Embed Size (px)
Citation preview
Cigarette Smoking and Alveolar Bonein Young Adults: A Study UsingDigitized RadiographsGuillermo M. Rosa,* Gabriela Q. Lucas,†‡ and Oscar N. Lucas‡§
Background: Evidence indicates that cigarette smoking is one of the most significant risk factors for peri-odontal diseases; however, there have been few radiographic prospective studies of alveolar bone in youngpopulations. The purpose of this study was to evaluate the effect of smoking on alveolar bone in youngadults.
Methods: Eighty-one dental students (mean age: 20.5 years), considered not to have periodontitisaccording to clinical criteria, participated in this study. Forty-two subjects were smokers (mean consump-tion was 14.1 cigarettes/day for ‡2 years), and 39 subjects had never smoked. A parallel-arm prospectivedesign was used. All subjects took part in a dental hygiene program (DHP) that included oral hygiene in-structions, mechanical debridement, and polishing. The following clinical variables were measured beforeand after the DHP: plaque index (PI), gingival crevicular fluid (GCF) flow rate, gingival index (GI), probingdepth, and clinical attachment level (CAL). Standardized posterior vertical bitewing radiographs were takenand digitized preexperimentally and on days 180, 365, and 545. The following analyses were performed:bone height measurement (BHM), computer-assisted densitometric image analysis (CADIA), and qualita-tive analysis of digital subtraction radiography (DSR). Repeated-measures multiple-way analysis of vari-ance (ANOVA) was performed between the groups, and one-way ANOVA was performed within the groups.
Results: The mean PI and GI were significantly greater in the smokers (P <0.01). The mean GCF flow ratewas significantly lower in the smokers (P <0.01). CAL and the number of sites with recession were signifi-cantly greater in the smokers (P <0.001). The BHM indicated a significantly lower mean alveolar bone heightin the smokers (P <0.01). The smokers showed significantly lower CADIA values, which indicated a lowerbone density on days 0 (P <0.05), 180, 365, and 545 (P <0.01). CADIA values decreased during the studyin the smokers, with significant differences on day 545 (P <0.05). The smokers had a significantly highermean percentage of sites that had decreased density, as assessed by DSR (P <0.001). In the smokers,the mean percentage of sites with decreased density, as assessed by DSR, had increased significantly bydays 365 (P <0.05) and 545 (P <0.01).
Conclusions: Smoking produces an adverse effect on clinical periodontal variables and alveolar boneheight and density, acting as a potential risk factor for alveolar bone loss, even at an early age with low to-bacco consumption. It is very important to inform young smokers about the risk of this habit in relation toperiodontal health. J Periodontol 2008;79:232-244.
KEY WORDS
Alveolar bone loss/etiology; image analysis, computer-assisted; periodontal diseases/etiology;radiography, dental, digital; risk factors; smoking/adverse effects.
* Currently, Department of Research, Graduate School Foundation, Resistencia, Chaco, Argentina; previously, Department of Physiology, School ofDentistry, National University of the Northeast, Corrientes, Argentina.
† Department of Pediatric Dentistry, School of Dentistry, National University of the Northeast.‡ Department of Research, Graduate School Foundation.§ Health Sciences Graduate School, Catholic University of Salta, Salta, Argentina.
doi: 10.1902/jop.2008.060522
Volume 79 • Number 2
232

It has been clearly demonstrated that the mainetiologic factor in periodontal diseases is the in-fection produced by dental plaque. Furthermore,
evidence indicates that a number of risk factors af-fect the initiation and progression of periodontal dis-eases. These risk factors can modify the protectiveand destructive host responses as well as the path-ogenic flora.1,2 Considerable evidence from epide-miological research3,4 indicates that tobaccosmoking is related directly to the incidence and prev-alence of a variety of medical problems includingcancer, cardiovascular diseases, chronic obstructivepulmonary disease, and low birth weight. In addition,smoking seems to be one of the most significant riskfactors in the development and progression of peri-odontal disease.1,5,6 The postulated mechanisms ofincreased periodontal disease progression in smok-ers include alterations in the host response, such asreductions in serum immunoglobulin (Ig) G2 levels,7
and impairment of various neutrophil functions, suchas phagocytosis8 and aerobic antimicrobial func-tions.9 Other reported effects of smoking on the peri-odontium are suppression of fibroblast and osteoblastfunctions,10,11 alterations in gingival blood flow,5 andreductions in the gingival crevicular fluid flow.5,12
It has been well documented by meta-analyses thatsmoking adversely affects bone13,14 by reducingbone mineral content.15 Law and Hackshaw16 re-ported an increased risk for fractures in smokers,and smoking is considered to be a risk factor for oste-oporosis.17 Because bone is one of the tissues that ismost affected by periodontal diseases, it is very im-portant to diagnose periodontal disease and followits progression. The study of alveolar bone by intraoralradiographs provides information that cannot be ac-quired by any other non-invasive method.18 In recentyears, many computer-assisted radiographic imagecapture and analysis methods have been developed,validated, and applied in many fields through clinicaland animal model research.19-24
Although the harmful effect of smoking on overallgeneral health is well established, people continueto smoke. Also, the association between cigarettesmoking and periodontal diseases represents a signif-icant oral health problem.5 Most of the previous stud-ies2,5-7 on tobacco smoking and periodontal diseasesfocused on adult populations of smokers, mostly withsevere forms of periodontal diseases in whom smok-ing of long duration, age, general health problems,and other risk factors may coexist. The impact of cig-arette smoking on the overall prevalence of periodon-titis in a young adult population has gathered someattention in the last decade, and some studies haveevaluated the relationship between smoking and peri-odontal tissues in young adults. The associationbetween smoking and periodontal bone loss was re-
ported by Mullally et al.25 in young subjects diagnosedwith aggressive periodontitis. Recently, a relativelyhigh prevalence of aggressive periodontitis associ-ated with smoking, among others risk factors, wasfound in young Israeli army recruits by Levin et al.26
and in an urban population in southern Brazil by Susinand Albandar.27 Additionally, tooth loss was found tobe associated with smoking in young adults.28,29
These studies raise some concerns about the possibledamage to periodontal tissues that have been ex-posed to tobacco for a short time in young smokers.Some cross-sectional studies30-33 evaluated the rela-tionship between smoking and periodontal clinicalparameters in young individuals with minimal or noperiodontal destruction. A case-control study34 re-ported that smoking was a major factor associatedwith periodontal destruction in a group of youngJordanian adults. This is of major concern becausethe prevalence of smoking in young adults and ado-lescents, especially in young women, is not decreas-ing in some developing countries such as Argentina,Chile, and Brazil.35 Most previous studies27,28,30,32,34
on smoking in young adults used cross-sectional ex-perimental designs in which clinical parameters wereevaluated. There is little information available fromprospective studies about periodontal condition andalveolar bone loss in young smokers.
The aim of this prospective study was to evaluatethe effect of smoking on alveolar bone in young adultswith a few years of tobacco consumption. This wasdone using computer-assisted techniques for themeasurement of digitized radiographs.
MATERIALS AND METHODS
Experimental SubjectsThe experimental subjects were selected randomlybetween 2001 and 2002 from second-year dental stu-dents who were invited to join this study at the Schoolof Dentistry, National University of the Northeast.Each subject completed a questionnaire and had aroutine oral and periodontal examination. The ques-tionnaire gathered demographic information, a detaileddental-medical history, and smoking information.The inclusion criteria were: subjects aged between17 and 26 years without any dental complaints; sub-jects having all premolars and molars (excluding thirdmolars); and subjects considered not to have peri-odontitis, as identified by clinical examination, accord-ing to the following criteria: no more than one toothwith a site of interproximal attachment loss ‡2 mm,and the site could not have probing depth (PD) >3mm. Additionally, subjects could have attachmentloss associated with recession.31 The exclusion criteriawere: medical conditions that required treatment withantibiotics, steroids, or non-steroidal anti-inflammatory
J Periodontol • February 2008 Rosa, Lucas, Lucas
233

drugs; a systemic disease that might affect the peri-odontal condition, e.g., diabetes mellitus or acquiredimmunodeficiency syndrome; individuals who had re-ceived periodontal therapy in the previous year or whoregularly used local antimicrobial chemical agents;subjects who were undergoing orthodontic treatment;and known pregnancy. Therefore, the subjects were asample of well-motivated young dental attenders un-dergoing routine dental care.30
Cigarette smoking status was obtained from a writ-ten questionnaire completed by each subject, whichwas reported to be a valid method for estimatingsmoking prevalence.36,37 Subjects were consideredsmokers if they had been smoking ‡10 cigarettes aday38 for at least the last 2 years. Table 1 shows thedemographic characteristics of the 81 selected sub-jects who agreed to participate and fulfilled the estab-lished criteria. They were categorized into two groups.The smokers consisted of 42 individuals who reportedconsuming a mean of 14.1 cigarettes/day for a meanof 4.3 years (range: 2 to 8 years). The non-smokersincluded 39 subjects who responded that they hadnever smoked. Former smokers were not includedin the study. The mean age was almost the same inboth groups, and all subjects were white.
This research project was approved by the Re-search and Human Rights Committee, School of Den-tistry, National University of the Northeast and theDoctoral Theses Committee, School of Dentistry, Na-tional University of Cordoba, Cordoba, Argentina. Itwas conducted in accordance with the Helsinki Dec-laration of 1975, as revised in 2000. Every step ofthe study was explained to all of the subjects, and itwas stated clearly that their participation was volun-tary. Written informed consent was obtained fromall subjects to participate and to have their radio-graphs examined as part of the study.
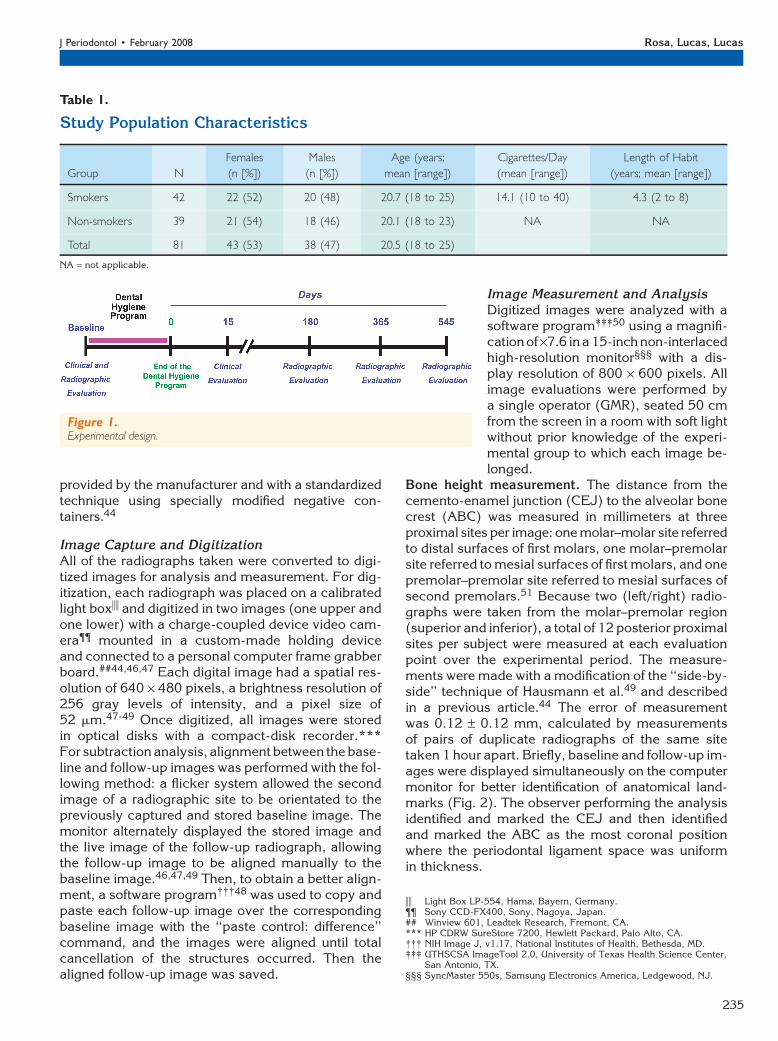
Experimental DesignA parallel-arm prospective design was used (Fig. 1).After enrollment in the study, all individuals wereevaluated clinically and radiographically (baselineevaluation). Then, with the purpose of obtaining auniform periodontal status, all subjects underwent arigorous dental hygiene program (DHP). The DHPconsisted of approximately two sessions per week,for 3 weeks, of oral hygiene instructions (brushingand flossing), scaling (quadrant by quadrant at 1-weekintervals and using selected hand instruments), andpolishing with rotary instruments. The endpoint ofthe mechanical treatment included removal of supra-gingival and subgingival calculus and stain to achievea smooth surface. Fifteen days later, a second clinicalevaluation was performed to assess the effect of theDHP on baseline periodontal status. After this, eachsubject continued throughout the study with a per-
sonal oral hygiene routine (as instructed during theDHP) and with no professional periodontal mainte-nance. On days 180, 365, and 545, standardized pos-terior vertical bitewing radiographs were taken, andradiographic variables were evaluated. At the end ofthe study, periodontal therapy was performed asneeded. The exit criteria during the study were: allthe exclusion criteria established for enrollment inthe study, a reported change in smoking habits (re-viewed at each session), appearance of proximal car-ies diagnosed by bitewing radiographs, and theappearance of any adverse effects that required addi-tional treatment.
Clinical MeasurementsAll subjects were examined by a single observer(GMR) using a University of North Carolina straightperiodontal probe.i39 The vestibular and lingual sur-faces of eight teeth (upper and lower first molarsand upper and lower second premolars) were selectedfor this study. The presence of dental plaque was re-corded using the Silness and Loe plaque index (PI).40
Clinical gingival inflammation was evaluated in me-sial, central, and distal areas of the vestibular and lin-gual surface using the Loe gingival index (GI).41 Thegingival crevicular fluid (GCF) flow rate was measuredfollowing a standard technique.12 GCF was collectedfor 60 seconds with standard filter papers strips¶ andmeasured immediately with a measuring device.#42
PD30,31,39 and clinical attachment level (CAL)30,39,43
were measured. Theprobing measurementsweremadein millimeters at six sites per tooth (disto-buccal, buc-cal, mesio-buccal, disto-lingual, lingual, and mesio-lingual).39 Forty-eight sites were evaluated in eachsubject. The number of sites with gingival recessionwas calculated for each subject.
Radiographic Bitewing TechniqueThe radiographic and measurement techniques weredescribed in detail previously and evaluated in termsof their reproducibility.44 In brief, intraoral D speedand size #2 dental film** was used in a standardizedway with a modified posterior vertical bitewing align-ment device.††44,45 Only one dental x-rayequipment‡‡
was used, with the exposure parameters fixed at60 kV(p), 15 mA, and 1 second. For each subject,two radiographs (left/right) were taken from themolar–premolar region at each evaluation. Film pro-cessing was done with fresh solutions of chemicals§§
following the time/temperature table for 26.5�C
i University of North Carolina Probe, UNC15 – XPTU 17/15, Hu-Friedy,Chicago, IL.
¶ Periopaper, OraFlow, Plainview, New York.# Periotron 8000, OraFlow.** D speed Intraoral Film, Eastman Kodak, Rochester, NY.†† XCP bite-wing instrument, Rinn Manufacturing, Elgin, IL.‡‡ DSJ X Ray Dental Equipment, Dental San Justo, Buenos Aires,
Argentina.§§ Kodak GBX Chemicals, Eastman Kodak.
Cigarette Smoking and Alveolar Bone in Young Adults Volume 79 • Number 2
234
provided by the manufacturer and with a standardizedtechnique using specially modified negative con-tainers.44
Image Capture and DigitizationAll of the radiographs taken were converted to digi-tized images for analysis and measurement. For dig-itization, each radiograph was placed on a calibratedlight boxii and digitized in two images (one upper andone lower) with a charge-coupled device video cam-era¶¶ mounted in a custom-made holding deviceand connected to a personal computer frame grabberboard.##44,46,47 Each digital image had a spatial res-olution of 640 · 480 pixels, a brightness resolution of256 gray levels of intensity, and a pixel size of52 mm.47-49 Once digitized, all images were storedin optical disks with a compact-disk recorder.***For subtraction analysis, alignment between the base-line and follow-up images was performed with the fol-lowing method: a flicker system allowed the secondimage of a radiographic site to be orientated to thepreviously captured and stored baseline image. Themonitor alternately displayed the stored image andthe live image of the follow-up radiograph, allowingthe follow-up image to be aligned manually to thebaseline image.46,47,49 Then, to obtain a better align-ment, a software program†††48 was used to copy andpaste each follow-up image over the correspondingbaseline image with the ‘‘paste control: difference’’command, and the images were aligned until totalcancellation of the structures occurred. Then thealigned follow-up image was saved.
Image Measurement and AnalysisDigitized images were analyzed with asoftware program‡‡‡50 using a magnifi-cationof ·7.6 ina 15-inch non-interlacedhigh-resolution monitor§§§ with a dis-play resolution of 800 · 600 pixels. Allimage evaluations were performed bya single operator (GMR), seated 50 cmfrom the screen in a room with soft lightwithout prior knowledge of the experi-mental group to which each image be-longed.
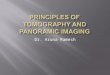
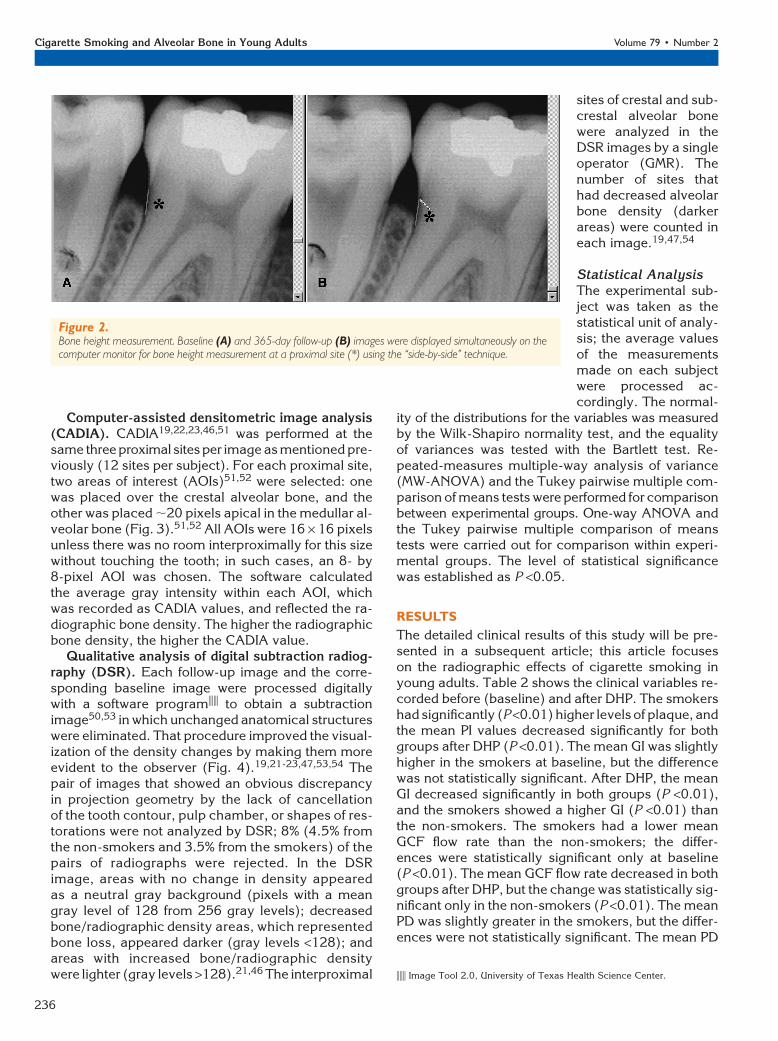
Bone height measurement. The distance from thecemento-enamel junction (CEJ) to the alveolar bonecrest (ABC) was measured in millimeters at threeproximal sites per image: one molar–molar site referredto distal surfaces of first molars, one molar–premolarsite referred to mesial surfaces of first molars, and onepremolar–premolar site referred to mesial surfaces ofsecond premolars.51 Because two (left/right) radio-graphs were taken from the molar–premolar region(superior and inferior), a total of 12 posterior proximalsites per subject were measured at each evaluationpoint over the experimental period. The measure-ments were made with a modification of the ‘‘side-by-side’’ technique of Hausmann et al.49 and describedin a previous article.44 The error of measurementwas 0.12 – 0.12 mm, calculated by measurementsof pairs of duplicate radiographs of the same sitetaken 1 hour apart. Briefly, baseline and follow-up im-ages were displayed simultaneously on the computermonitor for better identification of anatomical land-marks (Fig. 2). The observer performing the analysisidentified and marked the CEJ and then identifiedand marked the ABC as the most coronal positionwhere the periodontal ligament space was uniformin thickness.
Figure 1.Experimental design.
Table 1.
Study Population Characteristics
Group N
Females
(n [%])
Males
(n [%])
Age (years;
mean [range])
Cigarettes/Day
(mean [range])
Length of Habit
(years; mean [range])
Smokers 42 22 (52) 20 (48) 20.7 (18 to 25) 14.1 (10 to 40) 4.3 (2 to 8)
Non-smokers 39 21 (54) 18 (46) 20.1 (18 to 23) NA NA
Total 81 43 (53) 38 (47) 20.5 (18 to 25)
NA = not applicable.
ii Light Box LP-554, Hama, Bayern, Germany.¶¶ Sony CCD-FX400, Sony, Nagoya, Japan.## Winview 601, Leadtek Research, Fremont, CA.*** HP CDRW SureStore 7200, Hewlett Packard, Palo Alto, CA.††† NIH Image J, v1.17, National Institutes of Health, Bethesda, MD.‡‡‡ UTHSCSA ImageTool 2.0, University of Texas Health Science Center,
San Antonio, TX.§§§ SyncMaster 550s, Samsung Electronics America, Ledgewood, NJ.
J Periodontol • February 2008 Rosa, Lucas, Lucas
235
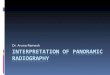
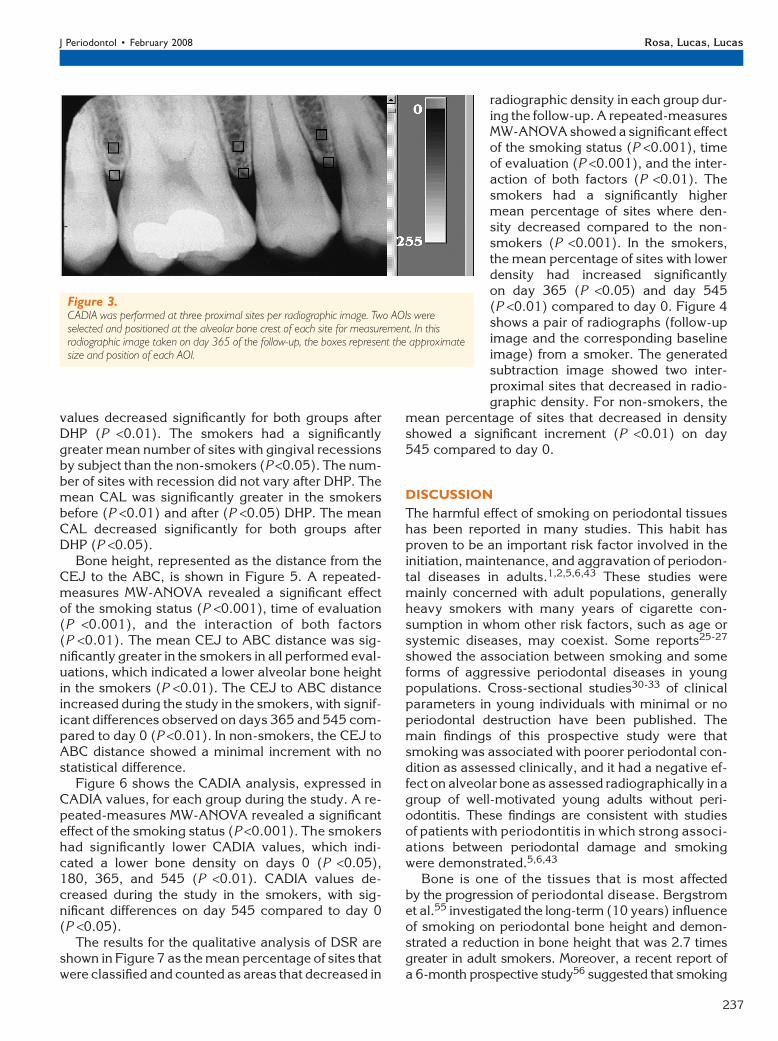
Computer-assisted densitometric image analysis(CADIA). CADIA19,22,23,46,51 was performed at thesame threeproximal sitesper image as mentioned pre-viously (12 sites per subject). For each proximal site,two areas of interest (AOIs)51,52 were selected: onewas placed over the crestal alveolar bone, and theother was placed ;20 pixels apical in the medullar al-veolar bone (Fig. 3).51,52 All AOIs were 16 · 16 pixelsunless there was no room interproximally for this sizewithout touching the tooth; in such cases, an 8- by8-pixel AOI was chosen. The software calculatedthe average gray intensity within each AOI, whichwas recorded as CADIA values, and reflected the ra-diographic bone density. The higher the radiographicbone density, the higher the CADIA value.
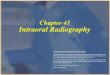
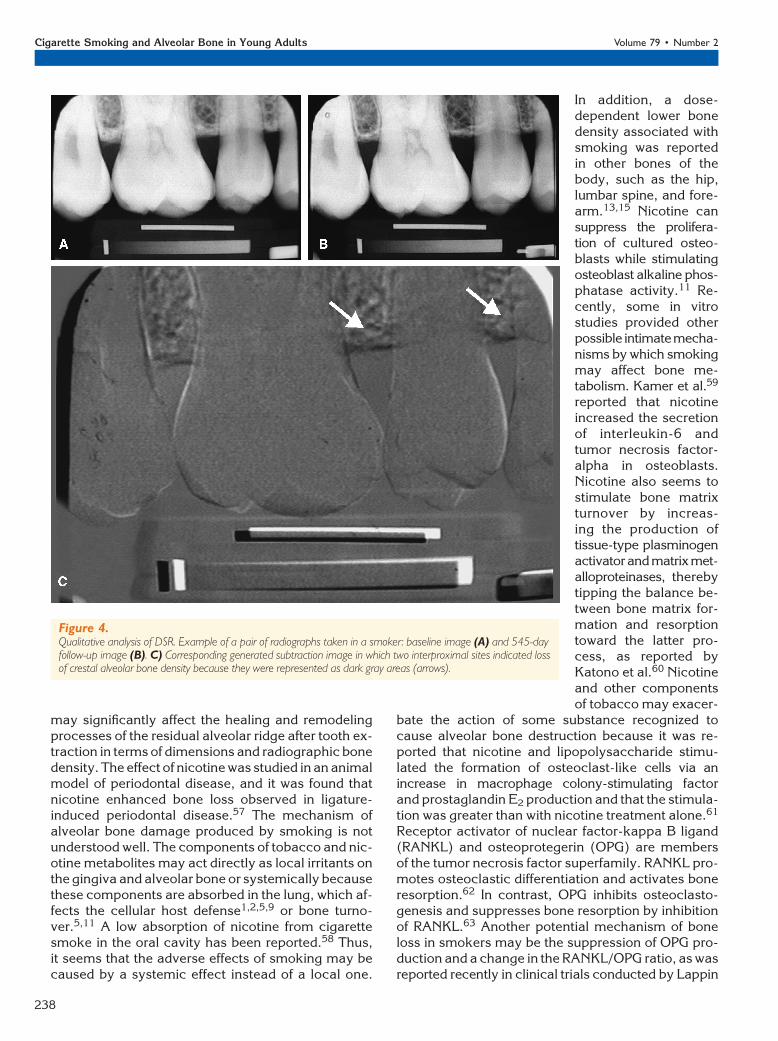
Qualitative analysis of digital subtraction radiog-raphy (DSR). Each follow-up image and the corre-sponding baseline image were processed digitallywith a software programiii to obtain a subtractionimage50,53 in which unchanged anatomical structureswere eliminated. That procedure improved the visual-ization of the density changes by making them moreevident to the observer (Fig. 4).19,21-23,47,53,54 Thepair of images that showed an obvious discrepancyin projection geometry by the lack of cancellationof the tooth contour, pulp chamber, or shapes of res-torations were not analyzed by DSR; 8% (4.5% fromthe non-smokers and 3.5% from the smokers) of thepairs of radiographs were rejected. In the DSRimage, areas with no change in density appearedas a neutral gray background (pixels with a meangray level of 128 from 256 gray levels); decreasedbone/radiographic density areas, which representedbone loss, appeared darker (gray levels <128); andareas with increased bone/radiographic densitywere lighter (gray levels >128).21,46 The interproximal
sites of crestal and sub-crestal alveolar bonewere analyzed in theDSR images by a singleoperator (GMR). Thenumber of sites thathad decreased alveolarbone density (darkerareas) were counted ineach image.19,47,54
Statistical AnalysisThe experimental sub-ject was taken as thestatistical unit of analy-sis; the average valuesof the measurementsmade on each subjectwere processed ac-cordingly. The normal-
ity of the distributions for the variables was measuredby the Wilk-Shapiro normality test, and the equalityof variances was tested with the Bartlett test. Re-peated-measures multiple-way analysis of variance(MW-ANOVA) and the Tukey pairwise multiple com-parison of means tests were performed for comparisonbetween experimental groups. One-way ANOVA andthe Tukey pairwise multiple comparison of meanstests were carried out for comparison within experi-mental groups. The level of statistical significancewas established as P <0.05.
RESULTS
The detailed clinical results of this study will be pre-sented in a subsequent article; this article focuseson the radiographic effects of cigarette smoking inyoung adults. Table 2 shows the clinical variables re-corded before (baseline) and after DHP. The smokershad significantly (P <0.01) higher levels of plaque, andthe mean PI values decreased significantly for bothgroups after DHP (P <0.01). The mean GI was slightlyhigher in the smokers at baseline, but the differencewas not statistically significant. After DHP, the meanGI decreased significantly in both groups (P <0.01),and the smokers showed a higher GI (P <0.01) thanthe non-smokers. The smokers had a lower meanGCF flow rate than the non-smokers; the differ-ences were statistically significant only at baseline(P <0.01). The mean GCF flow rate decreased in bothgroups after DHP, but the change was statistically sig-nificant only in the non-smokers (P <0.01). The meanPD was slightly greater in the smokers, but the differ-ences were not statistically significant. The mean PD
Figure 2.Bone height measurement. Baseline (A) and 365-day follow-up (B) images were displayed simultaneously on thecomputer monitor for bone height measurement at a proximal site (*) using the ‘‘side-by-side’’ technique.
iii Image Tool 2.0, University of Texas Health Science Center.
Cigarette Smoking and Alveolar Bone in Young Adults Volume 79 • Number 2
236
values decreased significantly for both groups afterDHP (P <0.01). The smokers had a significantlygreater mean number of sites with gingival recessionsby subject than the non-smokers (P <0.05). The num-ber of sites with recession did not vary after DHP. Themean CAL was significantly greater in the smokersbefore (P <0.01) and after (P <0.05) DHP. The meanCAL decreased significantly for both groups afterDHP (P <0.05).
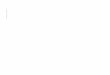
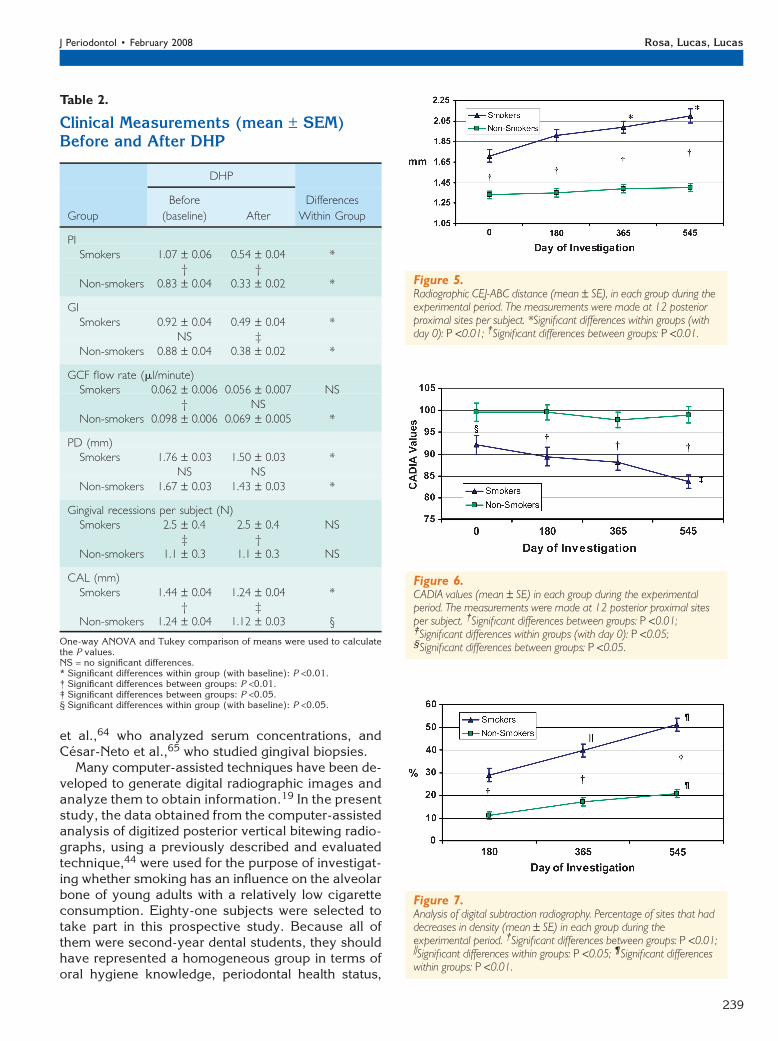
Bone height, represented as the distance from theCEJ to the ABC, is shown in Figure 5. A repeated-measures MW-ANOVA revealed a significant effectof the smoking status (P <0.001), time of evaluation(P <0.001), and the interaction of both factors(P <0.01). The mean CEJ to ABC distance was sig-nificantly greater in the smokers in all performed eval-uations, which indicated a lower alveolar bone heightin the smokers (P <0.01). The CEJ to ABC distanceincreased during the study in the smokers, with signif-icant differences observed on days 365 and 545 com-pared to day 0 (P <0.01). In non-smokers, the CEJ toABC distance showed a minimal increment with nostatistical difference.
Figure 6 shows the CADIA analysis, expressed inCADIA values, for each group during the study. A re-peated-measures MW-ANOVA revealed a significanteffect of the smoking status (P <0.001). The smokershad significantly lower CADIA values, which indi-cated a lower bone density on days 0 (P <0.05),180, 365, and 545 (P <0.01). CADIA values de-creased during the study in the smokers, with sig-nificant differences on day 545 compared to day 0(P <0.05).
The results for the qualitative analysis of DSR areshown in Figure 7 as the mean percentage of sites thatwere classified and counted as areas that decreased in
radiographic density in each group dur-ing the follow-up. A repeated-measuresMW-ANOVA showed a significant effectof the smoking status (P <0.001), timeof evaluation (P <0.001), and the inter-action of both factors (P <0.01). Thesmokers had a significantly highermean percentage of sites where den-sity decreased compared to the non-smokers (P <0.001). In the smokers,the mean percentage of sites with lowerdensity had increased significantlyon day 365 (P <0.05) and day 545(P <0.01) compared to day 0. Figure 4shows a pair of radiographs (follow-upimage and the corresponding baselineimage) from a smoker. The generatedsubtraction image showed two inter-proximal sites that decreased in radio-graphic density. For non-smokers, the
mean percentage of sites that decreased in densityshowed a significant increment (P <0.01) on day545 compared to day 0.
DISCUSSION
The harmful effect of smoking on periodontal tissueshas been reported in many studies. This habit hasproven to be an important risk factor involved in theinitiation, maintenance, and aggravation of periodon-tal diseases in adults.1,2,5,6,43 These studies weremainly concerned with adult populations, generallyheavy smokers with many years of cigarette con-sumption in whom other risk factors, such as age orsystemic diseases, may coexist. Some reports25-27
showed the association between smoking and someforms of aggressive periodontal diseases in youngpopulations. Cross-sectional studies30-33 of clinicalparameters in young individuals with minimal or noperiodontal destruction have been published. Themain findings of this prospective study were thatsmoking was associated with poorer periodontal con-dition as assessed clinically, and it had a negative ef-fect on alveolar bone as assessed radiographically in agroup of well-motivated young adults without peri-odontitis. These findings are consistent with studiesof patients with periodontitis in which strong associ-ations between periodontal damage and smokingwere demonstrated.5,6,43
Bone is one of the tissues that is most affectedby the progression of periodontal disease. Bergstromet al.55 investigated the long-term (10 years) influenceof smoking on periodontal bone height and demon-strated a reduction in bone height that was 2.7 timesgreater in adult smokers. Moreover, a recent report ofa 6-month prospective study56 suggested that smoking
Figure 3.CADIA was performed at three proximal sites per radiographic image. Two AOIs wereselected and positioned at the alveolar bone crest of each site for measurement. In thisradiographic image taken on day 365 of the follow-up, the boxes represent the approximatesize and position of each AOI.
J Periodontol • February 2008 Rosa, Lucas, Lucas
237
may significantly affect the healing and remodelingprocesses of the residual alveolar ridge after tooth ex-traction in terms of dimensions and radiographic bonedensity. The effect of nicotine was studied in an animalmodel of periodontal disease, and it was found thatnicotine enhanced bone loss observed in ligature-induced periodontal disease.57 The mechanism ofalveolar bone damage produced by smoking is notunderstood well. The components of tobacco and nic-otine metabolites may act directly as local irritants onthe gingiva and alveolar bone or systemically becausethese components are absorbed in the lung, which af-fects the cellular host defense1,2,5,9 or bone turno-ver.5,11 A low absorption of nicotine from cigarettesmoke in the oral cavity has been reported.58 Thus,it seems that the adverse effects of smoking may becaused by a systemic effect instead of a local one.
In addition, a dose-dependent lower bonedensity associated withsmoking was reportedin other bones of thebody, such as the hip,lumbar spine, and fore-arm.13,15 Nicotine cansuppress the prolifera-tion of cultured osteo-blasts while stimulatingosteoblast alkaline phos-phatase activity.11 Re-cently, some in vitrostudies provided otherpossible intimatemecha-nisms by which smokingmay affect bone me-tabolism. Kamer et al.59
reported that nicotineincreased the secretionof interleukin-6 andtumor necrosis factor-alpha in osteoblasts.Nicotine also seems tostimulate bone matrixturnover by increas-ing the production oftissue-type plasminogenactivatorandmatrixmet-alloproteinases, therebytipping the balance be-tween bone matrix for-mation and resorptiontoward the latter pro-cess, as reported byKatono et al.60 Nicotineand other componentsof tobacco may exacer-
bate the action of some substance recognized tocause alveolar bone destruction because it was re-ported that nicotine and lipopolysaccharide stimu-lated the formation of osteoclast-like cells via anincrease in macrophage colony-stimulating factorand prostaglandin E2 production and that the stimula-tion was greater than with nicotine treatment alone.61
Receptor activator of nuclear factor-kappa B ligand(RANKL) and osteoprotegerin (OPG) are membersof the tumor necrosis factor superfamily. RANKL pro-motes osteoclastic differentiation and activates boneresorption.62 In contrast, OPG inhibits osteoclasto-genesis and suppresses bone resorption by inhibitionof RANKL.63 Another potential mechanism of boneloss in smokers may be the suppression of OPG pro-duction and a change in the RANKL/OPG ratio, as wasreported recently in clinical trials conducted by Lappin
Figure 4.Qualitative analysis of DSR. Example of a pair of radiographs taken in a smoker: baseline image (A) and 545-dayfollow-up image (B). C) Corresponding generated subtraction image in which two interproximal sites indicated lossof crestal alveolar bone density because they were represented as dark gray areas (arrows).
Cigarette Smoking and Alveolar Bone in Young Adults Volume 79 • Number 2
238
et al.,64 who analyzed serum concentrations, andCesar-Neto et al.,65 who studied gingival biopsies.
Many computer-assisted techniques have been de-veloped to generate digital radiographic images andanalyze them to obtain information.19 In the presentstudy, the data obtained from the computer-assistedanalysis of digitized posterior vertical bitewing radio-graphs, using a previously described and evaluatedtechnique,44 were used for the purpose of investigat-ing whether smoking has an influence on the alveolarbone of young adults with a relatively low cigaretteconsumption. Eighty-one subjects were selected totake part in this prospective study. Because all ofthem were second-year dental students, they shouldhave represented a homogeneous group in terms oforal hygiene knowledge, periodontal health status,
Table 2.
Clinical Measurements (mean – SEM)Before and After DHP
DHP
Group
Before
(baseline) After
Differences
Within Group
PISmokers 1.07 – 0.06 0.54 – 0.04 *
† †Non-smokers 0.83 – 0.04 0.33 – 0.02 *
GISmokers 0.92 – 0.04 0.49 – 0.04 *
NS ‡Non-smokers 0.88 – 0.04 0.38 – 0.02 *
GCF flow rate (ml/minute)Smokers 0.062 – 0.006 0.056 – 0.007 NS
† NSNon-smokers 0.098 – 0.006 0.069 – 0.005 *
PD (mm)Smokers 1.76 – 0.03 1.50 – 0.03 *
NS NSNon-smokers 1.67 – 0.03 1.43 – 0.03 *
Gingival recessions per subject (N)Smokers 2.5 – 0.4 2.5 – 0.4 NS
‡ †Non-smokers 1.1 – 0.3 1.1 – 0.3 NS
CAL (mm)Smokers 1.44 – 0.04 1.24 – 0.04 *
† ‡Non-smokers 1.24 – 0.04 1.12 – 0.03 §
One-way ANOVA and Tukey comparison of means were used to calculatethe P values.NS = no significant differences.* Significant differences within group (with baseline): P <0.01.† Significant differences between groups: P <0.01.‡ Significant differences between groups: P <0.05.§ Significant differences within group (with baseline): P <0.05.
Figure 5.Radiographic CEJ-ABC distance (mean – SE), in each group during theexperimental period. The measurements were made at 12 posteriorproximal sites per subject. *Significant differences within groups (withday 0): P <0.01; †Significant differences between groups: P <0.01.
Figure 6.CADIA values (mean – SE) in each group during the experimentalperiod. The measurements were made at 12 posterior proximal sitesper subject. †Significant differences between groups: P <0.01;‡Significant differences within groups (with day 0): P <0.05;§Significant differences between groups: P <0.05.
Figure 7.Analysis of digital subtraction radiography. Percentage of sites that haddecreases in density (mean – SE) in each group during theexperimental period. †Significant differences between groups: P <0.01;iSignificant differences within groups: P <0.05; ¶Significant differenceswithin groups: P <0.01.
J Periodontol • February 2008 Rosa, Lucas, Lucas
239

and social class. Smoking status was measured byusing a self-administered questionnaire instead ofa more quantifiable method; e.g., serum cotininelevels, which might have provided additional infor-mation, such as a possible exposure–response rela-tionship. This would seem to be a limitation of thestudy; however, measurement of smoking by self-administered questionnaires has proven to be a validmethod.36,37 Moreover, because subjects were volun-teers it was not practical to obtain serum samples dur-ing follow-up. Subjects were classified as smokers ornon-smokers, and both groups were well-balanced interms of age and gender (Table 1). All subjects en-rolled in a DHP to improve their periodontal statusprior to follow-up. Clinical variables were measuredat baseline and after a DHP. Radiographic variableswere recorded preexperimentally and on days 180,365, and 545 of investigation.
The accumulation of dental plaque was higher forsmokers than for control subjects. Similar results werereported by Al-Wahadni and Linden34 in a case-control study of young Jordanians smokers. The in-vestigators concluded that this observation was dueto poorer oral hygiene practices that smokers re-ported. In the present study, the baseline regular per-sonal oral hygiene routine was not evaluated, but allsubjects were included in a rigorous oral hygiene pro-gram to standardize these measures. Results com-parable to ours were found in other studies,31,33,66
while no significant differences in dental plaque be-tween smokers and non-smokers were found in somestudies.6,8,30,38,43 Clinical gingival inflammation wasalmost the same in both groups at baseline. Afterthe DHP, a significant reduction in clinical gingival in-flammation was observed in the two groups, andsmokers showed more clinical inflammation thannon-smokers. Studies have found greater30,31,33 andequal43 levels of gingival inflammation in smokerscompared to non-smokers. Al-Wahadni and Linden34
also found increased signs of gingival inflammation inyoung smokers. The higher levels of clinical inflam-mation found are in agreement with histologic findingsfrom biopsies of periodontal tissues of smokers.67
The GCF flow rate was significantly lower insmokers at baseline. After the DHP, the GCF flow ratewas reduced significantly in non-smokers, but the dif-ference between the groups was not statistically sig-nificant. Similar results were published by Kinaneand Radvar.38 The tendency of smokers to have adiminished GCF flow rate has been reported.12,38
Persson et al.68 found results comparable to thoseof the present study, with similar population and meth-odology. In part, this observation could be explainedby the action of smoking products, such as nicotineand its metabolites, which produce vasoconstrictionin gingival vessels, as reported in an animal model.69
The tendency of smokers to have deeper pocketshas been reported6,30,43 and observed by Machucaet al.32 in a population of young adult smokers. Inthe present study, smokers showed a slightly highermean PD, but the differences were not statisticallysignificant. The mean number of sites with gingi-val recession was approximately two-fold higher insmokers. Gunsolley et al.31 found similar results ina cross-sectional study in a slightly older populationwith minimal attachment loss. Moreover, sites with re-cession were reported to be more frequent in subjectswho used smokeless tobacco.5 Other studies33,43
found no significant differences in the prevalence ofthe number of sites with recession between smokersand non-smokers. The local effects of smoking, suchas a reduction in gingival blood flow, may explain theadditional number of sites with recession in subjectswho smoke. Although gingival blood supply couldnot be measured easily clinically in the present study,the GCF flow rate at baseline was significantly lower insmokers. This strongly suggests that this local mech-anism may increase the frequency of sites with reces-sion. CAL was significantly greater in smokers than innon-smokers; this indicated less periodontal attach-ment in these individuals. This observation wasreported in a similar population30,32 and in oldergroups38,43 and could be explained by in vitro findingsthat showed that tobacco products (nicotine and co-tinine) inhibited the attachment and growth of fibro-blasts derived from human periodontal ligament.10
Alveolar bone height, the distance from the CEJ tothe ABC, was measured in proximal sites of standard-ized, digitized posterior vertical bitewing radiographswith a computer-assisted technique. Smokers had adecreased bone height at all stages of the study,and bone loss was noted in these subjects after 365and 545 days of follow-up. In comparison, non-smokers had a constant alveolar bone height duringthe same period. The statistical analysis disclosedthat the duration of smoking had a negative effecton the alveolar bone height measured. These find-ings are in agreement with the literature,5 data fromcross-sectional studies published by Feldman et al.,70
Bergstrom et al.,71 and Mullally et al,25 and data fromlongitudinal studies published by Machtei et al.72 andBergstrom et al.55 All of these studies were conductedin an older population (mean age >39) with a longerduration of smoking (mean >10 years). The currentpopulation under study was different because sub-jects were younger, and total tobacco consumptionwas lower. Recently, Levin et al.26 reported a greaterprevalence of crestal bone height loss associated withaggressive periodontitis among young army recruitswho smoked.
The CADIA technique was validated in vitro24 andin vivo46 and was used previously in other fields of
Cigarette Smoking and Alveolar Bone in Young Adults Volume 79 • Number 2
240

periodontics, mainly to evaluate periodontal regenera-tive therapy23,52 and dental implants.73 In the presentstudy, CADIA was performed inalveolarproximal bonesites of the posterior vertical bitewing radiographs.Smokers exhibited a lower radiographic bone densityat all points of the study compared to non-smokers,and the mean bone density had decreased in thesesubjects on day 545 compared to day 0. In non-smokers, the mean radiographic bone density showedminimal variations throughout the study. These re-sults indicate a harmful effect of smoking on the alve-olar bone density in these individuals. Payne et al.74
demonstrated, by alveolar bone height measurementand CADIA, that postmenopausal female smokerswere more likely to lose alveolar bone height and den-sity than non-smokers. The harmful effect of smokingon alveolar bone density in the present study could notbe associated with age-related hormonal changes be-cause the population was young healthy adults.
DSR was evaluated in vitro by induced bone le-sions54 and in vivo,21,46,75 demonstrating a greaterdiagnostic capacity than conventional radiography.It also was used previously to evaluate regenerativeperiodontal therapy23 and dental implants.73 In thepresent study, three radiographic subtraction imageswere obtained from each site between the baseline im-age and the images taken on days 180, 365, and 545.By the qualitative analysis of the subtraction images,smokers showed a greater proportion of sites with lossof bone density than non-smokers, and the proportionof these sites increased throughout the duration of thestudy. These results suggest a detrimental effect ofsmoking on alveolar bone radiographic density.
The 6- to 12-month reentry procedure has been thegold standard for the evaluation of changes in alveolarbone in most clinical regenerative studies during thelast decades.23 Despite the limitations of radiographicanalysis,19,20,22-24 it remains the only non-invasivemethod for bone evaluation in young subjects withno periodontal destruction. A direct digital radiographsystem could have been used; the benefit of this sys-tem includes elimination of processing time and a re-duction in radiation.22 However, an indirect digitalradiograph method26 was preferred because of thesize of the direct detector (thickness and area), whichwas not adequate for the vertical bitewing technique.The resolution provided and the cost of the systemwere other limitations.
According to the results obtained during 18 monthsof follow-up with three computer-assisted techniquesfor evaluating radiographic images, smoking had aharmful effect on alveolar bone crest height and den-sity. These results corroborated data published incross-sectional70,71 and longitudinal55,72 studies witha different and older population. The experimental de-sign and the methodology used in the present study
allowed us to detect deleterious changes in boneheight and density in this young population with afew years of tobacco consumption. Our results con-firm previous reports about young smokers in cross-sectional30-32 and longitudinal66 clinical studies andin clinical/radiographic studies.25,26,34
Although the subjects who participated in this lon-gitudinal study did not represent a sample of theArgentinean young population because they wereall dental students, they correspond to a homogenoussubset with regard to oral hygiene knowledge, peri-odontal health status, and social class. The findingthat smoking may impact alveolar bone parametersnegatively in a well-motivated young population likethis is of concern. The patterns of change on boneparameters evaluated over 18 months of follow-upmight indicate that smoking is already damagingthe alveolar bone in these subjects, who were clini-cally diagnosed to be free from destructive periodon-tal disease. It may be that alveolar bone loss later inadult life depends to a great extent on smoking inyouth; at least one prospective cohort study76 re-ported that smoking in adolescence was a strong pre-dictor of loss of periodontal attachment occurring bythe mid-twenties. Despite public information cam-paigns, a substantial proportion of the populationcontinues to smoke. Furthermore, current trends insome developing countries, such as Argentina (where;32% to 34% of young people smoke), do not show asignificant decrease in the number of young individ-uals acquiring the habit.35
The results from this study showed that smokinghas a harmful effect on clinical and radiographic peri-odontal variables in a young population with low to-bacco consumption. Therefore, it is very importantto improve the periodontal monitoring of this popula-tion of young smokers and to advise them to discon-tinue this habit as a preventive measure. Because themean age at which the subjects in this study acquiredthe habit was ;16 years, and surveys35 reported thatthe beginning age for smoking in Argentina is ;17years, it is imperative that health education be tar-geted at teenagers who should be given appropriateadvice and help to stop smoking. Dental teams shouldbe especially prepared to give advice. In addition,specific information about the adverse effects ofsmoking should be given to dental students by incor-porating this information into the curriculum. Al-though a strong association between smoking andperiodontal disease was reported, and cigarettesmoking is considered an important risk factor forperiodontal disease progression,5,6 additional in vitroand animal research needs to be conducted withthe aim of clarifying the intimate mechanism bywhich smoking produces detrimental effects on theperiodontium.
J Periodontol • February 2008 Rosa, Lucas, Lucas
241
CONCLUSION
Smoking produces an adverse effect on bone heightand density, acting as a potential risk factor for alve-olar bone loss at early age, at the beginning of thehabit, and even with low tobacco consumption.
ACKNOWLEDGMENTS
The authors are grateful for the assistance and contri-butions of the staff of the Physiology Department andAuthorities of School of Dentistry, National Universityof the Northeast and the Graduate School Foundation,and they extend special thanks to the experimentalsubjects. This study was supported by a General Sec-retary of Science and Technique (National Universityof the Northeast) grant and the Department of Re-search, Graduate School Foundation. The data pre-sented are part of the material used in the doctoralthesis of Guillermo M. Rosa at the National Universityof Cordoba, Cordoba, Argentina. The authors reportno conflicts of interest related to this study.
REFERENCES1. Offenbacher S. Periodontal diseases: Pathogenesis.
Ann Periodontol 1996;1:821-878.2. American Academy of Periodontology. The pathogen-
esis of periodontal diseases (informational paper).J Periodontol 1999;70:457-470.
3. Ezzati M, Lopez AD. Regional, disease specific pat-terns of smoking-attributable mortality in 2000. TobControl 2004;13:388-395.
4. Wald NJ, Hackshaw AK. Cigarette smoking: An epi-demiological overview. Br Med Bull 1996;52:3-11.
5. American Academy of Periodontology. Tobacco useand the periodontal patient (position paper). J Peri-odontol 1999;70:1419-1427.
6. Haber J, Wattles J, Crowley M, Mandell R, JoshipuraK, Kent RL. Evidence for cigarette smoking as a majorrisk factor for periodontitis. J Periodontol 1993;64:16-23.
7. Quinn SM, Zhang JB, Gunsolley JC, Schenkei HA,Tew JG. The influence of smoking and race on adultperiodontitis and serum IgG2 levels. J Periodontol1998;69:171-177.
8. Guntsch A, Erler M, Preshaw PM, Sigusch BW, KlingerG, Glockmann E. Effect of smoking on crevicularpolymorphonuclear neutrophil function in periodon-tally healthy subjects. J Periodontal Res 2006;41:184-188.
9. Pabst MJ, Pabst KM, Collier JA, et al. Inhibition ofneutrophil and monocyte defensive functions by nic-otine. J Periodontol 1995;66:1047-1055.
10. James JA, Sayers NM, Drucker DB, Hull PS. Effects oftobacco products on the attachment and growth ofperiodontal ligament fibroblasts. J Periodontol 1999;70:518-525.
11. Fang MA, Frost PJ, Iida-Klein A, Hahn TJ. Effects ofnicotine on cellular function in UMR 106-01 osteoblast-like cells. Bone 1991;12:283-286.
12. Rosa GM, Lucas GQ, Lucas ON. Study of the crevicularfluid flow rate in smokers. Acta Odontol Latinoam2000;13:51-60.
13. Ward KD, Klesges RC. A meta-analysis of the effectsof cigarette smoking on bone mineral density. CalcifTissue Int 2001;68:259-270.
14. Kanis JA, Johnell O, Oden A, et al. Smoking and frac-ture risk: A meta-analysis. Osteoporos Int 2005;16:155-162.
15. Hollenbach KA, Barrett-Connor E, Edelstein SL,Holbrook T. Cigarette smoking and bone mineral den-sity in older men and women. Am J Public Health 1993;83:1265-1270.
16. Law MR, Hackshaw AK. A meta-analysis of cigarettesmoking, bone mineral density and risk of hip fracture:Recognition of a major effect. BMJ 1997;315:841-846.
17. Lane NE. Epidemiology, etiology, and diagnosis of os-teoporosis. Am J Obstet Gynecol 2006;194(2 Suppl.)S3-S11.
18. Armitage GC. Periodontal diseases: Diagnosis. AnnPeriodontol 1996;1:37-215.
19. Bragger U. Digital imaging in periodontal radiography:A review. J Clin Periodontol 1988;15:551-557.
20. Hausmann E. A contemporary perspective on tech-niques for the clinical assessment of alveolar bone.J Periodontol 1990;61:149-156.
21. Jeffcoat MK. Radiographic methods for the detectionof progressive alveolar bone loss. J Periodontol 1992;63:367-372.
22. Reddy MS. Radiographic methods in the evaluation ofperiodontal therapy. J Periodontol 1992;63:1078-1084.
23. Toback GA, Brunsvold MA, Nummikoski PV, MastersLB, Mellonig JT, Cochran DL. The accuracy of radio-graphic methods in assessing the outcome of peri-odontal regenerative therapy. J Periodontol 1999;70:1479-1489.
24. Hausmann E. Radiographic and digital imaging inperiodontal practice. J Periodontol 2000;71:497-503.
25. Mullally BH, Breen B, Linden GJ. Smoking and patternof bone loss in early-onset periodontitis. J Periodontol1999;70:394-401.
26. Levin L, Baev V, Lev R, Stabholz A, Ashkenazi M.Aggressive periodontitis among young Israeli armypersonnel. J Periodontol 2006;77:1392-1396.
27. Susin C, Albandar JM. Aggressive periodontitis in anurban population in southern Brazil. J Periodontol 2005;76:468-475.
28. Ylostalo P, Sakki T, Laitinen J, Jarvelin MR, KnuuttilaM. The relation of tobacco smoking to tooth loss amongyoung adults. Eur J Oral Sci 2004;112:121-126.
29. Susin C, Haas AN, Opermann RV, Albandar JM. Toothloss in a young population from south Brazil. J PublicHealth Dent 2006;66:110-115.
30. Linden GJ, Mullaly BH. Cigarette smoking and peri-odontal destruction in young adults. J Periodontol1994;65:718-723.
31. Gunsolley JC, Quinn SM, Tew J, Gooss CM, BrooksCN, Schenkein HA. The effect of smoking on individ-uals with minimal periodontal destruction. J Periodon-tol 1998;69:165-170.
32. Machuca G, Rosales I, Lacalle JR, Machuca C, BullonP. Effect of cigarette smoking on periodontal status ofhealthy young adults. J Periodontol 2000;71:73-78.
33. Muller HP, Stadermann S, Heinecke A. Gingival re-cession in smokers and non-smokers with minimalperiodontal disease. J Clin Periodontol 2002;29:129-136.
34. Al-Wahadni A, Linden GJ. The effects of cigarettesmoking on the periodontal condition of young Jorda-nian adults. J Clin Periodontol 2003;30:132-137.
Cigarette Smoking and Alveolar Bone in Young Adults Volume 79 • Number 2
242
35. Ministry of Health of the Nation. The National Programof Tobacco Control. Basic information: Characteristicsof consumption (in Spanish). Available at: http://www.msal.gov.ar/htm/site_tabaco/caracteristicas.asp.Accessed March 22, 2007.
36. Petitti DB, Friedman GD, Kahn W. Accuracy of infor-mation on smoking habits provided on self-administeredresearch questionnaires. Am J Public Health 1981;71:308-311.
37. Vartiainen E, Seppala T, Lillsunde P, Puska P. Valida-tion of self reported smoking by serum cotinine mea-surement in a community-based study. J EpidemiolCommunity Health 2002;56:167-170.
38. Kinane DF, Radvar M. The effect of smoking onmechanical and antimicrobial periodontal therapy.J Periodontol 1997;68:467-472.
39. Pihlstrom BL. Measurement of attachment level in clin-ical trials: Probing methods. J Periodontol 1992;63:1072-1077.
40. Silness J, Loe H. Periodontal disease in pregnancy. II.Correlation between oral hygiene and periodontalcondition. Acta Odontol Scand 1964;22:121-135.
41. Loe H. The gingival index, the plaque index and theretention index system. J Periodontol 1967;38:610-616.
42. Chapple IL, Cross IA, Glenwright HD, Matthews JB.Calibration and reliability of the Periotron 6000 forindividual gingival crevicular fluid samples. J Peri-odontal Res 1995;30:73-79.
43. Grossi SG, Zambon J, Machtei EE, et al. Effects ofsmoking and smoking cessation on healing after me-chanical periodontal therapy. J Am Dent Assoc 1997;128:599-607.
44. Rosa GM, Lucas GV, Lucas ON. Bone height mea-surement on digitized radiographs (in Spanish). RevAsoc Odontol Argent 2001;89:347-353.
45. Potter BJ, Shrout MK, Harrell JC. Reproducibility ofbeam alignment using different bite-wing radiographictechniques. Oral Surg Oral Med Oral Pathol OralRadiol Endod 1995;79:532-535.
46. Bragger U, Burgin W, Fourmousis I, Schmid G, SchildU, Lang NP. Computer-assisted densitometric imageanalysis of digital subtraction Images: In vivo error ofthe method an effect of thresholding. J Periodontol1998;69:967-974.
47. Byrd V, Mayfield-Donahoo T, Reddy MS, Jeffcoat MK,Birmingham A. Semiautomated image registration fordigital subtraction radiography. Oral Surg Oral MedOral Pathol Oral Radiol Endod 1998;85:473-478.
48. Shrout MK, Weaver J, Potter BJ, Hildebolt CF. Spatialresolution and angular alignment tolerance in radio-metric analysis of alveolar bone change. J Periodontol1996;67:41-45.
49. Hausmann E, Allen K, Carpio L, Christersson LA,Clerehugh V. Computerized methodology for detectionof alveolar crestal bone loss from serial intraoralradiographs. J Periodontol 1992;63:657-662.
50. Parsell DE, Gatewood RS, Watts JD, Streckfus CF,Jackson M. Sensitivity of various radiographic meth-ods for detection of oral cancellous bone lesions. OralSurg Oral Med Oral Pathol Oral Radiol Endod 1998;86:498-502.
51. Payne JB, Zachs NR, Reinhardt RA, Nummikoski PV,Patil K. The association between estrogen status andalveolarbonedensitychanges inpostmenopausalwomenwith a history of periodontitis. J Periodontol 1997;68:24-31.
52. Brown GD, Mealey BL, Nummikoski PV, Bifano SL,Waldrop TC. Hydroxyapatite cement implant for re-generation of periodontal osseous defect in humans.J Periodontol 1998;69:146-157.
53. Grondahl HG, Grondahl K, Webber RL. A digital sub-traction technique for dental radiography. Oral SurgOral Med Oral Pathol 1983;55:96-102.
54. Katsarsky JW, Levine MS, Allen KM, Hausmann E.Detection of experimentally induced lesions subtrac-tion images of cancellous alveolar bone. Oral SurgOral Med Oral Pathol 1994;77:674-677.
55. Bergstrom J, Eliasson S, Dock J. A 10-year prospec-tive study of tobacco smoking and periodontal health.J Periodontol 2000;71:1338-1347.
56. Saldanha JB, Casati MZ, Neto FH, Sallum EA, NocitiFH Jr. Smoking may affect the alveolar processdimensions and radiographic bone density in maxil-lary extraction sites: A prospective study in humans.J Oral Maxillofac Surg 2006;64:1359-1365.
57. Nociti FH, Nogueira GR, Primo MT, et al. The influenceof nicotine on the bone loss rate in ligature-inducedperiodontitis. A histometric study in rats. J Periodontol2000;71:1460-1464.
58. Hukkanen J, Jacob P 3rd, Benowitz NL. Metabolismand disposition kinetics of nicotine. Pharmacol Rev2005;57:79-115.
59. Kamer AR, El-Ghorab N, Marzec N, Margarone JE 3rd,Dziak R. Nicotine induced proliferation and cytokinerelease in osteoblastic cells. Int J Mol Med 2006;17:121-127.
60. Katono T, Kawato T, Tanabe N, et al. Nicotine treat-ment induces expression of matrix metalloproteinasesin human osteoblastic Saos-2 cells. Acta BiochimBiophys Sin (Shanghai) 2006;38:874-882.
61. Tanaka H, Tanabe N, Shoji M, et al. Nicotine andlipopolysaccharide stimulate the formation of osteo-clast-like cells by increasing macrophage colony-stimulating factor and prostaglandin E2 productionby osteoblasts. Life Sci 2006;78:1733-1740.
62. Lerner UH. New molecules in the tumor necrosis factorligand and receptor superfamilies with importance forphysiological and pathological bone resorption. CritRev Oral Biol Med 2004;15:64-81.
63. Jin Q, Cirelli JA, Park CH, et al. RANKL inhibitionthrough osteoprotegerin blocks bone loss in experi-mental periodontitis. J Periodontol 2007;78:1300-1308.
64. Lappin DF, Sherrabeh S, Jenkins WM, Macpherson LM.Effect of smoking on serum RANKL and OPG in sex,age and clinically matched supportive-therapy peri-odontitis patients. J Clin Periodontol 2007;34:271-277.
65. Cesar-Neto JB, Duarte PM, de Oliveira MC, TambeliCH, Sallum EA, Nociti FH. Smoking modulates inter-leukin-6:interleukin-10 and RANKL:osteoprotegerinratios in the periodontal tissues. J Periodontal Res2007;42:184-191.
66. Muller HP, Stadermann S, Heinecke A. Longitudinalassociation between plaque and gingival bleeding insmokers and non-smokers. J Clin Periodontol 2002;29:287-294.
67. Katsuragi H, Hasegawa A, Saito K. Distribution ofmetallothionein in cigarette smokers and non-smokersin advanced periodontitis patients. J Periodontol 1997;68:1005-1009.
68. Persson L, Bergstrom J, Gustafsson A, Asman B.Tobacco smoking and gingival neutrophil activity inyoung adults. J Clin Periodontol 1999;26:9-13.
J Periodontol • February 2008 Rosa, Lucas, Lucas
243

69. Clarke NG, Shephard BC. The effects of epinephrineand nicotine on gingival blood flow in the rabbit. ArchOral Biol 1984;29:789-793.
70. Feldman RS, Bravacos JS, Rose CL. Associationbetween smoking different tobacco products and peri-odontal disease indexes. J Periodontol 1983;54:481-487.
71. Bergstrom J, Eliasson S, Preber H. Cigarette smokingand periodontal bone loss. J Periodontol 1991;62:242-246.
72. Machtei EE, Hausmann E, Schmidt M, et al. Radio-graphic and clinical response to periodontal therapy.J Periodontol 1998;69:590-595.
73. Stentz WC, Mealey BL, Numminosky PV, GunsolleyJC, Waldrop TC. Effects of guided bone regenerationaround commercially pure titanium and hydroxyapatite-coated dental implants. I Radiographic analysis. J Peri-odontol 1997;68:199-208.
74. Payne JB, Reinhardt RA, Nummikoski PV, DunningDG, Patil KD. The association of cigarette smokingwith alveolar bone loss in postmenopausal females.J Clin Periodontol 2000;27:658-664.
75. Nummikoski PV, Steffensen B, Hamilton K, Dove SV.Clinical validation of a new subtraction radiographytechnique for periodontal bone loss detection. J Peri-odontol 2000;71:598-605.
76. Hashim R, Thomson WM, Pack AR. Smoking in adoles-cence as a predictor of early loss of periodontal attach-ment.CommunityDentOralEpidemiol2001;29:130-135.
Correspondence: Dr. Guillermo M. Rosa, Cordoba 456 (CP3500) Resistencia, Chaco, Argentina. E-mail: [email protected].
Submitted December 31, 2006; accepted for publicationAugust 10, 2007.
Cigarette Smoking and Alveolar Bone in Young Adults Volume 79 • Number 2
244