Embed Size (px)
Citation preview

Drug and Alcohol Dependence, 18 (1986) 77-85 77 Elsevier Scientific Publishers Ireland Ltd.
C I R C A D I A N RHYTHM OF REM S L E E P OF CHRONIC ALCOHOLICS D U R I N G ALCOHOL WITHDRAWAL
NOBUHIKO IMATOH a, YQICHI NAKAZAWA a, HIROHARU OHSHIMA a, MASAHIKO ISHIBASHF and TOSHITO YOKOYAMA b
aDepartment of Neuropsychiatry, Kurume University School of Medicine, 67 Asahi-Machi, 830 Kurume and bjuzenkai-Kaisei Hospital, 200-1 Asa-Machi, Munakata (Japan)
(Received February 5th, 1986)
SUMMARY
Sleep structures were polygraphically investigated during the alcohol withdrawal periods of six male alcoholics. Polygraphic recordings were taken 10 days, i month and 3 months after hospitalization. Total sleep time was almost equal among the three recording nights for each patient. Stages 3 and 4 sleep were remarkably reduced on all the recording nights. REM sleep time was normal throughout the study. REM latency decreased in many patients on the 10th day, and gradually increased on the follow- ing nights. A very important change was observed in the distribution of REM sleep. Maximal duration was noted in the first REM episode on the 10th day in four of the six. On the second recording night the second REM episode was the longest in five of the six subjects. On the last recording night many patients exhibited a normal distribution of REM sleep. These findings which suggest that the acrophase of REM sleep is advanced by several hours for a few months after alcohol withdrawal have also been observed in patients with endogenous depression. Although our patients did not show any depressive symptoms during the study, one of them developed a severely depressive state after he began to drink alcohol thereafter.
Key Words: Chronic alcoholics- Alcohol wi thdrawal- REM sleep- Circadian rhythm
INTRODUCTION
The effects of acute alcohol ingestion on the sleep parameters of normal healthy subjects are somewhat inconsistent in previous studies because of
0376-8716/86/$03.50 © Elsevier Scientific Publ ishers Ireland Ltd. Pr inted and Published in Ireland
78
differences in the experimental designs [1]. However, both a decrease in REM sleep [2-7] and an increase in slow wave sleep (SWS) (stages 3 and 4) [5] during alcohol nights, and rebound increases of REM sleep during the withdrawal nights have been reported. On the other hand pronounced changes have been noted after withdrawal from alcohol, i.e. a marked decrease in SWS and an increase in stage 2 sleep persisting for a long period [8-12]. Although stage 1-REM sleep, a stage of sleep concomitant with rapid eye movements and tonic submental EMG, is observed for a few days after cessation of alcohol consumption [11,13-16], little change in the amount of usual REM sleep has been noted except for a few days after alcohol withdrawal [8,10,11].
Recent sleep studies have been carried out taking into account bior- hythm, and Johnson [17] and Zarcone et al. [18] investigated periodicity in the sleep of abstinent alcoholics. As far as we know, however, the distribu- tion of REM episodes occurring in the sleep of abstinent alcoholics has not been reported. As described in the present study we noted a change in the distribution of REM sleep for a few months after alcohol withdrawal.
SUBJECTS AND METHODS
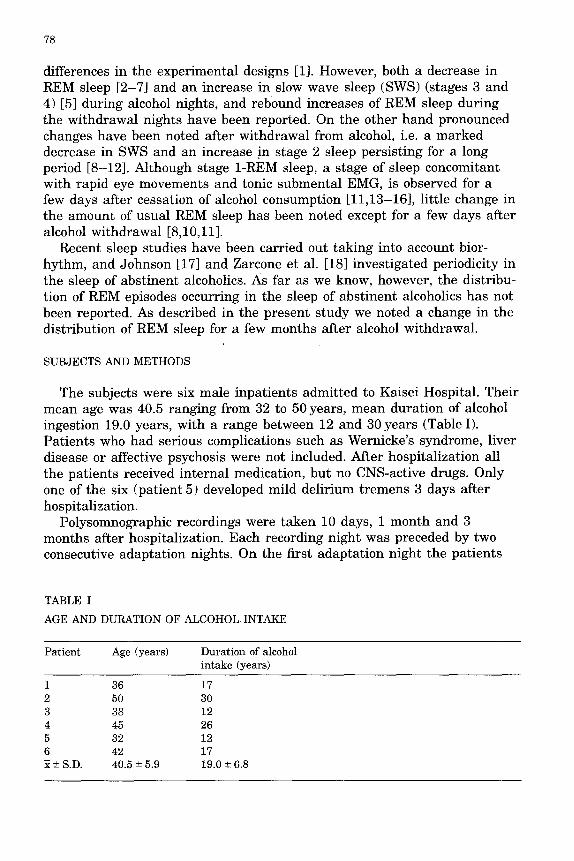
The subjects were six male inpatients admitted to Kaisei Hospital. Their mean age was 40.5 ranging from 32 to 50 years, mean duration of alcohol ingestion 19.0 years, with a range between 12 and 30 years (Table I). Patients who had serious complications such as Wernicke's syndrome, liver disease or affective psychosis were not included. After hospitalization all the patients received internal medication, but no CNS-active drugs. Only one of the six (patient 5) developed mild delirium tremens 3 days after hospitalization.
Polysomnographic recordings were taken 10 days, 1 month and 3 months after hospitalization. Each recording night was preceded by two consecutive adaptation nights. On the first adaptation night the patients
TABLE I
AGE AND DURATION OF ALCOHOL INTAKE
Patient Age (years) Duration of alcohol intake (years)
1 36 17 2 50 30 3 38 12 4 45 26 5 32 12 6 42 17 ~±S.D. 40.5±5.9 19.0±6.8
79
were followed without application of electrodes, but with their application on the second night. Sleep recording and record analysis were performed according to the criteria of Rechtschaffen and Kales [19]. Sleep stage scoring was performed on each 20 s recording by one of the authors who was unaware of the date of the recordings. Recordings were continued from 2230 until the patients awoke spontaneously the next morning. REM latency was est imated as the time from the onset of the first stage 2 sleep to the onset of the first REM episode minus any awakefulness during that interval. Prior to the study the patients were informed of the experimental procedures, and full consent was verbally obtained. A two-tailed t-test was employed in the statistical analysis ot the two related samples.
RESULTS
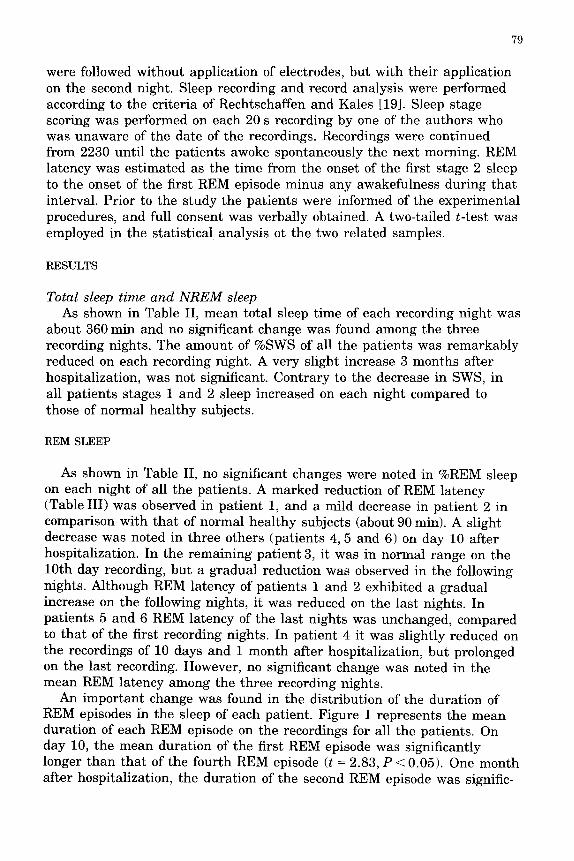
Total sleep time and N R E M sleep As shown in Table II, mean total sleep time of each recording night was
about 360 min and no significant change was found among the three recording nights. The amount of %SWS of all the patients was remarkably reduced on each recording night. A very slight increase 3 months after hospitalization, was not significant. Contrary to the decrease in SWS, in all patients stages 1 and 2 sleep increased on each night compared to those of normal heal thy subjects.
REM SLEEP
As shown in Table II, no significant changes were noted in %REM sleep on each night of all the patients. A marked reduction of REM latency (Table III) was observed in patient 1, and a mild decrease in patient 2 in comparison with that of normal healthy subjects (about 90 rain). A slight decrease was noted in three others (patients 4, 5 and 6) on day 10 after hospitalization. In the remaining patient 3, it was in normal range on the 10th day recording, but a gradual reduction was observed in the following nights. Although REM latency of patients 1 and 2 exhibited a gradual increase on the following nights, it was reduced on the last nights. In patients 5 and 6 REM latency of the last nights was unchanged, compared to that of the first recording nights. In patient 4 it was slightly reduced on the recordings of 10 days and 1 month after hospitalization, but prolonged on the last recording. However, no significant change was noted in the mean REM latency among the three recording nights.
An important change was found in the distribution of the duration of REM episodes in the sleep of each patient. Figure 1 represents the mean duration of each REM episode on the recordings for all the patients. On day 10, the mean duration of the first REM episode was significantly longer than that of the fourth REM episode (t = 2.83, P < 0.05). One month after hospitalization, the duration of the second REM episode was signific-
80
r/3 £ ©
m © O
< c Z 0
m 0
©
O
©
m <
o
N
N
c~
O
N
+1 +[ +1
c~
fN
~ +1
o
bl
m
z
z
© 0
m
z e
R ©
©
£ Z o
M m
e £
g
Z
co +1
o
+1 ao
ao
o,1 +1 ao
+J
81
[ IOD.
3o I
301 I
• I
II III IV
REM Per iods
IM.
5M.
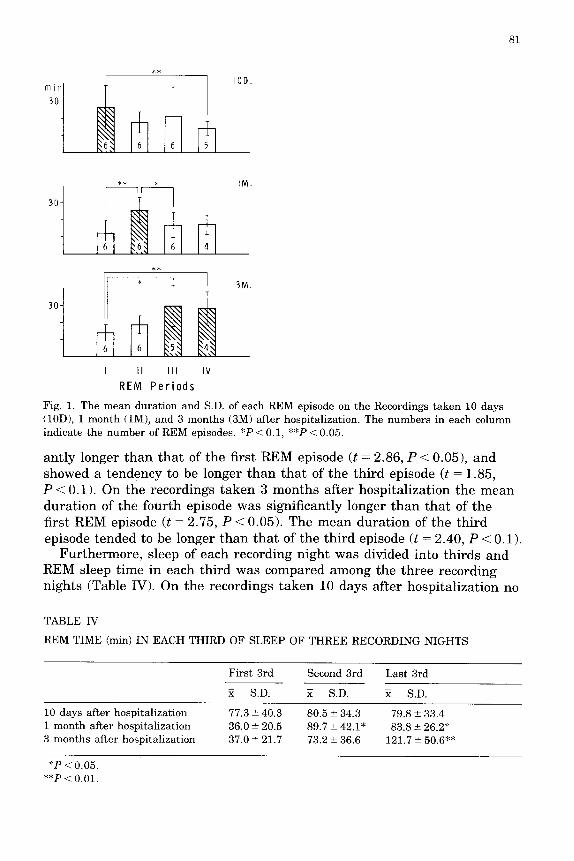
Fig. 1. The m e a n d u r a t i o n a n d S.D. of each R E M episode on t he Record ings t a k e n 10 days (10D), 1 m o n t h (1M), a n d 3 m o n t h s (3M) a f te r hospi ta l iza t ion . The n u m b e r s in each c o l u m n indica te t he n u m b e r of R E M episodes. *P < 0.1, **P < 0.05.
antly longer than that of the first REM episode (t = 2.86, P < 0.05), and showed a tendency to be longer than that of the third episode (t = 1.85, P < 0.1). On the recordings taken 3 months after hospitalization the mean duration of the fourth episode was significantly longer than that of the first REM episode (t = 2.75, P < 0.05). The mean duration of the third episode tended to be longer than that of the third episode (t = 2.40, P < 0.1).
Furthermore, sleep of each recording night was divided into thirds and REM sleep time in each third was compared among the three recording nights (Table IV). On the recordings taken 10 days after hospitalization no
TABLE 1V
REM TIME (min) IN E A C H T HIR D OF S L E E P OF T H R E E R E C O R D I N G N I G H T S
F i r s t 3 rd Second 3rd L a s t 3rd
S.D. ~ S.D. H S.D.
10 days a f te r hosp i t a l i za t ion 1 m o n t h a f te r hosp i t a l i za t ion 3 m o n t h s a f t e r hosp i t a l i za t ion
77.3 +_ 40.3 80.5 -+ 34.3 79.8 +- 33.4 36.0 -+ 20.5 89.7 -+ 42.1" 83.8 -+ 26.2* 37.0 -+ 21.7 73.2 -+ 36.6 121.7 _+ 50.6**
*P < 0.05. **P < 0.01.
82
L .
C ~
m
i
i
i
g
i i
~ b
o
E
c/1
s -
C~
t -
c~
r -
f -
Q
E
c~
iIJ
c ~
Lf%
" T "
~ t
F
. . . . . . . . . _ _ J
-]
~\\\\\\\\~
i
c~
O
E
- - J ~ D -
~ C
r ~
Z
J ~
! mR
m I
~ o _
c~f
t a
o
E
c~
c~ b~
83
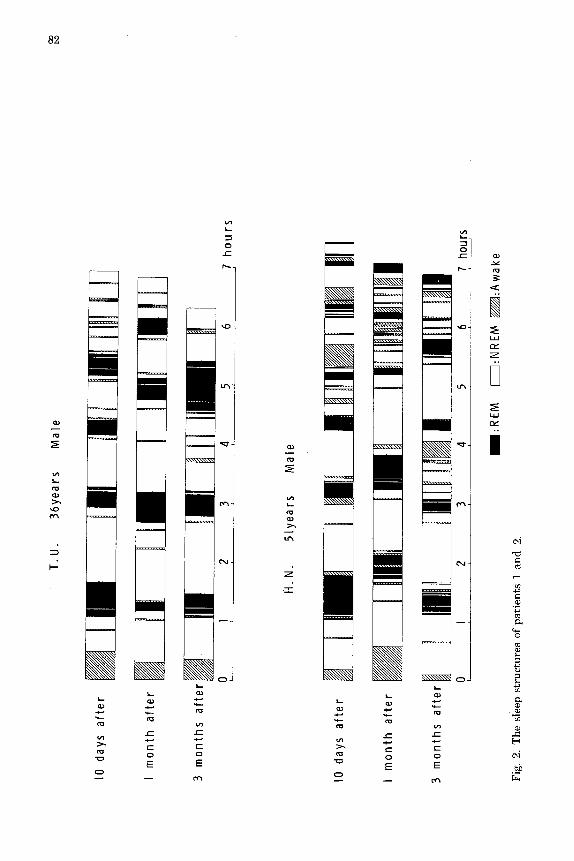
significant change was noted among the REM time in each third. On the recordings taken one month after, however, the REM time in the second (t = 2.60, P < 0.05) and the last third (t -- 2.74, P < 0.05) was significantly higher than that of the first third. On the recordings taken 3 months after, REM time in the last third was significantly higher than that in the first third (t = 4.84, P < 0.01). Figure 2 represents the duration of succes- sive NREM and REM episodes for every night of patients 1 and 2.
Stage 1-REM sleep was not recorded for any of the recording nights of all the patients.
DISCUSSION
Many previous studies in which sleep of withdrawn chronic alcoholics was recorded have paid attention to a marked and prolonged decrease in SWS, but not to changes in the distribution of REM sleep during sleep. We found two notable changes in REM sleep occurring during alcohol with- drawal: an abnormal distribution of REM sleep and a reduction of REM latency. Although REM latency showed interindividual differences, many patients tended to show a decrease in latency on the i0 th day of hospitali- zation when compared to that of normal heal thy subjects, and a few patients showed an increase on the last recording nights. To test the possibility that a decrease of REM latency resulted from a reduction of SWS preceding the first REM episode [20], the possible existence of a correlation was investigated between REM latency and SWS time during the first NREM episode, but no significant correlation was observed be- tween them (r = 0.4316).
(2) An important change was also noted in the distribution of the duration of REM sleep. In normal heal thy subjects, REM sleep has a circadian rhy thm with an acrophase in the early morning [21], i.e. if the subjects follow their usual bed time the duration of REM sleep is minimal in the first REM episode or in the first third of the night's sleep, and then it gradually increases toward the last REM episode in the early morning. In the present study, however, the mean duration of the first REM episode was significantly longer than that of the fourth episode on the 10th day after hospitalization. One month after hospitalization, the mean duration of the second REM episode was maximal and significantly higher than that of the first episode. Three months after hospitalization, the mean duration of the fourth episode was significantly longer than that of the first episode. The abnormal distribution of REM sleep on day 10 and 1 month after hospitalization was also demonstrated by dividing the night sleep into thirds. Although REM time in each third did not differ significantly from the recordings taken on day 10, Rem time in the second and the last thirds was significantly longer than that of the first third 1 month after. Three months after, REM time in the last third was significantly longer than that during the first third. These findings suggest that the acrophase
84
of REM sleep is advanced several hours at least a few months after alcohol withdrawal, in comparison with that of normal healthy subjects. This is, as far as we know, the first observation suggesting an alteration in the circadian rhythm of REM sleep in abstinent alcoholics (though Bfinning and Moser [22] and Enright [23] previously reported that alcohol lengthens the circadian leaf-movement of the bean plant or the endogenous tidal circadian rhythmicity of the isopod). Although sleep recording was not under taken before alcohol withdrawal, it might be supposed that chronic ingestion of alcohol or its withdrawal may affect the circadian pacemaker of REM sleep in human brain. Circadian rhythm has been noted in many biological variables in man, such as sleep-wake cycle, core temperature, plasma level of cortisol, urine volume, and some urine constituents [24,25]. Therefore, further investigations on these variables in chronic alcoholics before and after alcohol withdrawal are indicated.
Reduced REM latency, an increased amount of REM sleep in the first half of the night's sleep and a marked decrease in SWS are also found in patients with endogenous depression [26-28]. The sleep structures obser- ved in the present patients on the 10th day and 1 month after withdrawal are similar to those found in depression, but not to those on the 3 months after because the temporal organization of REM sleep returned to normal while reduced SWS still persisted. In endogenous depression an advanced circadian rhythm has been noted in the sleep-wake cycle (early morning awakening), core temperature, etc. [29,30], and these chronobiological abnormalities are considered to be an important pathogenesis of endogen- ous depression by some researchers [29,30]. Our patients, however, did not complain of early morning awakening, and exhibited neither diurnal change of mood nor depressive symptoms. However, one patient (patient 1) developed a severely depressive state for 2 months and at tempted to commit suicide when he began to consume alcohol after discharged from the hospital. He had had no depressive episodes before and a disposition for depression was not found in his family. Alcoholism is frequently associated with depression [31,32] and Weissman et al. [33] noted secon- dary depression in chronic alcoholics. It is of interest that our patient 1 demonstrated a considerable reduction of REM latency and a marked increase in REM time in the first REM episode on the 10th day after alcohol withdrawal.
ACKNOWLEDGEMENTS
The authors are grateful to Prof. K. Inanaga for his support.
REFERENCES
1 D.C. Kay et al., Human Pharmacology of sleep, in: R.L. Williams and I. Karacan (Eds.), Pharmacology of Sleep, John Wiley & Sons, New York, 1976, pp. 83-210.
85
2 S.C. Gresham et al., Science, 140 (1963) 1226. 3 J.B. Knowles et al., Q.J. Stud. Alcohol, 29 (1969) 324. 4 A.W. MacLean and J. Cairns, in: M.H. Chase, W.C. Stern and P.L. Walter (Eds.), Sleep
Research, Vol. 4, Brain Information Service/Brain Research Institute, University of California, Los Angeles, 1975, p. 107
5 L. Williams et al., in: M.H. Chase, W.C. Stern and P.L. Walter (Eds.), Sleep Research, Vol. 4, Brain Information Service/Brain Research Institute, University of California, Los Angeles, 1975, p. 122.
6 R.B. Yules et al., Electroenceph. Clin. Neurophysiol., 20 (1966) 109. 7 R.B. Yules et al., Arch. Gen. Psychiatry, 16 (1967) 94. 8 J. Adamson and J.A. Burdick, Arch. Gen. Psychiatry, 28 (1973) 146. 9 R.P. Allen et al., J. Nerv. Ment. Dis., 153 (1971) 424.
10 L.C. Johnson et al., Arch. Gen. Psychiatry, 22 (1970) 406. 11 T. Kotorii et al., Folia Psychiat. Neurol. Jpn., 34 (1980) 89. 12 A.M.I. Wagman and R.P. Allen, in: M.M. Gross (Ed.), Alcohol Intoxication and Withdrawal,
Experimental Studies 11, Plenum Press, New York, 1975, pp. 453-466. 13 M.M. Gross et al., J. Nerv. Ment. Dis., 142 (1966) 493. 14 T. Kotorii et al., Drug Alcohol Depend., 10 (1982) 125. 15 Y. Nakazawa et al., Drug Alcohol Depend., 8 (1981) 111. 16 M. Tachibana et al., in: E.D. Weitzman (Ed.), Advances in Sleep Research Vol. 2, Spectrum
Publ., NewYork, 1976, pp. 177-205. 17 L.C. Johnson, in: N. Mello and J.H. Mendelson (Eds.), Recent Advances in the Study of
Alcoholism, Washington, D.C.U.S. Government Printing Office, 1971, pp. 288-316. 18 V. Zarcone et al., in: M.M. Gross (Ed.), Alcohol Intoxication and Withdrawal, Vol. 11,
Plenum Press, New York, 1975, pp. 431-451. 19 A. Rechtschaffen and A. Kales, A manual of standardized terminology, techniques, and
scoring system for sleep stages of human subjects, NHI Publ., Washington, D.C.U.S. Government Printing Office, 1968, pp. 1-62.
20 A. Lubin et al., Psychophysiol, 10 (1973) 27. 21 S. Endo, Sleep, 4 (1981) 319. 22 E. Bfinning and I. Moser, Proc. Natl. Acad. Sci. U.S.A., 70 (1973) 3387. 23 J.T. Enright, Z. Vergl. Physiol., 75 (1971) 332. 24 J. Aschoff, Science, 148 (1965) 1427. 25 J. Vernikos-Danellis et al., Waking Sleeping, 1 (1977) 365. 26 J.C. Gillin et al., Arch. Gen. Psychiatry, 36 (1979) 85. 27 J.C. Gillin et al., Human Neurobiol., 1 (1982) 211. 28 D.J. Kupfer et a l , J. Affect. Disorders, 6 (1984) 43. 29 T.A. Wehr et al., Science, 206 (1979) 710. 30 T.A. Wehr et al., Arch. Gen. Psychiatry, 37 (1980) 257. 31 J.E. Overall et al., Arch. Gen. Psychiatry, 29 (1973) 218. 32 M. Pottenger et al., J. Nerv. Merit. Dis., 166 (1978) 562. 33 M.M. Weissman et al., Arch Gen. Psychiatry, 34 (1977) 854,









![(1935) The advent of Alcoholics Anonymous [ AA ] · 2018. 3. 8. · (1935) The advent of Alcoholics Anonymous [ AA ] (1950) E. M. Jellinek’sresearch postulates that many Alcoholics](https://img.pdfslide.us/doc/110x75/6054a65ff4b14c04b54c5d1b/1935-the-advent-of-alcoholics-anonymous-aa-2018-3-8-1935-the-advent.jpg)