-
Part 7: The Era of Reperfusion: Section 2: Acute Stroke
Print ISSN: 0009-7322. Online ISSN: 1524-4539 Copyright 2000
American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville
Avenue, Dallas, TX 75231Circulation doi:
10.1161/01.CIR.102.suppl_1.I-204
2000;102:I-204-I-216Circulation.
http://circ.ahajournals.org/content/102/suppl_1/I-204World Wide
Web at:
The online version of this article, along with updated
information and services, is located on the
http://circ.ahajournals.org//subscriptions/is online at:
Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be
found online at: Reprints:
document. Permissions and Rights Question and Answer this
process is available in theclick Request Permissions in the middle
column of the Web page under Services. Further information
aboutOffice. Once the online version of the published article for
which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright
Clearance Center, not the EditorialCirculationin Requests for
permissions to reproduce figures, tables, or portions of articles
originally publishedPermissions:
by guest on March 5, 2014http://circ.ahajournals.org/Downloaded
from by guest on March 5,
2014http://circ.ahajournals.org/Downloaded from
-
Part 7: The Era of ReperfusionSection 2: Acute Stroke
Major Guidelines Changesc Intravenous administration of
tissue-type plasminogen ac-
tivator (tPA) for patients with acute ischemic stroke and
nocontraindications is recommended:Within 3 hours of onset of
stroke symptoms (Class I)Between 3 and 6 hours of onset of stroke
symptoms
(Class Indeterminate)c Intra-arterial fibrinolysis within 3 to 6
hours after the onset
of symptoms may be beneficial in patients with occlusionof the
middle cerebral artery (Class IIb).
IntroductionA stroke is a disruption in blood supply to a region
of thebrain that causes neurological impairment. Stroke is
rankedamong the top 3 leading causes of death in most countries
andis the leading cause of brain injury in adults.
Internationallymillions of people have a new or recurrent stroke
each year,and nearly a quarter of these people die.1 The stroke
rate isdeclining in most western and northern European
countries,but there is a large and increasing rate in Russia,
possiblyattributable to a higher prevalence of hypertension.2
Althoughstroke mortality and attack rates are falling in many
countries,the gain achieved by prevention has been counterbalanced
bya growth in the aging population (more people at risk).3,4
Strokes can be classified into 2 major categories, ischemicand
hemorrhagic. Approximately 85% of all strokes areischemic.5
Ischemic strokes occur primarily because a bloodvessel supplying
the brain is occluded, usually by a thrombusor embolism.
Hemorrhagic strokes are the result of rupture ofa cerebral artery.
Associated spasm of the artery and variousdegrees of bleeding
occur. Until recently, care of the strokepatient was largely
supportive, focusing on prevention andtreatment of respiratory and
cardiovascular complications. Nospecific therapy was available to
alter the course and extent ofthe evolving stroke. Therefore,
little emphasis or need wasplaced on rapid transport or
intervention.
Fibrinolytic therapy now offers healthcare providers
anopportunity to possibly limit the extent of neurologicaldamage
and to improve outcome in stroke patients. Atime-dependent benefit
similar to that observed in patientswith acute myocardial
infarction (AMI) is possible. The timeavailable for treatment,
however, is limited.6 Early recogni-tion of stroke and rapid
triage, evaluation in the EmergencyDepartment (ED), and definitive
management are essential.79
Early RecognitionEarly treatment of stroke depends strongly on
recognition ofthe event by the patient, family members, or
bystanders.10Common symptoms of transient ischemic attack (TIA)
andstroke are described in Table 1.
Role of EMS in Stroke CareRapid activation of the EMS system is
essential to optimizecare of the patient with stroke. Stroke
patients who use theEMS system arrive at the hospital faster than
those who donot, a major advantage for time-critical treatment.1118
Fur-thermore, emergency dispatchers can send the
appropriateemergency team with a priority dispatch response and
pro-vide instructions for care of the patient until arrival of
EMSpersonnel.1921 EMS personnel can then quickly transport
thepatient to a stroke center and notify the facility before
arrivalto ensure rapid hospital-based evaluation and
treatment.Initial contact of the family physician and transport of
thepatient by car have been shown to delay patient arrival
andinitial evaluation at the hospital. Such delays may render
thepatient ineligible for fibrinolytic therapy.11,15,19
Only half of stroke patients currently use the EMS systemfor
transport to the hospital.11,22 Strokes that occur when thepatient
is alone or sleeping may further delay prompt recog-nition and
action.23 Eighty-five percent of strokes occur athome.22 As a
result, public education programs have appro-priately focused their
efforts on persons at risk for stroke andtheir friends and family
members. Public education hasreduced the time to arrival at the
ED.8,12
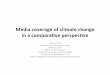
The 7 Ds of Stroke ManagementKey points in the management of
stroke can be remembered byusing the mnemonic of the 7 Ds:
Detection, Dispatch, Delivery,Door, Data, Decision, and Drug (see
algorithm for suspectedstroke).24 Delay may occur at any point, so
the response at eachpoint must be skilled and efficient. The first
3 Ds (detection,dispatch, and delivery) are the responsibility of
BLS providers inthe community, including the lay public and EMS
responders.Detection occurs when a patient, family member, or
bystanderrecognizes the signs and symptoms of a stroke or TIA
andactivates the EMS system (by phoning 911 or other
emergencyresponse number). EMS dispatchers must prioritize the call
for asuspected stroke patient as they would for a victim of AMI
orserious trauma and dispatch the appropriate EMS team with
hightransport priority. EMS providers must respond rapidly,
confirmthe signs and symptoms of stroke, and transport the
patient(delivery) to a stroke center (a hospital that can provide
fibrino-
Circulation. 2000;102(suppl I):I-204I-216. 2000 American Heart
Association, Inc.Circulation is available at
http://www.circulationaha.org
I-204 by guest on March 5,
2014http://circ.ahajournals.org/Downloaded from
-
lytic therapy within 1 hour after arrival at the ED door).
Theremaining 3 Ds are performed in the hospital: data
includesobtaining a computed tomography (CT) scan, decision is
madein identifying candidates eligible for fibrinolytic therapy,
anddrug includes treating eligible patients with fibrinolytic
therapy.
Airway and VentilationAirway obstruction may be a major problem
in acute stroke,particularly if the patient loses consciousness.
Hypoxia andhypercarbia can occur as the result of inadequate
ventilation,contributing to cardiac and respiratory instability.
Aspiration
Figure. Algorithm for suspected stroke.
Part 7: Era of Reperfusion: Acute Stroke I-205
by guest on March 5, 2014http://circ.ahajournals.org/Downloaded
from
-
of secretions or gastric contents is a serious
complicationassociated with considerable morbidity and mortality.
EMSproviders must ensure that the patient has an adequate
airway.Assisted ventilation or tracheal intubation may be
required.
Vital SignsCheck vital signs (pulse, respirations, blood
pressure, andtemperature) frequently to detect abnormalities and
changes.Abnormal respirations are particularly prevalent in
comatosestroke patients and usually reflect serious brain
dysfunction.Hypertension often occurs after a stroke and may be
causedby underlying hypertension, a stress reaction to the
neurolog-ical event, or a physiological response to decreased
brainperfusion. Blood pressure often returns to normal
withoutantihypertensive treatment.25
A variety of cardiovascular problems may be present in
thepatient with stroke. Cardiac arrhythmias may contribute to
thecerebral thromboembolism, or they may be the consequenceof brain
injury. In particular, episodes of paroxysmal atrialfibrillation,
severe symptomatic bradycardia, or high-degreeatrioventricular
block may point to cardiac rhythm distur-bances as causative or
contributory. In the elderly and inpatients with diabetes, AMI with
atypical or undetectablesymptoms can occur.26,27 Obtain a 12-lead
ECG and attemptto rule out left ventricular mural emboli if an
acute or recentMI is suspected. Life-threatening cardiac
arrhythmias are apotential early complication of stroke,
particularly of intra-cranial hemorrhages.2830 Continuous
monitoring of cardiacrhythm and systemic perfusion is part of the
early manage-ment of a stroke patient.
General Medical AssessmentExamine the patient for evidence of
injury to the head orneck, because trauma is an important
consideration in thedifferential diagnosis of stroke. Blood
pressure in both upperextremities should be measured. A difference
of .10 mm Hgshould raise consideration of aortic dissection and
compro-mise of brain blood supply. Perform diagnostic studies
suchas CT or angiography if indicated by history or
clinicalfindings. Cardiac murmur, arterial bruit, absent pulse,
orother abnormalities should be sought during the cardiovascu-
lar examination. The presence of an ocular hemorrhage mayallow
early identification of intracranial bleeding.
Brief Emergency Neurological EvaluationThe emergency
neurological evaluation for stroke shouldinclude 6 key
elements:
c Stroke screen or scalec Time of onset of stroke signsc Level
of consciousnessc Type of stroke (hemorrhagic versus
nonhemorrhagic)c Location of stroke (carotid versus
vertebrobasilar)c Severity of stroke
Stroke Screen or ScalePerforming an extensive neurological
examination outsidethe hospital is impractical because it delays
transport of thepatient to the ED. To conduct an out-of-hospital
neurologicalevaluation, use a validated tool such as the
CincinnatiPrehospital Stroke Scale (Table 2) or the Los
AngelesPrehospital Stroke Screen (LAPSS)16 (Table 3).31,32
TheCincinnati scale is used to elicit any of the 3 major
physicalfindings suggestive of stroke: facial droop, arm drift,
andabnormal speech.31 LAPSS requires the examiner to rule outother
causes of altered level of consciousness (eg, history ofseizures or
severe hyperglycemia or hypoglycemia) and thenidentify asymmetry
(right versus left) in facial smile/grimace,grip, or arm strength.
Asymmetry in any category indicates apossible stroke18,32 These two
scales are sensitive and specificin identifying stroke
patients.18,31,32 Either evaluation can beperformed quickly.
Ambulance personnel can identify stroke patients withreasonable
sensitivity and specificity. Once a stroke is sus-pected, minimize
time in the field and immediately transportthe patient to a stroke
center.
Clinical signs and symptoms of acute stroke often fluctu-ate.
Deterioration or improvement can be detected by fre-quent and
repeated focal neurological examinations. Re-peated examinations
need not be exhaustive. The GlasgowComa Scale tests eye opening,
verbal response, and motor
TABLE 1. Common Signs and Symptoms of TransientIschemic Attack
(TIA) and Stroke
Unilateral paralysisWeakness, clumsiness, or heaviness, usually
involving1 side of the body
Unilateral numbnessSensory loss, tingling, or abnormal
sensation, usuallyinvolving 1 side of the body
Language disturbanceTrouble understanding or speaking (aphasia)
orslurred speech (dysarthria)
Monocular blindnessPainless visual loss in one eye, often
described as acurtain dropping
VertigoSense of spinning or whirling that persists at rest.
Isolated vertigois also a common symptom of many nonvascular
diseases; therefore, atleast one other symptom of TIA or stroke
should also be present.
AtaxiaPoor balance, stumbling gait, staggering, incoordination
of one sideof the body
TABLE 2. Cincinnati Prehospital Stroke Scale
Try to elicit one of the following signs (abnormality in any one
is stronglysuggestive of stroke):
Facial droop (have patient show teeth or smile):
Normal: both sides of face move equally well
Abnormal: one side of face does not move as well as the other
side
Arm drift (have patient close eyes and hold both arms straight
out for 10seconds):
Normal: both arms move the same or both arms do not move at
all(other findings, such as pronator grip, may be helpful)
Abnormal: one arm does not move or one arm drifts down
Abnormal speech (have the patient say you cant teach an old dog
newtricks):
Normal: patient uses correct words with no slurring
Abnormal: patient slurs words, uses the wrong words, or is
unable tospeak
From Reference 31.
I-206 Circulation August 22, 2000
by guest on March 5, 2014http://circ.ahajournals.org/Downloaded
from
-
response.33 It is useful for assessing the initial severity
ofneurological injury in patients with altered
consciousness,especially in cases of injury caused by
intracerebralhemorrhage.
Obtain the following information en route to or at thehospital.
(Do not delay transport to complete a more detailedevaluation.
Rapid transport is essential.)Time of Onset of SymptomsIf stroke
symptoms started within 6 hours of the arrival ofEMS personnel,
immediately notify the receiving hospital.Prearrival notification
of the receiving hospital shortens thetime to definitive
hospital-based evaluation and intervention.Provide results of the
stroke scale or screen, the GlasgowComa Scale score, and the
estimated time of symptom onsetin addition to standard information.
This allows the ED orCasualty Service time to prepare and
coordinate the patientstime-sensitive therapy. The receiving
hospital should have awritten plan to begin therapy as quickly as
possible.
Level of ConsciousnessDetermining the stroke patients level of
consciousness iscrucial. Depressed consciousness within hours of
the onset ofsymptoms implies severe brain injury with increased
intra-cranial pressure (ICP), usually due to an intracerebral
orsubarachnoid hemorrhage. Coma, the lack of any purposefulresponse
to external stimuli, is the result of damage to bothcerebral
hemispheres or the brain stem. Coma usually impliesmassive
hemorrhage, occlusion of the basilar artery, orcardiac arrest with
global brain ischemia. Massive ischemicstroke with cerebral edema
may cause coma but is rare. Donot overlook concurrent metabolic
problems. Consider drugoverdose, sepsis, or severe metabolic
abnormalities.
Type of Stroke (Ischemic Versus Hemorrhagic)The history and
physical findings of hemorrhagic and ische-mic stroke overlap (see
Table 4). Do not depend solely on
clinical presentation for diagnosis. In most cases,
noncontrastCT is the definitive test for differentiating ischemic
andhemorrhagic stroke. (CT is discussed in Emergency Diag-nostic
Studies.)Location of StrokeHigher cortical, language, visual,
cranial nerve, motor, andsensory functions should be assessed in
alert patients withbrain infarction. Neurological signs help
distinguish infarc-tion of the carotid territory from infarction
with a vertebro-basilar distribution. Crossed (cranial nerve palsy
with con-tralateral motor or sensory deficit) or bilateral
neurologicalsigns suggest that the infarct is located in the brain
stem.Specific patterns of deficit, such as pure sensory stroke
ordysarthria with a clumsy hand, may be present. Such
deficitssuggest a subcortical or lacunar infarct caused by
small-vessel disease. The specificity of clinical signs such as
puremotor deficit, however, is low. Distinguishing between lacu-nar
and nonlacunar infarcts on the basis of clinical features isoften
difficult, especially within hours of the onset of stroke.
Severity of StrokeThe National Institutes of Health Stroke Scale
(NIHSS) measuresneurological function, and scores on this scale are
correlated withthe severity of stroke and long-term outcome in
patients withischemic stroke.25,34,35 The scale provides a
reliable, valid, and
TABLE 3. Los Angeles Prehospital Stroke Screen (LAPSS)
For evaluation of acute, noncomatose, nontraumatic neurological
complaint: If items 1 through 6 are ALL checked yes (or unknown),
notify the receivinghospital before arrival of the potential stroke
patient. If any are checked no, follow appropriate treatment
protocol.
Interpretation: Ninety-three percent of patients with stroke
will have positive findings (all items checked yes or unknown) on
the LAPSS (sensitivity593%),and 97% of those with positive findings
will have a stroke (specificity597%). The patient may still be
having a stroke if LAPSS criteria are not met.
Criteria Yes Unknown No
1. Age .45 years [ ] [ ] [ ]
2. History of seizures or epilepsy absent [ ] [ ] [ ]
3. Symptom duration ,24 hours [ ] [ ] [ ]
4. At baseline, patient is not wheelchair bound or bedridden [ ]
[ ] [ ]
5. Blood glucose between 60 and 400 [ ] [ ] [ ]
6. Obvious asymmetry (right vs left) in any of the following 3
categories (must beunilateral)
[ ] [ ] [ ]
Equal R Weak L Weak
Facial smile/grimace [ ] [ ] Droop [ ] Droop
Grip [ ] [ ] Weak grip [ ] Weak grip
[ ] [ ] No grip [ ] No grip
Arm strength [ ] [ ] Drifts down [ ] Drifts down
[ ] [ ] Falls rapidly [ ] Falls rapidly
From References 18 and 32.
TABLE 4. Presenting Clinical Features of Hemorrhagic
andNonhemorrhagic Stroke
HeadacheDecreased Level of
ConsciousnessFocalDeficit
Infarction 11 1 111
Intracerebral hemorrhage 111 111 111
Subarachnoid hemorrhage 111 11 1
1 indicates mild; 11, moderate; and 111, severe.
Part 7: Era of Reperfusion: Acute Stroke I-207
by guest on March 5, 2014http://circ.ahajournals.org/Downloaded
from
-
easy-to-perform alternative to the standard neurological
evaluationfor patients with ischemic stroke, and it has been used
for triage ofpatients to different treatment protocols.36,37 The
NIHSS total scoreranges from 0 (normal) to 42 points, evaluating 5
major areas offunctioning:
1. Level of consciousness2. Visual function3. Motor function4.
Sensation and neglect5. Cerebellar function
The NIHSS is not a comprehensive neurological examina-tion (eg,
it does not record gait or all cranial nerve deficits),and more
detailed neurological assessment may be requiredin certain
cases.
The Scandinavian Stroke Scale was used in the
EuropeanCooperative Acute Stroke Study and has been shown
toidentify predictors of early and late progression in
strokepatients.38,39
The Hunt and Hess Scale (see Table 5) is often used tograde the
severity of stroke in patients with subarachnoidhemorrhage.40 The
Hunt and Hess grade is correlated withsurvival after subarachnoid
hemorrhage and the risk ofcomplications such as vasospasm. The
scale may be used toguide the timing of aneurysm clipping or
coiling.
Differential DiagnosisVery few nonvascular neurological diseases
will cause sud-den onset of focal brain dysfunction, the hallmark
of stroke.The list of potential diagnoses (see Table 6) is longer
if thepatient is comatose and the medical history is unavailable.
Ifthe patients condition gradually worsens over several days,
anonvascular neurological disease may be present.
Prehospital TransportEMS systems should develop protocols that
provide forpriority dispatch, treatment, and transport of patients
withsigns and symptoms of acute ischemic stroke. These proto-cols
should convey the same urgency as those for patientswith signs and
symptoms of AMI or major trauma (Class IIb).Give highest priority
to patients with a suspected stroke andairway compromise or an
altered level of consciousness.
In addition, triage and transport patients with acute onset
ofstroke symptoms to a facility that can begin fibrinolytictherapy
within 1 hour of arrival, unless that facility is .30minutes away
by ground ambulance (Class IIb).
ED Triage and TreatmentThe ED must be prepared for the arrival
of the stroke patientso that triage and therapy can begin
immediately. Maximum
time intervals for completion of diagnostic studies of
candi-dates for fibrinolytic therapy are listed in Table 7.
Emergency Diagnostic StudiesEmergency diagnostic studies are
used to establish stroke asthe cause of the patients symptoms, to
differentiate betweenbrain infarction and brain hemorrhage, and to
determine themost likely cause of the stroke. Protocols may
prioritize andstreamline the order of these tests.
CT is the most important diagnostic test for
differentiatingbetween infarction and hemorrhage or other
intracranialmasses.41 To avoid confusing blood and contrast
medium,perform CT without contrast enhancement. Withhold
antico-agulants and fibrinolytics until brain hemorrhage is ruled
out.
The CT scan of almost all patients with a recent intrace-rebral
hemorrhage will show increased density at the site ofbleeding.42
Findings in patients with subarachnoid hemor-rhage, however, may be
subtle (eg, the scan may show onlya thin, white layer adjacent to
the brain). Approximately 5%of patients with subarachnoid
hemorrhage will have normalfindings on the CT scan.43,44 Such
patients usually have asmall subarachnoid hemorrhage and are alert
with no focalneurological deficits (Hunt and Hess grade 1). If
clinicalsuspicion of subarachnoid hemorrhage remains despite
neg-ative findings on the CT scan, perform lumbar puncture.
Magnetic resonance imaging (MRI) is not part of theroutine
evaluation of acute stroke. MRI is very sensitive andwill detect
some lesions missed by CT. Although MRI candetect early
hemorrhage,45,46 it is not superior to CT. MRI isalso time
consuming and may hamper continuous observationof acutely ill
patients. New MRI techniques such as magneticresonance angiography
and diffusion- and perfusion-weighted MRI may help delineate the
site of occlusion or theregion of the brain at risk for
infarction.47,48 These techniques
TABLE 5. Hunt and Hess Scale for Subarachnoid Hemorrhage
Grade Neurological Status
1 Asymptomatic
2 Severe headache or nuchal rigidity; no neurological
deficit
3 Drowsy; minimal neurological deficit
4 Stuporous; moderate to severe hemiparesis
5 Deep coma; decerebrate posturing
From Reference 40.
TABLE 6. Differential Diagnosis of Stroke
Hemorrhagic stroke
Ischemic stroke
Craniocerebral/cervical trauma
Meningitis/encephalitis
Hypertensive encephalopathy
Intracranial mass
Tumor
Subdural/epidural hematoma
Seizure with persistent neurological signs (Todds paralysis)
Migraine with persistent neurological signs
Metabolic disturbances
Hyperglycemia (nonketotic hyperosmolar coma)
Hypoglycemia
Postcardiac arrest ischemia
Toxicological cause
Endocrine disorder (myxedema)
Uremia
Psychiatric syndromes
Shock and CNS hypoperfusion
CNS indicates central nervous system.
I-208 Circulation August 22, 2000
by guest on March 5, 2014http://circ.ahajournals.org/Downloaded
from
-
are being evaluated for use in clinical practice.
Diffusion-weighted MRI has been approved for use in stroke patients
bythe US Food and Drug Administration (Class Indeterminate).
Emergency cerebral angiography is performed in manypatients with
subarachnoid hemorrhage in anticipation ofaneurysm clipping.
Neurointerventional procedures such asaneurysm coiling,
angioplasty, and intra-arterial thrombolysisalso require emergency
angiography in certain patients. Manyother studies, including
echocardiography, ultrasonographyof the carotid artery, and
transcranial Doppler, can beperformed electively.
Emergency ManagementRapidly identify, evaluate, and treat all
patients with signsand symptoms of acute stroke. Stroke protocols
and pathwaysmay assist in the rapid assessment of these patients.
Clini-cians may find the use of a checklist helpful to
identifycontraindications to tPA therapy.49 Target times for
in-hospital evaluation and treatment are given in Table 7.50
General Emergency TherapyEstablish intravenous access en route
to the hospital or in theED (see Table 8). Administer normal saline
or lactatedRingers solution at a rate of 50 mL/h. Unless the
patient ishypotensive, avoid rapid infusions, which increase the
risk ofcerebral edema. Do not administer dextrose in water
unlesshypoglycemia is strongly suspected; this solution is
hypo-tonic and may increase cerebral edema.5157 Correct
hyper-glycemia and hyperthermia (Class IIa). Do not
routinelyadminister supplemental oxygen to nonhypoxic (oxygen
sat-uration .90%) stroke victims with minor or moderatestrokes.
Oxygen may be beneficial, however, to patients withsevere strokes,
but additional research is needed.58
Management of Elevated Blood PressureManagement of blood
pressure after acute ischemic or hem-orrhagic stroke is
controversial. Many patients have hyper-tension after an ischemic
or hemorrhagic stroke, but fewrequire emergency treatment. Elevated
blood pressure after astroke is not a hypertensive emergency unless
there are othermedical problems (eg, AMI or aortic dissection).59
In mostpatients, blood pressure will spontaneously decline as
pain,agitation, vomiting, and increased ICP are controlled.25
Antihypertensive treatment is reserved for patients withmarkedly
elevated blood pressures or specific medical indi-cations. Current
recommendations are based on the type ofstroke (hemorrhagic or
ischemic) and whether the patientwith ischemic stroke is a
candidate for fibrinolytic therapy. Inresponse to requests for
general guidance regarding themanagement of hypertension in stroke
patients, a table ofsuggested antihypertensive therapy approaches
is provided(see Table 9). It is important to note, however, that
thesesuggestions were based on consensus opinion and are
notevidence-based.
Antihypertensive therapy can be harmful. Antihypertensivetherapy
can lower the cerebral perfusion pressure and lead toworsening of
the stroke.59 In addition, the response of strokepatients to
antihypertensive therapy can be exaggerated. Useof short-acting
nifedipine is contraindicated.59 For patientswith an arterial
occlusion, maintenance of adequate collateralflow is of paramount
importance.
In candidates for fibrinolytic therapy, however, strictcontrol
of blood pressure is required to reduce the potentialfor bleeding.
Fibrinolytic therapy is not recommended forpatients who have a
systolic blood pressure .185 mm Hg ora diastolic blood pressure
.110 mm Hg at the time oftreatment (see Table 9).60,61 Simple
measures often can lowerblood pressure below this level. If more
aggressive measuresare required, do not use fibrinolytics.
Management of SeizuresRecurrent seizures are a potentially
life-threatening compli-cation of stroke. They can worsen the
stroke and should becontrolled. Administration of anticonvulsant
medications toprevent recurrent seizures is strongly recommended,
butprophylactic administration is not indicated.59 Protection ofthe
airway, administration of supplementary oxygen, andmaintenance of
normothermia are part of supportive care.
Benzodiazepines are first-line agents for treating
seizures.Intravenous diazepam (5 mg over 2 minutes to a maximum
of10 mg) or lorazepam (1 to 4 mg over 2 to 10 minutes) usuallywill
stop seizures but may produce respiratory depression.Lorazepam,
which has a short half-life, may be the superioragent.
Administration of these agents can be repeated, butthey should be
followed by a longer-acting anticonvulsantsuch as phenytoin,
fosphenytoin, or phenobarbital.
Management of Increased ICPDeath during the first week after
stroke commonly is caused bybrain edema and increased ICP.
Fortunately only 10% to 20% of
TABLE 7. NINDS-Recommended Stroke Evaluation Targets
forPotential Fibrinolytic Candidates*
Time Target
Door to doctor 10 Minutes
Door to CT completion 25 Minutes
Door to CT read 45 Minutes
Door to treatment 60 Minutes
Access to neurological expertise 15 Minutes
Access to neurosurgical expertise 2 Hours
Admission to monitored bed 3 Hours
NINDS indicates National Institute of Neurological Disorders and
Stroke; CT,computed tomography.
*Target times will not be achieved in all cases, but they
represent areasonable goal.
By phone or in person.
TABLE 8. General Management of Acute Stroke
1. Intravenous fluids Avoid D5W and excessive fluid loading
2. Blood sugar Determine immediately. Bolus of 50% dextroseif
hypoglycemic; insulin if .300 mg%
3. Thiamine 100 mg if malnourished, alcoholic
4. Oxygen Pulse oximetry. Supplement if SO2 ,90%
5. Acetaminophen If febrile
6. NPO If at risk for aspiration
7. Cardiac monitor
D5W indicates 5% dextrose in water; SO2, oxygen saturation.
Part 7: Era of Reperfusion: Acute Stroke I-209
by guest on March 5, 2014http://circ.ahajournals.org/Downloaded
from
-
stroke patients develop brain edema sufficient to cause
clinicaldeterioration. When brain edema is clinically suspect,
modestfluid restriction, elevation of the head of the bed (20 to
30),support of oxygenation and ventilation (avoidance of
hypoxemiaand hypoventilation), and control of agitation and pain
will helplower increased ICP. Goals of therapy are (1) reduction
ofincreased ICP, (2) maintenance of cerebral perfusion to
preventworsening of ischemia, and (3) prevention of brain
herniation.
Reduction of the partial pressure of CO2 in arterial gas(PaCO2)
through intubation and hyperventilation is the mostrapid means of
lowering ICP in cases of impending brainherniation. Optimal PaCO2
is 30 to 35 mm Hg.62 PaCO2 values#25 mm Hg are occasionally
acceptable in rapidly deterio-rating patients, but if such values
are sustained, ischemia ofthe brain may occur.62 Aggressive
tracheal suctioning in-creases ICP and should be avoided, with
suctioning reducedin frequency and duration to that necessary to
maintaintracheal tube patency.
Hyperosmolar therapy with mannitol is used to reduce themass
effect on diencephalic structures or to maximize cerebralperfusion
pressure. Mannitol can be given as a bolus (0.25 to 0.5g/kg per
dose given over 20 minutes rapidly) and repeated every6 hours to a
maximum dose of 2 g/kg daily.59 High initial dosesare given in
emergencies. The effect on ICP usually occurs about20 minutes after
administration. Lower doses (25 to 50 g every4 hours) given as
intermittent boluses are used to manage ICP
over longer periods. Furosemide, hypertonic saline, and
acet-azolamide may also help lower ICP.
High doses of barbiturates (eg, thiopental 1 to 5 mg/kg)rapidly
lower ICP and suppress electrical brain activity.Because high doses
of barbiturates suppress respiratoryactivity and may produce
vasodilation and myocardialdepression, they should be administered
in conjunctionwith mechanical ventilatory support and careful
bloodpressure monitoring. ICP must be monitored when abarbiturate
coma is induced, because the barbituratesobliterate the clinical
response. The ICP is used to evaluateresponse to therapy.
Routine measurement of ICP is not indicated, and the valueof ICP
measurement has not been shown. ICP measurement,however, may be
helpful in deteriorating patients, can guidetherapy, and can serve
as an indicator of prognosis andoutcome.59
Neurosurgical decompression can be lifesaving in somepatients
with high ICP and intracranial hemorrhage, edemaafter stroke, or
other mass effects on brain tissue. Surgery forcerebellar
hemorrhage or edema after stroke can produceremarkable improvement.
Pharmacological and ventilatorymeasures for controlling ICP are
much less effective thansurgery in patients with cerebellar
lesions. Corticosteroids arenot effective and should not be used.63
Cerebellar edema orhemorrhage frequently causes obstructive
hydrocephalus,
TABLE 9. Suggested Antihypertensive Therapy for Patients With
Acute Stroke
Blood Pressure* Treatment
Patients ineligible for fibrinolytic therapy
1. DBP .140 mm Hg Sodium nitroprusside (0.5 mg/kg per
minute).
Aim for 10% to 20% reduction in DBP.
2. SBP .220, DBP 121 to 140, or MAP.130 mm Hg
10 to 20 mg labetalol IV push over 1 to 2 minutes. May repeat or
double labetalol every 20minutes to a maximum dose of 150 mg.
3. SBP ,220, DBP #120, or MAP,130 mm Hg
Emergency antihypertensive therapy is deferred in the absence of
aortic dissection, AMI, severeCHF, or hypertensive
encephalopathy.
Candidates for fibrinolytic therapy
Pretreatment
1. SBP .185 or DBP .110 mm Hg 1 to 2 inches of nitropaste or 1
to 2 doses of 10 to 20 mg labetalol IV push. If BP is notreduced to
and maintained at ,185/110 mm Hg, do not administer
fibrinolytics.
During and after treatment
1. Monitor BP Check BP every 15 minutes for 2 hours, then every
30 minutes for 6 hours, and then every 1hour for 16 hours.
2. DBP .140 mm Hg Sodium nitroprusside (0.5 mg/kg per
minute)
3. SBP .230 or DBP 121 to 140 mm Hg (1) 10 mg labetalol IV push
over 1 to 2 minutes. May repeat or double labetalol every 10minutes
to a maximum dose of 150 mg, or give the initial labetalol bolus
and then start alabetalol drip at 2 to 8 mg/min.
(2) If BP is not controlled by labetalol, consider sodium
nitroprusside.
4. SBP 180 to 230 or DBP 105 to 120 mm Hg 10 mg labetalol IV
push. May repeat or double labetalol every 10 to 20 minutes to a
maximumdose of 150 mg, or give initial labetalol bolus and then
start a labetalol drip at 2 to 8 mg/min.
(Note: These suggestions are consensus rather than
evidence-based and should be individualized, with consideration
given to clinical status and baseline bloodpressure.)
DBP indicates diastolic blood pressure; SBP, systolic blood
pressure; MAP, mean arterial pressure; BP, blood pressure; IV,
intravenous; AMI, acute myocardialinfarction; and CHF, congestive
heart failure.
*Before treatment, all initial blood pressures should be
verified by repeating reading in 5 minutes.As estimated by one
third the sum of SBP and double DBP.Avoid labetalol in patients
with asthma, cardiac failure, or severe abnormalities in cardiac
conduction. For patients with refractory hypertension, consider
alternative therapy with sodium nitroprusside or enalapril.
I-210 Circulation August 22, 2000
by guest on March 5, 2014http://circ.ahajournals.org/Downloaded
from
-
necessitating ventricular drainage. Closely monitor patientswith
cerebellar lesions for neurological deterioration.
Pharmacological and Interventional TherapiesIschemic
StrokeFibrinolytic TherapyUse of intra-arterial and intravenous
fibrinolytic agents suchas tPA, streptokinase, ancrod, urokinase,
and prourokinase instroke patients has been evaluated in several
clinicaltrials.39,6472 The Cochrane Stroke Review group73
evaluated17 trials with .5000 patients in which .50% of
patientsreceived tPA. Fibrinolytic therapy significantly increased
theodds ratio of death within the first 10 days and at
follow-up,mainly because of fatal intracerebral hemorrhage.
Patientstreated within 3 hours, however, had reduced death
anddependency compared with patients treated within 3 to 6hours.
Overall, the proportion of patients with death ordisability was
reduced. It is difficult to draw conclusions fromthis review
because there was significant heterogeneityamong the comparison
trials.73 In the clinical trials reviewed,many different agents
were administered, with many differenttime intervals between onset
of stroke symptoms and drugadministration.
The National Institute of Neurological Disorders and Stroke
rtPAStroke Trial64 evaluated a single agent administered within 3
hoursof symptom onset in a prospective, blinded, randomized,
controlledclinical trial. Intravenous tPA was administered in a
dose of 0.9 mggiven as a 10% bolus over 1 minute, followed by a
1-hour infusionversus a placebo. In this trial, patients treated
with tPA within 3hours of onset of symptoms were at least 30% more
likely to haveminimal or no disability at 3 months compared with
those treatedwith placebo. The risk of fatal intracranial
hemorrhage, however,was 10 times greater in the tPA-treated group
(3% versus 0.3%). Asimilar increase in the frequency of all
symptomatic hemorrhages(6.4% versus 0.6%) was also observed in this
group. This increasein symptomatic hemorrhage did not lead to an
overall increase inmortality in the treated group.
Based on the results of parts I and II of the NationalInstitute
of Neurological Disorders and Stroke study,intravenous
administration of tPA is recommended forcarefully selected patients
with acute ischemic stroke ifthey have no contraindications to
fibrinolytic therapy andif the drug can be administered within 3
hours of the onsetof stroke symptoms (Class I). Contraindications
to tPA arelisted in Table 10.
Investigators have tried to extend the time for treatmentbeyond
3 hours by using various fibrinolytic agents andnew approaches to
administration (eg, intra-arterial thera-py).39,65 67,69 72
Evidence suggested that use of intravenoustPA 3 to 6 hours after
the onset of symptoms may bebeneficial in certain patients,73 but
recent studies havebeen discouraging. The ATLANTIS Trial found no
signif-icant differences in 90-day efficacy end points in
patientstreated between 3 and 5 hours.65 The Thrombolytic Ther-apy
in Acute Ischemic Stroke Study enrolled 142 patientsat 42 sites in
North America and found a small butsignificant benefit of tPA in
patients treated after 3 hourswhen assessed at 1 day; this benefit
was not maintained at
30 days.74 In both of these trials, the rate of
symptomaticintracerebral hemorrhage was increased. At this
timeroutine use of intravenous tPA .3 hours after the onset
ofsymptoms is not recommended (Class Indeterminate).
Results of a recent, randomized trial of
intra-arterialprourokinase suggest that use of intra-arterial
fibrinolyticagents 3 to 6 hours after the onset of symptoms may
bebeneficial in patients with occlusion of the middle
cerebralartery (Class IIb).71
Three large, randomized trials of streptokinase in patientswith
stroke have been reported.69,70,75 All 3 studies weresuspended
because of increased hemorrhage and mortality inthe group treated
with streptokinase. Do not use streptokinasein patients who have
had a stroke except in clinical studiesapproved by the appropriate
institutional review board.
Anticoagulant TherapyThe efficacy of anticoagulants in acute
stroke has not beenestablished. Heparin is frequently administered
to patientswith acute ischemic stroke, but its value is
unproved.76,77Heparin may help prevent recurrent embolism or
propagationof a thrombus, but it may lead to bleeding
complications,including brain hemorrhage. There is no consensus on
whenheparin therapy should be started or on the dose and durationof
therapy. Emergency physicians should consult the attend-ing
neurologist about the use of heparin in specific patients(Class
IIb). Low-molecular-weight anticoagulants have sev-eral advantages
not provided by unfractionated heparin.71 Useof
low-molecular-weight anticoagulants in the managementof stroke is
being evaluated.
Aspirin, warfarin, and ticlopidine reduce the risk ofsubsequent
stroke in patients with TIA.78 81 These anti-platelet agents should
be started within the first few daysafter a TIA. When started
within 48 hours of the onset ofischemic stroke, aspirin produces a
small but definite netbenefit in patients who are ineligible for
fibrinolytic
TABLE 10. Contraindications to tPA Therapy for AcuteIschemic
Stroke
Evidence of intracranial hemorrhage on pretreatment
evaluation
Suspicion of subarachnoid hemorrhage on pretreatment
evaluation
Recent (within 3 months) intracranial or intraspinal surgery,
serious headtrauma, or previous stroke
History of intracranial hemorrhage
Uncontrolled hypertension at time of treatment (see Management
of HighBlood Pressure)
Seizure at stroke onset
Active internal bleeding
Intracranial neoplasm, arteriovenous malformation, or
aneurysm
Known bleeding diathesis, including but not limited to
Current use of oral anticoagulants (eg, warfarin sodium),
aninternational normalized ratio .1.7, or a prothrombin time
.15seconds
Administration of heparin within 48 hours preceding the onset of
strokeand an elevated activated partial thromboplastin time at
presentation
Platelet count ,100 000/mm3
tPA indicates tissue plasminogen activator.
Part 7: Era of Reperfusion: Acute Stroke I-211
by guest on March 5, 2014http://circ.ahajournals.org/Downloaded
from
-
therapy.82,83 Antiplatelet therapy with aspirin 160 to 300mg
daily within 48 hours of onset of presumed ischemicstroke reduces
the risk of early recurrent ischemic strokewithout a major risk of
early hemorrhagic complicationsand improves long-term
outcome.84
The Cochrane Stroke Group completed a comprehensivereview of
anticoagulants in 21 trials involving 23 427 pa-tients. A number of
anticoagulants were used in clinical trials:standard unfractionated
heparin, low-molecular-weight hepa-rins, heparinoids, oral
anticoagulants, and thrombin inhibi-tors. The conclusion of the
Cochrane group was that imme-diate anticoagulant therapy in
patients with acute ischemicstroke is not associated with net gain
for either short- orlong-term benefit. Routine use of any type of
anticoagulant inacute ischemic stroke is not recommended.85
Other TreatmentsCalcium channelblocking drugs, volume expansion,
hemodi-lution, and low-molecular-weight dextran have not been
shownto improve clinical outcome after ischemic stroke. A number
ofcytoprotective agents are being investigated for use in
patientswith acute ischemic or hemorrhagic stroke. Many of these
agentshave been shown to provide no benefit in humans, even
thoughbenefit was shown in animal models.86
Hemorrhagic Stroke
Subarachnoid HemorrhagePatients with subarachnoid hemorrhage
often require emer-gency arteriography. If a saccular aneurysm is
detected, earlyintracranial surgery with clipping (or coiling) of
the aneurysmis usually advised.87 The calcium channelblocking
drugnimodipine (60 mg orally every 4 hours, 0.35 mg/kg) im-proves
outcome after subarachnoid hemorrhage.8892 Correc-tion of
hyponatremia and water loss is also important. Avoidstrict fluid
restriction, however, which may stimulate inap-propriate secretion
of antidiuretic hormone.
Intracerebral HemorrhageHemorrhage into the brain can be
devastating. Death may occurbecause of compression or distortion of
vital deep-brain structuresor increased ICP. Mortality is a
function of the volume and locationof the intracerebral bleeding.
Optimal management requires preven-tion of continued bleeding,
appropriate management of ICP, andtimely neurosurgical
decompression when warranted. Large intra-cerebral or cerebellar
hematomas often require surgical intervention.A CT scan is required
for differential diagnosis. Placement of aventriculostomy tube
through a burr hole can be lifesaving ifhydrocephalus is the cause
of coma.
Appendix A: NIH Stroke ScaleQuick and Easy Version
Category Description ScoreBaseline
Date/Time Date/Time
1a. Level of consciousness (LOC) Alert 0
(Alert, drowsy, etc) Drowsy 1
Stuporous 2
Coma 3
1b. LOC questions Answers both correctly 0
(Month, age) Answers 1 correctly 1
Incorrect 2
1c. LOC commands Obeys both correctly 0
(Open, close eyes, make fist, let go) Obeys 1 correctly 1
Incorrect 2
2. Best gaze Normal 0
(Eyes openpatient follows examiners finger or face) Partial gaze
palsy 1
Forced deviation 2
3. Visual No visual loss 0
(Introduce visual stimulus/threat to patients visual Partial
hemianopia 1
field quadrants) Complete hemianopia 2
Bilateral hemianopia 3
4. Facial palsy Normal 0
(Show teeth, raise eyebrows, and squeeze eyes shut) Minor 1
Partial 2
Complete 3
I-212 Circulation August 22, 2000
by guest on March 5, 2014http://circ.ahajournals.org/Downloaded
from
-
Appendix A: Continued
Category Description ScoreBaseline
Date/Time Date/Time
5a. Motor armleft No drift 0
(Elevate extremity to 90 and score drift/movement) Drift 1
Cant resist gravity 2
No effort against gravity 3
No movement 4
Amputation, joint fusion (explain) 9
5b. Motor armright No drift 0
(Elevate extremity to 90 and score drift/movement) Drift 1
Cant resist gravity 2
No effort against gravity 3
No movement 4
Amputation, joint fusion (explain) 9
6a. Motor legleft No drift 0
(Elevate extremity to 30 and score drift/movement) Drift 1
Cant resist gravity 2
No effort against gravity 3
No movement 4
Amputation, joint fusion (explain) 9
6b. Motor legright No drift 0
(Elevate extremity to 30 and score drift/movement) Drift 1
Cant resist gravity 2
No effort against gravity 3
No movement 4
Amputation, joint fusion (explain) 9
7. Limb ataxia Absent 0
(Fingernose, heel down shin) Present in 1 limb 1
Present in 2 limbs 2
8. Sensory Normal 0
(Pin prick to face, arm, trunk, and legcompare side Partial loss
1
to side) Severe loss 2
9. Best language No aphasia 0
(Name items, describe a picture, and read sentences) Mild to
moderate aphasia 1
Severe aphasia 2
Mute 3
10. Dysarthria Normal articulation 0
(Evaluate speech clarity by patient repeating listed words) Mild
to moderate dysarthria 1
Near to unintelligible or worse 2
Intubated or other physicalbarrier
9
11. Extinction and inattention No neglect 0
(Use information from prior testing to identify neglect or
Partial neglect 1
double simultaneous stimuli testing) Complete neglect 2
Individual Administering Scale:
Adapted with permission from Spilker J, Kongable G. The NIH
Stroke Scale: its importance and practical application in the
clinical setting. Stroke Intervent.2000;2:714. For further
information, please refer to the website
http://www.stroke-site.org.
Part 7: Era of Reperfusion: Acute Stroke I-213
by guest on March 5, 2014http://circ.ahajournals.org/Downloaded
from
-
References1. Broderick JP, Brott T, Tomsick T, Huster G, Miller
R. The risk of
subarachnoid and intracerebral hemorrhages in blacks as compared
withwhites. N Engl J Med. 1992;326:733736.
2. Stegmayr B, Vinogradova T, Malyutina S, Peltonen M, Nikitin
Y,Asplund K. Widening gap of stroke between east and west:
eight-yeartrends in occurrence and risk factors in Russia and
Sweden. Stroke.2000;31:28.
3. Thorvaldsen P, Davidsen M, Bronnum-Hansen H, Schroll M.
Stablestroke occurrence despite incidence reduction in an aging
population:stroke trends in the Danish monitoring trends and
determinants in car-diovascular disease (MONICA) population.
Stroke. 1999;30:25292534.
4. Thorvaldsen P, Kuulasmaa K, Rajakangas AM, Rastenyte D, Sarti
C,Wilhelmsen L. Stroke trends in the WHO MONICA project.
Stroke.1997;28:500506.
5. Williams GR, Jiang JG, Matchar DB, Samsa GP. Incidence
andoccurrence of total (first-ever and recurrent) stroke. Stroke.
1999;30:25232528.
6. Grotta JC. The importance of time. In: Proceedings of a
National Sym-posium on Rapid Identification and Treatment of Acute
Stroke. Bethesda,Md: National Institute of Neurological Disorders
and Stroke; 1997:59.
7. Pepe PE. Overview: the initial links in the chain of recovery
for brainattack: access, prehospital care, notification, and
treatment. In: Pro-ceedings of a National Symposium on Rapid
Identification and Treatmentof Acute Stroke. Bethesda, Md: National
Institute of Neurological Dis-orders and Stroke; 1997:1728.
8. Spilker JA. Overview: the importance of patient and public
education inacute ischemic stroke. In: Proceedings of a National
Symposium on RapidIdentification and Treatment of Acute Stroke.
Bethesda, Md: NationalInstitute of Neurological Disorders and
Stroke; 1997:119126.
9. Sayre MR, Swor RA, Honeycutt LK. Prehospital identification
andtreatment. In: Proceedings of a National Symposium on Rapid
Identifi-cation and Treatment of Acute Stroke. Bethesda, Md:
National Institute ofNeurological Disorders and Stroke;
1997:3544.
10. Kothari R, Sauerbeck L, Jauch E, Broderick J, Brott T,
Khoury J, Liu T.Patients awareness of stroke signs, symptoms, and
risk factors. Stroke.1997;28:18711875.
11. Barsan WG, Brott TG, Broderick JP, Haley EC, Levy DE, Marler
JR.Time of hospital presentation in patients with acute stroke.
Arch InternMed. 1993;153:25582561.
12. Alberts MJ, Perry A, Dawson DV, Bertels C. Effects of public
andprofessional education on reducing the delay in presentation and
referralof stroke patients. Stroke. 1992;23:352356.
13. The National Institute of Neurological Disorders and Stroke
(NINDS)rt-PA Stroke Study Group. A systems approach to immediate
evaluationand management of hyperacute stroke. Experience at eight
centers andimplications for community practice and patient care.
Stroke. 1997;28:15301540.
14. Crocco TJ, Kothari RU, Sayre MR, Liu T. A nationwide
prehospitalstroke survey. Prehosp Emerg Care. 1999;3:201206.
15. Ferro JM, Melo TP, Oliveira V, Crespo M, Canhao P, Pinto AN.
Ananalysis of the admission delay of acute strokes. Cerebrovasc
Dis. 1994;4:7275.
16. Kothari R, Jauch E, Broderick J, Brott T, Sauerbeck L,
Khoury J, Liu T.Acute stroke: delays to presentation and emergency
department eval-uation. Ann Emerg Med. 1999;33:38.
17. Morris DL, Rosamond WD, Hinn AR, Gorton RA. Time delays
inaccessing stroke care in the emergency department. Acad Emerg
Med.1999;6:218223.
18. Kidwell CS, Saver JL, Schubert GB, Eckstein M, Starkman S.
Design andretrospective analysis of the Los Angeles Prehospital
Stroke Screen(LAPSS). Prehosp Emerg Care. 1998;2:267273.
19. Kothari R, Barsan W, Brott T, Broderick J, Ashbrock S.
Frequency andaccuracy of prehospital diagnosis of acute stroke.
Stroke. 1995;26:937941.
20. Zachariah B, Dunford J, Van Cott CC. Dispatch life support
and the acutestroke patient: making the right call. In: Proceedings
of a NationalSymposium on Rapid Identification and Treatment of
Acute Stroke.Bethesda, Md: National Institute of Neurological
Disorders and Stroke;1997:2934.
21. Davalos A, Castillo J, Martinez-Vila E, Cerebrovascular
Diseases StudyGroup of the Spanish Society of Neurology. Delay in
neurologicalattention and stroke outcome.. Stroke.
1995;26:22332237.
Appendix B: Scandinavian Stroke Scale(Scandinavian Stroke Study
Group, 1985)
1. Consciousness
Fully conscious6
Somnolent, can be awakened to full consciousness4
Reacts to verbal command but is not fully conscious2
Stupor (reacts to pain only)0
Coma0
2. Orientation
Correct for time, place, and person6
Two of these (time, place, person)4
One of these2
Completely disoriented0
3. Speech
No aphasia10
Impairment of comprehension or expression disability6
More than yes/no but not longer sentences3
Only yes/no or less0
4. Eye movement
No gaze palsy4
Gaze palsy present2
Forced lateral gaze0
5. Facial palsy
None/dubious/slight2
Present0
6. Gait
Walks at least 5 m without aids12
Walks with aids9
Walks with help of another person6
Sits without support3
Bedridden/wheelchair0
7. Arm, motor power (assessed only on affected side)
Raises arm with normal strength6
Raises arm with reduced strength5
Raises arm with flexion in elbow4
Can move but not against gravity2
Paralysis0
8. Hand, motor power (assessed only on affected side)
Normal strength6
Reduced strength in full range4
Some movement, fingertips do not reach palm2
Paralysis0
9. Leg, motor power (assessed only on affected side)
Normal strength6
Raises straight leg against resistance with reducedstrength5
Raises leg with flexion of knee against gravity4
Can move but not against gravity2
Paralysis0
10. Foot paresis
None2
Present0
I-214 Circulation August 22, 2000
by guest on March 5, 2014http://circ.ahajournals.org/Downloaded
from
-
22. Lyden PD, Rapp K, Babcock T, Rothcock J. Ultra-rapid
identification,triage, and enrollment of stroke patients into
clinical trials. J StrokeCerebrovasc Dis. 1994;4:106107.
23. Bornstein NM, Gur AY, Fainshtein P, Korczyn AD. Stroke
during sleep:epidemiological and clinical features. Cerebrovasc
Dis. 1999;9:320322.
24. Hazinski MF. Demystifying recognition and management of
stroke. CurrEmerg Card Care. 1996;7:89.
25. Broderick J, Brott T, Barsan W. Blood pressure during the
first minutesof focal cerebral ischemia. Ann Emerg Med.
1993;22:14381443.
26. Maggioni AP, Franzosi MG, Farina ML, Santoro E, Celani MG,
Ricci S,Tognoni G, Gruppo Italiano per lo Studio della
Streptochinasi nellInfartoMiocardico (GISSI). Cerebrovascular
events after myocardial infarction:analysis of the GISSI trial.
BMJ. 1991;302:14281431.
27. Mooe T, Eriksson P, Stegmayr B. Ischemic stroke after acute
myocardialinfarction: a population based study. Stroke.
1997;28:762767.
28. Silver FL, Norris JW, Lewis AL. Early mortality following
stroke: aprospective review. Stroke. 1984;45:492496.
29. Tokgozoglu SL, Batur MK, Topcuoglu MA. Effects of stroke
localizationon cardiac autonomic balance and sudden death. Stroke.
1999;30:13071311.
30. Korpelainen JT, Sotaniemi KA, Makikallio A. Dynamic behavior
of heartrate in ischemic stroke. Stroke. 1999;30:10081013.
31. Kothari RU, Pancioli A, Liu T, Brott T, Broderick J.
Cincinnati Pre-hospital Stroke Scale: reproducibility and validity
[see comments]. AnnEmerg Med. 1999;33:373378.
32. Kidwell CS, Starkman S, Eckstein M, Weems K, Saver JL.
Identifyingstroke in the field: prospective validation of the Los
Angeles PrehospitalStroke Screen (LAPSS). Stroke. 2000;31:7176.
33. Teasdale G, Jennett B. Assessment of coma and impaired
consciousness:a practical scale. Lancet. 1974;2:8184.
34. Brott G, Adams HP Jr, Olinger CP, et al. Measurements of
acute cerebralinfarction: a clinical examination scale. Stroke.
1989;20:864870.
35. Lyden P, Lu M, Jackson C, Marler J, Kothari R, Brott T,
Zivin J, NINDStPA Stroke Trial Investigators. Underlying structure
of the NationalInstitutes of Health Stroke Scale: results of a
factor analysis. Stroke.1999;30:23472354.
36. Lewandowski CA, Frankel M, Tomsick TA, Broderick J, Frey J,
ClarkW, Starkman S, Grotta J, Spilker J, Khoury J, Brott T, and the
EmergencyManagement of Stroke (EMS) Bridging Trial Investigators.
Combinedintravenous and intra-arterial r-TPA versus intra-arterial
therapy of acuteischemic stroke. Stroke. 1999;30:25982609.
37. DeGraba TJ, Hallenbeck JM, Pettirew KD. Progression in acute
stroke:value of the initial NIH Stroke Scale score on patient
stratification infuture trials. Stroke. 1999;30:12081212.
38. Davalos A, Toni D, Iweins F, Lesaffre E, Bastianello S,
Castillo J. Neu-rological deterioration in acute ischemic stroke:
potential predictors andassociated factors in the European
Cooperative Acute Stroke Study(ECASS) I. Stroke.
1999;30:26312636.
39. Hacke W, Kaste M, Fieschi C, Toni D, Lesaffre E, von Kummer
R,Boysen G, Bluhmki E, Hoxter G, Mahagne MH, et al.
Intravenousthrombolysis with recombinant tissue plasminogen
activator for acutehemispheric stroke: the European Cooperative
Acute Stroke Study(ECASS). JAMA. 1995;274:10171025.
40. Hunt WE, Hess RM. Surgical risk as related to time of
intervention in therepair of intracranial aneurysms. J Neurosurg.
1968;28:1420.
41. Gilman S. Imaging the brain. N Engl J Med. 1998;338:812
820,889896.
42. Davis KR, Ackerman RH, Kistler JP. Computed tomography of
cerebralinfarction: hemorrhagic, contrast enhancement, and time of
appearance.Comput Tomogr. 1977;1:7186.
43. Sames TA, Storrow AB, Finkelstein JA, Magoon MR. Sensitivity
ofnew-generation computer tomography in subarachnoid hemorrhage.
AcadEmerg Med. 1996;3:1620.
44. Adams HP Jr, Kassell NF, Torner JC, Sahs AL. CT and clinical
corre-lations in recent aneurysmal subarachnoid hemorrhage: a
preliminaryreport of the Cooperative Aneurysm Study. Neurology.
1983;33:981988.
45. Linfante I, Llinas RH, Caplan LR. MRI features of
intracerebral hemor-rhage within 2 hours from symptom onset.
Stroke. 1999;30:22632267.
46. Schellinger PD, Jansen O, Fiebach JB. A standardized MRI
stroke pro-tocol: comparison with CT in hyperacute intracerebral
hemorrhage.Stroke. 1999;30:765768.
47. Baird AE, Benfield A, Schlaug G. Enlargement of human
cerebral ische-mic lesion volumes measured by diffusion-weighted
magnetic resonanceimaging. Ann Neurol. 1997;41:581589.
48. Tong DC, Yenari MA, Albers GW. Correlation of perfusion and
diffusionweighted MRI with NIHSS score in acute (,6.5 hour)
ischemic stroke.Neurology. 1998;50:864870.
49. Hazinski MF, Cummins RO, Field JM. 2000 Handbook of
EmergencyCardiovascular Care for Healthcare Providers. Dallas, Tex:
AmericanHeart Association; 2000.
50. Barsan WG. Overview: emergency department management of
stroke. In:Proceedings of a National Symposium on Rapid
Identification andTreatment of Acute Stroke. Bethesda, Md: National
Institute of Neuro-logical Disorders and Stroke; 1997:4954.
51. Weir CJ, Murray GD, Dyker AG. Is hyperglycemia an
independentpredictor of poor outcome after acute stroke? results of
a long-termfollow-up study. BMJ. 1997;314:13031306.
52. Helgasun CM. Blood glucose and stroke. Stroke.
1988;19:10491053.53. De Courten-Myers GM, Kleinholz M, Hulm P, et
al. Hemorrhagic infarct
conversion in experimental stroke. Ann Emerg Med.
1992;21:210215.54. Broderick JP, Hagen T, Brott T. Hyperglycemia
and hemorrhagic trans-
formation of cerebral infarcts. Stroke. 1995;26:48484887.55. Yip
PK, He YY, Hsu CY et al. Effect of plasma glucose on infarct
size
in focal cerebral ischemia reperfusion. Neurology.
1991;41:899905.56. Chew W, Kucharczky J, Moseley M. Hyperglycemia
augments ischemic
brain injury: in vivo MR imaging spectroscopic study with
nicardipine incats with occluded middle cerebral arteries. Am J
Neuroradiol. 1991;12:603609.
57. Vazquez-Cruz J, Marti-Vilata JT, Ferrer L. Progressing
cerebralinfarction in relation to plasma glucose in gerbils.
Stroke. 1990;21:16211642.
58. Ronning OM, Guldvog B. Should stroke victims routinely
receive sup-plemental oxygen? a quasi-randomized controlled trial.
Stroke. 1999;30:20332037.
59. Adams HJ, Brott T, Crowell R, Furlan A, Gomez C, Grotta J,
HelgasonC, Marler J, Woolson R, Zivin J, Feinberg W, Mayberg M.
Guidelines forthe management of patients with acute ischemic
stroke: a statement forhealthcare professionals from a special
writing group of the StrokeCouncil, American Heart Association.
Stroke. 1994;25:19011914.
60. Brott T, Lu M, Kothari R, Fagan SC, Frankel M, Grotta JC,
Broderick J,Kwiatkowski T, Lewandowski C, Haley EC, Marler JR,
Tilley BC.Hypertension and its treatment in the NINDS rt-PA Stroke
Trial. Stroke.1998;29:15041509.
61. Adams HJ, Brott T, Furlan A, Gomez C, Grotta J, Helgason C,
Kiat-kowski T, Lyden P, Marler J, Torner J, Feinberg W, Mayberg M,
ThiesW. Guidelines for Thrombolytic Therapy for Acute Stroke: a
supplementto the guidelines for the management of patients with
acute ischemicstroke. Circulation. 1996;94:11671174.
62. Broderick JP, Adams HP, Barsan W, Feinberg W, Feldmann E,
Grotta J,Kase C, Krieger D, Mayberg M, Tilley B, Zabramski JM,
Zuccarello M.Guidelines for the management of spontaneous
intracerebral hemorrhage:a statement for healthcare professionals
from a special writing group ofthe Stroke Council, American Heart
Association. Stroke. 1999;30:905915.
63. Qizilbash N, Lewington SL, Lopez-Arrieta JM. Corticosteroids
for acuteischaemic stroke. Cochrane Database Syst Rev.
2000;2:CD000064.
64. The National Institute of Neurological Disorders and Stroke
rt-PA StrokeStudy Group. Tissue plasminogen activator for acute
ischemic stroke.[see comments]. N Engl J Med.
1995;333:15811587.
65. Clark W, Wissman S, Albers GW, Jhamanda JH, Madden KP,
HamiltonS, for the ATLANTIS Stroke Study Investigators.
Recombinanttissue-type plasminogen activator (Alteplase) for
ischemic stroke 3 to 5hours after symptom onset: the ALANTIS study:
a randomized controlledtrial. JAMA. 1999;282:20192026.
66. Andreotti F, Pasceri V, Hackett DR, Davies GJ, Haider AW,
Maseri A.Preinfarction angina as a predictor of more rapid coronary
thrombolysisin patients with acute myocardial infarction. N Engl J
Med. 1996;334:712.
67. The MAST-I Collaborative Group. Thrombolytic and
antithrombolytictherapy in acute ischemic stroke: Multicenter Acute
Stroke TrialItaly(MAST-I). In: del Zoppo GJ, Mori E, Hacke W, eds.
ThrombolyticTherapy in Acute Ischemic Stroke. New York, NY:
Springer-Verlag;1993:8694.
68. Hacke W, Kaste M, Fieschi C, von Kummer R, Davalos A, Meier
D,Larrue V, Bluhmki E, Davis S, Donnan G, Schneider D, Diez-Tejedor
E,Trouillas P, Second European-Australasian Acute Stroke Study
Investi-gators. Randomised double-blind placebo-controlled trial of
thrombolytictherapy with intravenous alteplase in acute ischaemic
stroke (ECASS II)[see comments]. Lancet. 1998;352:12451251.
Part 7: Era of Reperfusion: Acute Stroke I-215
by guest on March 5, 2014http://circ.ahajournals.org/Downloaded
from
-
69. Multicentre Acute Stroke Trial-Italy (MAST-I) Group.
Randomised con-trolled trial of streptokinase, aspirin, and
combination of both in treatmentof acute ischaemic stroke. Lancet.
1995;346:15091514.
70. Shahar E, McGovern PG. Trials of streptokinase in severe
acuteischaemic stroke [letter]. Lancet. 1995;345:578.
71. del Zoppo GJ, Higashida RT, Furlan AJ, Pessin MS, Rowley HA,
GentM, Prolyse in Acute Cerebral Thromboembolism (PROACT)
Investi-gators. PROACT: a phase II randomized trial of recombinant
pro-urokinase by direct arterial delivery in acute middle cerebral
artery stroke[see comments]. Stroke. 1998;29:411.
72. Furlan A, Higashida R, Wechsler L, Gent M, Rowley H, Kase C
PM,Ahuja A, Callahan F, Clark WM, Silver F, Rivera F, for the
PROACTinvestigators. Intra-arterial prourokinase for acute ischemic
stroke: thePROACT II Study: a randomized controlled trial. JAMA.
1999;282:20032011.
73. Wardlaw JM, del Zoppo G, Yamaguchi T. Thrombolysis for
acuteischaemic stroke. Cochrane Database Syst Rev.
2000;2:CD000213.
74. Clark WM, Albers GW, Madden KP, Hamilton S, thrombolytic
therapy inacute ischemic stroke study investigators. The rtPA
(alteplase) 0- to6-hour acute stroke trial, part A (A0276g):
results of a double-blind,placebo-controlled, multicenter study.
Stroke. 2000;31:811816.
75. ISIS (Second International Study of Infarct Survival)
CollaborativeGroup. Randomized trial of intravenous streptokinase,
oral aspirin, bothor neither among 17,187 cases of suspected acute
myocardial infarction:ISIS-2. Lancet. 1988;2:349360.
76. Gilles Geraud AB. Is anticoagulant therapy too frequently
used in ische-mic stroke? Cerebrovasc Dis. 1991;1(suppl
1):120123.
77. Marsh EE III, Adams HP Jr, Biller J. Use of antithrombotic
drugs in thetreatment of acute ischemic stroke: a survey of
neurologists in practice inthe United States. Neurology.
1989;39:16311634.
78. Antiplatelet Trialists Collaboration. Secondary prevention
of vasculardisease by prolonged antiplatelet treatment. BMJ.
1988;296:320331.
79. The Dutch TIA Trial Study Group. A comparison of two doses
of aspirin(30 mg vs 283 mg a day) in patients after a transient
ischemic attack orminor ischemic stroke. N Engl J Med.
1991;325:12611266.
80. Barnett HJ. Aspirin in stroke prevention: an overview.
Stroke. 1990;21(suppl IV):IV-40IV-43.
81. Hass WK, Easton JD, Adams HP Jr, Ticlopidine Aspirin Stroke
StudyGroup. A randomized trial comparing ticlopidine hydrochloride
with
aspirin for the prevention of stroke in high-risk patients. N
Engl J Med.1989;321:501507.
82. International Stroke Trial Collaborative Group. The
International StrokeTrial (IST): a randomized trial of aspirin,
subcutaneous heparin, both, orneither among 19,435 patients with
acute ischaemic stroke. Lancet. 1997;349:15691581.
83. Chinese Acute Stroke Trial Collaborative Group. CAST:
randomizedplacebo-controlled trial of early aspirin use in 20,000
patients with acuteischaemic stroke. Lancet. 1997;349:16411649.
84. Gubitz G, Sandercock P, Counsell C. Antiplatelet therapy for
acuteischaemic stroke. Cochrane Database Syst Rev.
2000;2:CD000029.
85. Gubitz G, Counsell C, Sandercock P, Signorini D.
Anticoagulants foracute ischaemic stroke. Cochrane Database Syst
Rev. 2000;2:CD000024.
86. Clark WM, Williams BJ, Sacco KA, Zweifler RM, Sabounjian
LA,Gamman RE, for the Citicoline Stroke Study Group. A
randomizedefficacy trial of citicoline in patients with acute
ischemic stroke. Stroke.1999;31:25922597.
87. Mayberg MR, Batjer HH, Dacey R, Diringer M, Haley EC, Heros
RC,Sternau LL, Torner J, Adams HP Jr, Feinberg W, et al. Guidelines
for themanagement of aneurysmal subarachnoid hemorrhage: a
statement forhealthcare professionals from a special writing group
of the StrokeCouncil, American Heart Association. Stroke.
1994;25:23152328.
88. Allen GS, Ahn HS, Preziosi TJ, Battye R, Boone SC, Boone SC,
ChouSN, Kelly DL, Weir BK, Crabbe RA, Lavik PJ, Rosenbloom SB,
DorseyFC, Ingram CR, Mellits DE, Bertsch LA, Boisvert DP, Hundley
MB,Johnson RK, Strom JA, Transou CR. Cerebral arterial spasm: a
controlledtrial of nimodipine in patients with subarachnoid
hemorrhage. N EnglJ Med. 1983;308:619624.
89. Neil-Dwyer G, Mee E, Dorrance D, Lowe D. Early intervention
withnimodipine in subarachnoid haemorrhage. Eur Heart J.
1987;8(supplK):4147.
90. Peturk KC, West M, Mohr G, et al. Nimodipine treatment in
poor-gradeaneurysm patients: results of a multi-center double-blind
placebo-controlled trial. J Neursorug. 1988;68:505517.
91. Philippon J, Grob R, Dagreeou F. Prevention of vasospasm in
subarach-noid haemorrhage: a controlled study with nimodipine. Acta
Neurochir(Wien). 1986;82:110114.
92. Pickard JD, Murray GD, Illingworth R. Effect of oral
nimodipine oncerebral infarction and outcome after subarachnoid
haemorrhage: Britishaneurysm nimodipine trial. BMJ.
1989;298:636642.
I-216 Circulation August 22, 2000
by guest on March 5, 2014http://circ.ahajournals.org/Downloaded
from