Embed Size (px)
Citation preview

Clin. Radiol. (1969) 20, 465-472
C H Y L U R I A A N D L Y M P H A T I C R E N A L F I S T U L A
O S C A R C R A I G and F. J. W O O D R O F F E
from the Radiological Department, St. Mary's Hospital, London, W.2 and Paddington General Hospital, London, W.9
Three cases of lymphatic renal fistula are described. Two of the patients had f rank chyluria which was filarial in origin. The third patient in whom there was no possibility of filarial infection, had a chylous efftux from the scrotum, and a very small lymphatic renal fistula. The lymphangiographic findings in each case are shown. The common site of lymphatic obstruction and the sequence of events leading to cbyluria are described. The frequency of the disability and the prognosis is considered. The value of lymphangiography and the relative importance of other tests in the investigation are outlined. Final ly the discussion covers the question of medical and surgical treatment.
ALTHOUGH many cases of chyluria are recorded in the world literature, few have been described in British journals . Filarial chyluria forms the main group from abroad; non-filarial chyluria is rare in Great Britain and overseas. Comparatively few cases have been investigated with lymphangio- graphy, as it is only since 1962, with the in t roduct ion of oily contrast medium for lymphangiography that it has been possible to demonstrate convincingly the exact site of the lymphatic fistula and of the lymphatic block preoperatively.
The following cases are presented because of their rarity and also to demonstrate the value of lymphangiography in (1) detecting the site of the lymphatic-renal fistula (2) evaluating the degree and extent of the lymphatic disorder and (3) illustra- ting the site of the lymphatic block.
Case 1.--E.E., age 52, male. This patient, a healthy look- ing West Indian from British Guiana, was first seen in 1963. He gave a two year history of passing 'cloudy' urine. This was intermittent with periods lasting 1 month when the urine was clear. Since his present complaint began he had lost 2 stones in weight.
On examination, fleshy lymph nodes were palpable in both groins, right more than left. The cardiovascular system was normal apart from a blood pressure of 180/110. There were no other relevant findings clinically.
Urine: Filaria Bancrofti present. Protein, red blood cells and pus cells found. Blood: A night sample of blood con- tained microfilaria. Hb: 14.7 grms. % W.B.C. 4,000. Eosin~phils 8 ~. E.S.R.: 22 mm./hr. (Wintrobe). Chest x-ray: Normal.
I.V.P. : Normal pelvicalycine system on both sides. The ureters and bladder were normal. Cystoscopy: There was a milky urinary efflux from the right ureter. The left ureteric efflux and the bladder were normal. Right retrograde pye- logram: Normal. No lymphatic backflow.
Four days after completing a course of Hetrazan he developed acute retention. The bladder was drained and no obvious obstruction was found. He was discharged on
11/7/65. He continued to attend the out patient department and was still passing cloudy urine.
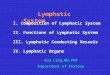
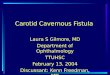
A lymphangiogram was requested to detect any lymphatic- renal fistula. The patient was transferred to St. Mary's Hospital and a lymphangiogram was carried out on 3/9/66, 10 ml. of fluid Neo-hydriol were introduced into a foot lymphatic on each side. The films showed lymphangeictasis of the pelvic and abdominal lymphatics (Fig. 1). The groin glands were enlarged but many of the para-aortic glands failed to fill, very likely due to fibrosis (Fig. 2). Collateral channels were also outlined, and retrograde filling of right renal lymphatics from the right para-aortic chain was seen (Fig. 3). The thoracic duct was demonstrated; it was dilated and tortuous (Fig. 4) but was not visualised in its upper part. The appearances were those of lymphatic duct blockage with a lymphatic-renal shunt on the right.
There is little doubt that this is a case of filarial chyluria. Mainly because of the presence of abdominal lymphangiec- tasis, local surgical therapy was not performed and conserva- tive treatment was continued.
Case 2.--L. de V., age 53, male. This patient, a civil servant from Trinidad, first complained of passing milky urine in 1958. This had been intermittent. During the attacks he had noticed a great loss of strength and energy and over the past year he had lost 20 lbs. in weight. There was a past history of a right pleural effusion. Physical examination did not reveal any significant abnormality, other than enlarged inguinal lymph nodes. Blood: Negative for microfilaria in day and night samples. Hb. : 14-8 grms. % W.B.C. 15,000. Eosinophils 1 ~. E.S.R. 2 mm./hr.. Urine: No microfilaria found; moderate number of red cells present; culture sterile. Filarial skin test positive.
X-ray chest: Pleural thickening and calcification. No other abnormalities. I.V.P.: Normal. Cystoscopy: Normal. Retrograde pyelogram: Normal. He was given a course of Hetrazan. The chyluria settled and his weight increased. He was discharged.
In November 1966 the patient again presented with loss of weight and strength and passing milky urine. His urine contained a large quantity of chyle and albumin. I.V.P. and retrograde pyelography were normal. He was transferred to St. Mary's for lymphangiography. There was good filling of the pelvic and abdominal lymphatics and only minimal pelvic lymphangiectasis was present. Few para-aortic
465

466 C L I N I C A L R A D I O L O G Y
Fro. 1 Fie. 2
FIG. 1--Enlargement of groin glands, lymphangiectasis of pelvic and abdominal lymphatics. Fro. 2--Gross abdominal lymphangiectasis, absence of normal gland filling, collateral channels
visible. Lymphatic renal fistula on the right.
FIG. 3 FIG. 4
FIG. 3.--Later film showing more contrast in lymphatic renal fistula. FIG. 4.--Dilated and tortuous thoracic duct.

CHYLURIA AND LYMPHATIC RENAL FISTULA 467
nodes were outlined. There was a large lymphatic-renal shmat on the left and multiple lymphatic channels passing into the left kidney were outlined (Figs. 5 and 6). A film taken two hours later as part of an I.V.P. showed that most of the contrast had gone fi'om the lymphatics. A little oily contrast still remained in the calyces (Fig. 7). The rapidity of the disappearance of the contrast suggested that the shunt was large. It was felt that retrograde pyelography would surely demonstrate pelvi-lymphatic backflow, but careful distension of the left renal pelvis and calyces under image intensification failed to demonstrate any lymphatic backflow.
The thoracic duct was not demonstrated in this case but neither was its termination which is so frequently seen on routine lymphangiography. However on the chest x-ray there was filling of a lymphatic vessel overlying the left upper zone of the chest, and rather marked filling of the right para- tracheal glands (Figs. 8 and 9).
Because of the loss of weight and strength and the absence of marked abdominal or pelvic lymphangiectasis, it was decided that operative treatment was justified. Perivascular stripping of the renal pedicle was carried out-- the lymphatic vessels being removed.
Fit. 5 FI~. 6 Fro. 5--No gross lymphangiectasis. Left lymphatic renal fistula. F~G. 6--Coned view of lymphatic
renal fistula.
FIG. 7 FIG. 8 Fro. 9 FIG. 7---Rapid disappearance of contrast from fistula. Fie. 8--Filling of small lymphatic in left upper zone. Filling of mediastinal
glands. F~G. 9--Lateral film showing marked filling of glands in mediastinum.

468 CLINICAL RADIOLOGY
FI~. 11
Case 3.--This young man, aged 23, was born in England and had never been in a filarial area. In 1960 he presented with a four year history of milky white discharge from the right side of the scrotum. For this the left side of the scrotum had been joined to the left thigh two years previously but shortly after~the operation the right leg began to swell. When seen again the right side of the scrotum was enlarged with thickened skin containing white vesicles which discharged milky fluid when pricked. The fluid from the vesicles was identified as chyle. A lymphangiogram with aqueous con- trast medium was performed and demonstrated tortuous and varicose lymphatics in the right half of the pelvis. Reflux was demonstrated into the right scrotal lymphatics. A block dissection of the lymphatics, vessels and nodes was made over the area from the right common iliac artery down to the femoral ring. Post operatively the leakage of chyle stopped and the vesicles dried up.
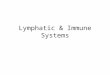
He was seen again in 1966 complaining of an increase in the swelling of the right leg. There was no further chylous discharge or chyluria. A lymphangiogram was carried out on the right. Approximately 7 c.cs. of oily contrast medium were introduced. The films showed moderate lymphangiec- tasis of the pelvic lymphatics (Fig. 10). There was cross flow into scrotal lymphatics which passed upwards to pelvic channels, and retrograde flow of lymph into the left renal lymphatics indicating a left lymphatic-renal shunt (Fig. 11). In addition there was a large lymphatic cyst in the pelvis and a further one in the right paracolic gutter (Figs. 12, 13 and 14). The patient during the preceding year or two had suf- fered from intermittent lower abdominal pain. It seems likely that this was due to distension of the lymphatic cysts. No abnormalities were seen in the leg lymphatics.
This patient is being treated conservatively at present. I t seems probable that there is some obstruction to the lym- phatic pathway in the cisterna chyli region, and frank chyluria is likely to develop in the future.*
* Since this paper was submitted for publication the patient has been re-admitted with a chylothorax.
Fm. 12 Oily contrast in pelvic lymphatic cyst and in
right paracolic gutter.
D I S C U S S I O N
The causes o f chyluria can be classified as fol lows : - -
(1) Parasitic (a) Filariasis (b) Echinococcus (c) Cysticercus cellulosae (d) Ascaris lumbricoides (e) Malaria

C H Y L U R I A A N D L Y M P H A T I C R E N A L F I S T U L A 469
FIG. 13 FIG. 14
FtG. 13--Erect film showing the downward extension of the lymphatic cyst. FrG. 14--A.P. film in right lateral decubitus showing the right lateral border of the cyst. The combination of these films show that the cyst is larger than would appear
on Fig. 12.
(2) Non-Parasitic (a) Lymphatic aneurysm (b) Thoracic duct obstruction
by glands, tumours, trauma, abscess or tu- berculosis.
In practice the vast majority of cases of chyluria are parasitic in origin due to infestation with the filarial worm Wucheria Bancrofti. Al- though other parasites have been incriminated in the literature there is little proof that they play any significant role in the aetiology. It is possible that they may be found in the same patient harbouring the filarial parasite. Non-parasitic chyluria is also a great rarity and there are very few reports of these in the literature. According to Manson Bahr (1966) if a patient has lived in a filarial endemic area for any time and subsequently develops chyluria, failure to demonstrate evidence of past or present filariasis cannot be regarded as excluding parasitic chyluria.
The first published record of the disease was by Chapotin in 1812 from Mauritius. Van Dyke Carter in 1862 put forward the theory that the disease was caused by the escape of chyle and lymph into the bladder due to the rupture of a lymphatic varix. He thought that the parasite causing the condition lodged somewhere in the urinary tract. Wucherer in 1868 in Brazil recorded for the first time the finding of the filarial embryo in the urine of a chyluric patient. In 1872 Lewis in Calcutta found the filarial embryo in both the blood and lymphatic fluid and also noted a relationship between chyluria and elephantiasis. Remlinger in 1924 described what he thought were cases of non- filarial chyluria in Morocco, and considered that they were due to rupture of lymphatic cysts into the urinary tract. Abeshouse in 1934 demonstrated
that during retrogradepyelography, pyelolymphatic backflow occurred in these cases, and formed the opinion that the chyle enters the urine from the kidneys. His conclusions seem to be correct but the acceptance of pyelolymphatic backflow as evid- dence for this is of course erroneous. This aspect will be discussed later in the paper.
It is interesting that Ackerman in 1863 described the sequence of events leading to chyluria which is that most widely accepted to-day and which has now been verified by lymphangiography. Ackerman postulated organic obstruction in the lymphatic vessels between the bowel and the thoracic duct. This produces an increase in intralymphatic pressure leading to lymphangiectasia, followed by valvular incompetence in the lymphatic vessels and retrograde flow of chyle producing a lymphatic- renal shunt. The kidney is a favoured site for rupture of the lymph vessels because of their fragility in this region, their close association with the renal calyces and the inadequacy of collateral vessels in this area.
The common cause appears to be an obstruction, usually partial, to the cisterna chyli or thoracic duct. When due to filariasis the larvae enter the lymphatics, and ascend to the lymph nodes where maturity is reached. As long as the adult parasite remains alive it apparently does little damage; at most it may cause lymphangitis but no obstruction at this stage. Death of the adult parasite produces a granulomatous inflammatory reaction. Necrosis occurs with later obliteration of the lymphatics by scarring. The lymph nodes are also scarred and obstructed. This has been confirmed by the absence of good lymph gland filling on lymphangiography. It may, however, be many years after the death of the

470 CLINICAL
adult worm before the condition appears. Obstruc- tion of the lymphatic pathway does not invariably lead to chyluria. The varicose abdominal lympha- tics can rupture into the alimentary tract, pleural, peritoneal or pericardial sacs, or discharge through the scrotum.
In 1939 Ray and Rao presented 254 cases of chyluria from 12,368 cases of filarial infection investigated in Calcutta. They found the incidence of chyluria to be 2-05% and the proportion of males to females 9 - - 1. In 78 ~ the night blood contained microfilaria, and the chylous urine was positive in 52 ~. There was of course no lympho- graphic evidence of lymphatic fistulae or obstruc- tion. Most of the reported cases of filarial chyluria have been found in Japanese, Puerto Ricans, Philippinos, Chinese, and East Indians. Kishimoto, Higuchi, Endo and Kai (1964) described the lymphangiographic demonstration of a lymphatic- renal fistula in a 61 year old Japanese male with chyluria, and stated that between 1959 and 1961 2,222 cases of chyluria were discovered in Japan. 77 ~ of these were from Southern Japan, where 10- 20 ~o of the local population harbour filaria.
Clinical Features.--Chyluria is intermittent, with periods of remission lasting many months. The patient's activity and posture influence the amount of chyle excreted in the urine. Exercising the legs increases the amount of lymphatic flow and also the degree ofchyluria.Conversely, bed rest decreases the chyluria; a high fat diet increases the chyluria and of course, a low fat diet leads to a decrease. It is not uncommon for blood to be passed with the chyle and a high fibrin content leads to clot for- mation. This may cause ureteric colic and even acute obstruction of a ureter or the bladder. Case 1 in this series developed acute retention, very likely on this basis.
A common feature is a history of weight loss, but the loss of fat may be so great as to lead to malnutrition. Associated renal infection is common Yamauchi (1945) considers pyelonephritis in vary- ing degrees to be present in practically all cases of chyluria. The fat evacuated in the urine is in a molecular form in a state of colloidal suspension. Lipuria, with which it may be confused, occurs in eclampsia, diabetes, renal disease and as a compli- cation of fractures. It is characterised by the excretion of fat in droplet form without fibrin.
A good ward test for chyluria is to give the patient 100 mgms of Sudan Red III mixed with l0 G. of butter. Urine is collected for the next 2 - - 6 hours. In cases of chyluria the urine appears bright orange.
R A D I O L O G Y
The Lymphatic Drainage of the Kiflney.~ Wesson (1946) has described the lymphatic drainage as follows : - -
1. Lymph vessels in the substance of the kidneys 2. A second plexus beneath the fibrous capsule 3. A plexus of vessels in the perinephric fat. The second and third plexuses communicate
freely with each other. The vessels from the plexus in the kidney converge to form 4 to 7 trunks which emerge from the renal hilum. Here they are joined by vessels from the plexus under the capsule. Following the course of the renal vein they end in the lateral aortic, glands. The perinephric vessels drain directly to the upper abdominal glands. The lymphangiogram in Case 2 shows the lymphatic vessels of the renal plexus coming directly off the minor calyces.
It seems likely that the chyle travelling from the mesenteric glands to the thoracic duct, on meeting an obstruction, is held up in dilated lymphatics. The dilatation of the lymphatics and the increased lymphatic pressure results in valvular insufficiency. Following this there is retrograde flow of lymph and chyle to the upper lumbar lymph glands. It is easy to see that this will readily result in back pressure on the intra-renal lymphatics which may then rupture into the minor calyces.
There have been many descriptions of a commu- nication between the lymphatics and the minor calyces (Campbell and Siedler (1937), Row (1952), L6gren (1953), Wood (1929).
Before the development of lymphangiography many authors (Wesson (1933), Hinman (1927), Yamauchi (1945), stressed the importance of pyelo- lymphatic backflow during retrograde pyelography in cases of chyluria. They accepted this as confir- matory evidence of the site of communication of the lymphatics and proof of the existence of a lymphatic renal shunt. Yamauchi reported uro- graphic studies in 32 cases of chyluria and found pyelolymphatic backflow in 6, pyelovenous back- flow in 3, pyelotubular backftow in 2, pyelovenous and pyelolymphatic backflow in 13, and no evidence of backflow in 8. The occurence of pyelolymphatic backflow during routine retrograde pyelography in familiar to all radiologists. It must be stressed that whereas pyelolymphatic backflow may occur more readily in cases of chyluria (and there is little proof of this), the finding of this phenomenon at retrograde pyelography has of itself little, if any, significance. It is widely appreciated that pyelolymphatic backflow may occur with excessive pressure or overfilling of the pelvis in the absence of any obvious pathology in the lymphatic vessels.

C H Y L U R I A A N D L Y M P H A T I C R E N A L F I S T U L A 471
Lymphangiography has now been performed in a number of these cases, (Pomeranz and Jones (1966), Kishimoto, et al., (1964), Kitteridge, et al., (1963), Choi and Wiedemer, (1964), and it has confirmed the mechanical factors resulting from lymphatic obstruction, lymphatic dilatation and backflow. In some of these cases abdominal lymphangiec- tasis has been seen, and in all published contrast studies it was possible to demonstrate the lymphatic- renal fistula. The site of the block, however, has not always been identified. In this respect it is important to obtain follow-up films for some days. Kitteridge, et aL, (1963) reported a 62 year old Puerto Rican with a history of chyluria for 30 years. This had been intermittent at first, but became constant over the past 2 years. Lymphangio- graphy showed lymphangiectasis of the pelvic lymphatics, and poor filling of the iliac and para- aortic glands. The thoracic duct was not seen on the earlier films. However, irregular areas of dilatation of the thoracic duct were seen at 24 hours. The duct was slow to empty and was still seen partially filled at 96 hours. It was only on the 72 hour film that a lymphatic renal shunt was demonstrated.
The great value of lymphangiography in these cases is to (1) detect the site of the lymphatic-renal fistula, (2) to demonstrate the full extent of the lymphatic disease: this will greatly influence the prognosis and form of treatment, and, (3) to try to demonstrate the site of the lymphatic block.
Prognosis.--The prognosis depends greatly on the severity of the chyluria and the degree of generalised lymphangiectasia. Ray and Rao (1939), in reviewing their large series from Calcutta, con- cluded that the prognosis as to life in chyluria is not unfavourable. They had many patients who maintained normal weight and were still in good health after chyluria for 20 years. However, Compston and Ellerker (1956) refer to "severe cases" in which the fat loss may be so great as to cause malnutrition which may be fatal. These cases are rare. They have also stated that sponta- neous healing may follow retrograde pyelography. One of the cases reported by Swanson in 1963 had a spontaneous cure following lymphangiography.
In considering the prognosis it is necessary to remember that the picture is usually one of a major lymphatic block, and that there is extensive and generalised lymphangiectasia in most. The presence of a lymphatic-renal fistula may act as a "safety valve" and prevent a more serious complication such as chylous ascites or rupture into the bowel or pericardial sac, If Case 3 in the present series
had had a larger fistula there would have been less pelvic lymphangiectasis and perhaps no chylous efflux from the scrotum.
Treatment.--The choice of treatment lies between the following : - -
A. Medical Bed rest Low fat Diet Anti filarial drugs
B. Irrigation of renal pelvis with 1/2000 silver nitrate or sodium iodide.
C. Surgery (1) Renal (a) Nephrectomy (b) Capsulectomy (c) Removal of lym-
phatics around renal pedicle.
(2) Performance of a lymphatic- venous anastomosis
(3) Direct attack on the site of lymphatic blockage.
There is still a great deal of divided opinion as to the best treatment. It would appear that the form of treatment must depend largely on the severity of the chyluria and the severity of the malnutrition and weight loss. Pomerantz and Jones (1966), discussing therapy, say that the frequently benign characteristics of the disease rarely make a radical procedure necessary, and Ray and Rao (1939) found that in the vast majority conservative treatment was satisfactory. Compson and Ellerker
(1956) advised nephrectomy if the patient's con- dition is deteriorating. This is drastic treatment and may lead to rupture of the lymphatics into the other kidney, or even to the more serious complication of chylous ascites. Yamauchi (1945) stated that nephrectomy, capsulectomy and the removal of peri-renal lymph-channels probably have no place in the treatment of chyluria. The case of a 52 year old Ohio farmer who had intermittent chyluria was discussed by Choi and Wiedemer (1964). Lymphan- giography demonstrated extensive lymphangiec- tasis in the abdomino-aortic and ilio-pelvic lymph vessels. There was an abnormal communication between the abdominal lymphatics and one kidney. It was thought that this was due to an obstructed thoracic duct although this had not been directly demonstrated. Renal de-capsulation and removal of lymphatic vessels around the vascular pedicle was carried out. The chyluria continued and 2 weeks after the operation the patient developed bulky foamy stools, Stool analysis revealed a vastly increased fat content. There seemed little doubt that lymphatic varices had ruptured into the bowel as a result of increased pressure following closure of the fistula. Torres and Estrada (1962) report 2

472 CLINICAL RADIOLOGY
cases, one a 50 year old Philippino who had chyluria for 3 months, and the other a 35 year old female Philippino with a 10 year history of chyluria. Renal decapsulation and stripping of the renal vascular pedicle was performed on each. At a 2 year follow up there was no recurrence of the chyluria in either.
Kishimoto, et al., report that during the 5 years between 1957 and late 1961, 70 patients with chyluria underwent surgery in Japan. The following results were obtained: Chyluria disappeared - - 7 5 . 7 ~ ; Chyluria improved - - 2 0 ~ ; Chyluria unchanged - - 4.3 ~ . These authors felt that results would be improved by a more meticulous removal o f lymphatics from around the renal vascularpedicle.
To summarise, it would appear that usually .conservative therapy can be adopted to treat ,chyluria. It is only when the patient is losing an .excessive quantity of weight, or where there is a genuine danger of malnutrition that surgery is indicated.
There have been no reports of successful direct surgery of a blocked thoracic duct. To date no good results have been reported from attempts to form a lymphatic-venous anastomosis. From the literature it would appear that renal decapsulation and peri-vascular lymphatic stripping of the renal pedicle is the operation of choice.
If, however, lymphangiography demonstrates very dilated abdominal lymphatics, the presence of :a lymphatic-renal fistula may be a "safety valve" which lowers the rising intra-lymphatic pressure. If for any reason this shunt is closed, it is possible that a further fistula may develop at another site, i.e., into the other kidney, bowel or peritoneal ,cavity. The finding of a very severe abdominal lymphangiectasis may in fact be a contra-indication ~to surgery.
Acknowledgements.--We wish to thank Dr. Carmichael Young, Mr. Stephen and Professor Irvine for permission to publish these cases under their care. We are indebted to Dr. Cardew and his Staff in the Photographic Department of St. Mary's Medical School for reproducing the prints of the x-rays.
REFERENCES
ABESHOUSE, B. S. 0934). Am. J. Surg., 25, 427-450. ACKERMANN, T. (1863). Dtsch. Kiln., 15, 221-233. CAMPBELL, M. F. & SEIDLER, V. B. (1937). Am. or. Roent.,
38, 602-606. CARTER, H. V. (1862). Med. Chit. Trans., 45, 189-208. CASERTA, S. J. (1956). New. EngL J. Med., 255, 1239-1241. CHAPOTIN, CH. (181"2). Topographie Medicale de File de
France, Paris, Didot, Jeune, 92. CHoI, J. K. & WIEDEMER, H. S. (1964). J. Urol., 92, 723-727. CONPSTON, N. & ELLERKER, A. G. (1956). Br. J. UroL, 28,
147-149. HINMAN, F. (1927). Surg. Gynae. Obstet., 44, 592-600. JOHNSTON, D. W. (1955). Ann. Intern. Med., 42, 931-937. KISHIMOTO, T., HIGUCHI, T., ENDO, M., & KAI, Y. (1964).
J. Urol., 92, 574-578. KIXTREDCE, R. D., HASHIM, S., ROHOL r, H. B., VAN ITALLIE,
T. B., & FINBY, N. (1963). Am. J. Roent., 90, 157-165. LAZARUS, J. A. & MARKS, M. S. (1946). Am. J. Surg., 71,
479-490. LEwis, T. R. (1872). On a haematozoon inhabiting human
blood: its relation to chyluria and other diseases. Calcutta, Office of the Supt. of Govern. Printing. Acta Med. Scand.,
LOWGREN, E. (1953). Acta Med. Scand., 144, 375-379. MANSON (1966). Tropical Diseases 16th Ed., Bailliere,
Tindal. Cassell, p. 681. POMERANTZ, M. & JONES, W. R. (1966). J. Am. Med. Ass.,
196, 452-454. RAY, P. N. & RAO, S. S. (1939). Br. J. Urol., 11, 48-64. REMLINGER, P. (1924). Maroc Mdd., 15, 109. Row, P. (1952). Med. J. Aust., 1, 847-849. TORRES, L. F. &; ESTRADA, J. (1962). J. Urol., 87, 73-76. WESSON, M. B. (1933). Urol. cutan. Rev., 37, 692-698. WESSON, M. B. (1946). Urologie roentgenology Lonaon
Kimpton, 239-243. WOOD, A. H. (1929). J. Urol., 21, 109-117. WUCHERER (1868). Gaz. Med. Bahia, 3, 97. YAMAUCHI, S. (1945). or. Uro., 54, 318-347.
PRINTED BY GEORGE OUTRAM & CO. LTD., 36 TAY STREET, PERTH, SCOTLAND