Embed Size (px)
Citation preview

PART I: CIRCADIAN VARIATION IN MYOCARDIAL ISCHEMIA: SILENT MYOCARDIAL ISCHEMIA AND TREATMENT
Circadian patterns of myocardial ischemia
In this overview we studied evidence for the occurrence of silent myocardial ischemia, its pathophysiologic mechanisms, and the circadian distribution of ischemic episodes. The correlation between many hemodynamic parameters and their potential as drug targets was assessed. ECG evidence of myocard,ial ischemia (ST segment), a parameter often used in exercise tests, also occurs during ambulatory monitoring. Use of the isotope rubidium-82 and positron emission tomography helped confirm the significance of these changes in the ST segment, both painful and silent. lschemia was detected by a reduction in the uptake of the isotope in a region of the heart reflecting a decrease in myocardial blood flow. Also it was shown that both painful and silent ischemia are caused by similar pathophysiologic mechanisms; such mechanisms include alterations in coronary blood flow and increases in myocardial oxygen demand. Episodes of ST segment depression show a circadian rhythm similar to that seen for heart rate and catecholamine release. The basic pattern shows a low incidence of ischemia at night, followed by a primary peak on rising, a decrease at midday, and then a secondary peak in the evening, with a final decrease again at night. Similar circadian rhythms have been described for acute cardiovascular events, and this may be important for treatment. (AM HEART J 1989;118:1084.)
Kim Fox, MD, FRCP, David Mulcahy, MD, MRCPI, Jennifer Keegan, and Christine Wright, SRN, London, England
Silent myocardial ischemia can be defined as objec- tive evidence of transient ischemia without the oc- currence of chest pain.l Silent ischemia has been known to occur for many years; however, with in- creasing recognition of its prevalence, information about the prognostic implications and recommenda- tions for treatment are emerging.
THE ROLE OF ST SEGMENT DEPRESSION AS AN INDICATOR OF SILENT MYOCARDIAL ISCHEMIA
When patients with coronary artery disease were studied over a 24-hour period, ST segment depres- sion was observed during periods of chest pain that occurred spontaneously and was detected by ambu- latory ECG monitoring or during treadmill exercise testing. 2, 3 However, ST segment depression can oc- cur without angina1 pain.2s 3
Wood et al.* were the first to describe ST segment depression during exercise as an indicator of ischemia with or without angina. At that time the ST segment changes were unexplained; however, their relation- ship to silent ischemia has recently been clarified.
Improvements in the rate of detection have been
From The National Heart Hospital.
Reprint requests: Kim Fox, The National Heart Hospital, Westmoreland Street, London, WlM 8BA, England.
4/O/ 15298
helped by the use of radionuclide imaging tech- niques. Selwyn et a1.j used the isotope rubidium-82, which was tracked in patients with angina by means of tomographic images taken with a positron camera (positron emission tomography). This technique has the advantage of allowing short-lived changes in the myocardium to be seen. Spontaneously induced ST segment depression was indicated by a defect in up- take of the isotope. The only disadvantage of the technique was that the isotope could only be injected at the onset of ST segment depression, so a variety of methods were needed to induce ST segment depres- sion. Mental stress produced by a simple arithmetic test produces myocardial ischemia that can be seen as ST segment defects.” Mental stress increases ox- ygen demand and systolic and diastolic blood pres- sure; this in turn increases the afterload. These ef- fects can also be triggered by cigarette smoking.8
ARE SILENT AND PAINFUL ISCHEMIA SIGNIFICANTLY DIFFERENT?
In a study of 150 patients with coronary artery disease,g differences between symptomatic and as- ymptomatic angina were observed. Myocardial is- chemia caused either by an excessive increase in my- ocardial demands for oxygen or by vasoconstriction may be accompanied by angina or may be silent. The silent and painful ischemia did not differ in terms of
1084

Volume 118 Number 5, Part 2 Circadian variations in ischemic burden 1005
m Total El a- Silent
01234 5676910 15 16 17 16 19 20
lime of day (hours)
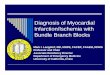
Fig. I. Circadian distribution of total and silent episodes of ischemia. (From Mulcahy D, et al. Lancet 1988;2:755. Reproduced with permission.)
ECG or hemodynamic parameters other than a small difference in the severity of ST segment depression, which appeared to be slightly greater in the episodes of angina.
This evidence suggests that silent ischemia should not be considered as a separate entity from angina pectoris. Cohn’* described the term total ischemic burden, whereby silent and painful episodes of is- chemia are classified as the same condition with the same pathophysiologic mechanisms. Theories pro- posed to explain why some episodes of myocardial ischemia are silent include a suggestion that the stimulus resulting in silent ischemia is quantitatively less than that which provokes painful ischemia,l’ or that patients with silent ischemia have a generalized defect in pain perception and do not recognize symptoms.12
Symptomatic and asymptomatic myocardial is- chemia can be of equivalent severity and duration. Silent ischemia may be caused by a decrease in cor- onary blood flow, an increase in myocardial oxygen demand, or most commonly by a combination of the two. Similarly, unstable angina or acute myocardial infarction produced by thrombosis and platelet ag- gregation may cause episodes of silent ischemia.
CIRCADIAN RHYTHMS IN MYOCARDIAL ISCHEMIA
In a study on forearm blood flow and its relation- ship to heart rate and the onset of ST segment depression, a circadian rhythm in blood flow and vascular resistance was observed; also a circadian
pattern of heart rate and time to onset of ST segment depression was seen. Resistance was at its lowest at 9:00 PM with flow being maximal; in the early hours of the night, resistance increases and thus flow is de- creased.
In a study of the circadian distribution of myocar- dial ischemia in 150 patients,13 it was found that to- tal ischemic burden (painful and silent ischemia) was maximal in the morning, with a trough just after midday followed by a further peak falling off again at night (Fig. 1). Other hemodynamic factors show sim- ilar circadian patterns.
In a study in our department of the circadian dis- tribution of pulmonary diastolic pressure, maximal pressures were observed during the night with lower levels throughout the day.14 This pattern was re- versed when the pattern for plasma epinephrine was observed. Systolic blood pressure was shown to have a similar pattern to that for the total ischemic bur- den, although the secondary peak in the afternoon was smaller in ambulatory patients.15
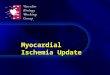
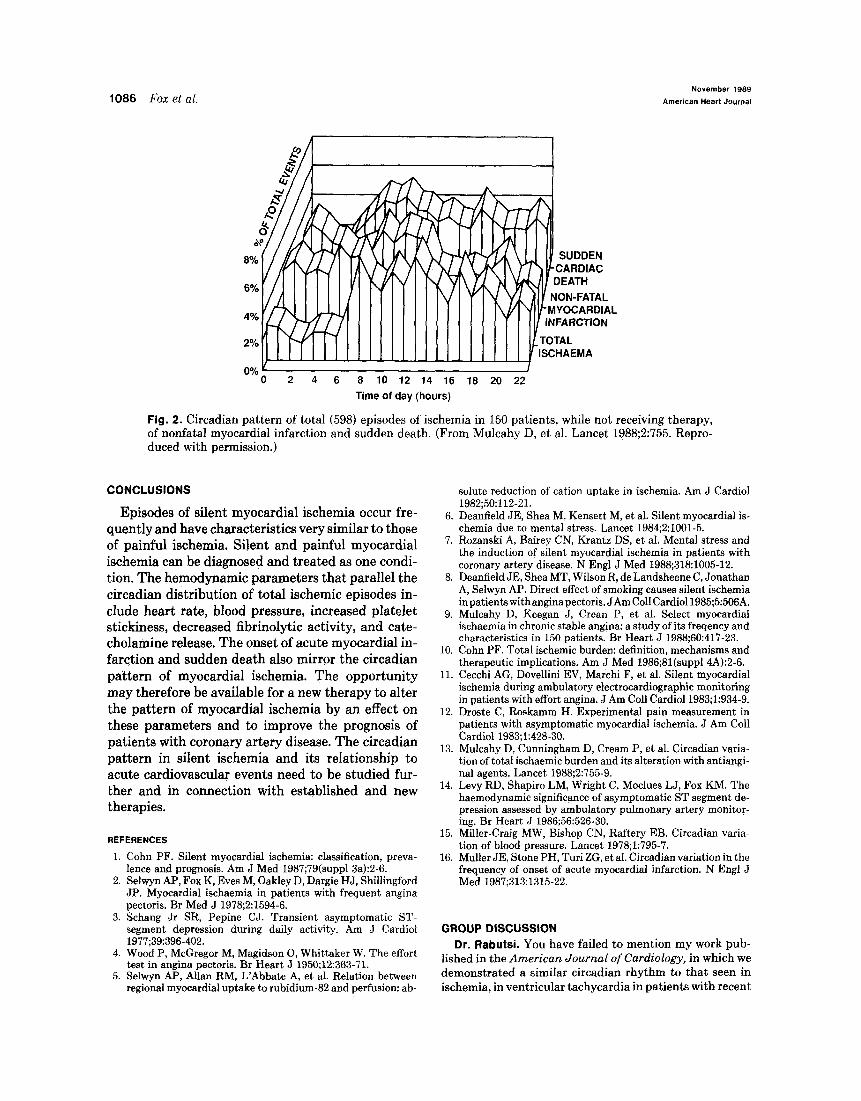
We can see from these findings that there is a cir- cadian pattern to myocardial ischemia, and effective treatment should attempt to alter the distribution of ischemia and flatten the peaks; those treatments should be aimed at coronary blood flow, myocardial oxygen demand, platelet aggregation, and other fac- tors that may promote the generation of this circa- dian distribution. Acute myocardial infarction and sudden cardiac death have been shown to have a similar distribution to ischemic episodes (Fig. 2).16
1086 Fox et al. November 1989
American Heart Journal
I NON-FATAL -MYOCARDIAL
” , ”
0 2 4 6 8 10 12 14 16 18 20 22 Time of day (hours)
Fig. 2. Circadian pattern of total (598) episodes of &hernia in 150 patients, while not receiving therapy, of nonfatal myocardial infarction and sudden death. (From Mulcahy D, et al. Lancet 1988;2:755. Repro- duced with permission.)
CONCLUSIONS
Episodes of silent myocardial ischemia occur fre- quently and have characteristics very similar to those of painful ischemia. Silent and painful myocardial ischemia can be diagnosed and treated as one condi- tion. The hemodynamic parameters that parallel the circadian distribution of total ischemic episodes in- clude heart rate, blood pressure, increased platelet stickiness, decreased fibrinolytic activity, and cate- cholamine release. The onset of acute myocardial in- farction and sudden death also mirror the circadian pattern of myocardial ischemia. The opportunity may therefore be available for a new therapy to alter the pattern of myocardial ischemia by an effect on these parameters and to improve the prognosis of patients with coronary artery disease. The circadian pattern in siIent ischemia and its relationship to acute cardiovascular events need to be studied fur- ther and in connection with established and new therapies.
REFERENCES
1. Cohn PF. Silent myocardial ischemia: classification, preva- lence and prognosis. Am J Med 1987;79(suppl3a):Z-6.
2. Selwyn AP, Fox K, Eves M, Oakley D, Dargie HJ, Shillingford JP. Myocardial ischaemia in patients with frequent angina pectoris. Br Med J 1978;2:1594-6.
3. Schang Jr SR, Pepine CJ. Transient asymptomatic ST- segment depression during daily activity. Am J Cardiol 1977;39:396-402.
4. Wood P, McGregor M, Magidson 0, Whittaker W. The effort test in angina pectoris. Br Heart J 1950;12:363-71.
5. Selwyn AP, Allan RM, L’Abbate A, et al. Relation between regional myocardial uptake to rubidium-82 and perfusion: ab-
solute reduction of cation uptake in ischemia. Am J Cardiol 1982;50:112-21.
6. Deanfield JE, Shea M, Kensett M, et al. Silent myocardial is- chemia due to mental stress. Lancet 1984;2:1001-5.
7. Rozanski A, Bairey CN, Krantz DS, et al. Mental stress and the induction of silent myocardial ischemia in patients with coronary artery disease. N Engl J Med 1988;318:1005-12.
8. Deanfield JE, Shea MT, Wilson R, de Landsheene C, Jonathan A, Selwyn AP. Direct effect of smoking causes silent ischemia inpatients withanginapectoris. JAm Co11 Cardiol1985;5:506A.
9. Mulcahy D, Keegan J, Crean P, et al. Select myocardial ischaemia in chronic stable angjna: a study of its freqency and characteristics in 150 patients. Br Heart J 1988;60:417-23.
10. Cohn PF. Total ischemic burden: definition, mechanisms and therapeutic implications. Am J Med 1986;81(suppl4A):2-6.
11. Cecchi AC, Dovellini EV, Marchi F, et al. Silent myocardial ischemia during ambulatory electrocardiographic monitoring in patients with effort angina. J Am Co11 Cardiol1983;1:934-9.
12. Droste C, Roskamm H. Experimental pain measurement in patients with asymptomatic myocardial ischemia. J Am Co11 Cardiol 1983;1:428-30.
13. Mulcahy D, Cunningham D, Cream P, et al. Circadian varia- tion of total ischaemic burden and its alteration with antiangi- nal agents. Lancet 1988;2:755-9.
14. Levy RD, Shapiro LM, Wright C, Moclues LJ, Fox KM. The haemodynamic significance of asymptomatic ST segment de- pression assessed by ambulatory pulmonary artery monitor- ing. Br Heart J 1986;56:526-30.
15. Miller-Craig MW, Bishop CN, Raftery EB. Circadian varia- tion of blood pressure. Lancet 1978;1:795-7.
16. Muller JE, Stone PH, Turi ZG, et al. Circadian variation in the frequency of onset of acute myocardial infarction. N Engl J Med 1987;313:1315-22.
GROUP DISCUSSION Dr. Rabutsi. You have failed to mention my work pub-
lished in the American Journal of Cardiology, in which we demonstrated a similar circadian rhythm to that seen in ischemia, in ventricular tachycardia in patients with recent

Volume 110
Number 5, Part 2 Circadian variations in ischemic burden
or nonrecent myocardial infarction. In another study pub- lished in part in the European Heart Journal, although a circadian distribution of thromboxane Bs production was observed in normal subjects, no significant rhythm was seen in patients with unstable angina except for a peak in the morning.
K. Fox. In unstable angina it is difficult to demonstrate a circadian pattern, because unstable angina itself may in- terfere with the circadian distribution of thromboxane Bs, raising the question of whether the changes in thrombox- ane Bs are cause or effect.
Silent myocardial ischemia
Myocardial ischemia can manifest itself as strictly silent or a combination of symptomatic and silent episodes. We have demonstrated that most asymptomatic patients have a higher threshold for pain than did symptomatic patients. Low sensitivity to pain in patients with silent ischemia may be related to both a neural pain inhibitory system and the release of endogenous opiates, the endorphins. &Endorphin release occurs during and after exercise; patients with asymptomatic ischemia had higher plasma ,&endorphin levels than did patients with symptomatic ischemia, especially during exercise. With naloxone treatment, the pain threshold of patients with silent myocardial ischemia (!%I) can be reduced to the same values as those of symptomatic patients. This supports the possibility of a role for endorphins in SM. Patients who experience both asymptomatic and symptomatic lschemic episodes do so because their pain threshold and endorphin regulatory system varies throughout the day and because severity and duration of ischemic episodes are different. Although there is controversy over the appropriate therapy for SMI, it is more likely that this should simply be treated in the same way as painful lschemia. (Au HEART J 1989; 118: 1087.)
Conrad Droste, MD, PhD,* and Helmut Roskamm, MD, Bad Krozingen, West Germany
Angina pectoris is a pain syndrome induced by my- ocardial ischemia that may present as typical or atypical angina pectoris. In some patients dyspnea can be considered an angina1 equivalent. At the end of this spectrum are patients with no symptoms of angina pectoris, although ischemia can be proved with different methods; this is called asymptomatic or silent myocardial ischemia @MI).
PATHOPHYSIOLOGY
Regarding pathophysiology, there are two differ- ent clinical pictures of silent ischemia: (1) patients with silent ischemia whose ischemia is always silent
From the Rehabilitationszentrum fiir Herzund Kreislaufkranke. Reprint requests: H. Roskamm, MD, Medical Director, Rehabilitationszen- trum fiir Herzund Kreislaufkranke, D-7812 Bad Krozingen, West Ger- many. *Supported by the Deutsche Forschungsgemeinschaft (SP-II B7-Dr 190 l- a. 4/o/15299
and (2) silent ischemic episodes in otherwise symp- tomatic patients.
In patients who are totally asymptomatic, a more individual, patient-related factor can be expected to be responsible for the lack of pain. To examine this theory, we investigated 30 patients with SMI and compared them with 30 patients who had symptom- atic myocardial ischemia.’ All patients had severe coronary artery disease with more than 70% stenosis in at least one vessel. In addition, all patients dem- onstrated substantial ST segment depression during several exercise tests. Vessel involvement, risk factor constellation, and functional variables (e.g., exercise tolerance, etc.) were not different between the symp- tomatic and the asymptomatic group.
Three different tests were used for experimental pain measurement. In an electrical pain test as described by Notermans,2 the magnitude of current in milliamperes that was sufficient to induce pain was measured. Most patients with SMI had a higher pain
1087