Embed Size (px)
Citation preview

Chronobiology and Mood Disorders
Vo l u m e 5 . N o . 42 0 0 3
in
neuroscienceclinical
Dialogu se
e
I SSN 1294-8322

Dialogu se
Editor-in-chiefJean-Paul MACHER, MD, Rouffach, France
Editorial BoardManfred ACKENHEIL, MD, München, GermanyCésar CARVAJAL, MD, Santiago de Chile, ChileMarc-Antoine CROCQ, MD, Rouffach, FranceMichael DAVIDSON, MD, Tel Hashomer, IsraelMargret R. HOEHE, MD, Berlin, GermanyBarry D. LEBOWITZ, PhD, Rockville, Md, USADeborah J. MORRIS-ROSENDAHL, PhD, Johannesburg, South AfricaRajesh M. PARIKH, MD, Bombay, IndiaDavid RUBINOW, MD, Bethesda, Md, USAPierre SCHULZ, MD, Chêne-Bourg, SwitzerlandCarol A. TAMMINGA, MD, Baltimore, Md, USA
International ConsultantJorge-Alberto COSTA E SILVA, MD, Rio de Janeiro, Brazil
Publication Director / Directeur de la PublicationJean-Philippe SETA, MD, Neuilly-sur-Seine, France

ear Colleagues,
The concept of chronobiology combines the notion of rhythms with objective phe-nomena reflecting the functioning of the living organism. Rhythms give a framework tothis functioning and are of great importance to our everyday life. Indeed, rhythms arepresent due to night and daylight cycles, meal periodicity, and social interactions, andeven in the work place. All these synchronizers—for which the German word“Zeitgeber” is often used, as a result of Jürgen Aschoff’s seminal research—leave animprint on our lives.There are endogenous rhythms that correspond to these exogenousrhythms, such as sleep-wake cycles, rhythms in hormonal secretions, and other biologi-cal rhythms in general.
In pathophysiology, some rhythms acquire an abnormal character, and some dis-orders exhibit specific rhythms. Examples include recurring episodes of manic-depres-sive illness, schizoaffective psychoses, and recurrent depression.
The understanding of this “chronological symptomatology” and its correlation withchronobiology is essential for two reasons. First, clinically or biologically suitable mark-ers must be defined, and, second, treatments stimulating or regulating rhythms must bedevised. For instance, rhythms may be stimulated by antidepressant drugs in depression,or regulated by chronobiotic substances, such as mood-regulating drugs.
We are convinced of the importance of a progress report on the current state ofthe art in these various fields, and we believe that the articles in this issue will provideplenty of food for thought.
Yours sincerely,
Jean-Paul Macher, MD Marc-Antoine Crocq, MD
E d i t o r i a l
D
309

310
Dialogues in Clinical Neuroscience is a quarterly publication that aims toserve as an interface between clinical neuropsychiatry and the neuro-sciences by providing state-of-the-art information and original insights intorelevant clinical, biological, and therapeutic aspects. Each issue addresses aspecific topic, and also publishes free contributions in the field of neuro-science as well as other non–topic-related material. All contributions arereviewed by members of the Editorial Board and submitted to expert con-sultants for peer review.
Indexed in EMBASE and Elsevier BIOBASE.
EDITORIAL OFFICES
Editor in Chief
Jean-Paul MACHER, MD
FORENAP - Institute for Research in Neuroscience and NeuropsychiatryBP29 - 68250 Rouffach - FranceTel: + 33 3 89 78 70 18 / Fax: +33 3 89 78 51 24
Secretariat and submission of manuscripts
Marc-Antoine CROCQ, MD
FORENAP - Institute for Research in Neuroscience and NeuropsychiatryBP29 - 68250 Rouffach - FranceTel: +33 3 89 78 71 20 (direct) or +33 3 89 78 70 18 (secretariat)Fax: +33 3 89 78 51 24 / E-mail: [email protected]
Production Editor
Sarah A. NOVACK, PhD
Servier International - Medical Publishing Division192 avenue Charles-de-Gaulle 92578 Neuilly-sur-Seine Cedex - FranceTel: +33 1 55 72 33 10 / Fax: +33 1 55 72 68 88 E-mail: [email protected]
PUBLISHER
Les Laboratoires Servier22 rue Garnier - 92578 Neuilly-sur-Seine Cedex - FranceE-mail: [email protected]
Copyright © 2003 by Les Laboratoires Servier
All rights reserved throughout the world and in all languages. No part of thispublication may be reproduced, transmitted, or stored in any form or by anymeans either mechanical or electronic, including photocopying, recording, orthrough an information storage and retrieval system, without the writtenpermission of the copyright holder. Opinions expressed do not necessarilyreflect the views of the publisher, editors, or editorial board. The authors, edi-tors, and publisher cannot be held responsible for errors or for any conse-quences arising from the use of information contained in this journal.
ISSN 1294-8322
Design: Christophe Caretti / Layout: Graphie 66Imprimé en France par SIP1, rue Saint Simon - 95310 Saint-Ouen-l’Aumône

C o n t e n t s
Page
311
309
366
389
371
399
353
343
327315313
ISSUE COORDINATED BY: Manfred ACKENHEIL
EditorialJean-Paul Macher, Marc-Antoine Crocq
In this issueManfred Ackenheil
State of the artChronobiology and mood disordersAnna Wirz-Justice
Concepts in human biological rhythmsAlain Reinberg, Israel Ashkenazi
Basic researchMelatonin and animal modelsPaul Pévet
Pharmacological aspectsLight treatment of mood disordersBarbara L. Parry, Eva L. Maurer
PosterSleep deprivation and antidepressant treatmentUlrich Voderholzer
Clinical researchDiagnosis and treatment of sleep disorders:a brief review for cliniciansVivien C. Abad, Christian Guilleminault
Treatment of seasonal affective disordersNicole Praschak-Rieder, Matthäus Willeit
Clinical applications of melatonin in circadian disordersAlfred J. Lewy

C o n t r i b u t o r s
Author affiliations: Centre for Addictionand Mental Health, PET Centre, Toronto,ON, Canada
Nicole Praschak-Rieder, MD
Author affiliations: Sleep and Mood Dis-orders Laboratory, Oregon Health ScienceUniversity, Portland, Ore, USA
Alfred J. Lewy, MD, PhD
Author affiliations: Stanford UniversitySleep Disorders Clinic and Research Cen-ter, Stanford University, School of Med-icine, Stanford, Calif, USA
Vivien C. Abad, MD, MBA
Barbara L. Parry, MD
Author affiliations: Department of Psy-chiatry, University of California, SanDiego, USA
Author affiliations: Centre for Chronobiol-ogy, Psychiatric University Clinic, Basel,Switzerland
Anna Wirz-Justice, PhD
Author affiliations: Department of Psy-chiatry and Psychotherapy, Klinikum ofthe Albert-Ludwig-University, Freiburg,Germany
Ulrich Voderholzer, MD, PhD
Author affiliations: Unité de Chrono-biologie, Fondation Adolphe de Rothschild,Paris, France
Alain Reinberg, MD, PhD
Author affiliations: Laboratoire de Neu-robiologie des Rythmes, UMR 7518 CNRS-Université Louis Pasteur, Strasbourg,France
Paul Pévet, PhD
312

This issue of Dialogues in Clinical Neuroscience is devotedto circadian rhythms and related disorders. Many patientswith psychiatric disorders show disturbances in circadianrhythms and frequently sleep disorders. These disorders areconsidered either to be the cause or the symptoms of thecorresponding psychiatric disorder. Whether they be thecause or the effect, it is important to take them into con-sideration for treatment decisions. Specific treatments,such as melatonin, light therapy, advanced and delayedsleep phase, and sleep deprivation, are reported here.Chronobiology (circadian, ultrarapid, and seasonalrhythms) is an essential component of human and animallives. Disturbances in these rhythms result in behaviorabnormalities and mental and somatic symptoms.
Exceptionally, in this issue two State of the art articles illus-trate the current knowledge of the complexity of circadianrhythms. In the first, Anna Wirz-Justice (page 315) refers todiurnal variations of mood and sleep disturbances indepression, leaving open the question of its etiological sig-nificance. Antidepressant treatments, medication, sleepdeprivation, and exposure to bright light (corresponding tosunlight) are discussed. The opposite of light—darkness—and the hormone melatonin are examined, as well as futureaspects, which are delineated in an extensive manner.
The second State of the art article by Alain Reinberg andIsrael Ashkenazi (page 327) is more conceptualized, relat-ing biological rhythms to environmental factors as adap-tive phenomena to the movement of the earth. In thissophisticated text, they focus on human chronobiologyand the problem of desynchronization, which can occurwithout clinical symptoms (which they call allochronism)or with numerous pathological symptoms (dyschronism).They describe diseases with chronic sleep disturbances, forexample, night shift workers who are intolerant to desyn-chronization.
The Basic research article by Paul Pévet (page 343) focus-es on the sleep hormone melatonin. The paper elucidatesthe role of melatonin in animals with special respect to cir-cadian and seasonal rhythms. The administration of exoge-nous melatonin shows the complexity of melatonin‘sactions. Depending on the dosage, the time of administra-tion, and the sensitivity of melatonin receptors, different
effects are reported. Melatonin has various effects, whichare mediated through the different melatonin receptors.Pharmacological treatment with melatonin or similar sub-stances has to consider this complexity.
Two articles in this issue deal with chronobiological disor-ders and techniques of light therapy. In the Pharmaco-logical aspects article, Barbara L. Parry and Eva L. Mau-rer (page 353) focus on phototherapy and its possiblemechanisms in various psychiatric conditions and subsyn-dromal states, including gender issues like premenstrualdysphoric disorder. It is a comprehensive article coveringmost of the existing relevant literature related to this topic.
More clinical aspects are covered in the Poster by UlrichVoderholzer (page 366) on sleep deprivation therapy, whichis one of the most effective therapies for severe depression.Unfortunately, it is only short-lasting, but its effect can beprolonged in combination with pharmacotherapy,advanced sleep phase therapy, and light therapy. Predictorsfor the response to sleep deprivation therapy from brainimaging and endocrine studies are discussed.
Sleep disorders are strongly related to disturbances of cir-cadian rhythms and are comprehensively described in theClinical research article by Vivien C. Abad and ChristianGuilleminault (page 371). They describe exactly the differ-ent forms of sleep disorders and present guidelines fortreatment. Additionally, other circadian rhythm disordersare mentioned and options for treatment with chronother-apy and light therapy are given. Restless legs syndrome,periodic limb movement disorders, obstructive sleep apnea,narcolepsy, and parasomnia are comprehensively discussed.
The second article to deal with light therapy is a Clinicalresearch article from Nicole Praschak-Rieder andMatthäus Willeit (page 389). It covers the treatment ofmood and also seasonal affective disorder (SAD), whichmay be a subform of major depression, recurrent, orbipolar disorder. The current knowledge of the patho-physiology of SAD and the various treatments with brightlight are presented as a first-line option for SAD. Recom-mendations for the general management of such disor-ders are given, also mentioning a combination of thera-pies with psychotropic drugs.
313
I n t h i s i s s u e . . .

In a Clinical research–oriented article, Alfred J. Lewy(page 399) describes two major melatonin activities inhumans as a marker of biological rhythms and a modu-lating hormone for the circadian phase. The regulation ofmelatonin secretion is described. The consequences fortreatment with exogenous melatonin are mentioned.Thus, exogenous melatonin (2 mg/day) should be given2 h before the dim light melatonin onset and therapeuticlight should be given at waketime. Sighted people are
compared with blind (sightless) people. Interestingly, suchstudies show that low dosages of melatonin (1 mg/day)have better effects than higher dosages (>3 mg/day).Guidelines for treatment of circadian sleep disorders inblind people are recommended. Delayed sleep phase syn-drome, advanced sleep phase syndrome, and jet lag arealso described. Recommendations for treatment or howto avoid these syndromes are given. The problem of shiftwork maladaptation is briefly discussed.
314
I n t h i s i s s u e . . .
Manfred Ackenheil, MD

n order for Dialogues in Clinical Neuroscience tobe truly designated “dialogues,” I will raise specific andcritical questions about the putative circadian rhythm dis-turbances in depression, provide a model within which tounderstand them, and summarize the present status andapplication of chronobiological therapies. This shortoverview will not go into detail of the clinical and exper-imental findings related to biological rhythms in depres-sion, which have been extensively reviewed elsewhere.1-9
Chronobiologists predicate their work on a primary axiom,that temporal order is essential for health. Psychological,behavioral, physiological, and hormonal rhythms arespecifically and functionally timed (entrained or syn-chronized) with respect to sleep and the day-night cycle.The converse premise implies that temporal disordermust have clinical correlates. Rhythmic characteristics of
S t a t e o f t h e a r t
315
Chronobiology and mood disorders Anna Wirz-Justice, PhD
I
Keywords: major depression; seasonal affective disorder; circadian rhythm; sleepdeprivation; light therapy; melatonin
Author affiliations: Centre for Chronobiology, Psychiatric University Clinic,Basel, Switzerland
Address for correspondence: Prof Dr Anna Wirz-Justice, Centre forChronobiology, Psychiatric University Clinic, Wilhelm Klein Strasse 27, CH-4025 Basel, Switzerland(e-mail: [email protected])
The clinical observations of diurnal variation of mood and early morning awakening in depression have been incorpo-rated into established diagnostic systems, as has the seasonal modifier defining winter depression (seasonal affective dis-order, SAD). Many circadian rhythms measured in depressive patients are abnormal: earlier in timing, diminished in ampli-tude, or of greater variability. Whether these disturbances are of etiological significance for the role of circadian rhythmsin mood disorders, or a consequence of altered behavior can only be dissected out with stringent protocols (eg, constantroutine or forced desynchrony). These protocols quantify contributions of the circadian pacemaker and a homeostaticsleep process impacting on mood, energy, appetite, and sleep. Future studies will elucidate any allelic mutations in “circadian clock”–related or “sleep”-related genes in depression. With respect to treatment, antidepressants and moodstabilizers have no consistent effect on circadian rhythmicity. The most rapid antidepressant modality known so far isnonpharmacological: total or partial sleep deprivation in the second half of the night. The disadvantage of sleep depri-vation, that most patients relapse after recovery sleep, can be prevented by coadministration of lithium, pindolol, sero-tonin (5-HT) reuptake inhibitors, bright light, or a subsequent phase-advance procedure. Phase advance of the sleep-wake cycle alone also has rapid effects on depressed mood, which lasts longer than sleep deprivation. Light is thetreatment of choice for SAD and may prove to be useful for nonseasonal depression, alone or as an adjunct to medica-tion. Chronobiological concepts emphasize the important role of zeitgebers to stabilize phase, light being the most impor-tant, but dark (and rest) periods, regularity of social schedules and meal times, and use of melatonin or its analoguesshould also be considered. Advances in chronobiology continue to contribute novel treatments for affective disorders. © 2003, LLS SAS Dialogues Clin Neurosci. 2003;5:315-325.
Copyright © 2003 LLS SAS. All rights reserved www.dialogues-cns.org

mood disorders were precisely described as far back asancient times. However, it is still unclear whether circa-dian rhythms are reliably linked with psychopathology, ifthey provide clues to underlying mechanisms, and howthey can be understood with respect to the establishedneurotransmitter models of depression.The first question is common to all clinical research: whatdo we mean by biologically homogeneous groups? Heretoo, diagnostic issues are the crux. In addition to the dis-tinction unipolar, bipolar, or seasonal affective disorder(SAD), the stage of the illness may be important forchronobiological disturbances.Acute depression is prob-ably different from chronic, and in rapid cyclers it isknown that there is a continuous shift in circadian phaseduring depression and that this reverses during mania.1
Given that antidepressants act on neurotransmittermechanisms also involved in circadian rhythm genera-tion and entrainment, only untreated patients may revealan “endogenous” rhythm disturbance, if present.The second question regards conceptual clarity.What dowe mean by a clock disturbance in depression? What onesees clinically may have its origins at a variety of differentlevels—not necessarily the hypothalamic biological clockitself, but epiphenomena related to altered rhythmicbehavior, disturbed sleep, or abnormal environmentalinput.The third question is whether the studies purporting todocument circadian rhythm disturbances in depressionhave been adequately carried out. Alas, methodologicalissues characterize most investigations—not in terms ofscientific caliber or intent, but because it was previouslynot sufficiently recognized how strongly “masking”(behavioral or environmental factors that modify thevariable measured) obscures the underlying endogenousrhythms.This is a particular problem with measuring thecore body temperature rhythm, since temperature is eas-ily and rapidly masked by motor activity, postural change,meals, etc. Cortisol increases with stress, particularly atthe evening nadir; thus, this circadian marker is also often
masked by psychophysiological response. Melatonin, thepineal hormone considered to provide the best estimateof circadian rhythm phase, is suppressed by light, partic-ularly in the evening: it is sensitive to masking by light aslow as ca 100 lux.10 Thus, even indoor room light maydelay the apparent onset of nocturnal secretion. Only inthe last decade have controlled protocols using state-of-the-art chronobiological techniques provided unequivo-cal circadian markers.The fourth question concerns which models are useful.Concepts of an underlying genetic and stress-related vul-nerability for depression can be discussed in terms ofboth neurotransmitter and circadian rhythm dysregula-tion. Here, I will draw on the two-process model of sleep-wake regulation11 as a way of understanding some aspectsof depressive symptomatology.The final question is whether we can find out about puta-tive circadian mechanisms underlying affective disorderthrough understanding clinically successful chronobiolog-ical treatments. Circadian rhythm or sleep manipulationsdo improve depression and provide some fascinating clues.
Clinical observations
Periodicity in affective disorders (from seasonal recur-rence to 48-h rapid cycling) is the clinical observation;diurnal variation of mood, early morning awakening, andsleep disturbances are the classical symptoms that havelinked depression with circadian rhythm function. Manyrhythms, such as core body temperature, cortisol,monoamine metabolism, are different in depressivepatients: phase advanced (timed earlier) with respect tothe sleep-wake cycle, diminished in amplitude, and/orwith day-to-day variability in their synchronization tosocial cues (entrainment).1 However, altered rhythmicitycould be either a cause or an effect of altered affectivestate. Both could independently reflect abnormalities ina third system, such as psychomotor activity. Apparentlability may be caused solely by lack of appropriate feed-back to the circadian system (eg, reduced activity). Inaddition, sleep disturbances are inextricably linked withdepressive illness.These clinical observations can be for-malized in terms of circadian and sleep physiology.
The neurobiology of circadian rhythms
Circadian rhythms are generated by a master pacemakerlocated in the suprachiasmatic nuclei (SCN) of the ante-
S t a t e o f t h e a r t
316
Selected abbreviations and acronymsHPA hypothalamo-pituitary-adrenal (axis)5-HT serotonin (5-hydroxytryptamine)PVN paraventricular nucleusrTMS repetitive transcranial magnetic stimulationSAD seasonal affective disorderSCN suprachiasmatic nucleusSSRI selective serotonin reuptake inhibitor

rior hypothalamus.12 Individual, genetically determinedendogenous periodicity is slightly different from 24 h (usu-ally longer) and requires daily synchronization to the 24-h day by “zeitgebers,” which are regularly recurringenvironmental signals. Light is the major zeitgeber for theSCN, transmitted by novel photoreceptors in retinal gan-glion cells.13 This nonvisual, non–image-forming pathwayvia the retinohypothalamic tract counts photons, in par-ticular the transitions at dawn and dusk, and is activelygated by a second clock in the eye.14 An indirect visualpathway reaches the SCN via the intergeniculate leaflet ofthe lateral geniculate complex. From the raphe nucleus, aserotonergic pathway provides nonphotic input to theSCN, and it is perhaps of some importance in the contextof depression that concentrations of serotonin (5-HT) inthe brain are highest in these nuclei.An important outputleads from the SCN to the paraventricular nucleus (PVN)and via a multisynaptic pathway to the pineal gland, wheremelatonin is synthesized at night and suppressed by lightduring the day. Melatonin transduces the night signal forthe body as the nocturnal duration of hormone secretion(“the day within”).15 Melatonin onset in the early eveninghas proved to be the most reliable biological marker of cir-cadian timing (provided samples are taken under dim lightconditions).16 The PVN is also the site of corticotropin-releasing factor synthesis, ie, part of the hypothalamo-pitu-itary-adrenal (HPA) axis.The nadir of the cortisol rhythmprovides a reliable output of the SCN clock (whereas themaximum is influenced by environmental factors).17
Zeitgeber stimuli, of which light is the most important,can phase shift—and thus entrain—the SCN.18,19 Lightduring the early part of the night induces phase delays,whereas light given in the second half of the night (afterthe core body temperature minimum) induces phaseadvances.18,19 Administration of exogenous melatoninshows patterns nearly opposite to phase shifting to light.20
Other nonphotic zeitgebers (exercise, perhaps sleep ordarkness, and nutrients) have been less well investigatedand are probably weaker zeitgebers than light.21 Socialzeitgebers (jobs, social demands or tasks, and personalrelationships) may act directly or indirectly on the SCN,since they determine the timing of meals, sleep, physicalexercise, and outdoor light exposure.These social factorsalso have the potential to disrupt circadian rhythms.22
Some of the particular psychosocial precipitants ofdepressive disorder, such as life events, chronic stresses,or lack of appropriate social support systems, may act asprecipitants by disrupting circadian rhythms.
Clocks everywhere
The concept of a master pacemaker driving all circadianrhythms has been very useful. It needs to be supple-mented by the concept of peripheral clocks distributedin every organ and perhaps in every cell.23 Each organhas its own relevant and specifically timed circadianrhythms—of heart rate, liver metabolism, and kidneytransport, and also of gene expression. Under normalconditions, all rhythms are synchronized by the SCN.23
The SCN signal is translated mainly by the PVN into ahormonal and autonomic signal to peripheral organs.Visceral, sensory, and hormonal information feeds backon the hypothalamus, providing fine-tuning to synchro-nize time-of-day input from the external light-dark cyclewith metabolic information from the inside.The phase ofeach rhythm can be adjusted by differential responses ofa given tissue’s circadian clock to a signal from the SCNor from the environment. Such a system can adjust wellto small, gradual changes in the input signal (such as sea-sonal changes in daylength), but may become temporar-ily and severely disorganized if the change in phase ofthis signal is abrupt and large (as is most obvious forrapid transmeridian travel and shift work). How couldthis system go wrong in affective disorders? Consider the vegetative symptoms that are an integralpart of the depressive syndrome, and often appear asforerunners. If sleep is no longer in correct alignmentwith the inner or outer clock, if food intake decreases, orif behavior turns inward so that motor activity declinesand the amount of outdoor light exposure is reduced (aswell as social contact), is it not conceivable that thesebehaviors each act on different clocks, shifting their tim-ing with respect to each other and the day-night cycle todifferent degrees? This temporal cacophony could initi-ate an internal stress reaction. Given the concept of afinal common neuroendocrine pathway of depression viahyperactivity of the HPA axis, this may be an importantmediating system from physiology to psyche.
Clock genes, sleep genes
Individual preference in timing of the sleep-wake cycle(chronotype, ie, whether “larks” or “owls”)24 is deter-mined by clock genes, of which 10 have been cloned sofar.25 Individual sleep and wake duration (long sleepersversus short sleepers) is also probably programmed incertain sleep genes26). Since the timing of sleep appears
Chronobiology and mood disorders - Wirz-Justice Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
317

to be rather important for mood, these genetic factorsmay be relevant to a chronobiological vulnerability fordepression, in that wrong or poor alignment of internalphase with the outdoor world increases susceptibility todepressive mood swings. Although familial forms of cir-cadian sleep disorders (such as advanced or delayedsleep phase syndrome) have been found, with allelicmutations on one or other of the clock genes,27-29 the firststudies in depression have been negative (eg, the clockgene in major depression30 or the per2 gene in bipolar dis-order31). Circadian clock-related polymorphisms seem tobe related, interestingly enough, to susceptibility to SADtogether with evening chronotype.32 This research is stillin its infancy.
Circadian rhythm desynchronization
It is unlikely, however, that affective disorders will becharacterized as simple clock gene mutations. Rather,internal desynchronization may be a major contributingfactor to mood state. New findings on desynchronizationin clock gene expression illustrate this vividly. The clockgenes in the SCN gradually adapt to a phase shift of thelight-dark cycle (as found in shift work and transmerid-ian travel), whereas clock genes in muscle, liver, and lungresynchronize at their own rates.33 This results in a dou-ble desynchronization, not only between internal (SCN)and external time, but also between different clocks andorgans within the body itself.The temporal orchestra canquickly get out of tune. Moreover, the different organclocks respond to different, specific zeitgebers; for exam-ple, food can shift the clock in the liver rather fast, butlight does not affect it; the SCN clock reacts to light, butis not influenced by meals.34 Peripheral clocks in musclemay be synchronized by exercise.This provides a new view on circadian rhythm distur-bances in depression. Since peripheral clocks comple-ment the central clock’s function of maintaining tempo-ral order, more clocks in body and brain only add to thepossibilities of this organization going awry. There maybe different patterns of desynchronization that result insimilar physiological or psychological consequences.Theclassical idea of internal circadian phase disturbances indepression can be extended to zeitgeber phase distur-bances.6 Even an apparently minor reduction in zeitge-ber strength or diminished behavior can loosen tempo-ral coordination, not only between internal rhythms, butalso with respect to the social and physical clock, result-
ing in mood detriments, diurnal variation, and day-to-daymood variability. However, the precise neurobiologicalmechanisms by which altered circadian phase relation-ships lead to altered mood state remain unknown.Bipolar disorder, in particular rapid cycling, is the moststriking example of a mood disorder linked to abnormalor changing circadian rhythm phase.1 Here the environ-ment (light or dark) as well as behavior (sleep or itsdeficit)35 strongly modulate affective state and, recently,these factors have begun to be used as treatments.36-39
Sleep regulation
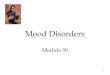
The sleep-wake cycle is the most obvious circadianrhythm in humans, and sleep disturbances are a promi-nent feature of depression. In the two-process model ofsleep regulation, a homeostatic process S increases dur-ing waking and declines exponentially during sleep; itinteracts with a circadian process C to determine the tim-ing and architecture of sleep.11 This model can also beused to describe possible disturbances in either processduring depression (Figure 1A). The clinical sleep distur-bance with early morning awakening could arise from animpaired build-up of S during waking (diminished sleeppressure) or an earlier timing of process C. There are anumber of sleep manipulations that improve clinical state(see below and Table I). The rapid antidepressant effectof one night’s sleep deprivation is proposed to act by ashort-term increase in process S to normal levels.40 Theslower antidepressant effect of a phase advance of thesleep-wake cycle8 may be related to more gradual shiftstowards a correct phase relationship with respect toprocess C. Other possibile abnormalities could lie in thedecline of S during sleep, or circadian period, phase, oramplitude (process C).
How to measure process C and S
The model helps clarify which biological markers couldbe measured to test these hypotheses (Figure 1B).Correct methodology is important to define experimen-tal conditions where masking is reduced. There are twomajor approaches, both requiring subjects to undergodemanding and highly controlled protocols.The first pro-tocol is the “constant routine,” in which subjects remainawake during an entire 24-h cycle or longer, with exter-nal and behavioral conditions constant (very low lightlevels not to affect the circadian pacemaker, supine pos-
S t a t e o f t h e a r t
318

ture in bed, and regular small isocaloric meals).The con-stant routine provides information about process C:amplitude and phase estimates of rhythms in, for exam-ple, melatonin, cortisol, and core body temperature.18
Only such parameters that are little affected by sleepdeprivation are valid as circadian markers. The secondprotocol is “forced desynchrony,” in which subjects liveon very long or very short sleep-wake cycles, while theclock remains at its endogenous period, somewhat longerthan 24 h. This protocol allows quantification of manymeasures with respect to either time of day (process C)or to duration of prior wakefulness (process S).18
Process C and S in SAD
Both the constant routine and forced desynchrony pro-tocols have been employed in patients with SAD, bothwhen depressed and euthymic, in winter and summer.The endogenous period appears normal.41 A phase delayin process C (as measured by core body temperature ormelatonin rhythms in constant routine) has been found,42
but not in all studies or all markers.41,43 The decline inprocess S (as measured by spectral analyses of the sleepelectroencephalogram [EEG]) was no different in SADpatients compared with controls.44,45 However, the rise inprocess S (as measured by spectral analyses of the wakeEEG) was different, indicating a factor related to day-time vigilance.46,47 Wake EEG patterns in evening chrono-types are similar to this,48 which may mean that the abovefinding is not pathogenetic for SAD, since the patientchronotype is skewed towards “owls,” shows the abovetendency to phase delay, and has common clock-relatedpolymorphisms.32
War of the zeitgebers?
What is fascinating is that both circadian and wake-depen-dent factors contribute to a subjective measure such asmood.This has been demonstrated in healthy subjects inboth protocols.6,41,49,50 The day-to-day change in patterns ofdiurnal mood variation in a forced desynchrony protocolhas remarkable similarities to the day-to-day variability indiurnal mood variation found in depressive patients, and
Chronobiology and mood disorders - Wirz-Justice Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
319
Figure 1. A. The two-process model of sleep regulation, considered interms of what could go wrong in depression. The homeosta-tic component (process S) builds up during wakefulness anddeclines during sleep. The circadian pacemaker (process C)ticks along at its individual (genetically programmed) endoge-nous period. Decreased amplitude would increase variabilityof daily timing and it would be more vulnerable to phaseshifts. If the rhythm was advanced or delayed in phase, theresultant altered phase relationships between process C andsleep timing could explain many depressive phenomena. B.Biological markers of process S and process C. The exponen-tial rise in sleep pressure can be followed by theta-alpha (θ/α)power in the wake electroencephalogram (EEG). The expo-nential decline in sleep pressure is evident in slow-wave activ-ity in the sleep EEG. In a constant routine protocol, therhythms of core body temperature (CBT), melatonin, and cor-tisol provide estimates of circadian phase and amplitude. Ina forced desynchrony protocol, the endogenous period of thecircadian pacemaker can be reduced as well as the relativecontributions of process C and process S to any given mea-sure, from psychological to physiological.
S decline
S
C
Endogenous period
Phase relationshipbetween C and sleep
A. Where can it go wrong in depression?
Sleep EEG,slow wakeactivity
Abnormal/unstablephase relationship
between C and sleep
B. How can we get evidence for disturbances?
Build-up of S
Phase
Amplitude
Homeostatic process
Zeitgebers
Circadian process
Wake EEGθ/α
Phase advance and decreased amplitudeCBT, melatonin, cortisol
Homeostatic process (EEG)
Circadian process (constant routine)
ZeitgebersDecreased
Social, light, food, activity
Endogenous period
Separate C and S (forced desynchrony)

even more similarity to the mood patterns following aphase advance of the sleep-wake cycle.8 Thus, mood fluc-tuations can indeed be understood in terms of abnormalor changing phase relationships.Mood-related cognitive and attributional disturbanceshave been postulated to be sequelae of shifting circadianrhythms.5 This is an important point for the above findings.If SAD patients are vulnerable to short winter days, is thisan abnormality of the biological clock, or is it rather a sub-jective interpretation of internal temporal disorder? Thefollowing findings are perhaps relevant to this argument.Some subjects in experiments where they live free oftime cues manifest spontaneous internal desynchroniza-tion, in that their sleep-wake cycle desynchronizes fromcircadian rhythms such as core body temperature. Theydo not notice that this phenomenon has occurred, nor dothey show any decrement in mood or performance—onthe contrary, they feel rather well.51 This is in marked con-trast to the situation resulting from external desynchro-nization, when sleep timing is shifted by shift work ortransmeridian travel. Here the internal desynchroniza-tion between sleep and the clock is additionally in con-flict with light and social zeitgebers in the outer world;and it is postulated that this aspect may underlie theoften-associated depressive disturbances.5,52
It may not only be phase relationships that are important,but perhaps also the light-dark ratio (daylength or pho-toperiod). Some of the evidence for SAD suggests that theduration of nocturnal melatonin secretion is important for
triggering psychopathology in winter.53 Conversely, in astudy of healthy subjects kept on long winter nights, onevolunteer became severely suicidal, even though all theothers felt remarkably well on this protocol.54
Diurnal variation or instability of mood can thus be quitewell explained by considering changing phase relation-ships between processes C and S. Even in healthy sub-jects, some phase relationships are favorable, others unfa-vorable. Modest but reliable mood decrements occurafter a phase delay of the sleep-wake cycle55 (reviewed inreference 5). Sudden delays (as induced by night shift orwestwards flights across time zones) can even precipitatedepressive symptoms in predisposed individuals with ahistory of affective illness.56,57 This points to a particularvulnerability of mood state when sleep is shifted laterwith respect to circadian rhythms. Such an associationalso appears to be valid for the circadian sleep disorderof delayed sleep phase syndrome (inappropriately latesleep timing with respect to the endogenous circadianclock). In these persons there is a high comorbidity ofdepressive symptoms.58 Conversely, flying east may bemore correlated with hypomanic or manic states.56,57
Psychopharmacology and circadian rhythms
The earliest link between psychopharmacology and circa-dian rhythms came from the observation that lithiumslows down circadian periodicity in plants.59 These effectsof lithium are consistent across species, including humans,60
S t a t e o f t h e a r t
320
Table I. Chronobiological therapies of major depression. Therapies in italics are for one or two studies only. TSD, total sleep deprivation; PSD, par-tial sleep deprivation; rTMS, repetitive transcranial magnetic stimulation; SSRI, selective serotonin reuptake inhibitor; SAD, seasonal affec-tive disorder; MD, major depression.
Sleep manipulations Zeitgebers
TSD Light therapy (SAD)
PSD (second half of the night) Light therapy (nonseasonal MD)
Phase advance of the sleep-wake cycle Light therapy as adjuvant to SSRIs (nonseasonal MD)
TSD followed by phase advance Dark or rest therapy (rapid-cyclers)
Repeated TSD or PSD Dark therapy (mania)
Repeated TSD or PSD with antidepressants
Single or repeated TSD or PSD plus:
• Light therapy
• Light therapy and phase advance
• rTMS
Single or repeated TSD or PSD plus
• Lithium
• SSRIs
• Pindolol

Chronobiology and mood disorders - Wirz-Justice Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
321
and are measurable even at the level of individual SCNneurones.61 However, attempts to generalize across vari-ous classes of antidepressant drugs have not been suc-cessful7: even though the monoamine oxidase inhibitor(MAOI) clorgyline lengthened circadian period,62 theMAOI moclobemide shortened it,63 and selective sero-tonin reuptake inhibitors (SSRIs) had no effect.63 Whenconsidering the model (Figure 1A), it is clear that drugscould act not only on circadian period but may also changephase position or phase relationships with the sleep-wakecycle, to enhance circadian amplitude or sensitivity to zeit-gebers. Evidence that imipramine and lithium modify thephase angle between the circadian temperature rhythmand the rest-activity cycle is interesting,64 as is the conceptthat stabilization of circadian rhythms may be a key actionof clinically effective mood-stabilizing drugs.65 In addition,sensitivity to light could be affected, as is the case withchronic clorgyline and lithium treatments.66
Nonpharmacological therapies
Sleep deprivation
Well documented is the rapid, usually short-lastingimprovement following total sleep deprivation and therapid return of depressive symptoms after subsequentrecovery sleep, indicating that the depressive process isstrongly sleep dependent.8 Additionally, sleep deprivationneeds to coincide with an early morning circadian phasefor optimal antidepressant response. Partial sleep depri-vation in the second half of the night or phase-advance ofthe sleep-wake cycle are equally efficacious (see Table Ifor a list of therapeutic modalities). The spontaneousswitch out of depression (and into hypomania and mania)often occurs after a “natural” sleep deprivation.This remarkable and immediate antidepressant modal-ity has been recognized for 30 years, but is little used ineveryday clinical practice. Perhaps it is the paradox oftaking sleep away from the depressive insomniac that hasa negative connotation for both patient and psychiatrist(“wake therapy” would be a more positive alternativename). Perhaps it is also the short-term nature of theresponse that has hindered its use, though the magnitudeof the clinical changes brought about by sleep depriva-tion still remain highly intriguing and may provide cluesfor understanding the pathophysiology of depression.Sleep deprivation is the paradigm par excellence fordepression research: rapid, nonpharmacological, and short
lasting. It may be the nonpharmacological nature of sleepdeprivation (it cannot be patented) that has contributedto its status as an “orphan drug.”67 It is surprising that nopharmaceutical company has focused on this model tosearch for that much-needed rapid-acting antidepressant.8
This lack may be remedied in the future; new researchreveals that, whereas sleep induces very few genes, wake-fulness increases expression of several groups of genes,68
and here comparisons with the effects of antidepressantdrug treatment may narrow down the candidates.Some committed proponents of sleep deprivation haverecognized its clinical usefulness to initiate rapidimprovement, particularly in the most severely depressedpatients in whom time is of the essence. Sleep depriva-tion is effective in all diagnostic subgroups of depression.The problem is the relapse after recovery sleep, and newstrategies have sought treatments to prevent this.Response appears to be well maintained by treatmentwith lithium, antidepressants (in particular SSRIs), or the5-HT1A receptor antagonist pindolol, as well as non-pharmacological adjuvants such as repetitive transcranialmagnetic stimulation (rTMS),69 light therapy, or phaseadvance of the sleep-wake cycle, or various combinationsthereof (see, for example, reference 36 and 70, reviewedin reference 8; Table I).
Light therapy
Light therapy can be considered to be the most success-ful clinical application of circadian rhythm concepts inpsychiatry to date. Light is the treatment of choice forSAD.71 The quality of recent SAD studies has beenexemplary, and the response rate is well above placebo(in fact, superior to analogous trials with antidepressantdrugs).72 The success of this nonpharmacological treat-ment has been astonishing, but it has taken rather longfor light therapy to be accepted by establishment psy-chiatry,72 and trials of other indications are still in theresearch phase. Its very success in SAD has limited usein other forms of depression (characterized as “it’s achronobiological treatment for a chronobiological sub-set of depressive patients”). However, light acts on thesame neurotransmitters, in particular serotonin, as themajor antidepressant drugs.71 This has been shown withtryptophan deletion tests, where relapse after successfullight therapy is induced, as well as the successful treat-ment of SAD patients by SSRIs.71 More direct evidenceof the immediate effects of light on serotonin turnover in

the brain has come from an in vivo study in healthy sub-jects: not only is serotonin turnover high in spring andsummer and low in autumn and winter (the pattern fol-lowing the hours of available sunshine), but serotoninturnover increases immediately after light exposure.73
Assuming that mood state is at least partially linked toserotonin turnover, the conclusions are obvious: morelight, better mood.The serotonin connection suggests that a broader use oflight therapy is indicated.A rapid response within a weekin SAD does not mean that other major depressive disor-ders will improve so fast: trials of light therapy over at least4 to 6 weeks, as would be standard for a drug treatmenttrial, are required.There is already good evidence for effi-cacy in bulimia, preliminary evidence for usefulness inprepartum and postpartum depression (clinical indicationswhere new nondrug therapies are sorely needed),74 andpromising findings in major depression, particularly as anadjuvant (Table I).74 Light is being recognized not only asa major zeitgeber necessary for our daily well-being (withapplications in the work place and in architecture), butalso as a “drug” that can be prescribed in dose, timing, andduration for specific diagnoses.71
An important step forward for the clinician has been thatall available randomized studies of light therapy for bothSAD and nonseasonal depression are being analyzed forefficacy, and will soon be published in the CochraneLibrary (www.cochrane.de).
“Dark” therapy
Single case studies of rapidly cycling bipolars have shownthat extending darkness (or rest, or sleep) immediatelystops the recurring pattern, which is a rather astonishingresult in these therapy-resistant patients.38,39 Further sup-port comes from recent findings that extended darkness(not rest and not sleep) in manic bipolar patients cancontrol their symptoms within days (B. Barbini, personalcommunication).The pineal hormone melatonin is designated the “hormoneof darkness.” Physiologically, it is important for timing thecascade of events initiating sleep in humans.20 The noctur-nal onset of melatonin secretion opens the gateway forsleep propensity, involving peripheral thermoregulatorymechanisms.75 The “warm feet effect” underlies its soporificaction and use in a variety of sleep disorders.20 The fewstudies administering melatonin to depressed patients haveindeed found improvements in sleep, but not in mood.76,77
Emerging therapies
New drugs, such as agomelatine (a melatonin agonist and5-HT2c antagonist), with a core action on circadianrhythms, are currently in development for the treatmentof mood disorders.A large multicenter study investigating agomelatine inmajor depression has yielded an excellent antidepressantresponse,78 which has been linked to the action of thecompound on the melatonergic and serotonergic systems.Moreover, the 5-HT2c receptor subtype is considered tobe relevant to the therapeutic properties of SSRIs, and—to link this to chronobiology—5-HT2c receptor agonists,which mimic the effects of light in rat CNS.79
Sleep shifts and zeitgebers as therapy
The above concepts point toward a multimodal approachto using chronobiological therapies in major depression.“Wake therapy” (increasing the level of process S) inducesrapid clinical improvement in all diagnostic subgroups;phase advance (changing the timing of sleep) maintainsthe response, as does light, drugs acting on the serotoner-gic system, or rTMS (which acts on the SCN80). Increasingzeitgeber strength improves the consistency of entrain-ment and circadian amplitude: this may be one mechanismunderlying the therapeutic efficacy of bright light and themelatonin agonist. There is evidence that depressedpatients, including those with SAD, have greater day-to-day and within-day mood variability than controls.81,82 InSAD patients, it has been shown that increasing zeitgeberstrength with light therapy reduced or eliminated bothgroup differences in mean level and variability of mood.82
Other zeitgebers (social cues, activity, and food) are impor-tant for improving behavioral feedback from peripheralclocks to overall entrainment stability. This is extremelyimportant in bipolar patients.37 The combination neededby the clinician for the sought-after rapid and long-lastingantidepressant, might well be an eclectic mix of these non-pharmacological modalities with antidepressant drugs.
Conclusion
We live in a 24-h society that is no longer strongly syn-chronized to the change in daylength or temperatureacross the seasons. A permanent “summer day” is theresult of artificial lighting, yet it is of insufficient intensityfor stable entrainment. Too little is known of the seque-
S t a t e o f t h e a r t
322

lae of irregular patterns of light exposure on a vulnera-ble circadian system, and how light could trigger or alle-viate a depressive phase. Could part of the increase inprevalence of depression in modern society be related tosuch factors? Genetic predisposition, hormonal fluctua-tions, environmental stress, and altered light-dark cyclescould all induce rhythm disturbances. Conversely, alteredsleep patterns, hyperarousal, eating behavior, and moodstate could feed back onto the circadian system via hor-mones and effects on peripheral oscillators. These new
insights provide us with useful strategies and a variety ofmethods to improve robustness of the circadian pace-maker and better synchronize its timing with respect tothe day-night cycle. It is interesting to reconsider thoseempirically developed 19th century psychiatric treat-ments, which consisted of establishing regularity in socialschedules and meal times, and manipulating sleep (albeitwith “cures”) and temperature (with cold baths), in termsof modern chronobiology and the importance of cor-rectly timed zeitgebers. ❏
Chronobiology and mood disorders - Wirz-Justice Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
323
REFERENCES
1. Wehr TA, Goodwin FK. Biological rhythms in manic-depressive illness. In:Wehr TA, Goodwin FK, eds. Circadian Rhythms in Psychiatry. Pacific Grove,Calif: The Boxwood Press; 1983:129-184.2. Wu JC, Bunney WE. The biological basis of an antidepressant responseto sleep deprivation and relapse: review and hypothesis. Am J Psychiatry.1990;147:14-21.3. Kuhs H, Tölle R. Sleep deprivation therapy. Biol Psychiatry. 1991;29:1129-1148.4. Leibenluft E, Wehr TA. Is sleep deprivation useful in the treatment ofdepression? Am J Psychiatry. 1992;149:159-168.5. Healy D, Waterhouse JM. The circadian system and the therapeutics ofthe affective disorders. Pharmacol Ther. 1995;65:241-263.6. Wirz-Justice A. Biological rhythms in mood disorders. In: Bloom FE,Kupfer DJ, eds. Psychopharmacology: The Fourth Generation of Progress. NewYork, NY: Raven Press; 1995:999-1017.7. Rosenwasser AM, Wirz-Justice A. Circadian rhythms and depression: clin-ical and experimental models. In: Redfern PH, Lemmer B, eds. Physiologyand Pharmacology of Biological Rhythms. Berlin, Germany: Springer Verlag;1997:457-486.8. Wirz-Justice A, Van den Hoofdakker RH. Sleep deprivation in depression:what do we know, where do we go? Biol Psychiatry. 1999;46:445-453.9. Boivin DB. Influence of sleep-wake and circadian rhythm disturbancesin psychiatric disorders. J Psychiatry Neurosci. 2000;25:446-458.10.Zeitzer JM, Dijk DJ, Kronauer RE, Brown EN, Czeisler CA. Sensitivity ofthe human circadian pacemaker to nocturnal light: melatonin phase reset-ting and suppression. J Physiol. 2000;526:695-702.11.Daan S, Beersma DGM, Borbély AA. Timing of human sleep: recoveryprocess gated by a circadian pacemaker. Am J Physiol. 1984;246:R161-R183.12.Klein DC, Moore RY, Reppert SM. Suprachiasmatic Nucleus: The Mind'sClock. New York, NY: Oxford University Press; 1991.13.Berson DM, Dunn FA, Takao M. Phototransduction by retinal ganglioncells that set the circadian clock. Science. 2002;295:1070-1073.14.Remé CE, Wirz-Justice A, Terman M. The visual input stage of the mam-malian circadian pacemaking system: I. Is there a clock in the mammalianeye? J Biol Rhythms. 1991;6:5-29.15.Wehr TA. Photoperiodism in humans and other primates: evidence andimplications. J Biol Rhythms. 2001;16:348-364.16.Lewy AJ. The dim light melatonin onset, melatonin assays and biolog-ical rhythm research in humans. Biol Signals Recept. 1999;8:79-83.17.Linkowski P, Van Onderbergen A, Kerkhofs M, Bosson D, Mendlewicz J,Van Cauter E. Twin study of the 24-h cortisol profile: evidence for geneticcontrol of the human circadian clock. Am J Physiol. 1993;264:E173-E181.18.Czeisler CA, Khalsa SBS. The human circadian timing system and sleep-wake regulation. In: Kryger MH, Roth T, Dement WC, eds. Principles andPractice of Sleep Medicine. 3rd ed. Philadelphia, Pa: WB Saunders Company;2000:353-375.19.Honma KI, Hashimoto S, Nakao M, Honma S. Period and phase adjust-ments of human circadian rhythms in the real world. J Biol Rhythms.2003;18:261-270.
20.Czeisler CA, Cajochen C, Turek FW. Melatonin in the regulation of sleepand circadian rhythms. In: Kryger MH, Roth T, Dement WC, eds. Principlesand Practice of Sleep Medicine. 3rd ed. Philadelphia, Pa: WB SaundersCompany; 2000:400-406.21.Danilenko KV, Cajochen C, Wirz-Justice A. Is sleep per se a zeitgeber inhumans? J Biol Rhythms. 2003;18:170-178.22.Monk TH, Kupfer DJ, Frank E, Ritenour AM. The Social Rhythm Metric(SRM): measuring daily social rhythms over 12 weeks. Psychiatry Res.1991;36:195-207.23.Buijs RM, Kalsbeek A. Hypothalamic integration of central and periph-eral clocks. Nature Rev Neurosci. 2001;2:521-526.24.Roenneberg T, Wirz-Justice A, Merrow M. Life between clocks: dailytemporal patterns of human chronotypes. J Biol Rhythms. 2003;18:80-90.25.Roenneberg T, Merrow M. The network of time: understanding themolecular circadian system. Curr Biol. 2003;13:R198-R207.26.Franken P, Chollet D, Tafti M. The homeostatic regulation of sleep needis under genetic control. J Neurosci. 2001;21:2610-2621.27.Jones CR, Campbell SS, Zone SE, et al. Familial advanced sleep-phasesyndrome: a short-period circadian rhythm variant in humans. Nat Med.1999;5:1062-1065.28.Ebisawa T, Uchiyama M, Kajimura N, et al. Association of structural poly-morphisms in the human period 3 gene with delayed sleep phase syn-drome. EMBO Rep. 2001;2:342-346.29. Iwase T, Kajimura N, Uchiyama M, et al. Mutation screening of the humanClock gene in circadian rhythm sleep disorders. Psychiatry Res. 2002;109:121-128.30.Desan PH, Oren DA, Malison R, et al. Genetic polymorphism at theCLOCK gene locus and major depression. Am J Med Genet. 2000;96:418-421.31.Shiino Y, Nakajima S, Ozeki Y, Isono T, Yamada N. Mutation screening ofthe human period 2 gene in bipolar disorder. Neurosci Lett. 2003;338:82-84.32.Johansson C, Willeit M, Smedh C, et al. Circadian clock-related poly-morphisms in seasonal affective disorder and their relevance to diurnalpreference. Neuropsychopharmacology. 2003;28:734-739.33.Yamazaki S, Numano R, Abe M, et al. Resetting central and peripheralcircadian oscillators in transgenic rats. Science. 2000;288:682-685.34.Schibler U, Ripperger J, Brown SA. Peripheral circadian oscillators inmammals: time and food. J Biol Rhythms. 2003;18:250-260.35.Wehr TA, Sack DA, Rosenthal N. Sleep reduction as a final commonpathway in the genesis of mania. Am J Psychiatry. 1987;144:201-204.36.Benedetti F, Barbini B, Campori E, Fulgosi MC, Pontiggia A, Colombo C.Sleep phase advance and lithium to sustain the antidepressant effect oftotal sleep deprivation in bipolar depression: new findings supporting theinternal coincidence model? J Psychiatr Res. 2001;35:323-329.37.Frank E, Swartz HA, Kupfer DJ. Interpersonal and social rhythm therapy:managing the chaos of bipolar disorder. Biol Psychiatry. 2000;48:593-604.38.Wehr TA, Turner EH, Shimada JM, Lowe CH, Barker C, Leibenluft E.Treatment of rapidly cycling bipolar patient by using extended bed rest anddarkness to stabilize the timing and duration of sleep. Biol Psychiatry.1998;43:822-828.39.Wirz-Justice A, Quinto C, Cajochen C, Werth E, Hock C. A rapid-cyclingbipolar patient treated with long nights, bedrest, and light. Biol Psychiatry.1999;45:1075-1077.

S t a t e o f t h e a r t
324
Cronobiología y trastornos afectivos
Las observaciones clínicas de la variación diurna del ánimo y el despertar precoz en la depresión se han incor-porado a sistemas diagnósticos establecidos, como es el caso de la modificación estacional que define la depre-sión invernal (trastorno afectivo estacional, TAE). Muchos ritmos circadianos medidos en pacientes depresi-vos son anormales: por ocurrir antes del tiempo que corresponde, tener una amplitud disminuida o una mayorvariabilidad. Para precisar si estas alteraciones tienen un significado etiológico en el rol que cumplen los rit-mos circadianos en los trastornos afectivos o si son una consecuencia de conductas alteradas se requiere deun análisis minucioso con protocolos muy estrictos (por ejemplo, rutina constante o desincronía forzada).Estos protocolos cuantifican las contribuciones del marcapaso circadiano y del proceso de sueño homeostá-tico que influyen en el ánimo, la energía, el apetito y el sueño. Estudios futuros aclararán algunas mutacio-nes alélicas de genes relacionados con el “reloj circadiano” o el “sueño” en la depresión. Respecto al trata-miento, los antidepresivos y los estabilizadores del ánimo no tienen efectos consistentes en la ritmicidadcircadiana. La estrategia antidepresiva más rápida conocida hasta la fecha es de tipo no farmacológico: la pri-vación total o parcial de sueño durante la segunda mitad de la noche. La desventaja de la privación de sueñoes que la mayoría de los pacientes recaen después de recuperar el sueño; esto puede prevenirse mediante lacoadministración de litio, pindolol, inhibidores de la recaptación de serotonina (5-HT), luz brillante, o a tra-vés de un procedimiento posterior de avance de fase. El avance de fase del ciclo sueño vigilia en forma exclu-siva tiene también rápidos efectos en el ánimo depresivo, lo que dura mayor tiempo que la privación desueño. La luz es el tratamiento de elección para el TAE y puede resultar útil en la depresión no estacional aladministrarla sola o en combinación con medicamentos. Los conceptos cronobiológicos enfatizan el impor-tante papel de los “zeitgebers” para estabilizar la fase, siendo la luz el más importante, pero también sedeben considerar los períodos de oscuridad (y reposo), la regularidad de los horarios sociales y de las comi-das y el empleo de melatonina o de sus análogos. Los avances en la cronobiología continúan para contribuira nuevos tratamientos para los trastornos afectivos.
40.Borbély AA, Wirz-Justice A. Sleep, sleep deprivation and depression. HumNeurobiol. 1982;1:205-210.41.Koorengevel KM, Beersma DGM, den Boer JA, Van den Hoofdakker RH.A forced desynchrony study of circadian pacemaker characteristics in sea-sonal affective disorder. J Biol Rhythms. 2002;17:463-475.42.Avery DH, Dahl K, Savage MV, et al. Circadian temperature and corti-sol rhythms during a constant routine are phase-delayed in hypersomnicwinter depression. Biol Psychiatry. 1997;41:1109-1123.43.Wirz-Justice A, Kräuchi K, Brunner DP, et al. Circadian rhythms and sleepregulation in seasonal affective disorder. Acta Neuropsychiatrica. 1995;7:41-43.44.Brunner DP, Kräuchi K, Dijk DJ, Leonhardt G, Haug HJ, Wirz-Justice A.Sleep electroencephalogram in seasonal affective disorder and in controlwomen: effects of midday light treatment and sleep deprivation. BiolPsychiatry. 1996;40:485-496.45.Koorengevel K, Beersma D, Den Boer J, van den Hoofdakker R. Sleep inseasonal affective disorder patients in forced desynchrony: an explorativestudy. J Sleep Res. 2002;11:347-356.46.Cajochen C, Brunner DP, Kräuchi K, Graw P, Wirz-Justice A. EEG and sub-jective sleepiness during extended wakefulness in seasonal affective disor-der: circadian and homeostatic influences. Biol Psychiatry. 2000;47:610-617.47.Putilov A, Donskaya OG, Jafarova OA, Danilenko KV. Waking EEG powerdensity in hypersomnic winter depression. 12th Annual Meeting of theSociety for Light Treatment and Biological Rhythms. 7-9 May 2000.Evanston, Ill. Abstracts p24.48.Taillard J, Philip P, Coste O, Sagspe P, Bioulac B. Circadian and homeo-static buildup of sleep pressure during extended wakefulness in morningand evening chronotypes. J Sleep Res. 2003. In press.
49.Boivin DB, Czeisler CA, Dijk DJ, et al. Complex interaction of the sleep-wake cycle and circadian phase modulates mood in healthy subjects. ArchGen Psychiatry. 1997;54:145-152.50.Schröder C, Knoblauch V, Renz C, Kräuchi K, Wirz-Justice A, Cajochen C.Circadian modulation of mood under differential sleep pressure conditions.Sleep. 2003;26(suppl):A101.51.Wever RA. The Circadian System of Man: Results of Experiments underTemporal Isolation. New York, NY: Springer Verlag; 1979.52.Healy D, Minors DS, Waterhouse JM. Shiftwork, helplessness and depres-sion. J Affect Disord. 1993;29:17-25.53.Wehr TA, Duncan WCJ, Sher L, et al. A circadian signal of change of sea-son in patients with seasonal affective disorder. Arch Gen Psychiatry.2001;58:1108-1114.54.Wehr TA, Moul DE, Barbato G, et al. Conservation of photoperiod-responsive mechanisms in humans. Am J Physiology. 1993;265:R846-R857.55.Surridge-David M, MacLean A, Coulter ME, Knowles JB. Mood changefollowing an acute delay of sleep. Psychiatry Res. 1987;22:149-158.56.Jauhar P, Weller MP. Psychiatric morbidity and time zone changes: astudy of patients from Heathrow airport. Br J Psychiatry. 1982;140:231-235.57.Young DM. Psychiatric morbidity in travelers to Honolulu, Hawaii. ComprPsychiatry. 1995;36:224-228.58.Regestein QR, Monk TH. Delayed sleep phase syndrome: a review of itsclinical aspects. Am J Psychiatry. 1995;152:602-608.59.Engelmann W. Lithium slows down the Kalanchoe clock. Z Naturforsch[B]. 1972;27:477.60.Johnsson A, Engelmann W, Pflug B, Klemke W. Influence of lithium ionson human circadian rhythms. Z Naturforsch [C]. 1980;35:503-507.

Chronobiology and mood disorders - Wirz-Justice Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
325
61.Abe M, Herzog ED, Block GD. Lithium lengthens the circadian period ofindividual suprachiasmatic nucleus neurons. Neuroreport. 2000;11:3261-3264.62.Wirz-Justice A, Campbell IC. Antidepressant drugs can slow or dissociatecircadian rhythms. Experientia. 1982;38:1301-1309.63.Wollnik F. Effects of chronic administration and withdrawal of antide-pressant agents on circadian activity rhythms in rats. Pharmacol BiochemBehav. 1992;43:549-561.64.Nagayama H. Chronic administration of imipramine and lithium changesthe phase-angle relationship between the activity and core body tempera-ture circadian rhythms in rats. Chronobiol Int. 1996;13:251-259.65.Klemfuss H, Kripke DF. Antimanic drugs stabilize hamster circadianrhythms. Psychiatry Res. 1995;57:215-222.66.Duncan WC, Johnson KA, Wehr TA. Decreased sensitivity to light of thephotic entrainment pathway during chronic clorgyline and lithium treat-ments. J Biol Rhythms. 1998;13:330-346.67.Wirz-Justice A. Why is sleep deprivation an orphan drug? Psychiatry Res.1998;81:281-282.68.Cirelli C. How sleep deprivation affects gene expression in the brain: areview of recent findings. J Appl Physiol. 2002;92:394-400.69.Eichhammer P, Kharraz A, Wiegand R, et al. Sleep deprivation in depres-sion stabilizing antidepressant effects by repetitive transcranial magneticstimulation. Life Sci. 2002;70:1741-1749.70.Colombo C, Lucca A, Benedetti F, Barbini B, Campori E, Smeraldi E. Totalsleep deprivation combined with lithium and light therapy in the treatmentof bipolar depression: replication of main effects and interaction. PsychiatryRes. 2000;95:43-53.71.Lam RW, Levitt AJ. Canadian Consensus Guidelines for the Treatment ofSeasonal Affective Disorder. Canada: Clinical & Academic Publishing; 1999.
72.Wirz-Justice A. Beginning to see the light. Arch Gen Psychiatry.1998;55:861-862.73.Lambert GW, Reid C, Kaye DM, Jennings GL, Esler MD. Effect of sunlightand season on serotonin turnover in the brain. Lancet. 2002;360:1840-1842.74.Lam RW. Seasonal Affective Disorder and Beyond. Light Treatment for SADand Non-SAD Conditions. Washington DC: American Psychiatric Press; 1998.75.Kräuchi K, Wirz-Justice A. Circadian clues to sleep onset mechanisms.Neuropsychopharmacology. 2001;25:S92-S96.76.deVries MW, Peeters FP. Melatonin as a therapeutic agent in the treat-ment of sleep disturbance in depression. J Nerv Ment Dis. 1997;185:201-202.77.Dolberg OT, Hirschmann S, Grunhaus L. Melatonin for the treatment ofsleep disturbances in major depressive disorder. Am J Psychiatry. 1998;155:1119-1121.78.Lôo H, Dalery J, Macher JP, Payen A. Pilot study comparing in blind thetherapeutic effect of two doses of agomelatine, melatoninergic agonist andselective 5-HT2C receptors antagonist, in the treatment of major depressivedisorders. Encephale. 2003;28:356-362.79.Kennaway DJ. Light, neurotransmitters and the suprachiasmatic nucleuscontrol of pineal melatonin production in the rat. Biol Signals Recept.1997;6:247-254.80.Ji R, Schlaepfer T, Aizenman C, et al. Repetitive transcranial magneticstimulation activates specific regions in rat brain. Proc Natl Acad Sci U S A.1998;95:15635-15640.81.Hall DP, Sing HC, Romanoski AJ. Identification and characterization ofgreater mood variance in depression. Am J Psychiatry. 1991;148:418-419.82.Krauss SS, Depue RA, Arbisi PA, Spoont M. Behavioral engagement level,variability, and diurnal rhythm as a function of bright light in bipolar II sea-sonal affective disorder: an exploratory study. Psychiatry Res. 1992;43:147-160.
Chronobiologie et troubles de l’humeur
Les observations cliniques de variations diurnes de l’humeur et de réveil matinal précoce dans la dépressionont été intégrées dans des systèmes diagnostiques établis tel le facteur saisonnier qui définit la dépressionhivernale (trouble affectif saisonnier, TAS). Beaucoup de rythmes circadiens mesurés chez les patients dépres-sifs sont anormaux : plus précoces, diminués en amplitude ou de plus grande variabilité. Seuls des protoco-les rigoureux (par exemple, routine constante ou désynchronisation forcée) sont à même de déterminer sices perturbations ont une signification étiologique quant au rôle des rythmes circadiens dans les troubles del’humeur ou si elles sont la conséquence d’une modification comportementale. Ces protocoles quantifientles participations respectives de l’oscillateur circadien et d’un processus homéostatique lié au sommeil ayantdes répercussions sur l’humeur, l’énergie, l’appétit et le sommeil. Les études à venir mettront en évidence,si tant est qu’elles existent, les mutations alléliques des gènes qui interviennent dans les phénomènes « d’hor-loge » ou de « sommeil » au cours de la dépression. En ce qui concerne le traitement, les antidépresseurs etles régulateurs de l’humeur n’ont pas d’effet constant sur le rythme circadien. L’effet antidépresseur le plusrapide connu à ce jour n’est pas pharmacologique : c’est la privation totale ou partielle de sommeil dans laseconde moitié de la nuit. L’inconvénient de la privation de sommeil, constitué par la rechute de la plupartdes patients après le sommeil de récupération, peut être prévenu par l’administration concomitante de li-thium, de pindolol, d’inhibiteurs de la recapture de la sérotonine (5-HT), de lumière vive ou par une procé-dure d’avance de phase. L’avance de phase dans les cycles veille-sommeil exerce par elle-même égalementdes effets rapides sur l’humeur dépressive qui se maintiennent plus longtemps que ceux de la privation desommeil. La photothérapie est le traitement de choix du TAS et pourra s’avérer utile dans la dépression nonsaisonnière, seule ou en association à un traitement médicamenteux. Les concepts chronobiologiques sou-lignent le rôle important des synchroniseurs dans la stabilisation de phase, la lumière étant le plus important.Cependant, les périodes d’obscurité (et de repos), la régularité des repas et des rythmes sociaux et l’utilisa-tion de la mélatonine ou de ses analogues doivent être également considérées. Les avancées en chronobio-logie continuent à contribuer au développement de médicaments nouveaux dans les troubles affectifs.


he rhythmic (as opposed to linear) expression ofbiological variables and the temporal organization of theserhythms represent an adaptation of organisms to therhythmic changes in the external environment. Periodicoscillations (rhythms) have been documented in biologi-cal variables in a whole spectrum of living organisms (fromunicellular to multicellular).1,2 However, this phenomenonis not merely a reaction to environmental changes; it isgenerally held that the rhythms are governed by an activesystem capable of self-sustained oscillations (endogenousrhythms).1 Consequently, the shape of rhythms and the
S t a t e o f t h e a r t
327Copyright © 2003 LLS SAS. All rights reserved www.dialogues-cns.org
Concepts in human biological rhythmsAlain Reinberg, MD, PhD; Israel Ashkenazi, PhD
Keywords: biological rhythm; temporal organization; desynchronization;allochronism; dyschronism; shift work; affective disorder
Author affiliations: Unité de Chronobiologie, Fondation Adolphe deRothschild, Paris, France (Alain Reinberg); Department of Human Geneticsand Molecular Medicine, School of Medicine, Tel Aviv University, Ramat Aviv,Israel
Address for correspondence: Alain Reinberg, Unité de Chronobiologie,Fondation Adolphe de Rothschild, 29 rue Manin, 75940 Paris Cedex 19,France(e-mail: [email protected])
T
Biological rhythms and their temporal organization are adaptive phenomena to periodic changes in environmen-tal factors linked to the earth’s rotation on its axis and around the sun. Experimental data from the plant and ani-mal kingdoms have led to many models and concepts related to biological clocks that help describe and understandthe mechanisms of these changes. Many of the prevailing concepts apply to all organisms, but most of the experi-mental data are insufficient to explain the dynamics of human biological clocks. This review presents phenomenathat are mainly characteristic of—and unique to—human chronobiology, and which cannot be fully explained byconcepts and models drawn from laboratory experiments. We deal with the functional advantages of the humantemporal organization and the problem of desynchronization, with special reference to the period (τ) of the circa-dian rhythm and its interindividual and intraindividual variability. We describe the differences between right- andleft-hand rhythms suggesting the existence of different biological clocks in the right and left cortices.Desynchronization of rhythms is rather frequent (one example is night shift workers). In some individuals, desyn-chronization causes no clinical symptoms and we propose the concept of “allochronism” to designate a variant ofthe human temporal organization with no pathological implications. We restrict the term “dyschronism” to changesor alterations in temporal organization associated with a set of symptoms similar to those observed in subjects intol-erant to shift work, eg, persisting fatigue and mood and sleep alterations. Many diseases involve chronic depriva-tion of sleep at night and constitute conditions mimicking that of night shift workers who are intolerant to desyn-chronization. We also present a genetic model (the dian-circadian model) to explain interindividual differences inthe period of biological rhythms in certain conditions.© 2003, LLS SAS Dialogues Clin Neurosci. 2003;5:327-342.

temporal order are products of the interaction betweenendogenous (genetically controlled) oscillators and thephases (synchronizing, entraining) of external cues.
Features of biological rhythm
The parameters of a biological rhythm are as follows1-6:• The period τ (τ≈24 h in circadian rhythm; and τ<20 h in
ultradian rhythm).• The acrophase (Φ, the peak time of the rhythm). This
parameter usually includes a phase reference within thetime axis of the rhythm (eg, for the circadian rhythmthe acrophase relates to a phase reference like mid-night, local time, or mid-sleep).
• The amplitude (A), the peak-to-trough difference.• The mean level, or mesor (M).Rhythms that follow a cosine curve can be characterizedby all four of these parameters, and rhythms that do notfollow cosine shape are mostly characterized by M and τ.The majority of the rhythms studied in nature, and espe-cially in humans, exhibit circadian periodicity, and thisreview will focus mainly on these (though most of discus-sions herein also apply to rhythms with other periodicities).Circadian rhythms have the following properties1-8:• They have a genetic origin.• They are controlled by biological clocks (or oscillators
or circadian pacemakers).• The biological clocks are reset (Φ) and calibrated
(τ=24 h) by environmental signals that also have τ=24 h,such as dawn/dusk (photic signals), activity/rest, ornoise/silence (nonphotic signals).These periodic envi-ronmental factors are called synchronizers,9 zeitge-
bers,10 or entraining agents.7 The range of periodentrainment of circadian rhythms by the zeitgebersmay vary between τ=20 h and τ=28 h.
• There is a general ubiquity7,8 of the properties of thebiological rhythms quoted above, from unicellulareukaryotes8,11,12 to humans.2,5,13 However, some variabil-ity exists and some differences can be observed amongplants,12 animals,13 strains of the same species,14 and evendifferent human individuals.5,13,15,16
The master clock versus temporal organization
In recent years, a large amount of information has accu-mulated about the genetic, molecular, physiological, andenvironmental induction of biological rhythms and abouthow they function in various genera and species. Due tothe variety and variability of this vast literature, it is nolonger an easy task to review concepts in human biolog-ical rhythms. We will first try to present the reasons forthis difficulty.Two schools of thoughts coexist in chronobiology. Oneconsiders that the study of biological rhythms must involvean analytical approach to phenomena and confine itself toreductionism.17 A relatively simple molecular geneticmodel is proposed,18-20 as is the existence of one domi-neering master clock (the suprachiasmatic nucleus [SCN]in mammals and certain species of birds) that controlsalmost all rhythmic functions.21,22 Consequently, most stud-ies of the circadian system focused on the recording of oneovert rhythm (eg, activity/rest), especially in rodent animalmodels, such as hamsters, rats, and mice.18,19 Although thisschool of thought has recently recognized the existence ofperipheral pacemakers and oscillators, they are placed ina lower hierarchical level than the master clock.The other school of thought favors a holistic perspectiveand considers that the studied subject (ie, man) as a wholeis engulfed by normal habitat and time cues.4,5,23-26 Both theliving organism and the rhythmic and nonrhythmicchanges in its environmental factors are taken intoaccount.Thus, a whole range of biological clocks—and notjust one—play a role, as well as a rather large set of genes,many with pleiotropic effects,16,27 rather than just a few.18-20
Another important point about this approach is theemphasis on temporal organization,4-7,23-26,28 rather than thestudy of one or two rhythms. For an organisms synchro-nized with τ=24 h, the study will document a set of bio-logical variables each characterized by its specific Φ(Figure 1).26 A review of the literature shows that even
S t a t e o f t h e a r t
328
Selected abbreviations and acronymsA amplitudeCRT choice reaction timeDH dominant hand L:D light/darkM meanNDH nondominant handΦ acrophase (peak time)PS paradoxical sleepREM rapid eye movementRT reaction timeSCN suprachiasmatic nucleusSD Sprague-Dawley (rat)SRT single reaction timeτ period

unicellular eukaryote organisms such as Acetabularia (analgae) and Euglena (a protist), which possess no nervousor endocrine systems, contain a population of oscillatorsand a temporal structure can be demonstrated.8-11
Terms such as temporal organization, temporal structure,temporal order, and time structure are synonymous.Various models have been proposed to better under-stand the “hierarchy” and the “coupling” between oscil-lators and/or biological clock systems.13,22,23
We propose that these two schools of thoughts are com-plementary rather than exclusive, but it is clear that anaccurate and objective definition is far from easy to make.Another difficulty resides in the fact that some authorsrecommend avoiding investigations on human subjects,since they believe that humans can only produce “sloppy”rhythms.29 It should be noted that this statement was made
without providing a definition of human rhythm sloppi-ness.This appears to come from the idea that many of thestudies carried out 20 years ago were investigations onmammalian rhythms conducted on laboratory hamsters,rats, and mice, for which the prominent synchronizer islight/dark (L:D) alternation. In these species, a photic sig-nal of few lux is powerful enough to synchronize rhythms,which should be compared with the 2500 lux (bright light)needed to synchronize human rhythms.13,30,31 Recent stud-ies show that even human rhythms can be entrained bylow intensity light.32
Another example that illustrates the confusion in defininga concept due to a focus on the rhythm of one variablerather than on the temporal order is the following. In the1970s, most sleep studies were extensively carried on cats,using electroencephalography (EEG). It was shown thatmost individuals of this species are frequent sleepers, witha polyphasic rhythmicity.According to Jouvet,33 no morethan 30% of cats exhibit a sleep/wake rhythm with τ=24 h.As a result, it was believed by some authors that cat is aspecies that does not possess a circadian organization—anidea that was a source of conflict between sleep and bio-logical rhythm specialists. However, cats exhibit circadianrhythms in their feeding behavior and activity/restrhythm.34,35 It proved difficult to bridge the gap betweenthose involved in sleep research in cats and those studyingcircadian rhythms in laboratory rodents.33
The final source of misunderstanding in concept defini-tion relates to the fact that the meaning of a given termevolves as time passes. Let us take the term chronobioticas an example.25,26,36-38 Simpson et al36 hypothesized thata drug might be able to phase shift all circadian rhythmsby resetting their respective Φs. In fact, there is still nosuch wonderdrug.37,38 Thereafter, the meaning of the termchronobiotic was restricted to a drug able to phase shiftor reset one39 or a limited number25,26 of rhythms.The lat-ter demonstrates once again the importance of studyingsystems or temporal order rather than just one rhythm.Considering the above examples, the definitions and con-cepts presented in this paper have been updated with ref-erence to the recent state of art.
Temporal organization
Temporal organization refers to the sequential array ofrhythms of various variables, each with a specific phaseon the time axis. An examination of the array providesinformation about the phase relationship between the
Concepts in human biological rhythms - Reinberg and Ashkenazi Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
329
Figure 1. Aspects of the human temporal organization: physiologicalfunctions of the cardiovascular system. The acrophase (Φ) loca-tion (blue circles) of any of the considered rhythms is not ran-domly distributed over 24 h. On the contrary, acrophases rep-resent physiologically validated temporal relationships. Thehealthy young human adults’ synchronization was approxi-mately 16 h of diurnal activity and 8 h of nocturnal rest.Reproduced from reference 26: Reinberg A. Chronobiologie Médicale,Chronothérapeutique. Paris, France: Flammarion Médecine-Sciences;2003. Copyright © 2003, Flammarion Médecine-Sciences.
Midnight Midnight6 AM Midday 6 PM
SleepBlood flowHeart rateSystolic blood pressureDiastolic blood pressureBlood volumeBlood
Urine
Renin activityAldosteroneCortisolAdrenalineNoradrenalineAtrial natriuretic factorPlatelets (number)Platelets (aggregability)FibrinogenHypercoagulability
AdrenalineNoradrenalinePotassiumSodium
Physiological function

rhythms, but does not show whether there is a causalinteraction between them. One example is body tem-perature rhythm and paradoxical sleep (PS) or rapid eyemovement (REM) rhythm. In humans, a physiologicaltrough in temperature coincides in time with the longest
episodes of PS.40,41 Animal experiments have demon-strated that hypothermia influences PS.42 Thus, while aphase relationship between the two rhythms does not initself imply a causal relationship, the physiological inter-action between the two variables raises the strong possi-
S t a t e o f t h e a r t
330
Figure 2. Distributions of circadian rhythm acrophases (Φ) according to the variables’ function. A to G illustrate the 24-h acrophase frequency distrib-ution of 7 groups of variables, and the dendrogram H shows the similarities along the groups by clusters on correlation scale (r). The uppercluster in H presents the greater similarities among the physiological variables (A), cognitive function (B), and hormones (C), where most ofthe acrophases occur in the late afternoon. In the inorganic molecules (D) and the organic molecules (E) groups (middle cluster H), mostacrophases aggregate around midday. The third cluster (lower cluster, H) contained cellular components (F) and enzymes (G), in which mostacrophases were distributed around midnight. Reproduced from reference 24: Ticher A, Ashkenazi IE, Reinberg A. Preservation of the functional advantage of human time structure. FASEB J. 1995;9:269-272.Copyright © 2003, Federation of American Societies for Experimental Biology.
A. Physiological variables
Midnight 6 AM Midday 6 PM Midnight0
10
20
30
Time
%
D. Inorganic molecules
Midnight 6 AM Midday 6 PM Midnight0
10
20
30
Time
%
F. Cellular components
Midnight 6 AM Midday 6 PM Midnight0
10
20
30
Time
%
B. Cognitive function
Midnight 6 AM Midday 6 PM Midnight0
10
20
30
Time
%
E. Organic molecules
Midnight 6 AM Midday 6 PM Midnight0
10
20
30
Time
%
G. Enzymes
Midnight 6 AM Midday 6 PM Midnight0
10
20
30
Time
%
C. Hormones
Midnight 6 AM Midday 6 PM Midnight0
10
20
30
Time
%
-0.5 0.0 r 0.5 1.0
ABC
DEFG
H

bility that they are coupled to the same oscillator or thatthere is a causal interaction between the two.A simplified circadian map of the temporal cardiovascu-lar organization of healthy young adults provides anotherexample (Figure 1). It presents the acrophases (Φs) of alimited number of physiological functions.The peak timelocations are not randomly distributed over 24 h, but cor-respond to the human needs related to diurnal activityand nocturnal rest. Here, there is a causal phase rela-tionship between the Φ of blood pressure and that ofvariables known to be involved in its control. The Φs ofrenin activity, aldosterone, cortisol, and catecholaminesprecede in phase the blood pressure Φ. Likewise, the Φsof aldosterone and cortisol precede the Φs of the urinaryexcretion of sodium and potassium.A similar temporal organization can be observed in therat (Sprague-Dawley [SD]), with a phase shift of 12 hwith regard to humans (these rodents are nocturnallyactive). Lemmer et al43 used transgenic SD rats, in whichthe mouse renin gene REN-2 had been inserted into theSD rat genome (TGR(mREN-2)). The transgenic ratsdeveloped hypertension and their blood pressure, renin,and aldosterone rhythms were phase shifted with regardto the heart rate rhythm, in comparison to the normaltemporal organization control of SD rats.43
This indicates that a physiological function, eg, cardio-vascular function, involves a set of rhythms, some ofwhich are independent of each other and some of whichexhibit strong interactions (or coupling). Consequently,temporal organization should generally be regarded as amultifactor rhythm system.
The functional advantage of human temporal organization
We have seen that the sequential array of rhythms over24 h constructs temporal organization.The rhythm phaseof each variable can be identified by location of its Φ.Another characteristic of rhythm is the ratio A/M, whichindicates the strength of the rhythm to shifting signals.Thus, to examine the question of whether temporal orga-nization is structured to endow the organism with a func-tional advantage, three parameters must be assessed:• Time-dependent distribution of the Φs of the variables’
rhythms.• Time distribution of variables’ rhythms according to
function.• Time distribution of the A/M ratio.
Ticher et al24 conducted such a study by computing theseparameters for 168 circadian rhythms of diurnally active(7 AM ±30 min to 11 PM ±60 min) young human subjects.The analysis showed that the distribution of the Φs over24 h exhibits a strong time dependence (Figure 2). TheΦs are unevenly distributed over 24 h and no Φ wasdetected between 5 AM and 7 AM. This time zone corre-sponds to the overall greatest vulnerability of the humanorganism, eg, the circadian Φ of the human mortalityrhythm, including all-cause mortality.25,26,44 The number ofΦs per hour was then clustered according to function.Seven groups were formed• 37 physiological rhythms (body temperature, blood
pressure, bronchial patency, etc).• 32 rhythms for cognitive function.• 27 rhythms for endocrine function.• 14 rhythms for metabolites.• 25 rhythms for organic molecules.• 18 rhythms for cellular components.• 15 rhythms for enzymatic activity.A correlation matrix of the pattern of distribution of theΦs between each of the 7 groups served as a basis forcluster analysis.The greater the coefficient r, the strongerthe similarity in the distribution of the Φs. An dendro-gram (H in Figure 2) can be constructed to visualize thesimiliarities.The level of correlation is shown by the dis-tance between each group. It can be seen that the corre-lation is very strong between physiological variables andcognitive function rhythms with Φs clustering in the lateafternoon. The correlation between cognitive functionand hormone rhythms remains strong. Organic and inor-ganic substance rhythms exhibit rather strong similaritieswith Φs clustering around 1 PM. Rhythms in cellular fea-tures and enzymatic activities also show a rather strongsimilarity with a cluster around midnight.The time distribution of A/M ratio also exhibited a sig-nificant time dependence with modes: at preawakingtime; postawaking time and morning meal; time of mid-day meal; time of evening meal; and around midnight(time of falling asleep). This suggests that “stronger”rhythms are clustered around the times where the humanis confronted with the domineering exogenous signals.These types of analyses enable us to explore the possibleadaptive value of the human temporal organization,which allows variables of each function to reach theirpeak time in phase with predictable environmentalchanges, such as night and day, in alternation with othersynchronizing signals.
Concepts in human biological rhythms - Reinberg and Ashkenazi Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
331

The synchronization of human circadian rhythms
The major environmental signals that trigger biologicalclocks in most animals in nature and in laboratoryrodents are related to the L:D alternation and photic sig-nals.7,13,21 Human circadian rhythms can also be synchro-nized by photic signals,30,31,45,46 but are mainly determinedby social signals, like those involving the senses of sight,sound, smell, or touch (or even other signals like roost-ers, which signaled the beginning of daily activity in thetime before clocks).47
The importance of nonphotic signals can be demon-strated by free-running experiments, in which a group ofsubjects is isolated from known time clues and cues.When each subject is isolated separately from the others,the circadian rhythm τ differs from 24 h, and it differsalso from subject to subject (range 24.3 to 25.4 h).5,13,48 Ingroup isolation, the rhythm τ (eg, sleep/wake) differsfrom 24 h, but is identical for all the subjects in the group(eg, τ=24.8 h),49,50 ie, social interaction synchronizes therhythms of subjects living closely in a group.Another nonphotic signal that triggers circadian rhythms,including those of human subjects, is physical activity.51-53
For example, nocturnal activity (15 min/h on ergomet-ric bicycle) induced a phase shift of body temperaturerhythms in two-thirds of subjects.51 In crewmembers of atransmeridian flight, diurnal outdoor exercise speeds upthe resynchronization of the urinary 17-hydroxycorti-costeroid circadian rhythm, compared with those with-out exercise.52
Masking effects
The advantage of a rhythm with the shape of a cosinefunction was discussed above. However, the patterns ofmany circadian rhythms deviate from that of an optimalcosine function. In many cases, a secondary peak orshoulder is observed in the 24-h pattern. This shouldermay indicate the presence of additional period compo-nent (eg, with τ<20 h), and the rhythm may be defined asa compound rhythm. However, the change may be dueto masking effect. Masking is the result of a direct influ-ence of one variable on another, or a direct influence ofan external stimulus on a variable, without reference toa rhythmic process.48 In natural settings and habitual lifeconditions, the body temperature rhythm curve is trape-zoidal rather than close to a cosine curve. Mills et al53 and
Czeisler and Wright46 proposed a constant routine pro-tocol, where the masking influences of ambient light,temperature, noise, food consumption, and activity levelare carefully controlled. Subjects stayed awake in reclin-ers for 24 to 48 h in dim light. In this condition, theunmasked rhythms of, for example, body temperature,exhibited a curve close to a cosine function.This type of experiment suggests that, in the real world,masking effects may alter the curve of many circadianrhythms. However, it should be noted that the constantroutine protocol, which involves sleep deprivation, mightalter the circadian period of a set of variables and its ade-quacy for this study will be discussed in another sectionof this paper.
Quantification of rhythm parameters withspecial reference to τ
In circadian rhythm studies, the critical parameter to bequantified is τ. In most investigations, it is assumed thatτ=24 h (as a mean) when subjects are synchronized witha diurnal activity and nocturnal rest with stable and reg-ular times (eg, awakening [lights on] at 7 AM and retiring[lights off] at 11 PM). Using this procedure, a set ofrhythms can be documented in subjects with a samplinginterval of, for example, 4 h over a 24- or 48-h period.Using this transverse sampling, other circadian parame-ters can be computed, such as Φ,A, and 24-h M, providedthe parameters exhibit statistically significant rhythms.However, with a transverse sampling of this kind, 24-hrhythm is computed, but not the circadian τ.This can onlybe obtained by longitudinal sampling over at least 7 days.With these requirements, inter- and intraindividualchanges can be taken into account, which is mandatoryto document human rhythms in certain circumstances.Prominent τ with the largest A, as well as other periods(with lower As) are quantified from time series by rele-vant methods including power spectra.5,6,16,26,28,44
The precise quantification of τ is critical to problems suchas one versus several biological clocks, as well as few ver-sus many clock genes.
One versus several biological clocks in primates
Experiments in rodents yielded a widely accepted modelfor the control of biological rhythms. According to thismodel, the SCN functions as a master (central) clock
S t a t e o f t h e a r t
332

Concepts in human biological rhythms - Reinberg and Ashkenazi Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
333
from which slave (peripheral) clocks, or subordinatestructures, receive their rhythm characteristics such as thecircadian τ, A, and Φ.13,18,21,22,54 According to Moore andSilver22:“... all of the available data support the view thatthe SCN is the circadian pacemaker responsible for pro-viding a temporal organization of behavioral, physiolog-ical, and endocrine functions. As pacemaker, the SCNsets the phase of oscillators of many physiological andendocrine rhythms in the body.”Transplantation of SCNin hamster tau mutants was associated with a rhythm ofactivity with the same τ as the donor rather than thehost.55 Genetic and molecular studies in rodents supportthis model.18,22,56,57
Is this model valid for other mammalian species?
In longitudinal studies, Jouvet et al42 assessed hourly thedistribution of PS in cats kept in isolation chambersunder continuous light (L:L). Under these conditions, arobust circadian rhythm of PS was detected in all normalcats, and in 4 out of 6 pontine cats (where all neural struc-tures rostral to the pons were removed), as well as in catswithout SCN or without hypothalamus.This result is evi-dence for the presence of a multioscillatory circadian sys-tem in this species.The squirrel monkey, a primate, has a prominent and sta-ble body temperature circadian rhythm.13 After totalbilateral SCN lesions, feeding and drinking behaviorslose their circadian rhythms, but the rhythm in body tem-perature was found to persist when studied over 1 yearpostlesion.13 Presumably, in primates, there are other bio-logical clocks outside the SCN, which are responsible forgenerating a rhythm for temperature, and other variables,such as cortisol rhythms in the rhesus monkey.58
There is no doubt that the SCN plays an important rolebecause it is the only anatomical structure in which a cir-cadian pacemaker has been identified and it is reset byphotic triggers. However, it seems that in cats and pri-mates (and presumably in many other species), othermajor pacemakers are present.
Desynchronization of human circadian rhythms
Aschoff and Wever recorded rhythms in human subjectsindividually isolated from known zeitgebers in long-term(>3 weeks) longitudinal experiments.48,59 They observedthat, after a fortnight, 28% of women and 23% of men,
exhibited τ ≅25 h for body temperature rhythm and τ=13to 36 h for sleep/wake rhythm. Thus, the phase relationbetween rhythms was distorted compared with the struc-ture of the normal temporal order in the isolated state.On this basis, it was suggested that the two documentedrhythms were driven by different biological clocks, a phe-nomenon called internal desynchronization.60
External desynchronization corresponds to a conditionin which the phase relation of rhythms are changed bymanipulating external synchronizers.This category refers,for example, to a phase shift of at least 5 h due to trans-meridian flight or shift work (even if the rhythm τ wasnot changed) and/or an induced change in τ, becominglonger or shorter than 24 h.The term desynchronization was used thereafter, toreport the experimental fact that, for a set of variables,the (endogenous) circadian τs can differ from oneanother and from 24 h in the same subject during longi-tudinal studies, even in the presence of natural zeitgebers.This was documented for circadian rhythms such as activ-ity/rest, body temperature, heart rate, grip strength ofboth hands, and cognitive performance.48,61-73
The τ of the circadian rhythm for hand grip strength mayeven differ between the right and left hands, as well asfrom 24 h.This was documented in a set of studies involv-ing both Caucasian and Asian shift workers,63,68,70 healthyvolunteers involved in placebo studies,64 geographerssojourning in the high Arctic summer,65 and saber fencersof the French Olympic team.66 Apart from the night shifts(about 4 nights out of 20) of shift workers,63,68,70 all subjectswere synchronized with diurnal activity and nocturnalrest. Test times were similar for both hands, eg, 4 to 6times a day during a 8- to 21-day span.With regard to thegrip strength circadian rhythm, 67 healthy adult malesand 24 adult women were investigated.The circadian τ ofthe dominant hand (DH) differed from 24 h and/or fromthat of the other hand in 49.2% of male subjects (33/67)and 50% of female subjects (12/24).The circadian periodof the nondominant hand (NDH) differed from 24 hand/or from that of the DH in 62.6% of male subjects(33/67) and 62.5% of female subjects (15/24). It shouldbe stressed that the activity/rest rhythm τ, which is pre-sumably controlled by the SCN, was equal to 24 h in95.6% of the subjects (87/91) involved in the studies.The finding of a circadian τ that differs among investi-gated physiological variables has been confirmed byMotohashi,67,68 in a Japanese population and byChandrawanshi and Pati,69 in an Indian population.

Thus, generalization of the laboratory rodent model tohuman beings is inadequate, and the hypothesis has tobe modified by stating that: apart from the SCN or inaddition to it, circadian rhythms of the human organismmay be driven by several clocks, which may differ fromeach other in their respective τ values.63-69
Functional circadian clocks in the human cortex
One avenue to explore to help understand multibiologicalclock systems is the difference in the τs for the circadianrhythms of the DH and NDH.The term functional is usedhere because these clocks do not necessarily have an elec-tive anatomical location, though they are undoubtedlycontrolled by brain activity. It has been suggested that eachof the brain cortex hemispheres has its own biologicalclock, and differences in the τ of grip strength rhythm maybe used to explore the presence of these different clocks.Longitudinal circadian rhythms in reaction time (RT) tolight and other signals were documented in two studies, totest the hypothesis that the prominent rhythm τ variesbetween the DH and the NDH when performing tasks ofdifferent complexity. These studies were carried in closecooperation between workers71 at Tel Aviv University anda group investigators72 at the Fondation Adolphe deRothschild in Paris. The French study72 assessed perfor-mance of easy single reaction time (SRT) tests involving aseries of 32 yellow light signals following simple and non-varying instructions; it also assessed the performance ofa complex and difficult task, a choice reaction time (CRT)test, involving a series of 96 yellow, red, or green signalsfollowing different instructions from test to test, includingwhich hand to use. The Israeli study71 explored DH andNDH RTs of men with an aviation background who wereexpert in the use of the pilot evaluation system, a flightsimulator designed as a modern cockpit with “hands onthrottle and stick” instrumentation to test performanceunder 7 scenarios of varying levels of complexity, fromeasy to very difficult.Despite differences in methods, subjects, and data gath-ering, the two studies yielded similar results. When thetask is easy (ie, SRT), the prominent period RT rhythmhas τ=24 h for both DH and NDH.When the task is com-plex and tricky (ie, CRT), the DH maintains a prominentτ=24 h in performance, while the NDH shows a promi-nent rhythm with τ ≠24 h, eg, τ=8 h, 6 h, or 12 h. Thesefindings suggest that:
• Biological clocks are present in right and left hemi-spheres of the human cortices.
• Functional differences in prominent performancerhythm are task-load–related, and the NDH side ismore sensitive than the DH.
The aim of another study73 was to assess the influence ofage and gender on the difference in τ for RT of the DHand NDH, in comparison to the grip strength rhythm.Healthy subjects of both genders were involved (9 ado-lescents [10 to 16 years old] and 15 adults [18 to 67 yearsold]).They were active between 8 AM ±1 h and 11 PM ±1 h;wrist actigraphs were used to assess the activity/restrhythm, as well as sleep logs. Data were gathered longi-tudinally at home and work four to seven times daily for11 to 20 days.In almost all cases, a 24-h sleep/wake rhythm wasdetected. For the SRT in adults, a prominent τ=24 h wasdocumented for both DH and NDH, whereas for theCRT a prominent τ=24 h was detected for DH, but τ<24h for the NDH. This phenomenon was not gender-related, but was age-related since it was seldom observedin adolescent subjects.Hand-side differences in grip strength rhythms in the sameindividuals were detected: τ was ultradian rather than cir-cadian in adolescent subjects, while τ frequently differedfrom that of the rhythm in CRT in mature subjects.These findings further support the hypothesis that func-tional biological clocks with varying periodicities exist inthe left and the right hemispheres of the human cortex.
Allochronism versus dyschronism
There is evidence of interest in human biological rhythmsand their implications for health and disease in ancientChinese cultures, since the time of the mythical emperorChennong (3000 to 4000 years ago). Sickness was relatedto an alteration of the yin-yang cycles, ie, when they arenot in harmony with those of the universe.47 In 1797,Lavoisier and Seguin74 were the first to report a rhythm of“about 24 h” in human body weight. They were soimpressed by the regularity of this cyclic phenomenon thatthey suggested an association of circadian rhythm alter-ations with states of pain and disease. However, the ques-tion of how to handle our biological rhythms to live to aripe old age and in good health remains unanswered.75
As stated in the introduction, the stable structure of tem-poral order is highly advantageous for the organism.Wehave also presented evidence63-73 that desynchonization
S t a t e o f t h e a r t
334

of a set of human circadian rhythms is rather frequent.Does this mean that a subject with an alteration of tem-poral organization is a sick (or potentially a sick) person? In the late 1970s, the answer to this question would havebeen “yes” because the prevailing assumption at thattime was that irregularity in a rhythm and/or changes inthe temporal organization corresponded to a pathologi-cal state, or at least to “... a statistically significant higher(P<0.05) chance of progression toward overt disease.”76
The values of the computed rhythm parameters wereaveraged from population studies without focusing oninterindividual variability. Dyschronism, a term coinedby Halberg et al76 was defined as a “time structure(including rhythm) alteration associated with demon-strable physical, physiological, or mental deficit, if not dis-ease.” The definition also states: “Dyschronism is notnecessarily a determinant of overt or occult disease.”To illustrate this definition, one can regard the clinicalintolerance to shift work as dyschronism, from the pointof view of medical chronobiology.77,78 Intolerance to shiftwork was defined by the following symptoms63,78,79:• Sleep alterations, like poor sleep quality, difficulty falling
asleep when retiring, frequent awakenings.• Persistent fatigue that does not disappear after sleep,
weekends, days off, and vacations.• Changes in behavior, consisting of unusual irritability,
tantrums, malaise, and feeling of inadequate perfor-mance.
• Digestive problems (which seem to be less frequentthan 20 years ago).
• The regular use of sleeping pills (barbiturates, benzodi-azepines, phenothiazines, tranquillizers, antidepressants,etc), especially when sleep cannot be controlled or evenimproved by these medications or others.
Sleep alterations, persistent fatigue, and regular use ofsleeping pills (an almost pathognomonic indicator ofintolerance to shift work) are present in any intolerantsubject. The intensity and number of symptoms varyfrom subject to subject.The occurrence of intolerance toshift work unrelated to age, duration of shift work, typeof industry, or type of rotation, including night work.Thisbattery of symptoms was used to clinically validate intol-erance to shift work in a set of prospective studies involv-ing more than 140 shift workers.63,67,68,77-79 A good toleranceamounted to 56% and poor tolerance to 46% of this pop-ulation.Dyschronism has been documented in male shift work-ers (age range: 25-58 years) in various types of industry
(oil refinery, steel industry, chemical engineering). Fourgroups were considered: 9 former nontolerant shift work-ers with diurnal work resumed for at least 18 months; 14shift workers with good tolerance; 17 shift workers withpoor and very poor tolerance (for the latter, symptomswere so severe that a clinical decision was made to trans-fer them from shift work). For at least 15 days, including1 or 2 night shifts, circadian rhythms of sleep/wake, oraltemperature, and grip strength of both hands were self-recorded 4 to 5 times per 24 h during the activity span.Prominent circadian τs were plotted in hours (Figure 3)with regard to both variables and tolerance to shiftwork.63 The τ of the sleep/wake rhythm (not shown) was24 h for 38 out of 40 subjects. For the group as a whole,only one variable, oral temperature, yielded statisticallysignificant (P<0.029) probability that desynchronizationfrom 24 h is related to intolerance to shift work.With regard to interindividual differences, it is clear thatdesynchronization is frequent and associated with symp-toms quoted above in subjects intolerant to shift work,while desynchronization can be present without clinicalcomplaint in tolerant or former shift workers. In manyhealthy subjects, one or several desynchronized circadianrhythms can be seen (eg, body temperature, grip strengthof both hands, or heart rate) without any decrease in per-formance or any symptom of shift work intolerance oraffective disorder.62,64-66,78 With the acquisition of newexperimental data, it is becoming clear that time-struc-ture variability (presumably genetically controlled) isvery common, as are environmentally induced changeswithout clinical symptoms.The general practitioner may be bewildered by the inher-ited variability, the flexibility of the system, and thechanges induced.We should therefore distinguish betweena normal variability from abnormal (pathological) changesof the temporal organization. In order to achieve this, atleast from a conceptual point of view, the idea of allochro-nism versus dyschronism was introduced.26
We assigned the term allochronism (allo = different) todesignate a variant form of alteration in the human tem-poral organization with no pathological implications.Werestrict the term dyschronism (dys = alteration, pertur-bation) to changes or alterations in the temporal organi-zation associated with a set of symptoms similar to thoseobserved in subjects intolerant to shift work.Terms like dyschronsis, dyschrony, jet lag, and jet lag syn-drome have been used to name transient subjective phe-nomena that may follow transmeridian flights,38,80,81 in
Concepts in human biological rhythms - Reinberg and Ashkenazi Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
335

which the primary consequence of these time zonechanges is fatigue.82 The major effect of a transmeridianflight (>5 time zones) is a Φ shift (phase shift) for the cir-cadian rhythm of most variables.5,6,13,25,44,78,80
The speed (or duration) of adjustment varies among thevariables for a given individual, as well among individu-als for a given variable.This phenomenon is named tran-sient desynchronization, since in most subjects thechanges in the temporal organization will disappear asthe subject becomes adjusted to the new local time.Transient desynchronization occurs in all subjects.However, some passengers—about 50% according toWinget et al80—suffer from the so-called jet lag symptomsuntil their adjustment is achieved.Using shift work and jet lag as our experimental models,we focused on the zeitgeber manipulations mainlyinvolved in allochronism and dyschronism. However,
other factors are capable of inducing allochronism witha change in the temporal organization without manip-ulation of zeitgebers. This is the case for age (eg, new-borns or the elderly), work load, complexity of task,unusual environment, odd psychological conditions suchas that of placebo effect,64 and intake of certain drugs(eg, lithium, β-blockers, or oral contraceptives).25,26,37,83
We do not yet have a practical diagnostic tool to distin-guish between allochronism and dyschronism. There isno doubt that such a tool would be extremely valuablefor assigning people to various work tasks and conditions.Dyschronism cannot be applied to all cases in whichthere is a change in the temporal order, but to individu-als who complain of persisting fatigue, sleep, and mooddisorders (and other related clinical symptoms); who takesleeping pills or other medications; in whom no directclinical cause can be documented; and in whom desyn-
S t a t e o f t h e a r t
336
Figure 3. Prominent circadian period τ resulting from power spectra analyses of longitudinal time series for 39 subjects. Prominent τs for all of the vari-ables and subjects were plotted for each of the four groups and their tolerance to shift work. Gray circles, oral temperature; blue triangles,right-hand grip strength; gray triangles, left-hand grip strength.Reproduced from reference 63: Reinberg A, Motohashi Y, Bourdeleau P, Andlauer P, Lévi F, Bicakova-Rocher A. Alteration of period and amplitude of circadian rhythmsin shift workers with special reference to temperature, right and left hand grip strength. Eur J Appl Physiol. 1988;57:15-25.Copyright © 1988, Springer-Verlag.
Prom
inen
t ci
rcad
ian
peri
od τ
(h)
Former shift workers
Shift workerswith good tolerance
Shift workers with tolerance:Poor Very poor
27
26
25
24
23
22
21

chronization of rhythms can be observed. Furthermore,the critical indicative parameter is a change in τ (changesin other rhythm parameters are secondary).
Clinical conditions that mimick those of dyschronism inshift workers
In many diseases and syndromes, patients may be chron-ically deprived of night sleep. This may be because thepatient’s condition prevents sleep, rather than because ofa sleep disorder per se.40,84 As even one or two sleep-deprived nights may deeply alter rhythms in body tem-perature, heart rate, self-rated vigilance, and mood inhealthy young subjects,85 this chronically induced sleepdeprivation mimics that which occurs in a night worker.In clinical practice, chronic deprivation of night sleep isa rather frequent condition and, as in the case of nontol-erant shift workers, it may lead to dyschronism. Usingactigraphic recordings, it is possible to evaluate sleepdeprivation related to various conditions, for example,sleep deprivation due to pain.86,87 Nocturnal exacerbationof pain is rather frequent in rheumatology and there arelarge interindividual differences.87-89 Following oral orhead/neck surgery, changes in temporal organizationwere also observed associated with restless and/or frag-mented sleep.90 Likewise, in cancer patients, Mormont etal91 showed that nocturnal sleep disruption is associatedwith statistically significant alteration in rhythms of mela-tonin, cortisol, and circulating lymphocytes.Although the conventional explanations for the observedalterations are the effects of factors like tumor type orgrowth rate, or the toxic effects of chemotherapy, thealteration of temporal order due to deprivation of nightsleep should not be excluded in this condition.Thus, dyschronism may be involved in a rather largevariety of circumstances, including chronic pain syn-drome, nocturnal asthma, persisting anxiety and stress,prostate adenoma, or fibroma with nocturnal urinaryvoiding.26
Affective disorders and dyschronism
Possible interference and interactions between psychi-atric disorders and biological rhythms have been dis-cussed widely.92-95 Special attention has been paid to affec-tive disorders, for which the occurrence of phase shifts ordrifts in some circadian rhythms (though not alwayslinked to changes in the circadian τ) have been reported.
The aim was to clarify to what extent rhythm alterationparticipates in the psychiatric problem.It has been hypothesized that depression occurs whencircadian oscillators are phase advanced relative to envi-ronmental zeitgebers.92-94 If this is correct, depression mayoccur when certain Φs are phase shifted with respect toone another, as is the case during shift work. In thisapproach, emphasis is placed upon Φ shifts or drifts inone or several variables, namely phase instability.Changes in rhythm τ and period instability have also beenconsidered. Pflug96 documented alteration in τ for bodytemperature rhythm of depressed patients. Likewise,Bicakova-Rocher et al97 recorded the body temperature ofpatients hospitalized for major affective disorders for sev-eral days and found that in half of the cases that the tem-perature τ was shorter than 24 h, while the sleep/wakerhythm τ remained at 24 h. Moreover, improvement inthese patients (treated by antidepressant or electroshocktherapy) was associated with the reoccurrence of a bodytemperature rhythm with τ=24 h.However, not all cases of affective disorders can be classi-fied as dyschronism, because, unlike the intolerance to shiftwork, which is always accompanied by changes in rhythmτ, in depression (even major affective disorder), only halfof all patients present a change in temperature τ.97
Furthermore, in shift workers, dyschronism disappears(both the symptoms and the desynchronization) when thesubject returns to regular lifestyle, and medications areineffective in the treatment of intolerance to shift work.We can thus conclude that there is a strong link betweenchanges in rhythm τ values and clinical symptoms indyschronism, whereas such a link is not present or elsevery weak in depressive states and can be evidenced inonly a fraction of cases. Consequently, depression anddyschronism presumably represent two different noso-logical entities.
Putative mechanisms involved in allochronism anddyschronism
In a discussion on depression, Kripke95,98 raised the ideathat it is the individual sensitivity to desynchronization,rather than the desynchronization itself, that tips the scalebetween the occurrence and nonoccurrence of clinicalsymptoms. This idea can be extended to interindividualdifferences in the occurrence of symptoms resulting fromintolerance to jet lag, shift work, and disease-relatedchronic deprivation of night sleep.
Concepts in human biological rhythms - Reinberg and Ashkenazi Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
337

Temporal organization variability has been known formany years. Its association with clinical and pathologicalconditions has also been documented. However, therehas been no attempt to array the temporal organizationvariants and, consequently, no experimental data areavailable with regard to the mechanisms that underliethis variability. We will offer here some hypotheses andmodels for possible putative mechanisms involved inallochronism (temporal organization variants withoutclinical symptoms) and dyschronism (temporal organi-zation variants with clinical symptoms).
Hypothesis
A rather large variety of environmental factors serve assignals that may affect the human temporal organization.Let us assume that two groups, A and B, are exposed toany of these signals. In group A, no changes in the timestructure are detected (nonreactors), while in group B,changes are detected (reactors). Group B can then dividedto two subgroups: group B1, in whom no clinical symptomsor complaints are encountered; and group B2, in whomclinical symptoms and complaints are found.According toour terminology, group B1 should be categorized as hav-ing allochronism and group B2 dyschronism.The presence of interindividual variability (with gender-related differences) and variability in the propensity ofhuman subjects to exhibit a change (even temporary, ie,reversible),48,64 suggests the involvement of genetic fac-tors. However, while the mere presence of variability canbe explained by simple models of genetic polymorphism,more complicated control mechanisms are needed toexplain why some people are more prone to change theirtemporal organization than others, even if natural zeit-gebers are present, and suggest how these changes can bereversed.
Temporal organization variability: a genetic model forallochronism
While evaluating the effects of external signals, someauthors forwarded the idea that certain zeitgebers arestrong, while others are weak.13,48 We propose that refer-ence to the strength or weakness of a zeitgeber will notrelate to the environmental signal itself, but to the sus-ceptibility of the subject to that zeitgeber. These differ-ences in the level of susceptibility should be channeledto describe differences among the internal oscillators that
govern the biological clocks. Hence, strong (stable) oscil-lators will be defined as those less prone to be affectedby changes in external signals, and weak (fragile) oscilla-tors as those which can more readily be affected by anychange in external signals.Our proposal gauges the strength of an oscillator by itscapacity to maintain τ=24 h when exposed to many chal-lenging circumstances. As an example of a strong oscil-lator, we would like to suggest the sleep/wake oscillator.This suggestion is based on the fact that, in our timeseries analyses, the τ of this rhythm seldom differed from24 h. Body temperature rhythm can serve as an exampleof a weak oscillator since documentation has revealedthat its τ frequently differs from 24 h.63,64,67,70,85,99,100
S t a t e o f t h e a r t
338
Figure 4. Periods of oral temperature rhythm: frequency distribution inCaucasian-French (CF) and Asiatic-Japanese (AJ) subjects. TheCF distribution includes the τ frequency distribution of 78 indi-viduals was extracted from data of Ashkenazi et al.16 In bothCF and AJ populations, the 0.8 h deviation unit was found toreach a higher degree of statistical significance, with P<0.02to P<0.0004 according to tests. Reproduced from reference 68: Motohashi Y, Reinberg AE, Ashkenazi IE,Bikcakova-Rocher A. Genetic aspects of circadian dyschronism: compar-ison between Asiatic-Japanese and Caucasian-French populations.Chronobiol Int. 1995;12:324-332. Copyright © 1995, Marcel Dekker.
Distribution of τs
τ (hours)
01
4
7
Nu
mb
er o
f C
F su
bje
cts
8
51
56
2
3
17.6
18.4
19.2
20.0
20.8
21.6
22.4
23.2
24.0
24.8
25.6
26.4
27.2
28.0
τ (hours)
01
4
7
Nu
mb
er o
f A
J su
bje
cts
8
30
5
6
2
3
16.0
16.8
17.6
18.4
19.2
20.0
20.8
21.6
22.4
23.2
24.0
24.8
25.6
26.4
27.2
28.0

However, within one population, there are interindividualdifferences with regard to the susceptibility levels of thesame oscillator. It seems that the strength or weakness ofoscillators does not exhibit a fixed level, but rather a rangeof levels.To find an explanation for this polymorphic phe-nomenon, we analyzed individual time series for 69 maleCaucasian-French (CF) shift workers16 and 42 male Asian-Japanese (AJ) shift workers.67,68 In 30% of both popula-tions, a change in temporal organization betweensleep/wake and oral temperature rhythms was observed.The τ of the sleep/wake rhythm seldom differed from 24h (in only 4 subjects of the AJ group and none of the CFgroup), while in 30% of both populations the τ of the tem-perature rhythm exhibited deviation from 24 h, whicharrayed as a symmetrical distribution around the 24-hvalue (Figure 4). In both groups, the interval of the devia-tions from the predominantly 24-h level clustered in mul-tiples of +0.8 h and -0.8 h (eg, 24+n[0.8 h] yielding τ=24.8h, 25.6 h, 26.4 h, 27.2 h, 28.0 h, etc; and 24-n[0.8 h], yieldingτ=23.2 h, 22.4 h, 21.6 h, 20.8 h, 20.0 h, etc; Figure 4).The analyses of these findings resulted in the dian-circa-dian model, which integrates the function of a constitutive(essential) gene that produces an exact τ=24 h (the diandomain) with a set of polygenes, the alleles of which canadd or subtract identical time entities (n[0.8 h]) to the 24-h period.16 Such an assembly of genes creates periods rang-ing from 20 to 28 h in the circadian domain. Further elab-oration of this genetic model suggests that these polygenesare usually repressed when natural zeitgebers are present.Induction of these genes will occur under conditions thatdistort or weaken the perception of the zeitgeber signals.The system will not behave like a “flip-flop” control, butthe intensity of its output will depend on the individuallyrelated strength of zeitgebers (eg, the time taken for a sus-ceptible individual to exhibit a change in temporal orga-nization in a given situation).This model allows “free run-ning” to be seen as a special case in which the entities of0.8 h (or multiplications thereof) are always induced.This model differs from conventional models based onattributing changes in τ to the effects of a single mutation.Although the possible presence of a multiple allele systemcan explain the range of deviation, it will still not be ade-quate to explain the change and restoration of the period.The polygene system with the inducible-repressible mod-
ification seems more appropriate to account for the vari-ous changes and dynamics found in rhythm periods.It is interesting to note that a year after the dian-circa-dian genetic model was presented, similar thoughts werealso presented for rhythm behavior in another species.Emery et al27 were examining a 24-h true-breeding strainof Drosophila melanogaster and reported that “period,phase, definition [the degree to which a rhythmic signalis obscured by noise], and rhythm waveform were allfound to vary continuously among the strains, althoughwithin each strain the rhythm phenotype was remarkablyconsistent.” This continuous variation contrasts with thediscrete period of the mutant phenotype reported byKonopka and Benzer.101 This is not cited to compare theresults of the two studies in humans16 and Drosophila,27
but to stress that even in Drosophila the oversimplifiedgenetic model does not fit well with the natural geneticvariability of the circadian system of this insect species.The advantages of the dian-circadian model reside in:• Providing a better understanding of observed phe-
nomena related to changes in temporal organizationand interindividual differences, as well as the effects ofjet lag and shift work.
• Consideration of the fact that the characteristics of cir-cadian rhythms cannot be reduced to the presence ofonly one phenotype, but instead relate to predictablephenotypic variability (polymorphisms).102
Conclusion
The present review did not attempt to cover all the con-cepts—established or contradictory—that prevail inchronobiology. Its aim was to present phenomena thatare mainly characteristic and unique to human chrono-biology and which cannot be fully explained by conceptsand model drawn from laboratory experiments withplants, insects, and rodents. Attention was given to non-photic signals that play a major role in affecting humanbiological rhythms, and the range of interindividual vari-ability (with an attempt to offer a genetic model). Specialemphasis was placed on distinguishing between states ofhuman health and disease that are connected to changesin temporal organization, and a conceptual classificationwas suggested for these situations. ❏
Concepts in human biological rhythms - Reinberg and Ashkenazi Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
339

S t a t e o f t h e a r t
340
Conceptos en ritmos biológicos humanos
Los ritmos biológicos y su organización temporalson fenómenos de adaptación a las variacionesperiódicas del ambiente relacionadas con la rota-ción de la tierra sobre su eje y alrededor del sol. Losdatos experimentales provenientes de los reinosvegetal y animal han dado origen a muchos mode-los y conceptos relacionados con relojes biológicosque ayudan a describir y comprender los mecanis-mos de estos cambios. Muchos de los conceptoscomunes se aplican a todos los organismos, pero lamayoría de los datos experimentales son insuficien-tes para explicar la dinámica de los relojes biológi-cos humanos. Esta revisión presenta los fenómenosque caracterizan la cronobiología humana demanera única y que no pueden ser totalmenteexplicados a través de conceptos y modelos pro-puestos a partir de experimentos de laboratorio.Ella está centrada en las ventajas funcionales de laorganización temporal humana y el problema de ladesincronización, con especial atención al período(τ) del ritmo circadiano y su variabilidad interindivi-dual e intraindividual. También se describen las dife-rencias entre los ritmos de los diestros y los zurdos,lo que sugiere la existencia de diferentes relojes bio-lógicos en las cortezas derecha e izquierda. La desin-cronización de los ritmos es un fenómeno relativa-mente frecuente (por ejemplo, el trabajo con turnosnocturnos). En algunos sujetos la desincronizaciónno se acompaña de ningún síntoma, por lo que sepropone el concepto de “alosincronía” (alo = dife-rente), para designar una variedad de la organiza-ción temporal humana que no tiene repercusionespatológicas. Se reserva el término “discronía” (dis =alteración, perturbación) para cambios o alteracio-nes asociadas con un conjunto de síntomas simila-res a los observados en sujetos que no toleran lostrabajos con turnos, como fatiga persistente y tras-tornos del ánimo y del sueño. Muchas enfermeda-des incluyen una privación crónica del sueño noc-turno y originan una sintomatología similar a la delos trabajadores con turnos nocturnos que no tole-ran la desincronización. También se presenta unmodelo genético (dian – circadiano) para explicarlas diferencias interindividuales en el período de losritmos biológicos en determinadas condiciones.
Concepts dans les rythmes biologiqueshumains
Les rythmes biologiques et leur organisation tempo-relle sont des phénomènes d’adaptation aux varia-tions périodiques de l’environnement liées aux rota-tions de la terre sur son axe et autour du soleil. Desdonnées expérimentales issues des règnes végétal etanimal ont fourni de nombreux modèles et conceptsconcernant les horloges biologiques. Ils permettentde décrire et de mieux comprendre les mécanismesde ces variations. Plusieurs des concepts majeurss’appliquent à tous les organismes mais ces donnéesexpérimentales ne suffisent pas à expliquer la dyna-mique des horloges biologiques humaines. Cetterevue présente des phénomènes qui caractérisent lachronobiologie humaine de manière unique et quine peuvent être entièrement expliqués par lesconcepts et les modèles expérimentaux. Elle est cen-trée sur l’avantage fonctionnel de l’organisationtemporelle humaine et les problèmes de désynchro-nisation, la référence critique étant la période τ desrythmes circadiens et sa variabilité intra- et interin-dividuelle. Ainsi, nous avons décrit des différencesentre les rythmes des mains droite et gauche quidonnent à penser que des horloges biologiques fonc-tionnelles différentes existent dans les cortex droit etgauche. La désynchronisation des rythmes est unphénomène relativement fréquent (par exemple : letravail posté). Chez certains sujets la désynchronisa-tion ne s’accompagne d’aucun symptôme, ce quiconduit au concept d’ « allosynchronisme » (allo =différent) qui désigne une variante de l’organisationtemporelle humaine, sans implication pathologique.Nous réservons le terme « dyschronisme » (dys = alté-ration, perturbation) aux changements ou aux alté-rations de l’organisation temporelle associés à dessymptômes s’observant chez les sujets qui ne tolèrentpas le travail posté : fatigue persistante, troubles del’humeur et du sommeil. De nombreuses maladiesinduisent une privation chronique du sommeil noc-turne et sont à l’origine d’une symptomatologie simi-laire à celle des travailleurs postés intolérants à ladésynchronisation. Nous présentons également unmodèle génétique « dien-circadien » pour expliquerles différences interindividuelles de périodes derythmes biologiques dans certaines circonstances.

Concepts in human biological rhythms - Reinberg and Ashkenazi Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
341
REFERENCES
1. Arendt J, Minors DJ, Waterhouse JM. Basic concepts and implications.In: Arendt J, Minors DJ, Waterhouse JM, eds. Biological Rhythms in ClinicalPractice. London, UK: Wright, Butterworth & Co; 1989:3-7.2. Haus E, Touitou Y. Principles of clinical chronobiology. In: Touitou Y, HausE, eds. Biological Rhythms in Clinical and Laboratory Medicine. Berlin, Germany:Springer-Verlag; 1992:6-33.3. Aschoff J. Circadian Clocks. Circadian vocabulary. Amsterdam, TheNetherlands: North-Holland Publishing Company; 1965. 4. Halberg F, Tong YL, Johnson EA. Circadian system phase. An aspect oftemporal morphology. In: von Mayersbach H, ed. The Cellular Aspect ofBiorhythms. Berlin, Germany: Springer-Verlag; 1967:20-48.5. Halberg F, Reinberg A. Rythmes circadiens et rythmes de bassesfréquences en physiologie humaine. J Physiol (Paris). 1967;59:117-200.6. Touitou Y, Haus E, eds. Biological Rhythms in Clinical and LaboratoryMedicine. Berlin, Germany: Springer-Verlag; 1992.7. Pittendrigh CS. Circadian rhythms and the circadian organization of liv-ing systems. Cold Spring Harb Symp Quant Biol. 1960;25:159-182.8. Edmunds LN Jr. Cellular and Molecular Basis of Biological Clocks. Berlin,Germany: Springer-Verlag; 1987.9. Halberg F, Visscher MG, Bittner JJ. Eosinophil rhythm in mice: range ofoccurrence; effects of illumination, feeding and adrenalectomy. Am JPhysiol. 1953;174:313-315.10. Aschoff J. Zeitgeber der tierischen Tagesperiodik. Naturwissenschaften.1954;41:49-56.11. Vanden Driessche TH. Les rythmes circadiens, mécanismes de la régu-lation cellulaire. La Recherche. 1971;2:255-261.12. Kerkhof GA. Interindividual differences in the human. In: Sweeney BM, ed.Rhythmic Phenomena in Plants. 2nd ed. San Diego Calif: Academic Press; 1987.13. Moore-Ede MC, Sulzman FM, Fuller CA. The Clocks That Time Us.Cambridge, Mass: Harvard University Press; 1992.14. Scheving L, Pauly JE. Circadian rhythms of physiological variables asreflected in rat bioassay. In: Altman R, Dittner DS, ed. Biology Data Book,Bethesda, Md: FASEB; 1973;2:1039-1047.15. Kerkhof GA. Interindividual differences in the circadian system. BiolPsychol. 1985;20:83-112.16. Ashkenazi IE, Reinberg A, Bicakova-Rocher A, Ticher A. The geneticbackground of individual variations of circadian rhythm period in healthyhuman adults. Am J Hum Genet. 1993;52:1250-1259.17. Manaker M. Special topic: circadian rhythms. Annu Rev Physiol.1993;55:657-659.18. King DP, Takahashi JS. Forward genetic approach to circadian clocks inmice. Cold Spring Harb Symp Quant Biol. 1996;61:295-302.19. Young MW, ed. Molecular Genetics of Biological Rhythms. New York, NY:Marcel Dekker; 1993.20. Dunlap JC. The genetic analysis of circadian rhythms. Annu Rev Physiol.1993;55:683-728.21. Moore RY. Organisation and function of a central nervous system cir-cadian oscillator: the suprachiasmatic hypothalamic nucleus. Fed Proc.1983;42:2783-2789.22. Moore RY, Silver R. Suprachiasmatic nucleus organization. ChronobiolInt. 1998;15:475-487.23. Pittendrigh CS. Temporal organization: reflections of a Darwinian clock-watcher. Annu Rev Physiol. 1993;55:17-54.24. Ticher A, Ashkenazi IE, Reinberg A. Preservation of the functionaladvantage of human time structure. FASEB J. 1995;9:269-272.25. Smolensky MH, Lamberg L. The Body Clock Guide to a Better Health. NewYork, NY: Henry Holt; 2000.26. Reinberg A. Chronobiologie Médicale, Chronothérapeutique. Paris, France:Flammarion Médecine-Sciences; 2003.27. Emery PTJ, Morgan E, Birly AJ. An investigation of natural genetic vari-ation in the circadian system of Drosophila melanogaster rhythm charac-teristics and methods of quantification. Chronobiol Int. 1994;11:72-84.28. Ashkenazi IE, Reinberg AE, Motohashi Y. Interindividual difference inthe flexibility of human temporal organization: pertinence to jet lag andshift work. Chronobiol Int. 1997;14:99-113.
29. Murphy PJ, Campbell SS. Physiology of the circadian system in animalsand humans. J Clin Neurophysiol. 1996;13:2-16.30. Turek F. Neurobiology of circadian rhythms in mammals. Bioscience.1983;33:439-444.31. Czeisler CA, Allan JS, Strogatz SH, et al. Bright light resets the humancircadian pacemaker independent of the timing of sleep wake cycle.Science. 1986;233:667-671.32. Danilenko KV, Wirz-Justice A, Krauchi K, Weber JM, Terman M. Thehuman circadian pacemaker can see the dawn’s early light. J Biol Rhythms.2000;15:437-446.33. Jouvet M. Les fiancailles difficiles de la chronobiologie et de l’hypnologie.Presented at the meeting of La Société Francophone de Chronobiologie.Lyon, France. May 1998.34. Randall W, Johnson RF, Randall S, Cunningham JT. Circadian rhythms infood intake and activity in domestic cats. Behav Neurosci. 1985;99:1162-1174.35. Randall W, Cunningham JT, Randall S, Luttschwager J, Johnson RF. Atwo-peak circadian system in body temperature and activity in the domes-tic cat Felis catus L. J Therm Biol. 1987;12:27-37.36. Simpson HW, Bellamy N, Bohlen J, Halberg F. Double-blind trial of apossible chronobiotic: quidon. Int J Chronobiol. 1973;1:287-311.37. Reinberg A, Smolensky MH, Labrecque G. The hunting of the wonder pillfor resetting all biological clocks. Ann Rev Chronopharmacol. 1988;4:171-200.38. Dawson D, Armstrong SM. Chronobiotics—drugs that shift rhythms.Pharmacol Ther. 1996;69:15-36.39. Lewy A, Saeeduddin A, Lathan Jackson JM, Sack RL. Melatonin shiftshuman circadian rhythms according to a phase response curve. ChronobiolInt. 1992;5:380-392.40. Benoit O, Foret J. Le Sommeil Humain. Paris, France: Masson; 1992.41. Czeisler CA, Zimmerman JC, Ronda JM, Moore-Ede MC, Weitzman ED.Timing of REM sleep is coupled to the circadian rhythm of body temper-ature in man. Sleep. 1980;2:329-346.42. Jouvet M, Buda C, Sastre JP. Hypothermia induces a quasi permanent para-doxical sleep state in pontine cats. In: Malan A, Canguilhem B, eds. Living inthe Cold II. Colloque INSERM. Paris, France: John Libbey Eurotext; 1989:487-497.43. Lemmer B, Witte K, Schänzer A, Findeisen A. Circadian rhythms in therenin-angiotensin system and adrenal steroids may contribute to theinverse blood pressure rhythm in hypertensive TGR(mREN-2)27 rats.Chronobiol Int. 2000;17:645-658.44. Reinberg AE, Smolensky MH. Biological Rhythms in Medicine. New York,NY: Springer-Verlag; 1983.45. Lewy AJ, Wehr TA, Goodwin FK, et al. Light suppress melatonin secre-tion in humans. Science. 1980;210:1267-1269.46. Czeisler CA, Wright KP. Influence of light on circadian rhythms inhumans. In: Turek FW, Zee PC, eds. Regulation of Sleep and Circadian Rhythms.New York, NY: Marcel Dekker; 1999:149-180.47. Reinberg A. Le Temps Humain et les Rythmes Biologiques. Paris, France:Éditions du Rocher; 1998.48. Wever RA. The Circadian System of Man. New York, NY: Springer-Verlag; 1979.49. Apfelbaum M, Reinberg A, Nillus P, et al. Rythmes circadiens de l'al-ternance veille-sommeil pendant l'isolement souterrain de sept jeunesfemmes. Presse Méd, 1969;77:879-882.50. Aschoff J, Fatranska M, Giedke H, et al. Human circadian rhythms in con-tinuous darkness: entrainment by social cues. Science. 1971;171:213-215.51. Eastman C, Hoese EK, Yougstedt SD, Liu L. Phase shifting human circa-dian rhythms with exercise during the night shift. Physiol Behav.1995;58:1287-1291.52. Shiota M, Sudou M, Ohshima M. Using outdoor exercise to decrease jetlag in airline crewmembers. Aviat Space Environ Med. 1996;67:1155-1160.53. Mills JN, Minors DS, Waterhouse JM. Adaptation to abrupt time shiftof the oscillator(s) controlling human circadian rhythms. J Physiol (Lond).1978;285:455-470.54. Rietveld WJ. The suprachiasmatic nucleus and other pacemakers. In:Touitou Y, Haus E, eds. Biological Rhythms in Clinical and Laboratory Medicine.Berlin, Germany: Springer-Verlag; 1992:55-64.55. Ralph MR, Foster RG, Davis FC, Manaker M. Transplanted suprachias-matic nucleus determines circadian period. Science. 1990;247:975-978.56. Hastings M. The brain circadian rhythms and clock genes. J Mol Biol.1998;317:1704-1707.

57. Abe H, Honma S, Namihira M, et al. Clock gene expression in thesuprachiasmatic nucleus and other areas of the brain during rhythm split-ting in CS mice. Mol Brain Res. 2001;87:92-99.58. Reppert SM, Perlow MJ, Underleider LG, et al. Effects of damage to thesuprachiasmatic area of the anterior hypothalamus on the daily melatoninand cortisol rhythms in the rhesus monkey. J Neurosci. 1981;1:1414-1425.59. Aschoff J, Wever RA. The circadian system of man. In: Aschoff J, ed.Handbook of Behavioral Neurobiology. Biological Rhythms. London, UK: Plenum;1981:311-331.60. Zulley J, Campbell SS. Napping behavior during “spontaneous internaldesynchronization” sleep remains in synchrony with body temperature.Human Neurobiol. 1985;4:123-126.61. Folkard S, Wever RA, Wildgruber CH. Multioscillatory control of circa-dian rhythms in human performances. Nature. 1983;305:223- 226.62. Monk T, Weitzman ED, Fookson JE, Moline ML. Circadian rhythms inhuman performance efficiency under free running conditions.Chronobiologia. 1984;11:343-354.63. Reinberg A, Motohashi Y, Bourdeleau P, Andlauer P, Lévi F, Bicakova-Rocher A. Alteration of period and amplitude of circadian rhythms in shiftworkers with special reference to temperature, right and left hand gripstrength. Eur J Appl Physiol. 1988;57:15-25.64. Reinberg A, Bicakova-Rocher A, Gorceix A, Ashkenazi IE, SmolenskyMH. Placebo effect on the circadian rhythm period t of temperature andhand-grip rhythms: interindividual and gender-related differences.Chonobiol Int. 1994;11:54-61.65. Reinberg A, Brossard T, André MF, et al. Interindividual differences ina set of biological rhythms documented during the high Arctic summer(79°N) in 3 healthy subjects. Chronobiol Int. 1984;1:127 -138.66. Reinberg A, Proux S, Bartal JP, Lévi F, Bicakova-Rocher A. Circadianrhythms in competitive saber fencers: internal desynchronization and per-formance. Chronobiol Int. 1985;2:195-201.67. Motohashi Y. Desynchronization of oral temperature and grip strengthcircadian rhythms in healthy subjects with irregular sleep–wake behav-ior. In: Hayes DK, Pauly JE, Reiter RJ, eds. Chronobiology in Clinical Medicine,General Biology and Agriculture. New York, NY: Wiley-Liss; 1990:57-63.68. Motohashi Y, Reinberg AE, Ashkenazi IE, Bikcakova-Rocher A. Geneticaspects of circadian dyschronism: comparison between Asiatic-Japaneseand Caucasian-French populations. Chronobiol Int. 1995;12:324-332.69. Chandrawanshi A, Pati AK. Could externally desynchronized circadianrhythms be resynchronized in shift workers. Biol Rhythm Res. 2000;31:160-176.70. Pati AK, Chandrawanshi A, Reinberg A. Shift work. Consequences andmanagement. Current Sci. 2001;81:32-52.71. Shub Y, Ashkenazi IE, Reinberg A. Difference between left- and right-hand reaction time rhythms: indications of shifts in strategies of humanbrain activities. Cogn Brain Res. 1997;6:141-146.72. Reinberg A, Bicakova-Rocher A, Nouguier J, et al. Circadian rhythmperiod in reaction time to light signal: difference between right- and left-hand side. Cogn Brain Res. 1997;6:135-140.73. Reinberg A, Bicakova-Rocher A, Mechkouri M, Ashkenazi I. Right- andleft-brain hemisphere. Rhythms in reaction time to light signals is task loaddependant: age, gender, and hand grip strength rhythm comparison.Chronobiol Int. 2002;19:1087-1106.74. Lavoisier A, Seguin A. Sur la transpiration des animaux. Mémoires del'Académie des Sciences Paris. 1797:601-612.75. Monk TH, Reynolds FR III, Kupfer DJ, Hoch CC, Carrier J, Houyck PR.Differences over the life span in daily life-style regularity. Chronobiol Int.1997;14:295-306.76. Halberg F, Carandente F, Cornelissen G, Katinas GS. Glossary of chrono-biology. Chronobiologia. 1977;4(suppl 1):1-189.77. Reinberg A, ed. Chronobiological field studies of oil refinery shift work-ers. Chronobiologia. 1979;6(suppl 1):1-122.78. Reinberg AE, Smolensky MH. Night and shift work and transmeridianflights. In: Touitou Y, Haus E, eds. Biological Rhythms in Clinical and LaboratoryMedicine. Berlin, Germany: Springer-Verlag; 1992:243-255.
79. Andlauer P, Reinberg A, Fourré L, Battle W, Duverneuil G. Amplitudeof the oral temperature circadian rhythm and tolerance to shift work. JPhysiol (Paris). 1979;75:507-512.80. Winget CM, Deroshia CW, Markley CL, Holley DC. A review of humanphysiological and performance changes associated with desynchronosisand biological rhythms. Aviat Space Environ Med. 1994;55:1085-1096.81. Monk T. Traffic accident increases as a possible indicant of dyschrono-sis. Chronobiologia. 1980;7:527-529.82. Reinberg A. Le rythme circadien de la fatigue. In: Serratrice G, Vildé JL,eds. Chronic Fatigue Syndrome. Paris, France: Springer-Verlag; 1991:61-82.83. Labrecque G, Sirois-Labrecque M, eds. Chronopharmacologie. Montreal,Canada: Presse de L’Université de Montréal; 2003.84. Turek FW, Zee PC, eds. Regulation of Sleep and Circadian Rhythms. NewYork, NY: Marcel Dekker; 1999.85. Benoit O, Foret J, Merle B, Reinberg A. Circadian rhythms (tempera-ture, heart rate, vigilance, mood) of short and long sleepers: effects ofsleep deprivation. Chronobiologia. 1981;8:341-350.86. Sadeh A, Hauri PJ, Kripke F, Lavie P. The role of actigraphy in the eval-uation of sleep disorders. Sleep. 1995;18:288-302.87. Labrecque G, Karzazi M, Vanier MC. Biological rhythms in pain andanalgesia. In: Redfern PH, Lemmer B, eds. Physiology and Pharmacology ofBiological Rhythms. Berlin, Germany: Springer-Verlag; 1997:619-650.88. Hermann D, Chan W, Smolensky MH Twenty-four-hour wrist actigraphyfor evaluation of nocturnal sleep of pain patients. 6th InternationalConference on Chronopharmacology. Amelia Island, Fla. 1994. Abstract XIII-2.89. Lavie P, Lorber M, Tzischinsky O, Epstein R, Sharf Y. Wrist actigraphicmeasurements in patients with rheumatoid arthritis: a novel method toassess drug efficacy. Drug Invest. 1992;(suppl 2):15-21.90. Farr LA, Todero CM, Boen LM. Advancement of circadian rhythms reducesdisruption and improves recovery from surgery. 6th International Conferenceon Chronopharmacology. Amelia Island, Fla. 1994. Abstract XV-4.91. Mormont MC, Claustrat B, Waterhouse JM, et al. Clinical relevance ofcircadian rhythm assessment in cancer patients. In: Touitou Y, ed. BiologicalClocks: Mechanisms and Applications. Amsterdam, The Netherlands: Elsevier;1998:497-505.92. Wehr TA, Goodwin FK, eds. Biological Rhythms in Psychiatry. Pacific Grove,Calif: Boxwood Press; 1983.93. Halaris A, ed. Chronobiology and Psychiatric Disorders. New York, NY:Elsevier Science; 1987.94. Taillard J, Lemoine P, Boule P, Drogue M, Mouret J. Sleep and heart ratecircadian rhythm in depression: the necessity to separate. Chronobiol Int.1993;10:63-72.95. Kripke DF. Phase-advance theory for affective illnesses. In: Wehr TA,Goodwin FK, eds. Biological Rhythms in Psychiatry. Pacific Grove, Calif:Boxwood Press; 1983:41-69.96. Pflug B. Circadian rhythms in depression. In: Rensing L, der Heiden U,Mackey MC, eds. Temporal Disorders in Human Oscillatory System. Berlin,Germany: Springer-Verlag; 1987:194-201.97. Bicakova-Rocher A, Gorceix A, Reinberg A, Ashkenazi IA, Ticher A.Temperature rhythms of patients with major affective disorders: reducedcircadian period length. Chronobiol Int. 1996;13:47-57.98. Kripke DF, Mullaney DJ, Savides TJ, Gillin JC. Phototherapy for nonseasonalmajor depressive disorders. In: Rosenthal NE, Blehar MC, eds. Seasonal AffectiveDisorders and Phototherapy. New York, NY: Gilford Press; 1989:342-356.99. Johnson A, Engelman W, Pflug B, Klemke W. Influence of lithium ionson human circadian rhythms. Z Naturforsch (C). 1980;35:503-507.100. Reinberg A, Smolensky M. Chronobiology and thermoregulation. In:Schönbaum E, Lomax P, eds. Thermoregulation Physiology and Biochemistry.New York, NY: Pergamon Press; 1990:61-100.101. Konopka RJ, Benzer R. Clock mutant of Drosophila melanogaster. ProcNatl Acad Sci U S A. 1971;58:2112-2116.102. Brok-Simoni F, Ashkenazi IE, Ramot B, Holtzman F. The diurnal rhythmof enzymes in human red blood cells: in vivo studies. Br J Haematol.1976;32:601-605.
S t a t e o f t h e a r t
342

he Earth’s rotation on its axis, the orbit of theEarth around the Sun, and the orbit of the Moon aroundthe Earth induce rhythmic geophysical phenomena.Organisms are thus affected by daily and seasonal vari-ations of many physical factors of their environment.Theability to adapt to this changing environment is an essen-tial survival mechanism. As a result, life has evolved toadapt to periodically changing environmental demands,and to anticipate them according to their predictability.Circadian and seasonal rhythms in biochemical, meta-bolic, endocrine, physiological, and behavioral processesare a fundamental feature of all living organisms, reflect-ing the need to ensure that biological functions occur ata given time of the day or year.The most obvious exam-ple is the fact that many animals are active only duringthe light period (diurnal species; human belong to thisgroup) or in the dark period (nocturnal species), and areinactive during the other part of the day (sleep/wakecycle). Other rhythms, such as reproduction, diapause,hibernation, fur color changes, and migration, can also begiven as examples. Precise timing is required at all levelsfrom behavior to gene expression, and its dysregulationcauses malfunction.Since the beginning of time, mankind has been fascinatedby the sun and the invariably changing seasons, andancient medical scripts include considerations on the vari-ation of disease through the seasons. Disorders of rhyth-micity are characteristic of—and may underlie—a variety
B a s i c r e s e a r c h
343
Melatonin in animal modelsPaul Pévet, PhD
Keywords: melatonin; animal model; seasonal function; circadian function;chronobiotic effect
Author affiliations: Laboratoire de Neurobiologie des Rythmes, UMR 7518CNRS-Université Louis Pasteur, Strasbourg, France
Address for correspondence: Laboratoire de Neurobiologie des Rythmes,UMR 7518 CNRS-Université Louis Pasteur, 12 rue de l’Université, 67000Strasbourg, France (e-mail: [email protected])
T
Melatonin is a hormone synthesized and secreted duringthe night by the pineal gland. Its production is mainly dri-ven by the circadian clock, which, in mammals, is situatedin the suprachiasmatic nucleus of the hypothalamus. Themelatonin production and release displays characteristicdaily (nocturnal) and seasonal patterns (changes in dura-tion proportional to the length of the night) of secretion.These rhythms in circulating melatonin are strong syn-chronizers for the expression of numerous physiologicalprocesses. In mammals, the role of melatonin in the con-trol of seasonality is well documented, and the sites andmechanisms of action involved are beginning to be iden-tified. The exact role of the hormone in the diurnal (cir-cadian) timing system remains to be determined.However, exogenous melatonin has been shown to affectthe circadian clock. The molecular and cellular mecha-nisms involved in this well-characterized “chronobiotic”effect have also begun to be characterized. The circadianclock itself appears to be an important site for the entrain-ment effect of melatonin and the presence of melatoninreceptors appears to be a prerequisite. A better under-standing of such “chronobiotic” effects of melatonin willallow clarification of the role of endogenous melatoninin circadian organization.© 2003, LLS SAS Dialogues Clin Neurosci. 2003;5:343-352.
Copyright © 2003 LLS SAS. All rights reserved www.dialogues-cns.org

of medical and behavioral disorders. For example, sleepand circadian rhythms are often disrupted in neurologicaldisorders and there is increasing evidence that alterationsin the sleep/wake cycle accompany many types of neuro-logical disorders. Moreover, in our modern human society,there is an increasing incidence of “circadian misalign-ment” caused by behaviors that perturb the relationshipbetween light-mediated and activity-related input to thecircadian system (eg, delayed resynchronization to localtime [jet lag] or shift work rotation associated with gen-eral malaise [especially insomnia] and decrements in workproductivity and increases in accidents).1 Additionally, inour aging society, there is a high incidence of circadian dis-orders, particularly disturbed sleep patterns, which reducethe quality of life. Moreover clinical responses to drugtherapies, including those for cancer,2 can crucially dependon the state of the patient’s circadian system.The challenge for scientists is to understand the func-tional mechanisms involved and develop strategies tocontrol or treat these disorders, which have importanteconomic and health consequences.The functional mechanism used for the daily or seasonalorganization of functions is far from well understood.Wenow know that, in mammals, these adaptive processesare organized within a circadian network comprising anendogenous self-sustained oscillator, synchronizing clockinputs, and various clock outputs. The major circadianoscillator is located in the suprachiasmatic nuclei (SCN)of the hypothalamus and the decoding of its geneticbackground is underway. Photic and nonphotic inputs actdirectly or indirectly on the rhythms of clock geneexpression to synchronize the circadian oscillations toexactly 24 h.3 The most efficient synchronizer is the dailylight/dark (LD) cycle, but other factors, such as foodrestriction, locomotor activity, and chronobiotic drugs,are well-defined clock synchronizers as well.4 The circa-dian oscillator outputs allow the internal synchronizationand temporal organization of physiological, endocrine,and behavioral functions. From the hypothalamic clock,various efferent pathways have been described, one of
the most important reaching the pineal gland. Thisendocrine structure synthesizes and releases melatonin.*Melatonin is synthesized and secreted during the darkperiod of the LD cycle, independent of whether the ani-mal is diurnally or nocturnally active, and the durationof the nocturnal production is proportional to the lengthof the night.8,9 Melatonin is thus an important efferenthormonal signal from the clock and its pattern of secre-tion provides both a daily and seasonal endocrine mes-sage to any structure or organ that can “read” it. It is nowwell established, as will be discussed below, that thesemessages are directly involved in the regulation of bothcircadian and seasonal rhythms in mammals.Before we start the description of current knowledge, itshould be mentioned that, at high doses, exogenouslyadministered melatonin has been reported to be a potentfree radical scavenger.10,11 This effect can be explainedthrough direct scavenging of free radicals or throughinteractions of enzyme that improve total antioxidativedefense capacity. Even though the physiological natureof such an effect could be questioned, it should not beneglected when assessing the therapeutic potential of thehormone,12 especially because the binding of melatoninto quinone reductase (QR2), an enzyme with well-known oxidoreductive properties, has recently beendemonstrated.13
Melatonin and seasonal function
The duration of the peak of melatonin secretion is pos-itively correlated with the length of the night period.Experimentally, it has been demonstrated that the brainis able to integrate photoperiodic information throughthese changes in duration of melatonin synthesis. Thisexplains the current use of this hormone in farming tocontrol seasonal functions (eg, fur growth, reproduction,and milk production). This also opens therapeutic per-spectives if we consider the hypothesis of Wehr14 that“the photoperiod-induced changes in the duration ofmelatonin secretion drive the annual cycle that occurs in
B a s i c r e s e a r c h
344
Selected abbreviations and acronymsDMH dorsomedial hypothalamusLD light/darkLH luteinizing hormonePT pars tuberalisSCN suprachiasmatic nucleusSP short photoperiod
*Although the pineal gland is the major source of melatonin, other sourcesdo exist. The retina is one such extrapineal source.5,6 However, and contraryto what happens in some nonmammalian vertebrates, mammalian retinalmelatonin does not contribute to circulating melatonin. The Harderian andlachrymal glands, gastrointestinal tract, red blood cells, platelets, andmononuclear cells have also been identified as sites of melatonin synthe-sis. Melatonin does not appear to be released into the general circulationfrom these tissues, at least under normal physiological conditions.7
Moreover, the synthesis of melatonin in these tissues does not appear tobe rhythmic.

Melatonin in animal models - Pévet Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
345
seasonal affective disorders.” The exact mechanism ofaction of melatonin is unclear.The duration of nocturnalmelatonin production is the key signal,8 but the existencewithin this signal of a melatonin-driven circadian rhythmof sensitivity to melatonin has been proposed to explainthe photoperiodic response.15 In fact, our understandingof melatonin’s physiological functions depends on theunderstanding of how and where its action is exerted.Considering the lipophilic nature of the hormone, inter-actions with specific intracellular proteins16,17 or nuclearreceptors cannot be excluded; however, melatonin seemsto exert its effects principally throughout high-affinity G-protein–coupled receptors. The introduction of 2-[125I]iodomelatonin (125I-Mel)18 heralded the develop-ment of the melatonin receptor field. The cloning of thefirst high-affinity melatonin receptor in 1994 by Ebisawaet al19 then led to the subsequent identification of threetypes of vertebrate melatonin receptors (MT1, MT2, andMel1c), and this very probably is only the beginning of along list. Considering the photoperiodic responses, themelatonin receptors involved most probably are of theMT1 subtype. Indeed, the gene of the only other mela-tonin receptor subtype found in mammals, MT2, is non-functional in two highly photoperiodic species, Siberianand Syrian hamsters (Weaver and Reppert, unpublisheddata cited in reference 20). The target sites mediatingmelatonin control of photoperiod-dependent seasonalfunctions and especially the annual sexual cycle have notyet been totally determined. Contrary to what is gener-ally claimed, melatonin receptors are present in a largenumber of structures in mammals (more than 110 brainstructures have been identified, among them the internalgranular layer and the external plexiform layer of theolfactory bulb, lateral septum, septohippocampal nucleus,caudate putamen, bed nucleus of the stria terminalis,SCN, mediobasal hypothalamic nuclei, paraventricularnuclei of the hypothalamus, paraventricular nuclei of thethalamus, intergeniculate leaflet, central and medialamygdaloid nucleus, inferior colliculus, fasciculusretroflexus, substantia nigra, and frontal, orbitofrontaland parietal cortex; numerous peripheral organs alsocontain melatonin receptors21-25). However, a great vari-ability has been noted in the number and location ofstructures among the species, as well as large differencesin receptor density between structures and in the samestructures between species. Few structures are common,even among species from the same family,21 and veryprobably this should be correlated to either the numer-
ous photoperiodic responses, which are different fromone species to another, or the many different effectsdescribed for melatonin.One structure, however, the pars tuberalis (PT) of thepituitary, which contains a very high density of melatoninreceptors in all mammals studied, is thought to be of pri-mary importance in photoperiodic response. Its densityof melatonin receptors exhibits clear seasonal changes inphotoperiodic species, but not in nonphotoperiodic mam-mals,26,27 and its implication in the control of seasonalsecretion of prolactin has been demonstrated.28-31 The PTis thus a good model to delineate the melatonin’s signaltransduction pathways32,33 and to study how the cellularresponse can distinguish between long- and short-dura-tion melatonin signals.The cyclic adenosine monophosphate (cAMP)-mediatedpathways appear to be central to the melatonin readout.Pretreatment with melatonin has been demonstrated toinduce a sensitization of adenylate cyclase, and a poten-tiated cAMP response to forskolin stimulation.34,35
Melatonin pretreatment that is effective in potentiatingcAMP accumulation in the PT is duration-dependent(between 0-16 h) and corresponds well with the durationof the nocturnal melatonin signal.34 The nocturnal mela-tonin signal is also crucial for the rhythmic expression inthe PT of several cAMP-responsive genes, including thetranscriptional inhibitor–inducible cAMP early repres-sor (ICER), and of several clock genes.36,37 Indeed, twocomponents of the molecular clock, namely Per1 andCry1, are rhythmically expressed in the PT. Furthermore,other components of the clock like Timeless, Clock, andPer2 (Pévet P et al, unpublished observations) are alsoexpressed in the PT, at least in the PT of some rodents,raising the possibility that the PT might contain a com-plete set of clock genes.33,36,38-41 However, the clock geneexpression in the PT differs from what is observed in theSCN or other peripheral tissues (peripheral oscillators)because it appears to be directly driven by melatonin.Removal of the pineal gland abolishes rhythmic PT geneexpression, and extension of the dark phase of the LDcycle dampens the amplitude of the Per1 in PT cells.39
Cry1 is rapidly and very strongly induced by melatoninadministration. In nontreated animals, a peak of expres-sion occurs during the dark phase (ie, at a time whenmelatonin is present in the bloodstream). This indicatesthat melatonin may gate the expression of Cry1 in thePT, suggesting that these clock genes are involved in themelatonin readout mechanism. Cry1 expression appears

to be anchored to the onset of melatonin secretion. It actsas a sensor of melatonin onset, rather than a marker ofthe duration of the melatonin signal.Per1 mRNA peaks early in the day, when blood plasmamelatonin levels are back to low levels. Per1 expressionthus appears to be linked to the offset of melatonin secre-tion. This dual effect of melatonin together with its pho-toperiod-dependent pattern in plasma levels may providethe basis of a time measurement mechanism.This modelmay help understand how the PT is involved in the sea-sonal control of prolactin secretion by the PT. The vali-dation of such a model will, however, require furtherexperiments and the complete understanding of themelatonin and photoperiodic readout requires a link withidentified downstream response in the PT.This is still dif-ficult. It is through the production of a prolactin-releas-ing (or release inhibitor) factor that the photoperiodicand melatonin information to lactotroph cells in the pitu-itary are relayed. This factor, termed “tuberalin,”30,42 hasnot yet been identified.Photoperiod-induced changes in prolactin secretion,however, are not enough to explain the seasonal sexualcycle.This implies that in order to mediate photoperiodicinformation melatonin must act on other target sites.Thisview is supported by the fact that Syrian hamsters bear-ing lesions to the dorsomedial hypothalamus (DMH) andinfused with melatonin to mimic short photoperiod (SP),display differential responses in terms of prolactin andluteinizing hormone (LH).43 While the prolactin responseremains intact, the LH response in blocked by the DMHlesion.43 Moreover, in sheep, melatonin implants in themediobasal hypothalamus block the effects of SP on LHbut not on prolactin, while implants close to the PTinhibit prolactin secretion.44 Interestingly, melatonin bind-ing sites have been detected in the DMH in the Syrianhamster, although with a very low density, and their den-sity depends on the photoperiod (Pévet P et al, unpub-lished data).The hypothesis of a parallel and concomitant action ofmelatonin on different structures to transduce the pho-toperiodic message is attractive. The photoperiod isknown, through changes in duration of melatonin secre-tion, to control not only the reproductive annual cycle, butalso a large number of other seasonal functions (eg, bodyweight, hibernation, daily torpor, fur color changes, andmigration). Furthermore, not all seasonal functions areexpressed in every species and different control mecha-nisms may be involved. For example, SP induces an acti-
vation of the sexual axis in sheep, but inhibition in Syrianand Siberian hamsters; and hibernation in the Syrianhamster is directly dependent on photoperiod, while inthe European hamster it is dependent on a “circannualclock” entrained by photoperiod. It thus seems likely thatmelatonin acts at different structures according to thespecies and the function.This concept would account forthe large interspecies differences observed in mammalsin the distribution of structures containing melatoninreceptors. Interestingly, and in support of this concept, apharmacological dissociation of photoperiodic-controlledseasonal functions has been reported. S 22153, a mela-tonin antagonist of MT1 and MT2 melatonin receptorsubtypes, caused a decrease in the duration of hibernationin Syrian hamsters under SP and low temperature, but didnot affect SP-induced gonadal atrophy.45
Melatonin and circadian function
In most nonmammalian vertebrates, the rhythmic syn-thesis and secretion of melatonin is the direct output ofcircadian clock, and the rhythmic changes in the concen-tration of circulating melatonin are fundamental to cir-cadian rhythmicity.46 In mammals, despite the presenceof melatonin receptors in the SCN of most species indi-cating hormonal feedback on the clock, the consensushas been that melatonin has only a limited role in circa-dian organization. This view has arisen, in part, sincepinealectomy has little effect on circadian organization.47
Melatonin rhythm, however, is only one of the outputs ofthe clock and it is probable that, for the organization ofcircadian activities, a number of different output signalsfrom the clock are involved in the distribution of circa-dian information to target tissues.48,49 This does not pre-clude an important role for melatonin in circadian orga-nization.36 After pinealectomy, for example, subtledesynchrony of several physiological functions has beendescribed,50 and the reentrainment of the rat locomotoractivity rhythm is modified after a phase shift of the LDcycle.51 One week after pinealectomy, the firing raterhythm of SCN neurons in vitro is altered, as well as thedaily rhythm of responsiveness to melatonin.52 It is alsoknown that melatonin interferes with metabolic activity(glucose utilization and protein synthesis) in the SCN.53
The SCN may use the daily melatonin signal to conveythe circadian message to any system that can “read” it, ie,to any structure or organ possessing melatonin receptors,either in the central nervous system or at the periphery.9,54
B a s i c r e s e a r c h
346

This concept helps explain numerous results in the liter-ature: the melatonin inhibition of spontaneous and lightevoked activity of cells in the intergeniculate leaflet55;melatonin-enhancing splenic lymphocyte proliferation56,57;melatonin-induced inhibition of leukocyte rolling andadhesion to rat microcirculation58; melatonin-inducedvasoconstriction of cerebral and tail arteries59; and mela-tonin regulation of emotional behavior.60
What could be the mechanism involved? Clock genes areexpressed widely in mammalian tissues. It appears thatcyclical expression of these genes in the periphery is dri-ven by the SCN. The role of melatonin in regulatingrhythmic clock gene expression in peripheral tissues asdescribed in the PT (see above) may be one of the mech-anisms for tissue-specific regulation of the phase ofrhythmicity. Interestingly, it has been demonstrated thatthe circadian rhythm of melatonin receptor density in ratPT is suppressed after pinealectomy and melatonin drives this rhythm directly.61,62 Even if the role of endoge-nous melatonin on clock functioning is not yet defined,the presence of melatonin receptors within the SCN indi-cates that exogenous melatonin affects circadian regula-tion, which is of potential therapeutic value.
Exogenous melatonin and circadian rhythms
Exogenous melatonin is known to be able to influence,directly or indirectly, the phase and/or the period of thecircadian clock. In terms of treatments, this means thatexogenous melatonin (or any agonist) can be used as apharmacological tool to manipulate sleep-wake cycleand other circadian rhythms (chronobiotic properties63).It has long been known that administration of melatonincan entrain free-running activity rhythms in rodents.20,64
Entrainment means that the period of the observedrhythm must adjust to, and equal, the synchronizer (zeit-geber) cycle (T), and a stable phase relation must beestablished between the rhythm and the zeitgeber cycle.This synchronization process occurs through daily phaseshifts. Administering melatonin for a series of T values,24 h, 23 h 50 min, 23 h 45 min, 23 h 35 min, and 23 h 25min65 has led to the definition of the limiting phaseadvance value to which the rat activity rhythm entrainsto melatonin at 35 min. The entrainment limits found inthis study correspond quite well to the maximum dailyphase shift values defined by the melatonin phaseresponse curve,66 and the magnitude of phase shiftresponses to a single melatonin injection67 (range 15-52
min). Daily acute melatonin administration in the ratthus causes “true” entrainment as defined by Enright et al.68
Interestingly, when melatonin is administered by dailyinfusion, the phase angle difference between theentrained rhythm and the zeitgeber (melatonin) dependsupon the duration of the infusion period. A negativephase angle is observed and its value increases with theduration of the infusion period.69 Moreover, with longinfusion times (8 h and, more especially, with 16 h), mela-tonin induces a change in the free-running period in thefirst days, suggesting that melatonin delays the pace-maker each day until entrainment occurs. In other words,with a long duration of infusion, entrainment occurs ear-lier than predicted by the model based on acute mela-tonin administration. The magnitude of the change inperiod increases significantly with the duration of infu-sion. These observations suggest that, beside its chrono-biotic properties, melatonin affects the circadian clockproperties (effect on the period τ?). This conclusion issupported by the results obtained after a “skeleton” infu-sion. Under these conditions, melatonin induced entrain-ment after a time during which circadian periods wereeither lengthened (in a fraction of the animals) or short-ened (in the others).69 This finding suggests that, toachieve entrainment, melatonin has to induce either aphase delay (when the period is shortened) or a phaseadvance (when the period is lengthened). Such a dualeffect of melatonin has also been reported in other stud-ies. For example, when rats received a 5 h phase advanceof the dark onset in LD conditions, those injected mela-tonin daily at the new dark onset reentrained withdecreased latency; some of the animals did so by phasedelays, whereas others did so by phase advances.66
Melatonin has been reported to entrain hamsters andArvicanthis ansorgei, a diurnal rodent, by inducing phaseadvances when the free-running period is longer than 24 hand phase delays when the period is shorter than 24 h.70-72
All these observations strongly suggest that the effects ofexogenous melatonin are complex and depend on theperiod before entrainment.Another potential effect of exogenous melatonin shouldbe considered. A single application of melatonin withinthe SCN, in vivo, induced a long-lasting increase in theamplitude of the nocturnal melatonin secretion.73 Thiseffect demonstrates that exogenous melatonin is able tosustain the oscillation of the clock and suggests a possi-ble role for endogenous melatonin in mammals.
Melatonin in animal models - Pévet Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
347

Sites of action for the effects of exogenous melatonin onthe circadian activities
In the experiments reported above, responsiveness tomelatonin is restricted to a narrow window of sensitivity,which is generally late in the subjective afternoon, butdepends upon the duration of the melatonin signal aswell as the previous free-running period.The finding thatpinealectomized rats entrain to daily melatonin admin-istration67,69 indicates that endogenous melatonin is notnecessary for the entrainment effect of exogenous mela-tonin, for example, by entraining a window of sensitiv-ity to melatonin.15 Nocturnal melatonin production is adirect output of the SCN circadian clock. Exogenousmelatonin is effective at a time when endogenous mela-tonin is not produced. Consequently, the effects of mela-tonin administration in vivo appear not to be related tothe role of endogenous melatonin on circadian function.This conclusion is reinforced by the observation that toobtain entrainment of the circadian activity rhythm ofrodents kept under constant darkness (DD), high dosesof melatonin have to be used, independently of the modeof administration.69,74,75 These doses of melatonin producepeak serum levels 100- to 1000-fold higher than theendogenous melatonin nighttime levels.The necessity ofsuch a high dose of melatonin is unlikely to be a conse-quence of its rapid metabolism. Appropriate photoperi-odic response is indeed obtained when melatonin isadministered via a similar subcutaneous infusion systemwith a dose that mimics the endogenous secretion pro-file.15,76 Most likely, this high dose of melatonin is neededbecause it is an integral part of the response observed.In vitro administration of melatonin can phase shift thefiring rate of SCN neuron brain slices (rat and mouse).77,78
It is principally for this reason that it is generally believedthat melatonin mediates these effects through the high-affinity melatonin receptors located within the SCN.61,79
The high correlation between the density of melatoninreceptors within the SCN and the ability of daily mela-tonin administration to entrain the free-running activityrhythm in mammals supports this view. In contrast to therat, mouse, and Djungarian hamster (rodents that can beentrained by daily melatonin administration and in whicha high density of melatonin receptors is observed withinthe SCN), the mink (Mustela vison) does not appear tohave specific melatonin receptors (at least 2-iodomela-tonin binding sites) within the SCN.This animal does notentrain to melatonin.80 Newborn Syrian hamsters express
melatonin receptors in the SCN, but the receptor num-ber decreases shortly after birth.81,82 Young hamsters areentrainable by daily acute melatonin administration,while, in the adult, melatonin is unable to entrain83,84 orsynchronize, except under particular experimental con-ditions (eg, long-term infusions which affect the τ).70,72
Since SCN-lesioned hamsters whose rhythmicity hadbeen restored with fetal hypothalamic graft are entrainedby daily melatonin injection, it is evident that the chrono-biotic effect of exogenous melatonin is the consequenceof an action on the clock.This conclusion is supported bythe observation that in vivo a melatonin receptor antag-onist (S 22153) blocks the phase-advancing effect ofmelatonin.85
Which receptor subtypes are involved? Siberian hamsterswithout a functional MT2 receptor show circadianresponses to melatonin.86 Similarly, the most robustentraining response to melatonin, synchronization ofdeveloping circadian pacemakers in Syrian hamsters bymelatonin injections, occurs in the absence of a functionalMT2 receptor within the SCN.87 This strongly suggests theimplication of MT1 receptors. In in vitro experiments inanimal models that possess both subtypes, the mecha-nisms involved appear to be more complex. An acuteinhibitory effect on neuronal firing and a phase-shiftingeffect in the rhythm in electrical activity have beendescribed.88 In mice with a targeted deletion of the MT1receptor, the acute inhibitory effect of melatonin was abol-ished, while the phase-shifting effect remained intact.88
However, this phase shift disappears when the MT2 antagonist 4-phenylpropionamidotetraline (4P-PDOT) isadded.89 This suggests that either a low density of MT2receptors is still capable of producing a phase shift or thatan as yet unidentified melatonin receptor subtype isinvolved. In contrast to previous studies, van den Top etal90 have recently demonstrated the absence of a specificwindow of sensitivity for melatonin to inhibit SCN neu-ronal activity. This lack of a window of sensitivity con-trasts with the phase-shifting effect of melatonin, andindicates that the cellular mechanisms involved in theacute inhibitory effect and in the phase-shifting effect ofmelatonin are distinct. This may be related to the twotypes of effects observed in vivo after daily 8 or 16 hmelatonin perfusions69 described above.The presence of MT1 and/or MT2 melatonin receptorsappears to be a necessary condition for the chronobioticeffect of melatonin. However, if these high-affinity mela-tonin receptors were the only mechanism involved, it
B a s i c r e s e a r c h
348

Melatonin in animal models - Pévet Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
349
would be difficult to explain why a pharmacological doseof melatonin is needed. This implies that other neuralmechanisms may be involved.Although a strong modula-tory role of exogenous melatonin on serotonin (5-hydroxy-tryptamine) 5-HT receptor–mediated responses has beenreported, the 5-HT system does not appear to be crucialto the effects of melatonin on circadian rhythms.91
Conclusions and perspectives
Melatonin is produced nocturnally by the pineal gland,in a pattern that reflects the phase and duration of thenight. The physiological roles of the hormone directlyrelate to the temporal information it conveys. In fact,nocturnal melatonin secretion is a hormonal output sig-nal of the circadian clock able to convey photoperiodicas well as circadian signals to multiple structures andorgans possessing melatonin receptors, within the brainor at the periphery.This explains why melatonin appearsto act in so many different systems.The use of melatonin to control seasonally expressedtraits of economic importance (milk and wood produc-
tion, etc) in farm animals is now well documented, and thesites and mechanisms of action involved are beginning tobe identified.The exact role of the hormone in the circa-dian timing system remains to be determined. However,due to the presence of melatonin receptors within theSCN itself, exogenous melatonin has been shown to affectthe circadian clock in animal models (chronobiotic effect).The observations that, in humans, melatonin improvessome circadian-based disorders refer to such propertiesand will lead to strategies to treat, prevent, or delay suchdisturbances. Melatonin, as explained above, acts throughseveral mechanisms. The hormone’s physiological func-tions—and thereby its therapeutic potential—will dependon our knowledge of its mechanism of action. Today, thepathways through which temporal information encodedin the melatonin signal is decoded in target tissues, andthe phenotypic nature of those target tissues, are not com-pletely understood. Experimental work in animal modelsis still needed to define exactly the therapeutic value ofthe hormone (for more perspectives with the use of phar-macological tools based on melatonin receptors and α-antagonists see reviews in references 63 and 92). ❏
REFERENCES
1. Rajaratnam SM, Arendt J. Health in a 24-h society. Lancet. 2001;358:999-1005.2. Fu L, Lee CC. The circadian clock: pacemaker and tumour suppressor. NatRev Cancer. 2003;3:350-361. 3. Challet E, Caldelas I, Graff C, Pévet P. Synchronization of the molecularclockwork by light- and food-related cues in mammals. Biol Chem.2003;384:711-719. 4. Challet E, Pévet P. Interactions between photic and nonphotic stimuli tosynchronize the master circadian clock in mammals. Front Biosci.2003;8:s246-s257. 5. Pévet P, Balemans MGM, Bary FAM, Noodergraef EM. The pineal of themole (Talpa europeae L.). V. Activity of hydroxyindole-O-methyltryptopholin the eyes and the pineal gland. Ann Biol Amin Biochem Biophys.1978;18:259-264.6. Tosini G, Menaker M. Circadian rhythms in cultured mammalian retina.Science. 1996;272:419-421.7. Djeridane Y, Pitrosky B, Vivien-Roels B, Pévet P. Long-term melatonininfusion induces large and stable increase in N-acetyltransferase activity,hydroxyindole-O-methyltransferase activity and melatonin content in theHarderian gland and eye of pinealectomized male Siberian hamster(Phodopus sungorus). J Pineal Res. 2000;29:65-73. 8. Bartness T, Bittman EL, Hastings MH, Powers JB, Goldman B. Timed mela-tonin infusion paradigm for melatonin delivery: what has it taught usabout the melatonin signal, its reception, and the photoperiodic controlof seasonal responses? J Pineal Res. 1993;15:161-190.9. Pévet P. Mélatonine et rythmes biologiques. Thérapie. 1998;53:411-420.10. Reiter RJ, Tan DX, Osuna C, Gitto E. Actions of melatonin in the reduc-tion of oxidative stress. A review. J Biomed Sci. 2000;7:444-458.11. Reiter RJ. Melatonin: clinical relevance. Best Pract Res Clin EndocrinolMetab. 2003;17:273-285.
12. Husson I, Mesples B, Bac P, Vamecq J, Evrard P, Gressens P.Melatoninergic neuroprotection of the murine periventricular white mat-ter against neonatal excitotoxic challenge. Ann Neurol. 2002;51:82-92.13. Nosjean O, Ferro M, Coge F, et al. Identification of the melatonin-bind-ing site MT3 as the quinone reductase 2. J Biol Chem. 2000;275:31311-31317.14. Wehr TA. Photoperiodism in humans and other primates: evidence andimplications. J Biol Rhythms. 2001;16:348-364.15. Pitrosky B, Kirsch R, Vivien-Roels B, Georg-Bentz I, Canguilhem B, PévetP. The photoperiodic response in Syrian hamster depends upon a mela-tonin-driven circadian rhythm of sensitivity to melatonin. J Neuroendocrinol.1995;7:889-895.16. Cardinali DP. Molecular biology of melatonin: assessment of the “micro-tubule hypothesis of melatonin action.” In: Birau N, Schloot W, eds. MelatoninCurrent Status and Perspectives. Oxford, UK: Pergamon; 1980:247-256. 17. Benitez-King G, Rios A, Martinez A, Anton-Tay F. In vitro inhibition ofCa2+/calmodulin-dependent kinase II activity by melatonin. Biochim BiophysActa. 1996;1290:191-196. 18. Vakkuri O, Lamsa E, Rahkamaa E, Ruotsalainen H, Leppaluoto J. Iodinatedmelatonin: preparation and characterization of the molecular structure bymass and 1H NMR spectrometry. Anal Biochem. 1984;142:284-289.19. Ebisawa T, Karne S, Lerner MR, Reppert SM. Expression cloning of ahigh affinity melatonin receptor from Xenopus dermal melanophores. ProcNatl Acad Sci U S A. 1994;91:6133-6137.20. Weaver DR. Melatonin and circadian rhythmicity in vertebrates: phys-iological roles and pharmacological effects. In: Turek FW, Zee PC, eds.Regulation of Sleep and Circadian Rhythms. New York, NY: Marcel Dekker;1999:197-262.21. Masson-Pévet M, George D, Kalsbeek A, Saboureau M, Lakhdar-GhazalN, Pévet P. An attempt to correlate brain areas containing melatonin-binding sites with rhythmic functions: a study in five hibernator species.Cell Tissue Res. 1994;278:97-106.

B a s i c r e s e a r c h
350
22. Stankov B, Capsoni S, Lucini V. Autoradiographic localization of puta-tive melatonin receptor in the brain of two old world primates,Cercopithecus aethiops and Papio ursinus. Neuroscience. 1993;52:459-468.23. Stankov B, Cozzi B, Lucini V, Fumagalli P, Scaglione F, Fraschini F.Characterization and mapping of melatonin receptors in the brain of threemammalian species: rabbit, horse and sheep. A comparative in vitro bind-ing study. Neuroendocrinology. 1991;53:214-221.24. Morgan PJ, Barrett P, Howell HE, Helliwell R. Melatonin receptors: local-ization, molecular pharmacology and physiological significance. NeurochemInt. 1994;24:101-146. 25. Poirel VJ, Cailotto C, Streicher D, Pévet P, Masson-Pévet M, Gauer F. MT1melatonin receptor mRNA tissular-localization by PCR amplification.Neuroendocrinol Lett. 2003;24:33-38. 26. Gauer F, Masson-Pévet M, Pévet P. Seasonal regulation of melatoninreceptors in rodents pars tuberalis: correlation to reproductive state. JNeural Transm. 1994;96:187-195. 27. Masson-Pévet M, Gauer F. Seasonality and melatonin receptors in thepars tuberalis in some long day breeder. In: Brown GM, Pévet P, Pang SF,eds. Melatonin Binding Sites in Endocrine and Immune system. Biological Signals.Basel, Switzerland: Karger; 1994;3:63-70.28. Lincoln GA, Clarke IJ. Photoperiodically induced cycles in secretion ofprolactin in hypothalamo-pituitary disconnected ram: evidence for trans-lation of the melatonin signal in the pituitary gland. J Neuroendocrinol.1994;6:251-260.
29. Graham ES, Webster CA, Hazlerigg DG, Morgan PJ. Evidence for thebiosynthesis of a prolactin-releasing factor from the ovine pars tuberalis,which is distinct from thyrotropin-releasing hormone. J Neuroendocrinol.2002;14:945-954. 30. Morgan PJ. The pars tuberalis: the missing link in the photoperiodicregulation of prolactin secretion? J Neuroendocrinol. 2000;12:287-295. 31. Hazlerigg DG, Morgan PJ, Messager S. Decoding photoperiodic timeand melatonin in mammals: what can we learn from the pars tuberalis? JBiol Rhythms. 2001;16:326-335.32. Von Gall C, Stehle JH, Weaver DR. Mammalian melatonin receptors:molecular biology and signal transduction. Cell Tissue Res. 2002;309:151-162.33. Von Gall C. Rhythmic clock gene expression in the hypophyseal parstuberalis is regulated by melatonin. Ann Anat. 2003;185:301-302.34. Hazlerigg DG, Gonzalez-Brito A, Lawson W, Hastings MH, Morgan PJ.Prolonged exposure to melatonin leads to time-dependent sensitizationof adenylate cyclase and down-regulates melatonin receptors in parstuberalis cells from ovine pituitary. Endocrinology. 1993;132:285-292. 35. Hazlerigg DG, Hastings MH, Morgan PJ. The recovery of ovine parstuberalis cells from melatonin-induced sensitization is a slow, protein syn-thesis-dependent phenomenon. J Endocrinol. 1994;142:127-138.36. Von Gall C, Garabette ML, Kell CA, et al. Rhythmic gene expression inpituitary depends on heterologous sensitization by the neurohormonemelatonin. Nat Neurosci. 2002;5:234-238.
Melatonina en modelos animales
La melatonina es una hormona que es sintetizada ysecretada durante la noche por la glándula pineal.Su producción es controlada principalmente por elreloj circadiano, el cual en los mamíferos está situadoen el núcleo supraquiasmático del hipotálamo. Laproducción y liberación de melatonina tiene perfilesde secreción característicos tanto diarios (nocturnos)como estacionales (cambios en la duración propor-cionales a la duración de la noche). Estos ritmos enla melatonina circulante son fuertes sincronizadorespara la expresión de numerosos procesos fisiológicos.En los mamíferos, el papel de la melatonina en elcontrol de la estacionalidad está bien documentado,y los sitios y mecanismos de acción involucrados seestán comenzando a identificar. El papel exacto dela hormona en el sistema de ritmo diurno (circa-diano) debe ser determinado. Sin embargo, se haobservado que la melatonina exógena afecta el relojcircadiano. Los mecanismos moleculares y celularesque participan en este efecto “cronobiótico” biencaracterizado también han comenzado a ser identi-ficados. El reloj circadiano en sí mismo parece ser unsitio importante para el efecto de arrastre de mela-tonina y la presencia de receptores de melatoninaparece ser un prerrequisito. Una mejor comprensiónde tales efectos “cronobióticos” de la melatoninapermitirá aclarar el papel de la melatonina endó-gena en la organización circadiana.
Mélatonine et modèles animaux
La mélatonine est une hormone synthétisée etsécrétée par la glande pinéale. Cette synthèse estsous le contrôle de l’horloge circadienne localiséechez les mammifères dans les noyaux suprachias-matiques de l’hypothalamus. La sécrétion de méla-tonine est nocturne (caractère journalier) et ladurée de cette sécrétion est proportionnelle à ladurée de la nuit (caractère saisonnier). Ces varia-tions rythmiques de la sécrétion de mélatonine per-mettent de distribuer à l’organisme un messagejournalier et saisonnier. Chez les mammifères, lerôle de la mélatonine dans le contrôle des fonctionssaisonnières est maintenant bien démontré et lessites et mécanismes d’action commencent à êtrebien identifiés. Le rôle exact de la mélatonine dansl’organisation journalière des fonctions reste àdéterminer. Toutefois des administrations de méla-tonine exogène sont connues pour agir sur le sys-tème circadien. Les mécanismes moléculaire et cel-lulaire impliqués dans cet effet « chronobiotique »de l’hormone commencent à être identifiés.L’horloge circadienne elle-même semble être lacible principale et la présence de récepteurs à lamélatonine est nécessaire. Déterminer ces méca-nismes d’action permettra de clarifier le rôle de lamélatonine endogène dans l’organisation circa-dienne des fonctions.

37. Korf HW, Von Gall C, Stehle J. The circadian system and melatonin:lessons from rats and mice. Chronobiol Int. 2003;20:697-710. 38. Messager S, Hazlerigg DG, Mercer JG, Morgan PJ. Photoperiod differ-entially regulates the expression of Per1 and ICER in the pars tuberalis andthe suprachiasmatic nucleus of the Siberian hamster. Eur J Neurosci.2000;12:2865-2870.39. Messager S, Garabette ML, Hastings MH, Hazlerigg DG. Tissue-specificabolition of Per1 expression in the pars tuberalis by pinealectomy in theSyrian hamster. Neuroreport. 2001;12:1-4. 40. Lincoln GA, Andersson H, Hazlerigg D. Clock genes and the long-termregulation of prolactin secretion: evidence for a photoperiod/circannualtimer in the pars tuberalis. J Neuroendocrinol. 2003;15:390-397. 41. Dardente H, Menet JS, Poirel VJ, et al. Melatonin induces Cry1 expressionin the pars tuberalis of the rat. Brain Res Mol Brain Res. 2003;114:101-106. 42. Hazlerigg DG, Hastings MH, Morgan PJ. Production of a prolactin-releas-ing factor by the ovine pars tuberalis. J Neurendocrinol. 1996;8:489-492.43. Maywood ES, Bittman EL, Hastings MH. Lesions of the melatonin- andandrogen-responsive tissue of the dorsomedial nucleus of the hypothala-mus block the gonadal response of male Syrian hamsters to programmedinfusions of melatonin. Biol Reprod. 1996;54:470-477. 44. Malpaux B, Migaud M, Tricoire H, Chemineau P. Biology of mammalianphotoperiodism and the critical role of the pineal gland and melatonin. JBiol Rhythms. 2001;16:336-347. 45. Pitrosky B, Delagrange P, Rettori MC, Pévet P. S 22153, a melatoninantagonist, dissociates different aspects of photoperiodic responses inSyrian hamsters. Behav Brain Res. 2002;138:145-152.46. Cassone VM. Melatonin’s role in vertebrate circadian rhythms.Chronobiol Int. 1998;15:457-473. 47. Underwood H, Goldman BD. Vertebrate circadian and photoperiodicsystems: role of the pineal gland and melatonin. J Biol Rhythms. 1987;2:279-315.48. Buijs RM, Kalsbeek A. Hypothalamic integration of central and periph-eral clocks. Nat Rev Neurosci. 2001;2:521-526. 49. Kramer A, Yang FC, Snodgrass P, et al. Regulation of daily locomotoractivity and sleep by hypothalamic EGF receptor signaling. Science.2001;294:2511-2515. 50. Lima FB, Machado UF, Bartol I, et al. Pinealectomy causes glucose intol-erance and decreases adipose cell responsiveness to insulin in rats. Am JPhysiol. 1998;275:E934-E941. 51. Armstrong SM. Melatonin: the interval Zeitgeber of mammals. In:Reiter RJ, ed. Pineal Research Review. Vol 7. New York, NY: Liss; 1989:157-202. 52. Rusak B, Yu GD. Regulation of melatonin-sensitivity and firing-raterhythms of hamster suprachiasmatic nucleus neurons: pinealectomy effects.Brain Res. 1993;602:200-204.53. Cassone VM, Roberts MH, Moore RY. Effects of melatonin on 2-deoxy-[1-14C]glucose uptake within rat suprachiasmatic nucleus. Am J Physiol.1988;255:R332-R337. 54. Cardinali DP, Pévet P. Basic aspects of melatonin action. Sleep Med Rev.1998;2:175-190. 55. Ying SW, Zhang DX, Rusak B. Effects of serotonin agonists and mela-tonin on photic responses of hamster intergeniculate leaflet neurons. BrainRes. 1993;628:8-16.56. Drazen DL, Bilu D, Bilbo SD, Nelson RJ. Melatonin enhancement ofsplenocyte proliferation is attenuated by luzindole, a melatonin receptorantagonist. Am J Physiol Regul Integr Comp Physiol. 2001;280:R1476-R1482. 57. Drazen DL, Nelson RJ. Melatonin receptor subtype MT2 (Mel 1b) andnot mt1 (Mel 1a) is associated with melatonin-induced enhancement ofcell mediated and humoral immunity. Neuroendocrinology. 2001;74:178-184. 58. Lotufo CM, Lopes C, Dubocovich ML, Farsky SH, Markus RP. Melatoninand N-acetylserotonin inhibit leukocyte rolling and adhesion to rat micro-circulation. Eur J Pharmacol. 2001;430:351-357.59. Regrigny O, Delagrange P, Scalbert E, Atkinson J, Chillon JM. Melatoninincreases pial artery tone and decreases the lower limit of cerebral bloodflow autoregulation. Fund Clin Pharmacol. 2001;15:233-238. 60. Kopp C, Vogel E, Rettori MC, et al. Regulation of emotional behaviourby day length in mice: implication of melatonin. Behav Pharmacol.1999;10:747-752.
61. Gauer F, Masson-Pévet M, Skene DJ, Vivien-Roels B, Pévet P. Dailyrhythms of melatonin binding sites in the rat pars tuberalis and suprachi-asmatic nuclei; evidence for a regulation of melatonin receptors by mela-tonin itself. Neuroendocrinology. 1993;57:120-126. 62. Gauer F, Masson-Pévet M, Stehle J, Pévet P. Daily variations in mela-tonin receptor density of rat pars tuberalis and suprachiasmatic nuclei aredistinctly regulated. Brain Res. 1994;641:92-98. 63. Pévet P. Melatonin. Dialogues Clin Neurosci. 2002;4:57-72.64. Redman J, Armstrong S, Ng KT. Free-running activity rhythms in the rat:entrainment by melatonin. Science. 1983;219:1089-1091.65. Slotten HA, Pitrosky B, Pévet P. Entrainment of circadian activityrhythms in rats to melatonin administered at T cycles different from 24hours. Neurosignals. 2002;11:73-80.66. Redman JR, Armstrong SM. Reentrainment of rat circadian activityrhythms: effects of melatonin. J Pineal Res. 1988;5:203-215.67. Warren WS, Hodges DB, Cassone VM. Pinealectomized rats entrain andphase-shift to melatonin injections in a dose-dependent manner. J BiolRhythms. 1993;8:233-245.68. Enright JT. Methodology. In: Aschoff J, ed. Handbook of BehavioralNeurobiology. Vol 4. New York, NY: Plenum Press; 1981;11-19. 69. Pitrosky B, Kirsch R, Malan A, Mocaer E, Pévet P. Organization of ratcircadian rhythms during daily infusion of melatonin or S 20098, a mela-tonin agonist. Am J Physiol. 1999;277:R812-R828.70. Kirsch R, Belgnaoui S, Gourmelen S, Pévet P. Daily melatonin infusionentrains free-running activity in Syrian and Siberian hamsters. In:Wettenberg L, ed. Light and Biological Rhythm in Man. New York, NY:Pergamon; 1993:107-120.71. Slotten HA, Krekling S, Sicard B, Pévet P. Daily administration of mela-tonin entrains circadian activity rhythms in the diurnal rodent Arvicanthisensorgei. Behav Brain Res. 2002;133:11-19.72. Schuhler S, Pitrosky B, Kirsch R, Pévet P. Entrainment of locomotor activ-ity rhythm in pinealectomized Syrian hamster by daily melatonin infusionunder different conditions. Behav Brain Res. 2002;133:343-350.73. Bothorel B, Barassin S, Saboureau M, Malan A, Pévet P. In the rat exoge-nous melatonin increases the amplitude of pineal melatonin secretion bya direct action on the circadian clock. Eur J Neurosci. 2002;16:1090-1098. 74. Cassone VM, Chesworth MJ, Armstrong SM. Dose-dependent entrain-ment of rat circadian rhythms by daily injection of melatonin. J BiolRhythms. 1986;1:219-229. 75. Slotten HA, Pitrosky B, Pévet P. Influence of the mode of daily mela-tonin administration on entrainment of rat circadian rhythms. J BiolRhythms. 1999;14:347-353.76. Pitrosky B, Masson-Pévet M, Kirsch R, Vivien-Roels B, Canguilhem B,Pévet P. Effects of different doses and durations of melatonin infusions onplasma melatonin concentrations in pinealectomized Syrian hamsters: con-sequences at the level of sexual activity. J Pineal Res. 1991;11:149-155.77. McArthur AJ, Hunt AE, Gillette MU. Melatonin action and signal trans-duction in the rat suprachiasmatic circadian clock: activation of proteinkinase C at dusk and dawn. Endocrinology. 1997;138:627-634.78. Gillette MU, McArthur AJ. Circadian actions of melatonin at thesuprachiasmatic nucleus. Behav Brain Res. 1996;73:135-139. 79. Vanecek J, Pavlik A, Illnerova H. Hypothalamic melatonin receptor sitesrevealed by autoradiography. Brain Res. 1987;435:359-362.80. Bonnefond C, Monnerie R, Richard JP, Martinet L. Melatonin and thecircadian clock in mink: effects of daily injections of melatonin on circa-dian rhythm of locomotor activity and autoradiographic localization ofmelatonin binding sites. J Neuroendocrinol. 1993;5:241-246. 81. Gauer F, Schuster C, Poirel VJ, Pévet P, Masson-Pévet M. Cloning exper-iments and developmental expression of both melatonin receptor Mel1AmRNA and melatonin binding sites in the Syrian hamster suprachiasmaticnuclei. Mol Brain Res. 1998;60:193-202. 82. Maywood ES, Bittman EL, Ebling FJ, Barrett P, Morgan P, Hastings MH.Regional distribution of iodomelatonin binding sites within the suprachi-asmatic nucleus of the Syrian hamster and the Siberian hamster. JNeuroendocrinol. 1995;7:215-223. 83. Grosse J, Velickovic A, Davis FC. Entrainment of Syrian hamster circa-dian activity rhythms by neonatal melatonin injections. Am J Physiol.1996;270:R533-R540.
Melatonin in animal models - Pévet Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
351

B a s i c r e s e a r c h
352
84. Hastings MH, Mead SM, Vindlacheruvu RR, Ebling FJ, Maywood ES,Grosse J. Non-photic phase shifting of the circadian activity rhythm ofSyrian hamsters: the relative potency of arousal and melatonin. Brain Res.1992;591:20-26. 85. Weibel L, Rettori MC, Lesieur D, Delagrange P, Renard P, Van Reeth O.A single oral dose of S 22153, a melatonin antagonist, blocks the phasead-vancing effects of melatonin in C3H mice. Brain Res. 1999;829:160-166.86. Weaver DR, Liu C, Reppert SM. Nature’s knockout: the Mel1b receptoris not necessary for circadian or reproductive responses in Siberian ham-sters. Mol Endocrinol. 1996;10:1478-1487.87. Viswanathan N, Davis FC. Single prenatal injections of melatonin or theD1-dopamine agonist SKF 38393 to pregnant hamsters sets the offsprings’circadian rhythms to phases. 180 degrees apart. J Comp Physiol A.1997;180:339-346.
88. Liu C, Weaver DR, Jin X, et al. Molecular dissection of two distinct actionsof melatonin on the suprachiasmatic circadian clock. Neuron. 1997;19:91-102.89. Hunt AE, Al-Ghoul WM, Gillette MU, Dubocovich ML. Activation ofMT(2) melatonin receptors in rat suprachiasmatic nucleus phase advancesthe circadian clock. Am J Physiol. 2001;280:C110-C118.90. van den Top M, Buijs RM, Ruijter M, Delagrange P, Spanswick D, HermesMLHJ. Melatonin generates an outward potassium current in rat suprachi-asmatic nucleus neurons in vitro independent of their circadian rhythm.Neuroscience. 2001;107:99-108.91. Slotten HA, Pitrosky B, Pévet P. Entrainment of rat circadian rhythmsby melatonin does not depend on the serotonergic afferents to thesuprachiasmatic nuclei. Brain Res. 2000;876:10-16. 92. Pévet P, Bothorel B, Slotten H, Saboureau M. The chronobiotic proper-ties of melatonin. Cell Tissue Res. 2002;309:183-191.

Initial studies
n 1981, Kripke1 exposed seven nonseasonallydepressed patients to bright white light shortly beforetheir usual time of arising. Depression scores werereduced on the following day. In a subsequent study,2 5new subjects were added, for a total of 12 subjects, includ-ing 11 males with major depressive disorder (MDD) (3with bipolar illness) according to research diagnostic cri-teria (RDC),3 who were on an inpatient psychiatricresearch ward. In counterbalanced order, the investiga-tors administered either bright white light (1000 to 2000lux) or dim red light (less than 25 lux) for 1 h, 2 h beforethe subject’s usual time of arising. The bright white lighttreatment produced significantly lower depression scoreson both the Hamilton4 and Beck5 ratings as comparedwith baseline. A follow-up pilot experiment of 12depressed inpatients6 showed that there was no indica-tion that 1 h awakening with exposure to dim red light(25 lux) had any antidepressant effect.After demonstrating that sunlight and bright artificiallight could suppress human melatonin secretion, Lewy etal7 reported on a patient with a bipolar II seasonal moodcycle whose winter depression remitted when his hoursof daylight were lengthened with bright fluorescent light(Vital-Lite) of 2000 lux between his time of awakening(6.00 AM) and 9.00 AM, and between 4.00 PM and 7.00 PM,thereby extending his daylength (photoperiod) to 13 h (aspring photoperiod). During light exposure, melatoninlevels declined by 88% between 1.00 and 5.00 AM.Winter depression has been found to improve whenpatients are exposed to bright full-spectrum light beforedawn and after dusk, thereby extending the photope-riod.8,9 Bright light consisted of 2500 lux of full-spectrumlight; dim light was 300 lux. Light was administered from5.00 AM to 8.00 AM, and 5.30 PM to 8.30 PM every day.Bright light had a marked antidepressant effect, whereas
P h a r m a c o l o g i c a l a s p e c t s
353
Light treatment of mood disordersBarbara L. Parry, MD; Eva L. Maurer, BS
IIn 1981, seven patients with nonseasonal depression weretreated with bright white light. In 1982, bright artificiallight was used to treat a manic-depressive patient with aseasonal mood cycle. In the last 20 years, a plethora ofstudies have further defined the depressive populations,who are responsive to light treatment; the optimal tim-ing, intensity, spectral frequency, and duration of treat-ment; its comparison with other pharmacological inter-ventions; predictors of response; side-effect profiles; viableplacebo-control conditions; alternative devices and formsof administration; potential mechanisms and anatomicalpathways mediating light’s physiological effects; and itsapplication to other disorders and subsyndromal states.These studies have been conducted across multiple coun-tries with surprisingly consistent results. Further work isneeded, as highlighted in this review, to clarify the specificmechanism of action in subtypes of depressive disordersand differential age and gender effects. Although themajority of work in this area is relatively new, it behoovesthe reader to remember that Solomon, almost 3000 yearsago, wrote in Ecclesiastes: “Truly the light is sweet and apleasant thing it is for the eyes to behold the sun” (11:7).© 2003, LLS SAS Dialogues Clin Neurosci. 2003;5:353-365.
Keywords: light treatment; phototherapy; mood disorder; depression; seasonalaffective disorder
Author affiliations: Department of Psychiatry, University of California, SanDiego, 9500 Gilman Drive, La Jolla, Calif, USA
Address for correspondence: Department of Psychiatry, University ofCalifornia, San Diego, 9500 Gilman Drive, La Jolla, CA 92093-0804, USA(e-mail: [email protected])
Copyright © 2003 LLS SAS. All rights reserved www.dialogues-cns.org

P h a r m a c o l o g i c a l a s p e c t s
354
dim light did not. The response could not be attributedto sleep deprivation.Thus, the initial studies of light treatment appearedpromising, but many questions remained concerning theoptimal timing and intensity of treatment intervention.
Methodological issues
Morning versus evening light
Wehr et al10 found that time of day and suppression ofmelatonin were not critical for antidepressant effects ofphototherapy, indicating that photoperiodic mechanismswere not mediating the efficacy of therapeutic response.A review of efficacy using a pooled clustering techniquefor light therapy of seasonal affective disorder (SAD)11
reported that 2500-lux intensity light exposure for 2 hdaily for 1 week resulted in significantly more remissionswhen administered in the early morning (53%) than inthe evening (38%) or at midday (32%). All three timeswere significantly more effective than dim light controls(11%). Exposure to morning plus evening light providedno benefit over morning light alone. In support of thephase-shift hypothesis for winter depression, twogroups12,13 found that morning bright light phase-advanced the dim-light melatonin onset (DLMO) andwas more antidepressant than evening light, which phase-delayed it. The DLMO generally was delayed in thepatients with winter depression compared with thehealthy control subjects. Avery et al14 also found thatimprovement was significantly greater with morning lightthan with evening light in 7 patients with winter depres-sion treated with 7 days of bright light for 2 h daily. Otherworkers,15-17 however, found that either morning orevening light therapy improved depressive symptoms inpatients with SAD, suggesting that more practical andflexible schedules for light therapy are appropriate forSAD, since time of day is not crucial.As Wirz-Justice andAnderson noted,18 prior morning light treatment mayprevent an evening light response, and it may potentiateresponses to subsequent morning light.
Duration of response and treatment
The efficacy of treatment of patients with SAD lastslonger after withdrawal with bright light (>2000 lux) thanwith dim light (<300 lux).19,20 Labbate et al21 reported
increased response rates in SAD after 2 weeks ratherthan 1 week of light treatment: 15% of nonresponders atweek 1 responded after week 2 of treatment. Byerley etal22 found that, in 3 patients with SAD treated with 2 h ofmorning light exposure, remission of symptoms within2 to 5 days was sustained during the 2-month treatmentperiod. With regard to daily duration of treatment, 2 h,but not 0.5 h, morning white light was an effective treat-ment for SAD.23 Doghramji et al24 reported that 2 h ofevening light was as effective as 4 h in SAD. As Wirz-Justice et al25 commented, in patients who may be super-sensitive to light, 1 h of 2500 lux may be the minimumlight exposure necessary to maintain an antidepressanteffect in SAD.
Spectral frequency
Oren et al26 compared green light and red light, andfound that green light induced greater antidepressanteffects than red light. Stewart et al,27 however, observedthat white light was more effective than green light inreducing endogenous symptoms, but not the atypicalsymptoms characteristic of winter depression. Otherworkers28 reported that ultraviolet (UV) light reduceddepressive symptoms, but that UV-blocked light reducedonly atypical depressive symptoms. Bielski et al29
reported that both broad-spectrum fluorescent light andcool white light were equally effective in reducing SADsymptoms of depression. Brainard et al30 found that whitelight had greater benefit than red or blue light in SAD.Levitt et al31 studied dim versus bright red (light-emittingdiode) light, and found there was no significant differ-ence in response rates between the two different illumi-nances of red light for SAD.
Alternative techniques: dawn simulation
Bright (1700 lux) dawn simulation (4.00-6.00 AM) was noteffective in reducing depression scores in seven patientswith winter depression compared with a standard bright(1700 lux) morning (6.00-8.00 AM) light treatment andcontributed to early morning awakening (EMA).32 Incomparing a gradual dawn signal with a hypothesizedplacebo condition, a rapid dawn signal, Avery et al33
found that improvement was similar for both treatments,but that EMA was more common with the gradual dawncondition. In a follow-up study34 of 22 patients with win-ter depression, 1 week of treatment with 2-h dawn simu-

lation peaking at 250 lux resulted in significantly lowerdepression scores than 1 week of treatment with a 30-mindawn simulation peaking at 0.2 lux. Norden and Avery35
also demonstrated that a slow dawn (a gradually increas-ing illuminance over 45 min peaking at 100 lux) was bet-ter than a rapid dawn (light rapidly increasing over a 4-speriod to 100 lux) in 16 patients with subsyndromal win-ter depression. In a second controlled study of dawn simulation of winter depression,Avery et al36 showed that 1.5 h of 250 lux dawn simulation with while light resultedin lower depression scores than 1.5 h of a 2 lux, red dawnsignal. Linjaerde et al37 found that symptoms of winterdepression improved 57% with lightbox treatment of1500 to 2500 lux for 2 h in the morning for 6 days com-pared with 40% for dawn simulation of 60 to 90 min with100 to 300 lux for 2 weeks. A controlled study of 95 sub-jects with SAD38 found that dawn simulation (1.5-h dawnsignal from 4.30-6.00 AM peaking at 250 lux), but notbright light treatment (10 000 lux for 30 min from 6.00-6.30 AM), was associated with greater remission ratesthan placebo (dim red light, 1.5-h dawn signal from 4.30-6.00 AM peaking at 0.5 lux).
Light visor
Stewart et al39 reported that a portable, head-mountedunit (HMU) was as efficacious as a standard lightbox forthe treatment of winter depression. In a study of 105 sub-jects across five centers,40 three intensities of a light visor(60, 600, and 3500 lux) for 2 weeks had equal antide-pressant efficacy in SAD. Teicher et al41 found no signifi-cant differences in therapeutic response between patientswith SAD who were treated with a dim (30 lux) red lightor a bright (600 lux) white light visor. In a controlledcomparison of a lightbox and a HMU in SAD,42 therewas no significant difference in response rates betweenpatients with SAD who received 2 weeks of light versuspatients who received no visible light by an HMU, orbetween patients who received the lightbox versus theHMU.
Summary
The majority of studies support the beneficial effects ofparticularly morning light in SAD for 2 h with at least2500 lux. UV light is not required for response. Dawnstimulation is an effective alternative, although the lightvisor is not.
Clinical phenomenology
Effects of latitude
In Iceland, Magnusson and Kristbjarnarson43 found that10 000-lux white light was more effective than 400-lux redlight for 40 min for 8 days for treatment of SAD: patientswho improved most on phototherapy also improvedmost during summer. In Norway, Lingjaerde et al44
reported that patients with SAD, after treatment with1500-lux white full-spectrum light for 2 h in the morningfor 6 days, had a 48% reduction in symptoms comparedwith a 56% reduction of patients receiving light and drugtreatment. Improvement at 1 week was maintained forthe rest of the season.In a follow-up study of SAD in Switzerland, Graw et al45
observed that 2 to 5 years after participation in a light ther-apy trial, 64% of the patients had a reduction in the inci-dence and severity of depressive episodes and the use ofantidepressant drugs. In a study of light therapy for SADin adolescents in Iceland,46 light therapy mildly improvedthe ability to concentrate and wake up in the morning insome students, but did not improve school attendance.
Predictors of response
Lam47 reported that hypersomnia, hyperphagia, andyounger age predicted morning light therapy responsein winter depression.Terman et al48 observed that, in 103subjects with winter depression given light treatment,responders were characterized by atypical symptoms,especially hypersomnia, afternoon or evening slump,reverse diurnal variation (evening worse), and carbohy-drate craving. Nonresponders were characterized mainlyby melancholic symptoms. A follow-up study of 59patients with winter SAD at the National Institute ofMental Health49 found that 42% remained purely sea-sonal.The occurrence of nonseasonal depression in 44%of patients was associated with greater severity of illnessand less responsiveness to light treatment. There is agreater improvement in mood in summer than with lighttreatment in winter in patients with SAD.50 In meta-analysis of dose-response relationships of phototherapyfor SAD,51 no significant effects between strong,medium, and dim light in reducing atypical symptoms ofdepression were found, but light intensity varied posi-tively with the antidepressant effects for typical symp-
Light treatment of mood disorders - Parry and Maurer Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
355

toms. Levitt et al52 found that response rates were simi-lar in SAD and subsyndromal SAD with morning brightlight therapy of 5000 lux for 3 weeks. Longer exposureof 45 to 60 min daily tended to be associated with betteroutcome. In examining the effects of light therapy onsuicidal ideation, Lam et al53 found that 67% of patientswith winter depression were clinical responders: 45% ofpatients showed a reduction in the suicide item score onthe Structured Interview Guide for the HamiltonDepression Rating Scale, Seasonal Affective DisordersVersion (SIGH-SAD).54
Prevention
Meesters et al55,56 observed that administration of lighttreatment at the first signs of a winter depression pre-vented it from developing into a full-blown depression.When light exposure was administered at a symptom-free period at the beginning of autumn, however, it wasnot successful in preventing the development of winterdepression.57 Partonen and Lonnqvist,58 in contrast, didfind that bright light given well in advance of the emerg-ing symptoms of winter SAD prevented a depressiveepisode.
Effects on hypersomnia
Hypersomnia has been associated with a superiorresponse to morning light.59 In an open study design,Lam et al60 found that patients with winter depressionwho had hypersomnia had greater improvement, partic-ularly in atypical depression symptoms than patientswith insomnia. Evening subjective sleepiness improveswith morning light, even a short 15-min exposure, inpatients with winter depression.61
Comparison with antidepressant medication
Wirz-Justice et al62 described a woman with SAD who,after remitting within a week in each of 6 separate trialsof light therapy, remitted within 2 weeks of initiatingcitalopram, despite the delayed sleep and intermittentawakening induced with citalopram, but not with lighttherapy. Ruhrmann et al63 found that 70% of 40 SADpatients treated with bright light (3000 lux 2 h daily)were responders compared with 65% treated with flu-oxetine (20 mg daily for 5 weeks). Light treatmentimproved depression scores faster, while fluoxetine had
a faster effect on atypical symptoms. In 13 SAD patients,Ghadirian et al64 compared light therapy for 2 weeks ortryptophan for 4 weeks in an open repeated-measuresdesign.Tryptophan was equally effective to light therapyin treating SAD, but relapse after withdrawal of trypto-phan occurred more slowly. Improvement of atypicaldepressive symptoms after 1 h of light therapy positivelycorrelated with improvement after 2 weeks of therapy.65
Comparison with natural light
Eastman66 documented that the perceived sunlight expo-sure in SAD patients in Chicago was twice as much insummer than in winter: the perceived daylength was 4 to5 h longer in summer than in winter, with a later per-ceived dusk contributing more to the lengthening thanan earlier perceived dawn.Wirz-Justice et al67 observed that 50% of patients withSAD remitted after a daily 1-h morning walk outdoorsin natural light, which phase-advanced the onset and/oroffset of salivary melatonin secretion, and decreasedmorning cortisol compared with low-dose artificial light,which did not modify depression self-ratings, or mela-tonin or cortisol patterns.The effects of bright light treat-ment (2500 lux) on subsyndromal SAD in the workplacehave been studied,68 and both morning and afternoonexposure resulted in similar levels of improvement inmood, energy, alertness, and productivity.
Side effects
Terman et al69 reviewed the ocular effects of particularlythe more recent treatment approach of using approxi-mately 10 000 lux light exposure for 30 min. Althoughophthamological examinations have thus far revealed noinduced abnormalities, precaution is warranted with useof photosensitizing antidepressant drugs that mayenhance UV– and visible-light–induced lesions. Baueret al70 observed the induction of hypomania in winterdepressives treated with 4 weeks of light treatment.Seasonality—but not diagnosis of major depression,bipolar disorder with seasonal pattern, or control sub-ject—predicted the emergence of manic symptoms.
The influence of comorbid and other disorders
Stewart et al71 questioned whether SAD and atypicaldepression might be subtypes of the same disorder.
P h a r m a c o l o g i c a l a s p e c t s
356

Bright artificial light (2500 lux, 6.00-8.00 AM and 6.00-8.00 PM), however, was less effective in treating patientswith atypical depression than with SAD, suggesting thatthe two disorders are separate with a different under-lying pathophysiology. Partonen and Lonnqvist72
observed that in patients with comorbid personality dis-order, the remission rate with light treatment was simi-lar to that of patients with recurrent winter depression,although there was a more variable course and anincreased risk of an earlier onset of a depressive episode.A controlled trial in 28 children (aged 7-17 years)73
investigated the efficacy of light therapy for the treat-ment of pediatric SAD. In a primary care setting,74
patients with SAD improved after light therapy, butbright white versus dim red light was not associated withgreater improvement.
Response to placebo
Eastman et al75 observed that 32 patients with SADresponded equally to 1 h of morning light (7000 lux) and1 h of morning placebo treatment (a deactivated nega-tive ion generator). Richter et al,76 comparing exposureto real bright light and placebo bright light perceivedthrough hypnosis, concluded that the findings did notsupport the hypothesis that the long-term results of lighttreatment in SAD were merely placebo effects. Termanand Terman77 reported that 58% of patients with SADresponded to high-density negative ionizer treatment,whereas 15% responded to low-density ion generatortreatment.A placebo-controlled trial of bright (6000 lux)morning light, bright evening light, or morning placebo(a sham negative ion generator) for 1.5 h daily for 4weeks,78 found that by using strict response criteria fromthe SIGH-SAD54 (50% decrease of baseline and ≤8),61% of SAD patients responded to morning light, 50%to evening light, and 32% to placebo; however, there wasno significant benefit on mean Hamilton depression rat-ing scores. A controlled trial of timed bright light andnegative air ionization (6 groups) in 158 patients withwinter depression,79 reported that low-density ionresponse was inferior to all other groups, that eveninglight response was reduced when preceded by treatmentwith morning light, and when stringent remission crite-ria were used, a higher response rate to morning thanevening light.In summary, SAD patients, in particular, are responsiveto light treatment. Carbohydrate craving and hyper-
somnia are predictors of response.Acute intervention ismore efficacious than prophylactic treatment. Lightadministration is as effective as antidepressant treatmentor natural light exposure. Side effects are minimal, withthe exception of the induction of mania in bipolarpatients, and there may be significant placebo effects.
Light treatment of nonseasonal mood disorders
Major depressive disorder
In an open trial with unmatched patient groups,Yerevanian et al80 found that 1 to 2 weeks of light treat-ment with ≥2000 lux was effective in reducing depressivesymptoms in seasonal, but not nonseasonal patients,whose functioning was more impaired (by unpaired t tests).Although the patient groups were unmatched, ina comparison of bright white light (2500 lux) and dimlight (50 lux) from approximately 7.00 to 9.00 AM for 7days in up to 42 patients who met RDC for nonseasonalMDD, other workers81-83 observed a significant reductionin depressive symptomatology in all patients, but the dif-ference between bright and dim light was not significant.In a 10-day study of morning (6.00-8.00 AM) or evening(6.00-8.00 PM) bright (1500 lux) light room treatment of90 patients with either seasonal or nonseasonal MDD,84
patients with seasonal pattern improved significantlymore than those with a nonseasonal pattern, irrespectiveof time of treatment, atypical symptoms, or carbohydratecraving. Yamada et al85 administered bright or dim lightin the morning or evening to 27 unmedicated patientswith nonseasonal depression by Diagnostic andStatistical Manual of Mental Disorders, Revised ThirdEdition (DSM-III-R)86 criteria and found that bright, butnot dim, light significantly improved clinical symptomsof depression, independent of the time of treatment.Thecircadian rhythm of body temperature was more sensi-tive to the entraining effects of bright light in depressedversus normal control subjects, but was not related toclinical improvement. In a reassessment of the speed,efficacy, and combined treatment effects for nonseasonaldepression, Kripke87 observed that light treatment pro-duced net benefits in the range of 12% to 35% oftenwithin a week, and that the effects for nonseasonal andseasonal depression were comparable and producedfaster antidepressant benefits than psychopharmaco-logical treatment.
Light treatment of mood disorders - Parry and Maurer Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
357

Inpatient studies
In the setting of a psychiatric hospital,Wirz-Justice et al88
reported that 61% of 37 nonmedicated patients withmajor depression responded to light treatment in a 10-day open trial using ceiling lights of 3000 lux either for8 h (5.00-9.00 AM and 4.00-8.00 PM) or 4 h only (5.00-9.00AM). Results of pilot data using 2 h of 10 000 lux lightalso suggested that further controlled trials were war-ranted in this population. In a controlled trial of hospi-talized veterans with nonseasonal MDD or depressedforms of bipolar disorder, Kripke et al89 found that the25 patients treated with bright white light (2000-3000lux) improved in measures of depression compared withthe 26 patients randomized to dim red light placebo-con-trol treatment. Two patients treated with bright whitelight became hypomanic. Partial relapse appeared within2 days. Patients treated in winter responded as well asthose treated in summer. Beauchemin and Hays90
observed that in a psychiatric inpatient unit, depressedpatients in sunny rooms had a significantly shorter hos-pital stay than those in dull rooms. In a follow-up study,91
they randomly assigned depressed inpatients to high andlow levels of artificial light and found that both unipolarand bipolar depressed patients responded more to brightthan dim light when used as an adjunct to pharma-cotherapy. Benedetti et al92 also found that length of hos-pitalization for 415 unipolar and 187 bipolar depressedinpatients was reduced in bipolar patients in easternrooms exposed to direct sunlight in the morning com-pared with western rooms. No effect was found in unipo-lar inpatients. In a placebo-controlled, crossover studyof bright light treatment of depression in institutional-ized older adults, Sumaya et al93 found that 50% ofpatients were no longer in the depressed range after 1week treatment with 10 000 lux, but their depressionscores were unchanged after placebo (300 lux) or con-trol (no treatment) conditions. Patients with higherdepression scores, associated with longer duration ofinstitutionalization, experienced the greatest improve-ment with the 10 000 lux treatment.
Interaction with medication and other antidepressanttreatment
Levitt et al94 administered a 2-week course of bright lighttherapy to 10 patients who presented during the wintermonths with major depression and who had failed an
adequate trial of antidepressants, or who had relapsedfollowing a successful course of antidepressants andfound that augmentation with bright lights resulted insubstantial improvement in 7 of the 10 patients.Holsboer-Trachsler et al95 reported that adjunctive treat-ment with bright light or sleep deprivation did not has-ten the onset of antidepressant action of the antidepres-sant trimipramine, but the groups were not balanced onbaseline prognostic factors. Neumeister et al96 adminis-tered bright (3000 lux) or dim (100 lux) light for 6 daysto depressed patients from the morning after they under-went partial sleep deprivation (PSD) treatment. Inresponders to PSD, bright light therapy prevented therelapse after the next night of sleep and significantly pro-longed the antidepressant effects of PSD up to 7 days.Patients treated with dim light relapsed after a recoverynight of sleep and showed no further improvement oftheir depressive symptoms after 1 week of dim lighttreatment. PSD nonresponders did not benefit from lighttreatment. Muller et al97 found that the side effects ofadjunct bright light therapy as compared with antide-pressant (trimipramine) monotherapy included aggra-vated sedation, restlessness, sleep disturbance, decreasedappetite, and vertigo. Prasko et al98 treated inpatients withrecurrent nonseasonal depression with (i) bright light(5000 lux from 6.00-8.00 AM) and impramine 150 mg/day;(ii) bright light and placebo; or (iii) dim red light (500 luxfrom 6.00-8.00 AM) and imipramine 150 mg/day. Patientsin all 3 groups improved significantly, but the improve-ment of patients with bright light plus placebo was non-significantly superior to the other two groups. Loving etal99 found that in 13 patients with MDD who underwenta half night of home wake therapy (sleep deprivation),those who subsequently received 10 000 lux bright whitelight for 30 min between 6.00 and 9.00 AM improved 27%in 1 week, compared with those receiving dim red(placebo) light at a comparable time.
Bipolar illness
The effects of 2 weeks of bright light and 1 week of dimlight were investigated in patients with bipolar II SADversus controls100 and bright light was found to reduce oreliminate all group differences and variability in behav-ioral engagement, a mood dimension specifically associ-ated with depression. Papatheodorou and Kutcher101
treated persistent depressive symptoms in adolescent-onset bipolar disorder with adjunctive light therapy (10
P h a r m a c o l o g i c a l a s p e c t s
358

000 lux twice per day): out of 7 patients, 3 showed amarked (70%) decrease in symptoms, 2 had a moderate(40%) decrease, and 2 had mild to no response. In 2patients with bipolar disorder and 1 with recurrentMDD, Praschak-Rieder et al102 observed that within thefirst week after beginning bright light therapy, 2 subjectsattempted suicide and the third patient developed suici-dal thoughts that were so acute and overwhelming thatthe light therapy had to be discontinued. In a patientwith rapid-cycling bipolar illness, Wirz-Justice et al103
found that extending the dark/rest period to 14 h (plusa 1-h midday nap) immediately stopped the rapid cyclingand when midday, then morning light therapy wasadded, depression gradually improved achieving near-euthymia. In 115 bipolar depressed inpatients treatedwith total sleep deprivation,104 morning light therapy(150 or 2500 lux) and ongoing lithium treatment signif-icantly enhanced and sustained the effects of total sleepdeprivation on mood, with no additional benefit whenthe two treatments were combined.
Women’s mood disorders
The efficacy of light treatment has been studied inwomen with premenstrual (late luteal phase) dysphoricdisorder.105-108 In an open trial of morning light therapy fortreatment of antepartum depression, Oren et al109
observed that, after 3 weeks of treatment, mean depres-sion ratings improved by 49%. Benefits were seenthrough 5 weeks of treatment and there was no evidenceof adverse effects of light therapy on pregnancy. In twopatients with postpartum depression,110 there was a 75%reduction in depressive symptoms with light therapy.In summary, the emerging evidence suggests the poten-tial efficacy of light treatment in MDD, in inpatients andoutpatients, and in women’s mood disorders. Light treat-ment may also enhance the efficacy of other antidepres-sant modalities.
Proposed mechanisms
Circadian timing
Lewy et al111 proposed that the timing of bright light is crit-ical for its antidepressant effect in SAD: the mechanismwas related to a phase-advance of circadian rhythms thatcorrected a pathogenic phase-delay.Terman et al112 foundthat the antidepressant effect of light in SAD was poten-
tiated by early-morning administration in circadian time,optimally about 8.5 h after melatonin onset or 2.5 h afterthe sleep midpoint, suggesting the importance of phaserelationships in treatment response.
Melatonin
Terman et al113 proposed that early morning and eveninglight exposure impacted a photosensitive interval inSAD patients, in which melatonin secretion overshootsits normal nocturnal phase. Despite equal suppressionof plasma melatonin levels, altered timing of light treat-ments has differential effects on mood.114 Danilenko etal115 found that daytime (12 noon and 4.00 PM) serummelatonin levels were higher in women with SAD com-pared with controls in winter; this difference disap-peared in the summer and after light treatment in thewinter. Light treatment and change in season alsoresulted in a phase-advance shift of melatonin in theSAD patients, associated with a decline in symptoms ofhyperphagia and carbohydrate craving. Partonen116
hypothesized that the induction of arousing stimulimediated by effects of melatonin and the blockade ofserotonin uptake mechanisms in the suprachiasmaticnucleus is necessary for the antidepressant effects oflight in SAD. In patients with SAD who underwent lighttreatment with full-spectrum or cool white light,117 bothtreatments reduced depression scores, advanced the tim-ing of the salivary melatonin rhythm (in both respondersand nonresponders), and increased its concentration. Inlight treatment of patients with seasonal and nonsea-sonal depression, melatonin amplitude was decreased bylight and its phase position was advanced by morninglight and delayed by evening light, but therapeutic out-come was not related to baseline melatonin phase posi-tion, the degree of light suppression of melatonin or therebound effect of serum melatonin levels followingbright light exposure.118
Serotonin
A study of patients with nonseasonal depression andhealthy subjects119,120 found that both bright as well asdim light augmented blood serotonin throughout theday. The influence of light was more pronounced onserotonin than on melatonin metabolism. Mellerup etal121 examined platelet paroxetine binding as an indirectmeasure of the effect of light therapy on serotonin
Light treatment of mood disorders - Parry and Maurer Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
359

uptake capacity in patients with winter depression.Theyfound that in responders, but not in nonresponders,platelet serotonin transporters decreased significantlyfollowing treatment. An extended study of the seroton-ergic agent meta-chlorophenylpiperazine (m-CPP)122
replicated the finding that m-CPP–induced activation-euphoria responses in untreated depressed patients withSAD, reflecting a state marker for the illness. This studyalso showed blunted corticotropin and norepinephrineresponses to m-CPP, suggesting trait abnormalities.Mood improvement after light treatment was associatedwith lowering of nocturnal core temperatures, compat-ible with deficient serotonin transmission during winterdepression. In a study of platelet serotonergic functionsin SAD, Stain-Malmgren et al123 found that respondersto light therapy had higher Km and lower Bmax for parox-etine binding than nonresponders, suggesting abnor-malities in the serotonin uptake mechanism withenhanced serotonin 5-HT2 receptor density that mayreflect an upregulation.
Effects of tryptophan depletion
Rapid tryptophan depletion reverses the antidepressanteffect of bright light therapy in patients with SAD,124,125
suggesting that the therapeutic effects of bright light inthis disorder may involve a serotonergic mechanism.Neumeister et al126 also demonstrated that catecholaminedepletion reversed the beneficial effects of light therapy,suggesting that brain catecholaminergic systems may alsobe involved.
Other neurotransmitters
In studies of platelet [3H]imipramine binding in patientswith or without SAD, and healthy controls, Szadoczky etal127,128 observed that, after incandescent light treatment,Bmax values increased in SAD patients parallel with clin-ical improvement. In patients with SAD, light therapyproduced a decrease in the urinary output of norepi-nephrine and its metabolites in association with signifi-cant decreases in depression ratings.129 In contrast,Rudorfer et al130 measured cerebrospinal fluid concen-trations of the principal metabolites of norepinephrine,serotonin, and dopamine and did not find differencesbetween SAD and healthy controls. Neither the trans-mitter measures nor their interrelatedness was affectedby phototherapy.
Endocrine function
On the basis of observed low serum prolactin concentra-tion in women with winter depression that was indepen-dent of season and bright light treatment, Partonen131
hypothesized a role for estrogen and serotonergic func-tion in SAD. Normal thyroid function in SAD does notalter with light treatment.132 Serum cortisol does not dif-fer between SAD and non-SAD patients, and no signifi-cant changes were seen as a result of light treatment,although melatonin appears to serve as a coordinatinghormone transducing light information for the phase posi-tion of cortisol.133 Partonen134 also hypothesized that brightlight, by normalizing increased corticotropin-releasing fac-tor (CRF) activity in the evening in SAD, might therebynormalize subjective sleepiness via its effects on neuronsof the paraventricular nucleus of the hypothalamus. Instudies of growth hormone (GH),Yatham et al135 reportedthat GH responses to sumatriptan (a 5-HT1D receptoragonist) were significantly blunted during winter depres-sion in SAD patients compared with healthy controls andwere normalized following light treatment.These findingssuggest a role for the serotonergic system in the mecha-nism of action of light therapy. In contrast, Shiah et al136
found that GH response to the γ-aminobutyric acid(GABA)B receptor agonist, baclofen, was not altered inSAD or by light therapy. On the basis of evidence thatheme moieties and bile pigments in plants and animalsmediate some of the nonvisual influences of light on bio-logical rhythms, Oren137 hypothesized that bilirubin, whichis a proposed photoreceptor given its similarity to thechromophore of phytochrome (a primary time-settingplant molecule), plays an evolutionary role in the regula-tion of rapid-eye movement (REM) sleep and in mediat-ing some of the antidepressant effects of light. He and hiscolleagues138 found that nocturnal bilirubin levels werelower in patients with winter depression compared withcontrols, and that levels increased in both groups duringthe night and increased in patients after 2 weeks of morn-ing light treatment that improved mood.
Sleep, hemispheric, and EEG changes
Bright light shortens sleep onset, decreases number ofawakenings, increases REM latency, attenuates REMlength, and improves morning alertness in patients withMDD.139 In SAD patients, Partonen et al140 found nosleep electroencephalographic (EEG) changes after
P h a r m a c o l o g i c a l a s p e c t s
360

treatment with bright light, although morning sleepinesswas reduced. SAD patients have the expected pattern ofEEG frontal asymmetry when depressed and followinglight-induced remission, although right hemispherecoherence is a state-dependent indicator of seasonaldepression.141 Winter depression is associated with a shiftof laterality from the left to the right that was normal-ized by bright light treatment.142 Brunner et al143 docu-mented normal homeostatic sleep regulation in SAD;although sleep EEG spectra in SAD, but not controls,showed modifications resembling those of recoverysleep after light treatment (perhaps reflecting sleep cur-tailment), the authors concluded that the effects of lighttreatment in SAD were unlikely to be mediated bychanges in sleep.A positive response to total sleep depri-vation in major depression is predictive of a beneficialoutcome of subsequent light therapy.144
Temperature regulation
In a review of the neurobiological effects of artificialbright light, Dilsaver145 reported that, based on measuresof core temperature, bright light subsensitizes muscarinicand nicotinic mechanisms.Although temperature curvesbetween SAD and controls were similar, light treatmentenhanced the amplitude of the core body temperaturerhythm in SAD patients during winter.146 There were noabnormalities in the baseline phase or amplitude of thetemperature rhythm in SAD patients versus controls,147
and antidepressant responses to light treatment wereunrelated to changes in the temperature rhythm. In con-stant routine conditions, Avery et al148 documented aphase-delay of temperature and cortisol rhythms inhypersomnic winter depression that phase-advanced withbright light treatment. Schwartz et al149 observed that coretemperature minima were lower during the extendedphotoperiod of summer compared with winter in SADpatients, but not controls. In studying the oscillations offacial skin and core temperatures in relation to slow-wave activity during sleep, Schwartz et al150 found thatbrain cooling activity, which oscillates in an ultradianmanner during sleep, is reduced during winter depres-sion, providing support for the hypothesis that brain tem-peratures are elevated during winter depression.
Functional anatomic and retinal sensitivity factors
Seggie et al151 observed that antidepressant medication(sinuequan) reversed the increased sensitivity to light indepression. Terman and Terman152 reported heightenedretinal sensitivity with increased light exposure andsupersensitivity of SAD patients relative to controls inwinter. UVA-spectrum light did not increase the anti-depressant response153 and illumination applied in theupper visual field was most effective.154 An increase incerebral blood flow is associated with recovery follow-ing light treatment for SAD.155
Other
Patients with non-SAD major depression show a morepronounced light-associated increment of parasympa-thetically controlled cardiac functions compared withother depressed patients and controls.156 Light therapynormalizes transducin (G1 protein) levels observed to bereduced in winter depression.157 No effects of light ther-apy were noted on basal glucagon levels in SAD andcomparison subjects.158 Immune-inflammatory markersare increased in SAD patients but are not altered by suc-cessful light therapy.159
In summary, the proposed mechanisms for light treatmentprimarily involve effects on the circadian timing system,melatonin, serotonin, and temperature regulation.
Conclusions
Light treatment is efficacious for SAD (winter-type) andan increasing database suggests that it has beneficial effectsin nonseasonal depression as well. In toto, bright light(>2500 lux) results in greater improvement than dim light;morning light of at least 3 to 4 days duration results inmore responders than evening light in SAD; UV-spectrumwavelengths are not required for antidepressant effects;and dawn-stimulation is an effective alternative. Lightvisors, in contrast, are not efficacious. Carbohydrate crav-ing is a predictor of response and there are minimal sideeffects with the exception of the risk of inducing mania inbipolar patients. Further investigation is warranted withrespect to light treatment’s mechanism of action. ❏
Light treatment of mood disorders - Parry and Maurer Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
361

P h a r m a c o l o g i c a l a s p e c t s
362
Fototerapia de los trastornos afectivos
En 1981 siete pacientes con depresión no estacionalfueron tratados con luz blanca brillante. En 1982 seutilizó luz artificial brillante para tratar a un pacientemaníaco-depresivo con un ciclo de ánimo estacional.En los últimos 20 años gran cantidad de estudios hanpermitido definir con mayor precisión, además de laspoblaciones de pacientes depresivos que respondena la fototerapia, el momento óptimo de la aplica-ción, la intensidad, la frecuencia del espectro y laduración del tratamiento. También se la ha compa-rado con otras intervenciones farmacológicas, se hanestudiado los predictores de respuesta, el perfil deefectos colaterales, el uso de placebos adecuados aestos estudios, diversos aparatos y formas de admi-nistración, potenciales mecanismos y vías anatómi-cas que median los efectos farmacológicos de la luzy su aplicación a otros trastornos y estados subsin-dromáticos. Estos estudios se han realizado en variospaíses con resultados sorprendentemente constan-tes. Se requiere de futuros trabajos, como se destacaen esta revisión, para aclarar el mecanismo de acciónespecífico en subtipos de trastornos depresivos ydiferenciar efectos según edad y sexo. Aunque lamayor parte del trabajo en esta área es relativa-mente nuevo, le corresponde al lector recordar queSalomón, hace casi 3000 años, escribió en elEclesiastés (11:7) “Verdaderamente la luz es dulce yes algo placentero para los ojos contemplar el sol.”
Luminothérapie des troubles de l’humeur
En 1981, sept patients atteints de dépression non sai-sonnière ont été traités par lumière blanche intense.En 1982, la lumière artificielle intense a été utiliséepour traiter un patient maniacodépressif souffrantd’un trouble cyclothymique saisonnier. Durant ces 20dernières années, une pléthore d’études ont mieuxidentifié les populations dépressives sensibles à laluminothérapie ; le rythme optimal du traitement,son intensité, sa fréquence spectrale et sa durée ; sa comparaison avec d’autres types de traitement ;les facteurs prédictifs de réponse ; les effets secon-daires ; les conditions placebo/témoin adaptées ; lestechniques alternatives et les différentes méthodesd’administration ; les voies anatomiques et les méca-nismes potentiels véhiculant les effets physiologiquesde la lumière ; et ses applications aux autres troubleset états sous-syndromiques. Ces études ont étéconduites dans de nombreux pays, la concordancedes résultats étant tout à fait surprenante. Commele souligne cet article, d’autres travaux sont néces-saires afin de clarifier les mécanismes d’action spéci-fiques dans les sous-types de troubles dépressifs etl’influence de l’âge et du sexe. Bien que la majoritédes travaux dans ce domaine soit relativementrécente, il incombe au lecteur de se souvenir de ceque Salomon, il y a presque 3 000 ans, écrivit dansl’Ecclésiaste (XI, 7) : « Douce est la lumière et il plaîtaux yeux de voir le soleil ».
REFERENCES
1. Kripke DF. Photoperiodic mechanisms for depression and its treatment.In: Perris C, Struwe G, Jansson B, eds. Biological Psychiatry. Amsterdam, TheNetherlands: Elsevier; 1981:1249.2. Kripke DF, Risch SC, Janowsky D. Bright white light alleviates depression.Psychiatry Res. 1983;10:105-112.3. Spitzer RL, Endicott J, Robins E. Research diagnostic criteria: rationale andreliability. Arch Gen Psychiatry. 1978;35:773.4. Hamilton M. A rating scale for depression. J Psychiatry Neurol Neurosurg.1960;23:56.5. Beck At, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory formeasuring depression. Arch Gen Psychiatry. 1961;4:561.6. Kripke DF, Risch S, Janowsky DS. Lighting up depression. PsychopharmacolBull. 1983;19:526-530.7. Lewy AJ, Kern HA, Rosenthal NE, Wehr TA. Bright artificial light treat-ment of a manic-depressive patient with a seasonal mood cycle. Am JPsychiatry. 1982;139:1496-1498.8. Rosenthal NE, Sack DA, Gillin JC, et al. Seasonal affective disorder: adescription of the syndrome and preliminary findings with light treatment.Arch Gen Psychiatry. 1984;41:72-80.
9. Rosenthal NE, Sack DA, Carpenter CJ, Parry BL, Mendelson WB, Wehr TA.Antidepressant effects of light in seasonal affective disorder. Am J Psychiatry.1985;142:163-170.10. Wehr TA, Jacobsen FM, Sack DA, Arendt J, Tamarkin L, Rosenthal NE.Phototherapy of seasonal affective disorder. Arch Gen Psychiatry.1986;43:870-875.11. Terman M, Terman JS, Quitkin FM, McGrath PJ, Stewart JW, Rafferty B.Light therapy for seasonal affective disorder: a review of efficacy.Neuropsychopharmacology. 1989;2:1-22.12. Lewy AJ, Bauer VK, Cutler NL, et al. Morning vs evening light treatmentof patients with winter depression. Arch Gen Psychiatry. 1998;55:890-896.13. Sack RL, Lewy AJ, White DM, Singer CM, Fireman MJ, Vandiver R.Morning vs evening light treatment for winter depression: evidence thatthe therapeutic effects of light are mediated by circadian phase shifts. ArchGen Psychiatry. 1990;47:343-351.14. Avery DH, Khan A, Dager SR, Cox GB, Dunner DL. Bright light treatmentof winter depression: morning versus evening light. Acta Psychiatr Scand.1990;82:335-338.15. James SP, Wehr TA, Sack DA, Parry BL, Rosenthal NE. Treatment of sea-sonal affective disorder with light in the evening. Br J Psychiatry.1985;147:424-428.

Light treatment of mood disorders - Parry and Maurer Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
363
16. Wirz-Justice A, Graw P, Krauchi K, et al. Light therapy in seasonal affec-tive disorder is independent of time of day or circadian phase. Arch GenPsychiatry. 1993;50:929-937.17. Lafer B, Sachs GS, Labbate LA, Thibault A, Rosenbaum JF. Phototherapyfor seasonal affective disorder: a blind comparison of three different sched-ules. Am J Psychiatry. 1994;151:1081-1083.18. Wirz-Justice A, Anderson J. Morning light exposure for the treatmentof winter depression: the one true light therapy? Psychopharmacol Bull.1990;26:511-519.19. Wirz-Justice A, Bucheli C, Graw P, Kielholz P, Fisch HU, Woggon B. Lighttreatment of seasonal affective disorder in Switzerland. Acta Psychiatr Scand.1986;74:193-204.20. Grota LJ, Yerevaian, Gupta K, Kruse J, Zborowski L. Phototherapy forseasonal major depressive disorder: effectiveness of bright light of high orlow intensity. Psychiatry Res. 1989;29:29-35.21. Labbate LA, Lafer B, Thibault A, Rosenbaum JF, Sachs GS. Influence ofphototherapy treatment duration for seasonal affective disorder: outcomeat 1 vs 2 weeks. Biol Psychiatry. 1995;38:747-750.22. Byerley WF, Brown J, Lebegue B. Treatment of seasonal affective dis-order with morning light. J Clin Psychiatry. 1987;48:447-448.23. Wirz-Justice A, Schmid AC, Graw P, et al. Dose relationships of morningbright white light in seasonal affective disorder. Experientia. 1987;43:574-576.24. Doghramji K, Gaddy JR, Stewart KT, Rosenthal NE, Brainard GC. Two-versus four-hour evening phototherapy of seasonal affective disorder. J NervMental Dis. 1990;178:257-260.25. Wirz-Justice A, Bucheli C, Schmid A, Graw. A dose relationship in brightwhite light treatment of seasonal depression. Am J Psychiatry. 1986;143:932-933.26. Oren DA, Brainard GC, Johnston SH, Joseph-Vanderpool JR, Sorek E,Rosenthal NE. Treatment of seasonal affective disorder with green light andred light. Am J Psychiatry. 1991;148:509-511.27. Stewart KT, Gaddy JR, Byrne B, Miller S, Brainard GC. Effects of green orwhite light for treatment of seasonal depression. Psychiatry Res. 1991;38:261-270.28. Lam RW, Buchanan A, Clark CM, Remick RA. Ultraviolet versus non-ultra-violet light therapy for seasonal affective disorder. J Clin Psychiatry.1991;52:213-216.29. Bielski RJ, Mayor J, Rice J. Phototherapy with broad spectrum white flu-orescent light: a comparative study. Psychiatry Res. 1992;43:167-175.30. Brainard GC, Sherry RG, Skwerer RG, Waxler M, Kelly K, Rosenthal NE.Effects of different wavelengths in seasonal affective disorder. J Affect Disord.1990;20:209-216.31. Levitt AJ, Joffe RT, King E. Dim versus bright red (light-emitting diode)light in the treatment of seasonal affective disorder. Acta Psychiatr Scand.1994;89:341-345.32. Avery D, Bolte MA, Millet M. Bright dawn simulation compared withbright morning light in the treatment of winter depression. Acta PsychiatrScand. 1992;85:430-434.33. Avery DH, Bolte AP, Cohen S, Millet MS. Gradual versus rapid dawn sim-ulation treatment of winter depression. J Clin Psychiatry. 1992;53:359-363.34. Avery DH, Bolte MA, Dager SR, et al. Dawn simulation treatment of win-ter depression: a controlled study. Am J Psychiatry. 1993;150:113-117.35. Norden MJ, Avery DH. A controlled study of dawn simulation in sub-syndromal winter depression. Acta Psychiatr Scand. 1993;88:67-71.36. Avery DH, Bolte AP, Wolfson JK, Kazaras AL. Dawn simulation comparedwith a dim red signal in the treatment of winter depression. Biol Psychiatry.1994;36:181-188.37. Lingjaerde O, Foreland AR, Dankertsen J. Dawn simulation vs lightboxtreatment in winter depression: a comparative study. Acta Psychiatr Scand.1998;98:73-80.38. Avery DH, Eder DN, Bolte MA, et al. Dawn simulation and bright lightin the treatment of SAD: a controlled study. Biol Psychiatry. 2001;50:205-216.39. Stewart KT, Gaddy JR, Benson DM, Byrne B, Doghramji K, Brainard GC.Treatment of winter depression with a portable head-mounted pho-totherapy device. Prog Neuropsychopharmacol Biol Psychiatry. 1990;14:569-578.40. Joffe RT, Moul DE, Lam RW, et al. Light visor treatment for seasonalaffective disorder: a multicenter study. Psychiatry Res. 1993;46:29-39.41. Teicher MH, Glod CA, Oren DA, et al. The phototherapy light visor: moreto it than meets the eye. Am J Psychiatry. 1995;152:1197-1202.
42. Levitt AJ, Wesson VA, Joffe RT, Maunder RG, King EF. A controlled com-parison of light box and head-mounted units in the treatment of seasonaldepression. J Clin Psychiatry. 1996;57:105-110.43. Magnusson A, Kristbjarnarson H. Treatment of seasonal affective disor-der with high-intenisty light. A phototherapy study with an Icelandic groupof patients. J Affect Disord. 1991;21:141-147.44. Lingjaerde O, Reichborn-Kjennerud T, Haggag A, Gartner I, Berg EM, NarudK. Treatment of winter depression in Norway. Short- and long-term effects of1500-lux white light for 6 days. Acta Psychiatr Scand. 1993;88:292-299.45. Graw P, Gisin B, Wirz-Justice A. Follow-up study of seasonal affective dis-order in Switzerland. Psychopathology. 1997;30:208-214.46. Magnusson A. Light therapy to treat winter depression in adolescentsin Iceland. J Psychiatry Neurosci. 1998;23:118-122. 47. Lam RW. Morning light therapy for winter depression: predictors ofresponse. Acta Psychiatr Scand. 1994;89:97-101.48. Terman M, Amira L, Terman JS, Ross DC. Predictors of response and non-response to light treatment for winter depression. Am J Psychiatry.1996;153:1423-1429.49. Schwartz PJ, Brown C, Wehr TA, Rosenthal NE. Winter seasonal affec-tive disorder: a follow-up study of the first 59 patients of the NationalInstitute of Mental Health Seasonal Studies Program. Am J Psychiatry.1996;153:1028-1036.50. Postolache TT, Hardin TA, Myers FS, et al. Greater improvement in sum-mer than with light treatment in winter in patients with seasonal affectivedisorder. Am J Psychiatry. 1998;155:1614-1616.51. Lee TMC, Chan CCH. Dose-response relationship of phototherapy forseasonal affective disorder: a meta-analysis. Acta Psychiatr Scand.1999;99:315-323.52. Levitt AJ, Lam RW, Levitan R. A comparison of open treatment of sea-sonal major and minor depression with light therapy. J Affect Disord.2002;71:243-248.53. Lam RW, Tam EM, Shiah IS, Yatham LN, Zis AP. Effects of light therapyon suicidal ideation in patients with winter depression. J Clin Psychiatry.2000;61:30-32.54. Williams JBW, Link MJ, Rosentahl NE, et al. Structured Interview Guide forthe Hamilton Depression Rating Scale, Seasonal Affective Disorders Version (SIGH-SAD). New York, NY: New York State Psychiatric Institute; 1998.55. Meesters Y, Lambers PA, Jansen JHC, Bouhuys AL, Beersma DGM, vanden Hoofdakker RH. Can winter depression be prevented by light treat-ment? J Affect Disord. 1991;23:75-79.56. Meesters Y, Jansen JH, Beersma DGM, Bouhuys AL, van den HoofdakkerRH. Early light treatment can prevent an emerging winter depression fromdeveloping into a full-blown depression. J Affect Disord. 1993;29:41-47.57. Meesters Y, Jansen JHC, Beersma DGM, Bouhuys AL, van denHoofkadder RH. An attempt to prevent winter depression by light expo-sure at the end of September. Biol Psychiatry. 1994;35:284-286.58. Partonen T, Lonnqvist J. Prevention of winter seasonal affective disor-der by bright-light treatment. Psychol Med. 1996;26:1075-1080.59. Avery DH, Khan A, Dager SR, Cohen S, Cox GB, Dunner DL. Morning orevening bright light treatment of winter depression. The significance ofhypersomnia. Biol Psychiatry. 1991;229:117-126.60. Lam RW, Buchanan A, Mador JA, Corral MR. Hypersomnia and morninglight therapy for winter depression. Biol Psychiatry. 1992;31:1062-1064.61. Partonen T. Effects of morning light treatment on subjective sleepinessand mood in winter depression. J Affect Disord. 1994;30:99-108. 62. Wirz-Justice A, van der Velde P, Bucher A, Nil R. Comparison of lighttreatment with citalopram in winter depression: a longitudinal single casestudy. Int Clin Psychopharmacol. 1992;7:109-116.63. Ruhrmann S, Kasper S, Hawellek B, et al. Effects of fluoxetine versusbright light in the treatment of seasonal affective disorder. Psychol Med.1998;28:923-933.64. Ghadirian AM, Murphy BEP, Gendron MJ. Efficacy of light versus tryp-tophan therapy in seasonal affective disorder. J Affect Disord. 1998;50:23-27.65. Sher L, Matthews JR, Turner EH, Postolache TT, Katz KS, Rosenthal NE. Earlyresponse to light therapy partially predicts long-term antidepressant effects inpatients with seasonal affective disorder. J Psychiatry Neurosci. 2001;26:336-338.66. Eastman C. Natural summer and winter sunlight exposure patterns inseasonal affective disorder. Physiol Behav. 1990;48:611-616.

P h a r m a c o l o g i c a l a s p e c t s
364
67. Wirz-Justice A, Graw P, Krauchi K, et al. Natural light treatment of sea-sonal affective disorder. J Affect Disord. 1996;37:109-120.68. Avery DH, Kizer D, Bolte MA, Hellekson C. Bright light therapy of sub-syndromal seasonal affective disorder in the workplace: morning vs after-noon exposure. Acta Psychiatr Scand. 2001;103:267-274.69. Terman M, Reme CE, Rafferty B, Gallin PF, Terman JS. Bright light ther-apy for winter depression: potential ocular effects and theoretical implica-tions. Photochem Photobiol. 1990;51:781-792.70. Bauer MS, Kurtz JW, Rubin LB, Marcus JG. Mood and behavioral effectsof 4-week light treatment in winter depressives and controls. J Psychiatr Res.1994;28:135-145.71. Stewart JW, Quitkin FM, Terman M, Terman JS. Is seasonal affective dis-order a variant of atypical depression? Differential response to light ther-apy. Psychiatry Res. 1990;33:121-128.72. Partonen T, Lonnqvist J. The influence of comorbid disorders and of con-tinuation light treatment on remission and recurrence in winter depression.Psychopathology. 1995;28:256-262.73. Swedo SE, Allen AJ, Glod CA. A controlled trial of light therapy for thetreatment of pediatric seasonal affective disorder. J Am Acad Child AdolescPsychiatry. 1997;36:816-821.74. Wileman SM, Eagles JM, Andrew JE. Light therapy for seasonal affec-tive disorder in primary care. Br J Psychiatry. 2001;178:311-316.75. Eastman CI, Lahmeyer HW, Watell LG, Good GD, Young MA. A placebo-controlled trial of light treatment for winter depression. J Affect Disord.1992;26:211-222.76. Richter P, Bouhuys AL, van den Hoofdakker RH, et al. Imaginary versusreal light for winter depression. Biol Psychiatry. 1992;31:531-537.77. Terman M, Terman JS. Treatment of seasonal affective disorder with ahigh-output negative ionizer. J Altern Complementary Med. 1995;1:87-92.78. Eastman CI, Young MA, Fogg LF, Liu L, Meaden PM. Bright light treat-ment of winter depression. A placebo-controlled trial. Arch Gen Psychiatry.1998;55:883-889.79. Terman M, Terman JS, Ross DC. A controlled trial of timed bright lightand negative air ionization for treatment of winter depression. Arch GenPsychiatry. 1998;55:875-882.80. Yerevanian BI, Anderson JL, Grota LJ, Bray M. Effects of bright incan-descent light on seasonal and nonseasonal major depressive disorder.Psychiatry Res. 1986;18:355-364.81. Volz HP, Mackert A, Stieglitz RD, Muller-Oerlinghausen B. Effect ofbright white light therapy on non-seasonal depressive disorder. J AffectDisord. 1990;19:15-21.82. Mackert A, Volz HP, Stieglitz B, Muller-Oerlinghausen B. Effects of whitelight on non-seasonal depressive disorder. Pharmacopsychiatry. 1990;23:151-154.83. Mackeert A, Volz HP, Stieglitz, Muller-Oerlinghausen B. Phototherapyin nonseasonal depression. Biol Psychiatry. 1991;30:257-268.84. Thalen BE, Kjellman BF, Morkrid L, Wibom R, Wetterberg L. Light treat-ment in seasonal and nonseasonal depression. Acta Psychiatr Scand.1995;91:352-360.85. Yamada N, Martin-Iverson MT, Daimon K, Tsujimoto T, Takahashi S.Clinical and chronobiological effects of light therapy on nonseasonal affec-tive disorders. Biol Psychiatry. 1995;37:866-873.86. American Psychiatric Association. Diagnostic and Statistical Manual ofMental Disorders. 3rd ed, revised. Washington, DC: American PsychiatricAssociation; 1987.87. Kripke DF. Light treatment for nonseasonal depression: speed, efficacyand combined treatment. J Affect Disord. 1998;49:109-117.88. Wirz-Justice A, Graw P, Roosli H, Glauser G, Fleischhauer J. An open trial oflight therapy in hospitalized major depression. J Affect Disord. 1999;52:291-292.89. Kripke DF, Mullaney DJ, Klauber MR, Risch SC, Gillin JC. Controlled trialof bright light for nonseasonal major depressive disorders. Biol Psychiatry.1992;31:119-134.90. Beauchemin KM, Hays P. Sunny hospital rooms expedite recovery fromsevere and refractory depressions. J Affect Disord. 1996;40:49-51.91. Beauchemin KM, Hays P. Phototherapy is a useful adjunct in the treat-ment of depressed in-patients. Acta Psychiatr Scand. 1997;95:424-427.92. Benedetti F, Colombo C, Barbini B, Campori E, Smeraldi E. Morning sun-light reduces length of hospitalization in bipolar depression. J Affect Disord.2001;62:221-223.
93. Sumaya IC, Rienzi BM, Deegan JF, Moss DE. Bright light treatmentdecreases depression in institutionalized older adults: a placebo-controlledcrossover study. J Gerontol. 2001;56A:M356-M360.94. Levitt AJ, Joffe RT, Kennedy SH. Bright light augmentation in antide-pressant nonresponders. J Clin Psychiatry. 1991;52:336-337.95. Holsboer-Trachsler E, Hemmeter U, Hatzinger M, Seifritz E, Gerhard U,Hobi V. Sleep deprivation and bright light as potential augmenters of anti-depressant drug treatment-neurobiological and psychometric assessmentof course. J Psychiatr Res. 1994;28:381-399.96. Neumeister A, Goessler R, Lucht M, Kapitany T, Bamas C, Kasper S. Brightlight therapy stabilizes the antidepressant effect of partial sleep depriva-tion. Biol Psychiatry. 1996;39:16-21.97. Muller MJ, Seifritz E, Hatzinger M, Hemmeter U, Holsboer-Trachsler E.Side effects of adjunct light therapy in patients with major depression. EurArch Psychiatry Clin Neurosci. 1997;247:252-258.98. Prasko J, Horacek J, Klaschka J, Kosova J, Ondrackova I, Sipek J. Brightlight therapy and/or imipramine for inpatients with recurrent non-seasonaldepression. Neuroendocrinol Lett. 2002;23:109-113.99. Loving RT, Kripke DF, Shuchter SR. Bright light augments antidepressanteffects of medication and wake therapy. Depress Anxiety. 2002;16:1-3.100. Krauss SS, Depue RA, Aribisi PA, Spoont M. Behavioral engagementlevel, variability and diurnal rhythm as a function of bright light in bipo-lar II seasonal affective disorder: an exploratory study. Psychiatry Res.1992;43:147-160.101. Papatheodorou G, Kutcher S. The effect of adjunctive light therapy onameliorating breakthrough depressive symptoms in adolescent-onset bipo-lar disorder. J Psychiatry Neurosci. 1995;20:226-232.102. Praschak-Rieder N, Neumeister A, Hesselmann B, Willeit M, Barnas C,Kasper S. Suicidal tendencies as a complication of light therapy for seasonalaffective disorder: a report of three cases. J Clin Psychiatry. 1997;58:389-392.103. Wirz-Justice A, Quinto C, Cajochen C, Werth E, Hock C. A rapid-cyclingbipolar patient treated with long nights, bedrest, and light. Biol Psychiatry.1999;45:1075-1077.104. Colombo C, Lucca A, Benedetti F, Barbini B, Campori E, Smeraldi E. Totalsleep deprivation combined with lithium and light therapy in the treatmentof bipolar depression: replication of main effects and interaction. PsychiatryRes. 2000;95:43-53.105. Parry BL, Rosentahl NE, Tamarkin L, Wehr TA. Treatment of a patientwith seasonal premenstrual syndrome. Am J Psychiatry. 1987;144:762-766.106. Parry BL, Berga SL, Mostofi N, Sependa PA, Kripke DF, Gillin JC. Morningversus evening bright light treatment of late luteal phase dysphoric disor-der. Am J Psychiatry. 1989;146:1215-1217.107. Parry BL, Mahan AM, Mostofi N, Klauber MR, Lew GS, Gillin JC. Lighttherapy of late luteal phase dysphoric disorder: an extended study. Am JPsychiatry. 1993;150:1417-1419.108. Lam RW, Carter D, Misri S, Kuan AJ, Yatham LN, Zis AP. A controlledstudy of light therapy in women with late luteal phase dysphoric disorder.Psychiatry Res. 1999;86:185-192.109. Oren DA, Wisner KL, Spinelli M, et al. An open trial of morning light ther-apy for treatment of antepartum depression. Am J Psychiatry. 2002;159:666-669.110. Corral M, Kuan A, Kostaras D. Bright light therapy’s effect on post-partum depression. Am J Psychiatry. 2000;157:303-304.111. Lewy AJ, Sack RL, Miller S, Hoban TM. Antidepressant and circadianphase-shifting effects of light. Science. 1987;235:352-354.112. Terman JS, Terman M, Lo ES, Cooper TB. Circadian time of morninglight administration and therapeutic response in winter depression. ArchGen Psychiatry. 2001;58:69-75.113. Terman M, Terman JS, Quitkin FM, et al. Response of the melatonincycle to phototherapy for seasonal affective disorder. J Neural Transm.1988;72:147-165.114. Winton F, Corn T, Huson LW, Franey C, Arendt J, Checkley SA. Effectsof light treatment upon mood and melatonin in patients with seasonalaffective disorder. Psychol Med. 1989;19:585-590.115. Danilenko KV, Putilov AA, Russkikh GS, Duffy LK, Ebbesson SOE.Diurnal and seasonal variations of melatonin and serotonin in women withseasonal affective disorder. Arct Med Res. 1994;53:137-145.116. Partonen T. Involvement of melatonin and serotonin in winter depres-sion. Medical Hypotheses. 1994;43:165-166.

Light treatment of mood disorders - Parry and Maurer Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
365
117. Rice J, Mayor J, Tucker A, Bielski RJ. Effect of light therapy on salivarymelatonin in seasonal affective disorder. Psychiatry Res. 1995;56:221-228.118. Thalen BE, Kjellman BF, Morkrid L, Wetterberg L. Melatonin in lighttreatment of patients with seasonal and nonseasonal depression. ActaPsychiatr Scand. 1995;92:274-284.119. Rao ML, Muller-Oerlinghausen BM, Mackert A, Stieglitz RD, Strebel B,Volz HP. The influence of phototherapy on serotonin and melatonin in non-seasonal depression. Pharmacopsychiatry. 1990;23:155-158.120. Rao ML, Muller-Oerlinghausen B, Macker A, Strebel B, Stieglitz RD.Blood serotonin, serum melatonin and light therapy in healthy subjects andin patients with nonseasonal depression. Acta Psychiatr Scand. 1992;86:127-132.121. Mellerup ET, Errebo I, Molin J, Plenge P, Dam H. Platelet paroxetinebinding and light therapy in winter depression. J Affect Disord. 1993;29:11-15.122. Schwartz PJ, Murphy DL, Wehr TA, et al. Effects of meta-chorophenylpiperazine infusions in patients with seasonal affective disor-der and healthy control subjects. Arch Gen Psychiatry. 1997;54:375-385.123. Stain-Malmgren R, Kjellman BF, Aberg-Wistedt A. Platelet serotoner-gic functions and light therapy in seasonal affective disorder. Psychiatry Res.1998;78:163-172.124. Lam RW, Zis AP, Grewal A, Delgado PL, Charney DS, Krystal JH. Effectsof rapid tryptophan depletion in patients with seasonal affective disorderin remission after light therapy. Arch Gen Psychiatry. 1996;53:41-44.125. Neumeister A, Praschak-Rieder P, Hesselmann B, Rao ML, Gluck J,Kasper S. Effects of tryptophan depletion on drug-free patients with sea-sonal affective disorder during a stable response to bright light therapy.Arch Gen Psychiatry. 1997;554:133-138.126. Neumeister A, Turner E, Matthews JR, et al. Effects of tryptophandepletion vs catecholamine depletion in patients with seasonal affectivedisorder in remission with light therapy. Arch Gen Psychiatry. 1998;55:524-530.127. Szadoczky E, Falus A, Arato M, Nemeth A, Teszeri G, Moussong-KovacsE. Phototherapy increases platelet imipramine binding in patients with win-ter depression. J Affect Disord. 1989;16:121-125.128. Szadoczky E, Falus A, Nemeth A, Teszeri G, Moussong-Kovacs E. Effectof phototherapy on 3H-imipramine binding sites in patients with SAD, non-SAD and in healthy controls. J Affect Disord. 1991;22:179-184.129. Anderson JL, Vasile RG, Mooney JJ, Bloomingdale KL, Samson JA,Schildkraut JJ. Changes in norepinephrine output following light therapyfor fall/winter seasonal depression. Biol Psychiatry. 1992;32:700-704.130. Rudorder MV, Skwerer RG, Rosenthal NE. Biogenic amines in seasonalaffective disorder: effects of light therapy. Psychiatry Res. 1993;46:19-28.131. Partonen T. Prolactin in winter depression. Medical Hypotheses.1994;43:163-164.132. Lingjaerde O, Reichborn-Kjennerud T, Haug E. Thyroid function in sea-sonal affective disorder. J Affect Disord. 1995;33:39-45.133. Thalen BE, Morkrid L, Kjellman BF, Wetterberg L. Cortisol in light treat-ment of seasonal and non-seasonal depression: relationship between mela-tonin and cortisol. Acta Psychiatr Scand. 1997;96:385-394.134. Partonen T. A mechanism of action underlying the antidepressanteffect of light. Medical Hypotheses. 1995;45:33-34.135. Yatham LN, Lam RW, Zis AP. Growth hormone response to sumatrip-tan (5-HT1D agonist) challenge in seasonal affective disorder: effects of lighttherapy. Biol Psychiatry. 1997:42:24-29.136. Shiah IS, Robertson HA, Lam RW, Yatham LN, Tam EM, Zis AP. Growthhormone response to baclofen in patients with seasonal affective disorder:effects of light therapy. Psychonueroendocrinology. 1999;24:143-153.137. Oren D. Bilirubin, REM sleep, and phototransduction of environmen-tal time cues. A hypothesis. Chronobiol Int. 1997;14:319-329.138. Oren DA, Desan PH, Boutros N, Anand A, Charney DS. Effects of lighton low nocturnal bilirubin in winter depression: a preliminary report. BiolPsychiatry. 2002;51:422-425.
139. Dietzel M, Saletu B, Lesch OM, Sieghart W, Schjerve M. Light treatmentin depressive illness. Polysomnographic, psychometic and neuroendocrino-logical findings. Eur Neurol Suppl. 1986;25:93-103.140. Partonen T, Appelberg B, Partinen M. Effects of light treatment onsleep structure in seasonal affective disorder. Eur Arch Psychiatry Clin Neurosci.1993;242:310-313.141. Allen JJ, Iacono WG, Depue RA, Arbisi P. Regional electroencephalo-graphic asymmetries in bipolar seasonal affective disorder before and afterexposure to bright light. Biol Psychiatry. 1993;33:642-646.142. Volf NV, Senkova NI, Danilenko KV, Putilov AA. Hemispheric languagelateralization in seasonal affective disorder and light treatment. PsychiatryRes. 1993;47:99-108.143. Brunner DP, Krauchi K, Dijk DJ, Leonhardt G, Haug HJ, Wirz-Justice A.Sleep electroencephalogram in seasonal affective disorder and in controlwomen: effects of midday light treatment and sleep deprivation. BiolPsychiatry. 1996;40:485-496.144. Fritzsche M, Heller R, Hill H, Kick H. Sleep deprivation as a predictor ofresponse to light therapy in major depression. J Affect Disord. 2001; 62:207-215.145. Dilsaver SC. Neurobiologic effects of bright artificial light. Brain Res Rev.1989;14:311-333.146. Rosenthal NE, Levendosky AA, Skwerer RG, et al. Effects of light treat-ment on core body temperature in seasonal affective disorder. Biol Psychiatry.1990;27:39-50.147. Eastman CI, Gallo LC, Lahmeyer HW, Fogg LF. The circadian rhythm oftemperature during light treatment for winter depression. Biol Psychiatry.1993;34:210-220.148. Avery DH, Dahl K, Savage MV, et al. Circadian temperature and corti-sol rhythms during a constant routine are phase-delayed in hypersomnicwinter depression. Biol Psychiatry. 1997;41:1109-1123.149. Schwartz PJ, Rosentahl NE, Turner EH, Drake CL, Liberty V, Wehr TA.Seasonal variation in core temperature regulation during sleep in patientswith winter seasonal affective disorder. Biol Psychiatry. 1997;42:122-131.150. Schwartz PJ, Rosenthal NE, Kajimura N, et al. Ultradian oscillations incranial thermoregulation and electroencephalographic slow-wave activityduring sleep are abnormal in humans with annual winter depression. BrainRes. 2000;866:152-167.151. Seggie J, Canny C, Mai F, McCrank E, Waring E. Antidepressant med-ication reverses increased sensitivity to light in depression: preliminaryreport. Prog Neuropsychopharmacol Biol Psychiatry. 1989;13:537-541.152. Terman S, Terman M. Photic and scotopic light detection in patientswith SAD and control subjects. Biol Psychiatry. 1999;46:1642-1648.153. Lam RW, Buchanan A, Mador JA, Corral MR, Remick RA. The effects ofultraviolet-A wavelengths in light therapy for seasonal depression. J AffectDisord. 1992;24:237-244.154. Lasko TA, Kripke DF, Elliot JA. Melatonin suppression by illuminationof upper and lower visual fields. J Biol Rhythms. 1999;14:122-125.155. Vasile RG, Sachs G, Anderson JL, Lafer B, Matthews E, Hill T. Changesin regional cerebral blood flow following light treatment for seasonal affec-tive disorder: responders versus nonresponders. Biol Psychiatry. 1997;42:1000-1005.156. Rechlin T, Weis M, Schneider K, Zimmermann U, Kaschka WP. Doesbright-light therapy influence autonomic heart-rate parameters? J AffectDisord. 1995;34:131-137.157. Avissar S, Schreiber G, Nechamkin Y, et al. The effects of seasons andlight therapy on G protein levels in mononuclear leukocyctes of patientswith seasonal affective disorder. Arch Gen Psychiatry. 1999;56:178-183.158. Oren DA, Berman RM, Anand A, Charney DS. No effect of light onbasal glucagon levels in winter seasonal depressives and comparison sub-jects. Psychiatry Res. 2000;94:263-266.159. Leu SJ, Shiah IS, Yatham LN, Cheu YM, Lam RW. Immune-inflammatorymarkers in patients with seasonal affective disorder: effects of light ther-apy. J Affect Disord. 2001;63:27-34.

366
Posters & images in neuroscience
Sleep deprivation and antidepressant treatment
The main limitation is the transient nature of the effect,since the majority—but not all—of the improved patientsexperience a relapse after the next night of sleep.2
Despite the rapid effects and low risk of relevant sideeffects (Table I),2-9 the method has remained an “orphandrug” or “orphan method.” This may be explained notonly by the effort and motivation needed by the patient
and by the frequent relapses after the next night of sleep,but also by the lack of funding for nonpharmacologicaland nonneurochemical research. Nevertheless, someprogress has been made within the last few years.A vari-ety of studies have focused on the problem of how toavoid relapses occurring after the next night of sleep andadditionally treated the patients with light therapy,lithium, or other drugs. Lower relapse rates after SDwere found when SD was combined with one of thesetherapeutic options (Table II).10-20
A further strategy has been to advance the sleep periodto an “unphysiological” time. Several uncontrolled stud-ies in small numbers of patients have indicated that thisphase advance procedure per se acts as an antidepres-sant. More recent studies have combined SD with a sub-sequent phase advance of the sleep period, over thecourse of either six or three nights and consistently foundthat a phase advance of the sleep period stabilizes theantidepressant effect of SD in about 60% of thosepatients who responded positively to SD.17-20 Only onestudy also included a control group which participated ina phase-delay protocol after SD instead of a phase-advance protocol.18 Significantly more patients relapsedin the phase-delay protocol compared with the phaseadvance protocol (Figure 1). This indicates that the high
Copyright © 2003 LLS SAS. All rights reserved
The mood-improving effect of sleep deprivation (SD) in depression is even today still not fullyunderstood. Despite the fact that mood and cognitive functions are lowered by prolonged sleeploss and despite convincing data that insomnia is a strong risk factor for subsequent depression,1
acute SD for one night or even partial SD in the second half of the night improves mood inabout 60% of depressed patients the day after.2,3 In this respect, among all types of antidepressanttreatments, SD elicits the fastest results, faster even than electroconvulsive therapy. Many authorscorrelate the likelihood of responding to SD with clinical variables. A summary of predictors islisted in Table I.
Table I. Clinical predictors of an antidepressant response to sleep depri-vation (SD) in depressed subjects and side effects. *Not based onsystematic documentation.
Predictive
• High level of arousal4
• High variability of mood swings5
• Diurnal and day-to-day mood variations6
• “Endogenous” and melancholic subtype2,3
• Bipolar subtype7
Not predictive2,3
• Age
• Sex
• Severity of depression
• Duration of depressive episode
• Duration of illness
• Earlier treatments
• Expectation of patients
Side effects of SD in depression*
• Tiredness, fatigue
• Switch to hypomania or mania in bipolar patients8
• Exacerbation of psychotic symptoms in psychotically
depressed patients9
• Lowering of seizure threshold
Table II. Therapeutic strategies to avoid relapses after successful sleepdeprivation in depression (selected papers).
• Antidepressants (clomipramine)10
• Lithium11-13
• Pindolol14
• Light therapy15,16
• Sleep phase advance over 3 to 6 nights17-20

response rate after SD and phase advance cannot beexplained by a placebo phenomenon alone and supportsthe hypothesis that, in depressed subjects, sleeping at cer-tain phases of the circadian rhythm, ie, especially late inthe night and in the morning, has depressogenic effects.Unfortunately, one major issue has been almost com-pletely neglected by researchers: does SD produce anylasting effects after 4 to 6 weeks, which is the typicalperiod for measuring the effects of antidepressants?There is only one controlled study using such a design.21
Twenty-four patients received amitriptyline without addi-tional SD, whereas 27 patients received amitriptyline plusa series of 6 partial SDs. Observer ratings, but not patientratings, demonstrated superiority of the combined treat-ment after 4 weeks. By the standards of evidence-basedmedicine, there is little evidence to date that SD therapyhas lasting effects over the course of several weeks.
Neurobiology of SD in depression
There is no generally accepted hypothesis concerningthe mechanism of action of SD, nor an explanation forthe observation that subsequent sleep after SD leads torelapses. A variety of neurobiological effects pointtoward potential mechanisms of action of the procedure(Table III).22-32
Based on the observations that hyperarousal and a highlevel of activation predict a favorable SD response,4 theantidepressant effect was explained using the two-processmodel of sleep regulation (Figure 2).33 In this model,depressed patients have a deficiency of process S (ie, sleepneed) with process C (circadian rhythm) remaining unaf-fected. Depression is characterized by a deficient build-upof process S (Figure 2). SD transiently leads to an increasein process S to normal, whereas relapse occurs after“recovery sleep” due to a return to low levels of S.Several brain imaging studies have tried to correlate theSD response with metabolic states of certain brain areas.Two early studies using single photon emission computedtomography (SPECT)22 and positron emission tomogra-phy (PET),23 respectively, found higher metabolic ratesin limbic areas in responders compared with nonrespon-ders.A more recent study24 confirmed these earlier find-ings: responders to SD had higher relative metabolicrates in the ventral anterior cingulate and in the medialprefrontal cortex (Figure 3), as well as in the posteriorsubcallosal gyrus at baseline than depressed patients whodid not respond to SD and normal volunteers.After SD,
significant decreases in metabolic rates occurred in themedial prefrontal cortex and frontal pole in the patientswho responded positively to SD.The brain imaging stud-ies convincingly demonstrated that acute antidepressantSD is able to change metabolic states of brain areas thatare involved in mood regulation.Many studies have assessed endocrine parameters beforeand after SD. The results have been inconsistent, whichmay be partially explained by methodological shortcom-ings. Several authors favor the hypothesis that the hypo-thalamo-pituitary-thyroid (HPT) axis plays a key role inmediating the antidepressant effects of SD.31,32
367
Poster by: Ulrich Voderholzer, MD, PhDDepartment of Psychiatry and Psychotherapy, Klinikum of the Albert-Ludwig-University,Hauptstrasse 5, 79104 Freiburg, Germany([email protected])
www.dialogues-cns.org
Figure 1. Antidepressant effects of total sleep deprivation (TSD) in onenight with a consecutive phase advance of the sleep period(blue circles) in comparison with a phase delay of the sleepperiod (gray circles). In the phase-advance group, the antide-pressant effect of SD (between day 0 and day 1) was stabilizeduntil day 8, whereas in the phase-delay group mood worsenedagain (mood was measured by a short version of the HamiltonDepression Rating Scale [HDRS], containing 6 items). This scaleis suitable for frequent ratings, whereas the 21-item HDRSwould not have been adequate within the study design.18
Advance / delayTSDH
DRS
6-it
em s
cale
0
2
4
6
8
10
12
0 1 2 3 4 5 6 7 8
Delay (n=20)Advance (n=20)
Table III. Neurobiological effects of sleep deprivation. In humans someof the studies were performed in depressed patients, whileother studies were in healthy subjects or in depressed patientsand healthy subjects.
• Decrease in limbic hypermetabolism22-24
• Increase in dopamine turnover25
• Increase in peripheral cytokines26,27
• Increase in cortisol28-30
• Increase in growth hormone secretion (recovery sleep)30
• Increase in thyroid hormones31,32

368
Posters & images in neuroscience
REFERENCES
1. Riemann D, Voderholzer U. Primary insomnia: a risk factor to developdepression? J Affect Disord. 2003;76:247-251.2. Wu JC, Bunney WE. The biological basis of an antidepressant responseto sleep deprivation and relapse: review and hypothesis. Am J Psychiatry.1990;147:14-21.3. Van den Hoofdakker RH. Total sleep deprivation: clinical and theoreti-cal aspects. In: Honig A, van Praag HM, eds. Depression: Neurobiological,Psychopathological and Therapeutic Advances. Chichester, UK: John Wiley &Sons Ltd; 1997:563-589.4. Bouhuys AL, van den Burg W, van den Hoofdakker RH. The relationshipbetween tiredness prior to sleep deprivation and the antidepressant responseto sleep deprivation in depression. Biol Psychiatry. 1995;37:457-461.5. Gordijn MC, Beersma DG, Bouhuys AL, Reinink E, Van den HoofdakkerRH. A longitudinal study of diurnal mood variation in depression; charac-teristics and significance. J Affect Disord. 1994;31:261-273. 6. Reinink E, Bouhuys N, Wirz-Justice A, van den Hoofdakker R. Predictionof the antidepressant response to total sleep deprivation by diurnal vari-ation of mood. Psychiatry Res. 1990;32:113-124.7. Barbini B, Colombo C, Benedetti F, Campori E, Bellodi L, Smeraldi E. Theunipolar-bipolar dichotomy and the response to sleep deprivation.Psychiatry Res. 1998;79:43-50.8. Colombo C, Benedetti F, Barbini B, Campori E, Smeraldi E. Rate of switchfrom depression into mania after therapeutic sleep deprivation in bipolardepression. Psychiatry Res. 1999;86:267-270.9. Benedetti F, Zanardi R, Colombo C, Smeraldi E. Worsening of delusionaldepression after sleep deprivation: case reports. J Psychiatr Res. 1999;33:69-72.10. Elsenga S, van den Hoofdakker RH. Clinical effects of sleep deprivation andclomipramine in endogenous depression. J Psychiatr Res. 1982/83;17:361-74.11. Baxter LR Jr, Liston EH, Schwartz JM, et al. Prolongation of the antide-pressant response to partial sleep deprivation by lithium. Psychiatry Res.1986;19:17-23.12. Grube M, Hartwich P. Maintenance of antidepressant effect of sleepdeprivation with the help of lithium. Eur Arch Psychiat Neurol Sci.1990;240:60-61.
13. Szuba MP, Baxter LR Jr, Altshuler LL, et al. Lithium sustains the acuteantidepressant effects of sleep deprivation: preliminary findings from acontrolled study. Psychiatry Res. 1994;51:283-295.14. Smeraldi E, Benedetti F, Barbini B, Campori E, Colombo C. Sustained anti-depressant effect of sleep deprivation combined with pindolol in bipolar depres-sion. A placebo-controlled trial. Neuropsychopharmacology. 1999;20:380-385.15. Neumeister A, Goessler R, Lucht M, Kapitany T, Bamas C, Kasper S.Bright light therapy stabilizes the antidepressant effect of partial sleepdeprivation. Biol Psychiatry. 1996;39:16-21.16. Colombo C, Lucca A, Benedetti F, Barbini B, Campori E, Smeraldi E. Totalsleep deprivation combined with lithium and light therapy in the treat-ment of bipolar depression: replication of main effects and interaction.Psychiatry Res. 2000;95:43-53.17. Berger M, Vollmann J, Hohagen F, et al. Sleep deprivation combinedwith consecutive sleep phase advance as a fast-acting therapy in depres-sion: an open pilot trial in medicated and unmedicated patients. Am JPsychiatry. 1997;154:870-872.18. Riemann D, König A, Hohagen F, et al. How to preserve the antide-pressant effect of sleep deprivation: a comparison of sleep phase advanceand sleep phase delay. Eur Arch Psychiatry Clin Neurosci. 1999;249:231-237.19. Benedetti F, Barbini B, Campori E, Fulgosi MC, Pontiggia A, Colombo C.Sleep phase advance and lithium to sustain the antidepressant effect oftotal sleep deprivation in bipolar depression: new findings supporting theinternal coincidence model? J Psychiatr Res. 2001;35:323-329.20. Voderholzer U, Valerius G, Schaerer L, et al. Is the antidepressive effectof sleep deprivation stabilized by a three day phase advance of the sleepperiod? A pilot study. Eur Arch Psychiatry Clin Neurosci. 2003;253:68-72.21. Kuhs H, Färber D, Borgstädt S, Mrosek S, Tölle R. Amitriptyline in com-bination with repeated late sleep deprivation versus amitriptyline alonein major depression. A randomised study. J Affect Disord. 1996;37:31-41.22. Ebert D, Feistel H, Barocka A. Effects of sleep deprivation on the lim-bic system and the frontal lobes in affective disorders: a study with Tc-99m-HMPAO SPECT. Psychiatry Res. 1991;40:247-251.23. Wu JC, Gillin JC, Buchsbaum MS, Hershey T, Johnson JC, Bunney WE Jr.Effect of sleep deprivation on brain metabolism of depressed patients. AmJ Psychiatry. 1992;149:538-543.
Another issue is the impact of SD on the hypothalamo-pituitary-adrenal (HPA) axis. Increased activity of thisaxis is one of the most consistent abnormalities in depres-sion and normalization of this hyperactivity is a correlateof clinical remission and has been suggested as the mech-anism of action of antidepressant treatment.34 In healthyhumans, acute SD increases cortisol secretion.28,29 In astudy that we conducted ourselves, we found a significantstimulatory effect of acute SD on nighttime cortisol in agroup of unmedicated depressed subjects, which was notrelated to treatment response.30 However, during the first
Figure 2. Two-process model of sleep deprivation (SD) and depression .This model can explain the antidepressant effect of SD byassuming that an insufficient build-up of process S (S standsfor sleep need), SD transiently increases the level of process S,thus, leading to the antidepressant effect. Recovery sleepdecreases process S to baseline levels leading to relapse intothe depressed state. This model fits well with clinical observa-tions that depressed patients have hyperarousal, which hasbeen shown to be a positive predictor of the SD response.4
Reproduced from reference 33: Borbély AA, Wirz-Justice A. Sleep, sleepdeprivation and depression. Hum Neurobiol. 1982;1:205-210. Copyright© 1982, Springer Verlag.
Clock time
Sleep deprivation
Leve
l of
proc
ess
S
S
6 16 23 4 6 16 23 4 6
C
Clock time
Leve
l of
proc
ess
S
Dec
reas
e in
dep
ress
ive
sym
ptom
s
6 16 23 4 6 16 23 4 6

369
Poster by: Ulrich Voderholzer
In summary, the SD response in depressive patients remains a highly interesting issue for depression research, since, contrary to all antidepressant drugs, it may significantly amelioratemood within one day. Understanding this effect and optimizing the duration of the effect, ie,preventing relapse after the response, might improve our ability to treat depression.
Figure 3. Positron emission tomography (PET) scan of depressed patientswho respond to total sleep deprivation (SD) in one night.24 Atbaseline, responders to SD had higher metabolic rates in theventral anterior cingulate and in the medial prefrontal cortex.The study confirmed earlier findings demonstrating an asso-ciation between high metabolic rates in limbic areas and thelikelihood to respond to SD.22,23
Adapted from reference 24: Wu J, Buchsbaum MS, Gillin JC, et al.Prediction of antidepressant effects of sleep deprivation by metabolicrates in the ventral anterior cingulate and medial prefrontal cortex. AmJ Psychiatry. 1999;156:1149-1158. Copyright © 1999, AmericanPsychiatry Association.
Z :-4.00 mm
6.0
3.0
0.0
-3.0
-6.0
-9.0
cm+6+30-3-6
X
YPercentdifference
+20.00
+13.33
+6.67
±0.00
-6.67
-13.33
-20.00%
half of the day after the night, SD responders in contrastto nonresponders had higher cortisol concentrationscompared with the day before SD.This finding does notnecessarily contradict the above relationship betweendepression and HPA axis hyperactivity for two reasons.First, the acute effects of antidepressant treatments onthe HPA axis may differ from the chronic effects. It hasbeen shown that electroconvulsive treatment and anti-depressants also initially stimulate the HPA axis. Second,two studies demonstrated acute antidepressant effects ofcortisol infusion compared with placebo.35,36
Another theory that possibly provides a link to the HPAeffects of SD focuses on the psychostimulant effects.Earlier studies reported an increase in dopamine, norepi-nephrine, and serotonin after SD, ie, similar neurobiolog-ical effects as after the intake of psychostimulants likeamphetamines (see reference 25 for an overview). Supportfor a psycho-stimulant theory also comes from brain imag-ing data, demonstrating effects of psychostimulants suchas amphetamines on metabolic rates similar to thoseobserved in SD.37 Since there is a functional coupling ofpsychostimulant effects and the HPA axis,38 a cortisolincrease following SD might therefore mediate psychos-timulant-like actions of increased aminergic neurotrans-mitter release.
24. Wu J, Buchsbaum MS, Gillin JC, et al. Prediction of antidepressant effectsof sleep deprivation by metabolic rates in the ventral anterior cingulate andmedial prefrontal cortex. Am J Psychiatry. 1999;156:1149-1158.25. Ebert D, Berger M. Neurobiological similarities in antidepressant sleepdeprivation and psychostimulant use: a psychostimulant theory of antide-pressant sleep deprivation. Psychopharmacology. 1998;40:1-10.26. Dinges DF, Douglas SD, Hamarman S, Zaugg L, Kapoor S. Sleep depriva-tion and human immune function. Adv Neuroimmunol. 1995;5:97-110.27. Voderholzer U, Hohagen F, Herr A, et al. Effects of sleep deprivation oncytokines in healthy and depressed subjects. In: Sperner-Unterweger B,Fleischhacker WW, Kaschka WP, eds. Psychoneuroimmunology. Hypotheses andCurrent Research. Advances in Biological Psychiatry. Basel, Switzerland: Karger;2001;20:98-109.28. Leproult R, Copinschi G, Buxton O, Van-Cauter E. Sleep loss results in anelevation of cortisol levels the next evening. Sleep. 1997;20:865-870.29. Spiegel K, Leproult R, Van-Cauter E. Impact of sleep debt on metabolicand endocrine function. Lancet. 1999;354:1435-1439.30. Voderholzer U, Weske G, Klein T, et al. Endocrine studies during sleep,sleep deprivation, and recovery sleep in depressed patients. Neuropsycho-pharmacology. 2000;23(suppl 2):S82-S83.
31. Parekh PI, Ketter TA, Altshuler L, et al. Relationships between thyroidhormone and antidepressant responses to total sleep deprivation in mooddisorder patients. Biol Psychiatry. 1998;43:392-394.32. Orth DN, Shelton RC, Nicholson WE, et al. Serum thyrotropin concen-trations and bioactivity during sleep deprivation in depression. Arch GenPsychiatry. 2001;58:77-83.33. Borbély AA, Wirz-Justice A. Sleep, sleep deprivation and depression. HumNeurobiol. 1982;1:205-210.34. Holsboer F, Barden N. Antidepressants and hypothalamic-pituitary-adrenocortical regulation. Endocr Rev. 1996;17:187-205.35. Goodwin GM, Muir WJ, Seckl JR, et al. The effects of cortisol infusionupon hormone secretion from the anterior pituitary and subjective moodin depressive illness and in controls. J Affect Disord. 1992;26:73-83.36. DeBattista C, Posener JA, Kalehzan BM, Schatzberg AF. Acute antidepres-sant effects of intravenous hydrocortisone and CRH in depressed patients: adouble-blind, placebo-controlled study. Am J Psychiatry. 2000;157:1334-1337. 37. Volkow ND, Wang GJ, Fowler JS, et al. Gender differences in cerebel-lar metabolism: text-retest reproducibility. Am J Psychiatry. 1997;154:50-55.38. Marinelli M, Rouge-Pont F, Deroche V, et al. Glucocorticoids and behav-ioral effects of psychostimulants. I: Locomotor response to cocaine dependson basal levels of glucocorticoids. J Pharmacol Exp Ther. 1997;281:1392-1400.


371
orty million Americans are afflicted with chronicdisorders of sleep and wakefulness, which interfere withwork, driving, and social activities. Sleep disorders cause38 000 cardiovascular deaths and cost over $16 billionannually.1 Indirect costs of accidents, property destruc-tion, litigation, hospitalization, and death add another $50to $100 billion.1 The most common sleep disordersinclude insomnia, sleep apnea, restless legs syndrome,and narcolepsy.1-3
Classification of sleep disorders
The International Classification of Sleep Disorders diag-nostic and coding manual 2000 lists four major categoriesof sleep disorders: dyssomnias; parasomnias; sleep disor-ders associated with mental, neurologic, or other medicaldisorders; and proposed sleep disorders (Table I).4-7
Dyssomnias are disorders characterized by either exces-sive sleepiness or difficulty initiating or maintaining sleep.4
On the basis of pathophysiological mechanisms, they canbe subdivided into intrinsic, extrinsic, and circadianrhythm sleep disorders.4-9 Intrinsic sleep disorders are dis-orders that originate or develop within the body or thatarise from causes within the body. Common intrinsic sleepdisorders include idiopathic and psychophysiologicalinsomnia, narcolepsy, obstructive sleep apnea syndrome(OSAS), periodic limb movement disorder (PLMD), andrestless legs syndrome (RLS).4-7 Sleep disorders caused byexternal factors are termed extrinsic sleep disorders andinclude inadequate sleep hygiene, environmental sleepdisorder, adjustment sleep disorder, insufficient sleep syn-drome, limit-setting sleep disorder, sleep-onset association
C l i n i c a l r e s e a r c h
Keywords: diagnosis; treatment; sleep disorder; insomnia; circadian rhythmdisorder; excessive somnolence; parasomnia
Author affiliations: Stanford University Sleep Disorders Clinic and ResearchCenter, Stanford University, School of Medicine, Stanford, Calif, USA
Address for correspondence: Christian Guilleminault, MD, Professor ofPsychiatry and Behavioral Sciences and Director of Training, Stanford SleepDisorders Center, 401 Quarry Road, Suite 3301, Stanford, CA 94305, USA(e-mail: [email protected])
F
Copyright © 2003 LLS SAS. All rights reserved www.dialogues-cns.org
Diagnosis and treatment of sleep disorders:a brief review for cliniciansVivien C. Abad, MD, MBA; Christian Guilleminault, MD
Sleep disorders encompass a wide spectrum of diseaseswith significant individual health consequences and higheconomic costs to society. To facilitate the diagnosis andtreatment of sleep disorders, this review provides aframework using the International Classification of SleepDisorders. Primary and secondary insomnia are differen-tiated, and pharmacological and nonpharmacologicaltreatments are discussed. Common circadian rhythm dis-orders are described in conjunction with interventions,including chronotherapy and light therapy. The diagno-sis and treatment of restless legs syndrome/periodic limbmovement disorder is addressed. Attention is focused onobstructive sleep apnea and upper airway resistance syn-drome, and their treatment. The constellation of symp-toms and findings in narcolepsy are reviewed togetherwith diagnostic testing and therapy. Parasomnias, includ-ing sleep terrors, somnambulism, and rapid eye move-ment (REM) behavior sleep disorders are described,together with associated laboratory testing results andtreatment.© 2003, LLS SAS Dialogues Clin Neurosci. 2003;5:371-388.

disorder, and hypnotic-, stimulant-, or alcohol-dependentsleep disorder.4-7 Circadian rhythm sleep disorders sharea common chronophysiological basis whereby there is adiscordance between the patient’s sleep pattern and thedesired or societal sleep norm.4-9 Examples of circadianrhythm sleep disorders include shift work sleep disorder,delayed sleep phase syndrome, and advanced sleep phasesyndrome.Parasomnias are characterized by undesirable behavioraland physical phenomena that occur predominantly dur-ing sleep.4-7 They include disorders of arousal, partialarousal, and sleep-stage transition.Sleep disorders can also be associated with mental dis-orders, such as psychoses, mood disorders, anxiety disor-ders, panic disorders, and alcoholism. Neurological con-ditions associated with sleep disorders include cerebraldegenerative disorders, dementia, parkinsonism, fatalfamilial insomnia, sleep-related epilepsy, electrical statusepilepticus of sleep, and sleep-related headaches.4,10 Sleepdisorders can occur with medical disorders, such as sleep-ing sickness, nocturnal cardiac ischemia, chronic obstruc-tive pulmonary disease, sleep-related asthma, sleep-related gastroesophageal reflux, peptic ulcer disease,irritable bowel syndrome and fibromyalgia.4,11-14
Proposed sleep disorders include short sleeper, longsleeper, subwakefulness syndrome, fragmentary myo-clonus, sleep hyperhidrosis, menstrual-associated sleepdisorder, pregnancy-associated sleep disorder, terrifyinghypnagogic hallucinations, sleep-related neurogenictachypnea, sleep-related laryngospasm, and sleep chok-ing syndrome.4
Approach to sleep disorders
History and physical examination
An accurate and detailed history from the patient, bedpartner, or family member combined with a sleep ques-tionnaire can elicit critical information. Most sleep com-plaints fall into three categories: insomnia (sleep onset,maintenance, or early morning awakening); excessivesleepiness; or abnormal behaviors during sleep.The pro-cedure is as follows.• Inquire into the chief complaint, when symptom(s)
started, the pattern since onset, and associated factors(medical, environmental, occupational, psychologi-cal/stress, lifestyle choices) that may have predisposedto or precipitated the illness, perpetuated the condi-tion, and improved or worsened symptoms.7
• Assess the impact of the sleep complaint on thepatient’s life, and inquire about meal and sleep sched-ules, sleep hygiene, restless legs sensation, snoring, wit-nessed apneic episodes, sweating, coughing, gasping/choking/snorting, dryness of the mouth, bruxism,excessive movements during sleep, periodic limbmovements, any abnormal behaviors during sleep, day-time sleepiness, presence of cataplexy, sleep paralysis,and hypnagogic or hypnapompic hallucinations.
• Ask about caffeine intake, alcohol and nicotine use, aswell as use of illicit drugs.
• Review the pertinent medical/surgical/psychiatric his-tory and past treatments, and their efficacy or lackthereof.
• Determine if there is any family history of sleep disor-ders (snoring, OSAS, narcolepsy, RLS).
A completed 2-week sleep log or sleep diary can be uti-lized to compute sleep efficiency, total sleep time, andnumber of awakenings during the night, and can be usedto diagnose sleep disorders and monitor efficacy of treat-ment. On the basis of the information from question-naires and sleep diary, the chief complaint, and the his-tory, a working diagnosis is outlined.
C l i n i c a l r e s e a r c h
372
Selected abbreviations and acronymsAHI apnea-hypopnea indexBIPAP bilevel positive airway pressureCPAP continuous positive airway pressureEDS excessive daytime somnolenceEMG electromyogramEOG electro-oculogramMSLT mean sleep latency testMWT maintenance of wakefulness testNPT nocturnal penile tumescenceNREM non–rapid eye movementOSAS obstructive sleep apnea syndromePLMD periodic limb movement disorderPMR progressive muscle relaxationPSG polysomnogramRBD REM behavior sleep disorderRDI respiratory disturbance indexREM rapid eye movementRLS restless legs syndromeSOL sleep-onset latencySWS slow-wave sleepUARS upper airway resistance syndromeWASO wake after sleep onset

Diagnosis and treatment of sleep disorders - Abad and Guilleminault Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
373
Dyssomnias Parasomnias Sleep disorders associated with Proposed sleep disordersmental,neurological, or other
medical disorders
• Intrinsic sleep disorders- Psychophysiological insomnia- Sleep state misperception- Idiopathic insomnia- Narcolepsy- Recurrent hypersomnia- Idiopathic hypersomnia- Posttraumatic hypersomnia- Central alveolar hypo-ventilation syndrome
- Periodic limb movement disorder
- Restless legs syndrome- Intrinsic sleep disorder NOS
• Extrinsic sleep disorders- Inadequate sleep hygiene - Environmental sleep disorder- Altitude insomnia- Adjustment sleep disorder- Insufficient sleep syndrome- Limit-setting sleep disorder- Sleep-onset association disorder
- Food allergy insomnia- Nocturnal eating (drinking)syndrome
- Hypnotic-dependent sleepdisorder
- Stimulant-dependent sleepdisorder
- Toxin-induced sleep disorder- Extrinsic sleep disorder NOS
• Circadian rhythm sleep disorders
- Jet lag syndrome- Shift work sleep disorder- Irregular sleep-wake pattern- Delayed sleep-phase syndrome
- Advanced sleep-phase syndrome
- Non–24-h sleep-wake disorder
- Circadian rhythm sleep disorder NOS
• Arousal disorders- Confusional arousals- Sleepwalking- Sleep terrors
• Sleep-wake transition disorders
- Rhythmic starts- Sleep starts- Sleep talking- Nocturnal leg cramps
• Parasomnias usually associated with REM sleep
- Nightmares- Sleep paralysis- Impaired sleep-related penileerections
- REM sleep-related sinusarrest
- REM sleep behavior disorder
• Other parasomnias- Sleep bruxism- Sleep enuresis- Sleep-related abnormal swallowing syndrome
- Nocturnal paroxysmal dystonia
- Sudden unexplained nocturnal death syndrome
- Primary snoring- Infant sleep apnea- Congenital central hypo-ventilation syndrome
- Sudden infant death syndrome
- Benign neonatal sleepmyoclonus
- Other parasomnias NOS
• Associated with mental dis-orders
- Psychoses- Mood disorders- Anxiety disorders- Panic disorders- Alcoholism
• Associated with neurologicaldisorders
- Cerebral degenerative disorders
- Dementia- Parkinsonism- Fatal familial insomnia- Sleep-related epilepsy- Electrical status epilepticus ofsleep
- Sleep-related headaches
• Associated with other medical disorders
- Chronic obstructive pulmonary disease
- Sleep-related asthma- Sleep-related gastroesopha-geal reflux
- Peptic ulcer disease- Fibromyalgia
- Short sleeper- Long sleeper- Subwakefulness syndrome- Fragmentary myoclonus- Sleep hyperhidrosis- Menstrual-associated sleepdisorder
- Pregnancy-associated sleepdisorder
- Terrifying hypnagogic hallucinations
- Sleep-related neurogenictachypnea
- Sleep-related laryngospasm- Sleep-choking syndrome
Table I. Classification of sleep disorders.4 NOS, not otherwise specified; REM, rapid eye movement.

Laboratory studies
Laboratory tests that are performed to assess and there-fore treat sleep disorders include the polysomnogram(PSG), multiple sleep latency test (MSLT), maintenance ofwakefulness test (MWT), actigraphy, video-PSG, noctur-nal penile tumescence monitoring (NPT), and electroen-cephalography (EEG), including 24-h ambulatory EEG.PSG is a complete, nocturnal, laboratory-based monitor-ing, which simultaneously records numerous variables dur-ing sleep. It includes sleep staging (EEG), electro-oculo-gram (EOG), submental electromyogram (EMG), nasalor oral airflow, respiratory effort, oximetry, electrocardio-gram (ECG), anterior tibialis EMG, and position moni-toring. Depending upon the clinical diagnosis, additionalparameters may be added: transcutaneous CO2 monitor-ing or end-tidal gas analysis; extremity muscle activity;motor activity movement; extended video-EEG; peniletumescence; esophageal pressure; gastroesophageal reflux;snoring; and continuous blood pressure recording.15-17
Modified forms of PSG include daytime nap PSG, split-night studies, and portable recording studies.18-21 DaytimePSG is reported to have a high negative predictive value(95% when the apnea-hypopnea index [AHI] ≥10) forOSAS, but results are inconsistent.18 Split-night studiesmay save time and money, but it is still controversialwhether diagnosis and treatment are adequately estab-lished.21,22 The American Academy of Sleep Medicine(AASM) has formulated guidelines for the use of PSGs,split-night studies, and portable recordings.15,16,19
The MSLT is used to confirm the diagnosis of narcolepsy;to assess complaints of moderate to severe sleepiness inpatients with mild to moderate OSAS, idiopathic hyper-somnia, PLMD, some circadian rhythm disorders, andunknown causes of excessive sleepiness; to evaluate thecomplaint of insomnia when moderate to severe exces-sive daytime sleepiness is suspected; and to assessresponse to treatment following therapy for disorders thatcause sleepiness when an additional sleep disorder thatproduces sleepiness is suspected.23,24 The MWT is used lesscommonly than the MSLT mainly to assess improvedalertness following therapeutic interventions.23-25
Actigraphy uses a small portable device that senses phys-ical motion and stores the resulting information.Actigraphic studies need to be conducted for a minimumof three consecutive 24-h periods.26,27 The AASM Standardsof Practice Committee recently updated practice parame-ters which state that actigraphy is not indicated for the rou-
tine diagnosis, assessment of severity, or management ofany of the sleep disorders.28 However, it may be a usefuladjunct that provides objective demonstration of multidayrest/activity patterns, which can be used to assist in thediagnosis, treatment, and/or assessment of treatmenteffects in various sleep disorders, including insomnia, cir-cadian rhythm disorders, RLS/PLMD, and disorders ofexcessive sleepiness.26
Video-PSG may be helpful in the diagnosis of patientswith arousal disorders or other sleep disruptions that arebelieved to be seizure-related.15,16 NPT for sleep-relatederections (SRE) is an adjunct in the diagnosis of impo-tence.29 It usually requires 2 nights of PSG, although 1night is sufficient if SRE is normal.Twenty-four hours ofEEG is monitored for patients with suspected epilepsy.
Description of common sleep disorders
It is beyond the scope of this review to describe the entiregamut of sleep disorders. We will focus on the followingcommon or severe sleep disorders: insomnia, circadianrhythm disorders, disorders of excessive somnolence (sleepapnea, narcolepsy, RLS/PLMD), and parasomnias.
Insomnia
Insomnia refers to almost nightly complaints of insuffi-cient amounts of sleep or not feeling rested after thehabitual sleep episode. As the most common sleep-wake–related disorder, it is more common in women andhas a prevalence ranging from 10% to 30%.2,3 It can beclassified based on severity (mild, moderate, severe) orduration (acute, subacute, chronic).4 Transient insomniacan occur in adjustment sleep disorders triggered byacute stress, travel, or sleeping in an unfamiliar environ-ment.7 Symptoms usually resolve once the stress isreduced or removed, or the individual’s adaptation to thestressor increases. For transient insomnia, treatment con-sists of education and advice about healthy sleep prac-tices. If these are insufficient, short-term treatment withhypnotics can be undertaken.Chronic insomnia may be primary, or secondary to cir-cadian rhythm, environmental, behavioral, medical, neu-rological, and psychiatric disorders. Vgontzas et al andRodenback and Hajak reported nyctohemeral activationof the hypothalamic-pituitary-adrenal axis (HPA) inpatients with chronic insomnia consistent with thearousal theory of insomnia.30,31 Vgontzas et al demon-
C l i n i c a l r e s e a r c h
374

strated a shift in interleukin-6 (IL-6) and tumor necrosisfactor (TNF) secretion from nighttime to daytime inchronic insomniacs, and postulated that these couldexplain the daytime fatigue and performance decrementsassociated with insomnia.32,33
The diagnosis of primary insomnia requires exclusion ofthe direct physiological effects of a substance or generalmedical condition. It does not occur exclusively during thecourse of a mental disorder or other sleep disorder.Among the primary insomnias, idiopathic insomnia rep-resents a lifelong sleep disturbance associated with reduc-tion in daytime alertness and performance, increased sleeplatency, and decreased sleep efficiency on PSG.4 Other pri-mary insomnias include psychophysiological insomnia andsleep-state misperception. Psychophysiological insomniarefers to maladaptive sleep-preventing behaviors, whichperpetuate the sleep disturbance.Typically, these patientssleep better in any place other than their own bedroom.PSG shows increased sleep latency, increased number ofawakenings, and poor sleep efficiency. Sleep-state misper-ception refers to complaints of sleep difficulties with noPSG evidence of significant sleep disturbance; the sleeplatency, quality, and architecture are normal. Inadequatesleep hygiene and behavioral disorders can also producechronic insomnia.4 Limit-setting disorder occurs in 5% to10% of children and is characterized by refusal to go tosleep when asked to do so and delaying bedtime; the PSGis normal.4,7
Secondary insomnia can result from medical, neurolog-ical, environmental, drugs, or psychiatric causes. Medicalcauses include pain, thyroid disease, acid reflux, coronaryartery disease, pulmonary disease (chronic obstructivepulmonary disease, asthma, sleep apnea, central alveolarhypoventilation syndrome), chronic renal insufficiency,eating disorders, thyroid dysfunction, fibromyalgia,menstrual-associated sleep disorder, and pregnancy.34-36
Neurological causes of insomnia include headaches,Parkinson’s disease, and sleep-related movement disor-ders (nocturnal myoclonus, RLS). Environmental sleepdisorders can be triggered by excessive noise, noxiousodors, bright light, or extremes of ambient temperature.Alcohol-, hypnotic-, and stimulant-dependent sleep dis-orders also contribute to chronic insomnia.Psychiatric disorders are characterized by sleep-onset dif-ficulties, frequent arousals, sleep fragmentation, shortenedtotal sleep time, and decreased sleep efficiency.These dis-orders include alcoholism, anxiety disorders, mood disor-ders, panic disorders, and psychoses. Preliminary data indi-
cate that chronic insomnia may precede depressiveepisodes by several years, and the question of systematictreatment of chronic insomnia as a means of avoidingdepression is being studied. Stressful life events can pre-cipitate chronic insomnia in predisposed individuals withneurotic depression, rumination, chronic anxiety, inhibi-tion of emotions, and inability to express anger.36 PSG inanxiety disorders shows increased sleep latency, decreasedrapid eye movement (REM) sleep, and reduced sleep effi-ciency, while PSG in mood disorders demonstrates fre-quent arousals and awakenings, decreased slow-wavesleep (SWS), decreased REM latency, increased firstREM period duration, and increased REM density.34
Insomnia assessment tools can utilize self-reporting meth-ods (sleep diary and Pittsburgh Sleep Quality Index) andobjective methods include actigraphy and PSG.26,37
Treatment for insomnia can be categorized into pharma-cological and nonpharmacological treatments. Pharma-cological strategies must achieve a balance between hyp-notic and adverse effects. Hypnotics are indicated inpsychophysiological insomnia for occasional intermittentuse or short-term (2 weeks) administration. Benzo-diazepine usage can result in impaired sleep quality, resid-ual sedation, memory or functional impairment the dayfollowing drug administration, or rebound insomnia.Other problems may include increased rates of falls,drowsiness, dizziness, cognitive impairment, and automo-bile accidents.35,38-40 Nonbenzodiazepine hypnotics, type Iselective γ-aminobutyric acid (GABA) receptor agents,such as zolpidem (t1/2=2.4 h), zopiclone (t1/2=5 h), and zale-plon (t1/2=1 h), have hypnosedative action similar to thebenzodiazepines and interact preferentially with ω1 recep-tors.41 Nonbenzodiazepines preserve psychomotor tasksand memory capacities better than benzodiazepines anddo not possess respiratory depressive side effects.35 Petitand colleagues suggest that pharmacological therapy belimited to 4 weeks.35
Nonpharmacological treatments for chronic insomniainclude stimulus control therapy, sleep restriction, sleephygiene education, cognitive therapy, paradoxical inten-tion, relaxation therapy and multicomponent ther-apy.34,35,42-48 Stimulus control therapy is based on thepremise that insomnia is a conditioned response to tem-poral (bedtime) and environmental (bed/bedroom cues)that are typically associated with sleep.34 Interventionsresult in reduction of sleep-onset latency (SOL) andwake after sleep onset (WASO) to 30 min or less, withtotal sleep time increased by 30 to 40 min.
Diagnosis and treatment of sleep disorders - Abad and Guilleminault Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
375

Sleep restriction creates a mild state of sleep deprivation,decreases sleep latency, and promotes more efficientsleep, with less internight variability.34 Interventions cur-tail the amount of time spent in bed to match sleep effi-ciency as determined through sleep diaries or actigraphy,with a caveat of a minimum of 5 h in bed. Adjustmentsare made weekly until optimal sleep duration is achieved.Sleep hygiene education promotes better sleep throughawareness of environmental factors (light, noise, temper-ature, and mattress) and health practices (diet, exercise,and substance use) that may be beneficial or detrimentalto sleep. Poor sleep hygiene complicates insomnia and hin-ders progress in therapy. Guilleminault et al reported sta-tistically significant improvement at the end of 4 weeks ininsomnia patients treated with sleep hygiene and lighttreatment.48
Cognitive therapy identifies patient-specific dysfunctionalsleep cognition, challenges their validity, and replaces themwith more adaptive substitutes using attention shifting,decatastrophizing, reappraisal, reattribution testing, andhypotheses testing.34,37,42,44,46
Paradoxical intention is a form of cognitive restructuringto alleviate performance anxiety and is based on thepremise that performance anxiety hinders sleep onset.34
It is a method that consists of persuading a patient toengage in his most feared behavior, ie, staying awake.Relaxation treatments include progressive muscle relax-ation (PMR), imagery training, meditation, and biofeed-back. Meta-analyses of PMR trials have demonstratedreduced SOL and WASO by an average of 20 to 30 minfrom baseline to posttreatment with equivalent increasesin total sleep time in addition to enhanced perception ofsleep quality.34,35 Studies on imagery training haveyielded variable results.34,35 Three studies on meditationdemonstrated significant improvements in SOL orWASO.34 Biofeedback training reduced SOL withimprovement rates similar to those obtained with stan-dard relaxation procedures.35 Various nonpharmacolog-ical treatments may be combined as multicomponenttherapy. Table II lists a combination of interventionsderived from stimulus control therapy, sleep restrictiontherapy, sleep hygiene, and light therapy.
C l i n i c a l r e s e a r c h
376
Table II. Multicomponent therapy instructions.
Reduce and limit intake of caffeine, tobacco, and other stimulants to the earlier part of the day. Discontinue nicotine and caf-
feine at least 4 to 6 h before bedtime
Avoid alcohol as a sleeping aid
Regularize sleep-wake schedule, meal times, and exercise time
Exercise daily, but not closer than 3 h before bedtime
If racing thoughts predominate during bedtime, set aside 15- to 20-min “worry time” earlier during the day. Use this to think
about or list worries, problems, concerns, etc
Avoid work-related or strenuous activities close to bedtime
Engage in relaxing, pleasant activities 1 to 2 h before bedtime to “wind down” from the stresses of the day. Focus on positive
thoughts at bedtime
Minimize noise, light, and excessive temperature during sleep. If needed, use earplugs, eye shades, or an electric blanket/air
conditioner
Go to bed only when sleepy
If sleep restriction is chosen as a treatment option, determine average estimated sleep time. Restrict the time in bed to the
average estimated sleep time and continue with the weekly sleep diary. Using the sleep diary, determine the sleep efficiency
(total sleep time/time in bed x100%) each week. Increase time in bed by 15 to 20 min when sleep efficiency >90%. Decrease
time in bed by 15 to 20 min when sleep efficiency <80%. Maintain time in bed if sleep efficiency is 80% to 90%. Adjust the time
in bed each week until the ideal sleep duration is obtained. The minimum time in bed is 5 h per night
Use the bedroom only for sleep and sex. Do not read or watch TV in bed
Get out of bed and go into another room when unable to fall asleep or return to sleep within 15 to 20 min. When out of bed,
engage in relaxing and pleasant activities in a dimly lit room. Return to bed only when sleepy again. If still unable to sleep,
repeat the same instructions
Maintain a regular arising time in the morning regardless of how much or how little sleep you got during the prior nights.
Expose yourself to outdoor light for 30 min within 15 min of arising
Avoid daytime napping unless there are safety issues. If so, take a short early afternoon nap (less than 1 h)

Circadian rhythm disorders
Delayed and advanced sleep phase disorders
Disorders of circadian sleep-wake rhythms can presentwith complaints of chronic insomnia as well as excessivedaytime somnolence.4,7,49-54 Delayed sleep phase syndromesufferers report inability to fall asleep until the early morn-ing hours and difficulty arising until late morning or earlyafternoon; sleep is normal after onset. PSG shows delayedsleep latency if the sufferer sleeps at the desired bedtimerather than the usual bedtime. In contrast, advanced sleepphase syndrome sufferers complain of severe inability todelay their bedtime (usually between 6 PM to 9 PM) andsubsequent awakening earlier than desired (often between1 AM to 3 AM).4,7,49,54 PSG performed at the person’s desiredbedtime reveals shortened sleep latency and early morn-ing awakening.Patients with delayed and advanced sleep phase insomniacan be treated with proper timing of bright light andbehavioral changes.4,7,49 The goal of light therapy is toentrain the endogenous sleep-wake rhythm to coincidewith the patient’s social and occupational schedule.Melatonin administration can be utilized to entrain free-running circadian rhythms and may be helpful in blindsubjects.51
For delayed sleep phase syndrome patients, Dahl utilizeschronotherapy with cognitive behavioral therapy toadvance the sleep phase, employing successive 3-h delaysin bedtime for 6 days.47 To minimize school or work dis-ruption, he prefers to start on a Thursday (Table III).To phase delay the circadian clock for advanced sleepphase syndrome patients, combine bright light exposure(10 000 lux for 30-45 min) between 7 and 9 PM togetherwith a 15-min delay in bedtime every few days.7 Once thedesired schedule is achieved for either phase delay orphase advance, it is crucial to lock in the wake-up time to
maintain a stable sleep-wake rhythm.The benefit of lighttherapy is dependent upon the magnitude of light inten-sity and exposure time. Either natural outdoors light ora light box (10 000 lux) or light visor (3000-5000 lux) canbe utilized, with minimum exposure of at least 30 min.
Shift work sleep disorder
Shift work sleep disorder sufferers complain of difficultyinitiating or maintaining sleep or poor quality sleep orexcessive sleepiness that is temporally related to a workperiod that occurs during the habitual sleep phase.4,7,55
These patients are chronically fatigued and have anincreased incidence of accidents at work. Shift workershave a higher incidence of chronic depression, emotionalproblems, family life dysfunction, excessive drug andalcohol use, ulcers, and myocardial infarction comparedto the general population. Disturbances in circadianrhythms with internal desynchrony secondary to workshift time changes or sleep loss are postulated to causethis disorder. PSG shows increased sleep latency, numer-ous arousals during sleep, and early awakening, as well assleep efficiency below 85%.4,7
A twofold approach to shift work problems involvestreatment directed individually toward the patient, inaddition to attempts to encourage the workplace(through occupational medicine and workers compensa-tion programs) to adapt to the worker’s needs andreduce the overall incidence of shift work–related sleepdisorders.55-60 Treatment recommendations include thefollowing: maintain a regular sleep and meal schedule;take naps to limit sleep loss; and practice good sleephygiene. If sleep is necessary during daylight hours, opti-mize sleep by darkening the room and screening fornoise and interruptions. Light environment is impor-tant—exposure to bright light during the first portion ofthe shift and protection from bright light after work (sun-
Diagnosis and treatment of sleep disorders - Abad and Guilleminault Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
377
Table III. Chronotherapy instructions to advance sleep phase.47
Patient takes responsibility for the success of the treatment and reorganizes habits and associations to improve sleep hygiene.
Cognitive behavioral therapy focuses on positive thoughts at bedtime
For adolescents, behavioral contract with parents/guardian specifies rewards and consequences
One-week induction phase. Stay up the whole night on Wednesday. Bedtime schedules are as follows: Thursday 6 AM to 3 AM,
Friday 9 AM to 5 AM, Saturday 12 noon to 8 AM, Sunday 3 AM to 12 midnight, Monday 6 AM to 2 AM, Tuesday and thereafter 9 AM to
6 AM. Stay in bed between 8.5 and 9 h
Maintenance phase. Adhere to the schedule rigidly for at least 1 month. After this, allow minor changes during the weekend
(wake-up time is still within 2 h of school or work time). Only permit one late night on the weekend, but impose strict wakeup
within 2 h of school or work time. No napping is allowed

glasses) and before sleep may be beneficial. Short–half-life hypnotics can be used by those who only occasion-ally work shifts to help initiate sleep; chronic hypnoticuse by long-term shift workers is not encouraged.7,55
Disorders of excessive somnolence
Sleep apnea, hypopnea, and upper airway resistance syndrome
Apnea is defined as cessation in airflow for longer than10 s. Hypopnea refers to an abnormal respiratory eventlasting longer than 10 s associated with at least a 30%reduction in thoracoabdominal movement or airflowcompared to baseline, associated with ≥4% oxygen desat-uration.61 Figure 1 demonstrates hypopneas seen duringPSG monitoring of a patient with sleep apnea. Apneasand hypopneas are combined to form the AHI (ratio of
total apneas and hypopneas to the total sleep time inhours), also known as respiratory disturbance index(RDI). An AHI>5 in an adult is abnormal. Apneas andhypopneas can result from upper airway obstruction(obstructive), loss of ventilatory effort (central), or a mix-ture of both (mixed). OSAS is characterized by repetitiveepisodes of upper airway obstruction that occur duringsleep, usually associated with oxygen desaturation.4 Theclinical features of OSAS are listed in Table IV. Somepatients have increased upper airway resistance withoutobserved apneas or hypopneas and exhibit increased res-piratory effort with Pes (esophageal pressure) crescendosand Pes reversals. Guilleminault et al described the upperairway resistance syndrome (UARS) in patients who hadPes-documented increased respiratory effort associatedwith increased arousals and daytime sleepiness.62-64
Sleep-disordered breathing (OSAS and UARS) in chil-dren peaks between ages 2 to 5 with a second peak in
C l i n i c a l r e s e a r c h
378
Figure 1. Hypopnea in a patient with obstructive sleep apnea syndrome. Note the low amplitude signals seen in the nasal cannula and airflow chan-nels with increasing effort demonstrated on the chest and abdominal (Abd) channels. The Pes (esophageal pressure [PES]) channel showscrescendo increases in esophageal pressure with reversal.
C3-A2
O1-A2
EMG
ROC-A1
LOC-A2
URAT
EKG
MIC
SpO2
Cannula
Airflow
Chest
Abd
PES
+100
+60
+80
-20-25-30-35

Diagnosis and treatment of sleep disorders - Abad and Guilleminault Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
379
middle to late adolescence. Continuous snoring, failureto thrive, mouth breathing, enlarged tonsils and adenoids,and predominance of hypopneas rather than apneas arecommon features in childhood OSAS.62,65-68 Children withsleep-disordered breathing have a threefold increase inbehavioral and neurocognitive abnormalities. It has beenestimated that 5% to 39% of attention-deficit/hyperac-tivity disorder (ADHD) could be attributed to sleep-dis-ordered breathing.65-69
In OSAS, the PSG demonstrates more than five obstruc-tive apneas per hour of sleep and one or more of the fol-lowing: frequent arousals associated with the apneas;bradytachycardia; and arterial oxygen desaturation inassociation with the apneas. Sleep architecture in OSASand UARS patients is abnormal with fragmented sleep(mainly during non–rapid eye movement [NREM] stagesI and II) and frequent arousals and awakenings. Theamount of SWS (NREM stages III and IV) and REMsleep is decreased.4,7 MSLT performed the day after thePSG may or may not demonstrate sleepiness (ie, meansleep latency <10 min).Treatment for OSAS consists of nonsurgical as well assurgical treatments. Nonsurgical treatment encompassesgeneral/behavioral measures, such as weight loss, bodyposition during sleep (avoid supine position), andmechanical measures, which include continuous positiveairway pressure (CPAP) or bilevel positive airway pres-sure (BIPAP) and oral appliances.A consensus statement by Loube and colleagues recom-mended CPAP treatment for all OSAS patients withRDI≥30 regardless of symptoms and for patients withRDI=5 or 30 events per hour if accompanied by symp-toms of excessive daytime somnolence, impaired cogni-
tion, mood disorders, insomnia, or documented cardio-vascular diseases (ischemic heart disease, hypertension),or stroke.70 Improvement or elimination of apneasimproves sleep architecture and reduces daytime sleepi-ness.71,72 Beneficial effects of CPAP or surgery reportedin patients with frequent sleep apneas (>20) and patientswith sleep-disordered breathing (RDI<20) without sub-jective pathological sleepiness include improvement inwell-being, mood, functional status, breathing, oxygen sat-uration, and cardiac rhythm.71-76 CPAP has also been suc-cessfully utilized to treat OSAS in infants and childrenyounger than 2 years of age.77,78 However, compliancewith CPAP is problematic, with published rates rangingfrom 65% to 95% when assessed subjectively.79-87 Strolloand colleagues have recommended management strate-gies for common side effects of nasal CPAP.80
Autotitrating continuous positive airway pressure(APAP) can be used to treat many patients with OSASor to identify an effective optimal fixed level of CPAP fortreatment, but is not recommended for patients with con-gestive heart failure, chronic obstructive pulmonary dis-ease, daytime hypoxemia and respiratory failure fromany cause, or prominent nocturnal desaturation otherthan from OSAS.88,89 Indications for BIPAP include intol-erance of CPAP, development of central apneas resultingin sleep fragmentation, mask leaks at a high CPAP pres-sure, and persistent alveolar hypoventilation.80 Patientswith OSAS on CPAP or BIPAP should be reevaluated atregular intervals to assess compliance, address problems,and reinforce the importance of continued treatment.Surgery is indicated for OSAS patients who have anunderlying specific surgically correctable abnormalitythat is causing sleep apnea and may be indicated in
Cardinal symptoms Other symptoms Physical examination findings
- Excessive sleepiness or insomnia- Frequent episodes of obstructed breathing during sleep
- Loud snoring- Morning headaches- Dryness of the mouth or sore throat onawakening
- Nonrestorative sleep- Gasping or choking at night- Gastroesophageal reflux- Sexual dysfunction with decreasedlibido and impotence
- Cognitive deficits with memory andintellectual impairment
- Decreased vigilance- Mood changes with either depression or anxiety
- Increased body mass index (BMI)- Nasal obstruction- High-arched hard palate- Low hanging soft palate- Large or long uvula- Crowded and small oropharynx with orwithout enlarged tonsils and adenoids
- Malocclusion of the jaw with overjet- Micrognathia, retrognathia, mandibularhypoplasia
- Macroglossia, scalloping of the tongue- Neck circumference >44 cm in men- Brachycephalic head shape
Table IV. Clinical features of obstructive sleep apnea syndrome.

patients who are not candidates for or have failed othernoninvasive treatments, desire surgery, and are medicallystable.90 Identification of the site(s) of obstruction is nec-essary in choosing the appropriate surgical intervention.Methods of localizing the site of obstruction includeendoscopy, pressure catheters, fluoroscopy, computedtomography (CT) scan, or magnetic resonance imaging(MRI).91 Surgical procedures can be divided into phase Iand phase II surgical procedures.92-96 Phase I involvespalatal and lingual surgery: tonsillectomy, uvulo-palatopharyngoplasty (UPPP), uvulopalatal flap (UPF),modified UPPP, palatal advancement, genioglossusadvancement, hyoid suspension, laser midline glossec-tomy, lingualoplasty, and radiofrequency of the softpalate and tongue base. Phase II procedures eitheradvance the jaws (maxillomandibular osteotomy) orwiden the jaws using distraction procedures.Central sleep apnea is characterized by either shallow orabsent breathing during sleep associated with one of thefollowing features: gasping, grunting, choking movements,frequent body movement, and cyanosis. The PSG showscentral apneic pauses >10 s (20 s in infancy) in duration,with one or more of the following: bradytachycardia; fre-quent arousals from sleep; or oxygen desaturation asso-ciated with apneas.4 MSLT may or may not demonstrate amean sleep latency <10 min. Treatment of central sleepapnea involves treatment of comorbid medical conditions(congestive heart failure, nasal congestion, OSAS), con-sideration of supplemental oxygen (1-2 L/min via nasalcannula), or use of acetazolamide (125-250 mg, two tothree times per day).7 Patients with central apneas beforeand after an arousal, without evidence of desaturation,may benefit from a trial of a hypnotic agent (zolpidem,5-10 mg at night).7
RLS and PLMD
RLS has a prevalence of 10% to 15% among patientsbetween the ages of 27 to 41 years.97 It consists ofunpleasant creeping or crawling sensations inside thecalves and generalized aches and pains in the legs asso-ciated with a desire to move the extremities, motor rest-lessness, worsening of symptoms at rest with at least tem-porary relief by activity, nocturnal worsening ofsymptoms (circadian pattern), and difficulty initiatingsleep in the absence of any medical, mental, or othersleep disorder that would account for the symptoms.97-99
RLS can be idiopathic or secondary to iron deficiency,
peripheral neuropathies, or uremia. There are two rec-ognized phenotypes in the idiopathic category: early-onset RLS starts before age 45 and progresses slowly,demonstrating autosomal dominant inheritance, whilelate-onset RLS starts after age 45 and progresses rapidly,with limited familial aggregation.101 Increased cere-brospinal fluid (CSF) hypocretin-1 levels are present inearly-onset RLS patients, whereas levels in late-onsetRLS patients are normal. Allen et al postulate thatincreased hypocretin levels may modulate or promoteinsomnia and increase motor activity.101
RLS involves various areas in the nervous system from thespinal cord up to the basal ganglia.98,101,102 Using singlephoto emission computed tomography (SPECT) andpositron emission tomography (PET), various researchershave demonstrated a decrease in dopamine D2 receptorbinding in the striatum of RLS patients, suggesting thatRLS is related to a deficiency of dopaminergic func-tion.97,100,102-104 Iron deficiency accompanying RLS may beassociated with hypofunction of the D2 receptor.97,100
More than 80% of RLS patients manifest periodic limbmovements (PLMs) during sleep.100 PLMs consist of fouror more repetitive episodes of muscle contraction (0.5-5 s in duration) separated by an interval (≥5 s but <90 s),which may be associated with an arousal. A PLM index(events/hour) >5 is abnormal. Tricyclic antidepressants,lithium, and selective serotonin reuptake inhibitors(SSRIs) can increase PLMs.Saletu and colleagues performed EEG mapping in RLSpatients and demonstrated an increase in both absoluteδ and absolute and relative α2 power, a decrease inabsolute and relative α1 power, an acceleration of thedominant frequency and the α centroid, and a slowing ofthe δ/θ centroid, as well as a nonsignificant attenuationin total power.105 These findings are characteristic of dis-sociated vigilance changes described in depression andcorrelated with higher depression and anxiety scores,lower quality of life, and deteriorated sleep qualitydespite normal Epworth Sleepiness scale scores.Treatment options for RLS include dopaminergic agents(pramipexole, ropinirole, pergolide, levodopa/carbidopa),opioids (oxycodone, propoxyphene), benzodiazepines(clonazepam), anticonvulsants (gabapentin, carba-mazepine), and clonidine.97,102,106-117 Patients with low serumferritin levels may benefit from iron therapy.Treatment with dopaminergic agents is complicated byrebound (worsening of symptoms at the end of the dos-ing period with late night or morning recurrence of
C l i n i c a l r e s e a r c h
380

symptoms and PLMs) and augmentation (worsening ofsymptoms seen with long-term use, particularly withhigher doses, presenting with earlier time-of-day onset ofsymptoms and expansion of symptoms beyond the legs).With levodopa, rebound occurs in 20% of RLS patients,while augmentation affects 82% of patients; augmenta-tion is increased in patients with more severe RLS and inthose receiving higher doses.7,106,117 Dopamine agonists areuseful in treating patients with RLS.108 Pergolide therapyreduced PLMs and increased total sleep time in 83% ofRLS patients, but mild augmentation also occurred.Augmentation may be managed through a combinationof behavioral strategies (walking and other physicalactivities) and medication-timing strategies.7,102
Narcolepsy
Westphal described the first unequivocal case of nar-colepsy in 1877, and Gelineau coined the term narcolepsyin 1880.The prevalence of narcolepsy in the United Statesis 1/2000.3,118 Narcolepsy is a neurological disorder thataffects men and women equally, with usual age of onsetbetween 15 and 30 years. It is characterized by the follow-ing tetrad of symptoms: excessive daytime somnolence(EDS), which can be a continuous feeling of sleepiness or“sleep attacks,” cataplexy, hypnagogic or hypnapompichallucinations, and sleep paralysis.4,118-125 Guilleminault et alreported that EDS alone or in combination with sleepparalysis or hypnagogic hallucinations is the initial symp-tom in 90% of patients and that 5% to 8% of patients pre-sent with cataplexy.126,127 Only 10% of patients experiencethe full tetrad.119
After onset, EDS persists daily, although it can fluctuateduring the day in a stereotyped individual pattern.Attention fluctuates modulated by situational circum-stances. The attack usually starts with drowsiness asso-ciated with blurry or double vision and usually lasts forless than 20 min. Sleepiness is often relieved by a sleepattack, but the relief lasts for only several hours.Cataplexy involves sudden bilateral atonia of striatedmuscles with partial or complete weakness that isbrought on by emotion or excitement. Laughter is themost typical trigger and, less frequently, anger or surprise.Other triggers include anticipation of something specialor hilarious, attempts at bantering, feeling amused, orimmobility in response to a call for immediate action.Thepatient’s “state” and circumstances also influencewhether an attack occurs: sleep deprivation or strong
feeling of sleepiness can lower the attack threshold. Theattacks start abruptly, but take several seconds to reachtheir maximum, with most attacks lasting less than aminute. During partial attacks, the knees may give wayand there may be sagging of the jaw, inclination of thehead, and weakness of the muscles responsible for speechso that the patient is either unable to speak or has slurredspeech. Even with severe attacks, eye movements andrespiration are spared. Neurological examination duringthe attack shows atonia, loss of tendon reflexes, andextensor plantar responses. Prolonged episodes may beassociated with hallucinations and rarely, “status cata-plexicus.” Video-polygraphic analysis of cataplecticattacks demonstrate three phases: (i) initial phase, con-sisting of arrest of eye movements and phasic, massive,inhibitory muscular events; (ii) falling phase, character-ized by a rhythmic pattern of suppressions and enhance-ments of muscular activity leading to the fall; and (iii)atonic phase, associated with complete muscle atonia.128
Injury is uncommon because most people are able to findsupport or sit down at the onset of the attack. A consis-tent individual pattern is seen.Attacks vary in frequencyfrom more than 10 per day to less than 1 per month.Hypnagogic hallucinations (at sleep onset) or hypnapom-pic hallucinations (on waking) represent vivid dreamlikeexperiences of visual imagery (constant or changing col-ored forms), auditory hallucinations, or tactile sensations.Smell and taste are rarely affected. Some patients describeout-of-body experiences at sleep onset.Attacks usually lastless than 10 min, and the frequency varies from less thanonce a month to more than once a day.Sleep paralysis represents inability to move either atsleep onset or upon awakening; the episode can last upto 10 min. Patients can be frightened because they areunable to open their eyes or move their fingers and feelthey have to struggle to move.Disturbed nocturnal sleep is the fifth component of the“tetrad” and is due to frequent awakenings. Althoughpatients typically have short SOL, they may have troublereturning to sleep once awakened. Other reported symp-toms include automatic behavior (episodes of amnesiaassociated with semipurposeful activity), subjective mem-ory impairment that is not validated during standardmemory testing, tiredness or fatigue, blurry or doublevision, and sexual dysfunction (which may be related todrug therapy).124
The PSG demonstrates SOL less than 10 min and REMsleep latency less than 20 min.4 An MSLT demonstrates
Diagnosis and treatment of sleep disorders - Abad and Guilleminault Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
381

a mean sleep latency of less than 5 min with two or moresleep-onset REM (SOREM) episodes.4 Figure 2 depictsSOREM during an MSLT nap.HLA typing demonstrates an increased frequency ofDQB1*0602 or DR2 in patients with narcolepsy, especiallywith cataplexy. Low CSF levels of hypocretin-1 are highlyassociated with narcolepsy with cataplexy (89.5%), par-ticularly in patients with cataplexy who are HLADQB1*0602–positive (95.7%).129-132
Stimulant medications are the mainstay of treatment ofEDS, with the objective of allowing the fullest possiblereturn of normal function for patients at work, home, andschool.118,122,123,125,133-135 The most common stimulants used,listed in incrementing order of relative efficacy are:pemoline, modafinil, dextroamphetamine, methamphet-amine, and methylphenidate.133,135 The maximum recom-mended daily dosages of stimulants in adults are: dex-troamphetamine sulfate, 100 mg; methamphetaminehydrochloride, 80 mg; and methylphenidate, 100 mg.133
Pemoline was utilized in the past, but is not currently rec-ommended due to concerns about the risk of acutehepatic failure.7 Apart from modafinil, all stimulants arecentrally acting sympathomimetic agents that enhancethe release of monoamines in the synaptic cleft and blocktheir reuptake.133,134 Modafinil is a novel stimulant with an
uncertain mechanism of action that may increasedopamine signaling.136 For newly diagnosed narcoleptics,modafinil may represent a reasonable initial choicebecause of its long duration of action, low frequency andseverity of side effects, and low potential for dependenceor tolerance. However, patients should be cautionedabout drug interference with other medications, such asoral contraceptives.There are no well-controlled studiesof pregnant women using stimulants.The benefits for thepatient have to be weighed against the potential risks forthe fetus. Mitler and colleagues recommend dosage reduc-tion or discontinuation of stimulants during attempts atconception and during pregnancy.133
REM-suppressant drugs are utilized in the treatment ofcataplexy, hypnagogic hallucinations, and sleep paralysis.Drugs that block norepinephrine reuptake, such as thetricyclic antidepressants, protriptyline, clomipramine, andimipramine, have been effective, but are frequently asso-ciated with tolerance and anticholinergic side effects.Tricyclics should not be discontinued abruptly because ofthe risk of severe aggravation of cataplexy, including sta-tus cataplecticus.136 SSRIs such as fluoxetine, paroxetine,and citalopram are also effective. Venlafaxine, a norepi-nephrine/serotonin reuptake inhibitor, is highly effectiveand well tolerated.
C l i n i c a l r e s e a r c h
382
Figure 2. Sleep-onset rapid eye movement (REM) during an mean sleep latency test (MSLT) nap in a patient with narcolepsy. Electroencephalogram(EEG) leads (C3-A2 and O2-A1) demonstrate low voltage mixed frequency theta activity. EMG-Chin shows atonia with phasic events. Electro-oculography (EOG) demonstrates REM.
C3-A2
O2-A1
REM
EKG
EMG-Chin
LOC-A2
ROC-A1

γ-Hydroxybutyrate (GHB), a short-acting putative neuro-transmitter that acts as a hypnotic, reduces cataplexy,hypnagogic hallucinations, and subjective sleepiness.Three to nine grams of GHB is administered in bed withhalf of the dose at bedtime and the remainder 2.5 to 3 hlater. Nausea, dizziness, and incontinence have beenreported with high doses. Due to the risk of precipitatingconfusional arousals and even coma, doses >9 g shouldnever be prescribed.Triazolam may be useful in treatinginsomnia in narcoleptics by increasing total sleep timeand sleep efficiency without affecting alertness the fol-lowing day.137
Nonpharmacological therapy includes regular sleep andwake times, short scheduled naps, prevention of sleepdeprivation, avoidance of shift work, and working in astimulating environment. Narcoleptic patients need to becautioned about driving risks when undertreated.
Idiopathic hypersomnia
Idiopathic hypersomnia is a clinically heterogeneous dis-order of chronic sleepiness without cataplexy that has aprevalence of 2 to 5/100 000.138,139 Symptoms presentbetween ages 15 to 30 years and include variable daytimedrowsiness (nonimperative versus irresistible), naps thatrange from short and refreshing to long and unrefresh-ing, prolonged nighttime sleep >12 h or restless sleepwith frequent arousals, sleep “drunkenness,” and auto-matic behavior associated with blank stares andmicrosleep episodes.4,138,139
Three subgroups of patients are recognized. Subgroup 1consists of patients with HLA Cw2 antigen and a posi-tive family history of EDS associated with autonomicdysfunction (syncope, orthostatic hypotension, Raynaud-type phenomena). Subgroup 2 consists of individuals whohad a viral illness (Guillain-Barre, mononucleosis, hepati-tis, atypical viral pneumonia) followed by persistent EDS.Subgroup 3 includes patients with no family history orviral infection prior to onset of EDS. The PSG demon-strates a combination of normal or long nocturnal sleep,and the MSLT performed the day after the PSG showsshort SOL without sleep-onset REM periods.139 Pharma-cological treatment involves use of stimulants, startingwith either modafinil or methylphenidate and switchingto dexedrine spansules if initial treatment is ineffective.Nonpharmacological treatment includes one scheduleddaily nap (noon or late afternoon) no longer than 45 min;avoidance of alcohol, sleep deprivation, heavy meals and
shift work; and observance of regular sleep (at least 8.5 h per night) and wake schedules.
Parasomnias
Parasomnias are characterized by undesirable physicalphenomena or behaviors that occur predominantly dur-ing sleep. Skeletal muscle activity and autonomic nervoussystem changes are prominent. Parasomnias are com-posed of disorders of arousal, partial arousal, and sleep-stage transition (Table I).Disorders of arousal are the most common form of para-somnia. They usually occur during SWS (NREM stagesIII and IV), and symptoms typically present in the firstthird of the night. Studies of twin cohorts and familieswith sleep terror and sleepwalking suggest that geneticfactors may be involved, and there may be a family historyof the same or other NREM arousal parasomnia.140-142
Factors that increase SWS, such as young age, naturaldeep sleeper, recovery from sleep deprivation, centralnervous system (CNS) depressant medications (seda-tives, hypnotics, alcohol), fever, and the hypersomniacperiod in Kleine-Levin syndrome, may aggravate thearousal disorder. Factors that lead to sleep fragmentation,including stress, environmental stimuli, endogenous stim-uli, pain, pregnancy, stimulants, thyroxine taken in theevening, migraine headaches, or Tourette’s syndrome,may trigger the parasomnia.
Confusional arousals (nocturnal sleep drunkenness)
This disorder is more common in children younger than5 years of age, becomes less frequent during adolescence,and is rare in adulthood. The patient partially awakensfrom a deep sleep during the first third of the night, isconfused and slow in mentation, disoriented to time andspace, poorly/partially responsive to external stimuli,manifests automatic behavior (picking at bedclothes),and moans and mumbles incomprehensibly.Attacks lastfrom 30 s to 10 min, and the patient is amnesic for thebehavior and for any dream-like or thought-like menta-tion. PSG shows movement arousal in SWS followed bydecreased amplitude of the EEG and the appearanceduring the period of mental confusion of either NREMstage I or a diffuse α that is slower by 1 to 2 Hz comparedto that of wakefulness. Confusional arousals in childrendo not necessarily warrant treatment. In adults whoexhibit aggression towards others or self-injury, room
Diagnosis and treatment of sleep disorders - Abad and Guilleminault Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
383

C l i n i c a l r e s e a r c h
384
safety precautions need to be implemented and condi-tions facilitating or triggering attacks need to be avoided.The attacks should be allowed to terminate sponta-neously. Benzodiazepines or tricyclic medications may beuseful as short-term therapy for a few days or weeks dur-ing periods when attacks are more common.
Sleep terrors
The peak prevalence of sleep terrors is between 5 and 7years of age. By age 8, half of the children are attack-free,while 36% continue to have attacks until adolescence.Episodes of sleep terror occur during the first third of thenight and also during daytime naps.The child sits up, emitsa piercing scream, and appears frightened, with increasedpulse and respiratory rates and profuse sweating. Theepisodes last from 30 s to 5 min, and the child is amnesicfor the events during the episode. PSG shows explosivearousal with marked increases in muscle tone, heart rate,and respiratory rate, and a rapid decrease in skin resis-tance. Facilitating and precipitating factors need to beavoided.Treatment may include either a short-acting ben-zodiazepine, such as midazolam (10-20 mg), oxazepam (10-20 mg), or clonazepam (0.5-2 mg). Patients unresponsiveto benzodiazepines may benefit from tricyclic antidepres-sants such as clomipramine, desipramine, or imipramine(10-50 mg at hour of sleep). If total control of the episodesoccurs and is sustained over several months, a slow andprogressive withdrawal of medication may be performed.
Sleepwalking (somnambulism)
The patient ambulates during sleep, is difficult to arouseduring an episode, and is usually amnesic following theepisode. Guilleminault et al indicated that children overthe age of 4 reported vague memories of having to act,run away, escape or defend themselves against monsters,animals, snakes, spiders, ants, intruders, or other threats,and that they felt completely isolated and fearful.143,144
Episodes usually occur in the first third of the night dur-ing SWS.4,143,144 This disorder has a peak age of onset at 5 years of age and peak prevalence at about 12 years.Most children outgrow the episodes by age 15. PSGrecordings demonstrate 2 abnormalities during the firstsleep cycle: frequent, brief, nonbehavioral EEG-definedarousals prior to the somnambulistic episode and abnor-mally low δ (0.75-2.0 Hz) EEG power on spectral analy-sis, correlating with high-voltage “hypersynchronic δ”
waves lasting 10 to 15 s occurring just prior to the move-ment.140,142-145 This is followed by stage I NREM sleep, andthere is no evidence of complete awakening.
REM behavior sleep disorder
In REM behavior sleep disorder (RBD), the patient com-plains of violent or injurious behavior during sleep withdisruption of sleep continuity and excessive motor activ-ity during dreaming, accompanied by loss of REM sleepEMG atonia.4,145-151 The frequency of nocturnal eventsvaries from several times a night to once every 3 months.The most common behaviors consist of arm flailing andpunching, kicking, and vocalizations; these behaviors occurin bed or result in falling out of bed. About 32% ofpatients report self-injury ranging from falling out of bedto striking or bumping into the furniture or walls. Olsonreported one patient attempted to fire an unloaded gun,while another attempted to set fire to his bed.147 Sixty-fourpercent of spouses report being assaulted during sleep.147
Dream content in RBD has aggressive themes in about89% of patients, with the most common one being defenseof the sleeper against attack. Although RBD is usuallyidiopathic, it can occur secondarily on a transient orchronic basis.Acute RBD can result from drug withdrawal(meprobamate, pentazocine, nitrazepam, and butalbital)152
or intoxication (biperiden, tricyclic antidepressants, mono-amine oxidase [MAO] inhibitors, or caffeine).149,153 ChronicRBD can be produced by drugs (tricyclic antidepressants,fluoxetine, venlafaxine, mirtazapine, selegeline, and anti-cholinergic medications), vascular problems (subarachnoidhemorrhage, vasculitis), tumors (pontine neoplasms,acoustic tumors), infectious/postinfectious diseases(Guillain-Barre), degenerative or demyelinating condi-tions (amyotrophic lateral sclerosis, fatal familial insom-nia, dementia, Parkinson’s disease, multiple sclerosis, olivo-pontocerebellar degeneration, Shy-Drager syndrome,multiple system atrophy), and developmental, congenital,or familial diseases (narcolepsy, Tourette’s syndrome,Group A xeroderma pigmentosum, mitochondrialencephalomyopathy).147,149,153-155 Because of the overwhelm-ing male preponderance (90%), questions of relationshipsbetween sexual hormones, aggression, and violence havebeen raised.148,149 Diffuse lesions of the hemispheres, bilat-eral thalamic abnormalities, or primary brain stem lesionsmay result in RBD.150
The PSG shows at least one of the following: excessiveaugmentation of chin-EMG tone or excessive chin/limb

Diagnosis and treatment of sleep disorders - Abad and Guilleminault Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
385
phasic EMG twitching associated with one or more ofthe following: excessive limb or body jerking, complexvigorous/violent behaviors, and absence of epileptic activ-ity in association with the disorder. Shirakawa and col-leagues performed MRI and SPECT imaging on 20patients with RBD and reported decreased blood flow inthe upper portions of the frontal lobe and pons.156 Albinand colleagues found decreased striatal dopaminergicinnervation in RBD patients.157
Treatment of RBD has been effective in 90% of patientsusing clonazepam starting at 0.5 mg at bedtime and grad-ually incrementing the dose until control is effected.Other drugs, such as gabapentin, clonidine, carba-mazepine, donezepil, levodopa, and melatonin have beenanecdotally reported to be useful.149,158-162
Environmental safety measures are very important.Potentially dangerous objects should be removed from
the bedroom, weapons (if any) should be stored andlocked away safely outside the bedroom with the keyentrusted to another person, the corners around the bedshould be padded or cushioned, the mattress may beplaced on the floor, and window protection should beconsidered.
Conclusions
Sleep disorders constitute a ubiquitous group of diseasesthat have important consequences for individual healthas well as economic costs to society. The diagnosis ofsleep disorders requires careful history taking, examina-tion, and laboratory testing.Although general guidelinesin management for the more common and importantsleep disorders have been discussed, treatment needs tobe tailored to the individual patient. ❏
Diagnóstico y tratamiento de los trastornosdel sueño: una breve revisión para los clínicos
Los trastornos del sueño incluyen un amplio espec-tro de enfermedades con consecuencias significati-vas para la salud individual y altos costos económi-cos para la sociedad. Para facilitar el diagnóstico ytratamiento de los trastornos del sueño esta revi-sión se estructuró utilizando la ClasificaciónInternacional de Trastornos del Sueño. Se diferen-cia el insomnio primario y secundario, y se discutenlos tratamientos farmacológicos y no farmacológi-cos. Se describen los trastornos comunes del ritmocircadiano en conjunto con intervenciones queincluyen la cronoterapia y la fototerapia. Tambiénse revisa el diagnóstico y tratamiento del síndromede las piernas inquietas o trastorno del movimientoperiódico de las piernas. Además se centra la aten-ción en la apnea obstructiva del sueño y el sín-drome de resistencia de la vía aérea superior y sutratamiento. Se revisa la constelación de síntomasy hallazgos de la narcolepsia, junto con las pruebasdiagnósticas y la terapia. Se describen las parasom-nias, incluyendo los terrores nocturnos, el sonam-bulismo y los trastornos de conducta asociados alsueño REM (movimiento rápido de ojos) junto conlos resultados de las pruebas de laboratorio y el tra-tamiento.
Diagnostic et traitement des troubles dusommeil : brève revue pour les cliniciens
Les troubles du sommeil comprennent un largespectre de maladies avec des conséquences signifi-catives individuelles en termes de santé et un coûtéconomique élevé pour la société. Pour faciliter lediagnostic et le traitement des troubles du sommeil,cette revue fournit un cadre utilisant la classificationinternationale des troubles du sommeil. Les insom-nies primaires et secondaires sont différenciées et lestraitements pharmacologiques et non pharmacolo-giques sont discutés. Les troubles courants du rythmecircadien sont décrits conjointement avec les inter-ventions dont la chronothérapie et la luxthérapie. Lediagnostic et le traitement du syndrome des jambessans repos/mouvements périodiques des membressont abordés. Les apnées obstructives du sommeil etle syndrome de résistance des voies aériennes supé-rieures et leur traitement reçoivent une attentionparticulière. La constellation de symptômes et lesacquisitions sur la narcolepsie sont passées en revueainsi que les épreuves diagnostiques et le traitement.Les parasomnies dont les terreurs nocturnes, le som-nambulisme et les perturbations des mouvementsoculaires rapides (REM, rapid eye movement) sontdécrits conjointement avec les résultats des tests delaboratoire et le traitement.

C l i n i c a l r e s e a r c h
386
REFERENCES
1. Understanding Sleep: Brain Basics. Office of Communications and Public Liaison,National Institute of Neurological Disorders and Stroke, Bethesda, Md.Available at: http://www.ninds.nih.gov/index.htm. Accessed 7 August 2003.2. Ohayon M, Guilleminault C. Epidemiology of Sleep Disorders. In:Chokroverty S, ed. Sleep Disorders Medicine. Woburn, Mass: ButterworthHeinemann; 1999:301-316.3. Partinen M, Hublin C. Epidemiology of Sleep Disorders. In: Kryger MH, RothT, Dement WC, eds. Principles and Practice of Sleep Medicine. Philadelphia, Pa:WB Saunders; 1979:558-579.4. American Academy of Sleep Medicine. The International Classification of SleepDisorders, revised: Diagnostic and Coding Manual. Rochester, Minn: AmericanAcademy of Sleep Medicine; 2000.5. Thorpy M. Classification of Sleep Disorders. In: Kryger MH, Roth T, DementWC, eds. Principles and Practice of Sleep Medicine. 3rd ed. Philadelphia, Pa: WBSaunders; 2000:547-557. 6. Thorpy M. Classification of Sleep Disorders. In: Chokroverty S, ed. SleepDisorders Medicine. Woburn, Mass: Butterworth Heinemann; 1999:287-300.7. Reite M, Ruddy J, Nagel K. Concise Guide to Evaluation and Management ofSleep Disorders. Washington, DC: American Psychiatric Publishing; 2002:1-273.8. Borbely A. Sleep: circadian rhythm vs recovery process. In: Koukou-LehmanM, ed. Functional States of the Brain: their Determinants. Amsterdam:Elsevier/North Holland; 1980:151-161.9. Zee P, Harsanyi K. Highlights of sleep neuroscience. In: Bowman T, ed. Reviewof Sleep Medicine. Burlington, Mass: Butterworth Heinemann; 2003:19-39.10. Silber MH. Neurologic treatment sleep disorders. Neurol Clin. 2001;19:173-186.11. Elsenbruch S, Thompson JJ, Hamish MJ, Exton MS, Orr WC. Behavioral andphysiological sleep characteristics in women with irritable bowel syndrome.Am J Gastroenterol. 2002;97:2306-2314.12. Moldofsky H. Management of sleep disorders in fibromyalgia. Rheum DisClin North Am. 2002;28:173-186.13. Chokroverty S. Diagnosis and treatment of sleep disorders caused by co-morbid disease. Neurology. 2000;54(5 suppl 1):S8-S15.14. Neubauer D. Sleep problems in the elderly. Am Fam Physician. 1999;59:2551-2560.15. Chesson, AL Jr, Ferber RA, Fry JM, et al. Practice parameters for the indi-cations for polysomnography and related procedures. Sleep. 1997:406-422.16. Chesson AL Jr, Ferber RA, Fry JM, et al. The indications for polysomnog-raphy and related procedures. Sleep. 1997;20:423-487.17. Keenan S. Polysomnographic technique: an overview. In: Bowman, ed. Reviewof Sleep Medicine. Burlington, Mass: Butterworth Heinemann; 2003:107-132.18. Chervin R. Use of clinical tools and tests in sleep medicine. In: Kryger MH,Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. 3rd ed.Philadelphia, Pa: WB Saunders; 2000:537-543.19. Thorpy M, Chesson A, Ferber R. et al. Practice parameters for the use ofportable recording in the assessment of obstructive sleep apnea. Sleep.1994;17:372-377.20. Van Kempeima AR, Rutgers SR, Strijers RL. The value of 1-hour daytimesleep recording in the diagnosis of the sleep apnea syndrome. J Sleep Res.1993;2:257-259.21. Coleman J. Sleep Studies. Current Techniques and Future Trends.Otolaryngol Clin North Am. 1999;32:195-210.22. Strohl KP. Timing, number and complexities of sleep studies. SleepBreathing. 1997;2:45-49. 23. Thorpy M. The Clinical Use of the Multiple Sleep Latency Test. TheStandards of Practice Committee of the American Sleep Disorders Association.Sleep. 1992;15:268-276.24. Mitler M, Carskadon M, Hirshkowitz M. Evaluating sleepiness. In: KrygerMH, Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. 3rd ed.Philadelphia, Pa: WB Saunders; 2000:1251-1257. 25. Doghramji K, Mitler MM, Sangal RB, et al. A normative study of the main-tenance of wakefulness test (MWT). Electroencephalogr Clin Neurophysiol.1997;103:554-56226. Littner M, Kushida C, Anderson W, et al. Practice parameters for the roleof actigraphy in the study of sleep and circadian rhythms: an update for 2002.Sleep. 2003;26:337-341.
27. Thorpy M, Chesson A, Derderian S. Practice parameters for the use of actig-raphy in the clinical assessment of sleep disorders. Sleep. 1995:18:285-287.28. Littner M, Kushida CA, Anderson WM, et al. practice parameters for therole of actigraphy in the study of sleep and circadian rhythms: an update for2002. Sleep. 2003;26:337-341.29. Ware J, Hirshkowitz M. Assessment of sleep-related erections. In: KrygerMH, Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. 3rd ed.Philadelphia, Pa: WB Saunders; 2000:1231-1237. 30. Vgontzas AN, Bixler EO, Lin HM, et al. Chronic insomnia is associated withnyctohemeral activation of the hypothalamic-pituitary-adrenal axis: clinicalimplications. J Clin Endocrinol Metab. 2001;86:3787-3794.31. Rodenbeck A, Hajak G. Neuroendocrine dysregulation in primary insom-nia. Rev Neurol (Paris). 2001;157:S57-S61.32. Vgontzas, AN, Zoumakis M, Papanicolaou DA, et al. Chronic insomnia isassociated with a shift of interleukin-6 and tumor necrosis factor secretionfrom nighttime to daytime. Metabolism. 2002;51:887-892.33. Vgontzas AN, Chrousos GP. Sleep, the hypothalamic-pituitary-adrenal axis,and cytokines: multiple interactions and disturbances in sleep disorders.Endocrinol Metab Clin. 2002;31:15-36.34. Morin C, Hauri P, Espie C, et al. Non-pharmacologic treatment of chronicinsomnia. Sleep. 1999;22:1134-1156.35. Petit L, Azad N, Byszewski A, et al. Non-pharmacological management ofprimary and secondary insomnia among older people: review of assessmenttools and treatments. Age Ageing. 2003;32:19-25.36. Kales A, Kales R. Evaluation and Treatment of Insomnia. New York, NY: OxfordPress; 1984:2-320.37. Buysee DJ, Reynolds CF 3rd, Monk TH, et al. The Pittsburgh Sleep QualityIndex: a new instrument for psychiatric practice and research. Psychiatr Res.1989;28:193-213.38. Holbrook A, Crowther R, Lotter A, et al. Meta-analysis of benzodiazepineuse in the treatment of insomnia. Can Med Assoc J. 2000;162:225-233.39. Shorr RI, Robin DW. Rational use of benzodiazepines in the elderly. DrugsAging. 1994;4:9-20.40. Vgontzas AN, Kales A, Bixler EO. Benzodiazepine side effects: role of phar-macokinetics and pharmacodynamics. Pharmacology. 1995;51:205-223.41. Terzano MG, Rossi M, Palomba V, et al. New drugs for insomnia: com-parative tolerability of zopiclone, zolpidem, and zaleplon. Drug Saf.2003;26:261-282.42. Harvey AG. A cognitive model of insomnia. Behav Res Ther. 2002;40:869-893.43. Johnson LC, Spinweber CL. Quality of sleep and performance in the Navy:a longitudinal study of good and poor sleepers. In: Guilleminault C, LugaresiE, eds. Sleep/wake Disorders: Natural History, Epidemiology, and Long-term Evolution.New York, NY: Raven Press; 1983.44. Backhaus J, Hohagen F, Voderholzer U, Riemann D. Long-term effective-ness of a short-term cognitive-behavioral group treatment for primary insom-nia. Eur Arch Psychiatry Clin Neurosci. 2001;251:35-41.45. Kales JD, Kales A, Bixler EO, et al. Biopsychobehavioral correlates of insom-nia, V. Clinical and behavioral correlates. Am J Psychiatry. 1984;141:1371-1376.46. Mamber R, Kuo T. Cognitive-behavioral therapies for insomnia. In: Chiong,Sateia, Carskadon, eds. Sleep Medicine. Philadelphia, Pa: Hanley & Belfus;2002:177-185.47. Dahl R. The Interface between Sleep Disorders and Behavioral/ EmotionalDisturbances Cases. Proceedings in the 9th Annual Course in Pediatric SleepMedicine by the School of Sleep Medicine, Palo Alto, Calif, March 22-26, 2003.48. Guilleminault C, Clerk A, Black J, et al. Nondrug treatment trials in psy-chophysiologic insomnia. Arch Intern Med. 1995;155:838-844.49. Baker S, Zee P. Circadian disorders of the sleep-wake cycle. In: Kryger MH,Roth T, Dement WC, eds. Principles and Practice of Sleep Medicine. 3rd ed.Philadelphia, Pa: WB Saunders; 2000:606-614.50. Turek F, Dugovic C, Zee P. Current Understanding of the circadian clockand the clinical implications for neurological disorders. Arch Neurol.2001;58:1781-1787.51. Skene DJ. Optimization of light and melatonin to phase-shift human cir-cadian rhythms. J Neuroendocrinol. 2003;15:438-441.52. Rivkees S. Mechanisms and clinical significance of circadian rhythms inchildren. Curr Opin Pediatr. 2001;13:352-357.53. Cardinali DP, Brusco LI, Lloret SP, Furio AM. Melatonin in sleep disordersand jet-lag. Neuroendocrinol Lett. 2002;23(suppl 1):9-13.

Diagnosis and treatment of sleep disorders - Abad and Guilleminault Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
387
54. Ondze B, Espa F, Ming LC, et al. Advanced sleep phase syndrome. RevNeurol (Paris). 2001;157(II Pt 2):S130-S134.55. Monk T. Shift work. In: Kryger MH, Roth T, Dement WC, eds. Principles andPractice of Sleep Medicine. 3rd ed. Philadelphia, Pa: WB Saunders; 2000:600-605.56. Burgess HJ, Sharkey KM, Eastman CI. Bright light, dark and melatonin canpromote circadian adaptation in night shift workers. Sleep Med Rev.2002;6:407-420.57. Quera-Salva MA. Rapid shift in sleep time and acrophase of melatoninsecretion in short shift work schedule. Sleep. 1996;19:539-543.58. Van Reeth O, Mennuni G. Fatigue and sleep: the point of view of thechronobiologist. Rev Med Brux. 2002;23:A288-A293.59. Horowitz TS, Tanigawa T. Circadian-based new technologies for nightworkers. Ind Health. 2002;40:223-236.60. Purnell MT, Feyer AM, Herbison GP. The impact of a nap opportunity dur-ing the night shift on the performance and alertness of 12-h shift workers. JSleep Res. 2002;11:219-227.61. Meoli A, Casey K, Clark R, et al. Hypopnea in sleep-disordered breathingin adults. Sleep. 2001;24:469-470.62. Guilleminault C, Stoohs R, Clerk A, Cetel M, Maistros P. A cause of exces-sive daytime sleepiness. The upper airway resistance syndrome. Chest.1993;104:781-787.63. Black JE, Guilleminault C, Colrain IM, Carrillo O. Upper airway resistancesyndrome. Central electroencephalographic power and changes in breathingeffort. Am J Respir Crit Care Med. 2000;162:406-411.64. Guilleminault C, Kim YD, Palombini L, Li K, Powell N. Upper airway resis-tance syndrome and its treatment. Sleep. 2000;23(suppl 4):S197-S200.65. Schecter M and the Section on Pediatric Pulmonology Subcommittee onObstructive Sleep Apnea Syndrome. Technical report: diagnosis and man-agement of childhood obstructive sleep apnea. Pediatrics. 2002;109:e69.66. Bower C, Gungor A. Update on the pediatric airway. Pediatric obstructivesleep apnea. Otolaryngol Clin North Am. 2000;33:49-75.67. Guilleminault C, Pelayo R, Leger D, Clerk A, Bocian R. Recognition of sleep-disordered breathing in children. Pediatrics. 1996;98:871-882.68. Chervin RD, Archbold KH, Dillon JE, et al. Inattention, hyperactivity, andsymptoms of sleep-disordered breathing. Pediatrics. 2002;109:449-456.69. Corkum P, Muldofsky H, Hogg-Johnson S, Humphries T, Tannock R. Sleepproblems in children with attention deficit/hyperactivity disorder: impact ofsubtype, comorbidity, and stimulant medication. J Am Acad Child AdolesPsychiatry. 1999;38:1285-1293.70. Loube DI, Gay PC, Strohl KP, et al. Indications for positive airway pressuretreatment of adult obstructive sleep apnea patients. A consensus statement.Chest. 1999;115:863-866.71. Mosk S. Self-reported depressive symptomatology, mood ratings, andtreatment outcome in sleep disorder patients. J Clin Psychol. 1989;45:51-60.72. Sforza E, Lugaresi, E. Daytime sleepiness and nasal continuous positive air-way pressure therapy in obstructive sleep apnea syndrome patients; effectsof chronic treatment and 1-night therapy withdrawal. Sleep. 1995;18:195-201. 73. Redline S, Adams N, Strauss ME, et al. Improvement of mild sleep-disor-dered breathing with CPAP compared with conservative therapy. Am J RespirCrit Care Med. 1998;157:858-865.74. Kribbs NB, Pack AI, Kline LR, et al. Effects of one night without nasal CPAPtreatment on sleep and sleepiness in patients with obstructive sleep apnea.Am Rev Respir Dis. 1993;14:1162-1168.75. Rajagopal KR, Bennett LL, Dillard TA, Tellis CJ, Tenholder MF. Overnightnasal CPAP improves hypersomnolence in sleep apnea. Chest. 1986;90:172-176.76. Engleman HM, Martin SE, Deary IJ, Douglas NJ. Effects of continuous pos-itive airway pressure treatment on daytime function in sleep apnoea/hypop-noea syndrome. Lancet. 1994;343:572-575.77. Downey R 3rd, Perkin RM, MacQuarrie J. Nasal continuous positive airwaypressure use in children with obstructive sleep apnea younger than 2 yearsof age. Chest. 2000;117:1608-1612.78. McNamara F, Sullivan C. Obstructive sleep apnea in infants and its man-agement with nasal continuous positive airway pressure. Chest. 1999;116:10-16.79. Anstead M, Phillips B, Buch K. Tolerance and intolerance to continuouspositive airway pressure. Curr Opin Pulm Med. 1998;4:351-354.80. Strollo PJ Jr, Sanders MH, Atwood CW. Positive pressure therapy. Clin ChestMed. 1998;19:55-68.
81. Hoffstein V, Viner S, Mateika S, Conway J. Treatment of obstructive sleepapnea with nasal continuous positive airway pressure patient compliance,perception of benefits, and side effects. Am Rev Respir Dis. 1992;145:841-845.82. Issa FG, Sullivan CE. Reversal of central sleep apnea using nasal CPAP. Chest.1984;90:165-171.83. Rauscher H, Popp W, Wanke T, Zwick H. Acceptance of CPAP therapy forsleep apnea. Chest. 1991;100:1019-1023.84. Rolfe I, Olson LG, Saunders NA. Long-term acceptance of continuous pos-itive airway pressure in obstructive sleep apnea. Am Rev Respir Dis.1991;144:1130-1133.85. Nino-Murcia G, McCann CC, Bliwise DL, Guilleminault C, Dement WC.Compliance and side effects in sleep apnea patients treated with nasal con-tinuous positive airway pressure. West J Med. 1989;150:165-169. 86. Sanders MH, Gruendl CA, Rogers RM. Patient compliance with nasal CPAPtherapy for sleep apnea. Chest. 1986;90:330-333.87. Waldhorn, RE, Herrick TW, Nguyen MC, O'Donnell AE, Sodero J,Potolicchio SJ. Long-term compliance with nasal continuous positive airwaypressure therapy of obstructive sleep apnea. Chest. 1990;97:33-38.88. Littner M, Hirshkowitz M, Davila D, et al. Practice parameters of the useof auto-titrating continuous positive airway pressure devices for titrating pres-sures and treating adult patients with obstructive sleep apnea syndrome.Sleep. 2002;25:143-147.89. Berry RB. The use of auto-titrating continuous positive airway pressurefor treatment of adult obstructive sleep apnea. Sleep. 2002;25:148-173.90. American Sleep Disorders Association. Practice parameters for the treat-ment of obstructive sleep apnea in adults: the efficacy of surgical modifica-tions of the upper airway. Sleep. 1996;19:152-155.91. Rama AN, Tekwani SH, Kushida CA. Sites of obstruction in obstructivesleep apnea. Chest. 2002;122:1139-1147.92. Sher A, Schechtman K, Piccirillo J. The efficacy of surgical modifications ofthe upper airway in adults with obstructive sleep apnea syndrome. Sleep.1996;19:156-177.93. Loube D. Technologic advances in the treatment of obstructive sleepapnea syndrome. Chest. 1999;116:1426-1433.94. Riley R, Powell N, Li K, Guilleminault C. Surgical therapy for obstructivesleep apnea-hypopnea syndrome. In: Kryger MH, Roth T, Dement WC, eds.Principles and Practice of Sleep Medicine. 3rd ed. Philadelphia, Pa: WB Saunders;2000:913-929.95. Powell N, Riley R, Guilleminault C. Radiofrequency tongue base reductionin sleep-disordered breathing. Otolaryngol Head Neck Surg. 1999;120:656-664.96. Riley R. Powell-Riley Stanford surgical protocol. Proceedings of theConference on Contemporary Surgical Concepts and Techniques in Snoringand Sleep Disordered Breathing. Burlingame, Calif. April 11-12, 2003.97. Montplaisir J, Nicolas A, Godbout R, Walters A. Restless legs syndrome andperiodic limb movement disorder. In: Kryger MH, Roth T, Dement WC, eds.Principles and Practice of Sleep Medicine. 3rd ed. Philadelphia, Pa: WB Saunders;2000:742-752.98. Hening WA. Restless legs syndrome: a sensorimotor disorder of sleep/wakemotor regulation. Curr Neurol Neurosci Rep. 2002;2:186-196.99. Stiasny K, Oertel WH, Trenkwalder C. Clinical symptomatology and treat-ment of restless legs syndrome and periodic limb movement disorder. SleepMed Rev. 2002;6:247-251.100. Montplaisir J, Nicolas A, Denesle R, Gomez-Mancilla B. Restless legs syn-drome improved by pramipexole. Neurology. 1999;52:938-943.101. Allen RP, Mignot E, Ripley B, Nishino S, Earley CJ. Increased CSF hypocre-tin-1 (orexin-A) in restless legs syndrome. Neurology. 2002;59:639-641. 102. Chokroverty S, Jankovic J. Restless legs syndrome. Neurology. 1999;52:907.103. Turjanski N, Lees AJ, Brooks DJ. Striatal dopaminergic function in rest-less legs syndrome: 18F-dopa and 11C-raclopride PET studies. Neurology.1999;52:932-937.104. Staedt J, Stoppe G, Kogler A, et al. Nocturnal myoclonus syndrome (peri-odic movements in sleep) related to central dopamine D2-receptor alteration.Eur Arch Psychiatry Clin Neurosci. 1995;245:8-10.105. Saletu M, Anderer P, Saletu B, et al. EEG mapping in patients with rest-less legs syndrome as compared with normal controls. Psychiatry Res.2002;115:49-61.106. Hening W, Allen R, Earley C, et al. The treatment of restless legs syn-drome and periodic limb movement disorder. Sleep. 1999;22:970-999.

107. Chesson A, Wise M, Davila D, et al. Practice parameters for the treatmentof restless legs syndrome and periodic limb movement disorder. Standards ofPractice Committee of the American Academy of Sleep Medicine. Sleep.1999;22:961-968.108. Comella C. Restless legs syndrome. Treatment with dopaminergic agents.Neurology. 2002;58:S87-S92.109. Walters AS, Wagner ML, Hening WA, et al. Successful treatment of theidiopathic restless legs syndrome in a randomized double-blind trial of oxy-codone versus placebo. Sleep. 1993;16:327-332.110. Kaplan PW, Allen RP, Buchholz DW, Walters, JK. A double-blind placebo-controlled study of the treatment of periodic limb movements in sleep usingcarbidopa/levodopa and propoxyphene. Sleep. 1993;16:717-723.111. Montagna P, Sassoli de Bianchi L, Zucconi M, et al. Clonazepam and vibra-tion in restless legs syndrome. Acta Neurol Scand. 1984;69:428-430.112. Boghen D, Lamothe L, Elie R, et al. The treatment of the restless legs syn-drome with clonazepam: a prospective controlled study. Can J Neurol Sci.1986;13:245-247.113. Thorp ML, Morris CD, Bagby SP. A crossover study of gabapentin in treat-ment of restless legs syndrome among hemodialysis patients. Am J Kidney Dis.2001;38:104-108. 114. Garcia-Borreguero D, Larrosa O, de la Llave Y, et al. Treatment of rest-less legs syndrome with gabapentin. A double-blind, cross-over study.Neurology. 2002;59:1573-1579.115. Telstaad W, Sorensen O, Larsen S, et al. Treatment of the restless legs syn-drome with carbamazepine: a double-blind study. BMJ (Clin Res Ed).1984;288:444-446. 116. Wagner ML, Walters AS, Coleman RG, Hening WA, Grasing K,Chokroverty S. Randomized, double-blind placebo-controlled study of cloni-dine in restless legs syndrome. Sleep. 1996;19:52-58.117. Guilleminault C, Cetel M, Philip P. Dopaminergic treatment of restlesslegs and rebound phenomenon. Neurology. 1993;43:443-445.118. Guilleminault C, Anagnos A. Narcolepsy. In: Kryger MH, Roth T, DementWC, eds. Principles and Practice of Sleep Medicine. 3rd ed. Philadelphia, Pa: WBSaunders; 2000:676-686.119. Overeem S, Mignot E, van Dijk JG, Lammers GJ. Narcolepsy: clinical fea-tures, new pathophysiologic insights, and future perspectives. J ClinNeurophysiol. 2001;18:78-105. 120. Stores G. Recognition and management of narcolepsy. Arch Dis Child.1999; 81:519-524.121. Gerhardstein R, Day R, Rosenthal L. Narcolepsy and other causes of exces-sive daytime sleepiness. Respir Care Clin N Am. 1999;5:427-446. 122. Guilleminault C, Pelayo R. Narcolepsy in children: a practical guide to itsdiagnosis, treatment, and follow-up. Paediatr Drugs. 2000;2:1-9.123. Krahn LE, Black JL, Silber MH. Krahn, L. Narcolepsy: new understand-ing of irresistible sleep. Mayo Clinic Proc. 2001;76:185-194.124. Aldrich M. Narcolepsy. N Engl J Med. 1990;323:389-394.125. Black J. Narcolepsy: evaluation and management. CNS News Special Ed.2001:25-29.126. Guilleminault C, Wilson RA, Dement WC. A study on cataplexy. ArchNeurol. 1974;31:255-261.127. Guilleminault C, Anders TF. The pathophysiology of sleep disorders inpediatrics. Part II. Sleep disorders in children. Adv Pediatr. 1976;22:151-174.128. Rubboli G, d'Orsi G, Zaniboni A, et al. A video-polygraphic analysis of thecataplectic attack. Clin Neurophysiol. 2000;111(suppl 2):S120-S128.129. Overeem S, Scammell T, Lammers G. Hypocretin/orexin and sleep: impli-cations for the pathophysiology and diagnosis of narcolepsy. Curr Opin Neurol.2002;15:739-745.130. Mignot E, Lammers GJ, Ripley B, et al. The role for cerebrospinal fluidhypocretin measurement in the diagnosis of narcolepsy and other hyper-somnias. Arch Neurol. 2002;59:1553-1562.131. Krahn LE, Pankratz VS, Oliver L, Boeve BF, Silber MH. Hypocretin (orexin)levels in cerebrospinal fluid of patients with narcolepsy: relationship to cata-plexy and HLA DQB1*0602 status. Sleep. 2002;25:733-736.132. Kanbayashi T, Inoue Y, Chiba S, et al. CSF hypocretin-1 (orexin-A) con-centrations in narcolepsy with and without cataplexy and idiopathic hyper-somnia. J Sleep Res. 2002;11:91-93.133. Mitler MM, Aldrich MS, Koob GF, Zarcone VP. Narcolepsy and its treat-ment with stimulants: ASDA standards of practice. Sleep. 1994;17:352-371.
134. Parkes D. Introduction to the mechanism of action of different treat-ments of narcolepsy. Sleep. 1994;17(8 suppl):S93-S96.135. Littner M, Johnson SF, McCall WV, et al. Standards of Practice Committee.Practice parameters for the treatment of narcolepsy: an update for 2000.Sleep. 2001;24:451-466.136. Scamell TE. The neurobiology, diagnosis, and treatment of narcolepsy.Ann Neurol. 2003;53:154-166.137. Thorpy MJ, Snyder M, Aloe FS, Ledereich PS, Starz KE. Short-term tria-zolam use improves nocturnal sleep of narcoleptics. Sleep. 1992;15:212-216.138. Bassetti C, Aldrich M. Idiopathic hypersomnia. A series of 42 patients.Brain. 1997;120:1423-1435.139. Guilleminault C, Brooks S. Idiopathic hypersomnia: a neurologicaldilemma. Sleep Med Rev. 2001;5:347-349.140. Broughton R. NREM arousal parasomnias. In: Kryger MH, Roth T, DementWC, eds. Principles and Practice of Sleep Medicine. 3rd ed. Philadelphia, Pa: WBSaunders; 2000:687-692.141. Kales A, Soldatos CR, Bixler EO, et al. Hereditary factors in sleepwalkingand night terrors. Br J Psychiatry. 1980;137:111-118.142. Abe K, Amatomi M, Oda N. Sleepwalking and recurrent sleep talking inchildren of childhood sleepwalkers. Am J Psychiatry. 1984;141:800-801.143. Guilleminault C, Poyares D, Abat F, Palombini L. Sleep and wakefulnessin somnambulism. A spectral analysis study. J Psychosom Res. 2001;51:411-416.144. Guilleminault C, Palombini L, Pelayo R, Chervin R. Sleepwalking andsleep terrors in prepubertal children: what triggers them? Pediatrics.2003;111:e17-e25.145. Guilleminault C, Moscovich A, Leger D. Forensic sleep medicine and noc-turnal wandering and violence. Sleep. 1995;15:173-184.146. Broughton RJ, Shimuzu T. Sleep-related violence: a medical and foren-sic challenge. Sleep. 1995;18:727-730.147. Olson E, Boeve B, Silbert M. Rapid eye movement sleep behaviour dis-order: demographic, clinical and laboratory findings in 93 cases. Brain.2000;123:331-339.148. Mahowald M, Schenk C. Medical-legal aspects of sleep medicine. NeurolClin. 1999;17:215-234.149. Mahowald M, Schenk C. REM sleep parasomnias. In: Kryger MH, Roth T,Dement WC, eds. Principles and Practice of Sleep Medicine. 3rd ed. Philadelphia,Pa: WB Saunders; 2000:724-741.150. Ferini-Strambi L, Zucconi M. REM sleep behavior disorder. ClinNeurophysiol. 2000;111(suppl 2):S136-S140.151. Schenck C, Bundlie S, Ettinger M, Mahowald M. Chronic behavioral dis-orders of human REM sleep: a new category of parasomnia. Sleep. 1986;9:293-308.152. Silber M. REM sleep behavior disorder associated with barbiturate with-drawal. APSS Abstract. Sleep Res. 1996;25:371. 153. Husain A, Miller P, Carwile S. REM sleep behavior disorder: potential rela-tionship to post-traumatic stress disorder. J Clin Neurophysiol. 2001;18:148-157.154. Onofrj M, Luciano AL, Thomas A, et al. Mirtazapine induces REM sleepbehavior disorder (RBD) in parkinsonism. Neurology. 2003;60:113-115.155. Schutte S, Doghramji K. REM behavior disorder seen with venlafaxine(Effexor). APSS Abstract. Sleep Res. 1996;25:364.156. Shirakawa S, Takeuchi N, Uchimura N, et al. Study of image findings inrapid eye movement sleep behavioural disorder. Psychiatry Clin Neurosci.2002;56:291-292.157. Albin RL, Koeppe RA, Chervin RD, et al. Decreased striatal dopaminergicinnervation in REM sleep behavior disorder. Neurology. 2000;55:1410-1412.158. Ringman JM, Simmons JH. Treatment of REM sleep behavior disorderwith donezepil: a report of three cases. Neurology. 2000;55:870-871.159. Bamford C. Carbamazepine in REM sleep behavior disorder. Sleep.1993;16:33.160. Mike ME, Kranz AJ. MAOI suppression of RBD refractory to clonazepamand other agents. Sleep Res. 1996;25:63.161. Takeuchi N, Uchimura N, Hashizume Y, et al. Melatonin therapy for REMsleep behavior disorder. Psychiatry Clin Neurosci. 2001;55:267-279.162. Kunz D, Bes F. Melatonin as a therapy in REM sleep behavior patients:an open-labeled pilot study on the possible influence of melatonin on REMsleep regulation. Mov Disord. 1999;14:507-511.
C l i n i c a l r e s e a r c h
388

easonal affective disorder (SAD), as originallydescribed in 1984,1 is a condition characterized by theannual recurrence of depressive episodes in fall and win-ter followed by remission of depressive symptoms inspring and summer.1 Patients with SAD have to meetdiagnostic criteria for major depression, recurrent, orbipolar disorder. In the latest version of the Diagnosticand Statistical Manual of Mental Disorders (DSM-IV),SAD is listed as a specifier of either bipolar or recurrentmajor depressive disorder, with a seasonal pattern ofmajor depressive episodes.2 Subsyndromal SAD is a dis-order with similar but milder symptoms that do notgrossly disrupt patients social and occupational func-tioning.3 The four central features characterizing SADare listed in Table I. Patients with SAD have the usualsymptoms of depression, including low mood, lack ofdrive, decreased concentration, and reduced interest.Typically, many SAD patients also tend to have a specificsymptom cluster consisting of the so-called reverse veg-etative or atypical depressive symptoms.These symptomsinclude increased sleep (70%-90% of SAD patients),increased appetite (70%-80%), carbohydrate craving(80%-90%), and weight gain (70%-80%).4
Pathophysiology
The etiology of SAD remains unclear. It is thought thatthe decreasing daylight period as winter approaches trig-gers depressive episodes in individuals vulnerable toSAD. However, although bright light exposure is used inthe treatment of SAD, no causal relation can be drawnbetween the occurrence of SAD and the shortage of lightin fall and winter. Patients with SAD may be sensitive tofactors that are common to various forms of recurrent
Keywords: seasonal affective disorder; depression; light therapy; pharma-cotherapy; treatment guidelines
Author affiliations: Centre for Addiction and Mental Health, PET Centre,Toronto, ON, Canada
Address for correspondence: Nicole Praschak-Rieder, MD, Centre for Addictionand Mental Health, PET Centre, 250 College Street, Toronto, Ontario, CanadaM5T 1R8(e-mail: [email protected])
C l i n i c a l r e s e a r c h
389
Treatment of seasonal affective disordersNicole Praschak-Rieder, MD; Matthäus Willeit, MD
S
Seasonal affective disorder (SAD) is a subform of majordepressive disorder, recurrent, or bipolar disorder with aregular onset of depressive episodes at a certain time ofyear, usually the winter. The treatment of SAD is similar tothat of other forms of affective disorder, except thatbright light therapy is recommended as the first-lineoption. Light therapy conventionally involves exposure tovisible light of at least 2500 lux intensity at eye level. Theeffects of light therapy are thought to be mediated exclu-sively by the eyes, not the skin, although this assumptionhas not yet been verified. Morning light therapy hasproven to be superior to treatment regimens in theevening. Response rates to light therapy are about 80%in selected patient populations, with atypical depressivesymptoms being the best predictor of a favorable treat-ment outcome. Data from randomized, controlled trialssuggest that antidepressants are effective in the treat-ment of SAD. Three double-blind, placebo-controlled tri-als have been conducted showing promising results forthe selective serotonin reuptake inhibitors (SSRIs) sertra-line and fluoxetine, as well as for moclobemide, areversible inhibitor of monoamine oxidase A. © 2003, LLS SAS Dialogues Clin Neurosci. 2003;5:389-398.
Copyright © 2003 LLS SAS. All rights reserved www.dialogues-cns.org

affective disorder, and SAD can be seen as a disorder dri-ven by endogenous annual rhythms and characterized byan imbalance of indoleamines, serotonin, and melatonin,as well as catecholamines, over the year.
Light therapy
Bright light therapy (BLT) has become a first-line clinicalstandard for treatment of SAD (Table II).The use of BLTas a therapy for SAD evolves directly out of neuroscience.In the early 1980s, knowledge that light could shift circa-dian and seasonal rhythms in animals, together with theheuristic idea of extending daylight during the wintermonths, led to the first clinical study on BLT in SAD.1
Since then, numerous studies have not only proven its effi-cacy, but also greatly refined our knowledge on treatmentstrategies, thereby allowing for astonishingly high responserates of 80% in selected patient populations.5 BLT is safe,effective, and it has few and benign side effects. It is gen-erally well accepted by the patients,6 and indications otherthan SAD, eg, disturbances of circadian rhythm due to jetlag or shift work,7,8 circadian-phase–related disturbancesin dementia,9,10 sleep disorders,11,12 and nonseasonal affec-tive disorders,13-15 are expanding research fields.
Efficacy
The first controlled clinical trial1 already showed the ben-eficial effects of light against symptoms of SAD. Sincethen, more than 60 controlled studies and two meta-analyses16,17 have shown the efficacy of this treatment.Using stringent criteria, the meta-analysis of Terman etal16 found remission rates of up to 67% of patients withmilder depression and up to 40% of more severelydepressed patients. These benefits were seen as early as1 week after beginning treatment. However, it is now
known that improvement may sometimes be seen as lateas 2 to 4 weeks after beginning BLT.18
The obvious obstacles in the search for plausible placebosand “blinded” designs for studying the efficacy of BLThave led to concerns about the adequacy of control con-ditions. Early studies mostly used dim-light of an intensityof 300 lux or less, delivered through a light source other-wise identical to that used in the active condition (mostlylight of 2500 lux intensity). As it was still possible to dis-tinguish between the bright and dim-light conditions, thesestudies have been questioned as to whether they measuredreal biological effects and whether they could reliably sep-arate a true antidepressant effect from placebo effects.However, fantasy and creativity of researchers in the fieldhas led to further studies, which now unequivocally provethat light is an active biological agent with antidepressanteffects in SAD. Some of these studies used (deactivated)negative ion generators as placebo condition.18-20 Like alight box, the negative ion generator is a device, has a plau-sible mechanism of antidepressant action, and requires thesubject to sit beside it. Light had the better antidepres-sant effect and produced significantly more remissions,although expectations were equal for both conditions.Interestingly enough, high doses of negative ions do seemto have an antidepressant effect as well.20
C l i n i c a l r e s e a r c h
390
Table I. Features of seasonal affective disorder (SAD).
Recurrent major depressive episodes that start around the
same time each year (eg, fall and winter) and end around
the same time each year (eg, spring and summer)
Full remission of symptoms during the unaffected period of
the year (eg, summer)
Over the lifetime course of the illness, there are relatively
more seasonal depressive episodes than nonseasonal
episodes
Seasonal depressive episodes occur in at least 2 consecutive
years
Table II. Guidelines for bright light therapy (BLT).
Light therapy is an effective first-line treatment for seasonal
affective disorder
A fluorescent light box with light intensities greater than
2500 lux is the preferred device for light therapy
An optimal starting dose for light therapy is 10 000 lux for
30 min/day
Light boxes emitting 2500 lux are effective with a treatment
duration of 2 h/day
Morning light is more effective than evening light. Patients
should be encouraged to undergo light therapy as early as
possible (eg, before/during breakfast). However, evening
light may be effective for some patients
Many patients will respond as early as after 1 week.
However, in some cases a response may occur after only 2 to
4 weeks
If there is no sufficient response after two treatment weeks,
the dose should be doubled to 30 min in the morning plus
30 min in the evening
If this regimen does not lead to sufficient improvement,
consider adding a pharmacological treatment (best evi-
dence available for serotonin reuptake inhibitors)

Another challenge for efficacy studies on light therapy isthe “light-noise” inevitably encountered in a normal liv-ing environment. Depending on weather conditions, out-door light intensities can easily surmount the intensitiesdelivered by a light box, even in the winter.This has beencompared to a study trying to prove the superiority of anantidepressant drug over placebo, with antidepressantsoccasionally delivered through the drinking water to allstudy subjects.21 Nevertheless, today there is sound evi-dence showing that antidepressant effects of light in SADare real biological treatment effects.16,20,22
Dose
Earlier studies have mostly used light intensities of 2500lux. This is much more than the typical indoor illumina-tion, ranging from 100 lux in average rooms to about 500lux in brightly illuminated ones. Outdoor light intensitiesgreatly vary with weather conditions ranging from about2000 lux on a rainy winter day to 10 000 lux or more(usually 50 000 to 300 000 lux) in direct sunshine. Today,light treatment with intensity of 10 000 lux has becomeclinical standard. One great advantage of higher inten-sity light is that it allows for shorter exposure times.Current clinical guidelines recommend beginning treat-ment with 10 000 lux for 30 min in the morning.23
Nevertheless, intensities of 2500 lux have shown to haveantidepressant effects when applied for 2 h daily.
Timing
A further finding that emerged from BLT studies is thesuperiority of morning light over light administered inthe evening.16,20,22 By further refining timing of lightadministration in relationship to the position of the cir-cadian phase,Terman and coworkers achieved remissionrates up to 80% in selected patient populations.5 Theywere able to show that response to BLT criticallydepends on time of delivery relative to the position of thecircadian phase as determined by the onset of melatoninsecretion in the evening (dim-light melatonin onset).Thestudy suggests that the ideal therapy time is around 8.5 hafter melatonin onset.Although the superiority of morning light in the majorityof patients with SAD had been demonstrated before,16,20,22
Terman and colleagues showed that, for clinical purposes,circadian phase position can simply and reliably be deter-mined by administration of a modified version Horne-Öst-
berg morningness-eveningness scale.24 The authors alsoprovide an online-questionnaire25 together with recom-mendations for individually optimized light therapy tim-ing as based on morningness-eveningness or individual cir-cadian phase position. In summary, now there is sufficientevidence that light administered in the early morning issuperior to evening light.
Dawn stimulation
Many patients with SAD experience markedly increasedduration of sleep during the winter months.1,4,26 Usually,most of these patients have to force themselves out of bedduring the weekdays despite feeling excessively drowsy.Dawn stimulation is a form of light therapy involving grad-ually increasing bedside light in the morning before awak-ening.27 Dawn stimulation has shown to improve symp-toms of SAD compared with placebo light signals.28,29 Inaddition, dawn stimulation appears to be effective in ame-liorating the difficulty awakening and morning drowsinessin SAD.30 In a comparison study, dawn stimulation using100 to 300 lux for 60 to 90 min every morning improvedsymptoms of SAD similarly to light therapy using 1500 to2500 lux for 2 h every morning.31
Adverse effects
The adverse effects of light therapy include headache, eye-strain, nausea, and agitation.32,33 Usually, adverse effects aremild and subside spontaneously or with dose reduction.Bright light in the evening may be associated with sleepdisturbances, and, occasionally, hypomania may arise dur-ing BLT.33 However, subjective benefits of light consis-tently outweigh its adverse effects.32,33 Altogether, itremains questionable whether the frequency of thesesymptoms under BLT significantly exceeds the frequencyof side effects seen under placebo conditions.
Risks
There are no absolute contraindications for light therapy.23
Animal studies suggest increased risk for retinal damagewith lithium, β-blockers, tricyclic antidepressants, and tryp-tophan. However, no such interactions have been reportedin humans, and there is no evidence that light therapy isassociated with ocular or retinal damage in humans.Patients with severe ophthalmological conditions orpatients taking photosensitizing medication should have
Treatment of seasonal affective disorders - Praschak-Rieder and Willeit Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
391

an ophthalmological examination before starting lighttherapy. However, it is important that the UV spectrum isfiltered out of the therapeutic light source.Although suicidality is commonly regarded as being ratherinfrequent in SAD, our own group has reported severe sui-cidal ideation and suicide attempts in three patients afterthe initiation of light therapy.34 All three patients had sui-cidal thoughts before light therapy was started.As alwayswhen dealing with depressed patients, patients with SADshould be carefully assessed for suicidality before lighttherapy, and therapy outcome should frequently and reg-ularly be evaluated by health care professionals.
Treatment predictors
Atypical depressive symptoms, specifically hyperphagia,hypersomnia, and carbohydrate craving, seem to be asso-ciated with favorable response to BLT.35,36 Younger agealso seems to predict a good response,37 while comorbidpersonality disorders seem to compromise the responseto BLT.38,39
Mechanism of action
Theories on the mechanism of action of BLT are closelyconnected to what is known about the pathogenesis ofSAD.40 Two main—mutually not exclusive—theorieshave been raised by researchers in the field: one concen-trates on the evidence for reduced serotonin neuro-transmission in SAD, the other theory relates light ther-apy–induced improvement to corrections of alteredcircadian rhythms during depression in SAD.
Serotonin
Several lines of evidence suggest an alteration in serotoninneurotransmission in SAD.40-42 A keystone of the serotoninhypothesis on the mechanism of action of light therapy isthe finding that lowering brain serotonin by tryptophandepletion leads to a transient depressive relapse in patientswith SAD who are in light therapy–induced remission.43
In line with this theory is the beneficial effect of selectiveserotonin reuptake inhibitors (SSRIs) in SAD.Althoughthere is evidence for a seasonal variation in serotoninneurotransmission,44 and although there seems to be aclose relationship between brain serotonin and atypicaldepressive symptoms,41 serotonergic alterations are notspecific for the pathogenesis of SAD or the antidepres-
sant action of light.They rather seem to constitute a path-way common to depressive syndromes and their treat-ment in general.
Circadian phase shifts
More specific for SAD are the theories concerning alter-ations in circadian and circannual rhythms. Neurons of thehypothalamic suprachiasmatic nucleus (SCN) act as themain “zeitgeber” in the mammalian organism. Having anintrinsic near to 24-h rhythm, they are also known as the“internal clock.”These neurons are reset by environmen-tal light, and they are believed to be the main determinantfor the position of the circadian phase. Several body func-tions, such as hormonal rhythms, including nocturnal mela-tonin secretion, sleep, or eating behavior, are subjected toa specific circadian rhythm. The best studied marker forthe position of the circadian phase is the onset of mela-tonin secretion by the pineal gland.45 In humans, the begin-ning of melatonin secretion occurs in the evening, usuallybetween 1 and 2 h before falling asleep. Light can shift theposition of the circadian phase, and amount and directionof that shift greatly depend on the time of light exposure:light in the evening leads to a phase delay (eg, melatoninonset occurs later), morning light advances the circadianphase.20,22
Early theories on the pathogenesis of SAD held that adelay in the circadian phase was responsible for theappearance of SAD symptoms.46 Although the phase-delay hypothesis on the pathogenesis of SAD did nothold up, as there does not seem a consistent pattern ofphase alterations in SAD, recent work has shown the cir-cannual variation in circadian phase to be altered inpatients with SAD when compared with healthy controlsubjects.47 Recent work by Terman and colleaguesshowed a correlation between light-induced changes inthe “phase angle” (the relationship between the circadianphase as measured by melatonin onset and, eg, sleeponset) and antidepressant response to light in SAD.5
Practical issues
Sufficient and clear instructions to patients are critical fora satisfactory treatment response. Patients should beinformed that the beneficial effects of light are not endur-ing, ie, that a relapse is to be expected after a few dayswhen treatment is discontinued.Although one study48 sug-gested a transcutaneous effect of light on melatonin secre-
C l i n i c a l r e s e a r c h
392

tion, these results have not been replicated.49,50 It is so farsafe to state that the antidepressant effect of light is medi-ated by the eye.The patient therefore needs to make surethat light of sufficient intensity meets the eye. Light pro-jection does not need to be foveal, ie, it is not necessary tolook directly into the light source.The ideal is an angle ofabout 30° to 60° to let enough light meet the eye and allowfor the patient to, for example, read or eat during lighttherapy.The intensity of light critically depends upon thedistance from the light source. Light boxes should be pow-erful enough to deliver an intensity of about 10 000 lux ata distance of 60 to 90 cm. If the light box is less powerful,treatment time should be expanded (see above). Patientsshould be encouraged to seek exposure to environmentallight on sunny days. Sunlight has much higher intensitythan light delivered by a light therapy device (see above).Despite the fact that light therapy is now recommendedas a treatment of choice for SAD, only in Switzerland hasthe economic argument that in the long run, light ischeaper than drugs, attained government endorsementand mandatory reimbursement by medical insurance.51
The fact that there is no reimbursement for light therapyhas been widely criticized by patients with SAD, their rel-atives, and experts in the field of SAD.52 Case reports onSAD patients resistant to several antidepressants, butfinally responsive to light therapy illustrate that, althoughdepressive symptoms may often be only moderate, SADcan lead to severe impairment in occupational and socialfunctioning and can precipitate catastrophic life events.52,53
Pharmacotherapy
Although light therapy is recommended as the first-lineoption for SAD, some patients do not experience suffi-cient relief of depressive symptoms with light. BLT canthen be supplemented with antidepressant drugs. Otherpatients with SAD feel unable to integrate light therapyinto their daily routine, or other logistical difficulties inadministering light therapy are present.The evidence ofSAD being associated with a dysfunction in brain sero-tonin systems has guided the search for promising phar-macological treatments of SAD. Data emerging frommulticenter placebo-controlled trials has led to the rec-ommendation of the SSRIs sertraline and fluoxetine asfirst-line treatments of SAD. Other antidepressant com-pounds, like monoamine oxidase inhibitors, dopaminer-gic and noradrenergic agents, melatonin, β-blockers asmelatonin antagonists, herbs, and nutritional supplements
like L-tryptophan and vitamin D have been investigatedin small studies.The efficacy of these medications has notyet been proven in SAD. Open trials, controlled studies,and placebo-controlled studies in SAD are listed inTables III to V.54-75 New pharmacological agents are ofpotential value in the treatment of SAD, for example,agomelatine (Valdoxan).This new dual melatonergic andspecific serotonergic antidepressant has been shown tobe efficient in the treatment of major depression76: itexhibits a specific core action on circadian rhythms, andtherefore could be of particular value in the treatment ofSAD. More specific studies are underway to more obtaininformation about its activity in SAD.
Open studies
A survey of open studies in SAD is given in Table III.54-61
There is some suggestion from pilot data with small sam-ple sizes that serotonergic agents like fluoxetine, citalo-pram, and trazodone may be treatment options forSAD.54,57 Tranylcypromine, a nonselective monoamine oxi-dase inhibitor was effective in the treatment of 14 patientsleading to an average 91% reduction in depressive symp-toms within 4 weeks of initiation of treatment.55 A studyin 20 patients indicates that St John’s wort (Hypericumperforatum) may be helpful in treating SAD. An add-ontherapy with bright light in 10 of these patients treatedwith hypericum did not lead to a significantly better treat-ment outcome.59 Two studies in 6 patients each report ben-eficial effects of the benzodiazepine alprazolam.56,60 A 6-week open trial investigating efficacy and tolerability ofreboxetine, a selective noradrenaline reuptake inhibitor,led to rapid full remission of depressive symptoms in 11out of 16 patients.61 A rapid relief of preexistent severeatypical symptoms was observed in 9 patients within the
Treatment of seasonal affective disorders - Praschak-Rieder and Willeit Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
393
Table III. Open studies of pharmacotherapy of seasonal affective disorder(SAD).54-61
Authors Number Medication
of patients
Jacobsen et al,54 1989 n=3 Fluoxetine, trazodone
Dilsaver and Jaeckle,55 1990 n=14 Tranylcypromine
Teicher and Glod,56 1990 n=6 Alprazolam
Wirz-Justice et al,57 1992 n=1 Citalopram
Lingjaerde et al,58 1993 n=5 Moclobemide
Martinez et al,59 1994 n=20 Hypericum
Yamadera et al,60 2001 n=6 Alprazolam
Hilger et al,61 2001 n=16 Reboxetine

first week of treatment. This finding is of pathophysio-logical interest since, so far, atypical depressive symptomslike increased appetite, carbohydrate craving, and hyper-somnia have been strongly associated with a dysfunctionin brain serotonin systems.
Controlled studies
Controlled studies of pharmacotherapy in SAD are pre-sented in Table IV.62-66 A study by Ruhrmann et al com-paring the SSRI fluoxetine and light therapy in 40patients with SAD found no significant difference intreatment outcome between the groups, but a fasteronset of antidepressant action in the light therapygroup.63
Because SAD is prevalent in winter when vitamin Dstores are typically low, and because light therapyincludes wavelengths that allow the skin to produce vit-amin D, the potential role of vitamin D in SAD has beeninvestigated in a small pilot study.65 Vitamin D wasreported to lead to a greater improvement of depressivesymptoms than light therapy. However, no difference invitamin D levels has been observed between patientswith SAD and healthy subjects,70,77 and the antidepressanteffect of light therapy has been shown to be independentof changes in vitamin D levels.77 So far, any benefits ofvitamin D on SAD remain unproven. In two small, pre-liminary trials, 4 to 6 g daily doses of the amino acid L-tryptophan, the precursor of serotonin, were as effectiveas light therapy.62,64 In a postal survey using an 11-itemrating scale, 301 patients with SAD treated with hyper-icum at 300 mg three times daily for 8 weeks were askedto report changes in their symptoms.66 Of these patients,
133 used additional light therapy. Significant overallimprovement was reported in both treatment groups.Improvement in sleep was greater in the hypericum andlight therapy group. However, double-blind research isneeded to confirm the usefulness of hypericum (St John’swort) for treating SAD.
Placebo-controlled studies
Table V58,67-75 presents placebo-controlled studies of phar-macotherapy in SAD. The best evidence for efficacy ofantidepressants in SAD comes from studies of SSRIs.Multicenter, double-blind, randomized studies of fluox-etine and sertraline confirm that these medications areeffective in the treatment of SAD. In the fluoxetine study(68 patients), significant improvement in mood was pre-sent in both fluoxetine and placebo-treated patients attermination of the study. However, there was significantsuperiority of fluoxetine over placebo in the clinicalresponse rates (59% versus 34%, respectively).71 In thesertraline study (187 patients), a significant superiority toplacebo in both clinical response rates (62% versus 46%,respectively) and depression scores was found.Althoughthey have been widely cited, the data from the sertralinestudy have only been published as an abstract so far.78 Adouble-blind study by Lingjaerde et al58 investigating theefficacy of moclobemide, a reversible inhibitor ofmonoamine oxidase A, versus placebo over 14 weeksfound no significant difference in depression scoresbetween groups at study termination. However, withinthe first week of treatment, patients in the moclobemidegroup, but not in the placebo group, had a significantreduction in atypical depression symptoms. Testing the
C l i n i c a l r e s e a r c h
394
Table IV. Controlled studies of pharmacotherapy of seasonal affective disorder (SAD).62-66 LT, light therapy.
Authors Number of patients Medication and study design Outcome
McGrath et al,62 1990 n=13 L-Tryptophan and LT No significant difference
versus L-tryptophan alone
Ruhrmann et al,63 1998 n=40 Fluoxetine versus LT No significant difference,
but faster onset of antidepressant
action in LT group
Ghadirian et al,64 1998 n=13 L-Tryptophan versus LT, No significant difference
crossover study
Gloth et al,65 1999 n=15 Vitamin D versus LT Vitamin D superior to LT
Wheatley,66 1999 n=168 Hypericum and LT Significant improvement in both
versus hypericum alone groups, improvement in sleep greater
in hypericum and LT group

Treatment of seasonal affective disorders - Praschak-Rieder and Willeit Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
395
hypothesis that a dopaminergic deficiency plays a role inthe pathophysiology of SAD, Oren et al conducted asmall study investigating the efficacy of levodopa pluscarbidopa as a treatment for SAD.68 No differences toplacebo were found in the rates of response. The mela-tonin hypothesis of SAD was tested in two studies usingthe β-blockers atenolol67 and propanolol69 to suppressmelatonin secretion. No difference in antidepressant effi-cacy was found between atenolol and placebo. Propanololwas superior to placebo in preventing a depressive relapsein patients with SAD who had previously responded to anopen treatment with propanolol. Supplementation withmelatonin has shown to be ineffective in patients withSAD when taken at night or in the morning.79 Melatoninhas also been reported to even reverse the benefits oflight therapy.80 However, a small pilot study with lowdoses of melatonin in the afternoon showed a significantdecrease in depression ratings compared to placebo.72
The authors argue that a replication of this finding in anadequate sample with documentation of expected phaseshifts would substantially support the phase shift hypoth-esis of SAD.A recent 1-year pilot study73 aimed at inves-tigating possible advantages of combining light therapywith the SSRI citalopram. No significant group difference
was found during the initial 10-day light therapy period.However, during the follow-up period depression ratingswere significantly lower in the citalopram group com-pared with the placebo group.The authors conclude thatlight therapy with continued SSRI treatment may be auseful strategy to achieve beneficial long-term effects inpatients with SAD. A study by Lingjaerde et al74 testingthe hypothesis that Ginkgo biloba extract may preventthe symptoms of winter depression in patients with SADyielded negative results. In a recent study metergoline,a nonspecific serotonin antagonist, did not demonstratea sustained significant effect on mood compared withplacebo.75
General management issues
Since there is little evidence comparing light therapy withantidepressant medication, the choice between these alter-natives relies on individual assessment of risks and bene-fits.23 Generally, light therapy is very well accepted bypatients.Availability and costs of a light therapy device aresometimes limiting factors, as is the time patients need tocommit for daily light therapy. However, BLT should beconsidered first-line treatment for moderately depressed
Table V. Placebo-controlled studies of pharmacotherapy of seasonal affective disorder (SAD).58,67-75 LT, light therapy.
Authors Number of patients Medication and study design Outcome
Rosenthal et al,67 1988 n=19 Atenolol versus placebo No significant difference
Lingjaerde et al,58 1993 n=34 Moclobemide versus placebo No significant difference, but
significant reduction of atypical
symptoms in moclobemide group
Oren et al,68 1994 n=25 Levodopa + carbidopa No significant difference
versus placebo
Schlager,69 1994 n=23 Propanolol versus placebo Significantly higher relapse rates in
placebo group
Oren et al,70 1994 n=27 Vitamin B12 (cyanocobalamine) No significant difference
versus placebo
Lam et al,71 1995 n=78 Fluoxetine versus placebo No significant difference, higher
response rate in fluoxetine group
Lewy et al,72 1998 n=10 Melatonin versus placebo Melatonin superior to placebo
Thorell et al,73 1999 n=8 LT and citalopram No significant difference between
versus LT and placebo citalopram and placebo during LT;
after LT citalopram superior to placebo
Lingjaerde et al,74 1999 n=27 Ginkgo biloba versus placebo No significant difference; gingko
significant more effective in
preventing new depressive episodes
Turner et al,75 2002 n=16 Metergoline versus placebo No significant difference

C l i n i c a l r e s e a r c h
396
Tratamiento de los trastornos afectivos estacionales
El trastorno afectivo estacional (TAE) es un subtipodel trastorno depresivo mayor recurrente o del tras-torno bipolar, con una aparición regular de episodiosdepresivos en cierta época del año, especialmente eninvierno. El tratamiento del TAE es similar al de otrostipos de trastorno afectivo, excepto que la terapiacon luz brillante se recomienda como opción de pri-mera línea. Convencionalmente la terapia lumínicase refiere a la exposición a luz visible de al menos2500 lux de intensidad a nivel del ojo. Se piensa quelos efectos de la fototerapia son mediados exclusi-vamente por los ojos, no por la piel, aunque estahipótesis no ha sido aun verificada. La terapia lumí-nica matinal ha probado ser superior a las aplicacio-nes vespertinas. Los porcentajes de respuesta a lafototerapia son cercanos al 80% en poblacionesseleccionadas de pacientes y los síntomas depresivosatípicos son el mejor predictor de una evoluciónfavorable al tratamiento. Datos de ensayos contro-lados, randomizados sugieren que los antidepresivosson efectivos en el tratamiento del TAE. Se han rea-lizado tres estudios doble ciego, controlados con pla-cebo que han mostrado resultados promisorios paralos inhibidores selectivos de la recaptación de sero-tonina (ISRS) sertralina y fluoxetina, y también paramoclobemida, un inhibidor reversible de la monoa-mino-oxidasa A.
Traitement du trouble affectif saisonnier
Le trouble affectif saisonnier (TAS) représente unsous-groupe des troubles dépressif majeur récurrentou bipolaire et se caractérise par l’installation régu-lière d’épisodes dépressifs à certaines périodes del’année, généralement en hiver. Le traitement duTAS est semblable à celui des autres formes de trou-bles affectifs, si ce n’est que la photothérapie àlumière vive est recommandée en première inten-tion. La photothérapie conventionnelle impliquel’exposition à une lumière du spectre visible d’uneintensité supérieure à 2 500 lux au niveau de l’œil.Les effets de la photothérapie sont considéréscomme médiés exclusivement par les yeux et non lapeau, bien que cette hypothèse n’ait pas encore étévérifiée. La photothérapie matinale s’est avéréesupérieure au schéma thérapeutique vespéral. Lestaux de réponse à la photothérapie sont d’environ80 % dans des populations sélectionnées de patients,les symptômes dépressifs atypiques étant le meilleurfacteur prédictif d’évolution thérapeutique favora-ble. Des données issues d’études randomisées,contrôlées, suggèrent que les antidépresseurs sontefficaces dans le traitement du TAS. Trois études endouble aveugle, contre placebo, ont été réalisées,montrant des résultats prometteurs pour les inhibi-teurs sélectifs de la recapture de la sérotonine (ISRS),la sertraline et la fluoxétine, ainsi que pour un inhi-biteur de la monoamine oxydase sélectif A (IMAOsélectif A), le moclobémide.
patients and patients with prominent atypical depressivesymptoms. Generally, light therapy alone or in combina-tion with antidepressants should be given for the durationof the dark time of year, ie, until April or May in the north-ern hemisphere.A trial of light therapy should last at least2 to 4 weeks. A trial of antidepressants should last 4 to 6weeks. Light therapy and medication trials should beapplied sequentially, as combining them from the begin-ning on will lead to a loss of information about whichtreatment is beneficial, or which treatment is causing sideeffects.A combination of both treatments should be con-
sidered if there is insufficient response to either pharma-cological or light treatment. If a depressive episode is resis-tant to the combination of BLT and an antidepressant,options are lengthening light treatment time, raising thedose of the antidepressant, or switching to a drug of a dif-ferent class.Although there are no specific data availablefor SAD, treatment should follow algorithms for treat-ment-resistant depression if a sufficient response still can-not be achieved. Pharmacological augmentation strategies,electroconvulsive therapy, or sleep deprivation proce-dures81 should then be considered. ❏

Treatment of seasonal affective disorders - Praschak-Rieder and Willeit Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
397
REFERENCES
1. Rosenthal NE, Sack DA, Gillin JC, et al. Seasonal affective disorder. Adescription of the syndrome and preliminary findings with light therapy.Arch Gen Psychiatry. 1984;41:72-80.2. American Psychiatric Association. Diagnostic and Statistical Manual of MentalDisorders. 4th ed. Washington, DC: American Psychiatric Association; 1994.3. Kasper S, Wehr TA, Bartko JJ, Gaist PA, Rosenthal NE. Epidemiologicalfindings of seasonal changes in mood and behavior. A telephone survey ofMontgomery County, Maryland. Arch Gen Psychiatry. 1989;46:823-833.4. Winkler D, Willeit M, Praschak-Rieder N, et al. Changes of clinical pat-tern in seasonal affective disorder (SAD) over time in a German-speakingsample. Eur Arch Psychiatry Clin Neurosci. 2002;252:54-62.5. Terman JS, Terman M, Lo ES, Cooper TB. Circadian time of morning lightadministration and therapeutic response in winter depression. Arch GenPsychiatry. 2001;58:69-75.6. Michalak EE, Hayes S, Wilkinson C, Hood K, Dowrick C. Treatment com-pliance in light therapy. Do patients do as they say they do? J Affect Disord.2002;68:341-342.7. Horowitz TS, Tanigawa T. Circadian-based new technologies for nightworkers. Ind Health. 2002;40:223-236.8. Burgess HJ, Sharkey KM, Eastman CI. Bright light, dark and melatonincan promote circadian adaptation in night shift workers. Sleep Med Rev.2002;6:407-420.9. Graf A, Wallner C, Schubert V, et al. The effects of light therapy on mini-mental state examination scores in demented patients. Biol Psychiatry.2001;50:725-727.10. Ancoli-Israel S, Martin JL, Kripke DF, Marler M, Klauber MR. Effect oflight treatment on sleep and circadian rhythms in demented nursing homepatients. J Am Geriatr Soc. 2002;50:282-299.11. Terman M, Lewy AJ, Dijk DJ, Boulos Z, Eastman CI, Campbell SS. Lighttreatment for sleep disorders: consensus report. IV. Sleep phase and dura-tion disturbances. J Biol Rhythms. 1995;10:135-147.12. Montgomery P, Dennis J. Bright light therapy for sleep problems inadults aged 60+. Cochrane Database Syst Rev. 2002:CD003403.13. Loving RT, Kripke DF, Shuchter SR. Bright light augments antidepres-sant effects of medication and wake therapy. Depress Anxiety. 2002;16:1-3.14. Oren DA, Wisner KL, Spinelli M, et al. An open trial of morning light ther-apy for treatment of antepartum depression. Am J Psychiatry. 2002;159:666-669.15. Benedetti F, Colombo C, Pontiggia A, Bernasconi A, Florita M, SmeraldiE. Morning light treatment hastens the antidepressant effect of citalopram:a placebo-controlled trial. J Clin Psychiatry. 2003;64:648-653.16. Terman M, Terman JS, Quitkin FM, McGrath PJ, Stewart JW, Rafferty B.Light therapy for seasonal affective disorder. A review of efficacy.Neuropsychopharmacology. 1989;2:1-22.17. Thompson C, Rodin I, Birtwhistle J. Light therapy for seasonal and non-seasonal affective disorder: a Cochrane meta-analysis. Soc Light TreatmentBiol Rhythms Abstr. 1999:11. Abstract.18. Eastman CI, Young MA, Fogg LF, Liu L, Meaden PM. Bright light treat-ment of winter depression: a placebo-controlled trial. Arch Gen Psychiatry.1998;55:883-889.19. Eastman CI, Lahmeyer HW, Watell LG, Good GD, Young MA. A placebo-controlled trial of light treatment for winter depression. J Affect Disord.1992;26:211-221.20. Terman M, Terman JS, Ross DC. A controlled trial of timed bright lightand negative air ionization for treatment of winter depression. Arch GenPsychiatry. 1998;55:875-882.21. Avery DH. A turning point for seasonal affective disorder and light ther-apy research? Arch Gen Psychiatry. 1998;55:863-864.22. Lewy AJ, Bauer VK, Cutler NL, et al. Morning vs evening light treatmentof patients with winter depression. Arch Gen Psychiatry. 1998;55:890-896.23. Lam RW, Levitt AJ. Canadian Consensus Guidelines for the Treatment ofSAD. A Summary of the Report of the Canadian Consensus Group on SAD.Vancouver, Canada: Clinical & Academic Publishing; 1999.24. Horne JA, Östberg O. A self-assessment questionnaire to determinemorningness-eveningness in human circadian rhythms. Int J Chronobiol.1976;4:97-110.
25. The Automated Morningness-Eveningness Questionnaire. Available at:http://www.cet.org. Norwood, NJ: Center for Environmental Therapeutics.Accessed 22 September 2003.26. Thalen BE, Kjellman BF, Morkrid L, Wetterberg L. Seasonal and non-seasonal depression. A comparison of clinical characteristics in Swedishpatients. Eur Arch Psychiatry Clin Neurosci. 1995;245:101-108.27. Terman M, Schlager D, Fairhurst S, Perlman B. Dawn and dusk simula-tion as a therapeutic intervention. Biol Psychiatry. 1989;25:966-970.28. Avery DH, Bolte MA, Dager SR, et al. Dawn simulation treatment ofwinter depression: a controlled study. Am J Psychiatry. 1993;150:113-117.29. Avery DH, Bolte MA, Wolfson JK, Kazaras AL. Dawn simulation com-pared with a dim red signal in the treatment of winter depression. BiolPsychiatry. 1994;36:180-188.30. Avery DH, Kouri ME, Monaghan K, Bolte MA, Hellekson C, Eder D. Isdawn simulation effective in ameliorating the difficulty awakening in sea-sonal affective disorder associated with hypersomnia? J Affect Disord.2002;69:231-236.31. Lingjaerde O, Foreland AR, Dankertsen J. Dawn simulation vs lightboxtreatment in winter depression: a comparative study. Acta Psychiatr Scand.1998;98:73-80.32. Terman M, Terman JS. Bright light therapy: side effects and benefitsacross the symptom spectrum. J Clin Psychiatry. 1999;60:799-808. Quiz 809.33. Labbate LA, Lafer B, Thibault A, Sachs GS. Side effects induced by brightlight treatment for seasonal affective disorder. J Clin Psychiatry. 1994;55:189-191.34. Praschak-Rieder N, Neumeister A, Hesselmann B, Willeit M, Barnas C,Kasper S. Suicidal tendencies as a complication of light therapy for sea-sonal affective disorder: a report of three cases. J Clin Psychiatry.1997;58:389-392.35. Oren DA, Jacobsen FM, Wehr TA, Cameron CL, Rosenthal NE. Predictorsof response to phototherapy in seasonal affective disorder. ComprPsychiatry. 1992;33:111-114.36. Terman M, Amira L, Terman JS, Ross DC. Predictors of response andnonresponse to light treatment for winter depression. Am J Psychiatry .1996;153:1423-1429.37. Lam RW. Morning light therapy for winter depression: predictors ofresponse. Acta Psychiatr Scand. 1994;89:97-101.38. Reichborn-Kjennerud T, Lingjaerde O. Response to light therapy in sea-sonal affective disorder: personality disorders and temperament as pre-dictors of outcome. J Affect Disord. 1996;41:101-110.39. Levitt AJ, Joffe RT, Brecher D, MacDonald C. Anxiety disorders and anx-iety symptoms in a clinic sample of seasonal and non-seasonal depressives.J Affect Disord. 1993;28:51-56.40. Lam RW, Levitan RD. Pathophysiology of seasonal affective disorder: areview. J Psychiatry Neurosci. 2000;25:469-480.41. Neumeister A, Konstantinidis A, Praschak-Rieder N, et al.Monoaminergic function in the pathogenesis of seasonal affective disor-der. Int J Neuropsychopharmacol. 2001;4:409-420.42. Willeit M, Praschak-Rieder N, Neumeister A, et al. [123I]-Beta-CIT SPECTimaging shows reduced brain serotonin transporter availability in drug-free depressed patients with seasonal affective disorder. Biol Psychiatry.2000;47:482-489.43. Neumeister A, Praschak-Rieder N, Besselmann B, Rao ML, Gluck J,Kasper S. Effects of tryptophan depletion on drug-free patients with sea-sonal affective disorder during a stable response to bright light therapy.Arch Gen Psychiatry. 1997;54:133-138.44. Neumeister A, Pirker W, Willeit M, et al. Seasonal variation of avail-ability of serotonin transporter binding sites in healthy female subjects asmeasured by [123I]-2 beta-carbomethoxy-3 beta-(4-iodophenyl)tropane andsingle photon emission computed tomography. Biol Psychiatry. 2000;47:158-160.45. Lewy AJ, Cutler NL, Sack RL. The endogenous melatonin profile as amarker for circadian phase position. J Biol Rhythms. 1999;14:227-236.46. Lewy AJ, Sack RL, Miller LS, Hoban TM. Antidepressant and circadianphase-shifting effects of light. Science. 1987;235:352-354.47. Wehr TA, Duncan WC, Jr, Sher L, et al. A circadian signal of change ofseason in patients with seasonal affective disorder. Arch Gen Psychiatry.2001;58:1108-1114.

C l i n i c a l r e s e a r c h
398
48. Campbell SS, Murphy PJ. Extraocular circadian phototransduction inhumans. Science. 1998;279:396-399.49. Lockley SW, Skene DJ, Thapan K, et al. Extraocular light exposure doesnot suppress plasma melatonin in humans. J Clin Endocrinol Metab.1998;83:3369-3372.50. Eastman CI, Martin SK, Hebert M. Failure of extraocular light to facili-tate circadian rhythm reentrainment in humans. Chronobiol Int.2000;17:807-826.51. Wirz-Justice A. Beginning to see the light. Arch Gen Psychiatry.1998;55:861-862.52. Kanofsky JD, Aspengren KL, Watts GR. Medicaid reimbursement forlight therapy. Am J Psychiatry. 2003;160:796-797.53. Ibatoullina E, Praschak-Rieder N, Kasper S. Severe atypical symptomswithout depression in SAD: effects of bright light therapy. J Clin Psychiatry.1997;58:495.54. Jacobsen FM, Murphy DL, Rosenthal NE. The role of serotonin in sea-sonal affective disorder and the antidepressant response to phototherapy.In: Rosenthal NE, Blehar MC, eds. Seasonal Affective Disorder andPhototherapy. New York, NY: Guilford; 1989:333-341.55. Dilsaver SC, Jaeckle RS. Winter depression responds to an open trial oftranylcypromine. J Clin Psychiatry. 1990;51:326-329.56. Teicher MH, Glod CA. Seasonal affective disorder: rapid resolution bylow-dose alprazolam. Psychopharmacol Bull. 1990;26:197-202.57. Wirz-Justice A, van der Velde P, Bucher A, Nil R. Comparison of lighttreatment with citalopram in winter depression: a longitudinal single casestudy. Int Clin Psychopharmacol. 1992;7:109-116.58. Lingjaerde O, Reichborn-Kjennerud T, Haggag A, Gartner I, Narud K,Berg EM. Treatment of winter depression in Norway. II. A comparison ofthe selective monoamine oxidase A inhibitor moclobemide and placebo.Acta Psychiatr Scand. 1993;88:372-380.59. Martinez B, Kasper S, Ruhrmann S, Moller HJ. Hypericum in the treat-ment of seasonal affective disorders. J Geriatr Psychiatry Neurol. 1994;7(suppl1):S29-S33.60. Yamadera H, Okawa M, Takahashi K. Open study of effects of alpra-zolam on seasonal affective disorder. Psychiatry Clin Neurosci. 2001;55:27-30.61. Hilger E, Willeit M, Praschak-Rieder N, Stastny J, Neumeister A, KasperS. Reboxetine in seasonal affective disorder: an open trial. EurNeuropsychopharmacol. 2001;11:1-5.62. McGrath RE, Buckwald B, Resnick EV. The effect of L-tryptophan on sea-sonal affective disorder. J Clin Psychiatry. 1990;51:162-163.63. Ruhrmann S, Kasper S, Hawellek B, et al. Effects of fluoxetine versusbright light in the treatment of seasonal affective disorder. Psychol Med.1998;28:923-933.64. Ghadirian AM, Murphy BE, Gendron MJ. Efficacy of light versus trypto-phan therapy in seasonal affective disorder. J Affect Disord. 1998;50:23-27.65. Gloth FM, 3rd, Alam W, Hollis B. Vitamin D vs broad spectrum pho-totherapy in the treatment of seasonal affective disorder. J Nutr HealthAging. 1999;3:5-7.
66. Wheatley D. Hypericum in seasonal affective disorder (SAD). Curr MedRes Opin. 1999;15:33-37.67. Rosenthal NE, Jacobsen FM, Sack DA, et al. Atenolol in seasonal affec-tive disorder: a test of the melatonin hypothesis. Am J Psychiatry.1988;145:52-56.68. Oren DA, Moul DE, Schwartz PJ, Wehr TA, Rosenthal NE. A controlledtrial of levodopa plus carbidopa in the treatment of winter seasonal affec-tive disorder: a test of the dopamine hypothesis. J Clin Psychopharmacol.1994;14:196-200.69. Schlager DS. Early-morning administration of short-acting β-blockersfor treatment of winter depression. Am J Psychiatry. 1994;151:1383-1385.70. Oren DA, Schulkin J, Rosenthal NE. 1,25-(OH)2-Vitamin D3 levels in sea-sonal affective disorder: effects of light. Psychopharmacology (Berl).1994;116:515-516.71. Lam RW, Gorman CP, Michalon M, et al. Multicenter, placebo-controlledstudy of fluoxetine in seasonal affective disorder. Am J Psychiatry.1995;152:1765-1770.72. Lewy AJ, Bauer VK, Cutler NL, Sack RL. Melatonin treatment of winterdepression: a pilot study. Psychiatry Res. 1998;77:57-61.73. Thorell LH, Kjellman B, Arned M, Lindwall-Sundel K, Walinder J,Wetterberg L. Light treatment of seasonal affective disorder in combina-tion with citalopram or placebo with 1-year follow-up. Int ClinPsychopharmacol. 1999;14(suppl 2):S7-S11.74. Lingjaerde O, Foreland AR, Magnusson A. Can winter depression beprevented by Ginkgo biloba extract? A placebo-controlled trial. ActaPsychiatr Scand. 1999;100:62-66.75. Turner EH, Schwartz PJ, Lowe CH, et al. Double-blind, placebo-con-trolled study of single-dose metergoline in depressed patients with sea-sonal affective disorder. J Clin Psychopharmacol. 2002;22:216-220.76. Lôo H, Hale A, D’haenen H. Determination of the dose of agomelatine,a melatoninergic agonist and selective 5-HT2c antagonist, in the treatmentof major depressive disorder: a placebo-controlled dose range study. IntClin Psychopharmacol. 2002;17:239-247.76. Partonen T, Vakkuri O, Lamberg-Allardt C, Lonnqvist J. Effects of brightlight on sleepiness, melatonin, and 25-hydroxyvitamin D(3) in winter sea-sonal affective disorder. Biol Psychiatry. 1996;39:865-872.77. Moscovitch A, Blashko C, Wiseman R. A double-blind, placebo-controlledstudy of sertraline in patients with seasonal affective disorder. New ResearchAbstracts, 151st Meeting of the American Psychiatric Association. Toronto,Canada.1995. Abstract.78. Wirz-Justice A, Graw P, Krauchi K, et al. Morning or night-time melatoninis ineffective in seasonal affective disorder. J Psychiatr Res. 1990;24:129-137.79. Rosenthal NE, Sack DA, Jacobsen FM, et al. Melatonin in seasonal affec-tive disorder and phototherapy. J Neural Transm Suppl. 1986;21:257-267.80. Graw P, Haug HJ, Leonhardt G, Wirz-Justice A. Sleep deprivationresponse in seasonal affective disorder during a 40-h constant routine. JAffect Disord. 1998;48:69-74.

399
C l i n i c a l r e s e a r c h
Clinical applications of melatonin in circadian disordersAlfred J. Lewy, MD, PhD
Keywords: melatonin; circadian phase; seasonal affective disorder; circadiansleep disorder; the blind; jet lag; shift work
Author affiliations: Sleep and Mood Disorders Laboratory, Oregon HealthScience University, Portland, Ore, USA
Address for correspondence: Sleep and Mood Disorders Laboratory,Oregon Health Science University, 3181 SW Sam Jackson Park Road,Portland, OR 97239, USA (e-mail: [email protected])
Chronobiological disorders and syndromes include sea-sonal affective disorder (SAD), total blindness, advancedand delayed sleep phase syndrome, jet lag, and shiftwork maladaptation. These disorders are treated byadjusting circadian phase, using appropriately timedbright light exposure and melatonin administration (atdoses of 0.5 mg or less). In some cases, it may be neces-sary to measure internal circadian phase, using the timewhen endogenous melatonin levels rise. © 2003, LLS SAS Dialogues Clin Neurosci. 2003;5:399-413.
Copyright © 2003 LLS SAS. All rights reserved www.dialogues-cns.org
elatonin appears to be useful in two ways to thefield of human chronobiology. One role is as a marker forbiological rhythms.The other role is as a circadian phase-shifting agent. Both roles appear to be important.In virtually all organisms, melatonin is produced mainlyduring nighttime darkness.1,2 In most vertebrates, circu-lating melatonin levels are derived exclusively from thepineal gland.3,4 In most mammals, the changing durationof melatonin production throughout the year is the cuefor seasonal rhythms.5 In some mammals, such ashumans, a feedback loop exists between melatonin andthe endogenous circadian pacemaker.6-13
An approximately 24-h (hence, circadian) rhythm inmelatonin is generated by 12 h of (usually daytime) inhi-bition of an otherwise constantly “on” signal from theparaventricular nucleus of the hypothalamus.14 This inhi-bition comes from the endogenous circadian pacemaker,located in the suprachiasmatic nucleus (SCN).15-17 Thepineal gland is then stimulated to produce melatonin forabout 12 h via a neural pathway that traverses throughthe intermedullary column and thoracic sympathetic out-flow (Figure 1).18 Preganglionic neurons synapse in thesuperior cervical ganglion with postganglionic neuronsthat enter the cranium and innervate pinealocytes.19 Thelatter release the sympathetic neurotransmitter, norepi-nephrine, which stimulates β1-adrenergic receptors andresults in the synthesis and secretion of melatonin, whichis then released into blood and cerebrospinal fluid(CSF).20 Receptors for melatonin have been identified ina number of sites, including the SCN.21,22
The approximately 24-h rhythm generated by the SCNbecomes precisely 24 h via photic input from ganglioncells in the retina.23,24 At least one novel photoreceptorhas been identified that mediates circadian entrain-ment.25 The pathway from the retina to the hypothala-mus, the retinohypothalamic tract, is different from thatwhich mediates vision.26
M

The light/dark cycle synchronizes the SCN, and there-fore its many driven circadian rhythms, to the 24-hday.27,28 Unique to melatonin, light acutely suppresses itsproduction.29 Thus, if the SCN has not turned off mela-tonin production in the morning, exposure to light will.Also, light exposure at the end of the day will suppressthe evening rise in melatonin production.30
These effects of light shape the melatonin profile. Asmentioned above, annual rhythms common to manymammals receive their seasonal time cue from the chang-ing duration of melatonin production, thought to definethe “biological night.” Whether or not humans haveimportant seasonal rhythms is a matter of some contro-versy.31,32 If humans have important seasonal rhythms, itis thought that the duration of melatonin productionwould regulate them. Not controversial is the fact that,similar to other animals, humans have circadian rhythmsthat are primarily regulated by the light/dark cycle.30,33-38
The endogenous melatonin profile as amarker for circadian phase position
In humans, the melatonin profile is the most reliablemarker for circadian phase (Figure 2).39-41 The time thatmelatonin levels rise appears to be a useful phase maker.The melatonin onset (MO) is a clearly demarcatedevent. It can be operationally defined in a number ofways, some of which use a threshold (2 pg/mL, 10 pg/mL,etc), which appears as a subscript in the acronym.42
In order to minimize the acute suppressant effect oflight, plasma samples are collected under dim light (opti-mally, less than 30 lux). Therefore, in sighted people this marker is called the dim light melatonin onset(DLMO).43 The plasma DLMO10 occurs on average
about 14 h after waketime in entrained, sighted people,and the DLMO2 occurs about 1 h earlier.13,44,45
The light zeitgeber (German for time-giver, or time cue)first occurs each day at waketime.46 In the circadian lit-erature, this is called zeitgeber time 0 (ZT 0). (Sometimesthe term circadian time [CT] is used under certain cir-cumstances; although they are technically different, ZTand CT will be used interchangeably in this monograph,in order to minimize confusion on the part of readerswho are not experts in chronobiology.) As mentionedabove, the average CT or ZT of the plasma DLMO10 is14 h in entrained, sighted people. The DLMO ZT alsodescribes the relationship between the circadian rhythmsthat are tightly coupled to the SCN (such as melatonin)and those that are more loosely coupled (such as the
C l i n i c a l r e s e a r c h
400
Selected abbreviations and acronymsASPS advanced sleep phase syndromeBFR blind free-runnerCSD circadian sleep disorderCT circadian timeDLMO dim light melatonin onsetDSPS delayed sleep phase syndromeMO melatonin onsetPRC phase response curvePSH phase shift hypothesisSAD seasonal affective disorderSCN suprachiasmatic nucleusZT zeitgeber time
Figure 1. Schematic diagram depicting neuroanatomic regulation ofmammalian melatonin production.Reproduced from reference 18: Vessely LH, Lewy AJ. Melatonin as a hor-mone and as a marker for circadian phase position in humans. In: PfaffD, Arnold A, Etgen A, Fahrbach S, Rubin R, eds. Hormones, Brain andBehavior, Vol 5. San Diego, Calif: Elsevier Science; 2002:121-141.Copyright © 2002, Elsevier Science.
Neuroanatomy of the circadian system
Pinealgland
Retinohypothalamictract
Paraventricularnucleus
Superiorcervicalganglion
Suprachiasmaticnuclei
Thoracicintermediolateral nuclei

sleep/wake cycle, for example, waketime).Therefore, anymismatch in circadian rhythms will be reflected in a ZTthat differs from the 14-h standard.
The light PRC
Light’s phase-shifting effects on circadian rhythms canbe explained by a phase response curve (PRC). Its essen-tial features are that light exposure in the morning causesa phase advance (shift to an earlier time) and that lightexposure in the evening causes a phase delay (shift to alater time).33,36,47 In addition, maximal phase shifts occurin the middle of the night, and minimal phase shifts occurduring the middle of the day.48-51 PRCs are usually plot-ted according to CT. The break points that separateadvance and delay responses for the light PRC are 12 hapart: they occur at CT 6 and CT 18. Converting to clocktime for an individual who habitually awakens at 7.00AM, these are 1.00 PM and 1.00 AM, respectively. Withregard to the light PRC, there are several investigatorswho think that these break points occur a few hourslater.52 The jury is out on this question.
As mentioned above, light is the most potent circadianzeitgeber in virtually all organisms. However, this was notfully appreciated in humans until it was shown thathumans require brighter light for this effect than otheranimals, which was dramatically demonstrated withrespect to acute suppression of melatonin production.53
The phase-shifting and suppressant effects of light arethought to be closely associated. Since sunlight (10 000-100 000 lux) is usually brighter than indoor light, humansmight be responding to the natural light/dark cycle, rela-tively unaffected by ordinary-intensity indoor light (200-500 lux).A second implication is that bright artificial lightcould be substituted for sunlight, in order to experimen-tally (and perhaps therapeutically) manipulate biologi-cal rhythms in humans.
Winter depression (SAD)
One of the first therapeutic uses of bright light was totreat winter depression, or seasonal affective disorder(SAD).54,55 Bright light has also been used to treat non-seasonal depression,56 which is reviewed elsewhere (see
Clinical applications of melatonin - Lewy Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
401
Figure 2. Relationship between the endogenous melatonin profile, the melatonin phase response curve (PRC), and the sleep/wake cycle. MO, mela-tonin onset; BFR, blind free-runner; CT, circadian time.Adapted from reference 41: Lewy AJ, Bauer VK, Hasler BP, Kendall AR, Pires MLN, Sack RL. Capturing the circadian rhythms of free-running blind people with0.5 mg melatonin. Brain Res. 2001;918:96-100. Copyright © 2001, Elsevier Science BV.
CT 18 CT 18
Relationship between thesleep/wake cycle and theendogenous melatoninprofile/melatonin PRC, whenthe latter has drifted into thenormal entrainment phase.
50
40
30
20
10
Sleep
CT 6
PRC2 pg/mL MO
(CT 13)
The end of the delayzone of the melatonin PRC is 7 h before the 2 pg/mL MO.
The 2 pg/mL occurs3 h before sleepduring normal entrainment.
The end of the advance zoneof the melatonin PRC is 5 hafter the 2 pg/mL MO.
The endogenous melatoninprofile and the melatoninPRC shift later after each dayin a BFR, relative to clocktime and sleep.
Endogenousmelatoninprofile
Plas
ma
mel
aton
inle
vels
(pg/
mL)
The greatest phase advances occurwhen exogenous melatonin is given here.

Parry’s and Wirz-Justice’s contributions to this vol-ume57,58), as well as many of the hypotheses for SAD (seeParry’s, Wirz-Justice’s and Praschak-Rieder’s contribu-tions to this volume57-59) and so these will not be coveredhere.This monograph will concentrate on diagnosing cir-cadian phase disorders using the endogenous melatoninprofile and on the basic principles for treating them.The leading hypothesis for SAD is the phase shifthypothesis (PSH).33 According to the PSH, the typicalSAD patient becomes depressed in the winter, at least inpart because of a phase delay of circadian rhythms(marked by the DLMO) with respect to sleep,33,60,61 hav-ing a mismatch in circadian rhythms (similar to jet lag),which persists for several months.Therefore, bright lightexposure should be most antidepressant when it is sched-uled in the morning, when it would be expected to causea corrective phase advance. Bright light exposure in themorning should certainly be more antidepressant thanevening bright light, which would be expected to cause aphase delay.The first major test of the PSH was a crossover study ofeight patients and seven control subjects.36 There was asmall, but statistically significant, delay of the DLMO inpatients compared to controls at prebaseline and at theend of the initial week of baseline conditions (sleep per-mitted only between 10.00 PM and 6.00 AM). Two hoursof morning bright light (2500 lux) caused advances in theDLMO; evening bright light caused delays. The combi-nation of morning plus evening light (which was the lasttreatment week) moved the DLMO towards its baselinetime. Morning light produced a significant antidepressanteffect compared with baseline and with evening light.Thecombination was again intermediate between that ofmorning light alone and evening light alone. This studywas by and large replicated a few years later.62,63 Sincethen, not much has changed in the recommended lighttreatment regimen, except that light intensity can be asgreat as 10 000 lux,64 and perhaps 1 h per day is sufficient,as long as it is scheduled immediately upon awakening.Once treatment is satisfactory, the duration of light expo-sure can almost always be reduced.65
Several other studies have supported these findings, butsome have not66,67: these studies were usually parallel-designed, so that patients themselves did not have theopportunity to compare light exposure at different times(which would have minimized the placebo component).In 1998, three independent research groups publishedlarge-N studies in which morning light was shown to be
more antidepressant than evening light, thereby movingthe field towards consensus about the superiority ofmorning light.45,68,69 However, superior efficacy of morn-ing light does not necessarily prove the PSH, because itcould be more antidepressant at this time for some rea-son other than causing a phase advance. However, it hasbeen shown that the antidepressant response to morninglight does, in some circumstances, correlate with theamount of phase advance in the DLMO. This was firstreported with respect to treatment group means,61 fol-lowed by an analysis70 of individual DLMOs and depres-sion scores collected independently.36,63 More recently, thislatter finding was essentially replicated using anotherdata set.71 Further support of the PSH along these lineswill be discussed below. It should also be noted that avery small subgroup of SAD patients appear to be cue-ing to dusk and should be treated with evening brightlight; clinically, these patients can be identified by a his-tory of early morning awakening year round, going tobed much earlier in the winter.65
In any event, the earliest and most common use of theDLMO has been to assess the phase-shifting effects oflight. Bright light has also been used to treat a number ofother circadian phase disorders, such as advanced sleepphase syndrome (ASPS), delayed sleep phase syndrome(DSPS), jet lag, and shift work maladaptation (seebelow).
The melatonin PRC
The phase-shifting effects of melatonin are also describedby a PRC.The melatonin PRC is about 12 h out of phasewith the light PRC.13,44 Both PRCs are phase-locked toeach other, as well as to the melatonin profile (Figure 2).As mentioned above, waketime is usually designated ZT 0. Sleep time is therefore usually ZT 16. In the mela-tonin PRC studies of sighted people, the baseline plasmaDLMO10 was designated CT 14. It is also designated CT 14 in free-running blind people. We call this phasemarker the MO in blind people. Saliva can also be used(at this time of the night, salivary melatonin levels areabout one-third those of plasma).72 Measuring the MO inblind people provides a reference point to determine thephase of the endogenous circadian pacemaker and themelatonin PRC. Unless stated otherwise, in the follow-ing the MO refers to the plasma 10 pg/mL threshold orits salivary equivalent (3 pg/mL). The melatonin PRCwas first described using four daily doses of 0.5 mg mela-
C l i n i c a l r e s e a r c h
402

tonin in sighted people. It has been by and large repli-cated by two other research groups.73,74
In sighted people who habitually awaken at 7.00 AM, thebreak points that divide the two intervals of the mela-tonin PRC occur at 1.00 PM (CT 6) and 1.00 AM (CT 18),just as with the light PRC. The phase-advance zone isbetween 1.00 AM and 1.00 PM; the phase-delay zone isbetween 1.00 AM and 1.00 PM. Once again, the phase-advance zone of the melatonin PRC extends from CT 6to CT 18, and the phase-delay zone extends from CT 18to CT 6. Therefore, once the time of the MO is known,the advance zone extends from 8 h before the MO until4 h after the MO. The delay zone extends from 4 h afterthe MO until 8 h before the MO.
Treating SAD patients with melatonin: the importance of creating “overlap”
Creating “overlap” may be an important principle inoptimizing melatonin’s phase-shifting effects. This wasdemonstrated in a pilot study treating SAD patients withmelatonin.75 In order to avoid the soporific side effect ofsleepiness that occurs in some people, the dose of mela-tonin is kept to a minimum, so as to reduce the initialspike in melatonin levels following an oral, immediate-release formulation. However, according to the mela-tonin PRC, the earlier melatonin is given in the afternoon(at least for the second half of the advance zone), thegreater the magnitude of the phase-advance shift. If a lowdose is given too early, however, there will be a mela-tonin-free interval between the end of the exogenouspulse and the beginning of the endogenous melatoninprofile that occurs about 14 h after waketime inentrained, sighted people.Therefore, a second (or even athird or possibly fourth) small dose of melatonin is givento create overlap between elevated melatonin levels aris-ing from exogenous and endogenous sources, so that theSCN is exposed to one continuous melatonin signal.Recently, a more definitive test of the PSH for SAD wascompleted, using three to four small doses of melatonin(0.075-0.1 mg) given every 2 h in the morning or in theafternoon/evening. One hundred patients were studiedover four winters. One-third of them did not receivemelatonin in any capsule, although all subjects took thesame number of capsules per day. Subjects were held toconsistent bedtimes and waketimes of their choosing.The results supported the PSH. In the most phase-delayedgroup of patients (those with a DLMO ZT >14.6), there
was a significant correlation between the amount of phasedelay at baseline and the severity of depression ratings.After 3 weeks of treatment, this correlation remained sig-nificant, but only if depression severity was analyzed withregard to the absolute difference from the hypothesized“normal” ZT of 14. Change scores analyzed in this waywere also statistically significant: as DLMO ZT normal-ized, depression ratings improved.This may be one of thefirst examples of a physiological marker that correlateswith psychopathology at baseline and posttreatment.These data are consistent with the clinical observationthat too much of a phase advance can result in a returnof symptoms. In any event, morning light appears to bemore antidepressant than evening light in typical SADpatients, because, at least in part, it is correcting a phasedelay that occurs in SAD patients when they becomedepressed in the winter. Using SAD as a model chrono-biological psychiatric (affective) disorder, it would nowseem timely to investigate other disorders, in order toassess the contribution of a mismatch between circadianrhythms to the pathology.
Treating free-running totally blind people with melatonin:
the importance of avoiding “spillover”
About 15% of blind people completely lack light per-ception. Most, if not all of them, have abnormal circadianrhythms, and many of them “free-run,” whereby theirMOs drift a little later each day. When they are out ofphase, they find it difficult to sleep at night and are tiredduring the day—a burden described by some as secondonly to lack of vision. A daily drift in sleep times is notusually observed. However, assessment of physiologicalrhythms clearly indicates this daily drift in the phase ofthe endogenous circadian pacemaker.Any of several cir-cadian rhythms can be measured, including cortisol andtemperature.76-79 However, these are masked by changesin activity.80 Melatonin production is masked only bylight,53 which is not an issue in blind people.A number of studies now document circadian abnor-malities in the totally blind population.81-83 The MO hasproved to be a useful phase marker in blind people,whether it is extracted from 1-h samples over 24 h orfrom sampling every 30 to 60 min within a narrower win-dow when it is expected to occur. However, as will beexplained below, assessing MOs is not absolutely neces-sary in diagnosing and treating most cases.
Clinical applications of melatonin - Lewy Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
403

Following the discovery that light can suppress melatoninproduction in humans,53 the obvious next step was to assessthe melatonin profiles of blind people. One-day assess-ments indicated that melatonin levels were continuouslyelevated for about 12 h out of every 24 h, similar to sightedpeople.84 However, it was not always confined to night.Two bilaterally enucleated people were studied longitudi-nally85: one of them appeared to be stably entrained, but180° out of phase (that is, melatonin levels peaked in themiddle of the day, week after week); the other was free-running with an intrinsic circadian period (tau, or τ) of 24.7 h (that is, the endogenous melatonin profile shiftedlater at a rate of about 0.7 h per day or about 5 h perweek). Several studies have since confirmed that the cir-cadian rhythms of blind people are of three types: nor-mally entrained, abnormally entrained, and free-running.85
When out of phase, these individuals have difficulty sleep-ing at night and take more naps during the day.The mela-tonin rhythm reflects the phase of all other endogenouscircadian rhythms, including those of cortisol, temperature,and sleep propensity (see above).As mentioned earlier, another use of melatonin is to giveit exogenously in order to cause phase shifts.13 Inspiredby animal studies,86 these effects were most conclusivelydemonstrated by entraining free-running blind people(blind free-runners [BFRs]) with a daily dose of mela-tonin.87 Although an early subject showed apparententrainment to a dose of about 7 mg,88-90 entrainment ofBFRs was conclusively demonstrated using a dose of 10 mg.87,91 Only one of seven BFRs failed to entrain to the10-mg dose; this BFR had the longest tau (24.9 h).Although the melatonin PRC was experimentally deter-mined in sighted people, it appears to apply to blind peo-ple as well. Currently, more is known about the phase-advance zone of the melatonin PRC: for at least the secondhalf of the advance zone, the earlier melatonin is given, thegreater the magnitude of the phase-advance shift.Whenmelatonin is given daily to a free-running blind person, themelatonin PRC will continue to drift later and later untilexogenous melatonin is hitting the point on the melatoninPRC that will produce a phase advance equal to the dailydrift (this is called the entrainment point on the melatoninPRC and will vary between individuals, depending in parton the intrinsic tau).Then, the endogenous pacemaker willlock on to the daily melatonin dose. For example, if a BFR’sintrinsic circadian period, or tau, is 24.4 h, the melatonindose will stop the pacemaker from drifting later when it isstimulating that part of the melatonin PRC when it pro-
C l i n i c a l r e s e a r c h
404
Figure 3. A totally blind subject with free-running circadian rhythms dur-ing four trials of oral melatonin administration. Each data pointrepresents an assessment of circadian phase as determined bysuccessive measurements of the time that endogenous plasmamelatonin concentrations rose above the 10 pg/mL threshold.Vertical lines represent the timing and duration of exogenousmelatonin administration. The slopes of the fitted regressionlines indicate circadian period (shown in hours beside theregression lines) during a given treatment. The calculated cir-cadian periods represent mean determinations between daysof assessment; fluctuation of circadian period probably occursas the melatonin dose stimulates different parts of the shiftingphase response curve (PRC). a. Baseline free-running circadianrhythm of 24.92 h. b. Administration of 10 mg melatonin for17 days beginning at CT 20.5 led to a shortened period of24.34 h without entrainment. c. Administration of 9 to 10 mgof melatonin over 83 days again failed to entrain this subjectbut shortened circadian period to 24.36 h. d. Administrationof 20 mg initially at CT 14.6 shortened the subject’s circadianperiod to 24.58 h after 60 days. e. Administration of 0.5 mg,initially at CT 20.6, caused entrainment (circadian period of23.98 h) after 47 days.Reproduced from reference 92: Lewy AJ, Emens JS, Sack RL, Hasler BP,Bernert RA. Low, but not high, doses of melatonin entrained a free-run-ning blind person with a long circadian period. Chronobiol Int.2002;19:649-658. Copyright © 2002, Marcel Dekker.
c
b
a
d
e
Time (h)
1240
Tim
e (d
ays)
1060
0
60
150
240
270
330
390
450
1120
1180
120
23.98 h
24.85 h
24.58 h
24.95 h
24.36 h
24.34 h
24.87 h
24.92 h
24.89 h
967248240

duces a phase advance of 0.4 h.Thus, entrainment occursand the pacemaker now functionally has a tau of 24.0 h.The finding that low doses of melatonin may be moreeffective than high doses, leading to the idea of avoidingspillover, is illustrated in the treatment of the one BFRwho failed to entrain to the 10-mg dose (recall that he hadthe longest tau, 24.9 h, in that study). Despite repeat treat-ment with 9 to 10 mg melatonin for 83 days and 20 mgmelatonin for 60 days (Figure 3),92 he failed to entrain,although his tau did shorten to 24.36 and 24.58 h, respec-tively. He was finally entrained with 0.5 mg melatonin.92
The melatonin PRC might explain why a lower dose ofmelatonin is more effective than higher doses (Figure4).92 While administering melatonin earlier in the advancezone causes a greater phase advance and while highermelatonin levels probably cause more of a phase advance(perhaps by stimulating more of the phase-advancezone), it appears that if the dose is too high, it will stim-ulate more of the delay zone and therefore reduce themagnitude of the phase advance. In other words, a lowerdose will have less “spillover” and might thus be moreeffective than a higher dose.
Clinical applications of melatonin - Lewy Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
405
Figure 4. Pharmacokinetic data from two different melatonin doses (0.5 and 10 mg) in relation to the endogenous melatonin profile and the mela-tonin phase response curve (PRC). The 0.5 mg dose and the endogenous melatonin profile are data from the subject in this study. The 10 mgdata were from another subject and were not collected beyond 10 h; it is clear that they cause more stimulation of the delay zone of themelatonin PRC than the 0.5 mg dose. By convention, circadian time (CT) 14 is the endogenous melatonin onset (MO). In free-running sub-jects, the endogenous melatonin profile and the melatonin PRC (which are phase-locked) drift later each day with respect to the sleep/wakecycle. Normal phase is when the MO occurs 2 h before sleep onset (14 h after waketime). Exogenous melatonin causes phase advances whenit is given between CT 6 and CT 18 and causes phase delays when it is given between CT 18 and CT 6; however, the concentrations andduration of exogenous melatonin levels as they spill over onto the wrong zone of the melatonin PRC may also affect the phase-shifting effectof exogenous melatonin. Reproduced from reference 92: Lewy AJ, Emens JS, Sack RL, Hasler BP, Bernert RA. Low, but not high, doses of melatonin entrained a free-running blind per-son with a long circadian period. Chronobiol Int. 2002;19:649-658. Copyright © 2002, Marcel Dekker.
Wake WakeSleep
10 mg dose
0.5 mg dose
Delay zone Advance zone of PRC Delay zone of PRC Advance zone
17 000
13 000
9000
5000
1000150
100
50
0
21 000
CT 0
7 AM 11 PM 11 PM7 AM
CT 6 CT 14 CT 18 CT 0 CT 6
Melatonin dosesgiven at CT 15
Endogenousmelatonin
profile
Plasmamelatonin
levels(pg/mL)
9 PM
The endogenous melatonin profile and the melatonin shift later after eachday in a blind person with free-running rhythms, relative to clock time and sleep.
The melatonin onset (MO) occurs 2 h beforesleep, when the MO has drifted into the normal phase.

The efficacy of low doses means that melatonin can beadministered well before sleep without causing daytimeor evening sleepiness. This is important, because thetreatment goal is not only entrainment, but also entrain-ment at the optimal phase. Indeed, in the original studyof 10 mg,87 successfully entrained BFRs had MOs occur-ring after sleep onset, often much later (Figure 5).93 Inother words, the MO occurred at the same time eachnight, but later than normal. As in animal studies, thegreater the pretreatment free-running tau, the laterentrainment occurs relative to the time of the entrainingstimulus. In our entrained BFRs, their sleep disorders hadimproved with treatment, but our subjects still had trou-ble falling asleep and getting up in the morning. About30% of people become sleepy on melatonin, and this sideeffect appears to be dose-related and is troublesome atdoses greater than 1 mg, certainly at 10 mg. Now that 0.5 mg has been shown to be an effective dose with min-imal soporific side effects, it can be administered earlierthan bedtime (which is when the 10 mg was originallygiven, in order to make use of this side effect). Melatonincan be given earlier in the evening, so that the MO occurs2 h before desired sleep time, thus resulting in optimalsleep quality.When shifting the clock time of exogenous melatoninadministration, the endogenous MO can be reset to anytime. Shifting the clock time of administration earliershould be done gradually, so as not to cross over thebreak point on the melatonin PRC. The clock time ofadministration can also be shifted later, which can bedone in 1 day without loss of entrainment. In either case,the pacemaker will shift with the time of the melatonindose. In blind people who appear to be entrained (or atleast have a tau virtually indistinguishable from 24.0 h)to a behaviorally related zeitgeber or to ambient light(perhaps in some blind people who are not bilaterallyenucleated), MOs can be reset earlier or later with a dailydose of melatonin, so that the MO occurs 14 h afterwaketime.Several years ago, we also proposed that the abscissa andordinate of Figure 5 could be reversed.94 Accordingly, thephase angle of entrainment could be used to predict tau.While the taus of BFRs are probably the most accurateestimate of the genetically programmed intrinsic tau(which might be of use in studying clock genes in humans95-
97), we also suggested that the DLMO ZT in sighted peo-ple might be a useful way to estimate at least the func-tional tau in people entrained to the light/dark cycle.
Melatonin treatment can be initiated at any time in BFRs
What would have happened if melatonin treatment wereinitiated in BFRs on the “wrong” zone of the melatoninPRC? In animal studies, it does not matter when theentraining stimulus is given: eventually, the pacemaker isstably entrained at a steady-state phase position, once theentraining stimulus comes into contact with the entrain-ment point of the PRC.98 However, in a study publisheda few years ago, the University of Surrey research groupfound that they were able to entrain only about half oftheir group of seven BRFs to a 5-mg dose of melatonin.99
They noted that entrainment was successful only whenmelatonin treatment was started on the advance zone ofthe PRC, but not when treatment was started on the delayzone, even if daily melatonin doses were continuedthrough a complete circadian beat cycle, so that eventuallymelatonin stimulated all of the advance zone.They furthernoted that this finding contradicted those of animal stud-ies, in which starting a zeitgeber on the delay zone did notaffect its capability to eventually cause entrainment (it justtook longer before the entrainment point was reached asthe pacemaker, and the PRC, drifted into phase). If theSurrey group is correct, this would mean that all BFRs
C l i n i c a l r e s e a r c h
406
Figure 5. Pretreatment tau predicts phase angle of entrainment (PAE).PAE is the interval (in hours) between the time of the bedtime10 mg melatonin dose and the entrained melatonin onset (MO)of the endogenous melatonin profile. This figure is an updatedversion of what has been previously reported, and the tau ofone person has been changed to 24.58 h from 24.63 h, cor-recting an error in the previous report. The horizontal dottedline indicates that entrainment will fail if the phase angle ofentrainment is more than 8 h.Reproduced from reference 93: Lewy AJ, Hasler BP, Emens JS, Sack RL.Pretreatment circadian period in free-running blind people may predictthe phase angle of entrainment to melatonin. Neurosci Lett.2001;313:158-160. Copyright © 2001, Elsevier Science.
Entrainment fails above this line
Tau (h)
-2
-1
2
5
Phas
e an
gle
of
entr
ain
men
t (h
)
6
7
8
9
3
4
0
1
24.0 24.2 24.4 24.6 24.8 25.0
10 mg melatonin
r2=0.5767
P<0.05

should have frequent MO assessments to determine onwhat day melatonin treatment should be initiated.Fortunately, this does not appear to be true.We found inseven out of seven BFRs that when low-dose melatonin isinitiated on the delay zone, entrainment eventually occurswhen melatonin is given at the entrainment point in theadvance zone.100 The following case (Figure 6) using 0.05mg is an example; in the other cases, a dose of 0.5 mg wasused. Recently, the Surrey group found that some BFRsentrained when 0.5 mg was initiated on the delay zone;however, they continue to recommend initiating melatonintreatment on the advance zone.
Very low doses of melatonin are effectivein entraining BFRs
In this case (Figure 6), a very low dose (0.05 mg) of mela-tonin was initiated in a BFR with a tau of 24.35 h on thedelay zone (CT 4.95). Initially, a clear increase in tauoccurred, consistent with a greater daily phase delay.Within a few days, melatonin was stimulating the advancezone and once the entrainment point was reached, thepacemaker locked on.As mentioned above, low doses ofmelatonin can usually entrain BFRs, no matter whentreatment is initiated. Therefore, at least for most blind
people, one does not need to start melatonin treatmenton the advance zone, although it may take longer toreach the entrainment point when treatment begins onthe delay zone. The clinical implications of this findingare very important: clinically, most blind people can betreated without having to measure their endogenous cir-cadian phase.Work is on-going to entrain BFRs to dosesof melatonin even lower than 0.05 mg. These doses pro-duce peak melatonin levels that are less than what ismaximally produced endogenously. Melatonin can alsoreset the phase of abnormally entrained blind people,even under circumstances when they may be entrainingto a poorly perceived ambient light/dark cycle.101
Guidelines for treating CSDs in blind people
The above database provides a preliminary set of treat-ment guidelines that should be effective in most blindpeople with circadian sleep disorders (CSDs). However,more studies need to be done, and there will clearly besome blind people who will have to be assessed using theMO for optimal treatment.• Not every blind person has a CSD. Most, if not all, blind
people completely lacking in light perception haveCSDs, or at least merit treatment to prevent an even-tual occurrence; however, the more light perception, themore likely stable entrainment at a normal phase willbe the case. In any event, the first step is to take a sleephistory to determine whether the patient has DSPS orASPS, or sometimes has both that regularly recur,which would suggest free-running circadian rhythms. Ifpossible, keeping a sleep diary—noting daily sleeptimes, naps, nighttime sleep quality, and daytime alert-ness—is advised; depressive symptoms may also occurwhen there is a mismatch between circadian rhythmsand the sleep/wake cycle.
• Melatonin treatment should then be started.A dose of0.5 mg at about 8.00 PM should result in entrainment ofBFRs and to optimal phase resetting in most blind peo-ple. Stable steady-state entrainment at the normal phasewill take shorter or longer, depending on the tau and onwhat day treatment was initiated. Although repeatedassessments of MOs can determine these parameterswith precision, they should not be necessary in most peo-ple: eventually this treatment should be successful. If 3months have passed without marked improvement,referral to sleep a disorder center or some other facilityin which MOs can be assessed is advised.
Clinical applications of melatonin - Lewy Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
407
Figure 6. Blue circles represent an assessment of circadian phase as deter-mined by the time that endogenous salivary melatonin concentrationscontinuously rose above the 0.7 pg/mL threshold. Vertical lines representthe timing and duration (days) of exogenous melatonin administration of0.05 mg (black line) and 0.025 mg (gray line). All times are presented inPacific Standard Time (some times have been converted from DaylightSaving Time).
0.05 mg
0.025 mg
Time (h)
240
180
120
Tim
e (d
ays) 90
60
30
0
150
210
0 1224122412

• In a few individuals, the 0.5 mg dose may cause someacute sleepiness. If unpleasant, the dose can be graduallytapered every 2 weeks in increments of 0.1 mg to as lowas 0.1 mg, and then in increments of 0.025 mg to 0.05 mg,if desired. However, for individuals who have longer taus,the dose should not be reduced below 0.3 mg. Individualswho report bouts of symptoms as often as every 4 to 6weeks are likely to have longer taus (>24.6 h).
• After finding a suitable maintenance dose, the clocktime of administration can then be adjusted if thepatient still complains of symptoms of ASPS or DSPS.When shifting the administration time earlier, advanc-ing it no more than 30 min every 2 weeks should be suf-ficiently conservative, so that the entrainment point willnot be crossed. Delaying a person with symptoms ofASPS need not be done incrementally. However, ineither case shifting the clock time should be stoppedwhen sleep symptoms abate.
• These patients should probably remain on melatonintreatment for the rest of their lives. Some minor shifts inclock time of administration may be required. If nottaken daily, escape from steady-state entrainment at thenormal phase will likely occur. However, after the pace-maker drifts through a complete cycle, the melatonindose should again capture the pacemaker at the optimalphase.
• Although long-term studies of melatonin need to bedone, it is likely that doses of 0.5 mg or less (which resultin levels within the same order of magnitude as thoseproduced by the pineal) should be safe.To date, no seri-ous, irreversible side effects have been unequivocallylinked to melatonin even at doses greater than 0.5 mg.Nevertheless, we recommend that continuous melatonintreatment be monitored by a physician or other respon-sible caregiver, who is familiar with the most recent sci-entific and medical literature.
Other circadian phase disorders
Research in SAD patients and blind people has helpedus understand how to treat circadian phase disorders andsyndromes in the general sighted population. These dis-orders include ASPS and DSPS, jet lag, and shift workmaladaptation.All of these disorders and syndromes areto a greater or lesser extent related to the circadian tim-ing system and can be phase typed, according to whetherthey are phase delayed or phase advanced (Table I).Treatment of these disorders is based on the light and
melatonin PRCs.44 To provide a corrective phase advance,bright light should be scheduled immediately upon awak-ening in the morning and melatonin should be taken inthe afternoon/evening. To provide a corrective phasedelay, bright light should be scheduled in the evening andmelatonin should be taken in the morning.
Delayed sleep phase syndrome
Melatonin and light are both effective in treatingDSPS.102,103 The first published report of treating DSPSwith light was in 1983.33 This topic is reviewed elsewhere.104
Most people with DSPS are younger and prefer to sleeplate in the morning, having difficulty falling asleep untilas late as 4.00 AM. These individuals can be treated byscheduling their waketimes to occur gradually earlier(perhaps 15 min every other day) until the desired wake-time is reached. Going outdoors immediately upon awak-ening for about 30 min will help advance the circadianrhythm of sleep propensity, as will taking 0.5 mg of mela-tonin about 8 h after waketime. One or both of thesetreatments may be necessary to hold the sleep/wake cycleto the desired time. If outdoor sunlight is not available orinconvenient, a portable fixture may be used for 30 to 60min; the fixture should be at a distance from the eyes sothat the intensity is about 10 000 lux. Research on themost potent wavelengths for phase shifting and melatoninsuppression may eventually result in some modificationof light sources. In the US, melatonin is widely available.If the dose of 0.5 mg happens to cause sleepiness in anindividual who is unusually sensitive to this side effect, itshould be decreased and a repeat dose should be givena few hours later. For individuals who become sleepy on(usually higher doses of) melatonin, 1 to 3 mg at bedtimemay be usefully taken to induce sleep.
Advanced sleep phase syndrome
ASPS generally occurs in older individuals, who tire earlyin the evening and wake up as early as 4.00 AM.The firstreference to treating ASPS with light was published in1985.105 This subject is reviewed elsewhere.104 Treatment rec-ommendations include 1 to 2 h of 10 000 lux exposure inthe evening, ending at least 1 h before desired bedtime.Melatonin (0.5 mg) should be taken at each awakeningand upon final arising in the morning.Whenever melatoninis taken during waketime, people should not drive if theyfeel sleepy and lowering the dose should be considered.
C l i n i c a l r e s e a r c h
408

Jet lag
Although sleep deprivation resulting from flying at nightcontributes to the malaise following air travel, there is lit-tle doubt that jet lag is caused by a mismatch betweencircadian rhythms that are tightly coupled to the endoge-nous circadian pacemaker and destination sleep/waketime. A good rule of thumb is that it takes 1 day torecover from every time zone crossed, with the caveatthat jet lag is usually worse when traveling east thanwhen traveling west.There have been numerous studies of light and melatoninin the amelioration of jet lag. These have been recentlyreviewed.106,107 The first study to test the effect of light onjet lag was published in 1984.108 The first study to test theeffect of melatonin on jet lag was published in 1986.109 Onthe whole, both have been shown to be somewhat effica-cious. However, optimal testing of melatonin in the treat-ment of jet lag has not yet occurred. For example, no peer-reviewed report has included taking 0.5 mg melatonin inthe afternoon before traveling east or in the morningbefore traveling west, which is what we recommend shouldbe done for up to 2 days before travel, as well as on theday of travel.Taking melatonin at destination is more com-plicated.After traveling across more than five time zones,melatonin can be taken at bedtime. However, as theendogenous circadian pacemaker adjusts to local time,bedtime may not be the best time—and may even be thewrong time—to take melatonin (see below).Bright light exposure is not convenient to schedule beforetravel.At destination, obtaining sunlight exposure at thecorrect time can greatly facilitate circadian realignment.Even more important, particularly after crossing morethan five time zones, is avoiding sunlight exposure at thewrong time, which will shift circadian rhythms in the direc-tion opposite to that traveled. When flying from LosAngeles to Madrid, for example, it would take severalmore days to delay the body clock 15 h than to advance it9 h. (However, extreme night owls might prefer to delaytheir clocks no matter which direction of travel.) Precise recommendations for obtaining and avoiding
sunlight at destination depend on what are thought to bethe light PRC’s break points. The following recommen-dations are based on a light PRC with the break pointsat CT 6 and CT 18, using the beginning of the light pulseas its phase reference. Using the middle of a relativelylong bout of bright light exposure as the phase reference,which is done in most human (but not animal) studies,would put these break points a few hours later; however,this requires people to schedule long periods of (prefer-ably bright) light exposure. Furthermore, a recent studyindicates that the beginning of the light pulse is its mostpowerful part, at least with respect to causing phaseadvances.After traveling across five or fewer time zones, start sun-light exposure as early as possible in the morning aftergoing east or as late as possible in the afternoon aftergoing west.After traveling across six or more time zones,obtain sunlight exposure in the middle of the day andavoid it in the morning after going east or at the end ofthe day after going west. On subsequent days, these timescan be shifted, as if one had traveled through fewer timezones (see below).Using both light and melatonin at the optimal times, it isreasonable to assume a rate of phase shifting of 3 h perday. For example, after traveling nine time zones to theeast, a person who habitually arises at 7.00 AM shouldavoid sunlight exposure before 10.00 AM and obtain atleast 30 min of it shortly after this time.The next day sun-light exposure should occur shortly after 7.00 AM.Melatonin should be taken at 2.00 PM before travel andat 11.00 PM upon reaching the destination. It should thenbe taken 3 h earlier each day until it is again taken at 2.00PM for a couple of days. After traveling nine time zonesto the west, take melatonin at 10.00 PM the first night, buton subsequent nights it should be taken only if awakeafter 1.00 AM and then again upon final awakening in themorning.After traveling six or more time zones to the west, brightlight should be avoided at the end of the day and sunlightshould be obtained in the middle of the day. After 1 or2 days, bright light should be obtained at the end of the
Clinical applications of melatonin - Lewy Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
409
Table I. Phase typing for circadian rhythm disorders.
• Phase-advanced type • Phase-delayed type
Advanced sleep phase syndrome (ASPS) Delayed sleep phase syndrome (DSPS)
East-to-west jet lag West-to-east jet lag
Night work maladaptation (work days) Night work maladaptation (weekends)
Typical seasonal affective disorder (SAD)

day. Melatonin can be taken at bedtime the first night atdestination, but should not be taken before 1.00 AM onsubsequent days, except under special circumstances.Optimal scheduling of light and melatonin depends onthe habitual waketime of an individual, the direction oftravel, the number of time zones crossed, and the pre-sumed rate of phase shifting.A complete table of instruc-tions would be helpful and will hopefully be availablesoon. We recommend taking the lowest dose of mela-tonin currently available or using a pill cutter. In a fewpeople, even the 0.5 mg dose may cause sleepiness imme-diately after taking it during the day. Lowering the dosefurther will reduce the soporific side effect, but then asecond dose should be taken a few hours later, particu-larly when a phase advance is desired, in order to createoverlap between the exogenous melatonin pulse and theendogenous melatonin profile, as described above.
Shift work maladaptation
Although it is quite clear that very few shift workersadapt their circadian rhythms to conform to their workschedules, there is no consensus as to how best to helpthem. This topic has been reviewed elsewhere. The firstuse of light to treat shift workers was published in 1987.110
The first use of melatonin to treat shift workers was pub-lished in the early 1990s.111,112 When trying to sleep at oddhours, shift workers have a type of jet lag. Night workershave the same problems as someone who has traveledthrough 12 time zones, in fact, worse, since air travelersusually adjust at a rate of at least 1 h per day, as men-tioned above. Night workers rarely adjust their circadianrhythms, probably because of the morning sunlight expo-sure that occurs on the way home from work. Eveningworkers have it somewhat easier. Chronobiologists uni-formly recommend staying on the same schedule everyday, week after week. Neither light nor melatonin wouldthen be necessary. However, workers (certainly those
who do so at night) are uniformly against sleeping dur-ing the day on their weekends. Because their circadianrhythms do not usually adapt to their work schedules,shift workers feel good only on their days off.After work-ing each night, they force themselves to sleep during theday when their body clocks would have them stay up, andof course their work suffers as they soldier through thewee hours of the night when their body clock would havethem sleep. A number of medical complaints oftenaccompany shift work, and the older one gets, the harderit is to adapt.Experts do not agree on how to help shift workers. Asmentioned above, part of the problem lies in the fact thatsome workers would rather feel better on their days offthan on their workdays, while managers understandablywant workers to be most rested and alert during theirhours of employment. Even if this issue is resolved, thenext conundrum is that one cannot shift more than 3 to4 h per day.Compromise schedules that rely on the use of appropri-ately timed bright light and/or melatonin administrationhave been proposed that stabilize circadian phase midwaybetween work and off-work schedules. For example,Eastman and associates have proposed such a compromiseschedule.113 We are in the process of developing our ownversion of a compromise schedule, but its implementationmay depend on the development of delayed-release mela-tonin formulations that are not yet available. ❏
Supported by grants from the Public Health Service (R01 MH56874 to DrsLewy and Sack; R01 MH55703, R01 AG21826 and R01 HD42125 to Dr Lewy;and MO1 RR00334 to the General Clinical Research Center of OHSU) andthe National Alliance for Research on Schizophrenia and Depression (2000NARSAD Distinguished Investigator Award to Dr Lewy). We are indebtedto the nursing staff of the General Clinical Research Center, to Dr RobertSack, Dr Jonathan Emens, Dr Paul Giger, Dr Kyle Johnson, Rick Boney,Nancy Stahl, Neil Cutler, Bryan Lefler, Krista Yuhas, and Angie Koenig fortheir valuable assistance, and to Keith Parrott, PharmD, for the formula-tion of the melatonin capsules.
C l i n i c a l r e s e a r c h
410
REFERENCES
1. Lerner AB, Case JD, Takahashi Y, Lee TH, Mori N. Isolation of melatonin,the pineal gland factor that lightens melanocytes. J Am Chem Soc.1958;80:2587.2. Arendt J. Melatonin and the Mammalian Pineal Gland. London, UK:Chapman & Hall; 1995.3. Lewy AJ, Tetsuo M, Markey SP, Goodwin FK, Kopin IJ. Pinealectomy abol-ishes plasma melatonin in the rat. J Clin Endocr Metab. 1980;50:204-205.
4. Neuwelt EA, Lewy AJ. Disappearance of plasma melatonin after removalof a neoplastic pineal gland. N Engl J Med. 1983;308:1132-1135.5. Goldman BD, Darrow JM. The pineal gland and mammalian photoperi-odism. Neuroendocrinology. 1983;37:386-396.6. Underwood H. Circadian rhythms in lizards: phase response curve formelatonin. J Pineal Res. 1986;3:187-196.7. Armstrong SM, Thomas EMV, Chesworth MJ. Melatonin-induced phase-shifts of rat circadian rhythms. In: Reiter RJ, Pang SF, eds. Advances in PinealResearch. London, UK: John Libbey; 1989:265-290.

8. Lewy AJ, Sack RL, Latham JM. Exogenous melatonin administration shiftscircadian rhythms according to a phase response curve. Presented at TheVth Colloquium of the European Pineal Study Group. Guildford, UK; 1990.Abstract 021.9. Lewy AJ, Sack RL, Latham JM. Circadian phase shifting of blind andsighted people with exogenous melatonin administration: evidence for aphase response curve. Soc Light Treatment Biol Rhythms Abst. 1990;2:22.10. Lewy AJ, Sack RL, Latham J. A phase response curve for melatoninadministration in humans. Sleep Res. 1991;20:461.11. Lewy AJ, Sack RL, Latham JM. Melatonin and the acute suppressant effectof light may help regulate circadian rhythms in humans. In: Arendt J, PevétP, eds. Advances in Pineal Research. London, UK: John Libbey; 1991:285-293.12. Lewy AJ. The pineal gland. In: Wyngaarden JB, Smith LH, Bennett JC, eds.Cecil Textbook of Medicine. Philadephia, Pa: WB Saunders; 1991:1246-1248.13. Lewy AJ, Ahmed S, Jackson JML, Sack RL. Melatonin shifts circadianrhythms according to a phase-response curve. Chronobiol Int. 1992;9:380-392.14. Pickard GE, Turek FW. The hypothalamic paraventricular nucleus medi-ates the photoperiodic control of reproduction but not the effects of lighton the circadian rhythm of activity. Neurosci Lett. 1983;43:67-72.15. Hendrickson AE, Waggoner N, Cowan WM. An autoradiographic andelectron microscopic study of retino-hypothalamic connections. Z Zellforsch.1972;135:1-26.16. Stephan FK, Zucker I. Circadian rhythms in drinking behavior and loco-motor activity of rats are eliminated by hypothalamic lesions. Proc Natl AcadSci U S A. 1972;69:1583-1586.17. Moore RY, Eichler VB. Loss of circadian adrenal corticosterone rhythmfollowing suprachiasmatic lesions in the rat. Brain Res. 1972;42:201-206.18. Vessely LH, Lewy AJ. Melatonin as a hormone and as a marker for cir-cadian phase position in humans. In: Pfaff D, Arnold A, Etgen A, FahrbachS, Rubin R, eds. Hormones, Brain and Behavior, Vol 5. San Diego, Calif: ElsevierScience; 2002:121-141.19. Ariëns-Kappers J. The development, topographical relations and inner-vation of the epiphysis cerebri in the albino rat. Z Zellforsch Mikrosk Anat.1960;52:163-215.20. Axelrod J, Zatz M. The β-adrenergic receptor and the regulation of cir-cadian rhythms in the pineal gland. In: Litwack G, ed. Biochemical Actionsof Hormones. New York, NY: Academic Press; 1977:249-268.21. Reppert SM, Weaver DR, Rivkees SA, Stopa EG. Putative melatoninreceptors are located in a human biological clock. Science. 1988;242:78-81.22. Dubocovich ML, Benloucif S, Masana MI. Melatonin receptors in themammalian suprachiasmatic nucleus. Behav Brain Res. 1996;73:141-147.
23. Gekakis N, Staknis D, Nguyen HB, et al. Role of the CLOCK protein inthe mammalian circadian mechanism. Science. 1998;280:1564-1569.24. Berson DM, Dunn FA, Takao M. Phototransduction by retinal ganglioncells that set circadian clock. Science. 2002;295:1070-1073.25. Provencio I, Rodriguez IR, Jiang G, Hayes WP, Moreira EF, Rollag MD. Anovel human opsin in the inner retina. J Neurosci. 2000;20:600-605.26. Moore RY, Lenn NJ. A retinohypothalamic projection in the rat. J CompNeurol. 1972;146:1-14.27. Schwartz WJ, Davidsen LC, Smith CB. In vivo metabolic activity of aputative circadian oscillator, the rat suprachiasmatic nucleus. J Comp Neurol.1980;189:157-167.28. Schwartz WJ, Gainer H. Localization of the "biological clock" in thebrain. JAMA. 1981;246:681.29. Illnerová H. Melatonin in rat pineal gland and serum; rapid paralleldecline after light exposure at night. Neurosci Lett. 1978;189-193.30. Lewy AJ, Sack RL, Singer CM. Immediate and delayed effects of brightlight on human melatonin production: shifting "dawn" and "dusk" shiftsthe dim light melatonin onset (DLMO). Ann N Y Acad Sci. 1985;453:253-259.31. Aschoff J. Annual rhythms in man. In: Aschoff J, ed. Handbook ofBehavioral Neurobiology. New York, NY: Plenum Press; 1981:475-487.32. Wehr TA, Aeschbach D, Duncan WC. Evidence for a biological dawnand dusk in the human circadian timing system. J Physiol. 2001:937-951.33. Lewy AJ, Sack RL, Fredrickson RH, Reaves M, Denney D, Zielske DR. Theuse of bright light in the treatment of chronobiologic sleep and mood dis-orders: the phase-response curve. Psychopharmacol Bull. 1983;19:523-525.34. Wever R, Polasek J, Wildgruber C. Bright light affects human circadianrhythms. Eur J Physiol. 1983;396:85-87.35. Lewy AJ, Sack RL, Singer CM. Assessment and treatment of chronobio-logic disorders using plasma melatonin levels and bright light exposure: theclock-gate model and the phase response curve. Psychopharmacol Bull.1984;20:561-565.36. Lewy AJ, Sack RL, Miller S, Hoban TM. Antidepressant and circadianphase-shifting effects of light. Science. 1987;235:352-354.37. Czeisler CA, Allan JS, Strogatz SH, et al. Bright light resets the humancircadian pacemaker independent of the timing of the sleep-wake cycle.Science. 1986;233:667-671.38. Eastman CI, Miescke KJ. Bright light improves the entrainment of thecircadian body temperature rhythm to a 26-h sleep-wake schedule inhumans. Sleep Res. 1986;15:271.39. Lewy AJ. Melatonin secretion as a neurobiological "marker" and effectsof light in humans. Psychopharmacol Bull. 1982;18:127-129.
Clinical applications of melatonin - Lewy Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
411
Experiencia clínica con melatonina en lostrastornos circadianos
Los síndromes y trastornos cronobiológicos incluyenel trastorno afectivo estacional (TAE), la cegueratotal, los síndromes de avance y retraso de fases delsueño, el jet lag y la mala adaptación a los turnoslaborales. Estos trastornos se tratan ajustando lasfases circadianas, mediante la utilización de untiempo apropiado de exposición a la luz brillante yla administración de melatonina (en dosis de 0,5 mgo menos). En algunos casos puede ser necesariomedir las fases circadianas internas utilizando elperíodo en que se elevan los niveles de melatoninaendógena.
Applications cliniques de la mélatonine dansles troubles circadians
Les syndromes et troubles chronobiologiquesregroupent le trouble affectif saisonnier (TAS), lesdesordres entraînés par la cécité totale, les syn-dromes type retard ou avance de phase, les symp-tômes liés aux changements de fuseaux horaires (jetlag), et les perturbations dues au travail posté. Cestroubles sont traités en réajustant le rythme circa-dien, grâce à l’utilisation judicieuse et minutée del’exposition à la lumière brillante et à l’administra-tion de mélatonine (0,5 mg ou moins). Parfois, ilsemble nécessaire de mesurer le rythme circadieninterne, au moment de l’élévation des concentra-tions de mélatonine endogène.

40. Lewy AJ. Human melatonin secretion (II): a marker for the circadian sys-tem and the effects of light. In: Post RM, Ballenger JC, ed. Neurobiology ofMood Disorders. Baltimore, Md: Williams and Wilkins; 1984:215-226.41. Lewy AJ, Bauer VK, Hasler BP, Kendall AR, Pires MLN, Sack RL. Capturingthe circadian rhythms of free-running blind people with 0.5 mg melatonin.Brain Res. 2001;918:96-100.42. Lewy AJ, Cutler NL, Sack RL. The endogenous melatonin profile as amarker for circadian phase position. J Biol Rhythms. 1999;14:227-236.43. Lewy AJ, Sack RL. The dim light melatonin onset (DLMO) as a markerfor circadian phase position. Chronobiol Int. 1989;6:93-102.44. Lewy AJ, Bauer VK, Ahmed S, et al. The human phase response curve(PRC) to melatonin is about 12 hours out of phase with the PRC to light.Chronobiol Int. 1998;15:71-83.45. Lewy AJ, Bauer VK, Cutler NL, et al. Morning versus evening light treat-ment of patients with winter depression. Arch Gen Psychiatry. 1998;55:890-896.46. Aschoff J, Hoffmann K, Pohl H, Wever R. Re-entrainment of circadianrhythms after phase shifts of the zeitgeber. Chronobiologia. 1975;2:23-78.47. Lewy AJ. Regulation of melatonin production in humans by bright arti-ficial light: evidence for a clock-gate model and a phase response curve.In: Brown GM, Wainwright SD, ed. The Pineal Gland: Endocrine Aspects.Advances in the Biosciences. Oxford, UK: Pergamon Press; 1985:203-208.48. Honma K, Honma S. A human phase response curve for bright lightpulses. Jpn J Psychiatry. 1988;42:167-168.49. Czeisler CA, Kronauer RE, Allan JS, et al. Bright light induction of strong(type O) resetting of the human circadian pacemaker. Science.1989;244:1328-1333.50. Wever RA. Light effects on human circadian rhythms. A review ofrecent Andechs experiments. J Biol Rhythms. 1989;4:161-186.51. Minors DS, Waterhouse JM, Wirz-Justice A. A human phase-responsecurve to light. Neurosci Lett. 1991;133:36-40.52. Eastman CI. Bright light on the night shift: circadian rhythms canadvance or delay. Sleep Res. 1991;20:453.53. Lewy AJ, Wehr TA, Goodwin FK, Newsome DA, Markey SP. Light sup-presses melatonin secretion in humans. Science. 1980;210:1267-1269.54. Lewy AJ, Kern HA, Rosenthal NE, Wehr TA. Bright artificial light treat-ment of a manic-depressive patient with a seasonal mood cycle. Am JPsychiatry. 1982;139:1496-1498.55. Rosenthal NE, Sack DA, Gillin JC, et al. Seasonal affective disorder: adescription of the syndrome and preliminary findings with light therapy.Arch Gen Psychiatry. 1984;41:72-80.56. Kripke DF, Risch SC, Janowsky D. Effect on depression of early awak-ening and bright light. Sleep Res. 1982;11:123.57. Parry BL, Maurer E. Light treatment of mood disorders. Dialogues ClinNeurosci. 2003;5:353-365.58. Wirz-Justice A. Chronobiology and mood disorders. Dialogues ClinNeurosci. 2003;5:315-325.59. Praschak-Rieder N, Willeit M. Treatment of seasonal affective disorders.Dialogues Clin Neurosci. 2003;5:391-400.60. Lewy AJ, Sack RL. Minireview: light therapy and psychiatry. Proc Soc ExpBiol Med. 1986;183:11-18.61. Lewy AJ, Sack RL, Singer CM, White DM, Hoban TM. Winter depressionand the phase shift hypothesis for bright light's therapeutic effects: his-tory, theory and experimental evidence. J Biol Rhythms. 1988;3:121-134.62. Avery DH, Khan A, Dager SR, Cox GB, Dunner DL. Bright light treatmentof winter depression: morning versus evening light. Acta Psychiatr Scand.1990;82:335-338.63. Sack RL, Lewy AJ, White DM, Singer CM, Fireman MJ, Vandiver R.Morning versus evening light treatment for winter depression: evidencethat the therapeutic effects of light are mediated by circadian phase shifts.Arch Gen Psychiatry. 1990;47:343-351.64. Terman M, Terman JS, Quitkin FM, et al. Dosing dimensions of lighttherapy: duration and time of day. In: Thompson C, Silverstone T, ed.Seasonal Affective Disorder. London, UK: CNS (Clinical Neuroscience)Publishers; 1989:187-204.65. Lewy AJ. Treating chronobiologic sleep and mood disorders with brightlight. Psychiatry Ann. 1987;17:664-669.66. Thalén B-E, Kjellman BF, Mørkrid L, Wibom R, Wetterberg L. Light treatmentin seasonal and nonseasonal depression. Acta Psychiatr Scand. 1995;91:352-360.
67. Wirz-Justice A, Graw P, Krauchi K, et al. Light therapy in seasonal affec-tive disorder is independent of time of day or circadian phase. Arch GenPsychiatry. 1993;50:929-937.68. Eastman CI, Young MA, Fogg LF, Liu L, Meaden PM. Bright light treat-ment of winter depression: a placebo-controlled trial. Arch Gen Psychiatry.1998;55:883-889.69. Terman M, Terman JS, Ross DC. A controlled trial of timed bright lightand negative air ionization for treatment of winter depression. Arch GenPsychiatry. 1998;55:875-882.70. Terman M. Problems and prospects for use of bright light as a thera-peutic intervention. In: Wetterberg L, ed. Light and Biological Rhythms in Man.Stockholm, Sweden: Pergamon Press; 1993:421-436.71. Terman JS, Terman M, Lo ES, Cooper TB. Circadian time of morninglight administration and therapeutic response in winter depression. ArchGen Psychiatry. 2001;58:69-75.72. Voultsios A, Kennaway DJ, Dawson D. Salivary melatonin as a circadianphase marker: validation and comparison to plasma melatonin. J BiolRhythms. 1997;12:457-466.73. Zaidan R, Geoffriau M, Brun J, et al. Melatonin is able to influence itssecretion in humans: description of a phase-response curve. Neuro-endocrinology. 1994;60:105-112.74. Middleton B, Arendt J, Stone BM. Complex effects of melatonin onhuman circadian rhythms in constant dim light. J Biol Rhythms. 1997;12:467-477.75. Lewy AJ, Bauer VK, Cutler NL, Sack RL. Melatonin treatment of winterdepression: a pilot study. Psychiatry Res. 1998;77:57-61.76. Sack RL, Lewy AJ, Hoban TM. Free-running melatonin rhythms in blindpeople: phase shifts with melatonin and triazolam administration. In:Rensing L, an der Heiden U, Mackey MC, ed. Temporal Disorder in HumanOscillatory Systems. Heidelberg, Germany: Springer-Verlag; 1987:219-224.77. Sack RL, Keith D, Lewy AJ. Cortisol and melatonin rhythms in free-run-ning blind people have identical periods. Sleep Res. 1989;18:441.78. Nakagawa H, Sack RL, Lewy AJ. Sleep propensity free-running in par-allel with the melatonin rhythm in a totally blind person. Sleep Res.1991;20:467.79. Nakagawa H, Sack RL, Lewy AJ. Sleep propensity free-runs with thetemperature, cortisol and melatonin rhythms in a totally blind person.Sleep. 1992;15:330-336.80. Waterhouse JM, Minors DS. Masking and entrainment. In: HekkensWTJM, Kerkhof GA, Rietveld WJ, ed. Trends in Chronobiology. Oxford, UK:Pergamon; 1988:163-171.81. Sack RL, Lewy AJ, Blood ML, Keith LD, Nakagawa H. Circadian rhythmabnormalities in totally blind people: incidence and clinical significance. JClin Endocr Metab. 1992;75:127-134.82. Lockley SW, Skene DJ, Arendt J. Changes in sleep in relation to circa-dian phase in the blind. In: Touitou Y, ed. Biological Clocks. Mechanisms andApplications. Amsterdam, The Netherlands: Elsevier; 1998:247-252.83. Skene DJ, Lockley SW, Arendt J. Melatonin in circadian sleep disordersin the blind. Biol Signals Receptors. 1999;8:90-95.84. Lewy AJ. Human plasma melatonin studies: effects of light and impli-cations for biological rhythm research. In: Birau N, Scholoot W, ed.Melatonin: Current Status and Perspectives. Advances in the Biosciences. Oxford,UK: Pergamon Press; 1981:397-400.85. Lewy AJ, Newsome DA. Different types of melatonin circadian secre-tory rhythms in some blind subjects. J Clin Endocrinol Metab. 1983;56:1103-1107.86. Redman J, Armstrong S, Ng KT. Free-running activity rhythms in the rat:entrainment by melatonin. Science. 1983;219:1089-1091.87. Sack RL, Brandes RW, Kendall AR, Lewy AJ. Entrainment of free-run-ning circadian rhythms by melatonin in blind people. N Engl J Med.2000;343:1070-1077.88. Sack RL, Stevenson J, Lewy AJ. Entrainment of a previously free-run-ning blind human with melatonin administration. Sleep Res. 1990;19:404.89. Sack RL, Lewy AJ. Melatonin administration phase advances endoge-nous rhythms in humans. Sleep Res. 1988;17:396.90. Sack RL, Lewy AJ, Blood ML, Stevenson J, Keith LD. Melatonin admin-istration to blind people: phase advances and entrainment. J Biol Rhythms.1991;6:249-261.
C l i n i c a l r e s e a r c h
412

91. Sack RL, Brandes RL, DeJongh EA, Pen S, Nordstrom S, Lewy AJ.Melatonin entrains free-running circadian rhythms in a totally blind per-son. Sleep. 1999;22(suppl):S138.92. Lewy AJ, Emens JS, Sack RL, Hasler BP, Bernert RA. Low, but not high,doses of melatonin entrained a free-running blind person with a long cir-cadian period. Chronobiol Int. 2002;19:649-658.93. Lewy AJ, Hasler BP, Emens JS, Sack RL. Pretreatment circadian period infree-running blind people may predict the phase angle of entrainment tomelatonin. Neurosci Lett. 2001;313:158-160.94. Lewy AJ, Bauer BK, Singer CW, Minkunas DV, Sack RL. Later circadianphase of plasma melatonin relative to usual waketime in older subjects.Sleep. 2000;23(suppl 2):A188.95. Gekakis N, Saez L, Delahaye-Brown A, et al. Isolation of timeless by PERprotein interaction: defective interaction between timeless protein andlong-period mutant PER. Science. 1995;270:811-815.96. Young MW. The tick-tock of the biological clock. Sci Am. 2000:64-71.97. Berson DM, Dunn FA, Takao M. Phototransduction by retinal ganglioncells that set circadian clock. Science. 2002;295:1070-1073.98. Pittendrigh CS, Daan S. A functional analysis of circadian pacemakersin nocturnal rodents: IV. Entrainment: pacemaker as a clock. J Comp Physiol.1976;106:291-331.99. Lockley SW, Skene DJ, James K, Thapan K, Wright J, Arendt J.Melatonin administration can entrain the free-running circadian system ofblind subjects. J Endocrinol. 2000;164:R1-R6.100. Lewy AJ, Emens JS, Bernert RA, Lefler BJ. Eventual entrainment of thehuman circadian pacemaker by melatonin is independent of the circadianphase of treatment initiation: clinical implications. J Biol Rhythms. In press.101. Lewy AJ, Emens JS, Sack RL, Hasler BP, Bernert RA. Zeitgeber heirar-chy in humans: resetting the circadian phase positions of blind peopleusing melatonin. Chronobiol Int. 2003;20:837-852.
102. Dahlitz M, Alvarez B, Vignau J, English J, Arendt J, Parkes JD. Delayedsleep phase syndrome response to melatonin. Lancet. 1991;337:1121-1123.103. Rosenthal NE, Joseph-Vanderpool JR, Levendosky AA, et al.Phototherapy for delayed sleep phase syndrome. Biol Psychiatry.1991;29:40S.104. Schenck CH, Mahowald MW, Sack RL. Assessment and managementof insomnia. JAMA. 2003;289:2475-2479.105. Lewy AJ, Sack RL, Singer CM. Melatonin, light and chronobiologicaldisorders. In: Evered D, Clark S, ed. Photoperiodism, Melatonin and the Pineal.London, UK: Pitman; 1985:231-252.106. Herxheimer A, Petrie KJ. Melatonin for the prevention and treatmentof jet lag. Cochrane Library. 2002;Disk issue 4:CD001520.107. Sack RL. Shift work and jet lag. In: Lee-Chiong TL, Sateia MJ, CarskadonMA, ed. Sleep Medicine. Philadelphia, Pa: Hanley and Belfus; 2002.108. Daan S, Lewy AJ. Scheduled exposure to daylight: a potential strategyto reduce "jet lag" following transmeridian flight. Psychopharmacol Bull.1984;20:566-568.109. Arendt J, Aldhous M, Marks V. Alleviation of "jet lag" by melatonin:preliminary results of controlled double-blind trial. BMJ. 1986;292:1170.110. Eastman CI. Bright light in work-sleep schedules for shift workers:application of circadian rhythm principles. In: Rensing L, an der Heiden U,Mackey MC, ed. Temporal Disorder in Human Oscillatory Systems. New York,NY: Springer-Verlag; 1987:176-185.111. Sack RL, Blood ML, Lewy AJ. Melatonin rhythms in night shift work-ers. Sleep. 1992;15:434-441.112. Sack RL, Blood ML, Lewy AJ. Melatonin administration promotes cir-cadian adaptation to night-shift work. Sleep Res. 1994;23:509.113. Eastman CI, Martin SK. How to use light and dark to produce circa-dian adaptation to night shift work. Ann Med. 1999;31:87-98.
Clinical applications of melatonin - Lewy Dialogues in Clinical Neuroscience - Vol 5 . No. 4 . 2003
413


S u p p o r t e d b y a n e d u c a t i o n a l g r a n t f r o m S e r v i e r
w w w . s e r v i e r . c o m
in
neuroscienceclinical
Dialogu se
eDialogues in Clinical Neuroscience e-mail alert service offers the opportu-nity to receive the Contents of each issue.
www.dialogues-cns.org
NEW
is now online

416
I n s t r u c t i o n s f o r a u t h o r sAIM AND SCOPEDialogues in Clinical Neuroscience is a quarterly publication that aimsto serve as an interface between clinical neuropsychiatry and the neu-rosciences by providing state-of-the-art information and originalinsights into relevant clinical, biological, and therapeutic aspects. Eachissue addresses a specific topic, and also publishes free contributions inthe field of neuroscience as well as other non–topic-related material.
GENERAL INSTRUCTIONSManuscripts should be provided on word-processor disks (3.5-in, forIBM, IBM-compatible, or Apple computers) with three hard copies(text and figures) printed on one side of standard-sized white bondpaper, double-spaced, with 1-inch/2.5-cm margins. Pages must be num-bered. Standard typed page = 25 lines; 250 words per page.All texts should be submitted in English. In the case of translations,the text in the original language should be included.Provide black and white photograph(s) of author(s).On the title page, provide: a title (concise and informative); full namesof authors (first name, middle name initial, and last name); highest aca-demic degrees (in country-of-origin language); affiliations (names ofdepartment[s] and institution[s]) at the time the work was done; ashort running title (no more than 50 letters and spaces); keywords (5to 10); corresponding author’s complete mailing address and tele-phone, fax, and e-mail; acknowledgments.Provide an abstract in English (125-150 words) (except for Editorials,Posters, and Letters to the Editor).Abstracts that are too short or longwill be edited by the editorial department or returned to the author.Abstracts will be translated into French and Spanish by the publish-er’s editorial department.Abbreviations should be used sparingly and expanded at first men-tion. A list of selected abbreviations and acronyms should be provid-ed (or will be prepared by the editorial department) where necessary.In the text include headings using a consistent style for the various lev-els of headings, to highlight key points and facilitate comprehensionof the text. The editorial department reserves the right to add, modi-fy, or delete headings when necessary.Use SI units.Use generic names of drugs.
REFERENCES All references should be cited in the text and numbered consecutive-ly using superscript arabic numerals. Presentation of the referencesshould be based on the Uniform Requirements for Manuscripts Sub-mitted to Biomedical Journals. Ann Intern Med. 1997;126:36-47 (“Van-couver style”). The author-date system of citation is not acceptable.“In press” references should be avoided. In the bibliography, titles ofjournals should be abbreviated according to the Index Medicus. Allauthors should be listed up to six; if there are more, only the first threeshould be listed, followed by “et al.” Where necessary, references willbe styled by the editorial department to Dialogues in Clinical Neuro-science copyediting requirements.Authors bear total responsibility forthe accuracy and completeness of all references and for correct textcitation. Example of style for references:
1. Schneider LS, Olin JT, Lyness SA, Chui HC. Eligibility of Alzheimer’s diseaseclinic patients for clinical trials. J Am Geriatr Soc. 1997;45:1-6.
2. Dubovsky J, Weber JL, Orr HT, et al. A second gene for familial febrileconvulsions maps on chromosome 19p. Am J Hum Genet. 1996;59(suppl1):A223.3. Carpenter WT Jr, Buchanan RW. Domains of psychopathology relevantto the study of etiology and treatment in schizophrenia. In: Schulz SC, Tam-minga CA, eds. Schizophrenia: Scientific Progress. New York, NY: Oxford Uni-versity Press; 1989:13-22.
FIGURES AND TABLES Submit figures as two sets of clear glossy prints. Figures should be ofgood quality or professionally prepared, numbered according to theirorder, with proper orientation indicated (eg,“top” or “left”), and fullyexplicit legends provided, not repetitive of text.All abbreviations usedshould be expanded in the legends.As figures and graphs may need tobe reduced or enlarged, all absolute values and statistics should beprovided. Illustrations will be reproduced in full color only when clear-ly necessary, eg, images from nuclear medicine or histology. Provideeach table on a separate sheet, with title above and description below.All figures and tables should be cited in the text, with distinct num-bering for figures and tables.
SPECIFIC FORMATS Editorial: no more than 400 words.
Pharmacological aspects; Clinical research; Basic research: 3000-5000 words (exclusive of abstract, references, tables, and figure leg-ends).
State of the art: maximum 7000 words (exclusive of abstract, refer-ences, tables, and figure legends).
Free papers: no more than 2500 words (exclusive of abstract, refer-ences, tables, and figure legends).
Posters / images in neuroscience: take up 2 facing printed pages ofthe journal. Posters may need to be edited to meet formatting require-ments. Legends must be provided with all illustrations.
Letters to the editor: (of no more than 500 words, and including nomore than 10 references) are welcomed. Letters will be selected by theEditor, and published according to available space. Unpublished let-ters will not be returned to the authors.
EDITORIAL ASSESSMENT AND PROCESSINGAll contributions to Dialogues in Clinical Neuroscience will bereviewed by members of the Editorial Board and submitted to expertconsultants for peer review.
All contributions to Dialogues in Clinical Neuroscience will be styledby the publisher’s editorial department according to the specificationsof the current edition of the American Medical Association Manual ofStyle (Williams & Wilkins). Page proofs and editorial queries will besent to the corresponding author for approval and should be returnedwithin 48 hours by fax and express mail. If this deadline is not met, thechanges made by the editorial department will be assumed to beaccepted by the author. Authors are responsible for all statementsmade in their work, including changes made by the editorial depart-ment and authorized by the author.Articles and abstracts will be edit-ed to required length or returned to the author if specific require-ments are not complied with.
COPYRIGHTCopyright of articles will be transferred to the publisher of Dialoguesin Clinical Neuroscience. The Copyright Transfer Agreement must besigned by the main author and all coauthors and returned to the pub-lisher.
For reproduction of copyrighted work, the author is required to obtainauthorizations from the author(s) (including self) and the publisher(s)and provide copies of these authorizations with the manuscript.

Dialogu se

C o n t e n t s o f l a t e s t i s s u e s
2003 · Volume 5 · No. 3
Anxiety II
EditorialJean-Paul Macher, Marc-Antoine Crocq______________________ 201
In this issuePierre Schulz __________________________________________________ 205
State of the artThe psychobiology of resilience and vulnerability to anxiety disorders: implications for prevention and treatmentDennis S. Charney ____________________________________________ 207
Basic researchEvolutionary aspects of anxiety disorders John S. Price __________________________________________________ 223
Pharmacological aspectsMedication dependence and anxietyLisa L. Von Moltke, David J. Greenblatt ____________________ 237
PosterfMRI in anxietyThérèse Schunck, Gilles Erb, Christian Gilles, Yann Hode,Izzie J. Namer, Hermann Fuder, Rémy Luthringer __________ 246
Clinical researchSleep and anxiety disordersLuc Staner______________________________________________________ 249
Obsessive-compulsive spectrum disordersAndrea Allen, Audrey King, Eric Hollander ________________ 259
Psychological and social aspects of resilience:a synthesis of risks and resourcesSaul Levine ____________________________________________________ 273
Free paperCombination pharmacotherapy in Alzheimer’s diseaseJacobo Mintzer, Dena Armstrong, Warachal E. Faison ______ 281
2003 · Volume 5 · No. 4
Chronobiology and Mood Disorders
EditorialJean-Paul Macher, Marc-Antoine Crocq______________________ 309
In this issueManfred Ackenheil ____________________________________________ 313
State of the artChronobiology and mood disordersAnna Wirz-Justice ____________________________________________ 315
Concepts in human biological rhythmsAlain Reinberg, Israel Ashkenazi ____________________________ 327
Basic researchMelatonin and animal models Paul Pévet______________________________________________________ 343
Pharmacological aspectsLight treatment of mood disordersBarbara L. Parry, Eva L. Maurer ____________________________ 353
PosterSleep deprivation and antidepressant treatmentUlrich Voderholzer ____________________________________________ 366
Clinical researchDiagnosis and treatment of sleep disorders:a brief review for cliniciansVivien C. Abad, Christian Guilleminault______________________ 371
Treatment of seasonal affective disordersNicole Praschak-Rieder, Matthäus Willeit ____________________ 389
Clinical applications of melatonin in circadian disordersAlfred J. Lewy__________________________________________________ 399
eEditor in Chief: Jean-Paul MACHER
For information on this journal contact: Dr Marc-Antoine CROCQ FORENAP - Institute for Research in Neuroscience and Neuropsychiatry - BP29 - 68250 Rouffach - France
Tel: +33 3 89 78 71 20 / 70 18 - Fax: +33 3 89 78 51 24 - E-mail: [email protected]
If you wish to receive future issues of Dialogues in Clinical Neuroscience, please [email protected]
This publication is supported by an educational grant from Servier — www.servier.com
www.dialogue-cns.org
04S
T01
7 B
A