new c!c regulations arere8uiring pt education on 0idney disease treatmentoptions accesses 7 don&t thin0 this man had his ISave my
vesselsJ class in!ormation or he would not allow anyone tostic0 him up and down both arms nother reason@ 7t is smart use o! patients time and energy
Pts who use this in!ormation stay healthier longer and startdialysis in a better place both physically and mentally 7!they come to us healthier = they start healthier in ESRDwith better Outcomes more choices and better 8uality o!
li!e 6hey ma0e better choices@ more open to dialysis options
when starting dialysis not an emergency "hen pt educationis done ahead o! starting dialysis Home dialysis is chosenmore o!ten

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 12/81
"hat is community-basededucation
• Patient education program thatincludes@
– *ultidisciplinary coaching program
– Stage-speci%c education
– Easy education re!erral process
– Kollow-up with patients and physicians
– Sessions are !ree !or patients and guests

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 13/81
Find a comfortable location and time.

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 14/81
Cocation • 6he course does not need to beheld in *aui although it would benice church down the street
with a large con!erence roomwor0s %ne• E9perience with renal treatment
options training reveaed wewould gain more patients in anon-medical location
• nd our participants haverein!orced that concept
• 6he Houston $ommunity-based$#D program sponsored byDaBita 0nown as E*PO"ER hashad nearly 200pt!famil"!friend
• T#e patient feedbac$ i %er"poiti%e

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 15/81
"hat is $ommunity-5ased Education
*ultidisciplinary $oaching
*ultidisciplinarycoaching program
7n!orm patients about their
0idney health 7mprove 8uality o! li!e
Preserve renal !unction
Help patients identi!y thebest treatment choice !or
their li!estyle 6ools to organi?e and trac0their health care
Health Diary

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 16/81
*ultidisciplinary education
• Multidisciplinary coaching program can ma0e a diLerence
• nurse a dietitian and a social wor0er attend each class topresent the in!ormation and answer 8uestions
• 6he goal is help patients learn as much as they can about0idney health
• 7n!ormed patients are less an9ious and more e8uipped toeLectively !ollow their treatment plan preserve renal!unction and improve their 8uality o! li!e
• $#D education helps patients to identi!y the best treatmentchoice !or their li!estyle and rein!orce early %stulaplacement

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 17/81
5ene%ts o! early interventionand education• Delay or prevent the worsening o!
cardiovascular disease hypertension anddiabetes
• Delay or prevent the progression to chronic0idney disease
• 7mprove outcomes i! 0idney replacementtherapy ever becomes necessary
• Psychologically prepare one !or 0idney disease
• Reduce health care costs
• #eep people employed and out o! the hospital

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 18/81
6ools Provided
• n initial postcard and 8uarterly e-newsletters• Baluable tools !rom a well-regarded website
http@MMdavitacom – GKR calculator and trac0er
– N)) $#D recipes – DaBita Diet Helper – $#D videos – *ore
• 6he health diary is a tool given to each $#Dpatient and is designed to help organi?e andtrac0 their health care "e recommend thatpatients utili?e their Health Diary !or all providervisits to maintain continuity o! care

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 19/81
6OOCS KOR 5E66ER $RE

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 20/81
Health Diary
&eo'rce for t#e patient
• Patient in!ormation
• Healthcare phone numbers
• History and Physical
• *edication list
• Cab wor0
• Diabetes and Hypertension
• Glossary

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 21/81
6he health diary
• 5oth the patients and the doctors really li0e this diary• ;ot only is it a great resource but it gives the patients
a central location to 0eep their valuable healthin!ormation
• 6hey just as0 !or copies and %le it away• "hen they go to any health pro!essional they have it• Even with Hurricane 70e = pic0 it up and go• 6he doctors li0e it when they can see all the
in!ormation• 5est !rom patients is the 8uestions to as0 the doctor• Reminds them o! the importance o! the medication 5P
or lab results

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 22/81
"hat stage am 7
• Stage . = GKR ) ccMminM.Q2m(
– #idney Damage with normal or high GKR
• Stage ( = GKR = 4) to / ccMminM.Q2m(
– #idney Damage with mildly decreased GKR
• Stage 2 = GKR = 2) to N ccMminM.Q2m(
– *oderate decreased GKR
• Stage = GKR = .N to ( ccMminM.Q2m(
– Severely decreased GKR
• Stage N = GKR - .N ccMminM.Q2m(
– #idney !ailure
NKF/KDOQI Clinical Practice Guidelines for Chronic Kidney Disease
6his is the 8uestion most patients as0 "e review 0idney !unction and thestages o! 0idney disease "e review how this calculation wor0s and that is
based on both 0idneys "e discuss that the stages are generally progressivebut that patients can impact or slow the progression o! 0idney disease withdiet medications and healthy behaviors Patients need to be in!ormed and
as0 lots o! 8uestions o! their health care team and physicians
8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 23/81
Glomerular %ltration rate
• 6he serum creatinine by itsel! is a very POOR wayto assess 0idney disease
• 7t does not ta0e into account variation in musclemass nutritional status or body habitus
• GKR measures how well your 0idneys %lter wasteproducts which tells your doctor how well your0idneys are wor0ing
• 7n ())( the ;ational #idney Koundation beganrecommending the use o! GKR instead o! just
serum creatinine !or a more accuratemeasurement o! 0idney !unction
• GKR is calculated !rom your blood creatinine agerace and gender
From AAKP Healthline, 2009 – Stephen Z. Fadem

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 24/81
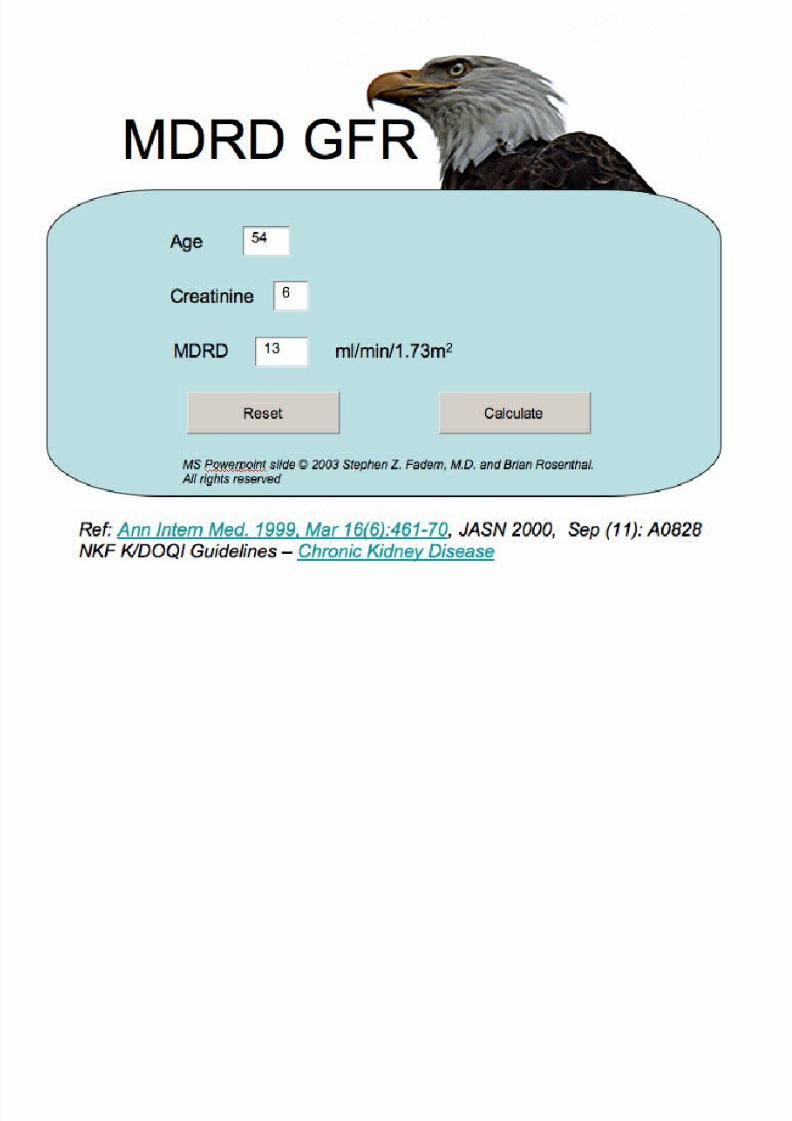
ssessment o! 0idney disease• Learning how well the kidney is functioning is important not only in screening and diagnosing chronic kidney disease (CKD), ut in following
its progress!
• "lthough there are #arious ways to do this, the simplest is the MD$D %&$ (glomerular filtration rate) which can e calculated using a
patient's age, race, gender and a laoratory test, known as the serum creatinine! he muscles are in a constant state of eing roken down
and eing repaired!• he creatinine is a yproduct of this reakdown and is generally stale in the lood from day to day!
• hile the serum creatinine is an indication of kidney function, its #ariation with muscle mass makes using the other factors mentioned
ao#e necessary!
• his e*uation was deri#ed from a large study pulished in +- that looked at how the modification of dietary protein would affect renal
disease – hence Modification of Diet in $enal Disease (MD$D)!
• his study re*uired a #ery accurate measurement of kidney function! he in#estigators noticed the mathematical relationships etween the
accurately measured %&$, age, race, creatinine and gender, and deri#ed the MD$D study e*uations still in use today!
• .t is also referred to as the e%&$! his %&$ is used to determine what stage of kidney disease one has, stages + and / eing #ery mild,
with %&$s ao#e 01 ml2min!
• hen the %&$ is greater than 01, other markers of kidney function such as an anormal urine or anormal ultrasound are necessary formaking the diagnosis! hen the %&$ is less than 01 for greater than three months, it indicates the presence of CKD!
• Once the GFR is calculated, and repeated in 3 months we also need to look at other markers of Kidney disease. While this is
necessary if the GFR is > 6, we also recommend testin! for markers stron!ly in e"eryone since it helps us re"erse the re"ersi#le
and !et a #etter dia!nosis. $arkers include the renal ultrasound and the urinalysis.
• "lthough the calculation in#ol#es some complicated math tricks, it was programmed for the .nternet shortly after it was disco#ered, and is
on the e at www!mdrd!com!
• he 3ational Kidney &oundation uses the same application! .t has also een programmed for handheld calculators!
• Many laoratories routinely report the MD$D %&$ along with the serum creatinine #alue! "s more and more laoratories standardi4e their
serum creatinine measurements to the 3ational .nstitute of 5tandards, the e*uation will change slightly, ut that change is also programmed
and a#ailale at www!mdrd!com!
• hen using the program, simply key in your serum creatinine, age, race and gender and your %&$ #alue will appear! he site will also
calculate your kidney disease stage! .t is important that you personally keep track of your serum creatinine and %&$ #alues!
Krom #P Healthline ()) = Stephen Kadem

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 25/81
:ou have heard about
$ystatin $• 5erum creatinine has a drawack in the measurement of glomerularfiltration rate (%&$) in that it may #ary according to muscle mass!
• Cystatin C is a +6 kilodalton protein that is filtered y the glomerulus andreasored and metaoli4ed y tuular cells! he amount that is e7cretedinto the urine is negligile! .ts production is #ery steady, and not dependenton muscle mass!
• .t has een proposed as an alternate marker for estimating %&$ y Dr! 8oeCoresh!
• "n ele#ated serum cystatin C le#el may indicate a worse cardio#ascular riskin patients with the metaolic syndrome! (+9-:016) !
• he literature is emerging, and showing that it has enefit as a marker! ;ereare two formulae that might e useful in demonstrating the relationshipsetween serum creatinine and serum cystatin C
• he serum cystatin C calculation is found at http<22touchcalc!com• %oe &oresh recommends a"era!in! the &ystatin & and the $'R' GFR

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 26/81
$linical evaluation o! patientsat increased ris0 !or $#D• All (atient
• *easurement o! blood pressure
• Serum creatinine to estimate GKR
• Protein to creatinine or albumin tocreatinine ratio in %rst * or randomuntimed spot urine specimen
• E9amination o! the urine sediment ordipstic0 !or red blood cells and whiteblood cells

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 27/81
Stage-Speci%c Education
6a0ing $ontrol o! #idney Disease
Civing with Stage 2 and Early Stage $#D
Kocus on preserving renal !unction
;ormal #idney !unctions M #idney Disease $ontrol o! co-morbidities M Diabetes M H6;
Diet and medication
Heart healthy behaviors
Preserving veins 7nsurance 8uestions
Tuestions to as0 physician

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 28/81
6reatment o! $#D
• 6reat the underlying disease
• 6reat associated problems
• Slowing the loss o! 0idney !unction
• Prevent heart disease
• Reduce complications
• Preparation !ordialysisMtransplantation
• #idney transplant or dialysis
NKF/KDOQI Clinical Practice Guidelines for Chronic Kidney Disease
8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 29/81

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 30/81
De%nition o! $hronic #idneyDisease• $hronic 0idney disease is de%ned as
either 0idney damage or GKR 4)ccMminM.Q2m( !or 2 months
• #idney damage is de%ned aspathologic abnormalities or mar0erso! damage including abnormalities in
blood or urine tests or imaging
NKF/KDOQI Clinical Practice Guidelines for Chronic Kidney Disease

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 31/81
$linical Practice Guidelines !or*anagement o! Hypertension in $#D
(ype of Kidney 'isease )lood *ressure(ar!et
+mm !-
*referred !entsfor &K', with or
withoutypertension
Other !ents to Reduce &/' Risk
and Reach )lood*ressure (ar!et
'ia#etic Kidney 'isease
0132
&4 inhi#itor or R)
'iuretic preferred,then )) or &&)
5ondia#etic Kidney'isease with rine (otal
*rotein7to7&reatinine
Ratio 8 m!2!
5ondia#etic Kidney
'isease with 9pot rine(otal *rotein7to7&reatinine
ratio 08 m!2! 5one preferred
'iuretic preferred,
then &4 inhi#itor,R), )) or &&)
Kidney 'isease in Kidney(ransplant Recipient
&&), diuretic, )),&4 inhi#itor, R)

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 32/81
$linical Practice Guidelines !or theDetection Evaluation and *anagement o!
$#D

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 33/81
)ta*e + and 2, (re%entin* eartDieae in CKD
• Traditional c%ri$ factor
• Nontraditional
ri$ factor

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 34/81
How $an :ou Protect :oursel! gainst Heart Diseasend High 5lood Pressure
• Get regular medical chec0ups
• $ontrol your blood pressure
• *onitor your blood pressure wee0ly
• $hec0 your cholesterol regularly = watch saturated !ats and!ructose
• "atch your diet - SC6• Regular doctor visits
• 5lood pressure - .2)M/)
• 7t ma0e ta0e several medications
• Don&t smo0e
• 7! you choose to drin0 do so in moderation• E9ercise regularly
• *anage stress

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 35/81

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 36/81
(raditional Risk Factors
• 5moking
• Cholesterol
• =esity• &amily ;istory
8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 37/81
5on (raditional Risk
Factors• .nflammation
• Mineral>one
disorder
• "nemia

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 38/81
$Es and R5s
• 6hese drugs are critical to care starting inStage . and (
• $ES and R5s have a compound eLect onbloc0ing the renin-angiotensin system
• 6he goal is to lower the blood pressure to.() mm Hg and to titrate proteinuria
• $ontraindications include allergy andbilateral renal artery stenosis
• Potassium levels should be monitoredclosely when patients are on $ES or R5S• <5eta bloc0ers ;S7DS $ES and R5S can
raise serum potassium>

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 39/81
5lood Pressure 7s Poorly $ontrolled inPatients "ith $#D

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 40/81
:nflammation
• "ssociated with CKD
• "therosclerosis
• ?ascular calcification
• 5tatins not helpful in CKD:
• C$@ not diagnostic
• M."

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 41/81
A7ercise "nd Kidney Care
• alk to your doctor aout starting ane7ercise program that's right for you!
• A7ercise can help you impro#e physicalfunctioning and emotional well>eing,
increase physical stamina, impro#e loodpressure and reduce the risk of heartdisease, lower cholesterol, help you sleepetter and control ody weight!
• .ncorporating consistent aeroic e7ercise,e#en taking a /1>minute walk, can help
especially if your CKD is a result ofhypertension or diaetes!

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 42/81
"atch meds and therapies
• void *et!ormin in Stage 2 and beyond
• $ontrast media =
– ;ephrogenic sclerosing %brosis may occur
with an *R7 due to galadinium contrast = soprocedure should be done without thiscontrast agent
– 7odine can be nephroto9ic = and patients
should be well hydrated pre procedure• ;S7DS should not be given to 0idney
patients
Here are some examples:

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 43/81
'iet• 5odium > +11 mmoles
• Lipids > pre dialysis
• Carohydrates > Diaetes
• @roteins > MD$D rial
• @otassium > watch ecause of "$Bs
and "CA inhiitors
8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 44/81
3utritional ips &or ;ealthy Kidneys
• .n order to help maintain healthy kidneys it is important to eat properly
• Keep track of daily calories
• Limit total fat
• atch high fructose corn syrup
• atch e7cess proteins and phosphorus > Monitor the amount of proteineaten
• ou may need to watch potassium > Learn aout potassium
• our dietitian can help you with recipes that fit your needs• Control salt intake• ake care of your ones – e7ercise and take #itamin D• Be sure to get enough iron• atch fluid intake• nderstand your nutritional plan

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 45/81
Stage 2 = *edical Kocus
• CKD /D etabolic bonedieae
• cidosis - 5icarbonate
• nemia = Erythropoietin
$lass rein!orces
bone and
heart healthy diet
8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 46/81
)ta*e 1
• a. Cardio%ac'lar ri$ and t#erap" ta"t#e co're
• b. (reparation,
+. Anemia 2. Acidoi 1. /lood pre're!ACE and A&/) . In3ammation 4. Diet 5. odalit" c#oice 6. Acce preparation
• c. odalitie of t#erap"
8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 47/81
(reparation
• Anemia
• Acidoi
• /lood pre're - ACE) 7 A&/)
• In3ammation
• Diet
• odalit" C#oice
• Acce (reparation

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 48/81
Anemia in CKD
• nemia management with EPO since .)s -
• #eep Hct ( – N Eng J Med 339:584-90, 1998
• #eep hgb .) - .( – $HO7R
• N Eng J Med 355:2071-2084, 2006.
• 23 worse when hgb target is .2N than ..(
– $RE6E
• N Eng J Med 355:2084-2098, 2006• ((3 worse when hgb is .2-.N than .)N-..N
• $hec0 7ron levels and correct %rst
• EPO can be given in the o+ce - monitor bloodwor0

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 49/81
EPOEPO
R5$R5$R5$ PRE$'RSOR

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 50/81
Acidoi
• 7ncreased protein catabolism o! aminoacids
• 7nhibition o! protein synthesis can cause a
low albumin• ccelerates renal osteodystrophy
• *odulates vitamin D and parathyroidhormone levels
• Evo0es insulin resistance

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 51/81
lbumin Synthesis
• $hronic acidosis impairs albuminsynthesis and causes negative
nitrogen balance – U$7 N@2N-N .N• lbumin - major mar0er !or
nutrition
• Cow serum albumin - ris0 !actor!or poor dialysis outcome• 7t is advisable not to restrict
dietary protein once the serumalbumin level starts to !all
* b li id iREGE;ER6ES

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 52/81
*etabolic cidosis
6he 0idney has a major responsibilityto eliminate and buLer acids 7n renal!ailure these acids accumulate
"hen the clearance !alls below (N ccper minute the accumulated acidscause loss o! appetite Protein storesand albumin !all and muscle isbro0en down and used as a nutrient
7t is not clear whether correction o!acidosis with bicarbonate solution ishelp!ul but there is consensus that
as renal !unction deteriorates andalbumin !alls the diet needs to beadjusted and i! that does not wor0dialysis is needed to correct theacidosis
REGE;ER6ES
5'KKER
SE$RE6ES
$7DS

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 53/81
5ene%ts o! anemiacorrection• 7mproved wor0 and aerobic capacity
• Reduced cardiovascularcomplications
• Reduced hospitali?ations• Decreased mortality
• 7mproved 8uality o! li!e
• 7mproved cognition
• 7mproved se9ual !unction/earab. Am J Kidney Dis. 200015 9'ppl 1:,)+1.
Fin$. Am J Kidney Dis. 200+16,18.
Ka';. Am J Kidney Dis. 2000159'ppl 1:,)1<.

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 54/81
Bascular $alci%cation
#idney damage causes decreasedphosphorus e9cretion 6his stimulatesphosphotonins to increase phosphoruse9cretion
Phosphotonins and 0idney damage decreasethe activation o! vitamin D
6his wea0ens muscles decreasing bonestrength
6his decreases the calcium depositing inbone and along with phosphorus = leads tochanges in blood vessel cells
$alcium deposits in blood vessels 7nAammation and Hyperlipidemia <metabolic
syndrome> ma0e this worse High !ructose corn syrup ma0es metabolic
syndrome wor0s
D7E6 7S 7*POR6;6VVV

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 55/81
$hronic #idney Disease nd *ineral 5one Disorder
• 6oo much phosphorus and
• Damaged 0idneys do not produce enoughvitamin D
• Bitamin D helps maintain calcium levels which0eep bones strong
• $alcium may build up in blood vessels with
$#D• "ithout enough vitamin D you are more li0elyto have wea0 bones that may brea0 easily

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 56/81
How to Protect gainst$#D *5D
• Bitamin D level• Parathyroid hormone level• Ergocalci!erol over the counter• Bitamin D is probably !or everyone =
regargless o! stage• t later stages you might need an
active !orm o! vitamin D
• E9ercise and diet management• 6he doctor may want to chec0 !or
vascular calci%cation

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 57/81
"hat ELect $an $hronic #idney DiseaseHave On 6he 5ody
• Heart disease
• High blood pressure
• Bitamin D de%ciency - bone andmineral disorder
• nemia
• *alnutrition and low serum albumin• cid buildup

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 58/81
&ecommendation
7nAammation - Dental hygiene %ber in earlystages e9ercise 0eep trim 7! we develop astomach illness li0e helicobacter get it
treated #eep toenails trim therosclerosis - $hec0 the serum
cholesterol CDC BCDC HDC - use diete9ercise medications <statins usually> to
0eep these numbers in the proper range
PHOSPHOR'S ;D B76*7;

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 59/81
PHOSPHOR'S ;D B76*7;D
$#D-*5D - void e9cessphosphorus in the dietand have vitamin Dlevels chec0ed 7! lowstart on ergocalci!erol or
cholecalci!erol Cater anactive vitamin D li0ecalcitriol do9ercalci!erolor paricalcitol will beneeded
Bascular calci%cation - sthe disease progressesrestrict phosphorus anduse a phosphate binder
8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 60/81
Stage-Speci%c EducationMakin Health! "hoi#esPreparing !or dialysis !or Stages and N $#D
– Symptoms o! 'remia
– $ontrolled dialysis start
– $#D and dialysis diet
– $ontrol o! co-morbidities = D*MH6;
– *edications = $all your ;ephrologist
– ccess = ;o to catheters :es to %stulas = Bein *ap – ll treatment choices
– 7nsurance issues
St d N $#D $l

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 61/81
Stage and N $#D $lass
• *a0ing Healthy $hoices
• Preparing !or dialysis in later Stage to early Stage N $hronic #idney Disease• 6his is the longer class due to the number o! 8uestions we have !rom the patients and !amily members• "e !ocus on maintaining the patients 0idney health as long as possible but also educate the patients on the symptoms o! uremia
and the transition process to ESRD• $lass detail@
– "hat 0idneys do – "hat causes 0idney disease = Symptoms o! 'remia = ;ausea and vomiting 6aste changes Swelling SO5 7tching Cac0 o! concentration
and memory issues – Preparing !or dialysis = Preventing the I$rash and 5urnJ admission to dialysis ;o one 0nows the e9act moment but wor0ing with your
doctor will help to get the time right !or you "e can delay but not !orever without it damaging your health due to malnutrition or heart orstro0e
– *anaging your health through diet Review diet changes at the end o! stage especially related to low protein potassium phosphorussalt and Auid "hat the stage N diet is !or the diLerent treatment modalities *ost o! the pts enjoy 0nowing their diet will get more proteinon ESRD than in stage
– $ontrol o! D* and H6; = Protect your heart and vasculature as well as your 0idney !unction never stops Dialysis patients do not die !romdialysis 6hey die !rom in!ection and $ardiacMBascular disease due to D* and H6; 5P and 5S = Heart healthy behaviors Diet E9erciseStop smo0ing "e all 0now it ,
– $ommon medicines !or people with 0idney disease Phosphorus binders Bitamin D Renal Bitamins 5icarbonate EPO Stay oL magnesiumaluminum products $all doctor !or any new meds prescribed or O6$ or !rom other doctors Stay away !rom 7B dye contrast
– ccess in!ormation and planning early with stage = ;o to catheters = yes to %stula&s Cots o! in!o about best choice and get it nowKistulas may ta0e months to mature 5e sure to get vein mapping done prior to surgery !or improved success with %stulas :ou don&t ta0ea trip without a map = you don&t want surgery without a map either $B$ catheters have more in!ections clotting hospitali?ations anddeaths 5e sure to remove $B$ catheters as soon as possible Getting a $B$ catheter may be necessary !or a short while !or initial dialysisbut getting your %stula now will shorten that time and may save your li!e
– n in-depth loo0 at all o! treatment choices@• Peritoneal Dialysis <PD>• Home Hemodialysis <HHD>• Hemodialysis <HD>
• ;octurnal hemodialysis• Sel!-$are hemodialysis
– 6ransplant – $onservative treatment
• $hoosing the right treatment !or your li!estyle especially i! you want to continue wor0ing or have active li!e
• 'nderstanding 7nsurance= state and !ederal insurances and when to apply !or secondary insurance especially i! want transplant dueto medication cost "e have saved patients money by assisting with insurance 8uestions

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 62/81
odalit" C#oice
• PD - Q3 o! population – Pre!erence values higher than !or HD Q-4
– Physicians in practice .. years along more li0ely to re!erto PD
– *ore li0ely recommended to men people with residual
!unction with weight less than ()) lb and the absence o!diabetes
• Hong #ong – Hal! the mortality
– N staL !or 2)) patients
– Cess mortality because residual !unction preservation
– Coss o! residual !unction is a cardiovascular ris0 !actor
8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 63/81
Stage = *edical !ocus
• *odalities = 7ncenter and Home Dialysis 6ransplant or $onservative therapy
• Re!erral !or access = Bein mapping and
surgery• Serum lbumin = Prevent malnutrition
• $ontinue other therapies = $E or R5
• nemia = Erythropoietin therapy
St N b t t t

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 64/81
Stage N = but not yet ondialysis• One-on-one modality options
– $onservative treatment = *edical dietmanagement Hospice ssistance
– 6ransplant = re!er early
– Home therapies <Peritoneal Home Hemodialysis>
– 7n-center therapies <7$HD ;octurnal Sel!-$are>
– Physicians !ocus - 6herapy choiceMtransition
PD R ! E l

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 65/81
PD Re!erences = Earlyre!erral helps
1. Bass EB, Wills S, Fink NE, et al: How strong are patients' preferences
in choices between dialsis !odalities and doses" #! $ %idne &is
:()*+-*, --
. Winkel!aer W/, 0lnn $, 2e3in , et al: 2ate referral and !odalit
choice in end+stage renal disease. %idne 4nt (-:1*+1**, --1
5. 2in /+2, /h6ang F+, W6 /+F, et al: Earl referral as an independent
predictor of clinical o6tco!e in end+stage renal disease on he!odialsis
and contin6o6s a!b6lator peritoneal dialsis. en Fail (:*51+*5, --
. 7ha!er 8, Hwang W, Fink NE, et al: 9S nephrologists'
reco!!endation of dialsis !odalit: res6lts of a national s6r3e. #! $
%idne &is 5(:11**+11(*, ---
*. Wang #+8, Wang 8, Woo $, et al: 4nfla!!ation, resid6al kidne
f6nction, and cardiac hpertroph are interrelated and co!bine ad3ersel
to enhance !ortalit and cardio3asc6lar death risk of peritoneal dialsis
patients. $ #! Soc Nephrol 1*:1;(+1), --

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 66/81
Home Hemodialysis
• Short - ( hour per day W 4 days perwee0
• Cong - Overnight W 4
• Prospective patients – Bisit during $#D
– Cogistics location and type o!e8uipment
• ;9Stage - Q) pounds
• ())/#Xhome <5aby#> – *ay need plumbing and electrical
• ;eed ample storage
• ;eed !or vascular access
• ;eed a partner
; t l H

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 67/81
;octurnal HomeHemodialysis
• *ay be able to stopbinders
• *ay need supplementalphosphorus
• Cess hypertensives• Cess epo
• Cess Auid restriction• ;octurnal in-center !orselect patients
A ( ti

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 68/81
Acce (reparation
• Arterio%eno'=t'la - +<55
• >at man" "ear – ?ein arteriali;e
– Arterie e@pand – Capillarie and
lar*er %eelaborb #oc$
– raft tranmit#oc$ and lat onl"aro'nd +8 mont#

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 69/81

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 70/81
Easy Education Re!erralProcessEasy education re!erral process
– 7denti!y patient
– 7n!orm patient
– Order education
– Re!er 1 Ka9
Empower 6eam – $all patient
– Schedule class

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 71/81
How the program wor0s
• 6he $#D community-based process begins and ends with the o+ce team
• Kirst the o+ce will need to identi!y patients who are Stage 2 and N that need$#D education
• ;e9t re!er those patients !or education by completing and !a9ing the re!erral!orm <show !orm> 6he patients are noti%ed enrolled in a class and called to
remind them o! class appro9imately . wee0 prior 6he day o! class patients willcomplete an attendance !orm and evaluate the class 6his data will be recordedat the call center
• 6he recorded data allows the educators to provide the o+ce with in!ormationaLecting patients and practice "e can e9tract the number o! your patientswho have attended a class which class they have attended their stage o! $#Daccess preparation !or dialysis type o! access modality choice just to name a
!ew o! the components
• 'ltimately the goal is help patients to ta0e control o! their $#D and i! dialysisis needed that they begin dialysis healthier and prepared

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 72/81
$ommunication is crucial
• ;ephrologist receives a letter !rom $#Deducator
– 7ndicates what class patient attended
– High lights Ino showsJ
– Cists concerns andMor modality interests i!e9pressed
• $#D patient receives a phone call !rom $#Deducator 1 education materials
– ssess !or additional teaching
– nswer 8uestions and provide resources
– 7nitial postcard mailing 1 8uarterly e-newsletters

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 73/81
Kollow-up
• "e will provide a !ollow up letter !or every patient that iseducated indicating which class the patient attendedYwhat material was coveredY any concerns theye9pressed and !or late stage patients their modalityinterest
• "e maintain telephonic contact with your patientsre!erred and educated to develop an understanding o!their education needs and to help support them throughadditional classes and guidance to resources spreviously mentioned an initial postcard and 8uarterly
e-newsletter are delivered to introduce the valuabletools that a well 0nown website DaBitacom oLers = GKRcalculator and trac0er over N)) $#D recipies DaBitaDiet Helper $#D videos and more
• ll medical 8uestions will be re!erred the physician

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 74/81
Summary o! Stages
• Pre-ESRD patient education does better when re!erred early to an educationprogram n educated patient will adhere better to the therapy that slowsprogression o! disease
• 7n the early stages . and ( = it is important to control !or diabetes and bloodpressure Generally an $E or an R5 is recommended – Bitamin D management should start early in the course o! disease – Some recommend restricting the use o! process !oods early – 7n addition to diet and blood pressure control with an $E or R5 control o! glucose is
valuable in diabetics• 5y Stage 2 patients are starting to mani!est signs o! anemia metabolic acidosis
and early metabolic bone disease – 6hey need to have laboratory studies = $a PO P6H lipid pro%le
• 5y stage the serum phosphorus is elevated Bitamin D analogs may benecessary Phosphorus control can be done with diet but most li0ely at thisstage will re8uire a binder – Patients have other choices beside in center hemodialyssi 7n stage it is important to
discuss options such as home hemodialysis and home peritoneal dialysis Patients whohave been educated are more li0ely to choose these modalities and are more satis%edwith them
– 6he patient should be evaluated early !or a permanent vascular access anddepending upon the modality chosen a %stula or peritoneal dialysis access placed
• Pre-ESRD classes lead to a smoother transition into a dialysis <stage N> regimen
8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 75/81
$#D Education 5ene%ts
Patients
Physician
6a9payers
Keel more engaged and in-control
Slow the progression o! renal disease
Healthier on Kirst Date o! Dialysis
Kree education to patients andcommunity
Physician able to compliment owneducation
Saves physician time resources andmoney Patients learn o! laws that protectthem
Patients stay employed andinsured
Decrease burden on *edicare

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 76/81
"in = "in - "in
• $#D Education is a "in-"in-"in program 7t isprovided to patients and the community at no cost orobligation
• Patients who attend are empowered to ta0e control o!
their 0idney health 6hey are provided with the toolsthey need to preserve renal !unction
• Physicians are able to compliment their own e9cellenteducation saving them time resources and money
• Kinally by helping patient to understand the laws thatprotect them we can help 0eep patients employedand maintain their insurance thus decreasing theburden on *edicare

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 77/81
How Do :ou Participate
• Establish $#D Education as part o! yourpractice
• Protocol@ Educate all patients Stages 2 and N• Process@
– 7denti!y eligible patient during o+ce visit – Patient communication <discussion and Ayer> – $linician orders education need using@
• Stic0y note• Re!erral !orm
– O+ce staL completes and !a9es re!erral !orm – $#D education team contacts patient and
schedules class
How to wor0 with a

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 78/81
How to wor0 with aphysician o+ce
• Every physician practice operates diLerently 6he 2biggest things to wal0 away !rom the meeting with are@ – 6he physicians commitment to re!er their $#D pts <get
granular as to are they willing to send Stage 2 pts as well as and N or just and N which is %ne too>
– solid detailed process in writing on how the doctor is going
to noti!y the administrative team o! the order !or educationand how the administrative team is going to send the !a9re!erral 7! the Physicians are willing to set a ZprotocolZ orZstanding orderZ that states the admin staL is to re!er all$#D pts <or all Stage MN pts> that is great because it ta0esthe step o! the physicians remembering to re!er !oreducation out o! the mi9
• n agreement on how o!ten you and the administrativestaL will touch base to ma0e sure everything is good
E l $#D Ed ti 5 %t P ti t&
8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 79/81
Early $#D Education 5ene%t Patient&s
"hat Houston $#D patients say about $#DEducation@
– I7 wish 7 had this in!ormation soonerJ
– I7 will really study my lab values and chec0 my dietJ
– I7 will tal0 to my doctor about my ;S7D&s anddecongestantsJ
– I6he health diary is e9cellent 7 really li0e the glossaryJ
– Is a !amily member 7 thin0 my !ather <patient> will!eel more com!ortable about the possibility o! dialysisJ
Success Stories,
S S i

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 80/81
Success Stories
• Patients need in!ormation and change canhappen – Pt went !rom stage to stage 2 and than0ed us !or
the class,
• O+ce staL tell o! a pt they were dreading to tellabout time to start dialysis – Pt said I7t&s O# 7 0now about itJ 6he o+ce nurse
was ama?ed
• ccess placements be!ore starting dialysis – s they should be
• 7nsurances saved or supplemental insuranceobtained be!ore ESRD

8/18/2019 Ckd / gagal ginjal kronik
http://slidepdf.com/reader/full/ckd-gagal-ginjal-kronik 81/81





























