Embed Size (px)
Citation preview

Churning: Children’s Coverage Discontinuity and
Its Consequences in Kentucky
Julia F. Costich and Svetla SlavovaCollege of Public HealthUniversity of Kentucky

What we know about discontinuity in children’s coverage
• NY: half lost coverage in a year despite most remaining technically eligible (Lipson 2003)
• 12 states: less than half timely renewed (Hill 2003)
• 4 states: half lapsed at renewal but one-fourth back in 2 months (Dick 2002)
• 7 states: two-thirds of disenrolled ineligible for SCHIP (but Medicaid?) (Riley 2002)
• Kansas: procedural and computer problems often at fault (Allison 2003)

Kentucky Children’s Health Insurance Program (KCHIP)
• Medicaid expansion to 150% FPL• Look-alike to 200% FPL• Administered by Dept. for Medicaid
Services• Eligibility determination by same
agency as cash assistance, food stamps, etc.
• Enrollment stable at ~50,000 children• Compare Medicaid at ~321,000

KCHIP Policy Changes
• 1998: Mail-in application, in-person renewal• 7/1/2000: Mail-in renewal with pre-populated
form and self-declaration of income• 6/1/2001: Return to in-person interview for
renewal• 7/1/2002: Mailed renewal reinstated; return
to in-person interview for initial application• Confusion among caseworkers and families

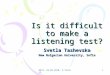
Percentage of All Children Enrolled in KCHIP or Medicaid, SFY 2003Data source: Kentucky Dept. for Medicaid Services
Adair
Allen
Anderson
Ballard
Barren
Bath
Bell
Boone
Bourbon
Boyd
Boyle
Bracken
Breathitt
Breckinridge
Bullitt
Butler
Caldwell
Calloway
Campbell
Carlisle
Carrll
Carter
Casey
Christian
Clark
Clay
Clinton
Crittenden
Cumberland
Daviess
Edmonson
Elliott
Estill
Fayette
Fleming
Floyd
Franklin
Fulton
Gallatin
Garrard
Grant
Graves
Grayson
Green
Greenup
Hancock
Hardin
Harlan
Harrison
Hart
Henderson
Henry
Hickman
Hopkins
Jackson
Jefferson
JessamineJohnson
Kenton
Knott
Knox
Larue
Laurel
Lawrence
Lee
Leslie Letcher
Lewis
Lincoln
Livingston
Logan
LyonMccracken
Mccreary
Mclean
MadisonMagoffin
Marion
Marshall
Martin
Mason
Meade Menifee
Mercer
Metcalfe
Monroe
Montgomery
Morgan
Muhlenberg
Nelson
Nicholas
Ohio
Oldham
Owen
Owsley
Pendleton
Perry
Pike
Powell
Pulaski
Robertson
Rockcastle
Rowan
Russell
Scott
Shelby
Simpson
Spencer
Taylor
ToddTrigg
Trimble
Union
Warren
Washington
Wayne
Webster
Whitley
Wolfe
Woodford
Prepared by: Julia F. Costich, College of Public Health
Under 30%
30-39%
40-49%
50-59%
Over 60%

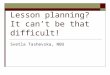
Fig. 1: KCHIP Enrollment May 2001-March 2004
45000
46000
47000
48000
49000
50000
51000
52000
53000
54000
55000
56000
May-01
Jun-01
Jul-01
Aug-01
Sep-01
Oct-01
Nov-01
Dec-01
Jan-02
Feb-02
Mar-02
Apr-02
May-02
Jun-02
Jul-02
Aug-02
Sep-02
Oct-02
Nov-02
Dec-02
Jan-03
Feb-03
Mar-03
Apr-03
May-03
Jun-03
Jul-03
Aug-03
Sep-03
Oct-03
Nov-03
Dec-03
Jan-04
Feb-04
Mar-04
End of mail-in application
Premiums
Recertif ication policy changes

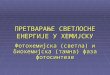
Fig. 2: Combined KCHIP and Children's Medicaid Enrollment, May 2001-March 2004
310000
320000
330000
340000
350000
360000
370000
380000
May-01
Jun-01
Jul-01
Aug-01
Sep-01
Oct-01
Nov-01
Dec-01
Jan-02
Feb-02
Mar-02
Apr-02
May-02
Jun-02
Jul-02
Aug-02
Sep-02
Oct-02
Nov-02
Dec-02
Jan-03
Feb-03
Mar-03
Apr-03
May-03
Jun-03
Jul-03
Aug-03
Sep-03
Oct-03
Nov-03
Dec-03
Jan-04
Feb-04
Mar-04

Problems with added eligibility office workload
Source: Family Resource & Youth Service Center Staff Survey
• Long waits in understaffed urban offices• Refusal to provide scheduled appointments• Overloaded phone system; unanswered voice mails• Unexpected requests for additional documentation• Inappropriate denial based on confusion• Staff reporting suspect immigration status• Failure or inability to accommodate working
families’ schedules

Churning effect
• 46% did not renew on time• New applications were 52% of total enrollment• Yet total enrollment grew by only 4%• Millions of wasted state dollars• Risk of gaps in coverage• Wide variation across the state• Timely renewal highest in Medicaid expansion


Data sources
• Open records request to Medicaid for data by county, month and program– “Requires” staff to provide data
• Data limitations– Not individual-level– “New” applications may be internal to system when renewal
deadline is missed by staff
• 3 categories– Number of children up for renewal– Number timely renewed– Number of new applications approved

Methodology• Percentage of all children (Census data)
enrolled in KCHIP or Medicaid– Critically important to include both because of
frequent movement between programs– Failure to account for movement overstates
churning
• Percentage of children eligible for renewal in either program who renewed on time
• New applications approved as percentage of total enrollment

Percentage of Children Enrolled and Percentage of Timely Renewals (R2
= .44)

New Approvals as Percentage of Total and Percentage of Timely Renewals (R2
= .55)

Methodology and statistical findings
• SAS univariate regression analysis• F test found p < .0001 for relationships
between – renewal and enrollment– new applications and non-renewal
• R2 = .44 and .55 respectively

Discussion
• Low rate of timely renewal similar to other studies’ findings
• Identified need for pre-termination contact, follow-up– Problem: hiring freezes, state budget deficit
• Next steps: – Determine whether supportive environment of
high-renewal counties can be replicated with outreach workers, volunteers
– Advocate for more realistic federal budget allocations

Limitations
• Inability to track individual children• Considerable migration among programs• Eligibility determination office practice
giving rise to spurious new applications• Possible delinking issues in information
systems• Antiquated eligibility determination system
may introduce errors